Embed Size (px)
Citation preview

Porcine Xenograft ValvesLong-term (60-89-month) Follow-up
JEFFREY B. LAKIER, M.D., FAREED KHAJA, M.D., DONALD J. MAGILLIGAN, JR., M.D.,
AND SIDNEY GOLDSTEIN, M.D.
SUMMARY An analysis of 211 patients who had porcine xenograft valve replacements at Henry FordHospital between October 1971 and March 1974, was accomplished, with 100% follow-up. The follow-upperiod extended from 60-89 months after implantation. One hundred sixty-seven patients with 192 valves sur-vived the perioperative period and were subjected to life table analysis. Hemodynamically significant porcinexenograft degeneration that required reoperation occurred in 18 patients, two of whom had infective endocar-ditis. Only four valves failed within 48 months of surgery. Ten of 42 (23.8%) patients with isolated aortic valvereplacement and eight of 102 patients (7.8%) patients with isolated mitral valve replacement required reopera-tion (p < 0.01). In patients under 25 years of age, six of nine surviving patients had repeat operations. Ourdata indicate that porcine xenograft degeneration is related to the duration of implantation and the age of thepatient at the time implantation was performed. In addition, porcine xenograft valves in the aortic position aremore likely to degenerate than are those in the mitral position.
THE GLUTERALDEHYDE-prepared porcine xeno-graft is one of the most encouraging valve substitutesavailable. The initial highly satisfactory resultsreported with this prosthesis have resulted in its usefor replacement of diseased aortic, mitral andtricuspid valves.' Although the porcine xenograftvalve has good hemodynamic features and a lowthromboembolic rate," 3' 4it has the same potentialfor late degeneration as other bioprosthetic valves.6Recent reports have suggested a low incidence ofdegeneration in adult patients7 and a higher rate inchildren.8 We recently described the echocardio-graphic characteristics of degenerated porcine xeno-grafts.9 Because of these observations we analyzed thefirst 211 patients in whom a gluteraldehyde porcinexenograft was implanted at this institution. Thisenabled us to obtain a minimum 5-year follow-up inorder to assess the long-term durability of the valve.
Methods
Two hundred eleven patients received 252 porcinevalve xenografts between October 1971 and March1974. All deaths during the initial hospitalization andup to I month postoperatively were considered peri-operative deaths, and accounted for 44 patients. Therewere 167 surviving patients with 192 valves 1 monthafter surgery. Information on all these was obtainedregarding cardiac status, hospital admissions aftervalve replacement, evidence of thromboembolicepisodes and current medication. A further 42 patientsdied during the follow-up period, leaving 125 patientsalive at the end of the study (March 1979). Of these,112 patients were evaluated at Henry Ford Hospital
From the Divisions of Cardiovascular Medicine and Cardiac andThoracic Surgery, Henry Ford Hospital, Detroit, Michigan.
Address for correspondence: Jeffrey B. Lakier, M.D., HenryFord Hospital, 2799 West Grand Boulevard, Detroit, Michigan48202.
Received July 19, 1979; revision accepted January 8, 1980.Circulation 62, No. 2, 1980.
during a closing period (January through March1979). The remaining 13 patients were unable toreturn for follow-up examination, but 12 were con-tacted by telephone and one by letter. If any symp-toms were reported the patient's physician was con-tacted.
Xenograft valve failure was diagnosed if there wasdisruption or distortion of the valve mechanism result-ing in a hemodynamic lesion necessitating xenograftreplacement. All patients included under this defini-tion of xenograft dysfunction thus had the valvesreplaced.
In this paper we assess the long-term durability ofthe porcine xenograft. Hence, the I-month mortalityor perioperative mortality is not included in long-termsurvival statistics. Several reports3' and our currentexperience indicate that there is no difference inperioperative mortality when using xenografts com-pared with other valve prostheses. Patients who de-veloped infective endocarditis and died during thecourse of therapy and in whom the cause of death wasnot due primarily to valve failure are not included inthe definition of valve dysfunction. Also, patients whodied without a necropsy being performed are not in-cluded as valve failures. Both of these groups are in-cluded in the overall mortality. Systemic thromboem-bolism was diagnosed if a persistent neurologic deficitoccurred postoperatively or if absent or diminishedperipheral pulses were noted. Bland systemic embolito other viscera were not noted in this series.
Patients with large left atria and those with atrialfibrillation were anticoagulated and were maintainedindefinitely on warfarin unless bleeding complicationsoccurred.
Statistical analysis comparing the rate of reopera-tion in the mitral and aortic groups was done using thechi-square method for cumulative actuarial analysis,based on a generalized Kruskal-Wallis test.'0 Statis-tical analysis comparing valve degeneration betweenthe younger patients (younger than 25 years) and olderpatients (older than 25 years) was done using standardchi-square testing.
313
by guest on July 4, 2018http://circ.ahajournals.org/
Dow
nloaded from
VOL 62, No 2, AUGUST 1980
Results
There were 192 porcine xenograft valve insertions inthe 167 patients who survived longer than 1 month.One hundred two patients had mitral valvereplacements, 42 aortic, 13 mitral and aortic, eightmitral and tricuspid and two mitral, aortic andtricuspid. Thus, 125 mitral, 57 aortic and 10 tricuspidporcine xenograft valves were followed long-term. Theage range of the patients was 8-77 years (mean age 50years). Nine patients were under 25 years. One hun-dred seventeen patients were female. At the end of thefollow-up period, 84 patients with mitral, 27 with aor-tic, eight with aortic and mitral, one with mitral, aor-tic and tricuspid and five with mitral and tricuspidporcine xenografts (total 125 patients) were alive.
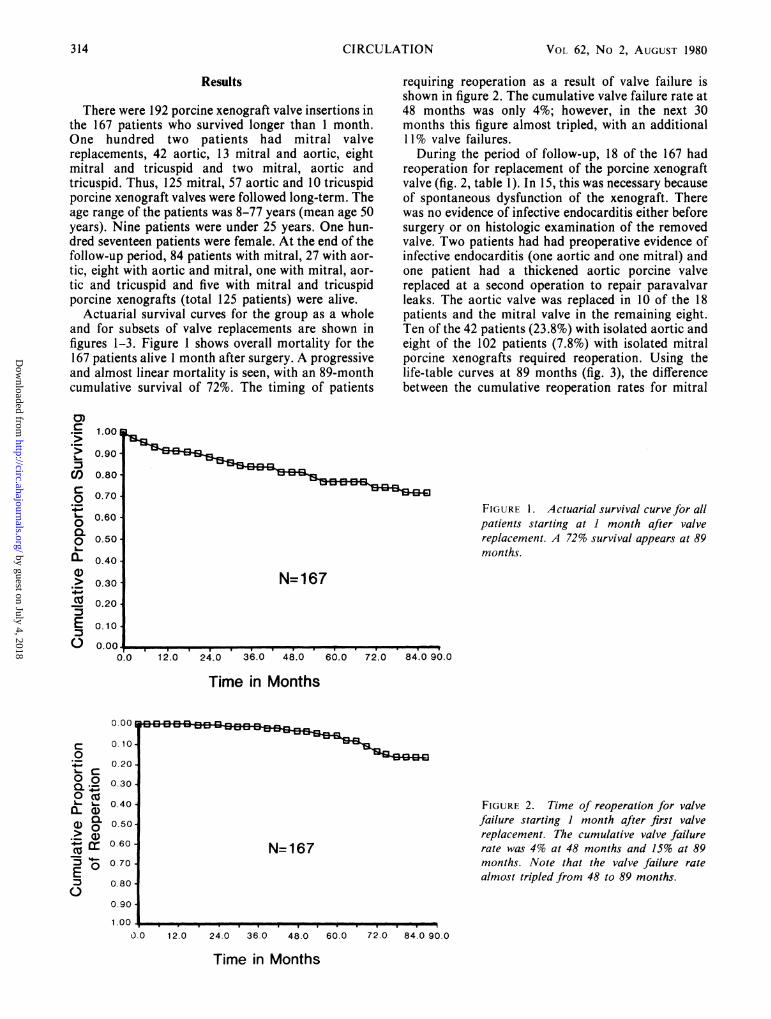
Actuarial survival curves for the group as a wholeand for subsets of valve replacements are shown infigures 1-3. Figure 1 shows overall mortality for the167 patients alive 1 month after surgery. A progressiveand almost linear mortality is seen, with an 89-monthcumulative survival of 72%. The timing of patients
requiring reoperation as a result of valve failure isshown in figure 2. The cumulative valve failure rate at48 months was only 4%; however, in the next 30months this figure almost tripled, with an additional11% valve failures.During the period of follow-up, 18 of the 167 had
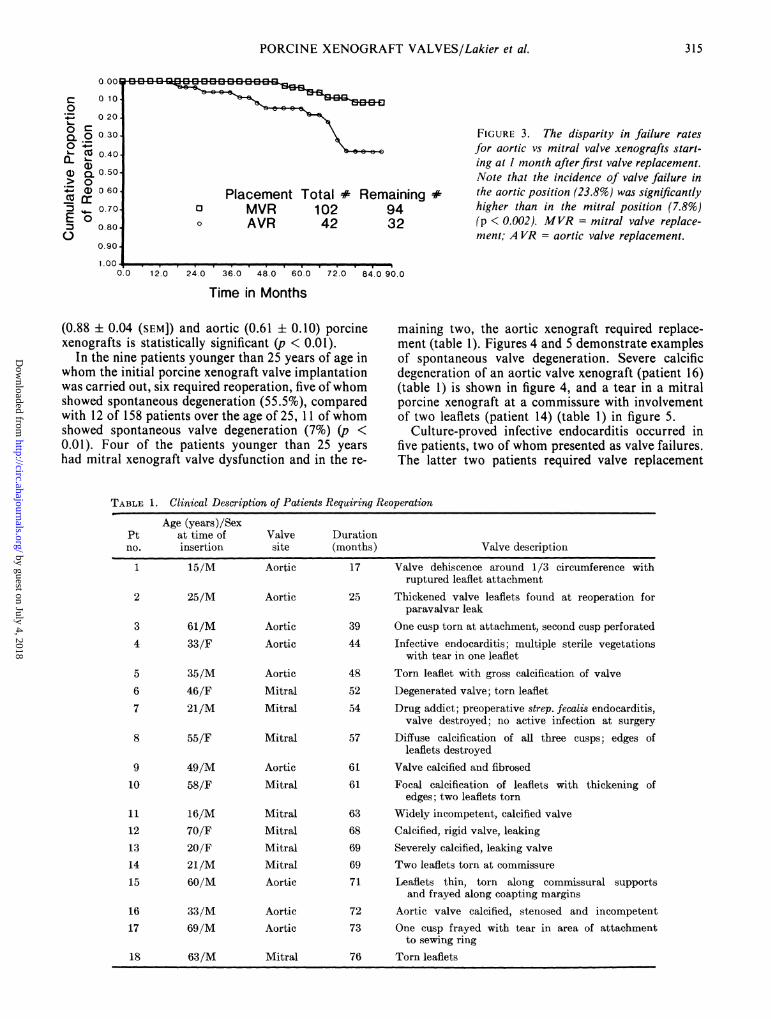
reoperation for replacement of the porcine xenograftvalve (fig. 2, table 1). In 15, this was necessary becauseof spontaneous dysfunction of the xenograft. Therewas no evidence of infective endocarditis either beforesurgery or on histologic examination of the removedvalve. Two patients had had preoperative evidence ofinfective endocarditis (one aortic and one mitral) andone patient had a thickened aortic porcine valvereplaced at a second operation to repair paravalvarleaks. The aortic valve was replaced in 10 of the 18patients and the mitral valve in the remaining eight.Ten of the 42 patients (23.8%) with isolated aortic andeight of the 102 patients (7.8%) with isolated mitralporcine xenografts required reoperation. Using thelife-table curves at 89 months (fig. 3), the differencebetween the cumulative reoperation rates for mitral
FIGURE 1. Actuarial survival curve for allpatients starting at 1 month after valvereplacement. A 72% survival appears at 89months.
N=167
Time in Months
--rl E4n3~ 33
N=167
FIGURE 2. Time of reoperation for valvefailure starting 1 month after first valvereplacement. The cumulative valve failurerate was 4% at 48 months and 15% at 89months. Note that the valve failure ratealmost tripled from 48 to 89 months.
0 . 0. 2 4 60.
O 0 12.0 24.0 36.0 48.0 60.0
Time in Months
0)
CO
L.0
0~
0a-
E
1.00
0.90
0.80
0.70
0.60
0.50
0.40
0.30
0.20
0.10
0.000..0 12.0 24.0 36.0 48.0 60.0 72.0 84.0 90.0
0.00
C 0.100
0.20L-C:
.2 0.30COm L 0.40
a) O 0.50.> CLX z 060D3 O~ 0.70
E 0.800.so
0.90
1.UV 1 .
72.0 84.0 90.0
314 CIRCULATION
E3 E3 E3 E3
1
by guest on July 4, 2018http://circ.ahajournals.org/
Dow
nloaded from
PORCINE XENOGRAFT VALVES/Lakier et al.
Remaining #9432
FIGURE 3. The disparity in failure ratesfor aortic vs mitral valve xenografts start-ing at I month after first valve replacement.Note that the incidence of valve failure inthe aortic position (23.8%) was significantlyhigher than in the mitral position (7.8%)(p < 0.002). MVR = mitral valve replace-ment; A VR = aortic valve replacement.
._
0.0 12.0 24.0 36.0 48.0 60.0 72.0 84.0 90.0
Time in Months
(0.88 ± 0.04 (SEM]) and aortic (0.61 ± 0.10) porcinexenografts is statistically significant (p < 0.01).
In the nine patients younger than 25 years of age inwhom the initial porcine xenograft valve implantationwas carried out, six required reoperation, five ofwhomshowed spontaneous degeneration (55.5%), comparedwith 12 of 158 patients over the age of 25, 1 1 of whomshowed spontaneous valve degeneration (7%) (p <0.01). Four of the patients younger than 25 yearshad mitral xenograft valve dysfunction and in the re-
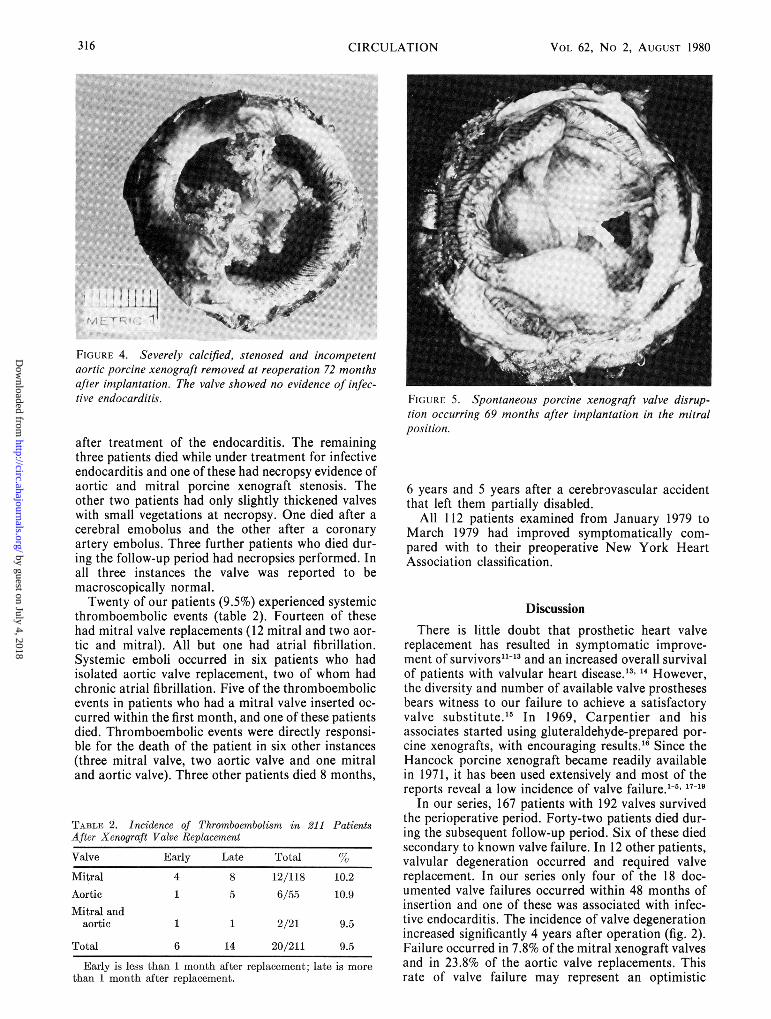
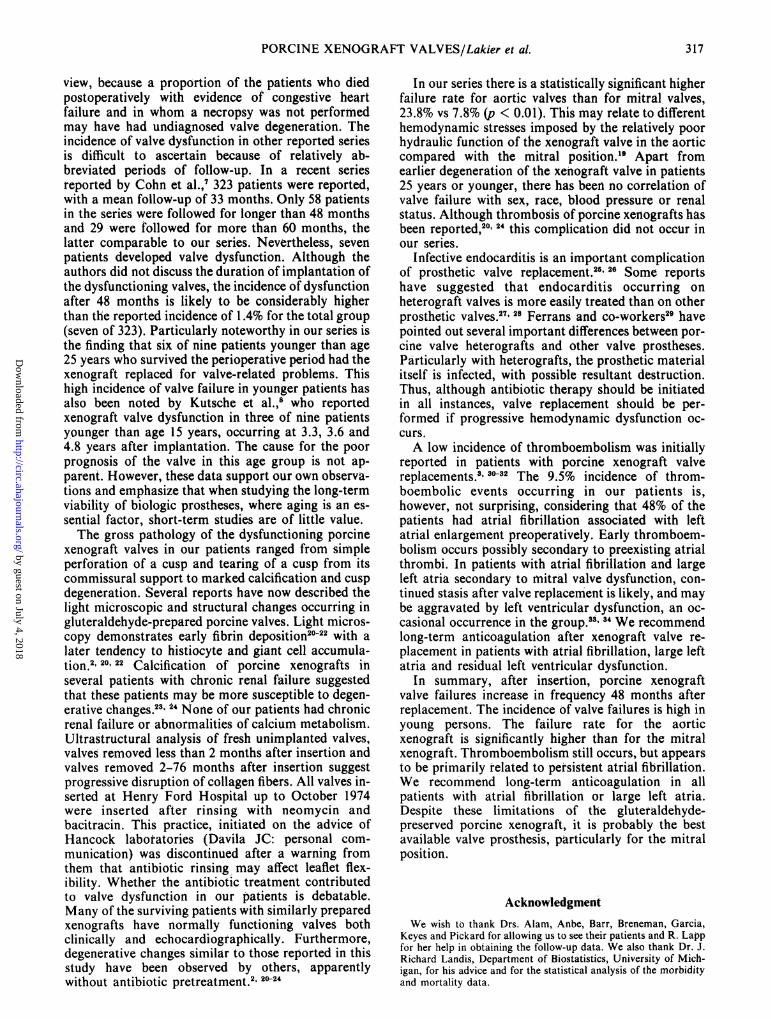
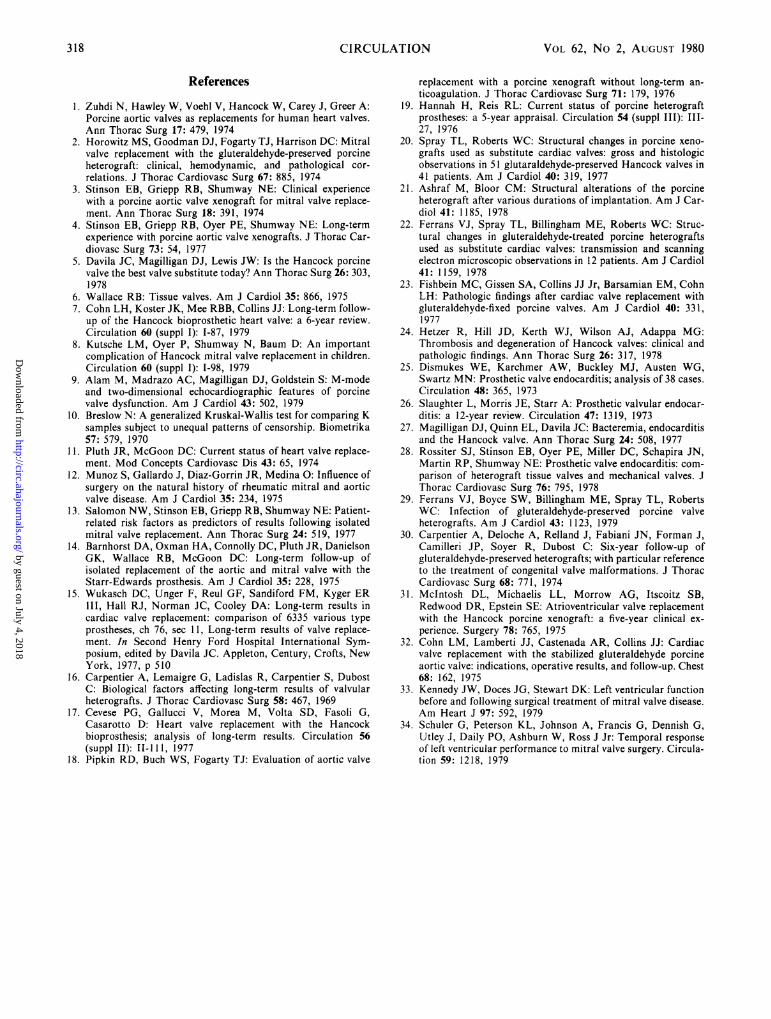
maining two, the aortic xenograft required replace-ment (table 1). Figures 4 and 5 demonstrate examplesof spontaneous valve degeneration. Severe calcificdegeneration of an aortic valve xenograft (patient 16)(table 1) is shown in figure 4, and a tear in a mitralporcine xenograft at a commissure with involvementof two leaflets (patient 14) (table 1) in figure 5.
Culture-proved infective endocarditis occurred infive patients, two of whom presented as valve failures.The latter two patients required valve replacement
TABLE 1. Clinical Description of Patients Requiring ReoperationAge (years)/Sex
Pt at time of Valve Durationno. insertion site (months) Valve description
1 15/M Aortic 17 Valve dehiscence around 1/3 circumference withruptured leaflet attachment
2 25/M Aortic 25 Thickened valve leaflets found at reoperation forparavalvar leak
3 61/M Aortic 39 One cusp torn at attachment, second cusp perforated4 33/F Aortic 44 Infective endocarditis; multiple sterile vegetations
with tear in one leaflet5 35/M Aortic 48 Torn leaflet with gross calcification of valve6 46/F Mitral 52 Degenerated valve; torn leaflet7 21/M Mitral 54 Drug addict; preoperative strep. fecalis endocarditis,
valve destroyed; no active infection at surgery8 55/F Mitral 57 Diffuse calcification of all three cusps; edges of
leaflets destroyed9 49/M Aortic 61 Valve calcified and fibrosed10 58/F Mitral 61 Focal calcification of leaflets with thickening of
edges; two leaflets torn11 16/M Mitral 63 Widely incompetent, calcified valve12 70/F Mitral 68 Calcified, rigid valve, leaking13 20/F Mitral 69 Severely calcified, leaking valve14 21/M Mitral 69 Two leaflets torn at commissure15 60/M Aortic 71 Leaflets thin, torn along commissural supports
and frayed along coapting margins16 33/M Aortic 72 Aortic valve calcified, stenosed and incompetent17 69/M Aortic 73 One cusp frayed with tear in area of attachment
to sewing ring18 63/M Mitral 76 Torn leaflets
c0
0CL
00-a)
cc-5
E0
o .oo
o. 10
0 20
O 0 30CO 0.40a)a) 0 500W) 0 60crM 0 70.0
0.80.
0.90-
1 .00
0
PlacementMVRAVR
Total #10242
r r%pifl ri rl -| r el m p1. E3 E3 lid~
q. 1 1 _.
315
F4 5;4 gzl gzl E3 E3 E3 E3 El
by guest on July 4, 2018http://circ.ahajournals.org/
Dow
nloaded from
VOL 62, No 2, AUGUST 1980
j;
FIGURE 4. Severely calcified, stenosed and incompetentaortic porcine xenograft removed at reoperation 72 monthsafter implantation. The valve showed no evidence of infec-tive endocarditis.
after treatment of the endocarditis. The remainingthree patients died while under treatment for infectiveendocarditis and one of these had necropsy evidence ofaortic and mitral porcine xenograft stenosis. Theother two patients had only slightly thickened valveswith small vegetations at necropsy. One died after acerebral emobolus and the other after a coronaryartery embolus. Three further patients who died dur-ing the follow-up period had necropsies performed. Inall three instances the valve was reported to bemacroscopically normal.Twenty of our patients (9.5%) experienced systemic
thromboembolic events (table 2). Fourteen of thesehad mitral valve replacements (12 mitral and two aor-tic and mitral). All but one had atrial fibrillation.Systemic emboli occurred in six patients who hadisolated aortic valve replacement, two of whom hadchronic atrial fibrillation. Five of the thromboembolicevents in patients who had a mitral valve inserted oc-curred within the first month, and one of these patientsdied. Thromboembolic events were directly responsi-ble for the death of the patient in six other instances(three mitral valve, two aortic valve and one mitraland aortic valve). Three other patients died 8 months,
TABLES 2. Incidence of Thromboembolism in 211 PatientsAfter Xenograft Valve Replacement
Valve Early Late Total
Mitral 4 8 12/118 10.2Aortic 1 5 6/55 10.9Mitral and
aortic 1 1 2/21 9.5
Total 6 14 20/211 9.5
Early is less than 1 month after replacement; late is morethan 1 month after replacement.
FIGURE 5. Spontaneous porcine xenograft valve disrup-tion occurring 69 months after implantation in the mitralposition.
6 years and 5 years after a cerebrovascular accidentthat left them partially disabled.
All 112 patients examined from January 1979 toMarch 1979 had improved symptomatically com-pared with to their preoperative New York HeartAssociation classification.
DiscussionThere is little doubt that prosthetic heart valve
replacement has resulted in symptomatic improve-ment of survivors"-" and an increased overall survivalof patients with valvular heart disease.'3' ` However,the diversity and number of available valve prosthesesbears witness to our failure to achieve a satisfactoryvalve substitute.'5 In 1969, Carpentier and hisassociates started using gluteraldehyde-prepared por-cine xenografts, with encouraging results.'6 Since theHancock porcine xenograft became readily availablein 1971, it has been used extensively and most of thereports reveal a low incidence of valve failure.'-5 17-19
In our series, 167 patients with 192 valves survivedthe perioperative period. Forty-two patients died dur-ing the subsequent follow-up period. Six of these diedsecondary to known valve failure. In 12 other patients,valvular degeneration occurred and required valvereplacement. In our series only four of the 18 doc-umented valve failures occurred within 48 months ofinsertion and one of these was associated with infec-tive endocarditis. The incidence of valve degenerationincreased significantly 4 years after operation (fig. 2).Failure occurred in 7.8% of the mitral xenograft valvesand in 23.8% of the aortic valve replacements. Thisrate of valve failure may represent an optimistic
316 CIRCULATION
by guest on July 4, 2018http://circ.ahajournals.org/
Dow
nloaded from
PORCINE XENOGRAFT VALVES/Lakier et al.
view, because a proportion of the patients who diedpostoperatively with evidence of congestive heartfailure and in whom a necropsy was not performedmay have had undiagnosed valve degeneration. Theincidence of valve dysfunction in other reported seriesis difficult to ascertain because of relatively ab-breviated periods of follow-up. In a recent seriesreported by Cohn et al.,7 323 patients were reported,with a mean follow-up of 33 months. Only 58 patientsin the series were followed for longer than 48 monthsand 29 were followed for more than 60 months, thelatter comparable to our series. Nevertheless, sevenpatients developed valve dysfunction. Although theauthors did not discuss the duration of implantation ofthe dysfunctioning valves, the incidence of dysfunctionafter 48 months is likely to be considerably higherthan the reported incidence of 1.4% for the total group(seven of 323). Particularly noteworthy in our series isthe finding that six of nine patients younger than age25 years who survived the perioperative period had thexenograft replaced for valve-related problems. Thishigh incidence of valve failure in younger patients hasalso been noted by Kutsche et al.,8 who reportedxenograft valve dysfunction in three of nine patientsyounger than age 15 years, occurring at 3.3, 3.6 and4.8 years after implantation. The cause for the poorprognosis of the valve in this age group is not ap-parent. However, these data support our own observa-tions and emphasize that when studying the long-termviability of biologic prostheses, where aging is an es-sential factor, short-term studies are of little value.The gross pathology of the dysfunctioning porcine
xenograft valves in our patients ranged from simpleperforation of a cusp and tearing of a cusp from itscommissural support to marked calcification and cuspdegeneration. Several reports have now described thelight microscopic and structural changes occurring ingluteraldehyde-prepared porcine valves. Light micros-copy demonstrates early fibrin deposition20-22 with alater tendency to histiocyte and giant cell accumula-tion.2 20 22 Calcification of porcine xenografts inseveral patients with chronic renal failure suggestedthat these patients may be more susceptible to degen-erative changes.23 2' None of our patients had chronicrenal failure or abnormalities of calcium metabolism.Ultrastructural analysis of fresh unimplanted valves,valves removed less than 2 months after insertion andvalves removed 2-76 months after insertion suggestprogressive disruption of collagen fibers. All valves in-serted at Henry Ford Hospital up to October 1974were inserted after rinsing with neomycin andbacitracin. This practice, initiated on the advice ofHancock laboratories (Davila JC: personal com-munication) was discontinued after a warning fromthem that antibiotic rinsing may affect leaflet flex-ibility. Whether the antibiotic treatment contributedto valve dysfunction in our patients is debatable.Many of the surviving patients with similarly preparedxenografts have normally functioning valves bothclinically and echocardiographically. Furthermore,degenerative changes similar to those reported in thisstudy have been observed by others, apparentlywithout antibiotic pretreatment.2 20 24
In our series there is a statistically significant higherfailure rate for aortic valves than for mitral valves,23.8% vs 7.8% (p < 0.01). This may relate to differenthemodynamic stresses imposed by the relatively poorhydraulic function of the xenograft valve in the aorticcompared with the mitral position.1' Apart fromearlier degeneration of the xenograft valve in patients25 years or younger, there has been no correlation ofvalve failure with sex, race, blood pressure or renalstatus. Although thrombosis of porcine xenografts hasbeen reported,20 24 this complication did not occur inour series.
Infective endocarditis is an important complicationof prosthetic valve replacement.25 26 Some reportshave suggested that endocarditis occurring onheterograft valves is more easily treated than on otherprosthetic valves.27' 28 Ferrans and co-workers29 havepointed out several important differences between por-cine valve heterografts and other valve prostheses.Particularly with heterografts, the prosthetic materialitself is infected, with possible resultant destruction.Thus, although antibiotic therapy should be initiatedin all instances, valve replacement should be per-formed if progressive hemodynamic dysfunction oc-curs.A low incidence of thromboembolism was initially
reported in patients with porcine xenograft valvereplacements.3' 30-32 The 9.5% incidence of throm-boembolic events occurring in our patients is,however, not surprising, considering that 48% of thepatients had atrial fibrillation associated with leftatrial enlargement preoperatively. Early thromboem-bolism occurs possibly secondary to preexisting atrialthrombi. In patients with atrial fibrillation and largeleft atria secondary to mitral valve dysfunction, con-tinued stasis after valve replacement is likely, and maybe aggravated by left ventricular dysfunction, an oc-casional occurrence in the group.33' 4' We recommendlong-term anticoagulation after xenograft valve re-placement in patients with atrial fibrillation, large leftatria and residual left ventricular dysfunction.
In summary, after insertion, porcine xenograftvalve failures increase in frequency 48 months afterreplacenment. The incidence of valve failures is high inyoung persons. The failure rate for the aorticxenograft is significantly higher than for the mitralxenograft. Thromboembolism still occurs, but appearsto be primarily related to persistent atrial fibrillation.We recommend long-term anticoagulation in allpatients with atrial fibrillation or large left atria.Despite these limitations of the gluteraldehyde-preserved porcine xenograft, it is probably the bestavailable valve prosthesis, particularly for the mitralposition.
AcknowledgmentWe wish to thank Drs. Alam, Anbe, Barr, Breneman, Garcia,
Keyes and Pickard for allowing us to see their patients and R. Lappfor her help in obtaining the follow-up data. We also thank Dr. J.Richard Landis, Departnient of Biostatistics, University of Mich-igan, for his advice and for the statistical analysis of the morbidityand mortality data.
317
by guest on July 4, 2018http://circ.ahajournals.org/
Dow
nloaded from
VOL 62, No 2, AUGUST 1980
References
1. Zuhdi N, Hawley W, Voehl V, Hancock W, Carey J, Greer A:Porcine aortic valves as replacements for human heart valves.Ann Thorac Surg 17: 479, 1974
2. Horowitz MS, Goodman DJ, Fogarty TJ, Harrison DC: Mitralvalve replacement with the gluteraldehyde-preserved porcineheterograft: clinical, hemodynamic, and pathological cor-relations. J Thorac Cardiovasc Surg 67: 885, 1974
3. Stinson EB, Griepp RB, Shumway NE: Clinical experiencewith a porcine aortic valve xenograft for mitral valve replace-ment. Ann Thorac Surg 18: 391, 1974
4. Stinson EB, Griepp RB, Oyer PE, Shumway NE: Long-termexperience with porcine aortic valve xenografts. J Thorac Car-diovasc Surg 73: 54, 1977
5. Davila JC, Magilligan DJ, Lewis JW: Is the Hancock porcinevalve the best valve substitute today? Ann Thorac Surg 26: 303,1978
6. Wallace RB: Tissue valves. Am J Cardiol 35: 866, 19757. Cohn LH, Koster JK, Mee RBB, Collins JJ: Long-term follow-
up of the Hancock bioprosthetic heart valve: a 6-year review.Circulation 60 (suppl I): 1-87, 1979
8. Kutsche LM, Oyer P, Shumway N, Baum D: An importantcomplication of Hancock mitral valve replacement in children.Circulation 60 (suppl I): 1-98, 1979
9. Alam M, Madrazo AC, Magilligan DJ, Goldstein S: M-modeand two-dimensional echocardiographic features of porcinevalve dysfunction. Am J Cardiol 43: 502, 1979
10. Breslow N: A generalized Kruskal-Wallis test for comparing Ksamples subject to unequal patterns of censorship. Biometrika57: 579, 1970
11. Pluth JR, McGoon DC: Current status of heart valve replace-ment. Mod Concepts Cardiovasc Dis 43: 65, 1974
12. Munoz S, Gallardo J, Diaz-Gorrin JR, Medina 0: Influence ofsurgery on the natural history of rheumatic mitral and aorticvalve disease. Am J Cardiol 35: 234, 1975
13. Salomon NW, Stinson EB, Griepp RB, Shumway NE: Patient-related risk factors as predictors of results following isolatedmitral valve replacement. Ann Thorac Surg 24: 519, 1977
14. Barnhorst DA, Oxman HA, Connolly DC, Pluth JR, DanielsonGK, Wallace RB, McGoon DC: Long-term follow-up ofisolated replacement of the aortic and mitral valve with theStarr-Edwards prosthesis. Am J Cardiol 35: 228, 1975
15. Wukasch DC, Unger F, Reul GF, Sandiford FM, Kyger ERIII, Hall RJ, Norman JC, Cooley DA: Long-term results incardiac valve replacement: comparison of 6335 various typeprostheses, ch 76, sec 11, Long-term results of valve replace-ment. In Second Henry Ford Hospital International Sym-posium, edited by Davila JC. Appleton, Century, Crofts, NewYork, 1977, p 510
16. Carpentier A, Lemaigre G, Ladislas R, Carpentier S, DubostC: Biological factors affecting long-term results of valvularheterografts. J Thorac Cardiovasc Surg 58: 467, 1969
17. Cevese PG, Gallucci V, Morea M, Volta SD, Fasoli G,Casarotto D: Heart valve replacement with the Hancockbioprosthesis; analysis of long-term results. Circulation 56(suppl II): II-111, 1977
18. Pipkin RD, Buch WS, Fogarty TJ: Evaluation of aortic valve
replacement with a porcine xenograft without long-term an-ticoagulation. J Thorac Cardiovasc Surg 71: 179, 1976
19. Hannah H, Reis RL: Current status of porcine heterograftprostheses: a 5-year appraisal. Circulation 54 (suppl III): III-27, 1976
20. Spray TL, Roberts WC: Structural changes in porcine xeno-grafts used as substitute cardiac valves: gross and histologicobservations in 51 glutaraldehyde-preserved Hancock valves in41 patients. Am J Cardiol 40: 319, 1977
21. Ashraf M, Bloor CM: Structural alterations of the porcineheterograft after various durations of implantation. Am J Car-diol 41: 1185, 1978
22. Ferrans VJ, Spray TL, Billingham ME, Roberts WC: Struc-tural changes in gluteraldehyde-treated porcine heterograftsused as substitute cardiac valves: transmission and scanningelectron microscopic observations in 12 patients. Am J Cardiol41: 1159, 1978
23. Fishbein MC, Gissen SA, Collins JJ Jr, Barsamian EM, CohnLH: Pathologic findings after cardiac valve replacement withgluteraldehyde-fixed porcine valves. Am J Cardiol 40: 331,1977
24. Hetzer R, Hill JD, Kerth WJ, Wilson AJ, Adappa MG:Thrombosis and degeneration of Hancock valves: clinical andpathologic findings. Ann Thorac Surg 26: 317, 1978
25. Dismukes WE, Karchmer AW, Buckley MJ, Austen WG,Swartz MN: Prosthetic valve endocarditis; analysis of 38 cases.Circulation 48: 365, 1973
26. Slaughter L, Morris JE, Starr A: Prosthetic valvular endocar-ditis: a 12-year review. Circulation 47: 1319, 1973
27. Magilligan DJ, Quinn EL, Davila JC: Bacteremia, endocarditisand the Hancock valve. Ann Thorac Surg 24: 508, 1977
28. Rossiter SJ, Stinson EB, Oyer PE, Miller DC, Schapira JN,Martin RP, Shumway NE: Prosthetic valve endocarditis: com-parison of heterograft tissue valves and mechanical valves. JThorac Cardiovasc Surg 76: 795, 1978
29. Ferrans VJ, Boyce SW, Billingham ME, Spray TL, RobertsWC: Infection of gluteraldehyde-preserved porcine valveheterografts. Am J Cardiol 43: 1123, 1979
30. Carpentier A, Deloche A, Relland J, Fabiani JN, Forman J,Camilleri JP, Soyer R, Dubost C: Six-year follow-up ofgluteraldehyde-preserved heterografts; with particular referenceto the treatment of congenital valve malformations. J ThoracCardiovasc Surg 68: 771, 1974
31. McIntosh DL, Michaelis LL, Morrow AG, Itscoitz SB,Redwood DR, Epstein SE: Atrioventricular valve replacementwith the Hancock porcine xenograft: a five-year clinical ex-perience. Surgery 78: 765, 1975
32. Cohn LM, Lamberti JJ, Castenada AR, Collins JJ: Cardiacvalve replacement with the stabilized gluteraldehyde porcineaortic valve: indications, operative results, and follow-up. Chest68: 162, 1975
33. Kennedy JW, Doces JG, Stewart DK: Left ventricular functionbefore and following surgical treatment of mitral valve disease.Am Heart J 97: 592, 1979
34. Schuler G, Peterson KL, Johnson A, Francis G, Dennish G,Utley J, Daily PO, Ashburn W, Ross J Jr: Temporal responseof left ventricular performance to mitral valve surgery. Circula-tion 59: 1218, 1979
318 CIRCIJLATION
by guest on July 4, 2018http://circ.ahajournals.org/
Dow
nloaded from

J B Lakier, F Khaja, D J Magilligan, Jr and S GoldsteinPorcine xenograft valves. Long-term (60-89-month) follow-up.
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1980 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.62.2.313
1980;62:313-318Circulation.
http://circ.ahajournals.org/content/62/2/313the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on July 4, 2018http://circ.ahajournals.org/
Dow
nloaded from