Embed Size (px)
Citation preview

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
LATE-BREAKING CLINICAL TRIAL
Pharmacist intervention in primary careto improve outcomes in patients with leftventricular systolic dysfunctionRichard Lowrie1*, Frances S. Mair2, Nicola Greenlaw3, Paul Forsyth1,Pardeep S. Jhund4, Alex McConnachie3, Brian Rae1, and John J.V. McMurray4,on behalf of the Heart Failure Optimal Outcomes from Pharmacy Study(HOOPS) Investigators1Long Term Conditions and Research, Pharmacy and Prescribing Support Unit, NHS Greater Glasgow and Clyde, Queens Park House, Victoria Infirmary, Langside Road, GlasgowG42 9TY, UK; 2General Practice and Primary Care, University of Glasgow, Glasgow, UK; 3Robertson Centre for Biostatistics, University of Glasgow, Glasgow, UK; and 4BHFCardiovascular Research Centre, University of Glasgow, Glasgow, UK
Received 18 October 2011; revised 2 November 2011; accepted 3 November 2011; online publish-ahead-of-print 14 November 2011
Background Meta-analysis of small trials suggests that pharmacist-led collaborative review and revision of medical treatment mayimprove outcomes in heart failure.
Methodsand results
We studied patients with left ventricular systolic dysfunction in a cluster-randomized controlled, event driven, trial inprimary care. We allocated 87 practices (1090 patients) to pharmacist intervention and 87 practices (1074 patients)to usual care. The intervention was delivered by non-specialist pharmacists working with family doctors to optimizemedical treatment. The primary outcome was a composite of death or hospital admission for worsening heart failure.This trial is registered, number ISRCTN70118765. The median follow-up was 4.7 years. At baseline, 86% of patients inboth groups were treated with an angiotensin-converting enzyme inhibitor or an angiotensin receptor blocker. Inpatients not receiving one or other of these medications, or receiving less than the recommended dose, treatmentwas started, or the dose increased, in 33.1% of patients in the intervention group and in 18.5% of the usual care group[odds ratio (OR) 2.26, 95% CI 1.64–3.10; P , 0.001]. At baseline, 62% of each group were treated with a b-blockerand the proportions starting or having an increase in the dose were 17.9% in the intervention group and 11.1% in theusual care group (OR 1.76, 95% CI 1.31–2.35; P , 0.001). The primary outcome occurred in 35.8% of patients in theintervention group and 35.4% in the usual care group (hazard ratio 0.97, 95% CI 0.83–1.14; P ¼ 0.72). There was nodifference in any secondary outcome.
Conclusion A low-intensity, pharmacist-led collaborative intervention in primary care resulted in modest improvements in pre-scribing of disease-modifying medications but did not improve clinical outcomes in a population that was relativelywell treated at baseline.
- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -Keywords Left ventricular systolic dysfunction † Primary care † ACE inhibitor † b-Blocker
IntroductionAlthough angiotensin-converting enzyme (ACE) inhibitors, angio-tensin receptor blockers (ARBs), and b-blockers reduce morbidityand mortality in patients with heart failure due to left ventricularsystolic dysfunction, there is evidence that these treatments areunderused, particularly in primary care.1 –5 Some patients who
should receive these medications do not and many receive lessthan evidence-based doses.2– 5 Pharmacists may play a role inimproving treatment through ‘collaborative medication review’, aprocess in which the pharmacist evaluates a patient’s medicationsand suggests changes which are enacted with the agreement ofthe patient and the family doctor.6– 9 A meta-analysis of small,short-term trials and observational data suggest that this
* Corresponding author: Tel: +44 141 201 5317, Fax: +44 141 201 5345, Email: [email protected]
Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2011. For permissions please email: [email protected]
European Heart Journal (2012) 33, 314–324doi:10.1093/eurheartj/ehr433
by guest on Novem
ber 15, 2014D
ownloaded from

intervention reduces the risk of hospital admission and possiblymortality in patients with heart failure studied in a secondarycare setting.6 – 10 We conducted a larger-scale, longer-term pro-spective randomized controlled trial to test the hypothesis that alow-cost, low-intensity pharmacist intervention to optimizemedical treatments, particularly ACE inhibitors, ARBs, andb-blockers, in patients identified in primary care with left ventricu-lar systolic dysfunction would reduce the composite outcome ofhospital admission for worsening heart failure or death, as wellas other clinically important outcomes.
Methods
Study design and patientsThe study was conducted within the National Health Service (NHS)which provides free health care to the population of the UK. Thedesign of our trial has been published and was consistent with Conso-lidated Standards of Reporting Trials.11 –13 Consenting patients wereeligible if aged ≥18 years and had left ventricular systolic dysfunctionconfirmed by cardiac imaging conducted at a local hospital (transthor-acic echocardiography in 90% of cases). Patients did not have to havesymptoms or signs of heart failure. Family doctors receive a semi-quantitative report of left ventricular systolic function (normal, mild,moderately or severely reduced) instead of ejection fraction. A keyexclusion criterion was registration with the heart failure nurseservice, which is provided to patients in our Health Board area recent-ly admitted to hospital with heart failure. This criterion excludedhigher-risk patients with more severe symptoms. Other exclusioncriteria included concurrent disease other than heart failure likely toreduce life expectancy; severe cognitive impairment or psychiatricillness; and dialysis or a resident in a long-term care facility. Thestudy was approved by the local ethics committee. All practices andpatients gave written informed consent. The study is registered,number ISRCTN70118765.
RandomizationWe used a cluster randomization design as this provides protectionagainst contamination across trial groups when trial patients aremanaged within the same setting as was the case in this study. Patientsin practices in the UK are managed by all general practitioners withinthe practice; as the control intervention was mediated by generalpractitioners, this precluded individual patient level randomization.Family practices were randomly allocated using a third-party auto-mated telephone interactive voice response system in a 1:1 ratio toreceive intervention or usual care. Stratification was by socioeconomicdeprivation (affluent, intermediate, or deprived) at the practice leveland the practice type (single-handed or group-practice).11
Study proceduresThe intervention was delivered by 27 primary care-based pharmacistsemployed by the NHS to work with family doctors and directly withpatients to promote rational, cost-effective prescribing.14 All participat-ing pharmacists had between 3 and 16 years of post-qualificationexperience. All had experience delivering primary care-based medica-tion review clinics for patients receiving multiple drug treatment. Sevenpharmacists held post-graduate clinical pharmacy qualifications. Fourpharmacists had hospital (ward-based) clinical pharmacy experience.Prior to commencing the intervention, all pharmacists attended one,in-house training day (contact time 7.5 h) covering the aetiology, symp-toms, and evidence-based management of heart failure. The day was
coordinated by three pharmacists who had a special interest in heartfailure therapeutics, and a general practitioner with a special interestin heart failure. The day comprised of a mixture of didactic teachingand interactive role-play sessions. An additional mandatory 3-hsession covered the methods of the trial. All pharmacists received aninformation pack with directed, heart failure-specific reading tosupplement their training.
As part of routine continuing professional development, eachpharmacist participated in a 3.5-h peer-led session every monthwhich involved group discussion of cases encountered in their medica-tion review clinics. As the study pharmacists were embedded withinprimary care practices, informal discussion on therapeutics occurredregularly between pharmacists, general practitioners, and nurseswithin the practice. There was also regular telephone contactbetween study pharmacists and the principal investigator or anotherpharmacist with a special interest in heart failure.
Patients from practices assigned to the intervention were offered a30-min appointment with a pharmacist. The main aim of this reviewwas optimization of medical treatment for left ventricular systolic dys-function according to guidelines (Supplementary material online). Ifthere was agreement between the pharmacist and the patient duringthe consultation and subsequently with the family doctor, medicationswere initiated, discontinued, or modified by the pharmacist during 3–4subsequent weekly or fortnightly consultations. Family doctors pro-vided usual care thereafter. No instructions were given to familydoctors in the usual care practices. The study pharmacists did notcollect information on symptoms or examine the patients as this wasnot part of their professional training. The cause of heart failure wasestablished by scrutinizing primary and secondary care (e.g. hospitalletters and discharge summaries) clinical records.
Study outcomesThe primary outcome was the composite of death from any cause orhospital admission for worsening heart failure, analysed as time to firstevent. Secondary endpoints included the composites of death from anycause or hospital admission for pre-specified cardiovascular causes(Supplementary material online), death from any cause, or hospitaladmission for any cause; total number of admissions (and patientsadmitted) for heart failure, cardiovascular causes, and any cause; anddays alive out of hospital. Outcome data were obtained from the Infor-mation Services Division (ISD) of the NHS in Scotland, which recordsall discharges from Scottish NHS hospitals (i.e. virtually all hospitaladmissions in Scotland) and the General Register Office which recordsall deaths. Hospital discharge data are reported to ISD with dischargediagnoses coded according to the International Classification of Diseasessystem, 10th revision.15,16 This approach to patient follow-up has beencompared favourably with traditional clinical trial methods.17,18 Althoughthe end-of-study date was 31 January 2011, data extraction did not occuruntil 25 July 2011 in order to ensure that all deaths and hospital admis-sions were entered into the national database.
We also compared the prescribing of medications between theintervention and usual care groups and evaluated health-care utiliza-tion, other than admissions, at 1 and 2 years of follow-up, e.g. thenumber of primary care contacts and hospital emergency room visits.
Statistical analysisThe trial data were managed and analysed by the Robertson Centre forBiostatistics, University of Glasgow. The primary analysis compared themain outcomes between the intervention and control groups using aCox proportional hazards frailty model, which accounted for thecluster-randomization design.11– 13 All analyses were performed using
Pharmacist intervention in primary care to improve outcomes in patients with left ventricular systolic dysfunction 315
by guest on Novem
ber 15, 2014D
ownloaded from

either SAS version 9.2 or R version 2.10.1 or greater. A significancelevel of 0.05 was used to test for statistical differences throughoutand all tests used were two-sided. Analyses were adjusted for thestratification variables and the following variables of prognostic import-ance: age, creatinine, grade of left ventricular systolic dysfunction, atrialfibrillation, respiratory disease, total number of medical treatments,and diuretic use.
We assumed the rate of the primary outcome would be 10% peryear in the control group and pharmacist intervention would lead toa relative risk reduction of 26%, based on the known benefits ofinitiating disease-modifying treatment and of higher doses of thosetherapies.1,19,20 We also assumed recruitment would last 2.6 yearsand follow-up would continue for 2 further years. Under these
assumptions, to have 80% power to detect a difference between treat-ments, the trial would require 673 patients to experience a primaryoutcome. Inflating the sample size by a factor of 1.55 to account forthe cluster randomization design, we needed 87 practices (1044patients) per group.11 –13 Due to longer than anticipated recruitment,blinded review of the data in September 2010 suggested that morethan 750 patients were expected to experience the primaryoutcome, providing 80% power to detect a 19% relative risk reduction.
Logistic regression models were used to examine the secondaryoutcomes including whether patients started or stopped a medicaltreatment or had a change in dose.
Safety was evaluated by examining hospital admissions for:symptomatic hypotension, collapse, or syncope; renal dysfunction,
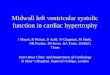
Figure 1 Study recruitment. §Five patients (from five practices, two intervention and three usual care) died in the period between baselinedata collection and practice randomization. *Information on treatment unavailable for two patients between baseline year 1 and one additionalpatient between the end of year 1 and the end of year 2. LVSD, left ventricular systolic dysfunction.
R. Lowrie et al.316
by guest on Novem
ber 15, 2014D
ownloaded from

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 1 Baseline characteristics of patients, according to study group*
Characteristic Pharmacist intervention (n 5 1092)a Usual care (n 5 1077)a
Age (years) 70.6 (10.3) 70.6 (10.1)
Age ≥70 years 597 (55%) 597 (55%)
Sex (female) 320 (29%) 329 (31%)
Blood pressureb
SBP (mmHg) 127 (17.4) 128 (17.4)
DBP (mmHg) 72 (10.1) 72 (10.2)
Left ventricular systolic function (%)c
Mild reduction 433 (42%) 390 (39%)
Moderate reduction 416 (41%) 439 (44%)
Severe reduction 170 (17%) 175 (17%)
BMI (kg/m2)d 28.0 (5.4) 28.0 (5.4)
Principal cause of left ventricular systolic dysfunction (%)
Ischaemic heart disease 874 (80%) 817 (76%)
Non-ischaemic heart disease 197 (18%) 230 (21%)
Unknown 21 (2%) 30 (3%)
Duration of LVSD (years)e 3.31 (1.54–5.85) 3.53 (1.76–5.87)
Medical history
Admission for heart failure in past year 19 (2%) 18 (2%)
Hypertension 548 (50%) 495 (46%)
Myocardial infarction 722 (66%) 665 (62%)
PCI 161 (15%) 144 (13%)
CABG 266 (24%) 268 (24%)
Atrial fibrillation or flutter 292 (27%) 304 (28%)
Diabetes mellitus 234 (21%) 212 (20%)
Stroke 148 (14%) 162 (15%)
Respiratory disease 326 (30%) 318 (30%)
Asthma 72 (7%) 82 (8%)
Smoker 262 (24%) 260 (25%)
Serum creatinine (mmol/L)f 109 (33) 107 (30)
eGFR (mL/min per 1.73 m2)g 61.3 (17.5) 62.6 (23.2)
Device treatment (%)h
Implantable cardioverter-defibrillator 19 (2%) 12 (1%)
Conventional pacemaker 22 (2%) 29 (3%)
Cardiac medicines at randomization (%)
ACE inhibitor 814 (75%) 768 (71%)
≥50% recommended dosei 695 (86%) 656 (86%)
≥100% recommended dosei 483 (59%) 472 (62%)
ARB 149 (14%) 181 (17%)
≥50% recommended dosei 102 (68%) 107 (59%)
≥100% recommended dosei 34 (23%) 35 (19%)
ACE inhibitor or ARB or both 944 (86%) 919 (85%)
b-Blocker 674 (62%) 664 (62%)
≥50% recommended dosei 339 (51%) 339 (52%)
≥100% recommended dosei 146 (22%) 128 (20%)
Aldosterone antagonist 54 (5%) 56 (5%)
Digitalis glycoside 149 (14%) 124 (12%)
Diuretic 667 (61%) 654 (61%)
Aspirin 751 (69%) 691 (64%)
Continued
Pharmacist intervention in primary care to improve outcomes in patients with left ventricular systolic dysfunction 317
by guest on Novem
ber 15, 2014D
ownloaded from

failure, or impairment; hyperkalaemia; asthma or chronic obstructivepulmonary disease; and bradycardia, atrioventricular block, or pace-maker implantation. Fisher’s tests were used to compare the interven-tion group with the usual care group.
Results
Study patientsAll general practices in our locality were approached and 174 of220 (79%) practices (covering 790 421 of 998 402, i.e. 79% ofpatients registered with a general practitioner in our HealthBoard area) took part in the trial. From 25 October 2004through 6 September 2007, 87 primary care practices (1090patients) were randomly assigned to pharmacist intervention and87 practices (1074 patients) to usual care (Figure 1). One patienthad incomplete follow-up due to emigration. The median durationof follow-up was 4.7 years (range 6 days to 6.2 years; 9362patient-years).
The two groups were balanced with respect to baseline charac-teristics (Table 1). Fifty-five per cent of patients were aged ≥70years. There was a high prevalence of ischaemic heart disease(80%) and respiratory disease (30%). A semi-quantitative assess-ment of left ventricular function was recorded in 2023 (93%)patients, with most having either a mild (41%) or a moderate(42%) reduction in systolic function. In a small reasonably repre-sentative subset of patient records (n ¼ 256; 12%), there wasdocumentation of a left ventricular ejection fraction value alongwith a semi-quantitative assessment of systolic function. In thesepatients, the mean ejection fraction was 36.8% (SD 6.5%) inthose with mildly reduced systolic function, 30.5% (7.5%) inthose with moderately reduced function, and 19.7% (7.7%) inthose with severely reduced function.
Although general practitioners do not routinely record theNew York Heart Association (NYHA) class in our area (and theNYHA class was not recorded by the study pharmacists), this
measure was documented in the records of 337 patients; 87(26%) were NYHA class I; 215 (64%) were NYHA class II; 33(10%) were NYHA class III; and 2 (1%) were in NYHA class IV.
Very few (1.7%) patients had been admitted to a hospital forheart failure in the year prior to randomization.
Medical treatmentIn each treatment group, �86% of patients were receiving an ACEinhibitor, ARB, or both (Table 1) and of these patients, 55%received 100% or more of the recommended dose. The propor-tion of patients receiving a b-blocker was 62% in each treatmentgroup. Of these, 21% were treated with 100% or more of therecommended dose (Table 1).
Patients not prescribed an ACE inhibitor, ARB, or b-blocker, ornot prescribed the recommended doses of these medications atbaseline, were potentially eligible for treatment optimization.Table 2 shows the effect of pharmacist intervention (patientswho died during the first and second years of follow-up wereexcluded from this analysis—dead patients could not receive theintervention). Pharmacist intervention during the first year of thetrial led to a greater frequency of initiation of an ACE inhibitoror ARB and a b-blocker, compared with usual care (Table 2).The same was true for increases in the dose of these treatments.At the end of year 1, an ACE inhibitor or ARB was started or thedose was increased in 168 of 507 (33.1%) patients in the interven-tion group and 95 of 514 (18.5%) patients in the usual care group[odds ratio (OR) 2.26, 95% CI 1.64–3.10, P , 0.001]. The propor-tions starting or having an increase in the dose of b-blocker were153 of 854 (17.9%) patients in the intervention group and 95 of855 (11.1%) patients in the usual care group (OR 1.76, 95% CI1.31–2.35, P , 0.001). The resultant proportion of patients receiv-ing an ACE inhibitor, ACE inhibitor or ARB and b-blocker at theend of year 1 and year 2 is shown in Table 3, as well as the propor-tions of those patients receiving at least 50% and at least 100% ofthe recommended dose (this table also takes account of
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 1 Continued
Characteristic Pharmacist intervention (n 5 1092)a Usual care (n 5 1077)a
Antithrombotic (antiplatelet or oral anticoagulant) 990 (91%) 969 (90%)
Amiodarone 20 (2%) 32 (3%)
Lipid lowering agent 863 (79%) 841 (78%)
Number of medicinesj 8.9 (4.0) 8.4 (3.5)
Data are the numbers of patients (%) or mean (SD). Percentages may not total 100 because of rounding. SBP, systolic blood pressure; DBP, diastolic blood pressure; BMI, bodymass index; PCI, percutaneous coronary intervention; CABG, coronary-artery bypass grafting; eGFR, estimated glomerular filtration rate; ACE, angiotensin-converting enzyme;ARB, angiotensin receptor blocker.aFive patients (two intervention and three usual care) died before randomization.bData missing for 83 patients.cData missing for 146 patients.dData missing for 154 patients.eData missing for 36 patients.fData missing for 296 patients.gData missing for 302 patients.hData missing for 3 patients.iPercentage of those prescribed an ACE inhibitor, ARB or b-blocker and with the dose recorded.jMedicines on repeat prescription.
R. Lowrie et al.318
by guest on Novem
ber 15, 2014D
ownloaded from

discontinuations and reduction in doses). These differences weresustained during the second year with no evidence of ‘catch-up’prescribing in the usual care group (see Table 3 and Supplementarymaterial online). There was no difference between treatmentgroups regarding dose reduction or discontinuation of thesedrugs. The proportion of patients collecting 80% or moreof prescriptions (from their general practice) was 99% inthe pharmacist intervention group vs. 99% in the usual caregroup for ACE inhibitors, 98 vs. 98% for ARBs, and 98 vs. 99%
for b-blockers (no difference between treatment groups for anydrug).
At the end of year 1, 5.0% of the pharmacist interventiongroup and 4.6% in the usual care group were prescribed analdosterone antagonist. At the end of year 2, the proportionswere 5.1 and 5.2%.
At baseline diltiazem or verapamil was used in 132 (6%) ofpatients, a non-steroidal anti-inflammatory drug in 144 (7%), ananti-depressant in 223 (10%) [a tricyclic in 73 (3%)] and a glitazone
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 2 Changes in key disease-modifying medicines between baseline and the end of the first year of follow-upa
Medical treatment Pharmacist intervention [n (%)] Usual care [n (%)] Odds ratio (95% CI) P-value
ACE inhibitor or ARBa
Startedb 39/131 (30) 27/149 (18) 2.03 (1.14–3.60) 0.02
Increased dosec 129/376 (34) 68/365 (19) 2.32 (1.57–3.44) ,0.001
Increased dose to ≥100% of targetc 86/376 (23) 40/365 (11) 2.46 (1.51–3.99) ,0.001
Started or increased dose 168/507 (33) 95/514 (18) 2.26 (1.64–3.10) ,0.001
b-Blockera
Startedb 50/388 (13) 35/388 (9) 1.56 (0.98–2.47) 0.06
Increased dosec 103/466 (22) 60/467 (13) 1.90 (1.29–2.79) 0.001
Increased dose to ≥100% of targetc 38/466 (8) 22/467 (5) 1.75 (0.99–3.09) 0.05
Started or increased dose 153/854 (18) 95/855 (11) 1.76 (1.31–2.35) ,0.001
aPatients who died (n ¼ 106) or were lost to follow-up (n ¼ 2) during the first year of follow-up were not included in this analysis.bPatients not taking this medicine at baseline.cPatients taking this medicine at baseline (but at ,100% of the target dose) and had dose recorded (number with missing dose: ACE inhibitor ARB n ¼ 1; b-blocker n ¼ 12).
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 3 Use of disease-modifying medicines at the end of the first and the second year of follow-up
Treatment End of year 1 End of year 2
Pharmacistintervention(n 5 1038)a
Usual care(n 5 1018)b
UnadjustedP-value
Pharmacistintervention(n 5 966)c
Usual care(n 5 958)d
UnadjustedP-value
ACE inhibitor
Any dose [n (%e)] 748 (72) 698 (69) 0.15 698 (72) 660 (69) 0.20
≥50% recommended dose [n (%f)] 649 (87) 591 (85) 0.09 595 (85) 524 (79) 0.01
≥100% recommended dose [n (%f)] 496 (66) 429 (61) 0.05 444 (64) 377 (57) 0.02
ACE inhibitor or ARB
Any dose [n (%e)] 884 (85) 842 (83) 0.11 843 (87) 800 (84) 0.03
≥50% recommended dose [n (%f)] 751 (85) 686 (81) 0.03 699 (83) 615 (77) ,0.001
≥100% recommended dose [n (%f)] 538 (61) 466 (55) 0.03 490 (58) 416 (52) 0.02
b-Blocker
Any dose [n (%e)] 660 (64) 625 (61) 0.31 631 (65) 601 (63) 0.24
≥50% recommended dose [n (%f)] 342 (52) 313 (50) 0.28 341 (54) 301 (50) 0.07
≥100% recommended dose [n (%f)] 171 (26) 139 (22) 0.09 169 (27) 135 (22) 0.06
aNumber dead or lost to follow-up year 1, n ¼ 52.bNumber dead or lost to follow-up year 1, n ¼ 56.cNumber dead or lost to follow-up year 2, n ¼ 124.dNumber dead or lost to follow-up year 2, n ¼ 116.ePercentage of individuals in the group available for analysis.fOf all patients prescribed these medicines at the end of the first and the second year.
Pharmacist intervention in primary care to improve outcomes in patients with left ventricular systolic dysfunction 319
by guest on Novem
ber 15, 2014D
ownloaded from

in 17 (1%). These drugs were discontinued more often in thepharmacist intervention group in the first year but the differencein rates of discontinuation between the two treatment groupswere not statistically significant (Supplementary material online).
Study outcomesDeath from any cause or hospital admission for heart failure(the primary outcome) occurred in 390 patients (35.8%) in theintervention group and 380 patients (35.4%) in the usual caregroup (Figure 2 and Table 4). The adjusted hazard ratio (HR) forthe primary outcome in the intervention group, whencompared with the usual care group, was 0.97, 95% CI 0.83–1.14, P ¼ 0.72). The effect of the intervention on this outcome
was consistent in an unadjusted analysis (Table 4) and across allpre-specified subgroups (Figure 3).
Death from any cause or hospital admission for a cardiovascularcause occurred in 487 patients (44.7%) in the intervention groupcompared with 475 patients (44.2%) in the usual care group (HR0.97, 95% CI 0.84–1.12, P ¼ 0.70). A total of 337 patients(30.9%) in the intervention group and 331 patients (30.8%) inthe usual care group died (HR 0.96, 95% CI 0.80–1.16, P ¼0.68). The number of deaths attributed to a non-cardiovascularcause was 155 in the intervention group and 169 in the usualcare group.
The number of patients admitted to hospital for any reason, fora cardiovascular cause, and for heart failure was similar in the twotreatment groups (Table 4). The total numbers of hospital
Figure 2 Main study outcomes.
R. Lowrie et al.320
by guest on Novem
ber 15, 2014D
ownloaded from

admissions (including second and subsequent hospital admissions)for any reason were 2205 vs. 2191 (P ¼ 0.84), for cardiovascularcauses 474 vs. 517 (P ¼ 0.19), and for heart failure 149 vs. 194(P ¼ 0.08), in the intervention group and the usual care group,respectively. Findings for the other pre-specified secondaryoutcomes and safety outcomes are reported in the Supplementarymaterial online.
DiscussionAlthough a meta-analysis of small, short-term studies suggestedthat pharmacist intervention improves clinical outcomes in patientswith heart failure,7 we did not confirm this in a much larger andlonger trial conducted in primary care, despite the intervention
leading to improvements in the use of disease-modifying medica-tions which persisted for at least 2 years.
There are a number of possible explanations for this finding. Thefrequency of use of ACE inhibitors and ARBs at baseline wasgreater than that reported in previous studies in primary care,and even in our pilot study, with 86% of patients prescribed atleast one of these medications.2 –5,21 The explanation for thisunexpected finding is uncertain, although in 2004, the year ourtrial started, the UK government introduced a new contract forfamily doctors linking pay to performance.22,23 Prescribing ofACE inhibitors (but not b-blockers) in patients with left ventricularsystolic dysfunction was one of the incentivized activities. As a con-sequence of the high baseline use of ACE inhibitors and ARBs,there was little scope to initiate these agents. There was alsolimited opportunity to increase the dose of these drugs as a high
Figure 2 Continued.
Pharmacist intervention in primary care to improve outcomes in patients with left ventricular systolic dysfunction 321
by guest on Novem
ber 15, 2014D
ownloaded from

proportion (55%) of subjects was already receiving the recom-mended dose at baseline. Furthermore, the dose was increasedin only about one-third of eligible patients in the interventiongroup (compared with 19% of those in the usual care group), pre-sumably because of tolerability and safety considerations, perhapsindicating that the rate of use and dosing of these drugs may havealready approached a ceiling level. Certainly, the rate of use of ACEinhibitors and ARBs and the doses that they were used at in ourtrial equal or exceed those in recent heart failure trials (despiteour patients being more elderly than in these other trials)24,25
and a national audit in the UK.26
Although there was more scope to improve b-blocker prescrib-ing, initiation of this type of medication and increase in the dose ofb-blocker were infrequent in both treatment groups. This lack ofsuccess may indicate that the brief period of tuition used toprepare the non-specialist pharmacists in our trial was insufficient.Unfamiliarity with the use of b-blockers, and persisting concernsabout their tolerability and safety, in left ventricular systolicdysfunction among family doctors at the time our trial started, aswell as the high prevalence of respiratory disease in our populationmay also have limited b-blocker use. Additionally, patients may alsohave been unwilling to take an additional medication given the highrate of multi-drug regimens in the population studied (47% werereceiving more than eight medications). Nevertheless, althoughthe rate of use of b-blockers was disappointing, the proportionof patients taking 100% or more of the recommended dose ofb-blocker by the end of the first year in the pharmacist interven-tion group (26%) compared favourably with the Systolic Heart
failure treatment with If inhibitor ivabradine Trial (SHIFT) wherethis proportion was 26% at baseline.24
A second explanation for the lack of effect of our interventionwas the relatively low frequency of hospital admission for heartfailure which meant that the majority of events contributing tothe primary composite outcome were fatal. In addition, only halfof the deaths that occurred were attributed to cardiovascularcauses. We excluded high-risk patients under the care of specialistheart failure nurses. Furthermore, falling hospital admission ratesfor heart failure have been reported in several countries15,27– 31
and, recently, cardiovascular deaths, as a proportion of overalldeaths, have also been reported to be declining in patients withheart failure.32 Consequently, there were fewer non-fatal andfatal events which might have been reduced through greater useof ACE inhibitors, ARBs and b-blockers. We believe that thesetwo factors—only a modest improvement in the use of disease-modifying treatment coupled with a low rate of modifiableevents—are the most likely explanation for a lack of improvementin clinical outcomes in our trial.
The low rate of use of aldosterone antagonists in our trial wasdue to the exclusion of more severely ill patients who wereunder the care of the specialist heart failure nurse service andhospital clinics. At the time of our trial, aldosterone antagonistswere only indicated in such patients.1 Clearly, if such a trial wererepeated today, the use of aldosterone antagonists would beencouraged by pharmacists.
Potentially harmful medications, e.g. rate-limiting calcium channelblockers, non-steroidal anti-inflammatory drugs, tricyclic
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 4 Primary and main secondary outcomes
Outcome Pharmacist intervention(n 5 1090)
Usual care (n 5 1074) Adjusted HR(95% CI)
AdjustedP-value
UnadjustedHR (95% CI)
UnadjustedP-value
Patientswith event
Event rate(n/100patient-year)
Patientswith event
Event rate(n/100patient-year)
Primary outcome
Death from any causeor admission for heartfailurea
390 (36%) 8.53 380 (35%) 8.57 0.97 (0.83–1.14) 0.72 0.99 (0.87–1.13) 0.91
Main secondary outcomes
Death from any causeor admission forcardiovascular cause
487 (45%) 11.54 475 (44%) 11.67 0.97 (0.84–1.12) 0.70 0.99 (0.87–1.11) 0.81
Death from any causeor admission for anyreason
758 (70%) 24.93 751 (70%) 25.46 0.96 (0.86–1.07) 0.41 0.97 (0.88–1.07) 0.55
Admissions
Heart failure 107 (10%) 2.34 114 (11%) 2.57 0.88 (0.67–1.16) 0.36 0.90 (0.71–1.14) 0.38
Cardiovascular causes 292 (27%) 6.92 280 (26%) 6.88 0.98 (0.81–1.19) 0.83 0.99 (0.84–1.18) 0.94
Any reason 711 (65%) 23.38 695 (65%) 23.56 0.97 (0.87–1.09) 0.61 0.98 (0.89–1.08) 0.73
Death 337 (31%) 7.10 331 (31%) 7.18 0.96 (0.80–1.16) 0.68 0.99 (0.85–1.16) 0.92
aThe number of events contributing to the primary composite in the intervention group was 283 deaths and 107 admissions for heart failure and in the usual care group 266 deathsand 114 admissions for heart failure.
R. Lowrie et al.322
by guest on Novem
ber 15, 2014D
ownloaded from

antidepressants, oral corticosteroids, and glitazones, wereprescribed in a very small proportion of patients at baseline, andpharmacist intervention did not lead to any greater discontinuationof these medicines, when compared with usual care duringfollow-up.
As explained in the ‘Methods’ section, we had to use a clusterrandomization design. We ensured good internal validity byaccounting for the clustered nature of the data in our samplesize calculations and ensuring blinding to the allocation status ofthose recruiting individuals into the trial and good external validityby providing information on numbers approached, recruited, andlost to follow-up. We therefore followed best practices in relationto this type of trial. Furthermore, although a major limitation of thisdesign is the lack of similarity of the study groups, our treatmentgroups were well matched.12,13
There were several limitations to our trial. The study pharma-cists were not trained to elicit signs and symptoms of heartfailure. We did not collect reasons why patients might have beenineligible for a specific treatment or unable to tolerate it (collectingthis information on the control group might have caused contam-ination). Ejection fraction was not reported to general practi-tioners, and natriuretic peptides measurements were notavailable in primary care at the time our patients were recruited.Although our trial did not achieve its goal of improving clinical
outcomes, it did demonstrate that modest and sustained improve-ments in the prescribing of disease-modifying medications can beachieved by a brief, focused collaborative intervention deliveredby non-specialist pharmacists given only a short period of training.However, the short period of training and brevity of interventionmay also have been limitations of our study. This was particularlytrue in relation to b-blockers where our intervention had a disap-pointingly small effect on the use of these drugs. Lessons for futuretrials may be that more intense training, more patient visits, andselective involvement of hospital specialists might be required tofully optimize treatment. It is also possible that the modificationof other treatments that we did not target, such as diuretics,may have improved the outcome and this could also be examinedin future studies. While this type of intervention may not benefit allpatients, it might improve clinical outcomes if aimed at those inmost need in terms of deficient background treatment or atthose at higher risk of modifiable events. This is a question thatmay be considered in future comparative-effectiveness trials.
ContributorsAll authors except P.S.J. designed the study and oversaw itsconduct. All authors participated in interpretation of the dataand writing of the report.
Figure 3 Subgroup analysis for the primary outcome.
Pharmacist intervention in primary care to improve outcomes in patients with left ventricular systolic dysfunction 323
by guest on Novem
ber 15, 2014D
ownloaded from

Supplementary materialSupplementary material is available at European Heart Journalonline.
AcknowledgementsAll participating general practices in Greater Glasgow and Clyde.Study pharmacists: Fiona Allen, Janet Black, Lorna Brown, SandraCahill, Hilary Campbell, Jan Currie, Colin Dougall, NoreenDownes, Anfrances Duggan, Lynn Duthie, Marie Galloway, AliaGilani, Alison Hair, Heather Harrison, Victoria Hunt, ChrisJohnson, Fiona Lambie, Marjorie McGhie, Pauline McLeod, Mari-Anne McLean, Raj Sabharwal, Shona Shaw, Kirstin Shearer,Sharon Smart, Iain Spierits, Sheila Tennant, Lynn Walker. Primarycare adviser: Des Spence. Pharmacy support: Sarah Darroch,Karen Vint, Alister McLaren, Nicola Watson.
FundingThe primary funder was the NHS in Greater Glasgow and Clyde. Thefunder played no role in data analysis or interpretation, writing of thereport, or the decision to submit for publication. The authors designedthe trial and oversaw its conduct. The report was prepared by allauthors who had unrestricted access to the data and made thedecision to submit for publication.
Conflict of interest: none declared.
References1. Dickstein K, Cohen-Solal A, Filippatos G, McMurray JJV, Ponikowski P,
Poole-Wilson PA, Stromberg A, van Veldhuisen DJ, Atar D, Hoes AW,Keren A, Mebazaa A, Nieminen M, Priori SG, Swedberg K. ESC guidelines forthe diagnosis and treatment of acute and chronic heart failure 2008: the TaskForce for the diagnosis and treatment of acute and chronic heart failure 2008of the European Society of Cardiology. Developed in collaboration with theHeart Failure Association of the ESC (HFA) and endorsed by the EuropeanSociety of Intensive Care Medicine (ESICM). Eur J Heart Fail 2008;10:933–989.
2. Bosch M, Wensing M, Bakx JC, van der Weijden T, Hoes AW, Grol RP. Currenttreatment of chronic heart failure in primary care; still room for improvement.J Eval Clin Pract 2010;16:644–650.
3. Calvert MJ, Shankar A, McManus RJ, Ryan R, Freemantle N. Evaluation of the man-agement of heart failure in primary care. Fam Pract 2009;26:145–153.
4. de Peuter OR, Lip GY, Souverein PC, Klungel OH, de Boer A, Buller HR,Kamphuisen PW. Time-trends in treatment and cardiovascular events in patientswith heart failure: a pharmaco surveillance study. Eur J Heart Fail 2011;13:489–495.
5. Persson H, Erntell H, Eriksson B, Johansson G, Swedberg K, Dahlstrom U.Improved pharmacological therapy of chronic heart failure in primary care: a ran-domised Study of NT-proBNP Guided Management of Heart Failure–SIGNAL-HF (Swedish Intervention study–Guidelines and NT-proBNP AnaLysisin Heart Failure). Eur J Heart Fail 2010;12:1300–1308.
6. Holland R, Desborough J, Goodyer L, Hall S, Wright D, Loke YK. Doespharmacist-led medication review help to reduce hospital admissions anddeaths in older people? A systematic review and meta-analysis. Br J Clin Pharmacol2008;65:303–316.
7. Koshman SL, Charrios TL, Simpson SH, McAlister FA, Tsuyuki RT. Pharmacistcare of patients with heart failure. A review of randomized trials. Arch InternMed 2008;168:687–694.
8. Roughead EE, Barratt JD, Ramsay E, Pratt N, Ryan P, Peck R, Killer G, Gilbert AL.The effectiveness of collaborative medicine reviews in delaying time to next hos-pitalization for patients with heart failure in the practice setting: results of acohort study. Circ Heart Fail 2009;2:424–428.
9. Chisholm-Burns MA, Lee JK, Spivey CA, Slack M, Herrier RN, Hall-Lipsy E,Zivin JG, Abraham I, Palmer J, Martin JR, Kramer SS, Wunz T. US Pharmacists’effect as team members on patient care. Systematic review and meta-analyses.Med Care 2010;48:923–933.
10. Gattis WA, Hasselblad V, Whellan DJ, O’Connor CM. Reduction in heart failureevents by the addition of a clinical pharmacist to the heart failure managementteam. Arch Int Med 1999;159:1939–1945.
11. Lowrie R, Mair FS, Greenlaw N, Forsyth P, McConnachie A, Richardson J, Khan N,Morrison D, Messow CM, Rae B, McMurray JJV. The Heart failure and OptimalOutcomes from Pharmacy Study (HOOPS): rationale, design, and baseline char-acteristics. Eur J Heart Fail 2011;13:917–924.
12. Campbell M, Grimshaw J, Steen N. Sample size calculations for cluster rando-mised trials. Changing Professional Practice in Europe Group (EU BIOMED IIConcerted Action). J Health Serv Res Policy 2000;5:12–16.
13. Campbell MK, Elbourne DR, Altman DG, CONSORT group. CONSORT state-ment: extension to cluster randomised trials. Br Med J 2004;328:702–708.
14. Gilley J. Towards rational prescribing. Br Med J 1994;308:731–732.15. Jhund PS, Macintyre K, Simpson CR, Lewsey JD, Stewart S, Redpath A,
Chalmers JWT, Capewell S, McMurray JJV. Long-term trends in first hospitaliza-tion for heart failure and subsequent survival between 1986 and 2003: a popula-tion study of 5.1 million people. Circulation 2009;119:515–523.
16. Lewsey JD, Gillies M, Jhund PS, Chalmers JWT, Redpath A, Briggs A, Walters M,Langhorne P, Capewell S, McMurray JJV, MacIntyre K. Sex differences in incidencemortality, and survival in individuals with stroke in Scotland, 1986–2005. Stroke2009;40:1038–1043.
17. Computerised record linkage: compared with traditional patient follow-upmethods in clinical trials and illustrated in a prospective epidemiological study.The West of Scotland Coronary Prevention Study Group. J Clin Epidemiol 1995;48:1441–1452.
18. Ford I, Murray H, Packard CJ, Shepherd J, Macfarlane PW, Cobbe SM, West ofScotland Coronary Prevention Study Group. Long-term follow-up of the Westof Scotland Coronary Prevention Study. N Engl J Med 2007;357:1477–1486.
19. Packer M, Poole-Wilson PA, Armstrong PW, Cleland JGF, Horowitz JD, Massie B,Ryden L, Thygesen K, Uretsky BF, on behalf of the ATLAS Study Group.Comparative effects of low and high doses of the angiotensin-convertingenzyme inhibitor, lisinopril, on morbidity and mortality in chronic heart failure.Circulation 1999;100:2312–2318.
20. Bristow MR, Gilbert EM, Abraham WT, Adams KF, Fowler M, Hershberger RE,Spencer K, Nahara KA, Ingersoll H, Kreuger S, Shusterman N. Carvedilolproduces dose-related improvements in left ventricular function and survival insubjects with chronic heart failure. Circulation 1996;94:2807–2816.
21. Spence D, Johnson C, Berry C, Maxwell F, Lowrie R, Blue L. Establishment of adisease register for patients with LVSD in primary care and comparison ofcurrent practice with evidence-based guidelines. Pharm J 2002;268:911–913.
22. Roland M. Linking physicians’ pay to the quality of care–a major experiment in theUnited Kingdom. N Engl J Med 2004;351:1448–1454.
23. Campbell S, Reeves D, Kontopantelis E, Middleton E, Sibbald B, Roland M. Qualityof primary care in England with the introduction of pay for performance. N Engl JMed 2007;357:181.
24. Swedberg K, Komajda M, Bohm M, Borer JS, Ford I, Dubost-Brama A,Lerebours G, Tavazzi L, on behalf of the SHIFT Investigators. Ivabradine and out-comes in chronic heart failure (SHIFT): a randomised placebo-controlled study.Lancet 2010;376:875–885.
25. Moss AJ, Hall WJ, Cannom DS, Klein H, Brown MW, Daubert JP, Estes NA III,Foster E, Greenberg H, Higgins SL, Pfeffer MA, Solomon SD, Wilber D,Zareba W, MADIT-CRT Trial Investigators. Cardiac-resynchronization therapyfor the prevention of heart-failure events. N Engl J Med 2009;361:1329–1338.
26. Cleland JG, McDonagh T, Rigby AS, Yassin A, Whittaker T, Dargie HJ, NationalHeart Failure Audit Team for England and Wales. The national heart failureaudit for England and Wales 2008–2009. Heart 2011;97:876–886.
27. Mosterd A, Reitsma JB, Grobbee DE. Angiotensin converting enzyme inhibitionand hospitalisation rates for heart failure in the Netherlands, 1980–1999: theend of an epidemic? Heart 2002;87:75–76.
28. Levy D, Kenchaiah S, Larson MG, Emelia BJ, Kupka MJ, Kalon KL, Murab M,Vasan RS. Long-term trends in the incidence of and survival with heart failure.N Engl J Med 2002;347:1397–1402.
29. Schaufelberger M, Swedberg K, Koster M, Rosen M, Rosengren A. Decreasingone-year mortality and hospitalization rates for heart failure in Sweden; Datafrom the Swedish Hospital Discharge Registry 1988 to 2000. Eur Heart J 2004;25:300–307.
30. Teng TH, Finn J, Hobbs M, Hung J. Heart failure: incidence, case fatality, and hos-pitalization rates in Western Australia between 1990 and 2005. Circ Heart Fail2010;3:236–243.
31. Ezekowitz JA, Kaul P, Bakal JA, Quan H, McAlister FA. Trends in heart failure care:has the incident diagnosis of heart failure shifted from the hospital to the emer-gency department and outpatient clinics? Eur J Heart Fail 2011;13:142–147.
32. Henkel DM, Redfield MM, Weston SA, Gerber Y, Roger VL. Death in heartfailure: a community perspective. Circ Heart Fail 2008;1:91–97.
R. Lowrie et al.324
by guest on Novem
ber 15, 2014D
ownloaded from