Embed Size (px)
Citation preview

Thorax 1992;47:651-656
Thepulmonary physician and critical care 3 Serieseditor: TWEvans
Pharmacotherapy in lung injury
M Messent, M J D Griffiths
The term adult respiratory distress syndrome(ARDS) was first used in 1967 to define thecondition of severe parenchymal lung injuryleading to refractory hypoxaemia in theabsence of left ventricular failure.' In 1972 itwas suggested that there are around 150 000cases of ARDS a year in the United Statesalone,2 but European data are scarce andestimates of incidence vary widely. A recentretrospective study in a single region of theUnited Kingdom identified 2 5 cases a year per100 000 population,3 suggesting that 1000-1500 cases of established ARDS occur inBritain each year. The associated mortality ishigh,4 approaching 70% in patients with sepsiscomplicated by ARDS and 90% when ARDSfollows aspiration pneumonia.5 The cause ofdeath depends on the underlying insult, its siteand severity, the response to treatment, and theincidence ofcomplications affecting other organsystems: irreversible respiratory failure is res-ponsible for only 16% of deaths,6 and mostdeaths are due to multiple organ failure.The clinical features that define ARDS can in
part be attributed to an increase in permeabilityof the alveolar-capillary membrane. It is nowapparent that increased vascular leakinessoccurs in other organs, such as the kidney,7 andall capillary beds seem likely to be influenced bythe disease process to a greater or lesser extent.The endothelium is emerging as an importantregulatory body in pulmonary8 and systemic'vascular control and endothelial damage hasimportant implications for the development ofboth ARDS and the syndrome of multipleorgan failure.Only a few of the patients with conditions
associated with the development of ARDS,develop the full blown syndrome.'" Con-sequently, there has been a growing awarenessthat ARDS represents the end of a spectrum ofacute lung injury. The clinical criteria used todiagnose the condition at present are thereforetoo broad to allow comparisons of diseaseseverity between different patients and clinicalcentres, which has important implications forthe scientific evaluation ofpotential therapeuticinterventions. Murray et al" have developed ascore for patients with lung injury that takesaccount of the appearance of the chest radio-graph, pulmonary compliance, the degree ofhypoxaemia, and the degree of positive endexpiratory pressure (PEEP) used in ventilatorysupport. These variables are graded forseverity, permitting the calculation of an
overall score of injury. Although this approachshould change the perception of ARDS as asingle disease entity and improve the way inwhich the efficacy ofnew treatments is assessed,limitations remain, including the omission of aloading factor for the underlying illness, whichundoubtedly influences prognosis.The treatment of lung injury up to and
including ARDS remains supportive. Despitethe use of sophisticated ventilatory techniquesand extracorporeal membrane oxygenation,mortality is unaltered and no specific pharma-cotherapy has been developed.
Aetiology and pathophysiologyTable 1 shows the most common causes ofacute lung injury and ARDS. These can bedivided into two groups: those that directlydamage the lung and those in which a remotedisease process is complicated by ARDS,presumably through the action of humoralinflammatory mediators. Probably identicalmediators directly damage the alveocapillarymembrane when released locally-for example,during pneumonia. Identifying these substan-ces and their mechanisms ofrelease, action, andinteraction therefore holds the key to under-standing the pathophysiology of ARDS andthus developing effective therapeutic interven-tions.
Sepsis is a systemic insult resulting in panen-dothelial damage, cardiovascular dysfunc-tion,'2 and ultimately multiple organ failure,which includes ARDS in up to a quarter ofcases.'3 Recent reports have described patientsfulfilling the criteria for the sepsis syndromewith no demonstrable focus of infection, sug-gesting that uncontrolled activation ofmediators of inflammation regardless of causecan reproduce clinical sepsis.'4 An identicalphenomenon has been described in patientswith ARDS in whom rigorous efforts were
Table 1 Conditions associated with the adultrespiratory distress syndrome
Pulmonary Non-pulmonary
Aspiration SepsisNear drowning Fat embolismSmoke inhalation HypovolaemiaDirect lung trauma Head injuryPneumonia Disseminated intravascular
coagulationPancreatitisEclampsia
Department ofAnaesthetics andIntensive Care, RoyalBrompton andNational Heart andLung Hospital, LondonSW3 6LYM MessentM J D GriffithsReprint requests to:Dr M Messent
651
on May 4, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.47.8.651 on 1 A
ugust 1992. Dow
nloaded from

Messent, Griffiths
T cell activation
Lipo,Tumour necrosis Tumour necrosis factor, Interferon cs, 11-4,11-5,factor ~~~11-2, Interferon a-
endotoxin factor, 11-6, B cell activation
ic\inflamllkon
\Tumou r necrosis factor,\Reactive-oxygen species,\elastase, membrane attack\complex\ | ~~~~~~Microvascular leak
Loss of hypoxicEndothelial damage 1, pulmonaryvasoconstriction
Intravascularthrombosis
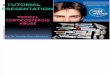
Figure 1 Some interactions between inflammatory mediators in the adult respiratorydistress syndrome initiated by endotoxaemia. Il-interleukin.
made to exclude infection.'5 A model of inter-actions between some mediators thought tocontribute to acute lung injury associated withsepsis is shown in figure 1.
The role of mediators in ARDSENDOTOXINInfusion of endotoxin or lipopolysaccharide, aGram negative bacterial cell wall component,produces clinical signs identical to the sepsissyndrome that include ARDS in experimentalanimal models.'6 The hydrophobic lipid Amoiety of lipopolysaccharide, which interactswith host and bacterial cell membranes, isthought to be responsible for most of thetoxicity of lipopolysaccharide and is highlyconserved between Gram negative species.Assays of lipid A in intensive care units haveshown predictably high concentrations inpatients with recognised sepsis. Raised con-centrations have also been found in patientswith haemodynamic compromise secondary tovariceal bleeding and major trauma, possibly asa result of translocation of bacteria or their cellwall constituents across gut mucosa whosebarrier function has been impaired byischaemia. All patients with ARDS in thisstudy had detectable endotoxaemia.'7
CYTOKINESMany toxic effects of lipopolysaccharide aremediated by the local and systemic release ofcytokines, which are low molecular weightglycoproteins. Technological advances of thelast decade have facilitated the identification,cloning, recombinant synthesis, and functionalstudy ofmany cytokines. 8 The large number ofmolecules, their complex interactions, andtheir often overlapping effects have complicatedassessment of the role of individual agents.There is, however, now compelling evidencethat the monokines (monocyte derived cyto-
kines); interleukins (IL) Il-l, 11-6, 11-8; andespecially tumour necrosis factor contribute tothe uncontrolled inflammatory cascade that ismanifest as the sepsis syndrome. Injection oftumour necrosis factor into rats produces pul-monary lesions indistinguishable from those ofARDS,"9 and raised concentrations of tumournecrosis factor and Il-l have been found inblood samples and bronchoalveolar lavage fluidtaken from patients with the clinical syn-drome.20"2 The relative contributions of directtoxic effects of monokines and those causedindirectly by products of activated cells andsecondary mediators are not clear.
In the fibroproliferative phase of ARDSlocally produced cytokines are thought toregulate the growth, chemotaxis, and metabolicactivity of lung fibroblasts, influencing theultimate balance between fibrosis and remodel-ling of normal lung tissues.22
NEUTROPHILSThe important role played by neutrophils inmediating acute lung injury has been estab-lished in both clinical studies and animalmodels.23 Depletion of neutrophils preventsacute lung injury in sheep following the injec-tion of neutrophil activators. Although ARDSoccurs in neutropenic patients, the extent oflung injury is increased by neutrophil sup-plementation. The importance of endothelialcell and neutrophil adhesion molecules inorchestrating interactions between the twocells is now established.24 Expression ofadherence molecules is controlled by activatorsof neutrophils, such as lipopolysaccharide,tumour necrosis factor, I1-1, and the productsof complement activation.25 Dissection of theindividual stages of neutrophil activation andadhesion is likely to provide targets for futureimmunopharmacological interventions. Themechanisms governing neutrophil responses inARDS are reviewed in a recent editorial in thisjournal by Donnelly and Haslett.26
Neutrophils damage endothelial cells direc-tly by the release of proteolytic enzymes (forexample, elastase), reactive oxygen species, andother inflammatory mediators (for example,platelet activating factor). Intravenous admin-istration of elastase increases pulmonary vas-cular resistance, induces pulmonary leucostasisand microembolisation, and increases the ven-ous admixture of oxygen.27 Experimentaladministration of agents that generate reactiveoxygen species causes pathological changesresembling those of ARDS.28 Apart fromdamaging endothelial cells directly, elastaseand reactive oxygen species inactivate proteaseinhibitors and detoxifying agents (such asglutathione) in their microenvironment, facil-itating their own actions and those of unrelatedinflammatory mediators. Studies of broncho-alveolar lavage fluid in patients with ARDShave produced evidence of increased oxidantand elastolytic activity.29 30
LIPID MEDIATORSLipid mediators are formed after the activationof membrane phospholipase A2 and probablymediate many ofthe inflammatory effects ofthe
652
on May 4, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.47.8.651 on 1 A
ugust 1992. Dow
nloaded from

Pharmacotherapy in lung injury
Acetyltransferase
Lipoxy!
Le
genase Cyclo-oxygenase
trienes rCyclic endoperoxides
Prostacyclin Thromboxanesynthetase synthetase
|Prostacyclin2 Thromboxane Ai
Figure 2 The synthetic pathway of lipid mediators in the adult respiratory distresssyndrome and sites ofpossible pharmacological manipulation.PAF-platelet activating factor; NSAIDs-non-steroidal anti-inflammatory drugs.
agents described above. The synthetic path-ways of these chemically related compoundsand means of their pharmacological manipula-tion are shown in figure 2. Platelet activatingfactor is released by white blood cells, endo-thelial cells and alveolar macrophages. Admin-istration of platelet activating factor causes
activation of platelets and neutrophils andreproduces many features ofendotoxic shock invivo," including pulmonary hypertension andoedema, decreased compliance, and broncho-constriction."The most extensively studied arachidonic
acid metabolites in acute lung injury are throm-boxane and the leukotrienes, whose actionsclosely resemble those of platelet activatingfactor." "
PEPTIDE MEDIATORS
Figure 3 shows how activation of theproteolytic cascades of the complement,coagulation, and contact systems by endotoxinmay contribute to the pathogenesis of ARDS.Intravenous C5a causes hypotension and leu-copenia in animals. This is associated with
Neutrophil activation
Alternative complement Endothelial
pathway damage
Membrane attackcomplex
Lipopolysaccharide- -Endothelium - Tissue factor
endotoxin lntravscular
thrombosis
Factor XII Coagulation cascade
|Contact system Bradykinin Vasodilation
Figure 3 Schematic representation of the possible role ofpeptide mediators in thepathogenesis of the adult respiratory distress syndrome initiated by endotoxaemia.
activation and aggregation of neutrophils,which can be seen in the lung and are associatedwith increased permeability of the pulmonaryendothelium.35 Activation products of com-plement are increased in human sepsis and apositive correlation has been shown betweentheir plasma concentrations and the develop-ment of ARDS.'6 This finding has not,however, been confirmed in subsequentstudies."7
PharmacotherapyCORTICOSTEROIDSCorticosteroid treatment has been advocatedfor patients at risk from ARDS and thosewhose disease is detected early in its course onthe basis of favourable reports from non-randomised trials. A prospective study bySchumer also suggested that corticosteroidsreduced the mortality in septic shock from38-4% to 10-5%.38 Nevertheless, two largerandomised controlled prospective studiesfailed to show any benefit from corticosteroidtreatment and suggested that mortality inpatients with sepsis may even be increased.'9 40Steroids have been used recently in patientsrecovering from ARDS who then developedthe signs of sepsis with no identifiable source.'5Results from this study and isolated casereports on similar patients4" suggest that fur-ther trials of steroids in the late phase ofARDSare warranted.
NEUTRALISATION OF THE EFFECTS OF ENDOTOXINTwo large trials have been published recentlydescribing the effects ofmonoclonal antibodiesto endotoxin core glycoprotein in the humansepsis syndrome.424' Both showed advantagesin terms of survival and resolution of systemfailures only in subgroups of patients. E5, amurine IgM antibody, significantly decreasedmortality in patients with Gram negative sepsiswith no evidence of circulatory shock. In thisgroup, 28% ofthe total, ARDS resolved in fourof 10 patients who received E5 compared withtwo of nine patients given placebo. By contrast,HA-lA, a human monoclonal IgM antibody,was found to be effective regardless of shock,but only in patients with proved Gram negativebacteraemia. Data specific to ARDS were notgiven, but in the group that responded all majormorbidities (including ARDS) resolved withinseven days in 38 of 61 patients given HA-lAcompared with 26 of 62 given placebo. Therewere no significant side effects attributable toeither antibody. Problems that may precludethe more widespread application of these noveltreatments include their high cost and difficul-ties in identifying those patients with Gramnegative bacteraemia (about 30%) rapidlyenough to maximise the therapeutic potential.
MODULATION OF THE CYTOKINE RESPONSEIt is theoretically possible to block the damag-ing effects ofcytokines at several levels (see table2), though most of these potential treatmentsare as yet untried in vivo. Animal studies haveshown that when administered prophylacti-cally neutralising antibodies for tumour
653
on May 4, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.47.8.651 on 1 A
ugust 1992. Dow
nloaded from

Messent, Griffiths
Table 2 Modulation of the cytokine response in the adult respiratory distress syndromeand sepsis
Inhibition of cytokine production
Binding of cytokines
Binding of cytokine receptors
Modulation of cytokine receptors
Interference with postreceptorevents
Induction of cell protection
Enhanced cytokine clearance
Corticosteroids,44 pentoxifylline,45 dietary n-3fatty acids,' interleukin-4,47
Monoclonal antibodies, CB0006 anti-TNFa,4haemofilters (eg polyacrylnitrite49)
Monoclonal antibody against the murine Il-Ireceptor."'
Down regulation of murine TNF and Il-l byIl-li"
Cyclooxygenase inhibitors ibuprofen,"prostacyclin and PGE,,53 antioxidants (egvitamin E,54)
Induction of production of antioxidant enzymesand heat shock proteins by Il-L."
High volume haemofiltration."
oxygen species by macrophages, and inducingT lymphocyte suppressor function, have beenthought to be of potential therapeutic benefit.63Patients with ARDS had an increased 30 daysurvival rate, though most were from a surgicalintensive care unit with inadequate documen-tation of pulmonary artery occlusion pres-sures,64 and a subsequent multicentre trial ofPGE, treatment failed to show a reduction inmortality.65
Inhibition of thromboxane by dazoxiben, aspecific thromboxane inhibitor, was not bene-ficial in established ARDS,66 but a randomisedprospective study in patients at risk showed areduced incidence in the group given ketocon-azole, which reduces plasma thromboxaneconcentrations in vivo.67
TNF-tumour necrosis factor; Il-1-interleukin 1; PGE,-prostaglandin E,.
necrosis factor protect against lethal endotox-aemia and bacteraemia,5758 though only onestudy has shown benefit when such antibodieswere given after injury.59 A phase 1 study of amurine IgG monoclonal antibody to recombi-nant human tumour necrosis factor in patientswith septic shock revealed no serious sideeffects,48 and results ofa larger study examiningtherapeutic efficacy are awaited.
Haemofiltration is a mainstay of the suppor-tive treatment of multiorgan failure andARDS, facilitating the correction of bio-chemical abnormalities and fluid balance; butrecent studies have also suggested that highvolume pumped veno-venous haemofiltrationmay be useful in removing mediators of sep-sis.56 No trials have assessed the possible benefitof introducing haemofiltration in sepsis orARDS earlier than is indicated by traditionalcriteria. Future developments in this area mayinvolve incorporation of antibodies or othermaterials known to bind cytokines into filtrationmembranes.
Non-steroidal anti-inflammatory drugsClinical data on the use of non-steroidal anti-inflammatory drugs in ARDS are scarce,though theoretically they should be ofbenefit inthe late and established phases of ARDS. Inanimal models ibuprofen and indomethacinhave been shown to alter the course of acutelung injury. In the early phases pulmonaryhypertension was reduced, arterial hypoxaemiadiminished, and neutrophil adherence andactivation decreased. The incidence of pul-monary oedema was also less in treatedsubjects."' So far, however, there is noevidence from any large clinical trial to supportthe use of non-steroidal anti-inflammatorydrugs despite encouraging experimental data(reviewed in ref 63).
PROSTAGLANDINProstaglandins (PG) El and E2, by preventingplatelet adherence, reducing pulmonary hyper-tension, causing a decrease in lymphokineproduction and the generation of reactive
ANTIOXIDANTSIn patients with early ARDS and in those athigh risk protection against reactive oxygenspecies mediated injury by the use ofN acetylcysteine has been shown to reduce injury. Theliver frees cysteine, itself a free radical scaven-ger, for incorporation into glutathione, apowerful scavenger of reactive oxygen species.Preliminary studies have been completed and amulticentre trial is now under way.' The use ofspecific antioxidants in ARDS is complicatedby the pro-oxidant effect of many of thesecompounds. Lower concentrations of theantioxidant vitamin E have been found inpatients who develop ARDS than in those whodo not,69 but high concentrations of bothvitamin E and vitamin C have been shown topromote lipid peroxidation, suggesting theyproduce damage mediated by free radicals.70 Inthe isolated perfused rat lung model reactiveoxygen scavenging with dimethylthioureaprevents damage caused by activated neutro-phils.7"
PENTOXIFYLLINEPentoxifylline is a methylxanthine derivativethat reduces the production of tumour necrosisfactor and Il-l and decreases the response ofneutrophils727' and the pulmonary endothe-lium to these cytokines. It also improves redcell deformability and decreases red cell andplatelet aggregation. The haemodynamicchanges associated with sepsis are ameliorated,as are indices of lung injury, when pentoxi-fylline is used either before or soon after apulmonary insult.74 Oxygen delivery is main-tained in models of haemodynamic shock,possibly by preventing white cell adherence inthe pulmonary and systemic microcircula-tions.75 This suggests a potential role for pen-toxifylline in ARDS, although this has yet to bedefined.
SURFACTANTThe increased activity mediated by reactiveoxygen species that is associated with ARDSreduces the concentration of alveolar surfac-tant. Surfactant production by type II pneu-mocytes is further influenced by hypoxia,hyperoxia, and infection. Bronchoalveolarlavage fluid from patients with ARDS containslow concentrations of surfactant.76 In the infan-
654
on May 4, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.47.8.651 on 1 A
ugust 1992. Dow
nloaded from

Pharmacotherapy in lung injury
tile respiratory distress syndrome instillation ofsurfactant has a profoundly beneficial effect onoutcome.77 Similarly, in animal studies exo-genous surfactant replacement has been shownto reduce shear forces in damaged lung andreduce injury.78 Trials are under way to assessthe value of surfactant in ARDS.
MANIPULATION OF THE L-ARGININE PATHWAYThere is now good evidence that induction ofnitric oxide synthase by inflammatorymediators contributes to the resistant hypoten-sion of septic shock.79 Reports of two suchpatients being successfully treated with aninhibitor of nitric oxide synthesis have beenpublished recently.80 The characteristic pul-monary circulatory changes of sepsis andARDS, however, are loss of hypoxic pulmon-ary vasoconstriction and hypertension. Studiesin rats have implicated nitric oxide in themodulation of hypoxic pulmonary vaso-constriction and have suggested that low dosetumour necrosis factor inhibits the action ofnitric oxide before disrupting the endo-thelium.8' 82 Hence inhaled nitric oxide hasbeen used in certain centres to decrease pul-monary vascular resistance and to improveoxygenation by decreasing intravascular shunt.Results have yet to be published. Concernabout the toxicity of inhaled nitric oxide hasbeen allayed by recent experience in animals83and patients.84 Furthermore, in many respectsinhaled nitric oxide is an ideal pulmonaryvasodilator as it is inactivated by haemoglobinin the circulation rapidly enough to preventsystemic actions and dilates only vessels sup-plying ventilated alveoli.
ConclusionsRecent advances suggest that similar inflam-matory processes may generate the sepsissyndrome and ARDS by their uncontrolledsystemic and pulmonary actions. Discovery ofan ever increasing number of inflammatorymediators has provided new targets forimmune therapy, but has also revealed a com-plex system with enormous redundancy,implying that a single agent is unlikely to beable to arrest the process once initiated. In thisrespect targeting initiators or early mediators,such as endotoxin, is an attractive option but itdepends on instituting treatment immediatelyafter the insult, which is not always feasible inthe clinical setting.Monoclonal antibody technology has
developed to such a level that binding ofindividual mediators or receptors is now beingused in clinical practice.85 Such treatments willbe expensive and should be introduced onlyafter their efficacy has been proved in large, welldesigned trials. Costs can also be offset againstthe benefits of decreased mortality in patientswho are often young and expected to recoverfully, and of a shorter time spent within theintensive care unit.Optimism about anti-inflammatory treat-
ments has been dampened by their consistentfailure in trials. Corticosteroids cannot berecommended for routine use in patients with
ARDS, though certain subgroups-for eam-ple, those with fat embolism-may benefit.Given the high incidence of infection com-plicating ARDS, immunosuppressant treat-ment must be used with caution. Of the newagents outlined above, inhaled nitric oxide isparticularly exciting, though its emerging roleas an immunomodulator and its interactionwith reactive oxygen species remain to becharacterised.
MM is supported by the BUPA Medical Research Trust, andMJDG is Wellcome clinical research fellow in intensive care.
1 Ashbaugh DG, Bigelow DB, Petty TL, Levine BE. Acuterespiratory distress in adults. Lancet 1967;ii:319-23.
2 Lung Programme, National Heart and Lung Institute.Respiratory diseases: task force on problems, researchapproaches, needs. Washington DC: Government PrintingOffice, 1972. (DHEW publication No NIH073-432.)
3 Webster NR, Cohen AT, Nunn JF. Adult respiratorydistress syndrome. How many cases in the UK? Anaes-thesia 1988;43:923-6.
4 Fein AM, Lippman M, Holtzman H, ElrazA, Goldberg SK.-"-4e-risk factors, incidence and prognosis of ARDS
following sepacemia. Chest 1983;83:40-2.5 Fowler AA, Hamman RF, Zerbe G6, Benson KN, Hyers
TM. Adult respiratory distress syndrome: prognosis afteronset. Am Rev Respir Dis 1985;132:472-8.
6 Montgomery B, Stager MA, Carrico CJ, Hudson LD.Causes of mortality in patients with the adult respiratorydistress syndrome. Am Rev Respir Dis 1985;143:485-9.
7 Kreutzfelder E, Joka T, Kienecke H, et al. Adult respiratorydistress syndrome as a specific manifestation of a generalpermeability defect. Am Rev Respir Dis 1988;137:95-9.
8 Lui SF, Crawley DG, Barnes PJ, Evans TW. Endotheliumderived relaxant factor modulates hypoxic vasoconstric-tion in isolated blood perfused rat lungs. Am Rev RespirDis 1991;143:32-7.
9 Vallance P, Moncada S. Effects of endothelially derived nitricoxide on peripheral arterial tone in man. Lancet 1989;ii:997-1000.
10 Fowler AA, Hamman RF, Good JT, et al. Adult respiratorydistress syndrome: risk with common predictors. AnnIntern Med 1983;98:593-7.
11 Murray JF. An expanded definition ofARDS. Am Rev RespirDis 1988;138:720-3.
12 Thijs LG, Schneider AJ, Groeneveld ABJ. The haemo-dynamics of septic shock. Intens Care Med 1990;16(suppl3):S182-6.
13 Bone RC, Fisher CJ, Clemmer TP, et al. The sepsissyndrome: a valid clinical entity. Crit Care Med 1989;17:389-93.
14 Leatherman JW, Schmitz PG. A pseudo-sepsis syndromeassociated with chronic salicylate intoxication. Chest1991;100:1391-6.
15 Meduri GU, Belenchia JM, Estes RJ, Wunderink RG, ElTorky M, Leeper V. Firoproliferative phase of ARDS.Clinical findings and effects of corticosteroids. Chest1991;100:943-52.
16 Brigham KL, Meyrick B. Endotoxin and lung injury. AmRev Respir Dis 1986;133:913-27.
17 Vijaykumar E, Raziuddin S, Wardle EN. Plasma endotoxinin patients with trauma, sepsis and severe haemorrhage.Clin Intens Care 1991;2:4-9.
18 Arai K, Lee F, Miyajima A, Miyatake S, Arai N, Yokota T.Cytokines: co-ordinators of immune and inflammatoryresponses. Ann Rev Biochem 1990;59:783-836.
19 Ferrari-Baliviera E, Mealy K, Smith RJ, Wilmore DW.Tumour necrosis factor induces ARDS in rats. Arch Surg1989;124:1400-5.
20 Jacobs RF, Tabor DR, Burks AW, Campbell GD. ElevatedIl-1 release by human alveolar macrophages duringARDS. Am Rev Respir Dis 1989;140:1686-92.
21 Hyers TM, Tricomi SM, Dettenmeier PA, Fowler AA.TNF levels in serum and bronchoalveolar lavage fluid ofpatients with the adult respiratory distress syndrome. AmRev Respir Dis 1991;144:268-71.
22 Knighton DR, Fiegel VD. Growth factors and repair. In:- Bihari DG, Cerra FB, eds. Multiple organ failure. New
f7) Iorizons III. California: Fullerton, 1989:371-89.i(23 Wepine JE, Beehler CJ. Neutrophils and ARDS: two inter-
locking perspectives in 1991. Am Rev Respir Dis 1991-144:251-2.
24 Wright SD, Detmers PA. Adherence promoting receptorson phagocytes. J Cell Sci 1988;9(suppl):99-120.
25 Leuwenberg JFM, Jeunehomme TMMA, Buurman WA.Induction of an activation antigen on human endothelialcells in vitro. Eur J Immunol 1989;18:1469-72.
26 Donnelly SC, Haslett C. Cellular mechanisms of acute lung
655
on May 4, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.47.8.651 on 1 A
ugust 1992. Dow
nloaded from

Messent, Griffiths
injury: implications for future treatment in adult res-piratory distress syndrome. Thorax 1992;47:260-4.
27 Stokke T, Burchardi H, Hensel A, Kostering H, Kartner T,Rahlf G. Continuous intravenous infusion of elastase innormal agranulocytic minipigs, effects on the lungs and theblood coagulation system. Resuscitation 1986;14:61-79.
28 Goris RJA, Nuytinck JKS, Boekholtz WKF, van BebberIPT, Schillings PHM. Multi-organ without bacteria. In:Novelli GP, ed. Oxygen free radicals in shock. Basel:Karger, 1986:76-88.
29 Lee CT, Fein-AM,Lippman M, Holtzman H, Kimbel P,Weinbau& stolytic activity in pulmonary lavagefluid from patients with ARDS. N Engl J Med 1981;304:192-6.
30 Cochrane GC, Spragg RG, Revak SD. Studies on thepathogenesis of ARDS: evidence of oxidant activity inbronchoalveolar lavage fluid. J Clin Invest 1983;71:754-61.
31 Pinkard RN, Ludwig JC, McManus LM. Platelet activatingfactors. In: Gallin JJ, Goldstein IM, Syderman R, eds.Inflammation: basic principles and clinical correlates. NewYork: Raven Press, 1988:139-67.
32 Hamasaki H, Mojarad M, Saga S, Tai HH, Said SI. PAFraises airway and vascular pressures and induces oedemain lungs perfused with platelet-free solution. Am RevRespir Dis 1984;129:742-6.
33 Demling RH. Role of prostaglandins in acute pulmonarymicrovascular injury. Ann NY Acad Sci 1982;384:517-34.
34 Voelkel NF, Stenmark KR, Reeves JT, Mathias MM,Murphy RC. Actions of lipoxygenase metabolites inisolated rat lungs. J Appl Physiol 1984;57:860-7.
35 Till GO, Ward PA. Complement-induced lung injury. In:Said SI, ed. The pulmonary circulation and acute lunginjury. Mount Kisco, New York: Futura, 1985:387-402.
36 Hammerschmidt DE, Hudson LD, Weaver LJ, CraddockPR, Jacobs HS. Association of complement activation andelevated plasma C5a with ARDS: patho physiologicalrelevance and possible prognostic value. Lancet 1980;i:947-9.
37 Duchateau J, Haas M, Schreyen H. Complement activationin patients at risk of developing ARDS. Am Rev Respir Dis1984;130: 1958-64.
38 Schumer W. Steroids in the treatment of clinical septicshock. Ann Surg 1976;184:333-41.
39 Bernard GR, Luce JM, Sprung CL, et al. High dosecorticosteroids in patients with the adult respiratorydistress syndrome. N Engl J Med 1987;317:1565-70.
40 Bone RC, Fisher CJ, Clemmer TP, et al. A controlledclinical trial of high dose methylprednisolone in thetreatment of severe sepsis and septic shock. N Engl J Med1987;317:653-8.
41 Braude S, MacNaughton P, Hughes D, Haslam P, EvansTW. Chronic adult respiratory distress syndrome-a rolefor steroids. Crit Care Med (in press).
42 Greenman RL, Schein RMH, Martin MA, Wenzel RP,Maclntyre NR, Emmanuel G. A controlled clinical trial ofE5 murine monoclonal IgM antibody to endotoxin in thetreatment of Gram negative sepsis. JAMA 1991;266:1097-102.
43 Ziegler EJ, Fisher CJ, Sprung CL, Straube RC, Sadoff JC,Foulke GE. Treatment of Gram negative bacteraemiawith HA- IA human monoclonal antibody againstendotoxin. N Engl J Med 1991;324:429-36.
44 Dinarello CA. Strategies for anti-Il-I therapies. Int JImmunopathol Pharmacol 1989;2:203-1 1.
45 Streiter RA, Remick PA, Ward PA. Cellular and molecularregulation ofTNF by pentoxifylline. Biochem Biophys ResCommun 1988;155:1230-6.
46 Endres S, Ghorbani R, Kelley VE. The effects of dietarysupplementation with n-3 polyunsaturated fatty acids onthe synthesis of Il-1 and TNF by mononuclear cells.N Engl JMed 1989;320:265-71.
47 Jansen JH, Fibbe WE, Willemze R, Kluin-Nelemans JC.11-4: a regulatory protein. Blut 1990;60:269-74.
48 Exley AR, Cohen J, Buurman W, Owen R, Hanson G,Lumley J. Monoclonal antibody to TNF in severe septicshock. Lancet 1990;335:1275-6. (
49 Bysani G, Shenep JL, Hildner WK, Stidham GL, RobersonPK. Detoxification of plasma containing lipopolysac-charide by adsorption. Crit Care Med 1990;18:67-71.
50 MacIntyre KW, DeLorezo W, Unovsky J. In vivo effects of /an anti-Il-I receptor antibody. Cytokine 1989;1:150.
51 van der Meer JWM. The effects of recombinant Il-1 andTNF on non-specific resistance to infection. Biotherapy1988;1:19-25.
52 Leeper-Woodford SK, Carey PD, Byrne K, Fisher BJ,Blocher C, Sugerman HJ, et al. Ibuprofen attenuatesplasma TNF activity during sepsis-induced acute lunginjury. J ApplPhysiol 1991;71:915-23.
53 Bihari DJ, Tinker J. The therapeutic value of vasodilatorprostaglandins in MOF associated with sepsis. Int CareMed 1988;15:2-7. f
54 WolfHRD, Seeger HW. Experimental and clinical results inshock lung treatment with vitamin E. Ann NY Acad Sci1982;393:392-409.
55 Polla BS. A role for heat shock proteins in inflammation. iImmunology Today 1988;9:134-5.
56 Storck M, Hartl WH, Zimmerer E, Inthorn D. Comparisonof pump driven and spontaneous continuous haemofiltra-tion in postoperative acute renal failure. Lancet 1991;337:452-5.
57 Beutler B, Milsark IW, Cerami A. Passive immunisationagainst cachectin/TNF protects mice from the lethaleffects of endotoxin. Science 1985;229:869-71.
58 Tracey KJ, Fong Y, Hesse DG, Manogue KR, Lee AT, KuoGC. Anti-cachectin/TNF monoclonal antibodies preventseptic shock during lethal bacteraemia. Nature 1987;330:662-4.
59 Hinshaw L, Olson P, Kuo G. Efficacy ofpost-treatment withanti-TNF monoclonal antibody in preventing the patho-physiology and lethality of sepsis in the baboon. CircShock 1989;27:362-4.
60 Hammond B, Fairman RP, Monroe P. The pulmonaryhypertension of sclerosing agents is prevented by cyclo-oxygenase inhibitors. Am J Med Sci 1985;290:98-101.
61 Palder SB, Huval W, Leicuk S. Reduction of polymorpho-nuclear leukocyte accumulations by inhibition of cyclo-oxygenase and thromboxane synthase in the rabbit.Surgery 1986;99:72-80.
62 Maderazo EG, Breaux SP, Woronick CL. Inhibition ofhuman polymorphonuclear leukocyte cell response byibuprofen. J Pharmacol Sci 1984;73:1403-6.
63 Metz C, Sibbald WJ. Anti-inflammatory therapy for acutelung injury. A review of animal and clinical studies. Chest199 1;100: 1 110-9.
64 Holdcroft JW, Vassar MJ, Weber CJ. Prostaglandin E1 andsurvival in patients with adult respiratory distress syn-drome. Ann Surg 1986;203:371-8.
65 Bone RC, Slotman G, Muander R, et al. Randomizeddouble-blind, multicentre study of prostaglandin E, inpatients with the adult respiratory distress syndrome.Chest 1989;96:114-9.
66 Leeman M, Beoynaems J-M, Degaute J-P, et al. Adminis-tration of dazoxiben, a selective thromboxane synthaseinhibitor, in the adult respiratory distress syndrome. Chest1985;87:726-30.
67 Slotman GJ, D'Arezzo A, Gann DS. Ketoconazole preventsacute respiratory failure in critically ill surgical patients.J Trauma 1988;28:648-54.
68 Van Asbeck BS, Hoidal J, Vercelloti GM, et al. Protectionagainst lethal hyperoxia by tracheal insufflation of ery-throcytes: role of red cell glutathione. Science 1985;227:756-9.
69 Richard C, Lemonnier F, Thibault M, et al. Vitamin Edeficiency and lipoperoxidation during adult respiratorydistress syndrome. Crit Care Med 1991;18:4-9.
70 Bast A, Haenen GRM, Doeleman CJA. Oxidants andantioxidants: state of the art. Am J Med 1991 ;suppl 3C:2-13S.
71 Fox R. Prevention of granulocyte-mediated oxidant lunginjury in rats by a hydroxyl radicle scavenger, dimethyl-thiourea. J Clin Invest 1984;4:1456-60.
72 Sullivan GW, Carpenter HT, Novick WJ, Mandell GL.Inhibition of the inflammatory action interleukin-1 andtumour necrosis factor (alpha) on neutrophil function bypentoxifylline. Infect Immunol 1988;56:1722-9.
73 Bessler H, Gilgal R, Djaldetti M, et al. Effect of pentoxy-fylline on the phagocytic activity, C-AMP levels andsuperoxide anion production by monocytes and poly-morphonuclear. Journal of Leukocyte Biology 1988;40:747-50.
74 Welsh CH, Lien D, Worthon GS, et al. Pentoxifyllinedecreases endotoxin-induced pulmonary neutrophilsequestration and extravascular protein accumulation inthe dog. Am Rev Respir Dis 1988;138:1106-14.
75 Coccia MT, Waxman K, Soliman MH. Pentoxifyllineimproves survival following hemorragic shock. Crit CareMed 1989;17:36-41.
76 Hallman M, Spragg R, Harrell JH, et al. Evidence of lungsurfactant abnormality in respiratory failure. J Clin Invest1982;70:673-83.
77 Merrit TA, Hallman M, Bloom BT, et al. Prophylactictreatment of very premature infants with human surfac-tant. N Engl JMed 1986;315:785-90.
78 Lachman B. Animal models and clinical pilot studies ofsurfactant replacement in adult respiratory distress syn-
dro\drome. Eur Respir J 1989;2(suppl 3):98-103.79- es DD, Cellek S, Palmer RMJ, Moncada S. Dexametha-
sone prevents the induction by endotoxin of nitric oxidesynthase and the associated effects on vascular tone. Aninsight into endotoxic shock. Biochem Biophys ResCommun 1990;173:541-7.
80 Ptros A, Bennett A, Vallance P. Effect of nitric oxide< synthase inhibitors on hypotension in patients with septic-> shock. Lancet 1991;338:1557-8.81 tiu SF, Crawley DE, Barnes PJ, Evans TW. Endothelium'-- derived relaxing factor inhibits hypoxic pulmonary
vasoconstriction in rats. Am Rev Respir Dis 1991;143:32-7.
8\iu SF, Dewar A, Crawley DE, Barnes PJ, Evans TW. Effectof tumour necrosis factor on hypoxic pulmonary vaso-
/-N constriction. J Appl Physiol 1992;72:1044-9.83 rostell C, Fratacci M-D, Wain JC, Jones R, Zapol WM.- Inhaled nitric oxide-a selective pulmonary vaso-
dilator reversing hypoxic pulmonary vasoconstriction.Circulation 1991;83:2038-47.
84 P pke-Zaba J, Higgenbottam TW, Dinh-Xuan AT, StoneD, Wallwork J. Inhaled nitric oxide as a cause of selectivepulmonary vasodilation in pulmonary hypertension.Lancet 1991;338:1173-4.
85 Hinds CJ. Monoclonal antibodies in sepsis and septic shock.BMJ 1992;304:132-3.
656
t
on May 4, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.47.8.651 on 1 A
ugust 1992. Dow
nloaded from