Embed Size (px)
Citation preview

THERAPEUTIC REVIEW
584 C J Clin Pharmacol 1992;32:584-596
Pharmacodynamics, Clinical Indications,and Adverse Effects of Heparin
Michael D. Freedman, MD, FCP
Heparins are a heterogenous group of naturally occurring glycosaminoglycans charac-terized by anticoagulant activity and a wide range of molecular weights (low molecularweight or fractionated heparins evolving within the past two decades). Cofactors for en-dogenous inhibitors of coagulation (antithrombin III and heparin cofactor II), heparinadministration results in a hypocoagulable state. Various platelet activities, includinginhibition of activity induced by platelet-derived growth factors on vascular smooth mus-cle, also have been noted. Divorced of anticoagulant nature, novel applications mayinclude a role in atherosclerosis prevention, acceleration of collateral coronary as well asperipheral circulation (i.e., angiogenesis), and continued (chronic) post-myocardial in-
farction therapy. Established indications include treatment of various thrombotic dis-eases, unstable angina, and thrombosis chemoprophylaxis in medical/surgical patients.
The antithrombotic potential of the heparins is used also in thrombosis management
related to extracorporeal circulatory assistance or dialysis devices. Heparin’s therapeuticpotential in the postphlebitic syndrome as well as in acute treatment of myocardial in-
farction (primarily and adjunctively with various thrombolytic agents) continues to un-
dergo evaluation; however, early data review shows favorable trends for its inclusion insituations that favor thrombus generation (e.g., anterior myocardial infarction).
Although associated with thrombocytopenia or hypertransaminasemia, the heparinsare relatively well tolerated. In a small subset of patients, a severe thrombocytopenia mayensue, which generally resolves on medication withdrawal. As this class of glycosamino-
glycans becomes better characterized, new indications may emerge for both native andthe newer fractionated heparins.
D iscovered and purified by J. McLean in 1917, hep-arm was originally distinguished by its ability to
inhibit canine blood from clotting for 24 hours (at0#{176}C).1’2In 1918, Howell and Holt3 described the anti-coagulating moiety (molecule) in more detail and,because of its abundance in the liver, labeled it hepa-nfl. Heparin preparations obtained from either por-cine or beef sources have been used clinically formore than half a century for prevention and treat-ment of thrombo-occiusive and embolic disease.7Development of several new modalities of venousthrombosis chemoprophylaxis (including “low mo-lecular weight heparins” [LMWHs] and “low-dose”native heparins both with and without dihydroergo-tamine), coincident with a renewed interest in pre-vention of venous thrombosis in high-risk surgicaland medical populations,#{176} have reawakened inter-est in these molecules.
From the Department of Medicine, New York Medical College, Valhalla,New York. Address for reprints: Michael D. Freedman, MD, FCP, Deb
bie Lane, Cross River, NY 10518.
In addition to their role as anticoagulants, non-an-ticoagulant actions of the heparin glycosaminogly-cans (GAGs) include regulation of angiogenesis,’1lipoprotein lipase modulation (plasma clearing ef-fect),12’13 maintenance of endothelial wall compe-tence, and inhibition of vascular smooth muscle pro-liferation (antiproliferative effect) after endothelialinjury.14”5 With special reference to this last prop-erty, and of particular public health interest, hasbeen an association frequently made between hepa-nfl administration and a beneficial effect on the evo-lution of atherosclerosis.8
CHEMISTRY OF THE HEPARINGLYCOSAMINOGLYCANS
The ubiquitous metachromatically staining mast cellhas long been recognized as one source of endoge-nous heparin’9 (along with varying but lesseramounts of heparin sulfate, dermatan sulfate, andchondroitin sulfate, other highly sulfated GAGs).

PREXALUKREINTISSUE FACTOR
HEFARIN-Alill
XII -XIIA
XI ‘CIA 4VlIAIX - PIXA
CA..CA++ , iiia -S
PLATELET
XA . PT
I
cFISRINOGEB( FRIN M THROMBINHEPARIN-I4C II
ii,W,SCUI.AR ENOOTHELIUM “.
‘.IcuLA OQT4 NUSCIC
/\
NHR’
#{149}-H OR -803-
R’ #{149}OOCH3 OR 503-
ARROWS INDICATE BINDING SITES
H2c05’
0803-
4
5/
HEPARIN, PHARMACODYNAMICS, CLINICAL INDICATIONS
THERAPEUTIC REVIEW 585
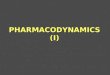
Tissues rich in mast cells (e.g., lung, intestine) be-come those from which commercial hepanin is ex-tracted. Hepanin also may be found in other hema-topoietically derived cells, such as basophils (wherethe principal GAGs are dermatan or chondroitin sul-fate).20 Hepanin GAGs also are produced in lesserquantity by various other cell lines, including vascu-lar endothelium. Characterized by elongated poly-sulfated GAG polymers (formerly referred to asmucopolysacchanides), these lengthy molecules areconspicuous in terms of alternating sulfoaminoglu-cosamine and uronic acid units (glucunonic or idur-onic), the occurrence of small amounts of N-acetyl-glucosamine (or unsubstituted glucosamine), and thepresence (in varying quantities) of a unique penta-sacchanide sequence found to be necessary for anti-thrombin III (ATIII) binding (Figure 1).
With a mean molecular weight of about 15,000 Da(range, 1,800-30,000 Da), hepanins are remarkablyheterogenous in both size and structure.21’22 Only aportion of the hepanin used clinically has high ATIIIaffinity, thus exhibiting very high anticoagulant ac-tivity. These high ATIII affinity-high anticoagulantactivity molecules are characterized by a molecularweight of 1800 to 5500 Da23’24 and constitute less than5% of native heparin (by mass). Referred to as “lowmolecular weight polymers” or “fractions,” theymay be obtained by separation from the larger mole-cules by gel filtration or ATIII affinity column chro-matography. Both methods effectively “filter” or“screen out” higher molecular weight molecules.More efficient methods of LMWH production in-volve modification of the entire molecular weightspectra of the native molecules by various chemicalor enzymatic agents.25
Figure 1. AT-Ill binding pentasacchonide.
Figure 2. Heparin actions.
Impurities found in chemically or enzymaticallymodified hepanin preparations, include dermatansulfate,26’27 which is of course capable itself of (effec-tive) antithrombotic activity,28 although possibly be-ing less hemorrhagic than equally antithromboticdoses of hepanin.29’3#{176} Ethylenediaminetetra-aceticacid also has been found in some heparin and LMWHformulations,31 although to a much lesser degree,and is additionally capable of perturbing hemostasis.Finally, the presence of nitrosamines (potent carcin-ogens) remains more than a theoretical possibility insome low molecular weight fractions.
PHARMACOLOGY AND PHARMACODYNAMICS
Heparin interacts with plasma serine protease inhibi-tors ATIII and heparin cof actor II (or dermatan cofac-ton). Binding to aminolysyl residues in ATIII, heparinis believed to cause a conformational change in thisenzyme, resulting in a multi-fold increase in its in-hibitory effects. Once formed, the hepanin-ATIII-serine protease complex rapidly disassociates into aninactive ATIII-serine protease complex, and the hep-arm molecule itself, which then will bind anotherATIII complex. Inhibition of activated coagulationfactors IX, X, XI, XII, and Kallikrein by the hepanin-ATIII complex has been reported (Figure 2).3233 Thehepanin-HC II complex, however, appears to reactonly to inhibit formation of thrombin.34
Heparins also have been reported to have high af-finity to platelet factor 4, effectively competing withATIII for heparin binding.35 To the extent that mostof the hepanins can cause inhibition of platelet aggre-gation to some degree, as well as inhibition of theeffects of platelet-derived growth factors on vascularsmooth muscle, these agents are properly considered“platelet active anticoagulants.”3’8 Finally, the hep-

ASNO ALITIES OF 51.000 yE ELS
MAJOC SURSERY
“Au-A
PREVIOUS TIISOIISOHMSOLISM
NEPIIROTIC SYNDROMe
ARTIFICIAL SUEMCES
ALTERm, N IN CONSTITUENTS OF eLoo ASEARA! ION OF SLOOP LOW
nypeav,aooar,y SaTES PAERPERIUM
MALISNASCY OBESITY
ESTIIOSEN THeRAPY PROLOSSER SERPENT
NYPERCOASULASLE SaTE PROLOSSED IMMOPILIZATION
E,ASETES MRLLIYUS CONJESTIVE HEART RCLURI
* Endogenous or native are used synonymously in this article to
describe nonfractionated heparins.
FREEDMAN
586 C J Clin Pharmacol 1992;32:584-596
arms specifically bind to vascular endothelium,39causing the release of at least two distinct GAGs(chondroitin sulfate being one) while altering the per-meability of the vessel wall.40’41
Prolonged heparin administration has been asso-ciated with development of osteopenia. Interest-ingly, this property appears to have a molecularweight dependence, because LMWHs have beenshown to be less “osteopenic” than endogenous* hep-arms.42 This “calcium-sparing” feature may be ofsome consequence in the patient requiring long-term administration of this type of anticoagulant(e.g., pregnancy, cardiac valve replacement, chronicvenous thrombosis prophylaxis, etc.).43 The exactnature of heparin-induced bone loss has not as yetbeen adequately elucidated.
Heparin pharmacokinetics have largely been de-termined using surrogate or biologic markers of activ-ity. Most widely used has been the activated partialthromboplastin time (APTT), whole blood clottingtime, or activated clotting time.45 Novel methods in-clude determination of anti-factor Xa using eitherclotting or amidiolytic assays. Experimental meth-ods include ATIII labeling and radiolabeled heparin.Because large interpatient variability to the effects ofheparin has been noted, individualized therapy toattain a given endpoint, generally a particular APTT,is often undertaken. Systemic absorption of nativehepanins is negligible after oral or nasal administra-tion and present but erratic after aerosolized inhala-tion.46 Therefore, hepanins have generally been ad-ministered subcutaneously or intravenously. Theydo not cross the placental barrier and hence are thedrugs of choice for pregnant patients requiring anti-coagulation.479
After single injection of (unfractionated) nativehepanin, half-life (t1/2) is dose dependent, the volumeof distribution remaining constant with decreasingtotal Cl as dose is increased. At any particular dose, itappears that the LMWHs have a more lengthy half-life (t#{189} 2 - 3 X native heparin) than their parentmolecules. Elimination kinetics (determined byanti-factor Xa or APTT determinations) appear to beprincipally mediated by a nonsaturable mecha-nisms. Concordant with this, elimination half-life isincreased in patients with kidney disease,50’51strongly suggestive of a major renal component toclearance.
CLINICAL APPLICATIONS
Clinical applications of the hepanins can be dividedinto those that are primarily related to anticoagulant
activity and those secondary to nonanticoagulant ac-tivity as well. The latter category probably repre-sents the majority of applications.
Venous Thrombosis Prophylaxis
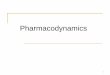
Factors predisposing to the development of venousthrombosis include disorders associated with orleading to venous stasis, hypercoagulability, or ve-nous trauma (Figure 3).5253 Although the majority ofvenous thrombosis prevention trials have beencarried out in the postorthopedic or abdominal sur-gery patient population (a commonly encounteredhigh-risk group), there are several studies involvingother high-risk groups, e.g., postneurosurgery, post-cranial trauma, post major trauma, thermal burn,congestive heart failure, acute myocardial infarction(MI; considered separately, see below), and othermedically related conditions requiring prolonged im-mobility.
The rate of deep venous thrombosis (DVT) forma-tion after general surgical procedures may be as highas 28%, whereas the rate after open prostatectomy orhip fracture is as high as 5Q%54.55 Consequently,rates of fatal pulmonary embolism in this patient pop-ulation may be as great as 2%.56 When comparedwith placebo or physical methods alone, a prepon-derance of data has demonstrated superiority of hep-arm (either low dose or “full dose”)5762 (Table I) forvenous thrombosis prophylaxis. Several meta-analy-ses using the results of well over 100 studies have6365suggested the same.
Augmentation with dihydroergotamine (DHE) (apotent vasoconstrictor) has recently undergone clin-ical evaluation. A meta-analysis examining results
Figure 3. Predisposing factors for thrombosis development.

HEPARIN, PHARMACODYNAMICS, CLINICAL INDICATIONS
THERAPEUTIC REVIEW 587
TABLE I
Prevention of Thrombosis in Medical/Surgical Patients: Selected Studies
DVI Results’Patient
Number Minor Major Hemorrhage2Reference Indication Study Group (n) (%) (%) (%)
Rosenberg s/p Major Randomized Heparin 50001U q8hr X 18 (55) 7.3 0 7et al. surgery Prospective Leg stim.3 (50) 24
Prospective Control (89) 23.6 20.25Nicolaides s/p Emergency Randomized Ml with heparin4 (18) 5.5 0
et al. admission to Prospective Ml without heparin (13) 38 0ROMI NoMI (20) 20 0
Gordon-Smith s/p Major Randomized Controls (50) 42 0et al. surgery Prospective Heparin 5000IU ql2hr X 3 (52) 13.5k 0
Heparin 50001U ql2hr X 10 (48) 8.3** 0Belch et al. CHF/COPD Randomized Controls (50) 26 0
Medical Prospective Heparin 50001U q8hr (50) 4* 0patients
Kakkar et al. s/p Major Randomized Heparin 50001U SCsurgery Double 2hr prior to surgery (39) 8*** NI
blinded then; 50001U ql2hr X 7dControl (placebo) (39) 42 NI
Handley A. s/p Admission Prospective Heparin 50001U IV, then; (26) 23 0to ROMI Randomized 75001U ql2hr X 7d
Control (24) 29 0
#{149}P < 0.003 compared with controls, crease in Hg requiring transfusion.* * P <0.01 compared with controls. Electrical leg muscle stimulation.* * P < 0.001 compared with controls. Continuous infusion of heparin. 1O,000IU q6hr x 36 hours, then oral antico
‘OW characterized as major or minor if trial indicates, otherwise considered agulat Ion.major. NI not indicated.
2 Major hemorrhagic risk characterized as blood loss causing significant de-
from 17 different studies66 demonstrated that 5000
LU twice daily of heparin plus 0.5 mg DHE may besuperior to low-dose heparin alone.67’#{176}
Effectiveness of several LMWHs for the preventionof thromboocclusive events when administered ineither a daily or twice daily subcutaneous fashion tohigh-risk medical672 and surgical73-77 populationsalso has been investigated. Table LI summarizes sev-eral major studies, most of which have demonstrateda relative superiority of LMWHs compared with na-tive heparins when used for the prophylaxis of deepvenous thrombosis after major surgery.
Despite a demonstrated utility in preventingthromboembolic disease, heparins unfortunatelystill remain very much underused for this indica-tion.78
Treatment of Established Thrombosis
Long employed as acute therapy for both DVT andpulmonary embolus, recent studies have confirmedheparin’s role in the treatment of thrombosis.79’80 Be-
cause of the prompt anticoagulant action of heparinafter parenteral administration, heparin has histori-cally been the preferred method of anticoagulationwhen rapidly required. This is often the case in acutetreatment of thrombosis, to prevent both extensionand thromboembolism (pulmonary embolism) whilepromoting dissolution of the thrombus itself,through promotion of endogenous recanalization(tPA activation).81 As noted above, the many studiesconducted in which heparin has been used clearlyindicate a decreased frequency of thromboembolismduring anticoagulation.
A study of proximal venous thrombosis therapycomparing acute heparinization followed by oral an-ticoagulant therapy with acute heparinization fol-lowed by continuing heparin therapy has shown afavorable tendency for resolution in the latter.82 Be-cause the serious hemorrhagic risks associated withheparin therapy of venous thrombosis may be ashigh as 18 to 22%, therapy of established thrombo-sis has been studied using both shorter periods ofparenteral therapy (before starting oral therapy with

FREEDMAN
588 #{149}J Clin Pharmacol 1992;32:584-596
TABLE II
Prevention of Thrombosis in Medical/Surgical Patients by LMWHs-Selected Studies
Reference IndicationStudyDesign Group Number
Results(%)
HemorrhageIncidence
Samama DVT prophylaxis Prospective PK10169 60mg qd (137) 2.9 4/137et al. s/p Major surgery Double-blind Heparin 50001U lID
PKlOl694OmgqdHeparin 50001U lIDPK1O1692OmgTIDHeparin 50001U lID
(133)(106)(110)(159)(158)
3.82.82.73.87.6
3/1332/1062/1101/1594/158
Kakkar et al. DVT prophylaxiss/p Surgery
ProspectiveRandomized
CY216 7500AXa qdHeparin, 5000IU BID
(196)(199)
2.5*7.5
10/1967/199
Turpie et al. DVT prophylaxiss/p Orthopedic surgery
ProspectiveDouble-blinded
PK10169 30mg qdPlacebo
(50)(50)
12**42
1/502/50
Enke et at. DVT prophylaxiss/p Major surgery
ProspectiveRandomized
CY 216 7500 AXa qdHeparin 5000IU TID
(960)(936)
2.8***4.5
47/960142/936
Berqgquis DVT prophylaxis Prospective Kabi 2165 5000 AXa qd (215) 6.4 25/215et at. s/p Major surgery Double blinded Heparin 50001U TID (217) 4.3 10/217
Dahan et al. DVI prophylaxisMedical high risk
ProspectiveDouble blind,
placebo controlled
PK 10169 60 mgPlacebo
(132)(131)
3#9
1/1322/131
Harenberg DVI prophylaxis Prospective Sandoz LMWH 1500 APTT (100) 3 0et al.
Turpie et at.
Medical high riskrandomized
DVI prophylaxisMedical high-risk
prospective
Double blinded
Double blindedRandomized
U qdx lOdHeparin 50001U lID X lOdOrg 10172 7500 AXa BIDPlacebo
(100)(50)(25)
44.0##
42
2/1002/502/50
Green et al. DVI prophylaxisCranial trauma
ProspectiveDouble blinded
Logiparin 3500 AXa qdHeparin 50001U liD
(20)(20)
0###25
00
P<0.05. ##P<0.005.“ P < 0.0007. ### P < 0.006.* * * P <0.034. ‘Increased post operative bloo d loss.# P = 0.03.
coumadin),TM differing regimens of constant infusionversus intermittent heparin administration,85 and oflate, with several LMWHs. Here, results do not seemto be overwhelmingly in favor of the LMWHs, but arenonetheless marginally favorable89 (Table III). In-termittent versus constant infusion administration isdealt with in the Adverse Drug Reactions section.9#{176}
Heparin’s therapeutic potential in the post-phie-bitic syndrome also has been investigated. Risk fac-tors that would enable high-risk patients to be fol-lowed before the syndrome manifesting itself arepoorly understood.91 Post-phlebitic disease affects upto 30% of those treated curatively for DVT, and is amajor cause of continued disability. Although sev-eral studies indicate more rapid thrombolysis (dur-ing the acute phiebitic state) with thrombolyticagents to be preventative, it is clear that the hemor-rhagic risks are also increased (by as much as 30%92).
Although the location of thrombus formation hasgenerally been limited to the deep venous systems of
the lower extremities (peripherally) or the pulmo-nary circulation (centrally), thrombosis therapy withheparin is not anatomically limited. In recent studiesof sinus cavernosis thrombosis93 and mural thrombo-sis after MI (see below), the efficacy of intravenousheparin has been demonstrated.
Role of Heparin After Myocardial Infraction
Heparins alone or in conjunction with oral anticoagu-lants have been studied after acute MI in efforts toprevent thrombus formation (intraventricularthrombus as well as DVT), prevent extension of rein-farction, and decrease long-term morbidity events.In an early study of the effects of heparin in 81 postin-farction patients, Marks et alY4 demonstrated a sta-tistically significant difference in the rate of DVT inheparin-treated patients. In another study of 52 pa-tients admitted to the hospital with a tentative diag-nosis of acute MI, Nicolaides et al.55 found that inten-

Hull et al.
Hull et al.
Wilson et al.
Reference Study Group Patients (n) Results (%)
5.2
g2
2503
28
Bratt et al. Randomized
Duroux et al. Randomized
(14)
(26)
(33)
(28)
(12)
(13)
(29)
(85)
(81)
One patient with PE, two patients with OW.2 Five patients with PE, six patients with OW.
Eight patients with OW, one patient with PE.Results of venographies.
HEPARIN, PHARMACODYNAMICS, CLINICAL INDICATIONS
THERAPEUTIC REVIEW 589
RandomizedDouble blindedRandomized
BlindedRandomized
Kakkar et al. RandomizedBlinded
TABLE Ill
Treatment of Thrombosis (Selected Studies)
Heparin IVHeparin SCHeparin SCWarfarinHeparin-adjusted dose (APPT)
intermittant administrationHeparin-adjusted dose (APTT)
constant infusionHeparin-standard dose
heparin 360 lU/kg/24 hrintermittant administration
Heparin-standard doseheparin 360 IU/g/24 hrconstant administration
Heparin-standard doseheparin 600 IU/kg/24 hrintermittant (100 lU/kgq4hr X 6
Inteimittant (150 IU q4hr X 4)250 AXa AXaICU/kg BID X 6d
Heparin 500 IU UH/kg/24 hrIV X 6 d
250 IU UH/kg/12 hr SC x 6days
240 U/kg/12 hr Kabi 2165 X10 days
120 U/kg/12 hr Kabi 2165 X10 days
5000 heparin lID AP1Tadjusted x 10 days
225 AXa ICU/kg CY216 BIDSC X 10 days
UH IV APTT adjusted x 10days
(58)(57)(35)(33)(29)
(36)
(12) 17
(16) 25
(7) 14
015 no change49 worsen77 improve31 no change26 worsen43 improve26 no change74 improve50 no change50 improve23 no change77 improve41 no change11 worsen48 improve20 no change6 worsen74 improve31 no change7 worsen62 improve
sive treatment with heparin for 3 days, followed byoral anticoagulation, reduced the incidence of DVT(and presumably morbidity).
Thromboembolic disease has been associated withintracardiac mural thrombus formation after MI,95infarct location being a prime determinant for likeli-hood of thrombus development (30-40% of patientswith anterior transmural infarcts developing left yen-
tricular thrombosis). Although one study suggestedthat full heparinization did not affect thrombus gen-eration,97 most investigations have demonstratedthat adequate heparinization (or coumadinization)has a salutatory role in decreasing the rate of muralthrombus formation after anterior infarctionY10#{176} Ina recent study of 221 patients status post anteriorwall MI, mural thrombus incidence was reduced

FREEDMAN
590 #{149}J Clin Pharmacol 1992;32:584-596
from 32% in a group administered 5000 IU heparinsubcutaneously twice daily to 11% in a group ad-ministered 12,500 IU heparin subcutaneously twicedaily,’#{176}’suggesting a dose response of mural throm-bus formation to heparin.
To ascertain risks and benefits of short-term hepa-rin therapy after MI, several large studies have beenundertaken. In the Medical Research Council102trial, a total of 1427 patients were enrolled within 3days of MI. Patients were randomly assigned to re-ceive either 36 hours of heparin plus oral phenin-dione (in a dose necessary to elevate the thrombotestlevels by 10-20%) or no heparin and an insignificantamount of phenindione. In a VA CooperativeTrial,103 999 men were enrolled after acute MI. Afterrandomization, patients were assigned to either ananticoagulated group (adjusted dose heparin withconcurrently adjusted warfarin) for 28 days or, alter-natively, placebo-matched injections. In these twolarge studies, overall rate of mortality, as well as DVTand secondary MI, was not different between groups
(Table IV). Both of these studies are of course compli-cated by the relatively prolonged oral anticoagulantdosing in addition to the heparin administration. Afurther role for heparin in the acute MI period iscurrently under investigation with concomitantthrombolytic use in the ISIS-3 and GISSI-2 studies(see following section).
Finally, long-term heparin administration to post-MI patients may reduce total morbidity and mortal-ity rates.18”#{176}4In a recent multicenter study, 728 pa-tients with MI during the preceding 6- to 18-monthperiod were randomized to receive either heparin orcontinue to receive their post-discharge medicationsalone (antiarythmics, etc.). The group to which hepa-nfl was added had a cumulative mortality rate 63%lower (P < .05). Fatal stroke, reinfarction, and pulmo-nary embolism were less frequent than in the controlgroup.105 Obvious difficulties involved in chronic ad-ministration are primarily those associated with themethod of administration (parenteral-subcutane-ous) and compliance. (n.b.: Studies of anticoagulants
TABLE IV
Heparins and Myocardlal Infarction (Selected Studies)
Reference Study Group Number Results
Nickolaides et al. Prevention of DVI Infarct confirmed, treatment 5.5% DVI rate’Pts s/p admission With 1O,000IU heparin q6hr X 6 infarct (18) 38% DVT rate3
to ROMI2 confirmed, controls (13)MRC Trial Prevention of Treated with heparin loading dose, then (712) Mortality = 16.2*
mortality for 10,000IU q6hr X 5 followed by oral Recurrent MI = 9,7*acute Ml Single anticoagulation anticoagulation X 28blinded dprospectively.
Randomized Control group, no heparin insufficient (715)oral anticoagulation to effectcoagulation
Mortality = 18%Recurrent Mi = 13%
VA Cooperative Trial Prevention of Treatment with heparin sc q8-l2hr to (500) Mortality =
mortality/ produce clotting time 2X normal then Recurrent MI = 4%*morbidity s/p oral anticoagulation X 28 dacute MIprospectively,
Randomized Control group, no anticoagulant Tx (499) Mortality = 11.2%Recurrent Ml = 6%
Neri Semen Late prevention of Treatment with heparin 12,5001U sc qd. (363) Mortality = 33%*.4reinfarction
Control group (365)
Cumulative CVevents = 33%*
Mortality = 6.3%Cumulative CV
events = 4.9%
Not significant. Includes two “seriously ill patients.”‘Includes one “seriously ill” patient.2 Rule out myocardial infarction.
Differences between cumulative mortality inP < 0.05.
the two groups is significant,

HEPARIN, PHARMACODYNAMICSI CLINICAL INDICATIONS
THERAPEUTIC REVIEW 591
and long-term survival/reinfarction have generallyinvolved oral anticoagulants without any use of hep-arm).
Adjunctive Therapy During/After Thrombolysisand Angioplasty
The role of heparin infusion during thrombolysis hasbeen under investigation since early studies usingthrombolytics. Several large studies are underway todetermine the role of heparin with thrombolysis inthe acute post-MI period.’06 The GISSI-2 (GruppoItaliano per lo Studio della Streptochinasi nell’ In-farto Miocardico) trial examines the effects of addingheparin to groups assigned to receive either tPA plusaspirin or streptokinase plus aspirin in the acutepost-MI period, and the ISIS-3 (International Study ofInfarct Survival) trial will examine the addition ofheparin to either streptokmnase, tPA, or APSAC.Pending these results, many investigators have rec-ommended the use of intravenous (systemic) hepa-rin to preclude thrombus formation around the cath-eter, prevent the propagation of existing thrombus,and (possibly) augment the fibrinolytic activity of thelytic agent.’#{176}7
In an early study comparing the effects of aspirin,either with or without heparin during percutaneoustransluminal coronary angioplasty, a greater rate ofacute thrombosis occurred using aspirin alone thanthe combination (7% versus 4.6%).b08 A large recentseries has reported that by prolonging the APTT to150 seconds using heparin, the rate of recurrent in-farction as well as ischemia was significantly low-ered from 10.7% to 2.6% and from 9.2% to 1.5% re-spectively.’#{176}9 Acute administration of either hepa-rin, or heparin with a thrombolytic agent, also hasbeen reported to aid in the resolution of percutane-ous transluminal coronary angioplasty-related in-traluminal thrombus.”#{176}
Treatment of Unstable Angina
Initially observed to have anti-anginal effects, hepa-rin administration during the acute phase of unsta-ble angina” has been demonstrated to decrease therisk of subsequent MI, and death.”25 Heparin ei-ther with or without aspirin (see Drug Interactions) isa drug of choice for acute exacerbations of unstableangina as well as for chronic therapy. Effects on plate-let function, depression of microthrombus forma-tion, inhibition of underlying vascular smooth mus-cle proliferation, and plaque stability are all proba-bly operative components of heparin’s actions.
Heparins and LMWHs in Hemodialysis and
Cardiopulmonary Bypass
Blood contact with various (synthetic) thrombogenicmaterials during use of extracorporeal circulationdevices and subsequent thrombus formation is theprincipal rationale for the concurrent administrationof heparin. Although anticoagulation is of necessityafter contact with either the dialysis membrane oroxygenator, the inability to completely neutralizethe administered anticoagulant may result in a se-vere hemorrhagic diathesis.’6”7 The concept of us-ing heparin-bonded membranes, in which heparin ischemically (or physically) affixed to the various ele-ments of the dialysis819 or cardiopulmonary by-pass unit,’2#{176}as well as limiting the heparin to thedevice by enzymatic removal in the effluent circuit,is under current development.
Promises that LMWHs might lead to fewer bleed-ing problems (perhaps referable to their decreasedantifactor Ila response compared with their antifac-tor Xa activity, their platelet activity, or their de-creased release of hepatic triglyceride lipase, aknown anticoagulant38) and therefore improved con-trol of hemostasis lead to other potential areas ofcurrent investigation. These include the use ofLMWHs for patients undergoing hemodialysis’2’3and cardiopulmonary bypass.124’6 Currently itwould not appear that LMWHs guarantee “resis-tance” from hemorrhage, however.
ADVERSE DRUG EXPERIENCE
Hemorrhage
Among therapeutic complications, the foremost isclearly hemorrhage. The possibility of both over-hemorrhage or concealed hemorrhage (e.g., retro-peritoneal,’27 intrathoracic) should always be in thedifferential diagnosis of new findings in the treatedpatient. Relationships between the risk of bleedingand the total amount administered per day, methodof administration, and intensity of monitoring ther-apy have been studied.128 Clearly, low-dosage regi-mens (e.g., venous thrombosis prophylaxis) are asso-ciated with less hemorrhage than are high-dose ther-apies (e.g., curative therapy of venous thrombosis).Intermittent intravenous administration (eitherAPTT adjusted or weight adjusted) has been asso-ciated with greater threat of hemorrhage than con-stant intravenous infusion.’29 Concurrently adminis-tered salicylates or sulfonylureas also have been as-sociated with increased bleeding (see DrugInteractions).
Monitoring therapy (e.g., with APTT) is only use-

FREEDMAN
592 #{149}J Clin Pharmacol 1992;32:584-596
ful if the information obtained correlates with thehemorrhagic risk. Because the risk of hemorrhage isnot only dependent on inhibition of coagulation fac-tors (also platelets, vascular integrity), the practicaluse of such monitoring when relatively low doses ofheparin may be limited. Monitoring and adjustingtherapy still may be indicated, however, whenhigher doses of heparin are being used or in high-riskpatients. As more heparin is administered, variousclotting parameters (including the APTT) becomemore sensitive prognostic indicators of hemorrhage,and thus are routinely monitored.
Heparin-Induced Thrombocytopenia
Some degree of thrombocytopenia has beenvariously reported in from 5 to 30% of individualsreceiving heparin. This finding is more commonwith the use of bovine preparations than porcineones, and generally evolves slowly over several days(1-4) of therapy resolving spontaneously or uponcessation of heparin administration (Type I HIT).’3#{176}Amore severe and rapidly fulminant form of heparin-induced thrombocytopenia (Type II HIT) occurs in alesser number of patients, and is typically character-ized by a delayed onset (6-10 days). Resultant para-doxical thrombosis (“white clot syndrome”) has re-cently been reviewed.’3’ Probably an immune re-sponse to both secondary and tertiary structure ofthe heparins, it has been observed with all molecularweight fractions of heparin (although heparin-induced thrombocytopenia occurring with theLMWHs may not occur with the same frequency aswith native heparin).’32 Treatment of HIT occurringsecondary to a specific native heparin may be with alow molecular weight heparin after no cross-reactiv-ity has been shown in a bioassay.’33
Hypertransaminasemia
Elevations of serum glutamicoxaloacetic transami-nase/serum glutamic-pyruvic transaminase havebeen observed in as many as 93% of subjects receiv-ing heparin. The time course of the reaction tendsto imply a benign and generally acute process. Gener-ally, hypertransaminasemias appear to becomemaximal within the first 7 days of therapy, returningto normal thereafter. One study comparing anLMWH with unfractionated heparin showed eleva-tions associated with both treatments (hypertrans-aminasemia was greater, however, with unfraction-ated heparin than with LMWH fraction).’35”36
Osteoporosis
Heparin has been recognized to induce development
of a progressive osteoporotic state after long-term ad-ministration.41”37”38 Mechanisms suggested for thisreaction have not been totally elucidated; however,early theories of a decrease in prostaglandin E, doesnot appear to be responsible.’39 Also, as noted for-merly, the LMWHs appear to lack this property andmay be indicated in those patients at increased riskof fracture.
Cutaneous Reactions
Skin necrosis, previously observed with the unfrac-tionated heparins, also has been observed with theLMWHs.140”41 Although the extent of this reaction isvariable, several deaths have been linked to it. Theexact mechanism of dermal destruction has been lik-ened to toxic epidermal necrolysis. The precisecause of this reaction, like that of osteoporosis andhypertransaminasemia, remains unclear.
Drug Interactions
Physiologic interactions with other drugs, althoughnot common, merit recognition. Heparin has beenshown to cause a relative prohemhorrhagic ten-dency when coadministered with salicylates,’42”43particularly cephalosporin antibiotics (moxalac-tam).1” The mechanism of this is thought to be con-comitant platelet inhibition and clotting factor inhi-bition. Of particular note to patients being treated forunstable angina or in the acute post-MI period hasbeen the observation that the effects of heparin maybe inhibited by concurrent intravenous nitroglyc-erin infusion.145 Finally, case reports of reactionswith sulfonylurea hypoglycemic agents have beenmade. 146
PERSPECTIVES FOR FUTURE DEVELOPMENT
Although the heparins have been known to us foralmost 75 years, and used clinically for at least twothirds of that time, the last 20 years have clearly beenthe most exciting. Although complications of hepa-rin therapy have historically caused the clinician totemper its use, and today’s penchant for obviation ofmost risk has not allayed that concern, new indica-tions for heparin as well as better characterization ofadverse reactions are clearly causing a reassessment.
Besides their role as anticoagulants, new applica-tions for these clearly multifunctional glycosamino-glycans, divorced of their anticoagulant activity,may include a role in the prevention of atherosclero-sis, acceleration of collateral coronary as well as pe-ripheral circulation (facilitation of healing process;angiogenesis), and continued (chronic) post-MI ther-

HEPARIN, PHARMACODYNAMICS, CLINICAL INDICATIONS
THERAPEUTIC REVIEW 593
apy. Indications based primarily on anticoagulant ac-tivity (e.g., use in extracorporeal circulations or aspreventive agents against venous thrombosis) willcontinue to grow.
The author thanks Dr. Sigmund Lasker, New York Medical Col-
lege, for his helpful review of the manuscript.
REFERENCES
1. McLean J: The thromboplastic action of cephalin. Am JPhysiol1916; 41:250.
2. McLean J: The discovery of heparin. Circulation 1959;19:75.
3. Howell WH, Holt E: The purification of heparin and its chemi-cal and physiologic reactions. Am J Physiol 1918;47:328.
4. Murray DWG, Best CH: I Am Med Assoc 1938; 110:118-127.5. Jorpes JE: in Hepurin in The Treatment of Thrombosis. NewYork: Oxford University Press, 1946.
6. Wilson JE, Byman U, Parkey RW: Hepanin therapy in venousthromboembolism. Am J Med 1981;70:808-816.
7. Crafoord C: Heparin and post-operative thrombosis. Acta ChirScand 1939;82:487-498.
8. Frishman WH, Ribner H: Anticoagulation in myocardial in-farction: Modern approach to an old problem. Am J Cardiol1979; 43:1207-1213.
9. Consensus Conference NIH: Prevention of venous thrombosisand pulmonary embolism. JAMA 1986; 256:744-749,
10. Resnekov L, Chediak J, Hirsch J, Lewis D: Antithromboticagents in coronary artery disease. Chest 1986;89:54S-67S.
11. Folkman J, Ingber DE: Angiogenesis: Regulatory role of hepa-nfl and heparin related molecules, in Lane DL, Lindahl U (eds.):Heparin, Chemical and Biological Properties, Clinical Applica-tions. Boca Raton, Florida: CRC Press, 1989.
12. Nilsson-Ehle P. Garfinkel AS, Schotz MC: Lipolytic enzymesand plasma lipoprotein metabolism, Annu Rev Biochem1980; 49:667-693.
13. Robinson DS: The function of plasma triglycerides in fattyacid transport. Comp Biochem 1970; 18:51.
14. Guyton JR, Rosenberg RD. Clowes AW, Karnovsky MJ: Inhibi-tion of rat arterial smooth muscle cell proliferation by hepanin. I.In vivo studies with anticoagulant and non-anticoagulant hepa-nfl. Circ Res 1980;46:625-634,
15. Clowes AW, Karnovsky Mi: Suppression by heparin of smoothmuscle cell proliferation in injured arteries. Nature 1977; 265:625-626.
16. Rosenberg RD, Reilly C, Fritze L: Atherogenic regulation byheparin-like molecules. Ann N Y Acad Sci 1985;454:270-278.
17. Rosenberg RD, Fnitze LMS, Castellot Jj, Karnovsky MJ: 1-lepa-rin-like molecules as regulators of atherogenesis. Nouv Rev Fr He-matol 1984;26:255-260.
18. Engelberg H, Kuhn R, Steinman M: A controlled study of theeffect of intermittent heparin therapy on the course of humancoronary atherosclerosis. Circulation 1956;1 3:489-498.
19. Straus AH, Nader HB, Dietrich CP: Absence of heparin or hep-arm-like compounds in mast-cell-free tissues and animals. Bio-
chim BiophysActa 1982; 717:478-485.20. Enerback L: The mast cell system, in Lane D, Lindahl U (eds.):Hepanin, Chemical and Biological Properties, Clinical Applica-tions. Boca Raton, Florida: CRC Press, 1989;97-113.
21. Roden L: Highlights in the history of hepanin. in Lane D, Lin-dahl U (eds.): Heparin, Chemical and Biological Properties, Clini-cal Applications. Boca Raton, Florida: CRC Press, 1989; 8-23.
22. Choay j: Structure and activity of hepanin and its fragments:An overview. Semin Thromb Hemost 1989;15(4):359-364.
23. Holmer E, Kunachi K, Soderstnom C: The molecular weightdependence of the rate-enhancing effect of hepanin on the inhibi-tion of thrombin, Factor Xa, Factor IXa, Factor XIla and kallikreinby antithnombin. Biochem J 1981;395-400.
24. Hirsch J, Ofosu FA, Levine M: The development of low molec-ular weight heparins for clinical use, in Verstrate M, Vermylen J,Lijnen HR, Arnout J (eds.): Thrombosis and Hemostasis, Leuven:Leuven University Press, 1987;425-448.
25. Freedman MD: Low molecular weight hepanins: An emergingnew class of glycosaminoglycan antithrombotics. J Clin Pharm1991; 31:298-306.
26. Perlin AS, Holme KR: NMR Spectra of hepanin in admixturewith dermatan sulfate and other glycosaminoglycans. Ann N YAcad Sci 1989; 556:471-472.
27. Perlin AS, Sauna! F, Cooper B, Folkman J: Dermatan sulfatein pharmaceutical heparins. Thromb Haemost 1987; 58:792.
28. Ofosu FA, Modi GJ, Smith LM, Cerskus AL, Hirsch J, Blajch-man MA: Heparin sulfate and dermatan sulfate inhibit the genera-tion of thrombin activity in plasma by complementary pathways,Blood 1985; 64:742-747,
29. Sie P, Ofosu FA, Fernandez MR. Buchanan M, Petitou M,Boneu B: Respective role of antithnombin III and hepanin cofactorII in the in vitro anticoagulant effect of hepanin and various sul-phated polysacchanides. Br I Haematol 1986; 64:707-714.
30. Frederick A, Ofosu FA, Buchanan MR, Anvani N, Smith M,Blajchman MA: Plasma anticoagulant mechanisms of heparin,hepanin sulfate and dermatan sulfate. Ann N Y Acad Sci19891;556:123-131.
31. Pangrazzi J, Oreste P, Naggi AM, Torn C, Maggi A, Donati MB,Casu B: Bleeding effects associated with hepanin contaminants.Ann NY Acad Sci 1989; 556:468-470.
32. Faneed I, Walenga JM, Hoppensteadt D, Hwan X, Raccuelli A:Comparative study on the in vitro and in viva activities of sevenlow-molecular-weight hepanins. Haemostasis 1988; 18(S3):3-16.
33. Rosenberg RD: Actions and interactions of antithrombin andheparin. N Engl J Med. 1975; 292:146-149.
34. Pratt CW, Whinna HC, Meade JB, Treanor RE, Church FC:Physicochemical aspects of heparin cofactor II. Ann N Y Acad Sci1989; 556:104-115.
35. Waltz DA, Hung G: In vivo studies of the binding of hepaninand its fractions to platelet factor 4. Semin Thromb Hemost1985; 11:40-47.
36. Messmore HL, Gniffon B, Fareed j, Coyne E, Seghatchian J: Invitro studies of the interactions of hepanin, low molecular weighthepanmn and the hepaninoids with platelets. Ann N Y Acad Sci
1989; 556:217-232.
37. Ellison N, Edmunds H, Colman RW: Platelet aggregation fol-lowing hepanin and pnotamine administration Anesthesiology1978; 18:65-68.
38. Heinnich D. Gong T. Schulz M: Effects of unfractionated andfractionated heparin on platelet function. Haemostasis 1988;18(suppl 3):48-54.
39. Banzu T, Van Run JML, Petituou M, Molho P. Tobelem C,Caen JP: Endothelial binding sites for hepanin, specificity and rolein hepanin neutralization. Biochem 1 1986; 238:847-854.
40. Blajchman MA, Young E, Ofosu FA: Effects of unfractionated

FREEDMAN
594 S J Clin Pharmacol 1992;32:584-596
hepanin, dermatan sulfate and low molecular weight hepanin onvessel wall permeability. Ann N Y Acad Sci 1989; 556:245-254,
41. Kraemer PM: Hepanin releases hepanin sulfate from the cellsurface. Biochem Biophys Res Commun 1977; 78:1334-1340.
42. Rupp wM, McCarthy HB, Rohde TD, Blackshear PJ. Golden-berg FJ, Buchwald H: Risk of osteoporosis in patients treated withlong term intravenous hepanin therapy. Curr Surg 1982; 39:419-
422.
43. Monreal M, Vinas L, Monreal U, Lavin 5, Lafoz E, Angles AM:Heparin-related osteoporosis in rats, A comparative study be-tween unfractionated hepanin and a low-molecular-weight hepa-nfl. Haemostasis, 1990; 20:204-207.
44. Jaffe MD, Willis PW: Multiple fractures involved with longterm sodium heparin therapy. JAm Med Assoc 1965; 193:158-160.
45. Thompson JM, Poller L: The activated partial thromboplastintime, in Thomas JM (eds.): Blood Coagulation and Haemostasis.Edinburgh: Churchill Livingstone, 1985; 301.
46. Hellgren M, Hagnevik K, Blomback M: Hepanin aerosol: Effecton blood coagulation and pulmonary function. Thromb Res1981; 21:493-502.
47. Cinsberg JS, Hirsh J, Turner DC, Levine MN, Burrows R: Risksto the fetus of anticoagulant therapy during pregnancy. ThrombHoemost 1989;61:197-203.
48. Forrestier F, Daffos F, Rainaut M, Toulemonde F: Low molecu-lar weight hepanin does not cross the placenta during the thirdtrimester of pregnancy. Thromb Haemost 1987;57:234.
49. Andrew M, Cade I. Buchanan MR: Low molecular weight hep-arm does not cross the placenta (abstr.). Thromb Haemost1983; 50:225.
50. Follea C, Laville M, Pozet N, Dechavanne M: Pharmacoki-netic studies of standard hepanin and low molecular weight hepa-nin in patients with chronic renal failure. Haemostasis1986; 16:147-151.
51. Groudable CH, TonThat H, Damani A, Durand D, CarnanobeC, Sie P. Boneu B: Low molecular weight heparin half life is pro-longed in haemodialysed patients. Thromb Res 1986;43:1-5.
52. Coffman JD: Deep venous thrombosis and pulmonary emboli:Etiology, medical treatment and prophylaxis, J Thorac Imaging1989;4:4-7.
53. Haake D, Berkman SA: Venous thromboembolic disease afterhip surgery: Risk factors, prophylaxis, and diagnosis. Clin Orthop1989; 212-231.
54. Kakkar V: The diagnosis of deep vein thrombosis using the 1125
fibninogen test. Arch Surg 1972; 104:152-159.
55. Paiemont GD, Desautels C: Deep vein thrombosis: Prophy-laxis, diagnosis and treatment: Lessons from orthopedic studies.Gun Cardiol 1990;13:V119-V222.
56. Clagett GP, Salzman EW: Prevention of venous thnomboem-bolism in surgical patients. N EngI J Med 1974;290(2):93-96.
57. Nicolaides AN, Kakkar VV, Renney JTG, Kidner PH, Huthchi-son DCS, Clarke MB: Myocardial infarction and deep vein throm-bosis. BrMedJ 1971;1:432-434.
58. Belch JJ, Lowe GDO, Ward AG, Forbes CD, Prentice CRM:Prevention of deep vein thrombosis in medical patients by lowdose hepanin. Scott Med J 1981;26:115-117.
59. Gordon-Smith IC, Grundy DJ, LeQuesne UP, O’Brien SE: Con-trolled trial of two regimens of subcutaneous hepanin in preven-tion of post operative deep vein thrombosis. Lancet 1972;1:1133-1135.
60. Rosenberg IL. Evans M, Pollack AV: Prophylaxis of post-opera-tive leg thrombosis by low dose subcutaneous hepanin or pre-oper-ative calf stimulation. Br Med 1 1975; 1:649.
61. Kakkar VV, Spindler J, Flute PT, Connigan T. Fossand DP. Crel-lin RQ: Efficacy of low doses of hepanin in prevention of deep vein
thrombosis after major surgery, a double blinded, randomised
study. Lancet 1972; 2:101-106.
62. Handley AJ: Low-dose hepanin after myocardial infarction.
Lancet 1972; 2:623-624.
63. Colditz GA. Tuden RU, Oster C: Rates of venous thrombosisafter general surgery: Combined results of randomised clinicaltrials, Lancet 1986; 2:143-146.
64. Clagett GP, Reisch JS: Prevention of venous thromboembo-lism in general surgical patient. Ann Surg 1988; 208:227-240.
65. Kakkar VV, Adams PC: Preventive and therapeutic approachto venous thromboembolic disease and pulmonary embolism: Candeath from pulmonary embolism be prevented? JACC 1986;
8:146B.
66. Cent M, Roberts RS: A meta-analysis of the studies of dihy-
droergotamine plus hepanin in the prophylaxis of deep vein throm-
bosis. Chest 1986;89(suppl):369.
67. The multicenter trial committee. JAMA 1984; 251:2960-2966.
68. Hirsch J: JAMA 1984;251:2985-2986.
69. Dahan D, Houlbert D, Coulin C, Cuzin E, Viltart C, Waler M,Segresta JM: Prevention of deep vein thrombosis in elderly medi-
cal in-patients by a low molecular weight heparin: A randomizeddouble blind trial. Heamostasis 1986;16:159-164.
70. Henenbeng J, Kalenbach B, Martin U. Zimmerman R: Random-ized double blinded study of normal and low molecular weighthepanin in general medical patients (abstr.). Thromb Haemost1987; 58:1492..
71. Turpie AGG, Hirsh J, Jay RM, Andrew M, Hull RD, LevineMN, Carter CJ, Powers PJ, Magnani HN, Gent M: Double-blindrandomized trial of org. 10172 low molecular weight heparinoidin the prevention of deep-vein thrombosis in thrombotic stroke.Lancet 1987; 1:523-526.
72. Green D, Lee MY, Lim AC, et a!: Prevention of thromboem-bolism after spinal cord injury using low-molecular weight hepa-nin. Ann Intern Med 1990;113:571-574.
73. Samama M, Bernard P. Bonnardot JP, Combe-Tamzali S, Lan-som Y, Tissot E: Low molecular weight hepanin (enoxipanine)compared with unfractionated heparin thrice daily in the preven-tion of postoperative thrombosis. A randomized multicenter trial,
Br J Surg 1988;75:128-131.
74. Kakkan VV, Murray W: Efficacy and safety of low molecularweight hepanin (CY216) in preventing post-operative venous
thromboembolism: A cooperative study. Br J Sung 1985; 766-791.
75. Turpie ACG, et al: A randomized controlled trial of a lowmolecular weight heparin (enoxapanine) to prevent deep vein
thrombosis in patients undergoing elective hip surgery. N Engi JMed 1986;315(15):925-929.
76. Enke A, Breddin K. The European FRAXIPARINE StudyGroup: Comparison of a low molecular weight heparin and Un-
fractionated hepanin for the prevention of deep vein thrombosis in
patients undergoing abdominal surgery. Br J Surg 1988;18:75,
1058-1063.
77. Bergqvis D, Burmark US, Fnisell J, Hallbrook T, Uindblad B,
Risberg B, Torngren 5, Wallin C: Low molecular weight hepanin
once daily compared with conventional low-dose hepanin twicedaily: a prospective double-blind multicenter trial on preventionof postoperative thrombosis. Br J Surg 1986; 73:204-208.
78. Anderson FA, Wheeler B, Goldberg RJ. Hosmer DW, ForcierA, Patwardhan NA: Physician practices in the prevention of ve-nous thromboembolism. Ann Intern Med 1991;115: 591-595.
79. Barnitt DW, Jordan SC: Anticoagulant drugs in the treatment

HEPARIN, PHARMACODYNAMICS, CLINICAL INDICATIONS
THERAPEUTIC REVIEW 595
of pulmonary embolism: A controlled trial. Lancet 1960;1:1309-1367.
80. Hull RD. Raskob CE, Hirsch J: A double blind randomizedtrial of IV. hepanin versus Subcutaneous heparin in the initialmanagement of proximal vein thrombosis. N Engl I Med1986; 315:1109.
81. Vairel EG, Brouty-Boye H, Toulemonde F, et al: Hepanin and alow molecular weight fraction enhance thrombolysis and by thispathway exercise a protective effect against thrombosis. Thromb
Res 1983; 30:219-224.
82. Hull R, Delmore T, Genton E, Hirsch J, Cent M, Sackett D,McLaughlin D, Armstrong P: Warfarin sodium versus low-doseheparin in the long term treatment of venous thrombosis. N Engl JMed 1979; 301:855-858.
83. Holm HA, Finnager B, Hartmann A, Laerum F, Lohren 0,Rund TE, Stray N: Treatment of deep venous thrombosis in 280patients: symptoms related to dosage. Acta Med Scand1984; 215:47-53.
84. Hull RD, Raskob CE, Rosenbloom D, et al: Heparin for 5 daysas compared to 10 days in the initial management of proximalvein thrombosis. N Engl J Med 1990; 322:1260-1264.
85. Wilson JE, Bynum U, Parkey RW: Heparin therapy in venousthromboembolism. Am J Med 1981;70:808-816.
86. Murray WJG, Malone PS, Parker C, Huber DE, Kakkar VV: Atrial of subcutaneous versus intravenous administration of lowmolecular weight (LMW) heparin and unfractionated (UH) hepa-nin in the treatment of established deep venous thrombosis (DVT).Br J Sung 1986; 73:216,
87. Bratt C, Tornebohm E, Granqvist S. Aberg W, Lockner D: Acomparison between low molecular weight hepanin (kabi 2165)and standard heparin in the intravenous treatment of deep throm-bosis. Thromb Haemost 1985; 54:813-817.
88. Kakkar VV, Murray WJG, Walters HL, Celister J, Malone P,Jones D: Treatment of deep vein thrombosis using a low molecularweight heparin (LMWH) (CY216). Thromb Haemost 1985; 54:35.
89. Duroux P: Treatment of proximal deep vein thrombosis of thelimbs by low-molecular weight heparin vs. unfractionated hepa-nin, a European multicenter trial. Congress of the InternationalSociety of Hematology, Milan, Italy, September 1988.
90. Hull RD. Raskob GE, Hirsch J, Jay RM, Leclerc JR, Ceerts WH,Rosenbloom D, Sackett DL, Anderson C, Harrison U, Gent M: Con-tinuous intravenous heparin compared with intermittent subcuta-neous heparin in the initial treatment of proximal vein thrombo-sis. N EngI J Med 1986;315:1109-1114.
91. Hirsh J, Hull, Russell D: Treatment of venous thromboembol-ism. Chest 1986; 89:426S-4335.
92. Coldhaber SZ, Buring JE, Lipnick RJ, Hennekens CH: Pooledanalysis of randomized trials of streptokinase and heparin in phle-bographically documented acute deep vein thrombosis. Am J Med1984; 76:393-397.
93. Einhaupl K, Villninger A, Meister W, Mehraein 5, Garner C,Rellkofer M, Haberl RL, Pfister HW, Schmiedek F: Heparin treat-ment in sinus venous thrombosis. Lancet 1991;338:597-600.
94. Marks P. Teather D: Subcutaneous hepanin: A logical prophy-laxis for deep vein thrombosis after myocardial infarction. Practi-tioner 1978; 220:425.
95. Johannessen KA, Nordrehaug JE, von den Lippe C: Incidenceof left ventricular thrombosis and cerebnovascular accident inacute myocardial infarction. Br Heart J 1984;51:553-556.
96. Kaplan K: Prophylactic anticoagulation following acute myo-cardial infarction. Arch Intern Med 1986; 146:593-597.
97. Gueret P. Dubourg 0, Ferrier A, Farcot JC, Rigaud M, Bour-
danias JP: Effects of full dose hepanin anticoagulation on the devel-opment of left ventricular thrombosis in acute transmural myo-cardial infarction. JAm Call Cardiol 1986; 8:419-426.
98. Nordrehaug JC, Johannessen K, Von Den Uippe G: Usefulnessof high dose anticoagulants in preventing left ventricular throm-bus in acute myocardial infarction. Am J Cardiol 1985;55:1491.
99. Meltzer RS, Visser CA, Fuster V: Intracardiac thrombi andsystemic embolization. Ann Intern Med 1986;104:689-698.
100. Ezekowitz MD, Aznin AA: Should patients with large ante-rior wall myocardial infarction have echocardiography to identifyleft ventricular thrombus and should they be anticoagulated?Cardiol Clin 1990; 21(1):105-120.
101. Turpie AGO, Robinson JG, et al: Comparison of high dosewith low-dose subcutaneous heparin to prevent left ventricularthrombosis in patients with acute transmural myocardial infarc-tion. N Engl J Med 1989; 320:352-357.
102. Assessment of short-term anticoagulation administrationafter cardiac infarction, Report of the working party on anticoagu-lant therapy in coronary thrombosis to the medical researchcouncil. Br Med J 1969;1:335-342.
103. Anticoagulants in acute myocardial infarction, results of acooperative clinical trial. JAMA 1973; 225:724-729.
104. Sayen JJ. Singer RB. Peirce C, Cooper LT, Horwitz 0: Long-term flexible dose hepanin in coronary heart disease, correlationof frequency of cardiovascular events with different hepanin dos-age levels, and observations on comparative mortality. Ann N YAcad Sci 1989;556:476-479.
105. Neri Semen CC, Rovelli F, Gensini GF, Pirelli S, CarnovaliM, Fortini A: Effectiveness of low-dose hepanin in prevention ofmyocardial infarction. Lancet 1987;2:937-942.
106. Topol El: How should intravenous thrombolytic agents foracute myocardial infarction be selected? Cardiovasc Clin1990; 21:57-75.
107. Van Breda A: Thrombolysis in arterial bypass grafts. Semin
Thromb Hemost 1991;17:7-13.
108. Zietler E: Drug treatment before and after percutaneoustransluminal recanalization, in Zeitler E, Gruntzig A, Schoop W(eds.): Percutaneous Vascular Recanalization. Technique Applica-tion, Clinical Results. Berlin: Springer-Verlag, 1978;000-000.
109. McCarry T, Gottlieb R, Zelenkofske S. Duca P. Kaspanian H,Kreulen T, Morganroth J: Relationship of anticoagulant level andcomplications after successful percutaneous transluminal angio-plasty (abstr.). Circulation 1990;82:189.
110. Kern MJ, Deligonul U, Presant 5, Vandonmael M: Resolutionof intraluminal thrombus with augmentation of hepanin duringpercutaneous transluminal coronary angioplasty. Am I Cardiol1986; 58:852-853.
111. Semen GGN, Abbate R, Prisco D, Carnovali M, Fazi A, Ca-solo CC, Bonechi F, Rogasi PC, Gensini F: Clinical investigations:Decrease in frequency of angina! episodes by control of thrombingeneration with low dose heparin: A controlled cross over random-ized study. Am Heart J 1988;115:45-53.
112. Theroux P, Ouimet H, McCans J, Latour JG, Joly P. Levy C,Pelletier E, Juneau M, Stasiak J, deCuise F, Pelletier GB, Rinzler 0,Waters DD: Aspirin hepanin or both to treat acute unsable angina.N Engl J Med 1988;319:1105-1111.
113. Telford AM, Wilson C: Trial of heparin versus atenolol inprevention of myocardial infarction in immediate coronary syn-drome. Lancet 1981; 1:1225-1228.
114. Williams DO, Kirby MG, McPherson K, Phear DM: Anticoag-ulant treatment in unstable angina. Br J Clin Prac 1986;40:114-116.

FREEDMAN
596 S J Clln Pharmacol 1992;32:584-596
115. Wallentin L for the RISC Study Group of Unstable CoronaryArtery Disease: Risk for myocardial infarction and death in a ran-domized placebo-controlled study (abstr.). Circulation 1989;(suppl. 2):lI-419.
116. Ireland H, Rylance PB, Kesteven P: Hepanin as an anticoagu-lant during extracorporeal circulation, in Lane DA, Uindahl U(eds.): Heparin, Chemical and Biological Properties, Clinical Ap-plications. Boca Raton, Florida: CRC Press, 1989.
117. Woodman RC, Hanker LA: Bleeding complications asso-ciated with cardiopulmonary bypass. Blood 1990; 76:1680-1697.
118. Schmer G, Teng UNU, Cole JJ, Vizzo JE, Francisco MM,Scribner BH: Successful use of a totally heparin grafted hemodialy-sis system in sheep. Trans Am Soc Artif Intern Organs1977; 22:654.
119. Schmitt E, Holtz M, Klinkmann H, Esther C, Courtney: Hepa-nfl binding and release properties of DEAE cellulose membranes.Biomatenials 1983;4:309.
120. Olsson P. Larm 0, Larsson R, Uins LE, Nilsson E, SwedenbongJ: Requirements for thromboresistance of surface-heparinized ma-terials. Ann N Y Acad Sci 1983;416:525-536.
121. Lane DA. Flynn AM. Ireland H, Anastassiades E, Curtis JR:On the evaluation of hepanin and low molecular weight heparinin hemodialysis for chronic renal failure. Haemostasis1986; 16:18-47,
122. Ireland H, Lane DA, Flynn A, Anastassiades E. Curtis JR: Theanticoagulant effect of heparinoid Org 10172 during hemodialysis:An objective assessment. Thromb Haemost 1986; 55:271-275.
123. Lane DA, Tew C, Ireland H, Flynn A, Curtis J: Hepanin andlow molecular weight hepanin(oid)s as anticoagulants in hemodial-ysis for chronic renal failure. Ann N Y Acad Sci 1989;556:456-458.
124. Gouault-Heilmann M, Huet Y. Contant C, Payen D, Bloch C:Cardiopulmonary bypass with a low molecular weight hepaninfraction (letter). Lancet 1983; 11:1374.
125. Aiach M, Dreyfus C, Michaud A: Low molecular weight hep-arm derivatives in experimental extra-corporeal circulation(ECC). Haemostasis 1984;14:325-332.
126. Massonet-Castel S. Pelissier E, Dreyfus G. Deloche A, AbryB, Guibourt P, Terrier E, Passelecq J, Jaulmes B, Carpentier A: Uowmolecular weight heparin in extracorponeal circulation. Lancet1984; 1:1182-1183.
127. Wilbanks OL, Fuller CH: Femoral neuropathy due to metro-penitoneal bleeding. Arch Intern Med 1973;132:83-86.
128. Levine MN, Himsh J, Kelton JC: Heparin induced bleeding, inLane DA, Lindahl U (eds.): Heparin, Chemical and Biological Prop-
erties, Clinical Applications. Boca Raton, Florida: CRC Press,1989; 517-531.
129. Salzman EW, Deykin D, Shapiro RM, Rosenberg R: Manage-ment of hepanin therapy. N EngI I Med 1975; 292:1046-1050.
130. Kelton JG: Hepanin induced thrombocytopenia. Heamostasis1986; 16:173-186.
131. Chang JC: White clot syndrome. A serious complication ofheparin therapy. Postgrad Med 1990;87:293-298.
132. Salzman EW: Low molecular weight hepanin: Is small beauti-ful? N Engl J Med 1986;315:957-959.
133. Roussi J, Houbouyan U, Goguel A: Use of low molecularweight heparin in hepanin induced thrombocytopenia with throm-botic complications. Lancet 1984; 2:1183.
134. Saffle JR. Russo J, Dukes CE, Warden OD: The effect of lowdose hepanin therapy on serum platelet and transaminase levels. JSurg Res 1980; 28:297-305.
135. . Freedman MD, Ueese F, Prasad R, Hayden D: An evaluationof the biological response to Fraxipanine, (a low molecular weighthepanin) in the healthy individual.J Clin Pharm 1990; 30:720-727.
136. Schwartz KA, Royen C, Kaufman DB, Penner JA: Complica-tions of hepanin administration in normal individuals. Am J He-matol 1985; 14:355-363.
137. Sackler JP, Uiu U: Hepanin induced osteoporosis. Br J Radial1973; 46:548-550.
138. Griffith CC, Nichols C. Asher J: Hepanin osteoporosis. JAMA1965; 193:91.
139. Humley MM, Cronwowicz C, Kream BE, Raisz UG: Effect ofhepanin on bone formation in cultured fetal rat calvania. CalcifTissue mt 1990;46:183-188.
140. Belilovsky C: Skin necrosis due to low molecular weight hep-ann, J Dermatol 1987; 23:51 (in French).
141. Condaliani F, Saiag P. Guillaume JC: Multiple sclerosis of theskin induced by Fraxipanine. Ann Dermatol Venereol1987; 114:1366-1368,
142. Walker AM, Jick H: Predictors of bleeding during hepanintherapy. JAMA 1980;244:1209.
143. Yett I-IS, Skillman JJ, Salzman EW: The hazards of aspirinplus heparin. N Engl I Med 1978; 298:1092.
144. FDA Drug Bulletin 1983;13:16.
145. Habbab MA. Haft Jl: Hepanin resistance induced by intrave-nous nitroglycerin, Arch Intern Med 1987; 147:857-860.
146. McKillop G, et a!: Possible interaction between hepanin anda sulphonylurea a cause of prolonged hypoglycemia? Br Med J1986; 293:1073.

本文献由“学霸图书馆-文献云下载”收集自网络,仅供学习交流使用。
学霸图书馆(www.xuebalib.com)是一个“整合众多图书馆数据库资源,
提供一站式文献检索和下载服务”的24 小时在线不限IP
图书馆。
图书馆致力于便利、促进学习与科研,提供最强文献下载服务。
图书馆导航:
图书馆首页 文献云下载 图书馆入口 外文数据库大全 疑难文献辅助工具