-
8/10/2019 Pharmacotherapy of Shock.ppt
1/23
10/27/2014 1
Pharmacotherapy
of Shock
-
8/10/2019 Pharmacotherapy of Shock.ppt
2/23
10/27/2014 2
Introduction
Review the current view on
etiology, pathophysiology and
management of shock withemphasis on pharmacotherapy.
Daniel Game, M.D.
O. D. Polk, Jr., M.D.
Wayne Davis, M.D.
-
8/10/2019 Pharmacotherapy of Shock.ppt
3/23
10/27/2014 3
Topics of Discussion
Pathophysiology of Shock
Types of Circulatory Shock
Management of Shock Inotropic Agents
Vasodilators
-
8/10/2019 Pharmacotherapy of Shock.ppt
4/23
10/27/2014 4
Shock
Term choc French for push or
impact was first published in 1743
by the physician LeDran Beliefsymptoms arose from fear
or some other form of altered
cerebral function
Crile in 1899 showed that
replacement of blood volume
decreased mortality experimentally
-
8/10/2019 Pharmacotherapy of Shock.ppt
5/23
10/27/2014 5
Determinants of Shock
Inadequate tissue perfusion
Sustained loss of effective circulatory
blood volume
Breakdown of cellular metabolism and
microcirculatory homeostasis
Hypoperfusion of peripheral tissue
that leads to a diminutive
transcapillary exchange function
Disproportion between VO2and DO2
-
8/10/2019 Pharmacotherapy of Shock.ppt
6/23
10/27/2014 6
Hemodynamic States of
Shock Hyperdynamic State
Hypodynamic State
Related to: Cardiac Output (CO)
Systemic Vascular Resistance
(SVR)
-
8/10/2019 Pharmacotherapy of Shock.ppt
7/23
10/27/2014 7
Pathophysiology of
Shock Shock develops with inadequate
capillary perfusion by decreased
Cardiac Output following heartattack (cardiogenic shock) or
blood/volume loss (hypovolemic
shock)
-
8/10/2019 Pharmacotherapy of Shock.ppt
8/23
10/27/2014 8
Mediators of Shock
Toxins
Endotoxins
Oligo- and polypeptides
Complement Factors
Opiods
TNF, Interleukins
Fatty Acid Derivatives
Arachidonic acid metabolites Varia
Calcium
-
8/10/2019 Pharmacotherapy of Shock.ppt
9/23
10/27/2014 9
Main Classes of Shock
Hypovolemic Shock
Distributive Shock Cardiogenic Shock
Obstructive Shock
-
8/10/2019 Pharmacotherapy of Shock.ppt
10/23
10/27/2014 10
Hypovolemic Shock
Hemorrhagic/Traumatic
Dehydrative Burn
-
8/10/2019 Pharmacotherapy of Shock.ppt
11/23
10/27/2014 11
Distributive Shock
Septic
Anaphylactic/
Anaphylactoid
Neurogenic
-
8/10/2019 Pharmacotherapy of Shock.ppt
12/23
10/27/2014 12
Obstructive Shock
Pulmonary Embolism
Cardiac Tamponade
Pneumothorax
-
8/10/2019 Pharmacotherapy of Shock.ppt
13/23
10/27/2014 13
Question
Which one of the folowing is the most common cause of severe
Lactic acidosis (blood lactate concentration >5 mmol/L)?
a. Ethanol intoxicationb. Severe liver disease
c. Circulatory shock
d. Ischemic bowel
e. Acute asthma
-
8/10/2019 Pharmacotherapy of Shock.ppt
14/23
10/27/2014 14
Management of Shock
Shock begins when DO2 to the
cells is inadequate to meet
metabolic demand The major therapeutic goals in
shock therefore are sufficient
tissue perfusion and oxygenation
Early diagnosis remains a major
problem
-
8/10/2019 Pharmacotherapy of Shock.ppt
15/23
10/27/2014 15
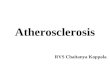
Pulmonary Artery
Catheter WaveformsRight Atrium Right Ventricle Pulmonary Artery
PCWP
-
8/10/2019 Pharmacotherapy of Shock.ppt
16/23
10/27/2014 16
Hemodynamic Characteristics inDifferent Types of Shock
Type Preload CO PVR SVR
Hemmorrhagic
Anaphylactic
Cardiogenic
Septic(Hyperdynamic)
Septic
(Hypodynamic)
/
-
8/10/2019 Pharmacotherapy of Shock.ppt
17/23
10/27/2014 17
QuestionThe wavefrom shown in this figure was observed while
attempting to advance a pulmonary arterial catheter, with
the
Balloon inflated, from the proximal pulmonatry artery to a
wedged position.
Wh
i
c
h
Which one of the following best explains the terminal
portion of the depicted waveform?
a. Pulmonary hypertensionb. Mitral regurgitation
c. Severe left ventricular dysfunction
d. Obstruction of the catheter tip
e. Pericardial tamponade
-
8/10/2019 Pharmacotherapy of Shock.ppt
18/23
10/27/2014 18
Inotropic Agents and
Vasodilators Vasoactive drugs are an important
pharmacologic defense in the
treatment of shock.
May be required to support BP in the
early stages of shock.
These agents may be needed to:
Enhance CO through the use of inotropic
agents
Increase SVR through the use of
vasopressors
-
8/10/2019 Pharmacotherapy of Shock.ppt
19/23
10/27/2014 19
Effects of Inotropic
Agents and VasodilatorsEpinephrine a1,b1, (b2) 0.020.5
Norepinephrine a1, b1 0 - 0.05
0.5Dopamine b2,DR, (a) 2 -12
Dobutamine b1, b2 2 - 12
Dopexamine b1, b2, DR 0 - 0.9 - 5
Vasopressin Angiotensin III 5 - 20
Amrinone PDI 5 -10
Drug Receptor CO SVR Dose Range
0 -
(mg/kg/min)
1
-
8/10/2019 Pharmacotherapy of Shock.ppt
20/23
10/27/2014 20
Effects of Inotropic
Agents and Vasodilators
Nifedipine 0 - 0.5 - 10
Nitroglycerin 0 - 3 - 5
Nitroprusside 0 - 0.5 - 5
Prostacyclin 10 - 40
2
Drug CO SVR Dose Range
(mg/kg/min)
-
8/10/2019 Pharmacotherapy of Shock.ppt
21/23
10/27/2014 21
DopamineAn endogenous precursor of norepinephrine with
multiple dose-related effects
Low Dose (0.5 - 3 mg/kg/min)
b2and dopaminergic (DR) effects
Enhanced blood flow to renal andsplanchnic beds
Moderate Dose (5 -10 mg/kg/min)
Positive inotropic effects
High Dose (>20 mg/kg/min)
a-actions (vasoconstriction)
-
8/10/2019 Pharmacotherapy of Shock.ppt
22/23
10/27/2014 22
Question
-
8/10/2019 Pharmacotherapy of Shock.ppt
23/23
10/27/2014 23
Reference
Pharmacotherapy of Shock. In: The Pharmacologic
Approach to the Critically Ill Patient, 3rded. Williams&
Wilkins,1994, pp 11041121.






![Expo Dr Campitos - Shock.ppt [Autoguardado]](https://img.dokumen.tips/doc/110x75/5695d08f1a28ab9b0292f0ec/expo-dr-campitos-shockppt-autoguardado.jpg)