Embed Size (px)
Citation preview

Current Psychological Research (1982), 2, 171-180
Phenobarbitone and Kinaesthetic After-effect
UMAGUPTA
Meerut University
The effect of phenobarbitone (phenobarbital), predominantly a central depressant, onkinaesthetic after-effect was examined. The subjects were selected after apreliminary testing with the Maudsley Personality Inventory. They were classifiedinto two groups: extraverts and introverts. The drug was used at different doselevels. A 2 x 4 randomized block design was replicated ten times. The study supportsthe following conclusions: (a) the extraverted subjects show larger kinaestheticafter-effect than introverted subjects under placebo condition; (b) phenobarbitonehas no effect on kinaesthetic after-effects in extraverted subjects except in smalldoses (30 rng) which reduce the size of the effect; (c) the drug in larger doses (60mg and 100 rng ) produces a significant increasing effect in the introverted gro~p.
Since the appearance of two reports by Kohl er and his colleagues indicating that themeasures of figural after-eff ect provide an index of cortical exci tabili ty (Kohl er &:
Wallach, 1944; Kohl er &: Dinnerstein, 1947), researchers (such as Klein &: Krech ,1952; Wertheimer &: Wertheimer, 1954; Eysenck, 1955) have argued that such measuresprovide information about neural functioning. They used terms such as corticalconducti vity, metabolic efficiency and reacti ve Inhibi tion respecti vely whendescribing the neural processes in terms of which people differ. Each group oftheorists suggested, however, that the hypothetical neural operations wereequi valent to the process of cortical satiation outlined by Kohl er and Wallach(1944). The basic principle implicit in this kind of research was that the index offigural after-effect provided an uncontaminated measure of cortical excitability.However, as suggested by Over (1970), the possibility that groups of subjects canshow different after-effects as a resul t of decision processes inherent in figuralafter-effect situations (such as judgement time, response set, instructions,stimulus properties, etc.) was ignored. The present interest is not so much in theinterpretations of the process underlying the phenomenon as in knowing how thephenomenon is affected by variation in the organismic state produced by drugs. The
0144-3887/82/0203-171 $02.00 © 1982 Praeger Publishers

172 u. Gupta
existence of the phenomenon has not been disputed, and it has been established forboth visual and kinaesthetic stimulation, but recently much attention has centred onthe kinaesthetic after-effect.
Kinaesthetic after-effect (KAE) is a perceptual phenomenon in which changes inwidth judgements of a standard block occur as a consequence of touching an aftereffect-inducing block different in width from the standard block. The area ofresearch is, however, fraught with numerous methodological complexities, primarilyrelated to problems of reliable measurement of the phenomenon and to its consistencyover time (Broadbent, 1961; PIatt, Hol tzm an & Larson, 1971; Mor gan & Hilgard, 1972;Weintraub, Green & Herzog, 1973; Weintraub & Herzog, 1973). Despite some criticismof KAE as a personality measure (Sales & Throop, 1972; McDonald, 1974), a new viewis emerging that a single administration of KAE (the one used in the present study)provides a valid and highly reliable index of after-effect (Baker et al , 1976, 1978;Kostin et al , 1978; Mishara & Baker, 1978).
The literature concerning the effects of drugs on KAE is scant. Wertheimer,Levine & Wertheimer (1955) investigated the effects of stimulating (50 mg ephedrinesulphate, 22 mg strychnine sulphate, and 100 mg nicotinic acid) and depressing (100mg pethidine hydrochloride, 200 mg quinalbarbi tone, and 600 cc of whisky) drugs oncertain perceptual measures, one of which was KAE. Both types of drugs reduced thesize of KAE but the decrease was significant only for the depressants. In anotherstudy, Poser, Knight and Lehmann (1958) reported that 15 mg dexamphetaminesignificantly reduced the size of KAE, but a 265 mg dose of sodium amylobarbitone
had no significant effect although six out of their ten subjects showed decreases inthe KAE. Eysenck and Easterbrook (1960) later reported that 5 mg of D-amphetaminesulphate, 90 mg of sodium amylobarbitone and 100 mg of meprobamate did not produceany significant effect on KAE. Costello (1962), on the other hand, reported that,contrary to expectations, an 800 mg dose of meprobamate reduced the size of KAE;results were, however, significant only for the descending trials.
In more recent experiments, Gupta (1974) found that, compared with the placebocondition, the size of KAE was significantly reduced under the influence of 10 mg ofD-amphetamine and enhanced with 100 mg of phenobarbitone. Despite the importance ofdose-response data in drug resear-ch our literature review shows that so far only one
study has appeared in which D-amphetamine was used in three doses (7.5 mg, 10.0 mg,12.5 rng) for investigating the effects on KAE (Gupta & Kaur, 1978). The authorsreported that the drug reduced the size of KAE in the extraverted group of subjectsand enhanced it in the introverted group. A similar inquiry with a depressing drugis needed; the present study was undertaken to remedy this deficiency.
The study aims to investigate the effects of a long-acting barbiturate,phenobarbitone, on KAE by using a dose-response research design. The barbituratesproduce depression of the central nervous system (CNS) ranging from ~ild sedation tocoma. The degree of depression obtained depends not only on the particularbarbiturate, the dose and the route of administration, however, but also on thedegree of excitability of the -CNS at the time of administration and the extent towhich previous experience with drugs has induced tolerance (Har vey , 1975).
Although many attempts have been made to localize the action of barbiturates tocertain gross regions of the brain stem, such as the midbrain tegmentum orhypothalamus, drugs of this class apparently act at all levels of the neuraxis; theeff ects are, however, more profound on the reticular acti va ting system (Har vey,1975). Because of their effects on a wide range of cellular functions in many vitalorgan systems barbiturates are known as general depressants and may be employed for

Phenobarbitone and Kinaesthetic After-effect 173
almost any condi tion in which a relati vely non-specific depression of the CNS isdesirable.
METHOD
The effects of the three doses (30 mg, 60 mg, 100 rng) of phenobarbitone on KAE wereinvestigated in two groups of subjects varying on the extraversion dimension ofpersonality. Calcium tablets were used as placebos.
Apparatus
The apparatus included an adjustable comparison block with a scale which wasadjustable in units of 0.05 inch (0.127 cm) fitted on to it, a 2.5-inch (6.35-cm)wide and 12.5-inch (31.75-cm) long after-effect-inducing block, and a 1.5-inch(3.81-cm) wide test block.
Subjects
The volunteer subjects were right-handed male postgraduate students of differentcolleges and uni versity teaching departments, who ranged in age from 21 to 25 years.They were selected on the basis of a preliminary testing with the Hindi translation(Das, 1961) of Eysenck's (1959) Maudsley Personality Inventory (MPI). The MPI wasadministered to 1500 students, 80 of whom were selected for the study. On the basisof their extraversion scores the subjects were di vided into two groups: E+(extraverts), with scores of 39 or more, and E- (introverts), with scores of 15 orless. The mean E score and the standard deviation for 1500 students were 26.8 :t 7.9.The extraversion scores of E+ and E- groups of subjects were 1.5 s s d , above andbelow the mean respectively. Each group consisted of 40 subjects, 10 of whom wererandomly assigned to each of the four treatment condi tions. In order to minimize anypossible effect of neuroticism, only those subjects who ranged on this dimensionbetween mean :t 1.0 s c d , (mean = 21.42; svd , = 10.31) were selected.
Procedure
Each subject was given only one treatment, placebo or phenobarbitone. Both theplacebo and phenobarbitone were in capsules of identical appearance and were takenorally with a draught of water. A double-blind procedure was adopted for drug
administration: an assistant administered the drug or placebo without knowing whateach subject would receive. Testing was done one hour after administration (Gupt a ,1974) •
Subjects were gi ven no information about the nature of the drug at any stage.Before the administration of drug or placebo, however, each subject was indi viduallytold that the experimenter wanted to study the effect of a drug on his capacity tojudge the width of certain blocks. He was also told that the drug was quite harmlessand that its effect would generally last for a few hours. It was made clear thatthere was no compulsion for the subject to participate in the study and that hewould not receive payment for acting as a subject. Each subject was contacted the
174 u. Gupta
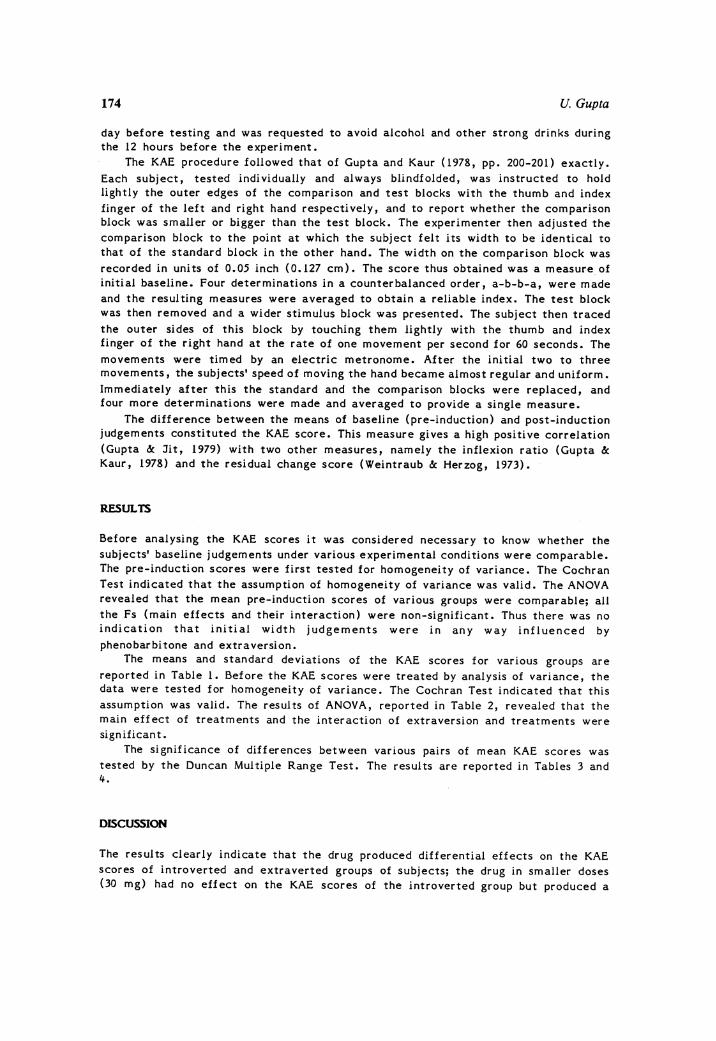
day before testing and was requested to avoid alcohol and other strong drinks duringthe 12 hours before the experiment.
The KAE procedure followed that of Gupta and Kaur (1978, pp. 200-201) exactly.
Each subject, tested individually and always blindfolded, was instructed to holdlightly the outer edges of the comparison and test blocks with the thumb and indexfinger of the left and right hand respecti vely, and to report whether the comparisonblock was smaller or bigger than the test block. The experimenter then adjusted thecomparison block to the point at which the subject felt its width to be identical tothat of the standard block in the other hand. The width on the comparison block wasrecorded in units of 0.05 inch (0.127 cm). The score thus obtained was a measure. ofinitial baseline. Four determinations in a counterbalanced order, a-b-b-a, were madeand the resulting measures were averaged to obtain a reliable index. The test blockwas then removed and a wider stimulus block was presented. The subject then traced
the outer sides of this block by touching them lightly with the thumb and indexfinger of the right hand at the rate of one movement per second for 60 seconds. The
movements were timed by an electric metronome. After the initial two to threemovements, the subjects' speed of moving the hand became almost regular and uniform.Immediately after this the standard and the comparison blocks were replaced, andfour more determinations were made and averaged to provide a single measure.
The difference between the means of baseline (pre-Inductlon) and post-inductionjudgements constituted the KAE score. This measure gives a high positive correlation(Gupta &: Jit, 1979) with two other measures, namely the inflexion ratio (Gupta &:Kaur, 1978) and the residual change score (Weintraub &: Herzog, 1973).
RESULTS
Before analysing the KAE scores it was considered necessary to know whether thesubjects' baseline judgements under various experimental conditions were comparable.The pre-induction scores were first tested for homogeneity of variance. The CochranTest indicated that the assumption of homogeneity of variance was valid. The ANOVArevealed that the mean pre-induction scores of various groups were comparable; allthe Fs (main effects and their interaction) were non-significant. Thus there was noindication that initial width judgements were in any way influenced by
phenobarbi tone and extraversion.The means and standard deviations of the KAE scores for various groups are
reported in Table 1. Before the KAE scores were treated by analysis of variance, thedata were tested for homogeneity of variance. The Cochran Test indicated that thisassumption was valid. The results of ANOVA, reported in Table 2, revealed that themain effect of treatments and the interaction of extraversion and treatments weresignificant.
The significance of differences between various pairs of mean KAE scores wastested by the Duncan Mul tiple Range Test. The resul ts are reported in Tables 3 and4.
DISCUSSION
The results clearly indicate that the drug produced differential effects on the KAEscores of introverted and extraverted groups of subjects; the drug in smaller doses(30 rng) had no effect on the KAE scores of the introverted group but produced a

Phenobarbitone and Kinaesthetic After-effect
Table I. Means and standard deviations of KAE scores
Phenobarbitone
175
Extraversion
LowHigh
Placebo
O. 13 (0.032)0.23 (0.09~)
30 mg
O.12 (0.038)O. 15 (0•05I)
60 mg
0.23 (O.09a)0.25 (0.12IJ
100 mg
0.48 ro.us:0.29 (0.09~)
Standard deviations are given in parentheses.
Table 2. Resul ts of analysis of variance
Source SS d.f. MS F P
Extraversion (EJ 0.002 I 0.002 <::1 NSTreatments (T) 0.711 3 0.237 29.625 0.001E x T 0.235 3 0.078 9.750 0.001Within 0.547 72 0.008
Table 3. Significance of differences between treatment means by the Duncan Test(n = 20 for each mean)
Means comp ared
Placebo and 60 mg dosePlacebo and 100 mg dose30 mg and 60 mg dose30 mg and 100 mg dose60 mg and 100 mg dose
Obtained Duncan value
3.0010.255.25
12.507.25
P
0.050.0010.0050.0010.001
significant increasing effect with larger doses (60 mg and 100 mg); and, conversely,the small dose decreased the KAE scores of the extraverted group (level ofsignificance was, however, only P< 0.08) while the larger doses had no effect onthe performance of this group. Thus the smaller dose was effective with extravertswhile the larger doses were effecti ve with introverts, and the effects were inopposi te directions. Another interesting feature of the resul ts is that theextraverts' performance with the 30 mg dose was comparable with that of introverts

176 U. Gupta
under the no-drug condition, while that of introverts with the 60 mg dose wascomparable with that of extraverts under the no-drug condition: that is,. the 30 mgdose of phenobarbi tone made extraverts perform on the KAE task like introverts
Table 4. Significance of differences between Extraversion x Treatment means by theDuncan Test (n = 10 for each mean)
Means compared Obtained Duncan value P.
E-: PI acebo and 60 mg dose 3.571 0.05Placebo and 100 mg dose 12.500 0.00130 mg and 60 mg dose 3.929 0.0530 mg and 100 mg dose 12.857 0.00160 mg and 100 mg dose 8.929 0.001
E+: Placebo and 30 mg dose 2.857 0.0830 mg and 60 mg dose 3.571 0.0530 mg and 100 mg dose 5.000 0.01
Placebo: E- and E+ 3.571 0.05100 mg dose: E- and E+ 6.785 0.001
working under the no -drug condition, and the 60 mg dose of the drug made introvertsperform on the task like extraverts under the no-drug condition.
Individuals varying on the extraversion scale have been reported to possessvarying degrees of arousal; introverts who are presumed to possess a high basiclevel of cortical excitation ·are alleged to be more aroused individuals than areextraverts who presumably possess a high basic level of cortical inhibition(Claridge, 1967; Eysenck, 1967; Davies &: Tune, 1970). The rel atl'onshlp betweenarousal and mental performance has hypothetically been described as curvilinear(Hare, 1970). Introverts under normal conditions probably work at the optimal levelof their performance (Eysenck, 1967); further increase or decrease in their level ofarousal may be detrimental to their performance. The prediction related to anenhancement in their level of arousal was supported in a recent study on KAE (Gupta&: Kaur, 1978) where the level of arousal was enhanced following administration of Damphetamine, a centrally stimulating drug (Innes &: Nickerson, 1975). The predictionin regard to decrement in performance as a consequence of decrease in level of
arousal was supported by the resul ts of the present study where the level of arousalwas depressed following administration of phenobarbitone (60 mg and 100 mg doses).But in states of suboptimally low levels of arousal (as may be the case withextraverts) when the level of arousal is enhanced following administration of 0amphetamine, extraverts' KAE scores become comparable with that of introvertsworking under the no-drug condition (Gupta &: Kaur, 1978); however, when their levelof arousal is further decreased following administration of phenobarbitone (as inthe present study) the performance (L. e., width judgements after a period ofinduction) is facilitated with smaller doses and the subjects perform on this task

Phenobarbitone and Kinaesthetic After-effect 177
as if their level of arousal has been increased, and their KAE scores becomecomparable with that of introverts working under the no-drug condition. Cohen (1975)and Franz (1975) suggest that barbiturates at low concentrations generally producean excitatory effect on some functions by depressing the ascending inhibitory systemof the reticular formation. Price (1975) also points out that at the lightest levelsthere is a release from inhibition in the extralemniscal systems, but on increasingdepth the excitatory process also becomes depressed and cortical responsivenessdeclines: that is, with higher concentrations the entire reticular system (both
acti vating and inhibl tory) becomes depressed by the barbiturates. The first part ofthis prediction (Price, 1975) seems true for extraverts who probably work
suboptimally under normal conditions (Eysenck, 1967); the latter part of theprediction is in fact related to the anaesthetic dose, the quantity of which maydiffer for the two groups of people under study.
ACKNOWLEDGEMENT
The author is grateful to B. S. Gupta for help in the planning and execution of thisstudy.
REFERENCES
Baker, A.H., Mishara, B.l., Kostin, I.W. &: Parker, L. (1976). Kinestheticaftereffect and personality: a case study of issues involved in constructvalidation. Journal of Personality and Social Psychology, 34, 1-13.
Baker, A.H., Mishara, B.L., Parker, L. &: Kostin, I.W. (1978). When 'reliability'fails, must a measure be discarded? The case of kinesthetic aftereffect. Journalof Research in Personality, 12, 262-273.
Broadbent, D.E. (1961). Psychophysical methods and indi vidual differences in thekinesthetic figural aftereffect. British Journal of Psychology, 52, 97-104.
Claridge, G.S. (1967). Personality and Arousal. London: Pergamon Press.Cohen, P.J. (1975). Signs and stages of anesthesia. In L.S. Goodman &: A. Gilman
(eds . }, The Pharmacological Basis of Therapeutics. New York: Macmillan.Costello, C.G. (1962). The effects of meprobamate on kinesthetic figur al
aftereff ects. Bri tish Journal of Psychology, 53, 17-26.Das, "G. (1961). Standardization of Maudsley Personality Inventory (MPI) on an Indian
population. Journal of Psychological Researches, 5, 7-9.Davies, D.R. &: Tune, G.S. (1970). Human Vigilance Performance. London: Staples
Press.Eysenck, H.J. (1955). Cortical inhlbi tion, figural aftereffect and theory of
personal!ty. Journal of Abnormal and Social Psychology, 51, 94-106.Eysenck, H.J. (1959). Manual of Maudsley Personality Inventory. London: Uni versi ty
of London Press.Eysenck, H.J. (1967). The Biological Basis of Personality. Springfield, IL: Thomas.Eysenck, H.J. &: Easterbrook, J.A. (1960). Drugs and personality. X. The effects of
stimulant and depressant drugs upon kinesthetic figural aftereffects. Journal ofMental Sci ence, 106, 852-854.
178 u. Gupta
Franz, D.N. (1975). Drugs acting on the central nervous system: introduction. InL.S. Goodman &. A. Gilman (eds , }, The Pharmacological Basis of Therapeutics. NewYork: Macmillan.
Gupta, B.S. (1974). Stimulant and depressant drugs on kinesthetic figuralaftereffects. Psychopharmacologia, 36, 275-280.
Gupta, B.S. &. Jit, R. (1979). Individual consistencies in kinesthetic figuralaftereffects. Psychological Studies, 24, 106-112.
Gupta, B.S. &: Kaur, S. (1978). The effects of dextroamphetamine on kinestheticfigural aftereffects. Psychopharmacology, 56, 199-204.
Hare, R.D. (1970). Psychopathy, Theory and Research. New York: WHey.Harvey, S.C. (1975). Hypnotics and sedativesathe barbiturates. In L.S. Goodman &: A.
Gilman (eds ,}, The Pharmacological Basis of Therapeutics. New York: Macmi1lan.Innes, I.R. &: Nickerson, M. (1975). Norepinephrine, epinephrine, and the
sympathomimetic amines. In L.S. Goodman &: A •. Gilman (e ds v ) , ThePharmacological Basis of Therapeutics. New York: Macmillan.
Klein, G. &: Krech, D. (1952). Cortical conductivity in the brain injured. Journal ofPersonality, 21, 118-148.
Konler, W. &: Dinnerstein, D. (1947). Figural aftereffects in kinesthesis. In A.Michotte (edv) , Miscellanea Psychologica. Louvain: Catholic Uni versity ofLouvain.
Kohler , W. &: Wallach, H. (1944). Figural aftereffects: an investigation of visualprocesses. Proceedings of the American Philosophical Society, 88, 265-357.
Kostin, I. W., Baker, A. H., Mishara, B.L. &. Parker, L. (1978). Kinestheticaftereffect, organismic state and retest reliability. British Journal ofPsychology, 69, 475-482.
McDonald, A. (1974). The lack of effect of D-amphetamine on perceptual reactance andpersonality. Journal of Abnormal Psychology, 83, 87-90.
Mlshara, B.L. &. Baker, A.H. (1978). Kinesthetic aftereffect scores are reliable.Applied Psychological Measurement, 2, 239-247.
Morgan, A. &: Hilgard, E. (1972) • The lack of retest reliabili ty for indi vidualdifferences in the kinesthetic aftereffect. Educational and PsychologicalMeasurement, 32, 871-878.
Over, R. (1970) • Indi vidual diff erences in figural aftereff ects. PsychologicalBulletin, 74, 405-410.
Platt , D., Holtzman, P. &. Larson, D. (1971). Individual consistencies in kinestheticfigural aftereffects. Perceptual and Motor Skills, 32, 787-795.
Poser, E.G., Knight, D.A. &. Lehmann, H.E. (1958). The Influence of Excitant andDepressant Drugs on Kinesthetic Figural Aftereffect. Paper read at the AnnualConvention of the APA.
Price, H.L. (1975). General anesthetics: intravenous anesthetics , In L.S. Goodman &:A. Gilman (eds .}, The Pharmacological Basis of Therapeutics. New York:Macmillan.
Sales, S. &. Throop, W. (1972). Relationship between kinesthetic aftereffect andstrength of the nervous system. Psychophysiology, 9, 492-497.
Weintraub, D.J. &: Herzog, T.R. (1973). The kinesthetic aftereffect: ritual versusrequisites. American Journal of Psychology, 86, 407-423.
Weintraub, D.J., Green, G.S. &. Herzog, T.·R. (1973). Kinesthetic aftereffects day byday: trends, task features, reliable indi vidual differences. American Journal ofPsychology, 86, 827-844.
Wertheimer, M. &: Wertheimer, N. (1954). A metabolic interpretation of individualdiff erences in figural aftereffects. Psychological Review, 61, 279-280.

Phenobarbitone and Kinaesthetic After-effect 179
Wertheimer, M., Levine, H. &: Wertheimer, N. (1955). The effect of experimentallyinduced changes in metabolism on perceptual measures of metabolic efficiency.Perceptual and Motor Skills, 5, 173-176.
UMA GUPTA clo Dr B.S. Gupta, Department of Psychology, Institute of AdvancedStudies, Meerut University, Meerut, India.
Date of acceptance for publication: June 1982