Embed Size (px)
Citation preview

PHILADELPHIA CHROMOSOME POSITIVE CHRONIC MYELOGENOUS LEUKEMIA DEVELOPING IN A PATIENT
W I T H ACUTE LYMPHOBLASTIC LEUKEMIA
D. P. KELSEN, MD, T. S. GEE, MD, A N D R. S. K. CHAGANTI, PHD
A patient with acute lymphoblastic leukemia (ALL) in remission for over five years and with no systemic chemotherapy for over two years developed a peripheral blood and bone marrow granulocytosis. While in remission from the ALL, cytogenetic studies revealed a normal karyotype. With the development of peripheral and marrow granulocytosis, repeat cytogenetic preparations demonstrated the presence of the Philadelphia chromosome. The long interval between the onset of ALL and CML, as well as the normal karyotype during remission from the ALL, causes us to favor the hypothesis that two separate dis- eases are present.
Cancer 43:1782-1787, 1979.
NTENSIVE COMBINATION CHEMOTHERAPY I has resulted in improved response rates and survival in adult patients with acute lymphoblastic leukemia (ALL).12,13 As more long term survivors are followed, the ap- pearance of new second malignancies may be expected, as is the case in a number of other cancers.2*4*10*27*35 T w o patients with ALL who developed a picture compatible with chronic myelogenous leukemia (CML) have been previously reported, but both cases have lacked the Philadelphia c h r o m o s o ~ n e . ~ ~ * ~ ~ Mauri e/ al. recently reported two patients who presented with apparently typical ALL, but when placed in remission, were found to have Philadelphia chromosome positive CML.20 We are reporting a patient with ALL in remission and off chemotherapy for two years, who developed Philadelphia chromo- some positive CML.
CASE REPORT A 53-year-old white female presented to another
hospital in September 1971 with fatigue and
Froin the Memorial Sloan-Kettering Cancer Center. Department o f Medicine. Hematology Service and the hhordtoly of Genetics, N e w York . N e w York.
Supported in part by Clinical Cancer Research Center CA-05826- 17. Fund # S 162.
Address for reprints: Timothy S. Gee, MD, Memorial Sloan-Kettering Cancer Center, 1275 York Avenue. Ncw York, NY 10021.
The authors thank Mr. Roller B. Bailey for technical assistance (cytogenetics).
Accepted for publication June 12. 1978.
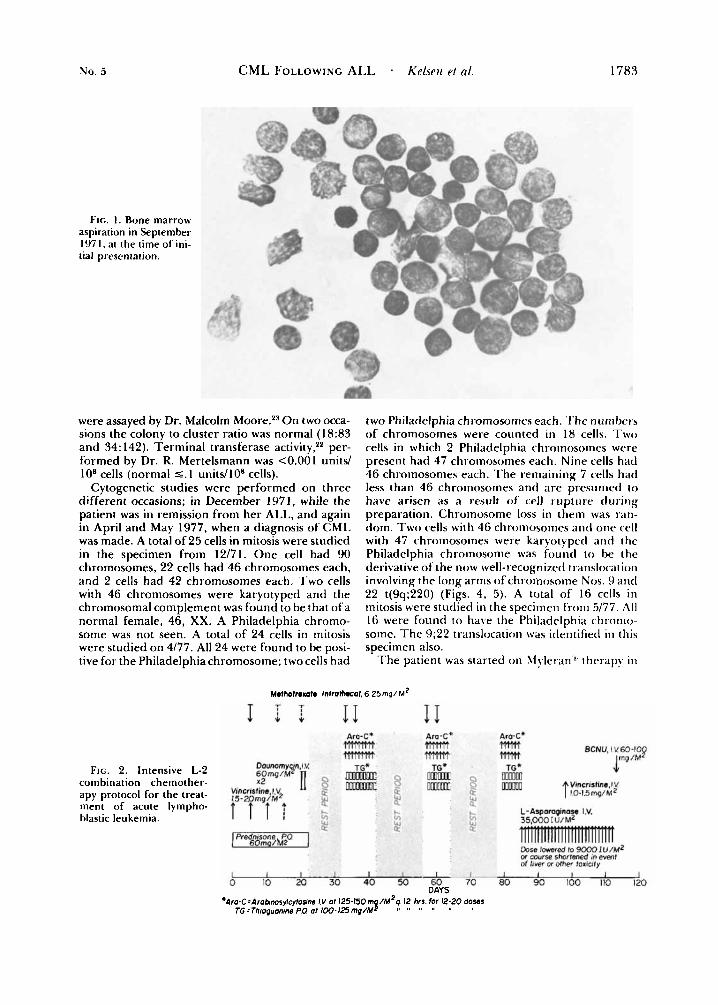
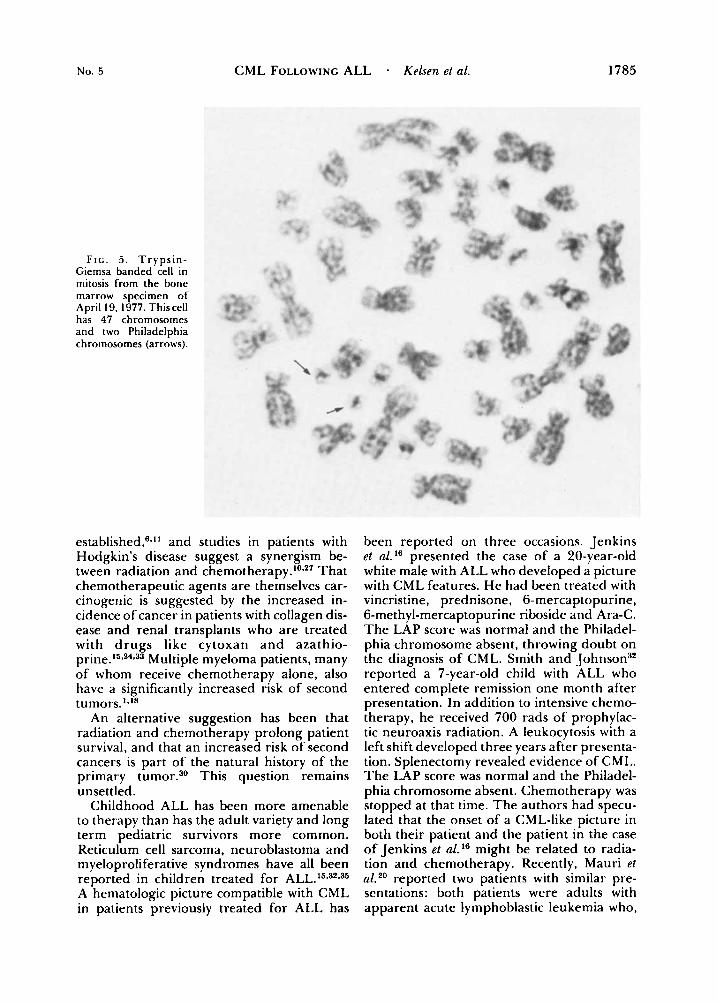
meiioinetr.orrag~iia. Examination revealed petechiae o n the oral mucosa, n o peripheral lymphade- nopathy or hepatospleiioniegaly. Chest x-ray a n d electrocardiogram were normal. Except for a uric acid of 7.4 mgldl and a lactic acid dehydro- genase of 3 13 units, her SMA 12 was within normal limits. T h e hemoglobin was 7.5 g/dl, white blood cell count 37,000/mm3 with 35% blasts and the platelet count was I I ,000/mm:'. A bone marrow aspiration revealed a cellular marrow with 40% lyinphoblasts (Fig. I ) . 'The patient was then re- ferred to Meinor-ial Sloan-Kettei-ing Cancer Center (MS-KCC). Repeat marrow aspiration confirmed the diagnosis of A L L and she was started on the L-2 protocol (Fig. 2). Complete remission was achieved in October 1971. She was subsequently admitted to MS-KCC on five occasions from 11/71 t o 12/73, either for Chemotherapy or for neutropenia with fever. T h e L-2 protocol was completed in Decem- ber 1974. a n d chemotherapy was stopped at that rime. Since then she has been followed at two month intervals with repeated bone marrow aspira- rioris. Except for a n episode o f localized herpes zoster, she was well until December 1976. At that time a CBC revealed a white blood cell count of 12,600 cells/nim3 with 65% polyniorphonuclear cells, 1% bands, 2% metamyelocytes, 1% rnyelo- cytes, 5% eosinophils, 4% basophils, 10% mono- rytes, 10%) lymphocytes and 2% atypical lympho- cytes. Bone marrow aspiration differential was 73.5% myeloid series, lymphoid 3.5%. erythroid l6.5%, blasts 37G, and monocytes 3.5% (Fig. 3). In May 1977, another bone marrow aspiration showed 86%' inyeloid cells, 8%' erythroid cells, 1.5% lymph- oid cells. 2% monocytes, and 2.5% blasts. Cel- lularity W;IS inrreased. T h e LAP score was 84 (normal 15-85). T h e vitamin BIZ level was 2,000 pg/nil (normal 150- 1100). Colony forming units
0008-543X/79/0500/1782 $0.80 0 American Cancer Society
1782
No. 5
FIG. I . Bone marrow aspiration in September 1971. at rhe rime of ini- tial presentation.
CML FOLLOWING ALL . Kclsr?r rl (ti.
were assayed by Dr. Malcolm Moore.23 O n two occa- sions the colony to cluster ratio was normal (18:83 a n d 34: 142). Terminal transferase activity," per- formed by Dr. R. Mertelsmann was <0.001 units/ lo8 cells (normal 5. I units/108 cells).
Cytogenetic studies were performed o n three different occasions; in December 1971, while the patient was in remission from her ALL, a n d again in April a n d May 1977, when a diagnosis of CML was made. A total of 25 cells in mitosis were studied in the specimen from 12/71. O n e cell had 90 chromosomes, 22 cells had 46 chromosomes each, a n d 2 cells had 42 chromosomes each. T w o cells with 46 chromosomes were karyotyped and the chromosomal complement was found to be that ofa normal female, 46, XX. A Philadelphia chromo- some was not seen. A total of 24 cells in mitosis were studied o n 4/77. All 24 were found to be posi- tive for the Philadelphia chromosome; two cells had
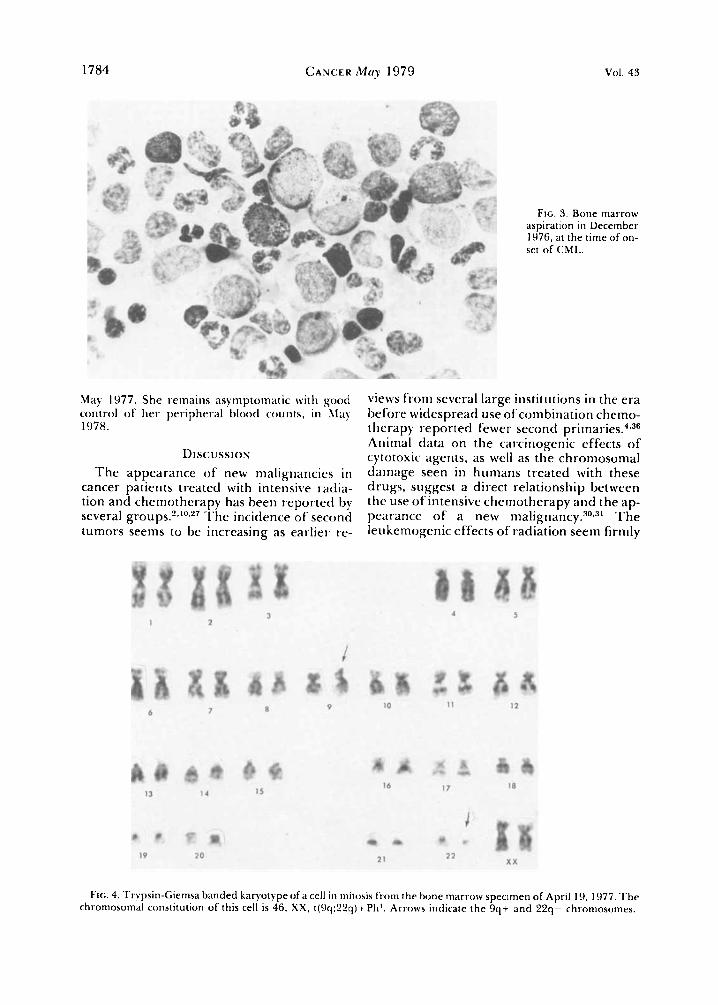
FIG. 2. Intensive L-2 combination chemother- apy protocol for the treat- ment of acute lympho- blastic leukemia.
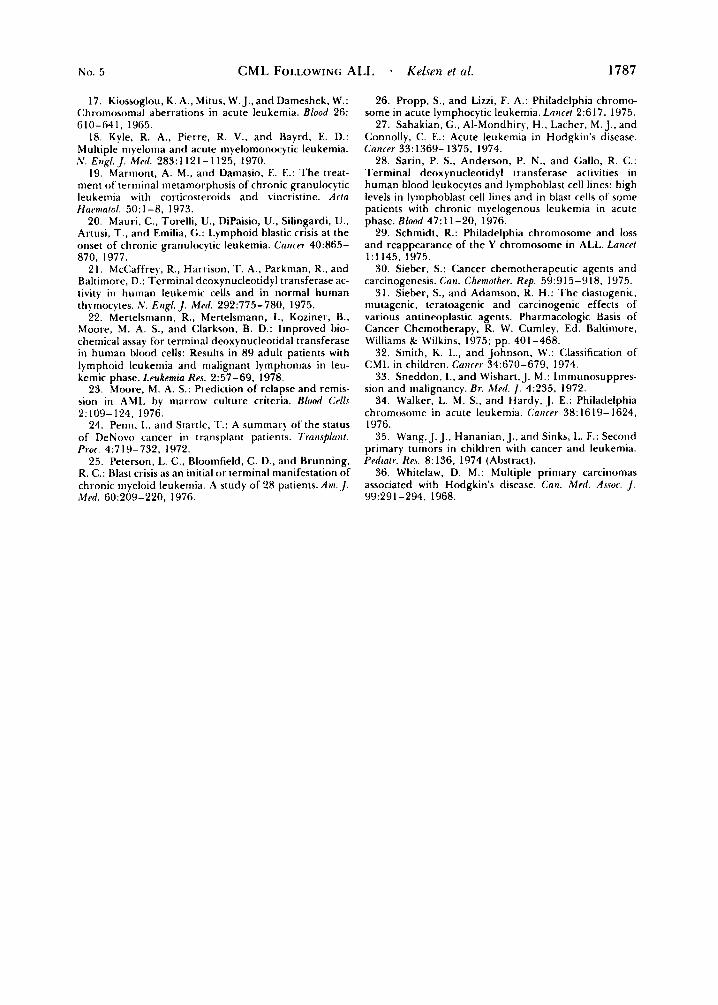
two Philadelphia chromosomes each. 'I'he numbers o f chromosomes were counted in 18 cells. T w o cells in which 2 Philadelphia chroniosoines were present had 47 chromosomes each. Nine cells had 46 chromosonies each. T h e remaining 7 cells had less than 46 chromosomes antl a r e pi-esumetl to have arisen as a result of' cell rup ture dur ing preparation. Chromosome loss in them was ran- dom. T w o cells with 46 chromosomes a n d one cell with 47 chromosomes were karyotyped a n d the Philadelphia chromosome was found t o be the derivative of the now well-recognized translocation involving the long arms of chroi~iosotiie Nos. 9 antl 22 t(9q;220) (Figs. 4, 5). A total of 16 cells in mitosis were studied in the specimen f'rom 5/77. .411 16 were found to have the Philadelphia chronio- some. T h e 9;22 translocation was identified in this specimen also.
T h e patient was started on h f y l ~ r a n ' ~ therapy in
Mefhofrexofe Infrolh.col, 6.25mg/M2
I1 T T
I l i 11
1783
Ara-C* Ara-C4 m m m m
Am-C' m mm BCNU, I V 6 0 - I O p
I ma / M TG* 4 -
Vmcrirfh,l V t 10-1.5 mg/MZ
mnm m
or wwse shortened in event of liver u Other toaiuty A IA & i o ' ' & 60 I 70 I 80 I 90 I 100 I 110 I 120 1
DAYS * A ' L ~ ~ O ~ C = A ~ O ~ I W S ~ ~ C Y ~ O S I I M I V a1 125-1501n$/M*q 12 hrs for 12-20 doses
TG=Throguanms PO at 1 0 0 - 1 2 1 i m p / M 'I '' "
1784 CANCER Mo? 1979 Vol. 43
May 1977. She remains asymptomatic with good control o f h e r peripheral blood counts , in RIay 1978.
D I scu ss ION
The appearance of new malignancies i n cancer patients treated with intensive radia- tion and chemotherapy has been reported by several T h e incidence of second tumors seems to be increasing as earlier re-
Flc. 3. Bone marrow aspiration in December 1976, at the time of on- set of ChlL.
views from several large institutions in the era before widespread use of combination chemo- therapy reported fewer second Animal data on the carcinogenic effects of cytotoxic agents, as well as the chromosomal damage seen in humans treated with these drugs, suggest a direct relationship between the use of intensive chemotherapy arid the ap- pearance of a new m a l i g r i a n ~ y . ~ ~ - ~ ~ T h e leukemogenic effects of radiation seem firmly
Fir;. 4. Trypsin-Gienisa banded karyotype of a cell in mitosis from the bone marrow specimen of April 19, 1977. T h e chromosomal constitution of this cell is 46. X X , t(9q;22q)+Ph'. Arrows indicate the 9q+ and 22q- c h r o n i o ~ o m e ~ .
No. 5 CML FOLLOWING ALL - Kelsen et al. 1785
F I G . 5 . T r y p s i n - Giemsa banded cell in mitosis from the bone marrow specimen of April 19, 1977. Thiscell has 47 chromosomes and two Philadelphia chromosomes (arrows).
established,'?." and studies in patients with Hodgkin's disease suggest a synergism be- tween radiation and c h e m ~ t h e r a p y . ~ ~ * ~ ' That chemotherapeutic agents are themselves car- cinogenic is suggested by the increased in- cidence of cancer in patients with collagen dis- ease and renal transplants who are treated with drugs like cytoxan and azathio- prine.15*24-33 Multiple myeloma patients, many of whom receive chemotherapy alone, also have a significantly increased risk of second tumors.'"*
An alternative suggestion has been that radiation and chemotherapy prolong patient survival, and that an increased risk of second cancers is part of the natural history of the primary tumor.30 This question remains unsettled.
Childhood ALL has been more amenable to therapy than has the adult variety and long term pediatric survivors more common. Reticulum cell sarcoma, neuroblastoma and myeloproliferative syndromes have all been reported in children treated for ALL.15*32*35 A hematologic picture compatible with CML in patients previously treated for ALL has
been reported on three occasions. Jenkins et a l l 6 presented the case of a 20-year-old white male with ALL who developed a picture with CML features. He had been treated with vincristine, prednisone, 6-mercaptopurine, 6-methyl-mercaptopurine riboside and Ara-C. The LAP score was normal and the Philadel- phia chromosome absent, throwing doubt on the diagnosis of CML. Smith and Johnson32 reported a 7-year-old child with ALL who entered complete remission one month after presentation. In addition to intensive chemo- therapy, he received 700 rads of prophylac- tic neuroaxis radiation. A leukocytosis with a left shift developed three years after presenta- tion. Splenectomy revealed evidence of CML. The LAP score was normal and the Philadel- phia chromosome absent. Chemotherapy was stopped at that time. The authors had specu- lated that the onset of a CML-like picture in both their patient and the patient in the case of Jenkins et al."? might be related to radia- tion and chemotherapy. Recently, Mauri et aL20 reported two patients with similar pre- sentations: both patients were adults with apparent acute lymphoblastic leukemia who,

1786 CANCEH M q 1979 VOl. 43
while in complete remission for less than one year, were found to have a marked granulo- cytosis, the LAP score was low, and the Phila- delphia chromosome was present in both cases. They concluded that their patients had presented with an initial lymphoblastic phase of CML.
Patients presenting with blastic CML with- out a chronic phase have been estimated to compose from 15-30% of the total blastic CML p o p ~ l a t i o n . ' ~ * * ~ T h e presence of 25 Philadelphia chromosome negative karyo- types two months after obtaining a remission froin ALL does not eliminate the possibility that the current case represents another pa- tient with Philadelphia chromosome positive CML presenting initially with lymphoblastic crisis. Bloomfield7 has reported on a similar observation in a patient with ALL. One of the authors (TSG) has also observed another pa- tient with initial Philadelphia chromosome positive lymphoblastic crisis who responded to cytotoxic chemotherapy. Subsequent cyto- genetic studies demonstrated a return to a normal Philadelphia chromosome negative karyotype.
Gee et al. l4 reported upon attempts with in- tensive therapy to eliminate the Philadelphia
chromosome from marrow cytogenetic prep- arations. They were successful in signifi- cantly reducing the percentage of cells with the Philadelphia chromosome in approxi- mately 30%) of cases, but only in 10% did the reduction of cells with the Philadelphia chromosome persist for more than eight months, even with continued maintenance chemotherapy. For a Philadelphia chromo- some positive blastic CML to relapse after being in remission for five years, two years without cytotoxic chemotherapy, is unlikely.
T h e absence of splenomegaly on initial presentation, as well as throughout the five years of remission, including at the time of diagnosis of Philadelphia chromosome posi- tive CML in 1976 is unusual for a patient with Philadelphia chromosome positive CML, but even more unusual for a case in the late or blastic phase.
One cannot exclude the possibility that this patient represents a case of initial Philadelphia chromosome positive CML presenting with a lymphoblastic crisis. However, the long remission and interval without chemo- therapeutic maintenance leads us to favor the possibility that t w o separate disease entities are present.
REFERENCES
I . Andersen, E., and Videbaek, A,: Stem cell leukemia in rnyelomatosis. Scand. J . Hat-rnatol. 7:201-207. 1970.
2. Arseneau, J . C., Sponzo, R. W., Levin, D. l.., Schnip- per, L. E. , Bonner. H., Young, R. C.. Canellos. G. P., Johnson, R. E.. and DeVita, V. T.: Nonlyrnphoinatous malignant tumors complicating Hodgkin's Disease. IV. Engl. J . M t d . 287: 1 1 19- 1122, 1973.
3. Aru, R. J. A,, Simone. J. V., Hustu, H. 0.. and Verzosa, M. S.: A comparative study of central nervous system irradiation and intensive chemotherapy early in remission of childhood acute Iymphocytic leukemia. Cnti - ccr 29:381-391, 1972.
4. Berg, J. W.: The incidence of multiple primary can- cers. I . Development of further cancers in patients with lymphomas, leukemias and myeloma.,/. A'n/l. Cnttrrr I f i s / .
38:741-752, 1967. 5. van Biervliet, J. P., van Hemel, J., Geurts, K . , Punt,
K.. and de Boer-van Wering, E.: Philadelphia chromo- some in acute lymphocytic leukemia. Lanrt-t 2:617. 1975.
6. Bizzozero. 0. J.. Jr.. Johnson, K. G., Ciocco. A , . Kawasaki, S., and Toyoda. S.: Radiation-related leukemia in Hiroshima and Nagasaki, 1946- 1964. An,/. IMrru.
7. Bloomfield. C. D.. Peterson, L. C., Yunis, J . , and Brunning, R. D.: T h e Philadelphia chromosome in adults presenting with acute leukemia: A comparison of Ph'+ and Ph'- patients. B i . J . Hncmalol. 36:347-357, 1977.
8. Boggs, D. R.: Hemopoietic stein cell theory in rela- tion to the possible lymphoblastic conversion of <:hlL.
9. Canellos, G. P.. DeVita, V. T., Whang-Peng,]., and
i i ' f d . 66~522-530. 1967.
B/OOff 44:449-453. 1974.
Carbone, P. P.: Hematologic and cytogenetic remission of blastic transformation in chronic granulocytic leuke- mia. Blood 38:671-679, 1971.
10. Canellos, G. P., DeVita. V. T., Arseneau, J . C.. Whang-Peng, J.. and Johnson, R. E. C.: Second malig- nancies complicating Hodgkin's Disease in remission. Lnfird 1:947-949, 1975.
1 1. Court-Brown, W.. and Abbott, J . D.: T h e incidence ot' leukemia in ankylosing spondylitis treated with x-rays. Lnncr/ I : 1283- 1285, 1955.
12. Dowling, M . D. , Kempin, S. . Gee, T., Dufour, M.. Noble. S., Clarkson. B., and Burchenal, J.: Improved survival in adult acute lymphocytic leukemia ( A I L ) . P r o f . Afn. ,'f.\.wr. (;/in. o t i c o [ . 18:C281, 1977 (Abstract).
13. Gee, T. S., Haghbin. M., Dowling. M. D.. Cun- ningham, I . , Middleman, M. P., and Clarkson, B. D.: Acute lymphoblastic leukemia in adults and children. (."tiCtr 37:
14. Gee, T. S., Cunningham, I., Dowling, M. D.. Chaghnnti, R., and Chrkson. B. D.: The L-5 Protocol: Intensive treatment for patients with chronic myeloge- nous leukemia. Proc. Int. Soc. Hematol.. European- African Division. Boll. Ist. SimoteT. Milan. 57:289-293. 1978.
15. Hoover, R., and Fraumeni, J.,,Jr.: Risk ofcancer in renal transplant patients. Lowr/ 2:55-57, 1973.
16. Jenkins, I). W.. Rivera, H. P., and Coltinan, C. A.: Case report: Acute lymphatic leukemia followed by a clinical picture indistinguishable from chronic granulo- cytic leukemia in the same patient. Am. J . Mcd. Sri. 264:
1256-1264. 1976.
329-333, 1972.
No. 5 CML FOLLOWING ALL - KeOen rt nl. 1787
17. Kiossoglou, K . A., Mitus, W. J., and Dameshek, W.: Chromosomal aberrations in acute leukemia, Blood 26: 610-641, 1965.
18. Kyle, R. A,, Pierre, R. V.. and Bayrd, E. D.: Multiple myeloma and acute myelomonocytic leukemia.
19. Marmont, A. M., and Damasio, E. E.: The treat- ment of terminal metamorphosis of chronic granulocytic leukemia with corticosteroids and vincristine. Ac/o Hawtoto / . 50: 1-8, 1973.
20. Mauri, C.. Torelli, U., DiPaisio, U.. Silingardi. U., Artusi, T.. and Emilia, G.: Lymphoid hlastic crisis at the onset of chronic granulocytic leukemia. Cartcar- 40:865- 870, 1977.
21. McCaffrey, R., Harrison. T. A.. Parkman, R., and Baltimore, D.: Terminal deoxynucleotidyl transferase ac- tivity in human leukemic cells and in normal human thymocytes. N. Ertgl. J. Mrd. 292:775-780, 1975.
22. Mertelsniann. R.. Mertelsmann, 1.. Koziner, B.. Moore, M. A. S., and Clarkson, B. D.: Improved hio- chemical assay for terminal deoxynucleotidal transferase in human blood cells: Results in 89 adult patients with lymphoid leukemia and malignant lymphomas in leu- kemic phase. Lrukemia Rrx 2:57-69, 1978.
23. Moore, M. A. S.: Prediction of relapse and remis- sion in A M I . by marrow culture criteria. B l d (:u//.c 2:109-124, 1976.
24. Penn, 1.. and Startle, T.: A summary of the status of DeNovo cancer in transplant patients. Tratisplnrit. Pror. 4:719-732, 1972.
25. Peterson, 1.. C.. Bloomfield, C. D., and Brunning, R. C.: Blast crisis as an initial o r terminal manifestation of chronic myeloid leukemia. A study of 28 patients. Am. , I . .Clrd. 60:?09-220, 1976.
A'. E I I ~ / . J . Md. 283: 1 12 1 - 1 125. 1970.
26. Propp, S., and Lizzi, F. A.: Philadelphia chromo- some in acute lymphocytic leukemia. Larice/ 2:617. 1975.
27. Sahakian, C., Al-Mondhiry, H., Lacher, M. J.. and Connolly, C. E.: Acute leukemia in Hodgkin's disease. Cnncrr 33:1369- 1375. 1974.
28. Sarin, P. S., Anderson, P. N., and Gallo, R. C.: Terminal deoxynucleotidyl transferase activities in human blood leukocytes and lyinphoblast cell lines: high levels in lymphoblast cell lines and in blast cells of some patients with chronic myelogenous leukemia in acute phase. Blood 47:1 1-20, 1976.
29. Schmidt, R.: Philadelphia chromosome and loss and reappearance of the Y chromosome in ALL. Larird 1:1145, 1975.
30. Sieber, S.: Cancer chemotherapeutic agents and carcinogenesis. Can. Chrmothrr. Rep. 59:9 15-9 18, 1975.
31. Sieber, S., and Adamson, R. H.: The clastogenic, mutagenic. teratoagenic and carcinogenic effects of various antineoplastic agents. Pharmacologic Basis of Cancer Chemotherapy. R. W. Cumley. Ed. Baltimore, Williams & Wilkins, 1975; pp. 401-468.
32. Smith, K. L., and Johnson, W.: Classification of CMI. in children. Corirrr- 34:670-679. 1974.
33. Sneddon, 1.. and Wishart, J. M.: Iinmunosuppres- sion and malignancy. Br. Icfrd. J . 4:235. 1972.
34. Walker, L. M. S., and Hardy, 1 . E.: Philadelphia chromosome in acute leukemia. Caricrr 38: 1619- 1624, 1976.
35. Wang, J. J., Hananian, J., and Sinks, I.. F.: Second primary tumors in children with cancer and leukemia. Prdta/r. Re.\. 8: 136. 1974 (Ahstract).
36. Whitelaw, D. M.: Multiple primary carcinomas associated with Hodgkin's disease. Cau. M r d . her. J . 993291-294, 1968.
























![[Ghiduri][Cancer]Chronic Myelogenous Leukemia](https://img.dokumen.tips/doc/110x75/577cc6ea1a28aba7119f80de/ghiduricancerchronic-myelogenous-leukemia.jpg)



