-
8/9/2019 Pleural Effusion Farm
1/40
Pleural effusion
-
8/9/2019 Pleural Effusion Farm
2/40
Pleura
Mesothelial lining of
each hemithorax Derived from
embryonic coelomic
lining
Visceral pleura: lung
Parietal pleura: wall-Costal
-Diaphragmatic
-Mediastinal
-Cervical
Pleural Cavity
Potential space between visceral & parietal pleura
Capillary layer of serous fluid produced by mesothelium
Reduces friction Surface tension provides cohesion between lung
and thoracic wall
-
8/9/2019 Pleural Effusion Farm
3/40
Pleural space
A relative vacuum in the space keeps the visceraland parietal
pleurae in close proximity.
The small volume of pleural fluid, which has been
calculated at 0.1-0.2 ml/kg/day, serves as alubricant to
facilitate movement of the pleuralsurfaces against each other in
the course ofrespirations.
This small volume of fluid is maintained throughthe balance of
hydrostatic and oncotic pressureand lymphatic drainage, a
disturbance of whichmay lead to pathology.
-
8/9/2019 Pleural Effusion Farm
4/40
Physiology of the Pleural Space
Pleural fluid production : Starling force
Hydrostatic pressure : intracapillary pressure
supply parietal and visceral pleura
Oncotic pressure : related with serum protein and
pleural fluid protein
Blood supply
Parietal pleura : intercostal artery
Visceral pleura : bronchial artery
-
8/9/2019 Pleural Effusion Farm
5/40
Physiology of the Pleural Space
Venous drainage
Parietal pleura : intercostal vein
Visceral pleura : pulmonary vein
intercostal vein P. > pulmonary vein P.
Parietal pleura P. > Visceral pleura P.
fluid from capillary at parietal pleura mesothelial cell
pleural space absorb to visceral pleura
-
8/9/2019 Pleural Effusion Farm
6/40
Physiology of the Pleural Space
In human
P. in pleural space < P. in parietal and visceral pleura
Pleural fluid from both parietal and visceral pleura
Pleural space
Lymphatic opening at parietal pleura
-
8/9/2019 Pleural Effusion Farm
7/40
Physiology of the Pleural Space
From: Cretien, J, Bignon, J., Hirsch, A, eds: The Pleura in
Health and Disease.
New York: Marcel Dekker, 1985, p182.
-
8/9/2019 Pleural Effusion Farm
8/40
Pleural effusion
A pleural effusion is an abnormal collection of fluid inthe
pleural space.
resulting from excess fluid production or decreased
absorption.
most common manifestation of pleural diseasePleural effusion is
an indicator of an underlying disease
process that may be pulmonary or nonpulmonary in
origin, acute or chronic.
-
8/9/2019 Pleural Effusion Farm
9/40
Pathophysiology
Normal pleural fluid has the followingcharacteristics: Clear
ultrafiltrate of plasma that originates from the
parietal pleura
pH 7.60-7.64
Protein content less than 2% (1-2 g/dL)
Fewer than 1000 WBCs per cubic millimeter
Glucose content similar to that of plasma
Lactate dehydrogenase (LDH) less than 50% of plasma Sodium,
potassium, and calcium concentration similar
to that of the interstitial fluid
-
8/9/2019 Pleural Effusion Farm
10/40
Pathophysiology
1. increase fluid production1.1Starling force pulmonary
capillary pressure (CHF)
plasma oncotic pressure
(hypoalbuminemia,cirrhosis) transudate intrapleural pressure
(atelectasis)
1.2 capillary permeability
capillary permeability (Pneumonia,PE) exudate
1.3 fluid leakage from
Ascites Mediastinum (rupture esophagus or thoracic duct)
Retroperitoneum ( pancreatic pseudocyst)
-
8/9/2019 Pleural Effusion Farm
11/40
Pathophysiology
2. decreased absorption
Decreased lymphatic drainage or Lymphaticobstruction
(malignancy) exudate
-
8/9/2019 Pleural Effusion Farm
12/40
Differentiation of transudates and exudates
Transudates
< 0.5
< 0.6
< 2/3 the upper
limit for serum
Exudates
> 0.5
> 0.6
>2/3 the upper
limit for serum
Pleural Fluid
Pleural/serumProtein
Pleural/serum
LDH
Pleural
LDH
Lights criteria
-
8/9/2019 Pleural Effusion Farm
13/40
Transudative Pleural effusions
Congestive heart failure
Cirrhosis
Nephrotic syndrome
Peritoneal dialysis
Superior vena cava obstruction
Myxedema Urinothorax
-
8/9/2019 Pleural Effusion Farm
14/40
Exudative Pleural Effusions
Neoplastic diseases
Metastatic disease
Mesothelioma
Infectious diseases
Bacterial infections
Tuberculosis
Fungal infections
Viral infections
Parasitic infections
-
8/9/2019 Pleural Effusion Farm
15/40
Exudative Pleural Effusions
Pulmonary embolization
Gastrointestinal disease
Esophageal perforation
Pancreatic disease
Intraabdominal abscesses
Diaphragmatic hernia
After abdominal surgery
Endoscopic variceal sclerotherapy
After liver transplant
-
8/9/2019 Pleural Effusion Farm
16/40
Exudative Pleural Effusions
Collagen-vascular diseases
Rheumatoid pleuritis
Systemic lupus erythematosus
Drug-induced lupus
Immunoblastic lymphadenopathy
Sjgren's syndrome
Wegener's granulomatosis Churg-Strauss syndrome
-
8/9/2019 Pleural Effusion Farm
17/40
Exudative Pleural Effusions
Post-coronary artery bypass surgery
Asbestos exposure
Sarcoidosis Uremia
Meigs' syndrome
Yellow nail syndrome
-
8/9/2019 Pleural Effusion Farm
18/40
Exudative Pleural Effusions
Trapped lung
Radiation therapy
Post-cardiac injury syndrome
Hemothorax
Iatrogenic injury
Ovarian hyperstimulation syndrome
Pericardial disease
Chylothorax
-
8/9/2019 Pleural Effusion Farm
19/40
Exudative Pleural Effusions
Drug-induced pleural disease
Nitrofurantoin
Dantrolene
Methysergide
Bromocriptine
Procarbazine
Amiodarone
-
8/9/2019 Pleural Effusion Farm
20/40
HistoryHistory
abdominal surgery alcoholism, pancreatitis
asbestos exposure
CA
cardiac surgery : CABG uremia
cirrhosis
trauma
post EGD drug
SLE
RA
-
8/9/2019 Pleural Effusion Farm
21/40
Sign & symptom
dyspnea
pleuritic chest pain
cough
fever hemoptysis
weight loss
-
8/9/2019 Pleural Effusion Farm
22/40
-
8/9/2019 Pleural Effusion Farm
23/40
DIAGNOSIS
CXR
U/S
CT scan
Thoracentesis Pleural biopsy
-
8/9/2019 Pleural Effusion Farm
24/40
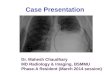
CXR
primary diagnostic tool because of its availability,accuracy,
and low cost
Pleural fluid typically collects in the pleural space on an
upright chest radiograph, primarily the posteriorcostophrenic
recess, followed by the lateral recess.
200 mL are required to cause blunting of the lateralrecess on a
posteroanterior (PA) film.
As little as 50 mL of fluid will cause blunting of theposterior
costophrenic recess on a lateral upright film.
A lateral decubitus chest radiograph may detect aslittle as 5 mL
of fluid.
-
8/9/2019 Pleural Effusion Farm
25/40
CXR
Small effusion : blunting of CP angle
Moderate effusion : meniscus sign
Massive effusion : trachea & mediastinal shiftto the
contralateral side
-
8/9/2019 Pleural Effusion Farm
26/40
Massive pleural effusion
often attributable to an underlying malignancy
Other conditions that must be considered include congestive
heart failure, tuberculosis (TB)
usually have an accompanying mediastinal shift to the
contralateral side differential diagnosis in the absence of
mediastinal shift :
carcinoma of the ipsilateral mainstem bronchus with or
without ipsilateral lung atelectasis
fixed mediastinum caused by fibrosis or tumor infiltration
ofmediastinal LN
tumor infiltration of the ipsilateral lung
malignant mesothelioma
complete atelectasis of the ipsilateral lung
-
8/9/2019 Pleural Effusion Farm
27/40
Bilateral pleural effusion
Systemic process
DDx
CHF Cirrhosis
nephrotic syndrome
hypoalbuminemia
-
8/9/2019 Pleural Effusion Farm
28/40
Unilateral pleural effusion
Local inflammation
DDx
Parapneumonic effusion
Empyema
TB
Parasitic infection
Tumor Trauma
Lymphatic obstruction
-
8/9/2019 Pleural Effusion Farm
29/40
CXR PA upright : 200 ml
-
8/9/2019 Pleural Effusion Farm
30/40
CXR lateral : 50 ml
-
8/9/2019 Pleural Effusion Farm
31/40
CXR lateral decubitus : 5 ml
-
8/9/2019 Pleural Effusion Farm
32/40
-
8/9/2019 Pleural Effusion Farm
33/40
empyema
-
8/9/2019 Pleural Effusion Farm
34/40
Lung abscess
-
8/9/2019 Pleural Effusion Farm
35/40
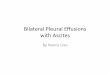
U/S
detect as little as 5-50 mL of pleural fluid
identify loculated fluid collections
guide needle insertion for thoracentesis orchest tube
placement
-
8/9/2019 Pleural Effusion Farm
36/40
-
8/9/2019 Pleural Effusion Farm
37/40
CT Scanning permits imaging of the entire pleural space,
pulmonary parenchyma and vasculature, mediastinum,and
pericardium.
Distinguishing benign from malignant pleuralinvolvement
One or more of the following suggests malignancy:
circumferential pleural thickening
nodular pleural thickening
parietal pleural thickening (>1 cm) mediastinal pleural
involvement
Distinguishing pleural disease (empyema) &pulmonary disease
(lung abscess)
-
8/9/2019 Pleural Effusion Farm
38/40
Pleural effusion
-
8/9/2019 Pleural Effusion Farm
39/40
-
8/9/2019 Pleural Effusion Farm
40/40