Embed Size (px)
Citation preview

58 Sleep Diagnosis and Therapy ♦ Vol 3 No 3 May-June 2008
Sleep Diagnosis and Therapy 2008; V3 N3, P. 58–60, Moses et al
Pilot Study Testing the Concept of Intraoral Nasal Dilation
Allen J. Moses,1 DDS, R. Gordon Klockow,2 DDS and Marcus Lieberman,3 PhD
muscles.1 The major portion of nasal resistance to inspiratoryair flow has been localized to the nasal valve. Resistance torespiratory air flow at the valve approximates half the airflowresistance of the entire respiratory system.2 Nasal dilators workagainst nasal collapsibility via the Bernoulli Principle anddecrease nasal air flow resistance via alar muscle dilation. Theeffectiveness of both external nasal dilators and intranasalmechanical dilators has been demonstrated.3,4,5
The question being tested is whether intraoral nasal dilatorscompare favorably to a gold standard, external nasal dilatorstrips (ENDS). The intraoral nasal dilators are discoid acrylicpads placed intraorally in the labial vestibule distal to the nares.They stretch the lip and thus distend the nares. Breathe RightNasal Strips® are the ENDs being utilized in this study.
The intraoral discoid shaped acrylic pads are affixed to aMandibular Advancement Device (MAD). MADs are success-fully used to treat Obstructive Sleep Apnea (OSA), hypopnea,Upper Airway Resistance Syndrome (UARS) and snoring.MADs support the tongue in a position more anterior thannormal, thus preventing collapse of the tongue on the airway.The acrylic discoid pads, 1⁄2 inch in diameter and 1⁄4 inch thick areembedded stainless steel wires extending from the buccalflanges on each side of the MAD. The dilators pads are posi-tioned in the height of the labial vestibule directly under thecuspids and slightly distal to the nares. The discoid dilatorpads are adjustable by bending the wires in or out and can beshortened by grinding on the acrylic.
MethodThis clinical study was designed to compare the efficacy ofthe ENDs vs 1⁄2 inch diameter acrylic discoid pads placed in themaxillary vestibule over the cuspids and slightly distal to thenares to stretch the lips and dilate the nostrils resulting inincreased nasal airflow. The objective measurement test deviceis an acoustic rhinometer (the ECCOVISION Acoustic Rhinometerdesigned by Hood Laboratories in Pembroke, Massachusetts). Theapparatus graphs and quantifies the patency of the nasal airwayby means of acoustic reflection; both site and degree of airwayobstruction can be determined by the simple, noninvasivediagnostic procedure.
Acoustic rhinometry is used primarily by otolaryngologists,allergists, dentists and plastic surgeons to accurately assessthe geometry of the nasal cavity. By coupling a reflection tubeto the nose and administering a series of clicks controlled bythe program, the computer-based system is able to plot thetiming and amplitudes of the reflected signal into a graph ofthe nasal airway. Applications of the technique includeassessing airway patency, the site/degree of airway obstructionand airway responsiveness to therapeutic intervention suchas MADs. The technique provides more information than tra-ditional rhinomanometry which does not provide clinical data
AbstractResistance to nasal airflow at the nares approximates halfthe airflow resistance of the entire respiratory system. Nasaldilation at the nares prevents collapsibility via the BernoulliPrinciple. Acoustic rhinometry was used to test a system of 1⁄2inch diameter acrylic discoid pads placed distal to the cuspidsat the height of the maxillary labial vestibule. They wereintended to stretch the lip and distend the nares. The intraoraldiscoid pads were anchored by orthodontic wire to a maxillaryadvancement device (MAD).
MADs are successfully used by dentists to treat obstructivesleep apnea (OSA) and snoring. The MAD with the acrylicdiscoid pads was compared to an identical control devicewithout the pads and also compared to a gold standard, externalnasal dilator strips (ENDS). The objective measurement devicewas an acoustic rhinometer.
Subjects in this study were patients in a clinical dentalpractice diagnosed with OSA by a boarded sleep specialist andetermined as appropriate candidates for treatment with a MAD.
This study demonstrated that the intraoral discoid padsplaced high in the maxillary labial vestibule distal to the cus-pids did not result in nasal dilation on a clinically or statisticallysignificant basis. They increased nasal dilation at the nares onlyslightly more than they decreased it. The external dilatornasal strips however do significantly increase cross-sectionaldimensions at the nares.
Introduction Human beings have a collapsible, flexible oropharyngealairway. This characteristic is a necessity for the articulationof speech. Periodic complete collapse of the tongue on theairway is the cause of Obstructive Sleep Apnea (OSA) andpartial collapse defines hypopnea. The nose is an incredibleorgan for olfaction, filtration, warming and humidification ofinspired air. As the air is drawn into the lungs in inhalation,excessive turbulence of the airflow and a greater demand by thediaphragm than the nasal airway can deliver creates negativepressure, facilitating airway collapse. Humans are obligate nasalbreathers. The mouth is merely a back up airway in cases ofnasal obstruction. Nasal valve incompetence, swollen allergicnasal membranes, enlarged turbinates and septal deviation areconditions that can impede nasal breathing.
The Nasal valve is a nozzle. Its cross-sectional area isstabilized by inspiratory isometric contractions of the alar dilator
1Assistant Professor, Rush University College of Medicine, Departmentof Psychology/Sleep Disorders and Surgery, Chicago, IL2R. Hillcrest Family Dental Center PC, Rensselaer, IN3Marcus Lieberman, PhD is Coroner of Jasper County, Indiana Chair of the Council on Communication for the Indiana Dental Association,Member of the Oral Health Task Force with the State Dept of Health
Sleep_3_3_pg 58-60 5/14/08 12:40 PM Page 58

Sleep Diagnosis and Therapy ♦ Vol 3 No 3 May-June 2008 59
Articles
2. Baseline Measurement, Acoustic Rhinometer – noappliance.
3. Fit the control appliance – MAD without the dilatorsAcoustic Rhinometer reading with control appliance.
4. Fit the MAD with the dilator. Adjust nasal dilators usinginterim readings with acoustic rhinometer.
5. Acoustic Rhinometer reading with discoid pads onmaximally adjusted MAD.
6. Place Breathe Right on nose of patient.7. Acoustic Rhinometer reading – Breathe Right and no
appliance.
Precautions to eliminate errors:
1. Uniformly place nasal adaptor parallel to dorsum of thenose.
2. Neutral electrocardiogram gel was used between nasaladaptor and nostril to assure adequate sealing.
3. Avoid undue pressure on the nostril to avoid deformingnostril and nasal valve.
4. Glasses removed from the nose during testing.5. Maintain head in a stable position, parallel to the ground.6. Subjects asked to close mouth, hold their breath and not
swallow during testing.7. Analysis done on the average of three technically accept-
able curves.8. All measurements done in same room.9. Maximum noise level in room was monitored and never
exceeded 60 dB.
Both the MAD with the nasal dilators and the control devicewere made out of identical material, to the same specifications.Any differences were unintended and based on individualcharacteristics of the laboratory technician. What is being testedis the value of the acrylic discoid dilators. To establish a relativestandard of effectiveness they are being compared to an exter-nal dilator, Breathe Right Nasal Strips™. Breathe Right NasalStrips™ are harmless non-invasive band-aid like devices onwhich a leaf spring is attached. When placed on the nose theleaf spring wants to straighten out, pulling on the tape andcomfortably expanding the nares. The effect of dilating thenares is to decrease nasal resistance and make airflow throughthe nose easier.
The minimal cross sectional area of the nasal cavity usuallyoccurs at the nasal valve. Eccovision acoustic rhinometry meas-ures the cross sectional airway at the nasal valves andturbinates. It can measure volume of the nose but it does notmeasure airflow. In fact during testing, the patient is holdingtheir breath. The appropriate measure for nasal dilation is com-paring the cross sectional area at the nares. Cross sectional areaof the nares with no appliance is compared to cross sectionalarea at the nares with control appliance, “nasal dilator” applianceand with a Breathe Right and no appliance.
It cannot be reasonably expected nor is there a scientificbasis for claims that decreased nasal resistance beyond thenares is a result of an intraoral nasal dilator. In fact, users ofEccovision acoustic rhinometry are cautioned in the manual thata serious constriction of the nasal airway at the nares will resultin inaccurate measurement of the airway volume beyond theconstriction. There is no scientific basis for a claim that increasedvolume of the nasal airway beyond the nares is a result of intra-oral nasal dilation. Based on the manufacturer’s cautionarystatement, such findings would probably be artifact.
on site or degree of obstruction; furthermore, the procedureis very easy to administer and interpret. The Eccovision™,being used in this study, has received FDA approval.
The protocol was to test patients diagnosed as havingOSA, referred to a clinical dental practice by a boarded sleepspecialist and for whom the dentist clinician determined thatan MAD was the appropriate and suitable treatment devicefor their OSA. Two appliances were fabricated, identical in allaspects except that one was made with the 1⁄2 inch diameteracrylic discoids (nasal dilators) and one without them.
The “control” appliance was initially fitted and the acousticrhinometry testing performed and recorded. The appliancewith the discoids was then fitted and adjusted using patientcomfort and the acoustic rhinometer to attain the maximumpossible rhinometer reading.
There was no clinical risk to those patients measured. Infact, they were at no greater risk than they would be performingtheir routine daily functions. The acoustic rhinometer testingwas a part of the normal clinical protocol, non-invasive andpainless. The patients measured for this study were pre-selectedas appropriate candidates for a MAD. All study patients weregiven a clinical informed consent form meeting HIPAArequire-ments, assuring them of their privacy, and risks. All signedand consented.
The following testing protocol was followed:
1. Patient reads, asks any questions and signs informedconsent.
Sleep_3_3_pg 58-60 5/14/08 12:41 PM Page 59

60 Sleep Diagnosis and Therapy ♦ Vol 3 No 3 May-June 2008
Articles
ConclusionThe intraoral discoid shaped pads placed high in the maxillaryvestibule and distal to the cuspids did not result in nasal dilationon a clinically or statistically significant basis. They increasednasal dilation at the nares only slightly more often than theydecreased it. The external nasal dilators however, do significantlyincrease the cross-sectional dimensions at the nares.
Resistance to airflow is a condition that predisposes and/orcauses sleep disturbed breathing. A decrease in resistance toairflow in the upper airway is a desirable clinical result. Useof a MAD is a recognized treatment modality for OSA. MADsby virtue of genioglossus advancement have been shown toeffectively reduce the AHI and thus may reduce upper airwayresistance. Scientific studies have shown MADs to be mostsuccessful on patients whose collapse is in the oropharyngealarea. A MAD can sometimes decrease the AHI without adecrease in resistance to airflow as noted on the PSG studyusing a pressure transducer in the oral/nasal cannula. Despitethe significant increase in cross-sectional area at the nares using
external nasal dilator strips, the dilator strips used alone havenot been shown to be effective in controlling OSA, and limitedsuccess reported with snoring. A promising area for futurestudy would appear to be measurement of the combined effectof ENDS used with MADs.
References1. Cole P. The four components of the nasal valve. Amer Jnl
Rhinology 2003, 17:107–114.2. Cole P, Roithman R. The nasal valve and current terminology.
Amer Jnl Rhinology 1996, 10:23–31.3. Amis TC, Kirkness JP, diSomma E, Wheatley JR. Nasal vestibule
wall elasticity: interactions with a nasal dilator strip. J Appl Physiol1999, 86:1638–1643.
4. Lorino AM, LoFaso F, Drogou I, Abi-Nader F, Dahan E, Coste A,Lorino H. Effects of different mechanical treatments on nasalresistance assessed by rhinometry. Chest 1998 114:166–170.
5. Griffin JW, Hunter G, Ferguson D, Sillers MJ. Physiologic effects of an external nasal dilator. Laryngoscope 1997 107(9):1235–1238.
Patient Base- Base- Control Control Moses Moses E.N.D. E.N.D.# line R line L R L R L R. L.
1 0.42 0.75 0.37 0.71 0.41 0.76 0.46 0.932 0.52 0.6 0.42 0.61 0.41 0.45 0.97 0.823 0.69 0.33 0.66 0.54 0.66 0.47 1.13 0.644 0.83 0.4 0.84 0.44 0.66 0.44 0.81 0.525 1.06 0.66 0.97 0.64 0.79 0.77 1.18 1.546 0.39 0.59 0.54 0.69 0.63 0.86 0.51 0.787 0.36 0.77 0.42 0.79 0.77 1.05 0.64 0.998 0.87 0.48 0.87 0.6 0.75 0.44 0.93 0.699 0.79 0.5 0.46 0.49 0.91 0.79 0.95 0.810 0.33 0.96 0.54 1.01 0.59 0.88 0.62 1.03
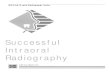
endmosescontrolbaseline
Condition
0.90
0.85
0.80
0.75
0.70
0.65
0.60
Mea
n A
rea
Left
Right
Right Left
Baseline .63 .60Control .61 .65Moses .66 .69END .82 .87
ResultsFor both right and left sides, there was an overall significantdifference in the mean areas across the four conditions (F=11.7,p<.001). However, only the E.N.D. condition showed a statis-tically significant difference from the baseline measurement.(t = 3.7, p=.005).
Sleep_3_3_pg 58-60 5/14/08 12:41 PM Page 60