Embed Size (px)
Citation preview
University of Minnesota
College of Pharmacy
Phar 6122 Pharmacotherapy II:
(Cardiology)
Robert J. Straka, Pharm.D. Course Director
Spring 2006

Phar 6122: Pathophysiology and Pharmacotherapy of Cardiovascular Disorders Spring 2006
Revised 01/13/06 Table of Contents and Reading Assignments
January 18t h Orientation and Course Overview Dr. Straka
Course Table of Contents and Readings Assignments .............................................................. 1 Course Information (6122 overview of all three sections) ........................................................ 8 Phar 6122 Course Schedule..................................................................................................... 14 Cardiovascular Section Information........................................................................................ 17 Advice for Exam Taking ......................................................................................................... 21 Helpful Abbreviations ............................................................................................................. 22 Introduction to Phar6122......................................................................................................... 24 Objectives................................................................................................................................ 25 Cardiac Anatomy Lecture........................................................................................................ 26
Suggested
American Heart Association. 2006 Heart and Stroke Statistical Update. (http://www.americanheart.org/downloadable/heart/1136308648540Statupdate2006.pdf)
January 18t h Hypertension I Dr. Straka
Objectives................................................................................................................................ 29 Hypertension Lecture .......................................................................................................... TBA
Required
DiPiro 6th ed. (2005), Chapter 13: Hypertension……….pp 185-217 Suggested
Barkis GL, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (The JNC 7 Report). JAMA. 2003;289:2560-2572. (http://www.nhlbi.nih.gov/guidelines/hypertension/index.htm) (http://www.courses.ahc.umn.edu/pharmacy/5822/JNC_7_Complete_Version_2003.pdf)
January 20t h Hypertension II Dr. Straka Objectives................................................................................................................................ 29 Hypertension Lecture .............................................................................................................. 30-56
January 23r d Hypertension III Dr. Straka
Objectives................................................................................................................................ 29 Hypertension Lecture .......................................................................................................... TBA
January 23r d Hypertension IV Dr. Straka
Objectives................................................................................................................................ 29 Hypertension Lecture .......................................................................................................... TBA
Page 1
Table of Contents 1/13/06
January 25t h Hyperlipidemia: Drug Pathophysiology Dr. Straka Objectives................................................................................................................................ 57 Hyperlipidemia Lecture....................................................................................................... TBA
Quiz 1
Take quiz online through WebCT Vista (http://vista.umn.edu) for the cardiovascular topic of hypertension.
Required Executive Summary of the Third Report of the National Cholesterol Education Program Expert Panel on Detection Evaluation, and Treatment of High Blood Cholesterol in Adults. JAMA 2001: 285(19) 2486-2496. Web access to ATP III guidelines: (http://www.nhlbi.nih.gov/guidelines/cholesterol/atp_iii.htm)
Suggested DiPiro 6th ed. (2005), Chapter 21: Hyperlipidemia……………pp 429-452
January 25t h Hyperlipidemia: Drug Therapy I Dr. Straka
Objectives................................................................................................................................ 57 Hyperlipidemia Lecture....................................................................................................... TBA
January 27t h Hyperlipidemia: Drug Therapy II Dr. Straka
Objectives................................................................................................................................ 57 Hyperlipidemia Lecture ...........................................................................................TBA
January30t h Hyperlipidemia: Drug Therapay III Dr. Straka
Objectives................................................................................................................................ 57 Hyperlipidemia Lecture....................................................................................................... TBA
Appendix A: Web Exercise Due Submit exercise with a stapled PDF abstract printout to cardiovascular TA at end of class on 1/30/06
January 30t h Review and Case Studies for Dr. Straka Hypertension and Hyperlipidemia
Objectives............................................................................................................................ TBA
Quiz 2
Take quiz online through WebCT Vista (http://vista.umn.edu) for the cardiovascular topic of dysipidemia.
February 1s t Coronary Syndromes: Chronic Stable Angina (SA), Dr. Straka Unstable Angina (UA or non-STEMI), and Myocardial Infarction (MI or STEMI) with Pathophysiology Overview
Objectives of Ischemic Heart Disease ..................................................................................... 58 Ischemic Heart Disease Lecture .......................................................................................... TBA
Page 2
Table of Contents 1/13/06
Objectives of Acute Coronary Syndromes .............................................................................. 58 Acute Coronary Syndromes Lecture ................................................................................... TBA Required
DiPiro 6th ed. (2005), Chapter 15: Ischemic Heart Disease…………….pp 261-290 Suggested
1) ACC/AHA 2002 Guideline Update for the Management of Patients with Chronic Stable Angina-Full Text. See the AHA website: (http://www.americanheart.org/presenter.jhtml?identifier=3006769)
2) ACC/AHA Guideline Update 2002 for the Management of Patients With Unstable Angina and Non--ST-Segment Elevation Myocardial Infarction. Access to the summary article at the AHA website: (http://circ.ahajournals.org/cgi/content/full/106/14/1893)
3) AHA/ACC 2004 Guidelines for the Management of Patients with ST-Elevation Myocardial Infraction. Access to the guideline at the AHA website: (http://circ.ahajournals.org/cgi/reprint/110/9/e82)
February 1s t Pharmacotherapy of Chronic Stable Angina (SA) Dr. Straka Part I
Objectives................................................................................................................................ 58 Ischemic Heart Disease and Chronic Stable Angina Lecture .............................................. TBA
February 3r d Cardiovascular Exam #1 Dr. Straka
Examination covers CV material from 1/18 to 1/30
February 6t h Pharmacotherapy of Chronic Stable Angina (SA) Dr. Straka Part II
Objectives................................................................................................................................ 58 Ischemic Heart Disease and Stable Angina Lecture............................................................ TBA
February 6t h Pharmacotherapy of UA/non-STEMI Dr. Gulseth Objectives................................................................................................................................ 59 Unstable Angina/non-STEMI Lecture ................................................................................ TBA Required
DiPiro 6th ed. (2005), Chapter 11: Cardiovascular Testing………………………..pp 149-170 DiPiro 6th ed. (2005), Chapter 16: Acute Coronary Syndromes……………….…..pp 291-319 February 8t h Pharmacotherapy of STEMI Dr. Gulseth
Objectives................................................................................................................................ 59 STEMI Lecture.................................................................................................................... TBA
February 8t h Antithrombotic Therapy in CV: Part I Dr. Gulseth
Objectives................................................................................................................................ 59 Antithrombotic Therapy Lecture......................................................................................... TBA
Page 3
Table of Contents 1/13/06
Suggested
1) CHEST: Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy 2004. Access CV website (http://www.courses.ahc.umn.edu/pharmacy/5822/CHESTACCP2004.html)
2) Guide to Anticoagulant Therapy: Heparin (AHA 2001 Scientific Statement). Access the AHA website (http://circ.ahajournals.org/cgi/content/full/103/24/2994)
3) AHA/ACC Foundation Guide to Warfarin Therapy (AHA 2003 Scientific Statement). Access the AHA website (http://circ.ahajournals.org/cgi/content/full/107/12/1692)
February 10t h Antithrombotic Therapy in CV: Part II Dr. Gulseth
Objectives................................................................................................................................ 59 Antithrombotic Therapy Lecture......................................................................................... TBA
February 13t h Review and Case Studies for Dr. Straka Ischemic Heart Disease
Objectives............................................................................................................................ TBA
Quiz 3
Take quiz online through WebCT Vista (http://vista.umn.edu) for the cardiovascular topics of ACS and Antithrombotic therapy. February 15t h Introduction to Arrhythmias: Dr. Straka Cardiac Conduction System and Rhythm Recognition
Objectives................................................................................................................................ 60 Cardiac Conduction System and Rhythm Recognition ....................................................... TBA
Required DiPiro 6th ed. (2005), Chapter 17: Arrhythmias…………………………….pp 321-356 ACLS Algorithms (will be provided)
February 15t h Guideline for the Management of Dr. Straka Supraventricular Arrhythmias
Objectives................................................................................................................................ 60 Supraventicular Arrhythmia Lecture ................................................................................... TBA
Suggested ACC/AHA/ESC Guidelines for the Management of Patients With Supraventricular Arrhythmias (AHA 2003 Guideline). Access the AHA website: (http://www.americanheart.org/downloadable/heart/1062186010820SVAFullTextGLfinal.pdf)
February 17t h Cardiovascular Exam #2 Dr. Straka Examination covers CV material from 1/18 to 2/13 February 20t h Therapy of Supraventricular Arrhythmias Dr. Ujhelyi
Objectives................................................................................................................................ 60 Supraventicular Arrhythmia Lecture ................................................................................... TBA
Page 4
Table of Contents 1/13/06
February 20t h Therapy of Ventricular Arrhythmias Dr. Ujhelyi
Objectives................................................................................................................................ 60 Supraventicular Arrhythmia Pharmacotherapy Lecture ...................................................... TBA
Quiz 4 Take quiz online through WebCT Vista (http://vista.umn.edu) for the cardiovascular topic of
Antiarrhythmia therapy. February 22n d ACLS Antiarrhythmic Drug Therapy Dr. Chapman
Objectives................................................................................................................................ 60 Therapy of Ventricular Arrhythmias Lecture...................................................................... TBA
February 22n d ACLS:Bradyarrhythmias and Tachyarrhythmias Dr. Chapman
Objectives................................................................................................................................ 60 ACLS Antiarrhythmic Drug Therapy Lecture..................................................................... TBA Algorithms for Cardiac Care ............................................................................................... TBA
Required
DiPiro 6th ed. (2005), Chapter 12: Cardiopulmonary Resuscitation ………pp 171-183
February 24th Overview Pharmacotherapy of Chronic Heart Failure (CHF) I Dr. Straka
Objectives................................................................................................................................ 61 Chronic Heart Failure Lecture............................................................................................. TBA
Required
DiPiro 6th ed. (2005), Chapter 14: Heart Failure………………..pp 219-260
February 27th Pharmacotherapy of Chronic Heart Failure (CHF) II Dr. Parra
Objectives................................................................................................................................ 61 Chronic Heart Failure Lecture............................................................................................. TBA
Suggested
AHA/ACC 2005 Guidelines for the Evaluation and Management of Chronic Heart Failure in the Adult. Access guideline at the AHA website (http://circ.ahajournals.org/cgi/reprint/112/12/e154)
February 27th Pharmacotherapy of Chronic Heart Failure (CHF) III Dr. Parra
Objectives................................................................................................................................ 61 Chronic Heart Failure Lecture............................................................................................. TBA
March 1st Treatment of the Patient with Acute Heart Failure I Dr. Chapman
Objectives................................................................................................................................ 62 Acute Heart Failure Lecture ................................................................................................ TBA
Appendix A: Web Exercise Due Submit 2 page review with a stapled PDF article printout to cardiovascular TA at end of class on 3/1/06
Page 5
Table of Contents 1/13/06
March 1st Treatment of the Patient with Acute Heart Failure II Dr. Chapman
Objectives................................................................................................................................ 62 Acute Heart Failure Lecture ................................................................................................ TBA
March 3rd Chronic Heart Failure Case Dr. Straka
Objectives............................................................................................................................ TBA March 6th Heart Failure Case Discussions Dr. Straka
Objectives............................................................................................................................ TBA
Quiz 5 Take quiz online through WebCT Vista (http://vista.umn.edu) for the cardiovascular topic of Heart
Failure therapy. March 8th Cardiovascular Advanced Topics I: Dr. Straka Lipids (Dr. Straka) TBA
Objectives............................................................................................................................ TBA
March 8th Pathophysiology and Drug Therapy of PE/DVT Dr. Gulseth
Objectives................................................................................................................................ 63 PE/DVT Lecture.................................................................................................................. TBA
Required DiPiro 6th ed. (2005), Chapter 19: Venous Thromboembolism……………pp 373-413
Suggested CHEST: Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy 2004. Access CV website (http://www.courses.ahc.umn.edu/pharmacy/5822/CHESTACCP2004.html)
Quiz 6
Take quiz online through WebCT Vista (http://vista.umn.edu) for the cardiovascular topics of Acute-HF/PE/DVT therapy.
March 10th Cardiovascular Exam #3 Dr. Straka Examination covers CV material from 1/18 to 3/8 April 21st CV/GI/Endo Oral Exam All
Twin Cities Prep Room ...................................................................................................... IERC Twin Cities Exam Rooms................................................................................................... IERC Duluth Prep Room............................................................................................................... TBA Duluth Exam Rooms ........................................................................................................... TBA
Page 6
Table of Contents 1/13/06
April 28th Pharmacy Day
No Class
May 8th-13th Phar 6122 Comprehensive Final Written Exam 3 hours
Exam Room......................................................................................................................... TBA Comprehensive Examination covers Cardiovascular/GI/Endocrine material from 1/18 to 5/5 Appendix A: Web Exercise
Exam Room............................................................................................................................. 65 Submit exercise with a stapled PDF abstract printout to cardiovascular TA at end of class on 1/30/06
Page 7
Phar 6122: Pharmacotherapy II (5 Credits) Pathophysiology and Pharmacotherapy of Cardiovascular Disorders Pathophysiology and Pharmacotherapy of Endocrine Disorders Pathophysiology and Pharmacotherapy of Gastrointestinal Disorders
Spring 2006
Course Outline 1/13/06
Overall Course Director: Robert J. Straka, Pharm.D., F.C.C.P.
Associate Professor, Clinical Pharmacist University of Minnesota 7-109 Weaver-Densford Hall Phone (612) 624-5663 Fax (612) 625-3927 E-mail: [email protected] Web Page: http://www.courses.ahc.umn.edu/pharmacy/5822/homepage1.html
Cardiovascular Section:
Course (6122) and Section (Cardiovascular) Director: Course Faculty, continued: Robert J. Straka, Pharm.D., F.C.C.P. Associate Professor University of Minnesota, WDH 7-109 Phone (612) 624-5663 Digital pager (651) 629-0163 Fax (612) 625-3927 E-mail: [email protected]
Michael Gulseth, Pharm.D., BCPS Department of Pharmacy Practice and Pharmaceutical Sciences Assistant Professor 2530 Peace Dr. Duluth, MN 55811 U of MN-Duluth Campus Phone: 218-726-6012 Fax: 218-726-6500 Email: [email protected]
R. Todd Burkhardt, Pharm.D. Teaching Assistant: Research Fellow, Cardiovascular Pharmacotherapy 7-189 WDH 308 Harvard St. SE. Minneapolis, MN 55455 Phone: 612-624-6489 Fax: 612-625-3927 Email: [email protected]
Scott Chapman, Pharm.D. Assistant Professor, College of Pharmacy Clinical Specialist, Critical Care and Cardiology Department of Pharmacy North Memorial Medical Center 3300 Oakdale Avenue N. Robinnsdale, MN 55422 Phone :763-520-3961 Email : [email protected]
David Parra, Pharm.D, BCPS Adjunct Assistant Professor, University of Minnesota, ECP Dept. and Clinical Pharmacy Specialist in Cardiology Department of Cardiology Veterans Affairs Medical Center 7305 N. Military Trail West Palm Beach, FL 33410-6400 Email: [email protected]
Michael R. Ujhelyi, Pharm.D. Senior Principal Scientist Cardiac Rhythm Management Research Medtronic Inc. Phone: (763) 514-3674 E-mail: [email protected]
Page 8
Endocrine Section: Section Director: Course Faculty, continued: Thomas E. Lackner, Pharm.D., CGP, FASCP Professor College of Pharmacy, University of Minnesota Phone: (612) 626-4135 Fax: (612) 625-3927 E-mail: [email protected]
Sarah M. Westberg, Pharm.D., BCPS Department of Pharmacy Practice and Pharmaceutical Sciences Assistant Professor 356 Kirby Plaza 1208 Kirby Drive Duluth, MN 55812 Phone: 218-726-6005 Email: [email protected]
Teaching Assistant: Ying-Chi “Alice” Lin, M.S. ECP Graduate Student 7-192 WDH Phone: (612) 624-9683 Email: [email protected]
Teaching Assistant: Varun Goel ECP Graduate Student 7-101 WDH Phone: (612) 624-6932 Email: [email protected]
Gastrointestinal Section: Section Director: Course Faculty, continued: David Guay, Pharm.D., FCP, FASCP, FCCP, CGP Professor College of Pharmacy, University of Minnesota Phone: (612) 626-5981 Fax: (612) 626-6095 E-mail: [email protected]
Randy Seifert Pharm.D. Department of Pharmacy Practice and Pharmaceutical Sciences Professor 366 Kirby Plaza 1208 Kirby Drive Duluth, MN 55812 Phone: (218) 726-6032 Email: [email protected]
Teaching Assistant: Manisha Lamba ECP Graduate Student Phone: (612) 626-2593 Email: [email protected]
All sections Duluth campus: Teaching Assistant Adam Pavek Pharm.D. Student Duluth, MN 55812 Phone: (218) 343-3637 E-mail: [email protected]
Learning Objectives: I. Cardiovascular Course Objectives: At the conclusion of the section, learners should be able to… 1. Demonstrate a clear understanding of the basic pathophysiology associated with common cardiovascular diseases and
syndromes. 2. Contrast and compare available pharmacotherapeutic options to manage patients with one or more common
cardiovascular disorders. 3. Apply their knowledge of pharmacotherapy to design, initiate, modify and evaluate pharmacotherapeutic plans for
specific patients with such conditions. 4. Be able to counsel patients receiving cardiovascular medications on their appropriate use. In order to consider this course a success you must be able to answer the following questions regarding the common medications used in a patient with cardiovascular disease: 1. Is this the optimal drug? 2. Is this the optimal dose? 3. What will I monitor for efficacy? 4. What will I monitor for toxicity? 5. Are there any significant drug interactions or adverse effects associated with this drug? 6. What are the alternatives and their benefits/risks/cost etc? 7. What is the overall goal of my therapeutic plan? 8. What is the evidence supporting the choice of drug therapy in my plan?
Page 9
II. Endocrine Course Objectives: At the conclusion of the section, learners should be able to… 1. Demonstrate a clear understanding of the basic pathophysiology associated with common Endocrine conditions. 2. Contrast and compare available pharmacotherapeutic options to manage patients with one or more common
Endocrine disorders. 3. Apply their knowledge of pharmacotherapy to design, initiate, modify and evaluate pharmacotherapeutic plans for
specific patients with such conditions. 4. Be able to counsel patients receiving agents commonly used to manage their Endocrine conditions. III. Gastrointestinal Course Objectives: At the conclusion of the section, learners should be able to… 1. Demonstrate a clear understanding of the basic pathophysiology associated with common Gastrointestinal
conditions. 2. Contrast and compare available pharmacotherapeutic options to manage patients with one or more common
Gastrointestinal disorders. 3. Apply their knowledge of pharmacotherapy to design, initiate, modify and evaluate pharmacotherapeutic plans for
specific patients with such conditions. 4. Be able to counsel patients receiving agents commonly used to manage their Gastrointestinal conditions. Required Texts The required readings for the course will be outlined in the final syllabus and include chapters from "Pharmacotherapy: A Pathophysiologic Approach", 6th edition, DiPiro et al (eds)., McGraw-Hill, New York, NY and selected cases from “Student’s Guide For Pharmacotherapy”, 6th Edition, 2005, Ed. Schwinghammer TL (McGraw Hill). Textbook chapters are assigned and listed in the Objectives and Readings sections. Students are strongly urged to read the assigned readings prior to class to aid in the understanding of lecture material. Questions from the required readings may be included in course examinations (in addition to lecture and handout material). Supplemental readings will be made available to interested students by arrangements with the course directors. Such readings may be valuable for future reference. Additional References and Course Web Addresses for lecture material may be found at the following: Cardiovascular Section: http://www.courses.ahc.umn.edu/pharmacy/5822/homepage1.html GI Section: http://www.courses.ahc.umn.edu/pharmacy/5880/ Endocrine Section: No website. In addition to the required readings, the Table of Contents provides a listing of suggested readings designed to supplement and enhance the student’s understanding of the course content. 1. Lexi-Complete™ available at: http://www.lexi.com/web/index.jsp . This PDA reference is a portable source for
general information and drug dosing. 2. Goodman and Gilman’s. The Pharmacologic Basis of Therapeutics, 10th Ed., McGraw-Hill, New York, NY, 2001.
This is a good source for information on basic pharmacology. Other Good Sources of Information Students are encouraged to utilize new and progressive methods of obtaining the latest and most up to date information. Specifically, there are numerous sources of information available on the Internet. As always, information on the Internet or sources other than material covered in the lectures and required readings should be viewed as supplementary material and not a primary source. The accuracy of information you may find on the Internet can rarely be ensured and should be viewed as supplementary to what is presented in class.
Page 10
Prerequisites: All students will have completed Anatomy and Physiology (Phar 6061), Medicinal Agents I (Phar 6154), Pharmacokinetics (Phar 6163), Pharmacology I (Phar 5101) and Pharmacotherapy I (Phar 6121), The student is responsible for this material to the extent that basic information taught in such classes will be built upon in this course. Thus, students are encouraged to review basic cardiovascular, endocrine, and gastrointestinal anatomy and physiology and specifically encouraged to review the section of Goodman and Gilman’s Pharmacological Basis of Therapeutics relevant to the classes of drugs covered. Instructors may briefly review this material but are not required to do so.
Student Evaluation and Grading
Phar 6122 Overall Course Grade: The overall 6122 course grade will be determined by the results of 5 quizzes (all within the CV pharmacotherapy section), 7 written exams (3 exclusively CV, 2 exclusively Endo, 2 exclusively GI), 1 Final comprehensive and combined written exam (CV, Endo and GI) and 1 comprehensive and combined Oral exam also covering CV, Endo, and GI sections. Exams will not be graded on a curve. The use of electronic devices such as Palm, other PDA’s, pocket computers, programmable calculators, and other devices with electronic data bases is not permitted during quizzes, written and oral exams unless specified by course or section director. Within each section, exams will be comprehensive and build on previous knowledge covered in each section. The final grade for the Phar6122 course will be determined according to a formula. The overall course grade will be determined from contributions from each of the three sections. The following is provided to guide you in the relative contributions of each section to the evaluation tools. Contribution (evaluation tool) Point (%) contribution from each section
and evaluation tool Minimum Passing Grade
CV section (3 exams, 5 quizzes) 38 > 60%* GI Section (two exams) (9+9)=18 > 60%* Endo Section (two exams) (7+7)=14 > 60%*
CV + GI +Endo 38+18+14= 70 Oral exam (CV, Endo, and GI**) 10
CV + GI + Endo + Oral exam 70+10= 80 6122 Final Written Exam (CV, Endo, and GI)*** 20 > 65% Final Grade 80+20 100 > 60% *Minimum passing grade refers to the indicated evaluation tools for each section **The oral exam accounts for 10% of the overall course grade. The oral exam will integrate and evaluate the application of knowledge gained from each of the three sections according to their approximate contributions to the lecture hours in the course at the time of the oral exam (55% cardiovascular, 25% GI, and 20% endocrinology). ***A comprehensive final exam for all three sections will contribute 20% toward the overall course grade. Approximate contributions of each section for this exam will be 40% GI, 40% endocrine and 20% CV. NOTE: In order to pass this course (Phar 6122), each student must pass the final written examination with a grade of 65% or higher. In addition, each student must earn an overall grade of 60% or higher for the indicated evaluation tools (see * in table above). (There will be no exceptions to this rule). Failure will require the student to re-take the entire course (all three sections). The exams will be returned and reviewed at some point either during or outside of class time. This will be your only chance to comprehensively review your exam. If you have extenuating circumstances, you may schedule an appointment with the section director (or the TAs , at the section director’s discretion) to review any of your exams. Grades will NOT be given out over the telephone. For Pharmacotherapy II (Phar 6122), there will be no make-up quizzes. We will, however, drop the lowest quiz score and provide one additional optional mechanism to discount one other quiz grade. (see optional writing assignment below)
Page 11
Letter Grade assignments appearing on your transcripts are as follows. Common rounding rules will be applied to the final grade (as per Microsoft Excel® where 0.5 and higher values are rounded up).
A ≥ 93% A- 90-92% B+ 87-89% B 83-86% B- 80-82% C+ 77-79% C 73-76% C- 70-72% D+ 67-69% D 60-66% F < 60%
Make up Policy: Please note MAKE-UP EXAMINATIONS, QUIZZES AND OTHER ASSIGNMENTS WILL NOT BE OFFERED EXCEPT UNDER THE FOLLOWING CIRCUMSTANCES: illness, verified by a note from a licensed professional; a family emergency, verified by a note from the professional person in attendance; or a University-sponsored event, verified by a note from the leader of the sponsoring organization. Additional circumstances will be considered at the discretion of the course or section director. If a student is unable to attend the scheduled exam, the relevant section director must be notified (by email and phone) at least 24 hours in advance of the exam time (where possible). If you do not receive a reply to your request prior to the examination time, please do NOT assume that your request has been granted; contact us again to confirm your request was received and processed. If an acceptable circumstance or adequate documentation is not provided, a grade of zero, on the exam, quiz etc. will be assigned by the course or section director. Unless there are extenuating circumstances, students must contact the section or course director within 24 hours of the missed scheduled exam, quiz or other assignment in order to be considered for a make up assessment. Unless there are extenuating circumstances, the make up exam date is generally not more than one week after the original exam date. Workload Expectations: The University of Minnesota defines one credit as equivalent to an average of three hours of learning effort per week (over a full semester) necessary for an average student to achieve an average grade in the course. For example, a student taking a three credit course that meets for three hours a week should expect to spend an additional six hours a week on coursework outside the classroom. You will get the most out of this course by actively participating in the assigned readings, pedagogical tools (quizzes, oral and written exams, review sessions, assignments etc.). Disability Accommodations: Any student with a documented disability (eg. physical, learning, psychiatric, vision, hearing, etc.) who needs to arrange reasonable accommodations must contact the course directors as well as each section director for the course. Documentation of the need for accommodations should be received within the first week of the course and at least 7 days before any exam or test. It is assumed that Disability Services (TC: http://ds.umn.edu/, 612-626-1333, Duluth: Access Center, http://www.d.umn.edu/access/ , 218-726-8217) has been contacted to document the disability and quantify the necessary accommodations before the beginning of the Semester. All discussions concerning this issue will remain confidential. Class Etiquette: The instructors expect all students to conduct themselves in a professional manner consistent with the University of Minnesota Pharmacy Student Code of Ethical Responsibility and Professional Behavior. Students will not engage in disruptive classroom conduct. This refers to behavior that substantially or repeatedly interrupts either the instructor's ability to teach or student learning. The classroom extends to any setting where a student is engaged in work toward academic credit or satisfaction of program-based requirements or related activities. Honor Code: Each student is bound by the following specific provisions as part of the honor code: Academic misconduct is any unauthorized act which may give a student an unfair advantage over other students, including but not limited to: falsification, plagiarism, misuse of test materials, receiving unauthorized assistance and giving unauthorized assistance. Specifically, each student will be required to do their own work on all quizzes (on line or written), tests, oral and written exams.
Page 12
Exam Dates: The instructors do not foresee any circumstances that would require a change in examination dates for the class as a whole. Course/Instructor Evaluation: Students will be given class-time to complete a written course evaluation to be completed near the conclusion of each section of this course. Section Director Office Hours: Dr. Straka will be available by appointment at the University (WDH 7-109). Students are encouraged to seek additional help early if needed. To facilitate this, Dr. Straka will have an ITV room booked every Wednesday from 0900-10:00 (Room 7-115F) for a walk in visit at any time throughout the cycle for the CV section. Other course faculty will be available on an appointment basis. Call (612) 624-5663 or email [email protected] for appointments with the course director and call the numbers listed for appointments with other course faculty (see Course Faculty listing). The TAs will have office hours posted on the CV website (http://www.courses.ahc.umn.edu/pharmacy/5822/CV_TA.html). Dr. Lackner (Section Director for Endocrinology) is available by appointment to meet with students on campus on Tuesdays and Fridays. Office hours can be scheduled with Dr. Lackner by appointment (612) 626-4135 or email [email protected]. Dr. Lackner is also available after lectures to answer individual and group questions and to meet with course liaisons. Dr. Guay (Section Director for Gastroenterology) is available to meet with students on campus by appointment Monday through Friday. Office hours can be scheduled with Dr. Guay on an appointment basis (call (612) 626-5981 or email [email protected]). Dr. Guay will be present at all lectures to answer individual and group questions and to meet with course liaisons. If desired, Dr. Guay will meet with students after each lecture.
Page 13
Phar 6122: Pharmacotherapy II Pathophysiology and Pharmacotherapy of Cardiovascular Disorders
Pathophysiology and Pharmacotherapy of Endocrine Disorders Pathophysiology and Pharmacotherapy of Gastrointestinal Disorders
Spring 2006
5 Credits COURSE SCHEDULE
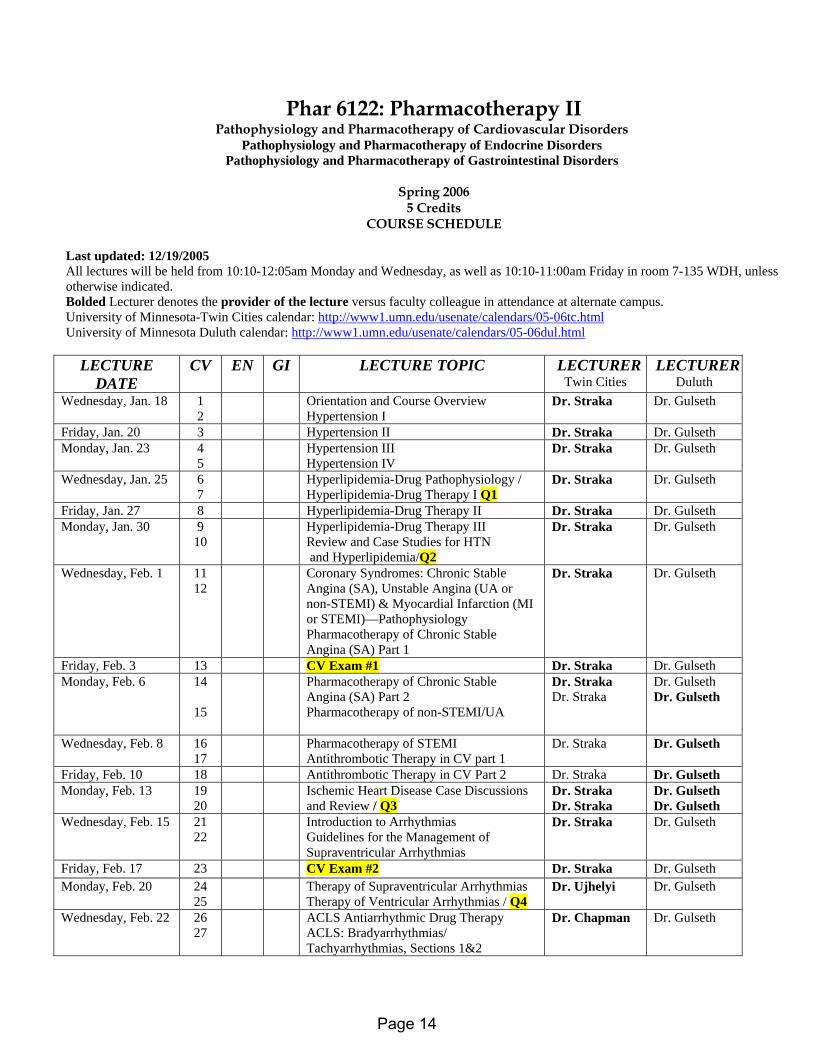
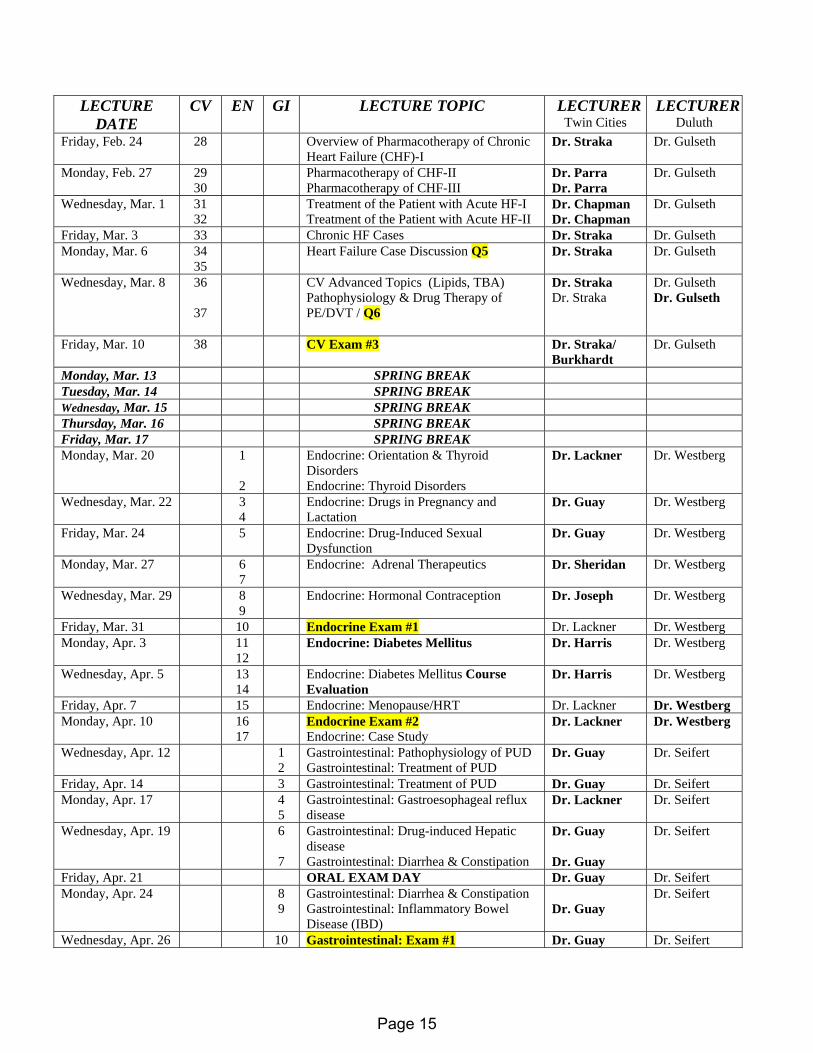
Last updated: 12/19/2005 All lectures will be held from 10:10-12:05am Monday and Wednesday, as well as 10:10-11:00am Friday in room 7-135 WDH, unless otherwise indicated. Bolded Lecturer denotes the provider of the lecture versus faculty colleague in attendance at alternate campus. University of Minnesota-Twin Cities calendar: http://www1.umn.edu/usenate/calendars/05-06tc.html University of Minnesota Duluth calendar: http://www1.umn.edu/usenate/calendars/05-06dul.html
LECTURE DATE
CV EN GI LECTURE TOPIC LECTURER Twin Cities
LECTURERDuluth
Wednesday, Jan. 18 1 2
Orientation and Course Overview Hypertension I
Dr. Straka Dr. Gulseth
Friday, Jan. 20 3 Hypertension II Dr. Straka Dr. Gulseth Monday, Jan. 23 4
5 Hypertension III
Hypertension IV Dr. Straka
Dr. Gulseth
Wednesday, Jan. 25 6 7
Hyperlipidemia-Drug Pathophysiology / Hyperlipidemia-Drug Therapy I Q1
Dr. Straka Dr. Gulseth
Friday, Jan. 27 8 Hyperlipidemia-Drug Therapy II Dr. Straka Dr. Gulseth Monday, Jan. 30 9
10 Hyperlipidemia-Drug Therapy III
Review and Case Studies for HTN and Hyperlipidemia/Q2
Dr. Straka Dr. Gulseth
Wednesday, Feb. 1 11 12
Coronary Syndromes: Chronic Stable Angina (SA), Unstable Angina (UA or non-STEMI) & Myocardial Infarction (MI or STEMI)—Pathophysiology Pharmacotherapy of Chronic Stable Angina (SA) Part 1
Dr. Straka Dr. Gulseth
Friday, Feb. 3 13 CV Exam #1 Dr. Straka Dr. Gulseth Monday, Feb. 6 14
15
Pharmacotherapy of Chronic Stable Angina (SA) Part 2 Pharmacotherapy of non-STEMI/UA
Dr. Straka Dr. Straka
Dr. Gulseth Dr. Gulseth
Wednesday, Feb. 8 16 17
Pharmacotherapy of STEMI Antithrombotic Therapy in CV part 1
Dr. Straka Dr. Gulseth
Friday, Feb. 10 18 Antithrombotic Therapy in CV Part 2 Dr. Straka Dr. Gulseth Monday, Feb. 13 19
20 Ischemic Heart Disease Case Discussions
and Review / Q3 Dr. Straka Dr. Straka
Dr. Gulseth Dr. Gulseth
Wednesday, Feb. 15 21 22
Introduction to Arrhythmias Guidelines for the Management of Supraventricular Arrhythmias
Dr. Straka Dr. Gulseth
Friday, Feb. 17 23 CV Exam #2 Dr. Straka Dr. Gulseth Monday, Feb. 20 24
25 Therapy of Supraventricular Arrhythmias
Therapy of Ventricular Arrhythmias / Q4 Dr. Ujhelyi Dr. Gulseth
Wednesday, Feb. 22 26 27
ACLS Antiarrhythmic Drug Therapy ACLS: Bradyarrhythmias/ Tachyarrhythmias, Sections 1&2
Dr. Chapman Dr. Gulseth
Page 14
LECTURE DATE
CV EN GI LECTURE TOPIC LECTURER Twin Cities
LECTURERDuluth
Friday, Feb. 24 28 Overview of Pharmacotherapy of Chronic Heart Failure (CHF)-I
Dr. Straka Dr. Gulseth
Monday, Feb. 27 29 30
Pharmacotherapy of CHF-II Pharmacotherapy of CHF-III
Dr. Parra Dr. Parra
Dr. Gulseth
Wednesday, Mar. 1 31 32
Treatment of the Patient with Acute HF-I Treatment of the Patient with Acute HF-II
Dr. Chapman Dr. Chapman
Dr. Gulseth
Friday, Mar. 3 33 Chronic HF Cases Dr. Straka Dr. Gulseth Monday, Mar. 6 34
35 Heart Failure Case Discussion Q5 Dr. Straka Dr. Gulseth
Wednesday, Mar. 8 36
37
CV Advanced Topics (Lipids, TBA) Pathophysiology & Drug Therapy of PE/DVT / Q6
Dr. Straka Dr. Straka
Dr. Gulseth Dr. Gulseth
Friday, Mar. 10 38 CV Exam #3 Dr. Straka/ Burkhardt
Dr. Gulseth
Monday, Mar. 13 SPRING BREAK Tuesday, Mar. 14 SPRING BREAK Wednesday, Mar. 15 SPRING BREAK Thursday, Mar. 16 SPRING BREAK Friday, Mar. 17 SPRING BREAK Monday, Mar. 20 1
2
Endocrine: Orientation & Thyroid Disorders Endocrine: Thyroid Disorders
Dr. Lackner Dr. Westberg
Wednesday, Mar. 22 3 4
Endocrine: Drugs in Pregnancy and Lactation
Dr. Guay Dr. Westberg
Friday, Mar. 24 5 Endocrine: Drug-Induced Sexual Dysfunction
Dr. Guay Dr. Westberg
Monday, Mar. 27 6 7
Endocrine: Adrenal Therapeutics
Dr. Sheridan
Dr. Westberg
Wednesday, Mar. 29 8 9
Endocrine: Hormonal Contraception Dr. Joseph Dr. Westberg
Friday, Mar. 31 10 Endocrine Exam #1 Dr. Lackner Dr. Westberg Monday, Apr. 3 11
12 Endocrine: Diabetes Mellitus
Dr. Harris Dr. Westberg
Wednesday, Apr. 5 13 14
Endocrine: Diabetes Mellitus Course Evaluation
Dr. Harris Dr. Westberg
Friday, Apr. 7 15 Endocrine: Menopause/HRT Dr. Lackner Dr. Westberg Monday, Apr. 10 16
17 Endocrine Exam #2
Endocrine: Case Study Dr. Lackner Dr. Westberg
Wednesday, Apr. 12 1 2
Gastrointestinal: Pathophysiology of PUD Gastrointestinal: Treatment of PUD
Dr. Guay
Dr. Seifert
Friday, Apr. 14 3 Gastrointestinal: Treatment of PUD Dr. Guay Dr. Seifert Monday, Apr. 17 4
5 Gastrointestinal: Gastroesophageal reflux disease
Dr. Lackner
Dr. Seifert
Wednesday, Apr. 19 6
7
Gastrointestinal: Drug-induced Hepatic disease Gastrointestinal: Diarrhea & Constipation
Dr. Guay Dr. Guay
Dr. Seifert
Friday, Apr. 21 ORAL EXAM DAY Dr. Guay Dr. Seifert Monday, Apr. 24 8
9 Gastrointestinal: Diarrhea & Constipation Gastrointestinal: Inflammatory Bowel Disease (IBD)
Dr. Guay
Dr. Seifert
Wednesday, Apr. 26 10 Gastrointestinal: Exam #1 Dr. Guay Dr. Seifert
Page 15
LECTURE DATE
CV EN GI LECTURE TOPIC LECTURER Twin Cities
LECTURERDuluth
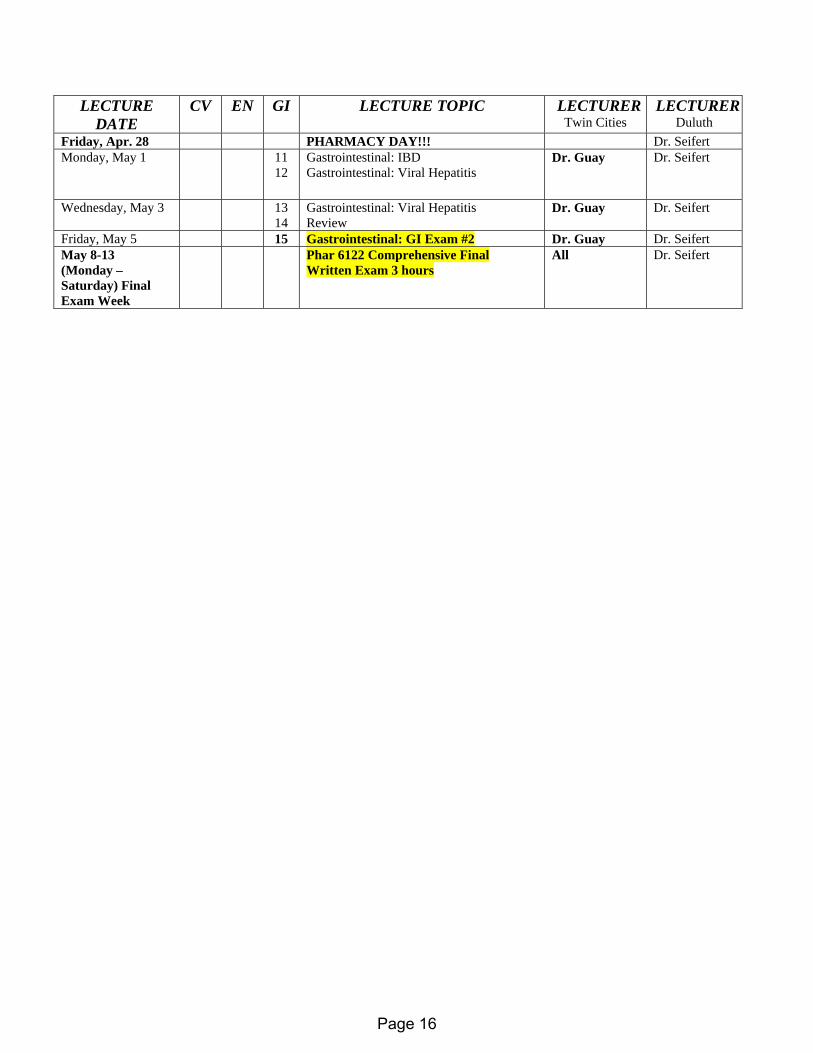
Friday, Apr. 28 PHARMACY DAY!!! Dr. Seifert Monday, May 1 11
12 Gastrointestinal: IBD Gastrointestinal: Viral Hepatitis
Dr. Guay Dr. Seifert
Wednesday, May 3 13 14
Gastrointestinal: Viral Hepatitis Review
Dr. Guay Dr. Seifert
Friday, May 5 15 Gastrointestinal: GI Exam #2 Dr. Guay Dr. Seifert May 8-13 (Monday – Saturday) Final Exam Week
Phar 6122 Comprehensive Final Written Exam 3 hours
All Dr. Seifert
Page 16
Course Info. Revised: 01/12/06
Phar 6122: Pharmacotherapy II Cardiovascular Section Course Information
Spring 2006 Course Overview and Goals What is the importance of this class and what is expected of the student who completes this course? Cardiovascular pharmacotherapy is one of the most exciting areas of medical care. Each one of us will have some degree of personal experience with cardiovascular disease in our lifetime. New and innovative approaches for treating cardiovascular diseases are constantly being evaluated. As a pharmacist, you can have a major impact on the care of patients with cardiovascular disease through your development of an understanding of the appropriate use of drugs for such patients. The objectives of this course should provide the basis for a pharmacist to care for a patient with common cardiovascular diseases. Required texts (see Course Outline) Other Good Sources of Information Students are encouraged to utilize new and progressive methods of obtaining the latest and most up to date information. Specifically, there are numerous sources of information available on the Internet. As always, information on the Internet or sources other than material covered in the lectures and required readings should be viewed as supplementary material and not a primary source. However, the accuracy of information you may find on the Internet cannot always be verified. The following sources of information may be useful in further exploring areas of interest or in obtaining information that may be useful in completing group projects. Below are several Web sites that provide excellent information or will at least guide you in the right direction.
1.Homepage for Phar 6122: Pathophysiology and Pharmacotherapy of Cardiovascular Disorders. (http://www.courses.ahc.umn.edu/pharmacy/5822/homepage1.html)
This site contains general course information, course-related news and announcements, and other interesting links.
2. Theheart.org (http://www.theheart.org/index.cfm) outstanding source of new info re: to Cardiovascular Pharmacotherapy. You may register for free and receive updates via email on news or just search the site as needed.
3.Pharmacy Web Page (http://www.pharmweb.net/) This site provides information for pharmaceutical and other health-related organizations, including a schedule of future conferences and discussion groups.
4.Medicine Online (http://www.mol.net/medj.htm) or (http://www.mol.net/) Here you will have access to information such as the table of contents of the most recent publications of many medical journals.
5.Pharminfonet (http://www.pharminfo.com)This site is a source for several types of pharmaceutical information, and within this site is the cardiovascular disease resources at (http://www.pharminfo.com/disease/cardio/card_rsc.html).
6.Virtual Hospital (http://www.vh.org/)This is the University of Iowa’s virtual hospital. Here you can find examples of cardiovascular-related cases.
7. OnHealth (http://onhealth.com/ch1/condctr/cardio/item,14121.asp) This site is geared towards general public but it provides nicely detailed information about prevention, diagnosis and
Page 17
Course Info. Revised: 01/12/06
treatment of cardiovascular diseases. It is very useful for description of variety of cardiac procedures.
8. American Heart Association (http://www.americanheart.org/) This site is very useful for accessing various Guidelines to manage patients with heart disease, retrieve updated official statistics re: Cardiovascular disease, obtain official AHA statements on selected topics of CV importance etc.
9. Lexi.com (http://www.lexi.com/web/index.jsp) 10. Micromedex (http://www.biomed.lib.umn.edu/micromedex/index.html) This site can be used to
search for summaries and detailed monographs of drugs, alternative medicine, toxicological management, reproductive risks, and acute/emergency care.
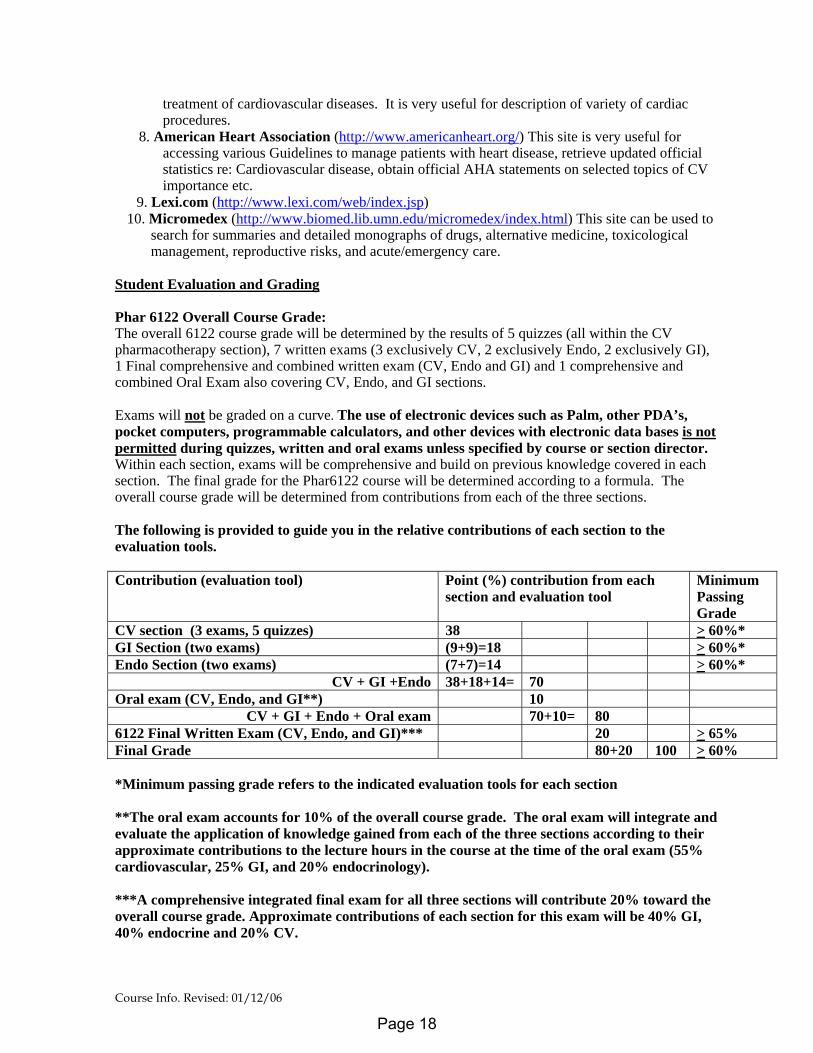
Student Evaluation and Grading Phar 6122 Overall Course Grade: The overall 6122 course grade will be determined by the results of 5 quizzes (all within the CV pharmacotherapy section), 7 written exams (3 exclusively CV, 2 exclusively Endo, 2 exclusively GI), 1 Final comprehensive and combined written exam (CV, Endo and GI) and 1 comprehensive and combined Oral Exam also covering CV, Endo, and GI sections. Exams will not be graded on a curve. The use of electronic devices such as Palm, other PDA’s, pocket computers, programmable calculators, and other devices with electronic data bases is not permitted during quizzes, written and oral exams unless specified by course or section director. Within each section, exams will be comprehensive and build on previous knowledge covered in each section. The final grade for the Phar6122 course will be determined according to a formula. The overall course grade will be determined from contributions from each of the three sections. The following is provided to guide you in the relative contributions of each section to the evaluation tools. Contribution (evaluation tool) Point (%) contribution from each
section and evaluation tool Minimum Passing Grade
CV section (3 exams, 5 quizzes) 38 > 60%* GI Section (two exams) (9+9)=18 > 60%* Endo Section (two exams) (7+7)=14 > 60%*
CV + GI +Endo 38+18+14= 70 Oral exam (CV, Endo, and GI**) 10
CV + GI + Endo + Oral exam 70+10= 80 6122 Final Written Exam (CV, Endo, and GI)*** 20 > 65% Final Grade 80+20 100 > 60% *Minimum passing grade refers to the indicated evaluation tools for each section **The oral exam accounts for 10% of the overall course grade. The oral exam will integrate and evaluate the application of knowledge gained from each of the three sections according to their approximate contributions to the lecture hours in the course at the time of the oral exam (55% cardiovascular, 25% GI, and 20% endocrinology). ***A comprehensive integrated final exam for all three sections will contribute 20% toward the overall course grade. Approximate contributions of each section for this exam will be 40% GI, 40% endocrine and 20% CV.
Page 18
Course Info. Revised: 01/12/06
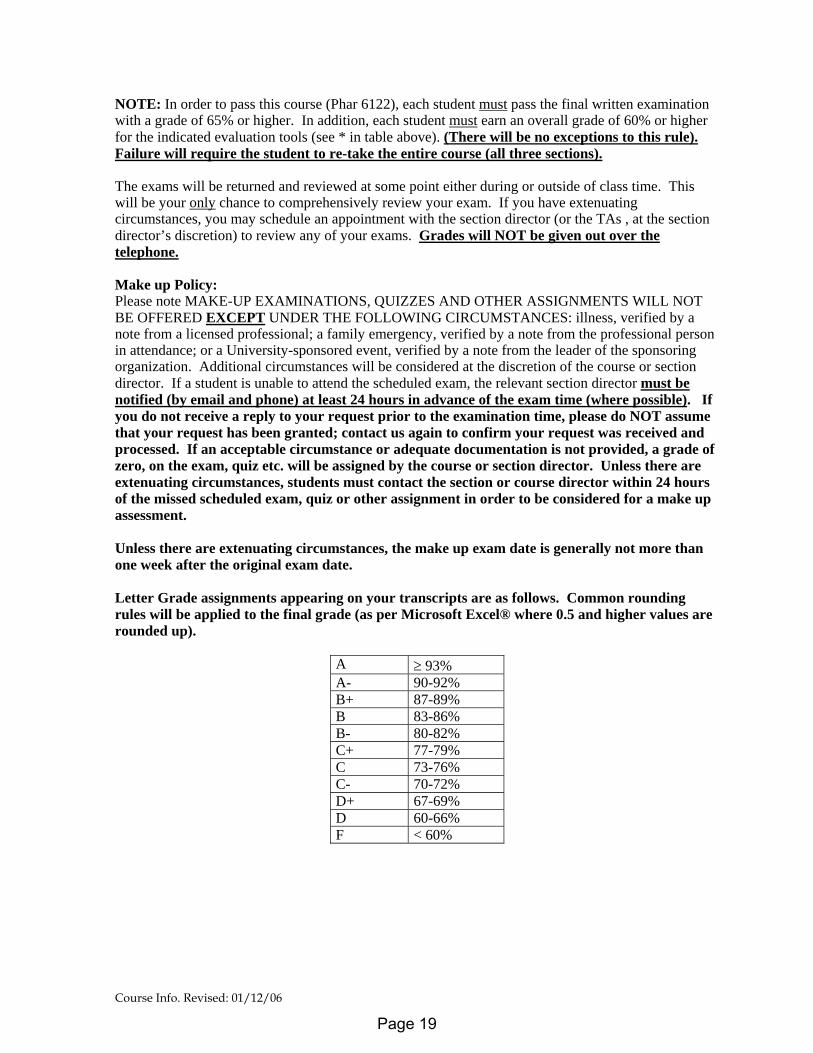
NOTE: In order to pass this course (Phar 6122), each student must pass the final written examination with a grade of 65% or higher. In addition, each student must earn an overall grade of 60% or higher for the indicated evaluation tools (see * in table above). (There will be no exceptions to this rule). Failure will require the student to re-take the entire course (all three sections). The exams will be returned and reviewed at some point either during or outside of class time. This will be your only chance to comprehensively review your exam. If you have extenuating circumstances, you may schedule an appointment with the section director (or the TAs , at the section director’s discretion) to review any of your exams. Grades will NOT be given out over the telephone. Make up Policy: Please note MAKE-UP EXAMINATIONS, QUIZZES AND OTHER ASSIGNMENTS WILL NOT BE OFFERED EXCEPT UNDER THE FOLLOWING CIRCUMSTANCES: illness, verified by a note from a licensed professional; a family emergency, verified by a note from the professional person in attendance; or a University-sponsored event, verified by a note from the leader of the sponsoring organization. Additional circumstances will be considered at the discretion of the course or section director. If a student is unable to attend the scheduled exam, the relevant section director must be notified (by email and phone) at least 24 hours in advance of the exam time (where possible). If you do not receive a reply to your request prior to the examination time, please do NOT assume that your request has been granted; contact us again to confirm your request was received and processed. If an acceptable circumstance or adequate documentation is not provided, a grade of zero, on the exam, quiz etc. will be assigned by the course or section director. Unless there are extenuating circumstances, students must contact the section or course director within 24 hours of the missed scheduled exam, quiz or other assignment in order to be considered for a make up assessment. Unless there are extenuating circumstances, the make up exam date is generally not more than one week after the original exam date. Letter Grade assignments appearing on your transcripts are as follows. Common rounding rules will be applied to the final grade (as per Microsoft Excel® where 0.5 and higher values are rounded up).
A ≥ 93% A- 90-92% B+ 87-89% B 83-86% B- 80-82% C+ 77-79% C 73-76% C- 70-72% D+ 67-69% D 60-66% F < 60%
Page 19
Course Info. Revised: 01/12/06
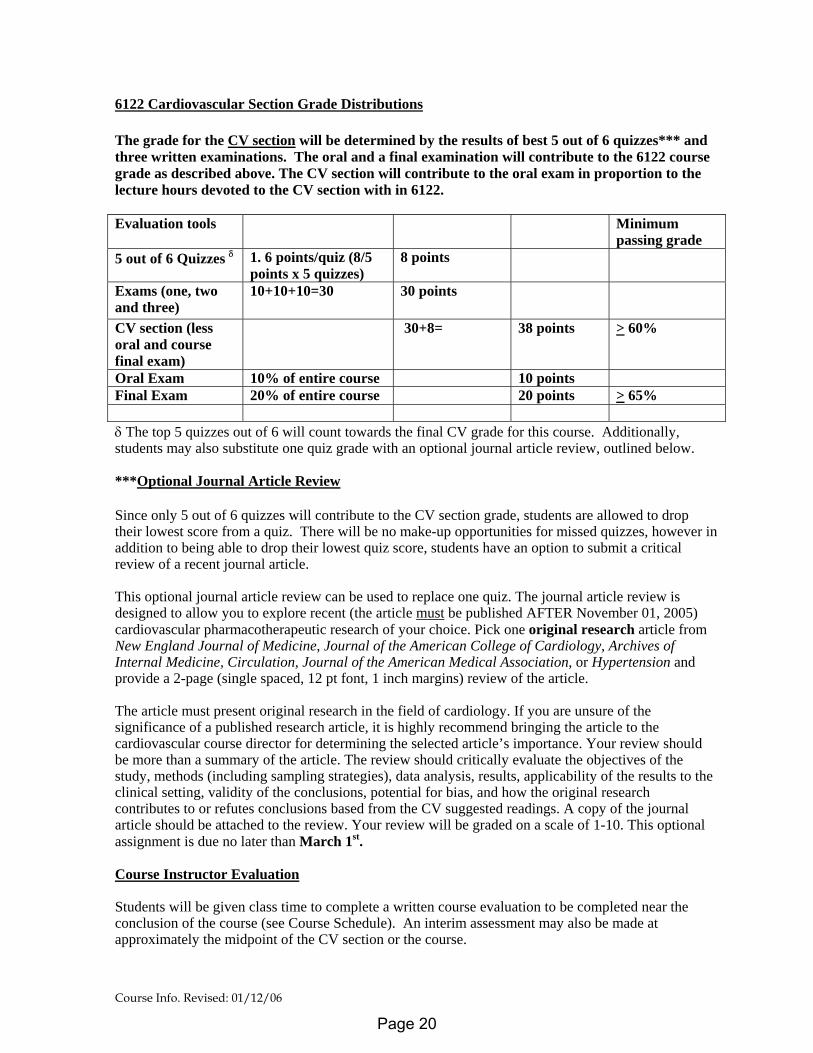
6122 Cardiovascular Section Grade Distributions The grade for the CV section will be determined by the results of best 5 out of 6 quizzes*** and three written examinations. The oral and a final examination will contribute to the 6122 course grade as described above. The CV section will contribute to the oral exam in proportion to the lecture hours devoted to the CV section with in 6122. Evaluation tools Minimum
passing grade 5 out of 6 Quizzes δ 1. 6 points/quiz (8/5
points x 5 quizzes) 8 points
Exams (one, two and three)
10+10+10=30 30 points
CV section (less oral and course final exam)
30+8= 38 points > 60%
Oral Exam 10% of entire course 10 points Final Exam 20% of entire course 20 points > 65% δ The top 5 quizzes out of 6 will count towards the final CV grade for this course. Additionally, students may also substitute one quiz grade with an optional journal article review, outlined below. ***Optional Journal Article Review Since only 5 out of 6 quizzes will contribute to the CV section grade, students are allowed to drop their lowest score from a quiz. There will be no make-up opportunities for missed quizzes, however in addition to being able to drop their lowest quiz score, students have an option to submit a critical review of a recent journal article. This optional journal article review can be used to replace one quiz. The journal article review is designed to allow you to explore recent (the article must be published AFTER November 01, 2005) cardiovascular pharmacotherapeutic research of your choice. Pick one original research article from New England Journal of Medicine, Journal of the American College of Cardiology, Archives of Internal Medicine, Circulation, Journal of the American Medical Association, or Hypertension and provide a 2-page (single spaced, 12 pt font, 1 inch margins) review of the article. The article must present original research in the field of cardiology. If you are unsure of the significance of a published research article, it is highly recommend bringing the article to the cardiovascular course director for determining the selected article’s importance. Your review should be more than a summary of the article. The review should critically evaluate the objectives of the study, methods (including sampling strategies), data analysis, results, applicability of the results to the clinical setting, validity of the conclusions, potential for bias, and how the original research contributes to or refutes conclusions based from the CV suggested readings. A copy of the journal article should be attached to the review. Your review will be graded on a scale of 1-10. This optional assignment is due no later than March 1st. Course Instructor Evaluation Students will be given class time to complete a written course evaluation to be completed near the conclusion of the course (see Course Schedule). An interim assessment may also be made at approximately the midpoint of the CV section or the course.
Page 20
Advice for Optimal Exam Taking in Phar 6122--Cardiology section
Robert Straka, Pharm.D. Spring 2006
The following are some suggestions and helpful hints for successfully writing an exam or a quiz in Dr. Straka's course. You are free to use this information any way you like. Our intent is to show you ways that you can minimize unnecessary loss of points on tests. • Write a complete order: When asked to recommend drug therapy for a patient always write a complete order
including drug, dose, route and schedule. You will only be given full credit for a complete order. • Convince us of your understanding of the subject: When we give the oral exam it is easy for us to determine
the depth of your knowledge by just asking a few more questions. However, on a written exam we can only go by your written response on the paper. It is up to you to explain your reasoning such that we have little doubt that you understand the concept.
• Understand the meaning of the term "Significant Statements": This point directly correlates to the previous
suggestion of convincing us of your understanding. Here are examples of poor and acceptable significant statements concerning the description of the MOA of warfarin:
- Warfarin is an anticoagulant and as such inhibits the formation of clots. (Poor answer) - Warfarin is an antithrombotic agent which inhibits the formation of the vitamin K dependent clotting factors II,
VII, IX and X, and thus results in the patient having an anticoagulated state. (acceptable answer) • Be specific but brief: This is a skill which most students are just beginning to develop. It may seem contradictory
to other suggestions above which state that you need to "convince us of your understanding of a subject", but then we ask you to be brief. However the suggestion here is to not write unnecessary statements which lack relevance. Think of what you want to say and then write it. It may not always be a very short response, but most times when only the pertinent points are mentioned, it should be concise.
• Examples given at the end of a question DO NOT count as answers: It is often difficult to fully describe what
type of answer we are searching for. Often an example helps. Sometimes the example will be an actual answer to the question and in these cases we are not giving away points. We will attempt to state that "3 answers other then the example" are needed, but in cases where we don't, it is assumed you realize that the examples don't count and should not be used as your answers.
• Units: When answering a question with a lab value, a measurement, a monitoring parameter, or anything else
requiring units, always include units or critical values (cut-off etc.) in your answer. You will lose points if units are left out of your answer.
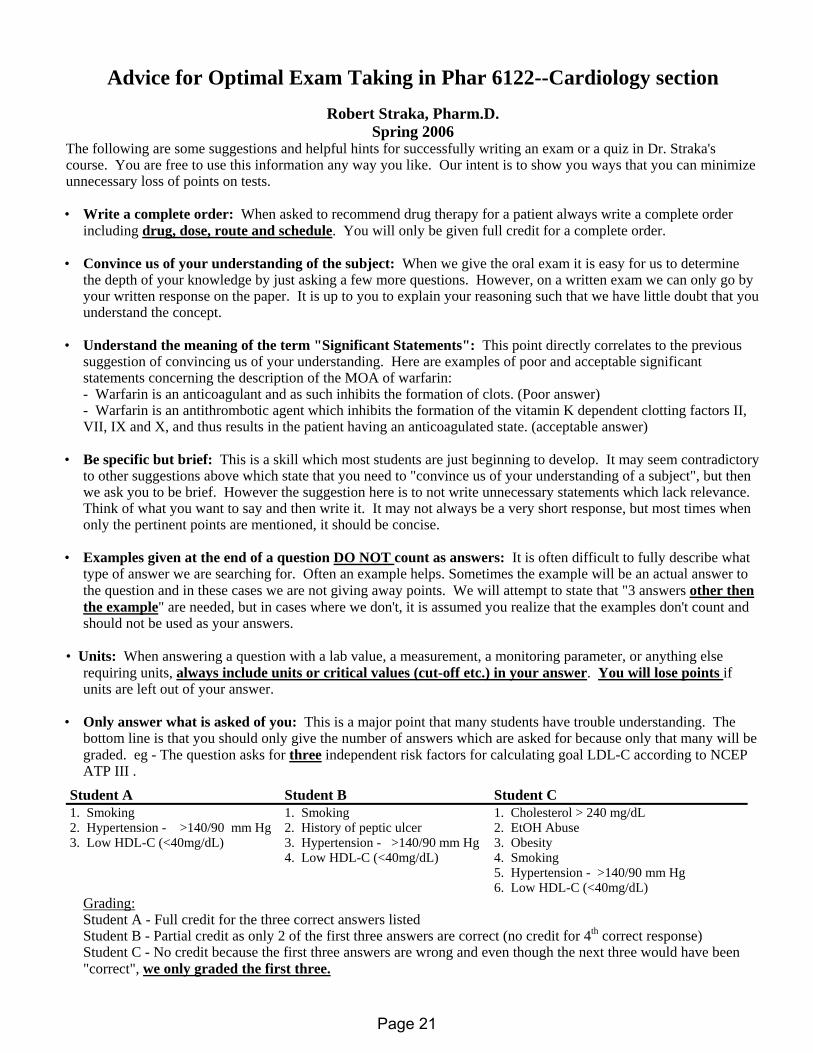
• Only answer what is asked of you: This is a major point that many students have trouble understanding. The
bottom line is that you should only give the number of answers which are asked for because only that many will be graded. eg - The question asks for three independent risk factors for calculating goal LDL-C according to NCEP ATP III .
Student A Student B Student C 1. Smoking 1. Smoking 1. Cholesterol > 240 mg/dL 2. Hypertension - >140/90 mm Hg 2. History of peptic ulcer 2. EtOH Abuse 3. Low HDL-C (<40mg/dL) 3. Hypertension - >140/90 mm Hg 3. Obesity 4. Low HDL-C (<40mg/dL) 4. Smoking 5. Hypertension - >140/90 mm Hg 6. Low HDL-C (<40mg/dL)
Grading: Student A - Full credit for the three correct answers listed Student B - Partial credit as only 2 of the first three answers are correct (no credit for 4th correct response) Student C - No credit because the first three answers are wrong and even though the next three would have been
"correct", we only graded the first three.
Page 21
Abbreviations 01/12/06
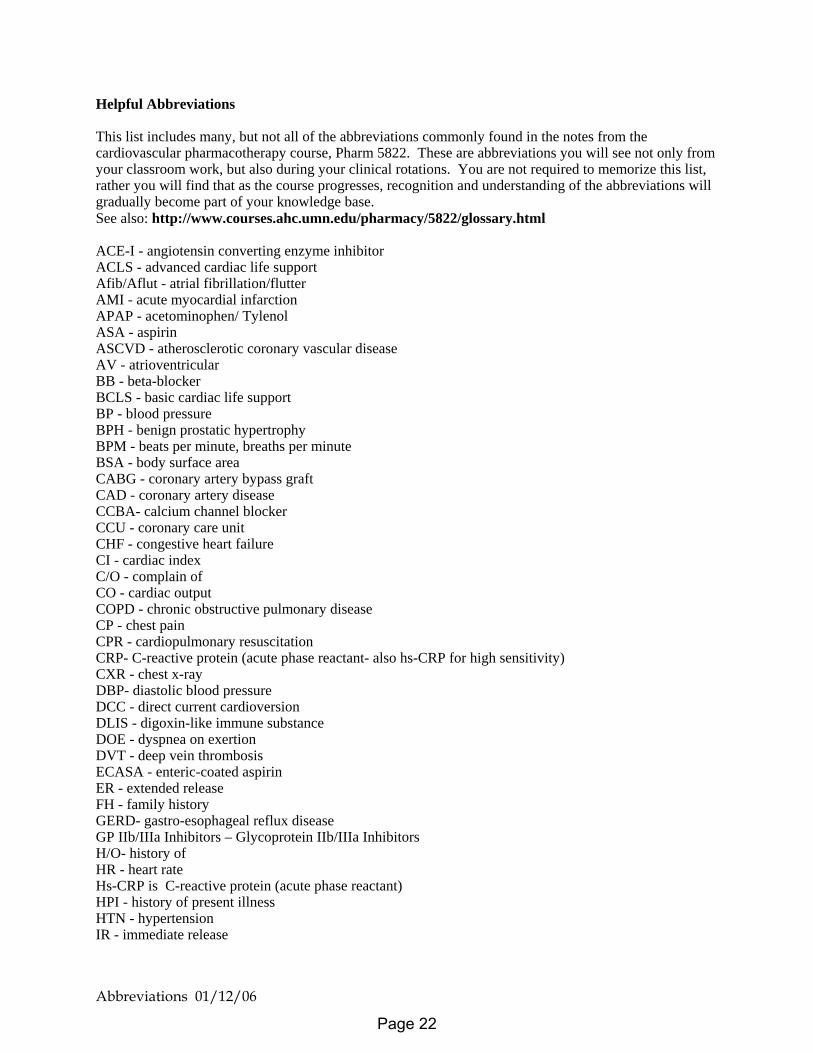
Helpful Abbreviations This list includes many, but not all of the abbreviations commonly found in the notes from the cardiovascular pharmacotherapy course, Pharm 5822. These are abbreviations you will see not only from your classroom work, but also during your clinical rotations. You are not required to memorize this list, rather you will find that as the course progresses, recognition and understanding of the abbreviations will gradually become part of your knowledge base. See also: http://www.courses.ahc.umn.edu/pharmacy/5822/glossary.html ACE-I - angiotensin converting enzyme inhibitor ACLS - advanced cardiac life support Afib/Aflut - atrial fibrillation/flutter AMI - acute myocardial infarction APAP - acetominophen/ Tylenol ASA - aspirin ASCVD - atherosclerotic coronary vascular disease AV - atrioventricular BB - beta-blocker BCLS - basic cardiac life support BP - blood pressure BPH - benign prostatic hypertrophy BPM - beats per minute, breaths per minute BSA - body surface area CABG - coronary artery bypass graft CAD - coronary artery disease CCBA- calcium channel blocker CCU - coronary care unit CHF - congestive heart failure CI - cardiac index C/O - complain of CO - cardiac output COPD - chronic obstructive pulmonary disease CP - chest pain CPR - cardiopulmonary resuscitation CRP- C-reactive protein (acute phase reactant- also hs-CRP for high sensitivity) CXR - chest x-ray DBP- diastolic blood pressure DCC - direct current cardioversion DLIS - digoxin-like immune substance DOE - dyspnea on exertion DVT - deep vein thrombosis ECASA - enteric-coated aspirin ER - extended release FH - family history GERD- gastro-esophageal reflux disease GP IIb/IIIa Inhibitors – Glycoprotein IIb/IIIa Inhibitors H/O- history of HR - heart rate Hs-CRP is C-reactive protein (acute phase reactant) HPI - history of present illness HTN - hypertension IR - immediate release
Page 22
Abbreviations 01/12/06
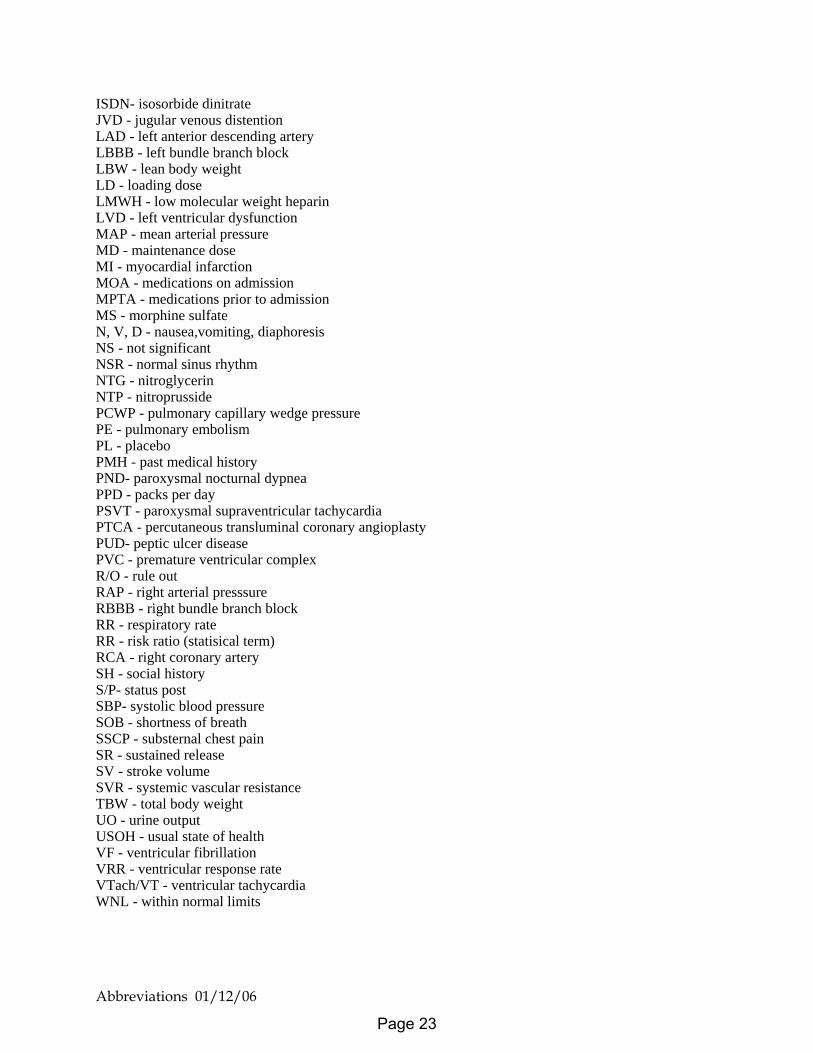
ISDN- isosorbide dinitrate JVD - jugular venous distention LAD - left anterior descending artery LBBB - left bundle branch block LBW - lean body weight LD - loading dose LMWH - low molecular weight heparin LVD - left ventricular dysfunction MAP - mean arterial pressure MD - maintenance dose MI - myocardial infarction MOA - medications on admission MPTA - medications prior to admission MS - morphine sulfate N, V, D - nausea,vomiting, diaphoresis NS - not significant NSR - normal sinus rhythm NTG - nitroglycerin NTP - nitroprusside PCWP - pulmonary capillary wedge pressure PE - pulmonary embolism PL - placebo PMH - past medical history PND- paroxysmal nocturnal dypnea PPD - packs per day PSVT - paroxysmal supraventricular tachycardia PTCA - percutaneous transluminal coronary angioplasty PUD- peptic ulcer disease PVC - premature ventricular complex R/O - rule out RAP - right arterial presssure RBBB - right bundle branch block RR - respiratory rate RR - risk ratio (statisical term) RCA - right coronary artery SH - social history S/P- status post SBP- systolic blood pressure SOB - shortness of breath SSCP - substernal chest pain SR - sustained release SV - stroke volume SVR - systemic vascular resistance TBW - total body weight UO - urine output USOH - usual state of health VF - ventricular fibrillation VRR - ventricular response rate VTach/VT - ventricular tachycardia WNL - within normal limits
Page 23
Reviewed: 12/19/2005
Introduction to Pharm 6122 Cardiovascular Section
Robert J. Straka, Pharm.D. Spring 2006
Outline 1) Introductions (Course Faculty, TA’s) 2) Required Texts (Other sources of readings, guidelines) 3) References (Web based and other sources) http://www.courses.ahc.umn.edu/pharmacy/5822/homepage1.html 4) Evaluation and Grading Exams
Quizzes Written Exams final oral exams 5) Course director availability, contact and evaluation 6) Overview Lecture Cardiac Anatomy Cardiac Conduction System Hemodynamic Monitoring Case Example
Page 24
Reviewed: 12/19/2005
PHAR 6122
Cardiovascular Section Robert J. Straka, Pharm.D.
Orientation, Anatomy, and Physiology Spring 2006
OBJECTIVES After attending lecture and reading the required material the learner will be able to: 1. Demonstrate an understanding of the materials, requirements and grading system for the
course. 2. Demonstrate a working knowledge of basic cardiovascular anatomy and physiology. (Draw
the major blood vessels associated with blood flow to and from the heart, label the major valves and coronary arteries perfusing the myocardium and label the major structures of the cardiac conduction system)
Page 25
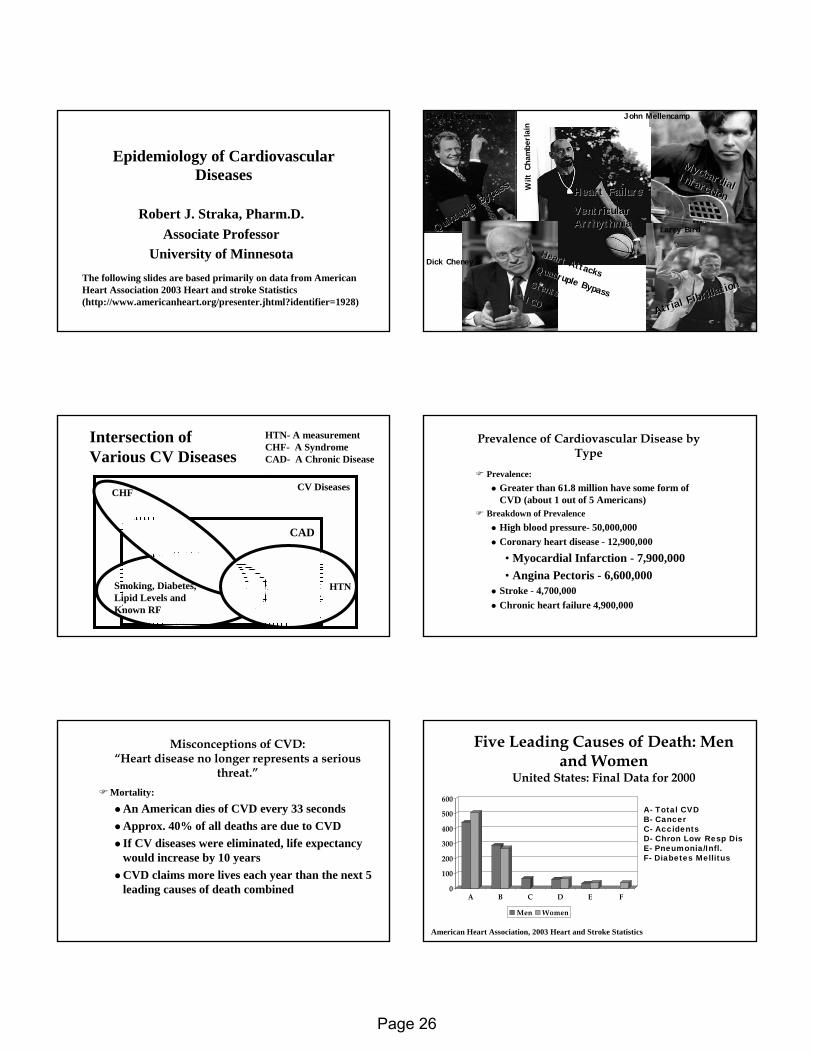
Epidemiology of Cardiovascular Epidemiology of Cardiovascular DiseasesDiseases
Robert J. Straka, Pharm.D.Robert J. Straka, Pharm.D.Associate ProfessorAssociate Professor
University of MinnesotaUniversity of MinnesotaThe following slides are based primarily on data from American Heart Association 2003 Heart and stroke Statistics (http://www.americanheart.org/presenter.jhtml?identifier=1928)
Quintup
le Bypa
ss
Quintup
le Bypa
ss
David Letterman John Mellencamp
Myocardial
Myocardial Infarction
Infarction
Wilt
Cha
mbe
rlain
Heart FailureHeart Failure
Ventricular Ventricular ArrhythmiaArrhythmia
Dick CheneyHeart Attacks
Heart AttacksQuadruple Bypass
Quadruple BypassStentsStents
ICDICD
Larry Bird
Atrial Fibril
lation
Atrial Fibril
lation
CV Diseases
Intersection of Various CV Diseases
HTN- A measurementCHF- A SyndromeCAD- A Chronic Disease
Smoking, Diabetes, Lipid Levels and Known RF
HTN
CAD
CHF
Prevalence of Cardiovascular Disease by Prevalence of Cardiovascular Disease by TypeType
PrevalencePrevalence::Greater than 61.8 million have some form of Greater than 61.8 million have some form of CVD (about 1 out of 5 Americans)CVD (about 1 out of 5 Americans)
Breakdown of PrevalenceBreakdown of PrevalenceHigh blood pressureHigh blood pressure-- 50,000,00050,000,000Coronary heart disease Coronary heart disease -- 12,900,00012,900,000
•• Myocardial Infarction Myocardial Infarction -- 7,900,0007,900,000•• Angina Pectoris Angina Pectoris -- 6,600,0006,600,000
Stroke Stroke -- 4,700,0004,700,000Chronic heart failure 4,900,000Chronic heart failure 4,900,000
Misconceptions of CVD: Misconceptions of CVD: “Heart disease no longer represents a serious “Heart disease no longer represents a serious
threat.”threat.”MortalityMortality::
An American dies of CVD every 33 secondsAn American dies of CVD every 33 secondsApprox. 40% of all deaths are due to CVDApprox. 40% of all deaths are due to CVDIf CV diseases were eliminated, life expectancy If CV diseases were eliminated, life expectancy would increase by 10 years would increase by 10 years CVD claims more lives each year than the next 5 CVD claims more lives each year than the next 5 leading causes of death combined leading causes of death combined
Five Leading Causes of Death: Men Five Leading Causes of Death: Men and Womenand Women
United States: Final Data for 2000United States: Final Data for 2000
0
100
200
300
400
500
600
A B C D E F
Men Women
A- Total CVDB- CancerC- AccidentsD- Chron Low Resp DisE- Pneumonia/Infl.F- Diabetes Mellitus
American Heart Association, 2003 Heart and Stroke Statistics
Page 26
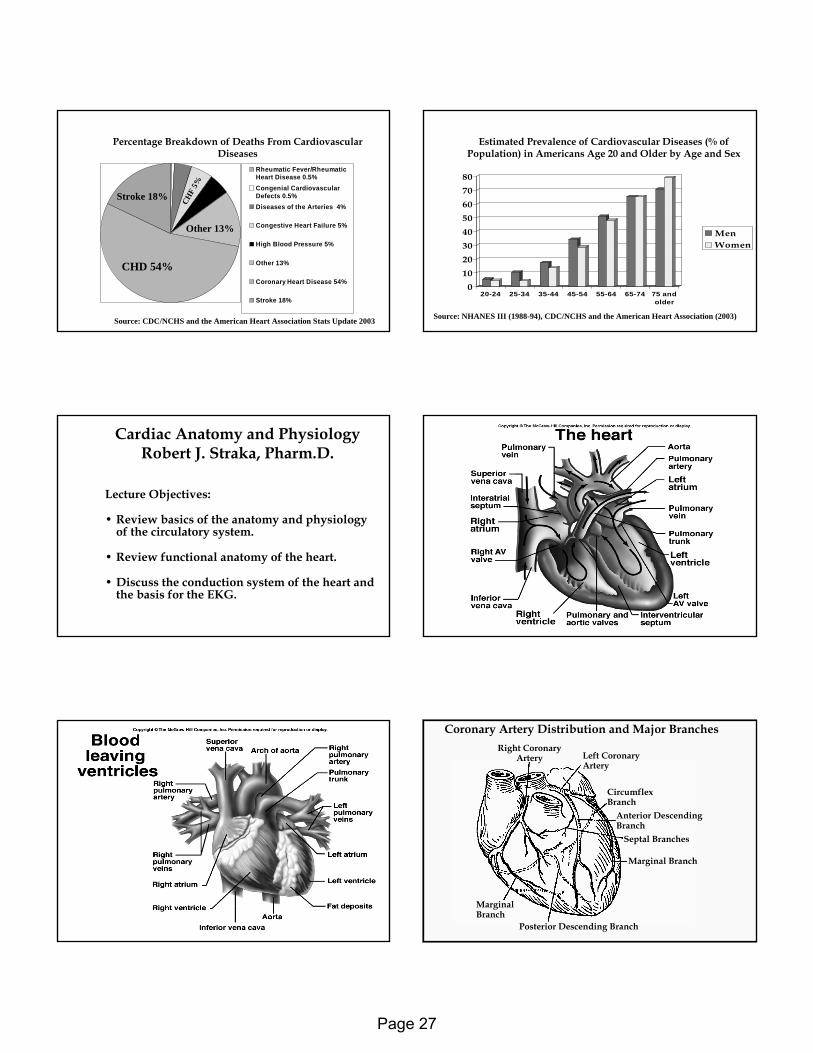
Percentage Breakdown of Deaths From Cardiovascular Percentage Breakdown of Deaths From Cardiovascular DiseasesDiseases
Rheumatic Fever/RheumaticHeart Disease 0.5%Congenial CardiovascularDefects 0.5% Diseases of the Arteries 4%
Congestive Heart Failure 5%
High Blood Pressure 5%
Other 13%
Coronary Heart Disease 54%
Stroke 18%
Source: CDC/NCHS and the American Heart Association Stats Update 2003
CHD 54%
Other 13%
Stroke 18%HTN 5%
CHF
5%
Estimated Prevalence of Cardiovascular Diseases (% of Estimated Prevalence of Cardiovascular Diseases (% of Population) in Americans Age 20 and Older by Age and SexPopulation) in Americans Age 20 and Older by Age and Sex
01020304050607080
20-24 25-34 35-44 45-54 55-64 65-74 75 andolder
MenWomen
Source: NHANES III (1988-94), CDC/NCHS and the American Heart Association (2003)
Cardiac Anatomy and Physiology Cardiac Anatomy and Physiology Robert J. Straka, Pharm.D.Robert J. Straka, Pharm.D.
Lecture Objectives: Lecture Objectives:
•• Review basics of the anatomy and physiology Review basics of the anatomy and physiology of the circulatory system.of the circulatory system.
•• Review functional anatomy of the heart.Review functional anatomy of the heart.
•• Discuss the conduction system of the heart and Discuss the conduction system of the heart and the basis for the EKG.the basis for the EKG.
Right CoronaryArtery Left Coronary
Artery
CircumflexBranch
Anterior DescendingBranch
Septal Branches
Marginal Branch
Posterior Descending Branch
MarginalBranch
Coronary Artery Distribution and Major Branches
Page 27
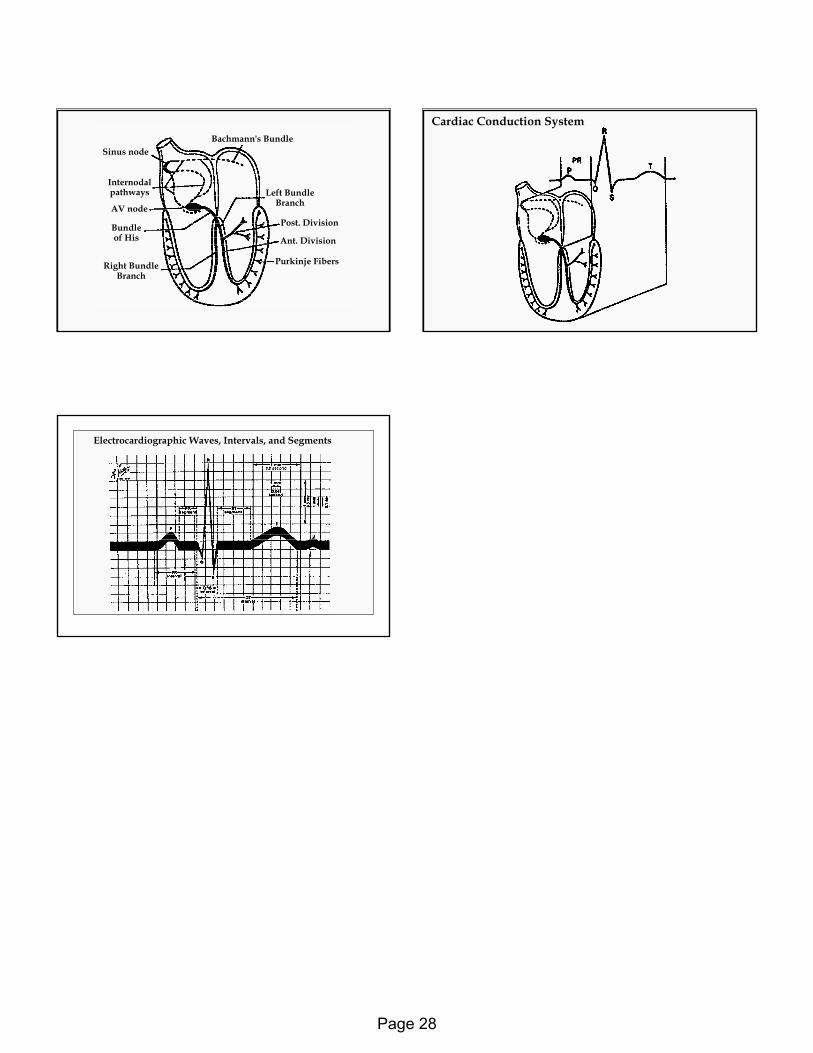
Bachmann's BundleSinus node
Internodalpathways
AV node
Bundleof His
Right BundleBranch
Left BundleBranch
Post. Division
Ant. Division
Purkinje Fibers
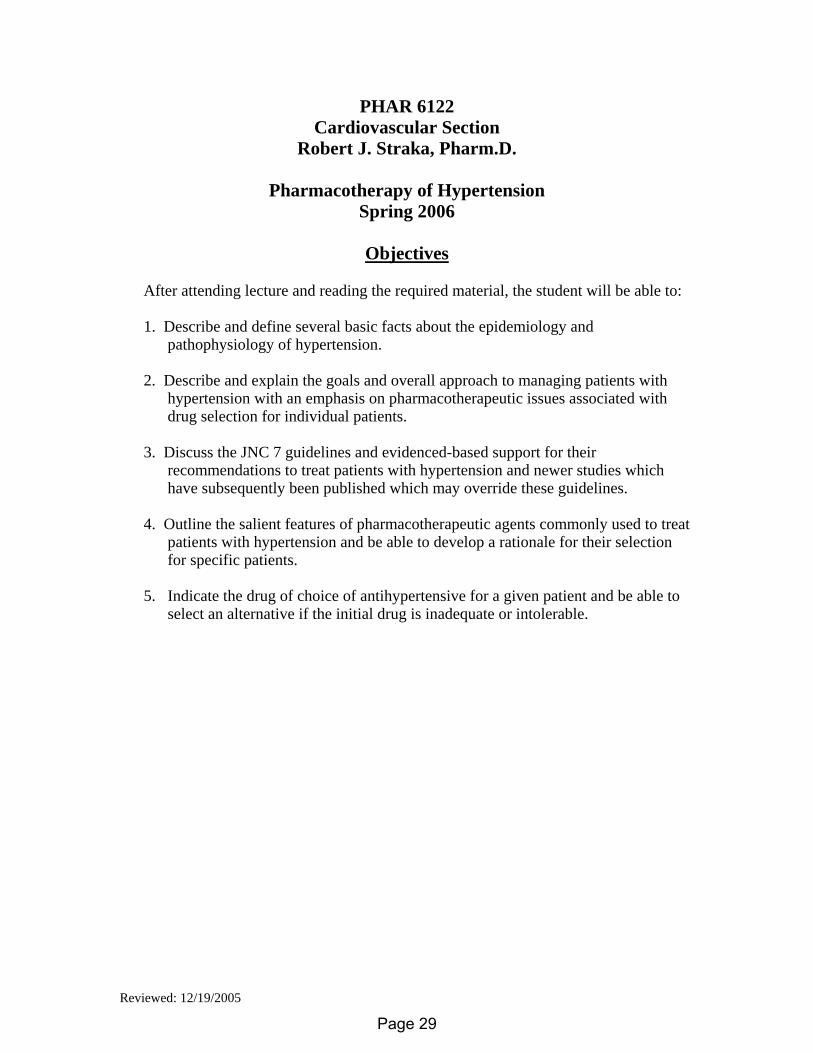
Cardiac Conduction System
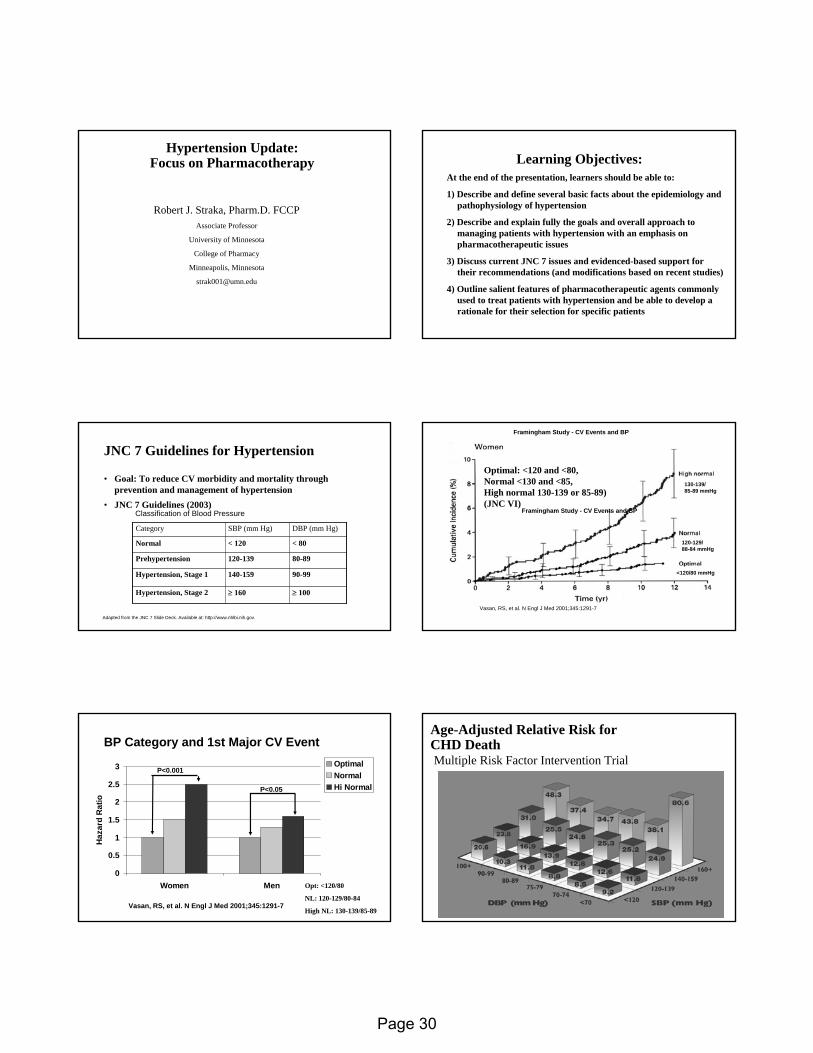
Electrocardiographic Waves, Intervals, and Segments
Page 28
Reviewed: 12/19/2005
PHAR 6122 Cardiovascular Section
Robert J. Straka, Pharm.D.
Pharmacotherapy of Hypertension Spring 2006
Objectives
After attending lecture and reading the required material, the student will be able to: 1. Describe and define several basic facts about the epidemiology and
pathophysiology of hypertension. 2. Describe and explain the goals and overall approach to managing patients with
hypertension with an emphasis on pharmacotherapeutic issues associated with drug selection for individual patients.
3. Discuss the JNC 7 guidelines and evidenced-based support for their
recommendations to treat patients with hypertension and newer studies which have subsequently been published which may override these guidelines.
4. Outline the salient features of pharmacotherapeutic agents commonly used to treat
patients with hypertension and be able to develop a rationale for their selection for specific patients.
5. Indicate the drug of choice of antihypertensive for a given patient and be able to
select an alternative if the initial drug is inadequate or intolerable.
Page 29
Hypertension Update: Hypertension Update: Focus on PharmacotherapyFocus on Pharmacotherapy
Robert J. Straka, Pharm.D. FCCPAssociate Professor
University of Minnesota
College of Pharmacy
Minneapolis, Minnesota
Learning Objectives:Learning Objectives:At the end of the presentation, learners should be able to:
1) Describe and define several basic facts about the epidemiology and pathophysiology of hypertension
2) Describe and explain fully the goals and overall approach to managing patients with hypertension with an emphasis on pharmacotherapeutic issues
3) Discuss current JNC 7 issues and evidenced-based support for their recommendations (and modifications based on recent studies)
4) Outline salient features of pharmacotherapeutic agents commonly used to treat patients with hypertension and be able to develop a rationale for their selection for specific patients
Adapted from the JNC 7 Slide Deck. Available at: http://www.nhlbi.nih.gov.
JNC 7 Guidelines for Hypertension JNC 7 Guidelines for Hypertension
• Goal: To reduce CV morbidity and mortality through prevention and management of hypertension
• JNC 7 Guidelines (2003)
≥ 100≥ 160Hypertension, Stage 2
90-99140-159Hypertension, Stage 1
80-89120-139Prehypertension
< 80< 120Normal
DBP (mm Hg)SBP (mm Hg)Category
Classification of Blood Pressure
130-139/85-89 mmHg
120-129/88-84 mmHg
<120/80 mmHg
Vasan, RS, et al. N Engl J Med 2001;345:1291-7
Framingham Study - CV Events and BP
Framingham Study - CV Events and BP
Optimal: <120 and <80, Normal <130 and <85, High normal 130-139 or 85-89) (JNC VI)
BP Category and 1st Major CV EventBP Category and 1st Major CV Event
0
0.5
1
1.5
2
2.5
3
Women Men
Haz
ard
Rat
io
OptimalNormalHi Normal
Vasan, RS, et al. N Engl J Med 2001;345:1291-7
P<0.001
P<0.05
Opt: <120/80
NL: 120-129/80-84
High NL: 130-139/85-89
AgeAge--Adjusted Relative Risk for Adjusted Relative Risk for CHD DeathCHD DeathMultiple Risk Factor Intervention TrialMultiple Risk Factor Intervention Trial
Page 30
Estimated 10Estimated 10--Year Risk (%) of Coronary Artery Disease for Year Risk (%) of Coronary Artery Disease for Various Combinations of Risk Factors for Men and WomenVarious Combinations of Risk Factors for Men and Women
57.5
38
28.823.4
16.5
8.713.7
56.4
36.8
27.7
11.39.25.5
17
0
10
20
30
40
50
60
70
MenWomen
BP Systolic 120 160 160 160 160 160 160Cholesterol 220 220 260 260 260 260 260HDL -C 50 50 50 35 35 35 35Diabetes - - - - + + +Cigarettes - - - - - + +LVH by ECG - - - - - - +
Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. JAMA. 2001;285:2486-2497.
34
21
17
1312
23
12
810
6
18
119
66
17
88
64
14
56
33
142+142+
125125--131131
<182<182182182--202202
203203--220220221221--244244
Cholesterol QuintileCholesterol Quintile(mg/dL)(mg/dL)
Systolic BP Quintile Systolic BP Quintile (mm Hg)(mm Hg)<118<118
118118--124124
132132--141141
CHD Deaths/10,000 PatientCHD Deaths/10,000 Patient--YearsYears
245+245+
NeatonNeaton et al. et al. Arch Intern MedArch Intern Med. 1992;152:56. 1992;152:56--64.64.
MRFIT: Impact of Elevated SBP and Total Cholesterol MRFIT: Impact of Elevated SBP and Total Cholesterol on CHD Mortality (N=316,099)on CHD Mortality (N=316,099)
Target Organ Damage in HypertensionTarget Organ Damage in Hypertension
HYPERTENSION
Adapted from JNC V. Arch Intern Med. 1993;1563:154.
Stroke
Retinopathy
LVHCHDCHF
Renalimpairment
Decreased arterialcompliance
Lowering BP Is Imperative in Reducing Lowering BP Is Imperative in Reducing Cardiovascular RiskCardiovascular Risk
Myocardial Infarction Stroke Heart Failure
20%-25%35%-40%
>50%
In clinical trials, antihypertensive therapy has been associated with reductions in:
JNC 7 Express. 2003. NIH Publication 03-5233.Neal B et al. Lancet. 2000;356:1955-1964.
JNC JNC -- 77
The Seventh Report
of the
Joint National Committee on Prevention, Detection, Evaluation, and Treatment of
High Blood Pressure
JAMA 2003; 289 (19): 2560-2572 May 21, 2003
Web Site
http://www.nhlbi.nih.gov/guidelines/hypertension/index.htm
JNC 7 HighlightsJNC 7 Highlights• For patients older than 50 years, SBP >140 mm Hg is a more important
CVD risk factor than DBP
• Patients with pre-hypertension require health-promoting lifestyle modifications to prevent CVD
• Thiazide-type diuretics should be used in drug treatment for most patients with uncomplicated hypertension, either alone or in combination with drugs from other classes
• High-risk conditions are compelling indications for the initial use of specific antihypertensive drug classes
• Most patients will require 2 or more antihypertensive agents to reach their goal blood pressure
• If BP is >20/10 mm Hg above goal, consideration should be given to initiating therapy with 2 agents, one of which should usually be a thiazide-type diuretic
The JNC 7 report. JAMA. 2003;289:2560-2572.JAMA 2003; 289 (19): 2560-2572 May 21, 2003
Page 31
Adapted from the JNC 7 Slide Deck. Available at: http://www.nhlbi.nih.gov.
JNC 7 Guidelines for Hypertension JNC 7 Guidelines for Hypertension
• Goal: To reduce CV morbidity and mortality through prevention and management of hypertension
• JNC 7 Guidelines (2003)
≥ 100≥ 160Hypertension, Stage 2
90-99140-159Hypertension, Stage 1
80-89120-139Prehypertension
< 80< 120Normal
DBP (mm Hg)SBP (mm Hg)Category
Classification of Blood Pressure
Benefits of Lowering BPBenefits of Lowering BP
• In stage 1 HTN and additional CVD risk factors, achieving a sustained 12 mmHg reduction in SBP over 10 years will prevent 1 death for every 11 patients treated
Adapted from the JNC 7 Slide Deck. Available at: http://www.nhlbi.nih.gov.
Heart Failure 50%
Myocardial Infarction 20-25%
Stroke Incidence 35-40%
Average Percent Reduction
*Controlled BP = SBP <140 mm Hg and DBP <90 mm Hg.
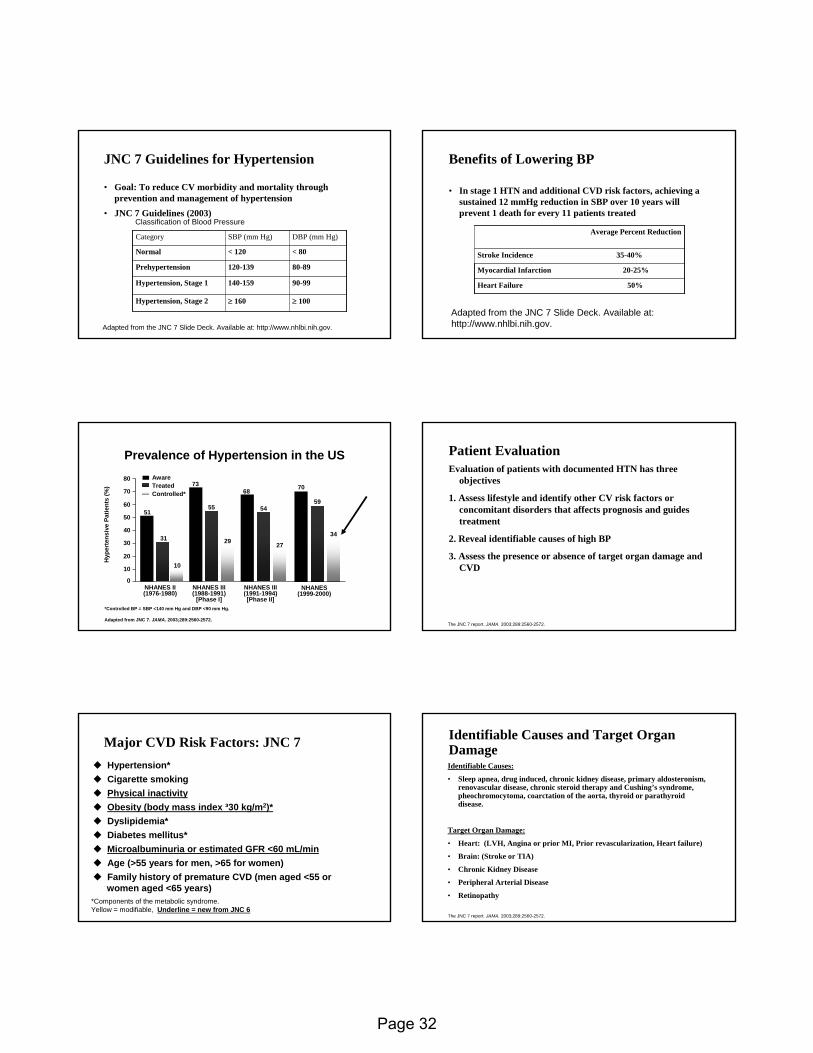
Adapted from JNC 7. JAMA. 2003;289:2560-2572.
Hyp
erte
nsiv
e Pa
tient
s (%
)
NHANES II(1976-1980)
NHANES III (1988-1991)
[Phase I]
NHANES III(1991-1994)[Phase II]
51
7368
31
55 54
10
29 27
AwareTreatedControlled*
10
20
30
40
50
60
70
80
0
Prevalence of Hypertension in the USPrevalence of Hypertension in the US
NHANES(1999-2000)
70
59
34
Patient EvaluationPatient EvaluationEvaluation of patients with documented HTN has three
objectives
1. Assess lifestyle and identify other CV risk factors or concomitant disorders that affects prognosis and guides treatment
2. Reveal identifiable causes of high BP
3. Assess the presence or absence of target organ damage and CVD
The JNC 7 report. JAMA. 2003;289:2560-2572.
Major CVD Risk Factors: JNC 7Major CVD Risk Factors: JNC 7Hypertension*Hypertension*Cigarette smokingCigarette smokingPhysical inactivityPhysical inactivityObesity (body mass index Obesity (body mass index ³³30 30 kg/mkg/m22))**Dyslipidemia*Dyslipidemia*Diabetes mellitus*Diabetes mellitus*Microalbuminuria or estimated GFR <60 mL/minMicroalbuminuria or estimated GFR <60 mL/minAge (>55 years for men, >65 for women)Age (>55 years for men, >65 for women)Family history of premature CVD (men aged <55 or Family history of premature CVD (men aged <55 or women aged <65 years)women aged <65 years)
*Components of the metabolic syndrome. *Components of the metabolic syndrome. Yellow = modifiable, Yellow = modifiable, Underline = new from JNC 6Underline = new from JNC 6
Identifiable Causes and Target Organ Identifiable Causes and Target Organ DamageDamageIdentifiable Causes:
• Sleep apnea, drug induced, chronic kidney disease, primary aldosteronism, renovascular disease, chronic steroid therapy and Cushing’s syndrome, pheochromocytoma, coarctation of the aorta, thyroid or parathyroid disease.
Target Organ Damage:
• Heart: (LVH, Angina or prior MI, Prior revascularization, Heart failure)
• Brain: (Stroke or TIA)
• Chronic Kidney Disease
• Peripheral Arterial Disease
• Retinopathy
The JNC 7 report. JAMA. 2003;289:2560-2572.
Page 32
Laboratory TestsLaboratory Tests• Routine Tests:
– ECG
– UA
– Blood glucose, and hematocrit
– Serum Potassium, creatinine, or the corresponding estimated GFR and Ca
– Lipid profile, after 9-12 hour fast, that includes HDL, LDL and TG
Optional Tests:
– Measurement of Urinary albumin excretion or albumin/creatinine ratio
– More extensive testing for identifiable causes not generally indicated unless BP control is not achieved
Adapted from the JNC 7 Slide Deck. Available at: http://www.nhlbi.nih.gov.
Goals of TherapyGoals of Therapy
• Reduce CVD and renal morbidity and mortality
• Treat to BP < 140/90 mmHg or BP < 130/80 mmHg in patients with diabetes or chronic kidney disease
• Achieve SBP goal especially in persons >50 years of age
Adapted from the JNC 7 Slide Deck. Available at: http://www.nhlbi.nih.gov.
JNC 7: Lifestyle ModificationJNC 7: Lifestyle Modification
2-4 mmHgModeration of alcohol consumption
4-9 mmHgPhysical activity
2-8 mmHgDietary sodium reduction
8-14 mmHgAdopt DASH eating plan
5-20 mmHg/10Kg wt lossWeight Reduction
Approximate SBP reduction (range)Modification
.Adapted from the JNC 7 Reference Card. Available at: http://www.nhlbi.nih.gov.
JNC 7 Algorithm for TreatmentJNC 7 Algorithm for Treatment
Adapted from the JNC 7 Slide Deck. Available at: http://www.nhlbi.nih.gov
JNC 7: Compelling Indications for JNC 7: Compelling Indications for Individual Drug ClassesIndividual Drug Classes
THIAZ, ACEIRecurrent stroke prevention
ACEI, ARBChronic kidney disease
THIAZ, BB, ACEI, ARB, CCBDiabetes
THIAZ, BB, ACEI, CCBHigh CVD risk
BB, ACEI, ALDO ANTPost-myocardial infarction
THIAZ, BB, ACEI, ARB, ALDO ANTHeart failure
Recommended Drug ClassesCompelling Indication
.
Adapted from the JNC 7 Reference Card. Available at: http://www.nhlbi.nih.gov.
Compelling Indications for Compelling Indications for Individual Drug Classes: JNC 7Individual Drug Classes: JNC 7
Recommended Clinical Trial BasisCompelling Indication
ALLHAT, HOPE, ANBP2, LIFE, CONVINCE
ACC/AHA Post-MI Guideline, BHAT, SAVE, Capricorn, EPHESUS
ACC/AHA Heart Failure Guideline,MERIT-HF, COPERNICUS, CIBIS, SOLVD, AIRE, TRACE, ValHEFT, RALES, CHARM
DIUR, BB, ACE, CCB
BB, ACEI, ALDO ANT
DIUR, BB, ACEI, ARB, ALDO-ANT
High CAD risk
Post-myocardialinfarction
Heart failure
Adapted from Chobanian et al. JAMA. 2003; Vol 289, No 19: 2560-2572.
Page 33
Recurrent stroke prevention
Chronic kidney disease
Diabetes
Compelling Indication
DIUR, ACEI
ACEI, ARB
DIUR, BB, ACE, ARB, CCB
Compelling Indications for Compelling Indications for Individual Drug Classes: JNC 7Individual Drug Classes: JNC 7
PROGRESS
NKF Guideline, Captopril Trial, RENAAL, IDNT, REIN, AASK
NKF-ADA Guideline,UKPDS, ALLHAT
Adapted from Chobanian et al. JAMA. 2003; Vol 289, No 19: 2560-2572.
Recommended Clinical Trial Basis
Studies Supporting the Guidelines Studies Supporting the Guidelines
• ALLHAT, ANBP2, VALUE ASCOT-BPL
• MERIT-HF, VALHFT, CHARM
• LIFE, LIFE Substudy
• HOPE , Micro-HOPE
• IDNT RENAAL
• AASK
Treatment Diabetes:Treatment Diabetes:Diabetes Care 29;S4Diabetes Care 29;S4--S42:2006S42:2006
• Initial drug therapy for those with a blood pressure >140/90 should be with a drug class demonstrated to reduce CVD events in patients with diabetes (ACE inhibitors, ARBs, β-blockers, diuretics, calcium channel blockers). (A)
– All patients with diabetes and hypertension should be treated with a regimen that includes either and ACE inhibitor or ARB (E)
Hypertension Management in Adults with Diabetes (Diabetes Care, Hypertension Management in Adults with Diabetes (Diabetes Care, VolVol 29 S429 S4--S42, S42, Supplements Jan 2006)Supplements Jan 2006)
Treatment Cont.Treatment Cont.
• If ACE inhibitors or ARBs are used, monitor renal function and serum potassium levels. (E)
• While there are no adequate head-to-head comparisons of ACE inhibitors and ARBs, there is clinical trial support for each of the following statements:– In patients with type 1 diabetes with hypertension and any degree of albuminuria, ACE
inhibitors have been shown to delay the progression of nephropathy. (A)
– In patients with type 2 diabetes, hypertension, and microalbuminuria, ACE inhibitors and ARBs have been shown to delay the progression to macroalbuminuria. (A)
– In those with type 2 diabetes, hypertension, macroalbuminuria (>300 mg/day), and renal insufficiency, an ARB should be strongly considered. (A)
Hypertension Management in Adults with Diabetes (Diabetes Care, Hypertension Management in Adults with Diabetes (Diabetes Care, Vol 29, S4Vol 29, S4--S42, Jan 2006)S42, Jan 2006)
ADA Clin Practice Guidelines; Diabetes Care. 2002;25(1):S85-S89.
• Standard urine dipsticks are not sensitive enough to detect microalbuminuria
Diagnostic Criteria for Diagnostic Criteria for AlbuminuriaAlbuminuria
Albuminuria
Normo-
Micro-
Macro-
SpotSpecimen(mcg/mL)
< 20
20-200
> 200
SpotSpecimen
(mcg/mg Cr)
< 30
30-299
≥ 300
24-hr TimedSpecimen
(mg)
< 30
30-299
≥ 300The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. May 21, 2003. JAMA 2003; 289 (19): 2560-2752
JNC 7: Goals for Prevention and JNC 7: Goals for Prevention and Management of HypertensionManagement of Hypertension• Reduce morbidity and mortality by least intrusive means
possible
– SBP <140 mm Hg and DBP <90 mm Hg (<130/80 for diabetics)
– SBP/DBP below these levels if treatment is tolerated
– Control other modifiable risk factors
Page 34
FollowFollow--up and Monitoringup and Monitoring
• Patients should return for follow-up and adjustment of medications until the BP goal is reached
• More frequent visits for stage 2 HTN or with complicating comorbid conditions
• Serum potassium and creatinine monitored 1-2 times per year
• After BP at goal and stable, follow-up at 3-6 month intervals
• Comorbidities, such as heart failure, associated diseases, such as diabetes, and the need for laboratory tests influence the frequency of visits
HOT: Cardiovascular Events in Diabetes HOT: Cardiovascular Events in Diabetes Patients and DBP LevelPatients and DBP Level
Hansson et al. Hansson et al. Lancet.Lancet. 1998;351:17551998;351:1755--1762.1762.
7.59.1
4.3
7.0
15.9
11.1
15.5
11.2
3.7
6.4
3.7
9.0
0
5
10
15
20
Eve
nts
per 1
000
Eve
nts
per 1
000
Pat
ient
Pat
ient
-- yea
rsye
ars
MI Stroke CV Mortality All Mortality
≤90 mm Hg DBP≤85 mm Hg DBP≤80 mm Hg DBP
PP=.016=.016
Additional Considerations in Additional Considerations in Antihypertensive Drug ChoicesAntihypertensive Drug Choices• Potential favorable effects:
– Thiazide diuretics useful in slowing demineralization in osteoporosis
– BBs useful in the treatment of atrial tachyarrhythmias/fibrillation, migraine, thyrotoxicosis(short term), essential tremor, or periopertative HTN
– CCBs useful in Raynaud’s syndrome and certain arrhythmias
– Alpha-blockers useful in prostatism.
Additional Considerations in Additional Considerations in Antihypertensive Drug ChoicesAntihypertensive Drug Choices• Potential unfavorable effects:
– Thiazide diuretics should be used cautiously in gout or history of significant hyponatremia
– BBs should be generally avoided in patients with asthma, reactive airway disease or second or third-degree heart block
– ACEIs and ARBs are contraindicated in pregnant women or those likely to be come pregnant
– ACEIs should not be used in individuals with a history of angioedema
– Aldosterone antagonists and K-sparing diuretics can cause hyperkalemia
Selected Side Effects With Selected Side Effects With Hypertensive MedicationsHypertensive Medications
• Cough (common)
• Angioedema (rare)
• Hyperkalemia (rare)
• Rash (rare)
• Loss of taste (rare)
• Leukopenia (rare)
ACE Inhibitors• Angioedema
(very rare)
• Hyperkalemia
• Edema of the ankle
• Flushing
• Headache
• Gingival hypertrophy
• Bronchospasm
• Bradycardia
• Heart failure
• May mask insulin-
induced hypoglycemia
Less Serious:
• Impaired peripheral
circulation
• Insomnia
• Fatigue
• Decreased exercise
tolerance
• Hypertriglyceridemia†
ARBsCalcium Channel Blockers*Beta Blockers
*Dihydropyridine†Except agents with intrinsic sympathomimetic activity JNC VI. Arch Intern Med. 1997;157:2413-2446.
No. of antihypertensive agents1 2 3 4
DBP, diastolic blood pressure; MAP, mean arterial pressure; SBP, systolic blood pressure.1. UKPDS 38. BMJ. 1998;317:703-713.2. Estacio RO et al. Am J Cardiol. 1998;82:9R-14R.3. Lazarus JM et al. Hypertension. 1997;29:641-650.4. Hansson L et al. Lancet. 1998;351:1755-1762.
5. Kusek JW et al. Control Clin Trials. 1996;16:40S-46S.6. Lewis EJ et al. N Engl J Med. 2001;345:851-860.7. ALLHAT. JAMA. 2002;288:2998-3007.
Multiple Antihypertensive Agents Multiple Antihypertensive Agents Are Often Needed to Achieve Target BPAre Often Needed to Achieve Target BP
SBP ≤140/DBP ≤90ALLHAT7
SBP ≤135/DBP ≤85IDNT6
•MAP ≤92AASK5
DBP ≤80HOT4
MAP ≤92MDRD3
DBP <75ABCD2
DBP <85 UKPDS1
•Target BP (mm Hg)•Trial
Page 35

Benefits of Combination TherapyBenefits of Combination Therapy
1. Dollery CT. Ann Rev Pharmacol Toxicol. 1977;17:311-323. JNC VI. Arch Intern Med. 1997;157:2413-2446.
3. Skolnik NS et al. Am Fam Physician. 2000;61:3049-3056.
• Combinations of low-dose agents from different classes have been shown:
– to provide additional antihypertensive efficacy1,2
– to minimize the likelihood of dose-dependent adverse events2,3
• Patient adherence is better with once-daily dosing2
Antihypertensive Drug ClassesAntihypertensive Drug Classes
• Diuretics
• Adrenergic inhibitors (β-blockers, α-blockers, central α-agonists, combined α-β blockers, peripheral agents)
• Direct vasodilators
• CCBs (dihydropyridines, nondihydropyridines)
• ACE inhibitors
• Angiotensin II receptor antagonists
• Drug combinations
The Sixth Report of the Joint National Committee on Prevention, The Sixth Report of the Joint National Committee on Prevention, Detection, Evaluation, and Detection, Evaluation, and Treatment of High Blood PressureTreatment of High Blood Pressure. November 1997. NIH publication 98. November 1997. NIH publication 98--4080.4080.
Diuretics• Well studied: Class of agents for HTN (SHEP, ALLHAT etc), useful
in CHF• Low acquisition cost• Proven Mortality benefit (HTN) (SHEP Study)• MOA:Decrease PVR in the long term• Monitor for: Hypokalemia, hyperuracemia, hyperglycemia,
hypercalcemia, Lipids, gynecomastia (spirionlactone) etc.• Which Agent?• ClCr > 30 ml/min thiazide (all probably work equally well)• ClCr < 30 ml/min loop diuretics or combination
Diuretics in Patients With HypertensionDiuretics in Patients With Hypertension
AdvantagesAdvantages
• Clinical trials showed decr. in cardiovascular morbidity and mortality
• Efficacious in white and African American patients
• Cost-effective
DisadvantagesDisadvantages
• Require monitoring for adverse effects on serum potassium/glucose/lipids
• In high doses, incr. risk for hyperglycemia/other metabolic abnormalities
GFR= glomerular filtration rate.GFR= glomerular filtration rate.National High Blood Pressure Education Program Working Group. National High Blood Pressure Education Program Working Group. Hypertension. Hypertension. 1994;23:2751994;23:275--285.285.
ββ --Blockers for HypertensionBlockers for Hypertension
• Mechanism: reduce cardiac work by negative inotropic, negative chronotropic and hypotensive (central and renin blocking) effects
• Pharmacologic Issues: High first pass, modest half-life, variable protein binding, cardioselectivity (dose dependent), intrinsic sympathomimetic activity, alpha-blockade
• Monitor: SE’s are extension of pharmacologic effects, bradycardia, hypotension, CHF, depression abrupt withdrawal, impotence, diabetes (Signs and Symptoms) lipid effects (decrease HDL, incr. trigs), reactive airway disease
• Outcomes: Several studies on outcomes in the area of Hypertension with/without diuretics or other agents (STOP-hypertension) and with post AMI, in CHF etc.
Beta Blocking AgentsBeta Blocking Agents
Non-Selective Selective*Alpha-Blocking
Activity
NadololPropranololTimolol
PindololCarteololPenbutolol
AtenololMetoprololEsmololBetaxololBisoprolol
Acebutolol LabetalolCarvedilol
- ISA + ISA + ISA- ISA
With
*Beta-1 Cardioselective
Page 36
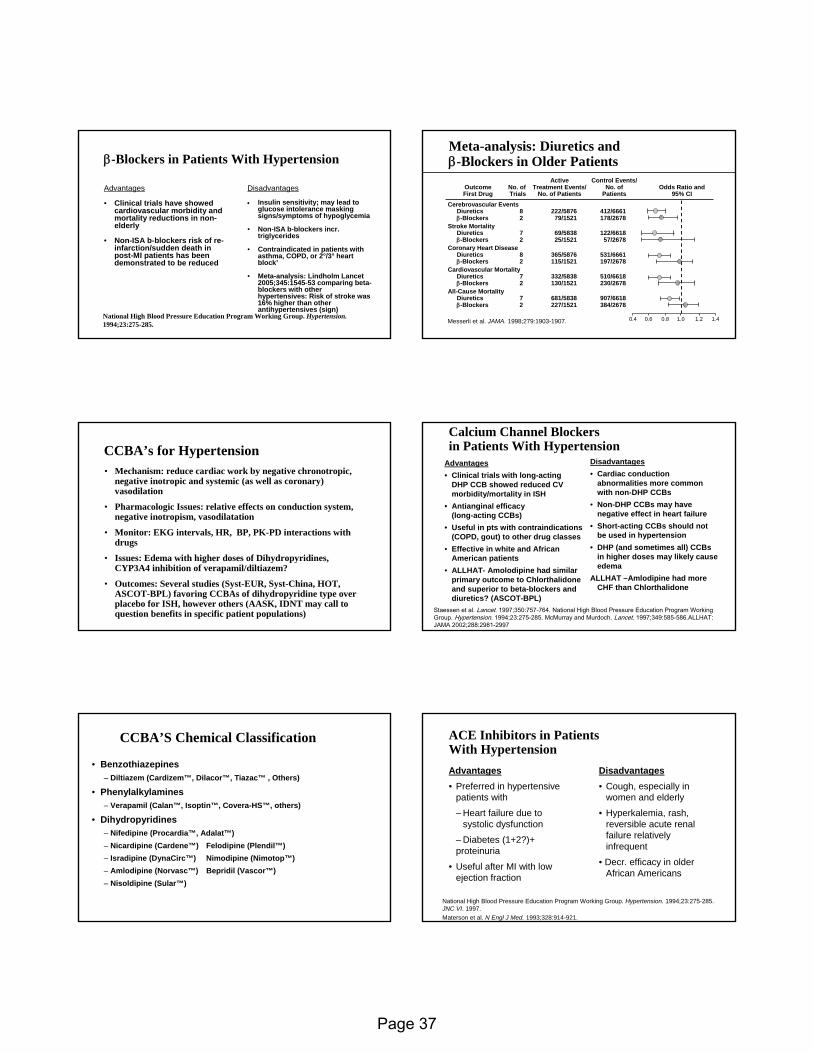
ββ--Blockers in Patients With HypertensionBlockers in Patients With Hypertension
National High Blood Pressure Education Program Working Group. National High Blood Pressure Education Program Working Group. Hypertension. Hypertension. 1994;23:2751994;23:275--285.285.
AdvantagesAdvantages
• Clinical trials have showed cardiovascular morbidity and mortality reductions in non-elderly
• Non-ISA b-blockers risk of re-infarction/sudden death in post-MI patients has been demonstrated to be reduced
DisadvantagesDisadvantages
• Insulin sensitivity; may lead to glucose intolerance masking signs/symptoms of hypoglycemia
• Non-ISA b-blockers incr. triglycerides
• Contraindicated in patients with asthma, COPD, or 2°/3° heart block’
• Meta-analysis: Lindholm Lancet 2005;345:1545-53 comparing beta-blockers with other hypertensives: Risk of stroke was 16% higher than other antihypertensives (sign)
MetaMeta--analysis: Diuretics and analysis: Diuretics and ββ--Blockers in Older PatientsBlockers in Older Patients
Control Events/No. of
Patients
ActiveTreatment Events/
No. of PatientsNo. of Trials
OutcomeFirst Drug
Odds Ratio and95% CI
0.4 0.6 0.8 1.0 1.2 1.4
Cerebrovascular EventsDiuretics 8 222/5876 412/6661β-Blockers 2 79/1521 178/2678
Stroke MortalityDiuretics 7 69/5838 122/6618β-Blockers 2 25/1521 57/2678
Coronary Heart DiseaseDiuretics 8 365/5876 531/6661β-Blockers 2 115/1521 197/2678
Cardiovascular MortalityDiuretics 7 332/5838 510/6618β-Blockers 2 130/1521 230/2678
All-Cause MortalityDiuretics 7 681/5838 907/6618β-Blockers 2 227/1521 384/2678
MesserliMesserli et al. et al. JAMA.JAMA. 1998;279:19031998;279:1903--1907.1907.
CCBA’sCCBA’s for Hypertensionfor Hypertension• Mechanism: reduce cardiac work by negative chronotropic,
negative inotropic and systemic (as well as coronary) vasodilation
• Pharmacologic Issues: relative effects on conduction system, negative inotropism, vasodilatation
• Monitor: EKG intervals, HR, BP, PK-PD interactions with drugs
• Issues: Edema with higher doses of Dihydropyridines, CYP3A4 inhibition of verapamil/diltiazem?
• Outcomes: Several studies (Syst-EUR, Syst-China, HOT, ASCOT-BPL) favoring CCBAs of dihydropyridine type over placebo for ISH, however others (AASK, IDNT may call to question benefits in specific patient populations)
DisadvantagesDisadvantages• Cardiac conduction
abnormalities more common with non-DHP CCBs
• Non-DHP CCBs may have negative effect in heart failure
• Short-acting CCBs should not be used in hypertension
• DHP (and sometimes all) CCBsin higher doses may likely cause edema
ALLHAT –Amlodipine had more CHF than Chlorthalidone
Calcium Channel BlockersCalcium Channel Blockersin Patients With Hypertensionin Patients With Hypertension
Staessen et al. Lancet. 1997;350:757-764. National High Blood Pressure Education Program Working Group. Hypertension. 1994;23:275-285. McMurray and Murdoch. Lancet. 1997;349:585-586.ALLHAT: JAMA 2002;288:2981-2997
AdvantagesAdvantages• Clinical trials with long-acting
DHP CCB showed reduced CV morbidity/mortality in ISH
• Antianginal efficacy (long-acting CCBs)
• Useful in pts with contraindications (COPD, gout) to other drug classes
• Effective in white and African American patients
• ALLHAT- Amolodipine had similar primary outcome to Chlorthalidone and superior to beta-blockers and diuretics? (ASCOT-BPL)
CCBA’S Chemical ClassificationCCBA’S Chemical Classification
• Benzothiazepines– Diltiazem (Cardizem™, Dilacor™, Tiazac™ , Others)
• Phenylalkylamines– Verapamil (Calan™, Isoptin™, Covera-HS™, others)
• Dihydropyridines– Nifedipine (Procardia™, Adalat™)– Nicardipine (Cardene™) Felodipine (Plendil™)– Isradipine (DynaCirc™) Nimodipine (Nimotop™)– Amlodipine (Norvasc™) Bepridil (Vascor™)– Nisoldipine (Sular™)
ACE Inhibitors in Patients ACE Inhibitors in Patients With HypertensionWith Hypertension
National High Blood Pressure Education Program Working Group. National High Blood Pressure Education Program Working Group. Hypertension. Hypertension. 1994;23:2751994;23:275--285. 285. JNC VIJNC VI. 1997. . 1997. MatersonMaterson et al. et al. N N EnglEngl J Med.J Med. 1993;328:9141993;328:914--921.921.
AdvantagesAdvantages• Preferred in hypertensive
patients with
– Heart failure due to systolic dysfunction
– Diabetes (1+2?)+ proteinuria
• Useful after MI with low ejection fraction
DisadvantagesDisadvantages• Cough, especially in
women and elderly
• Hyperkalemia, rash, reversible acute renal failure relatively infrequent
• Decr. efficacy in older African Americans
Page 37
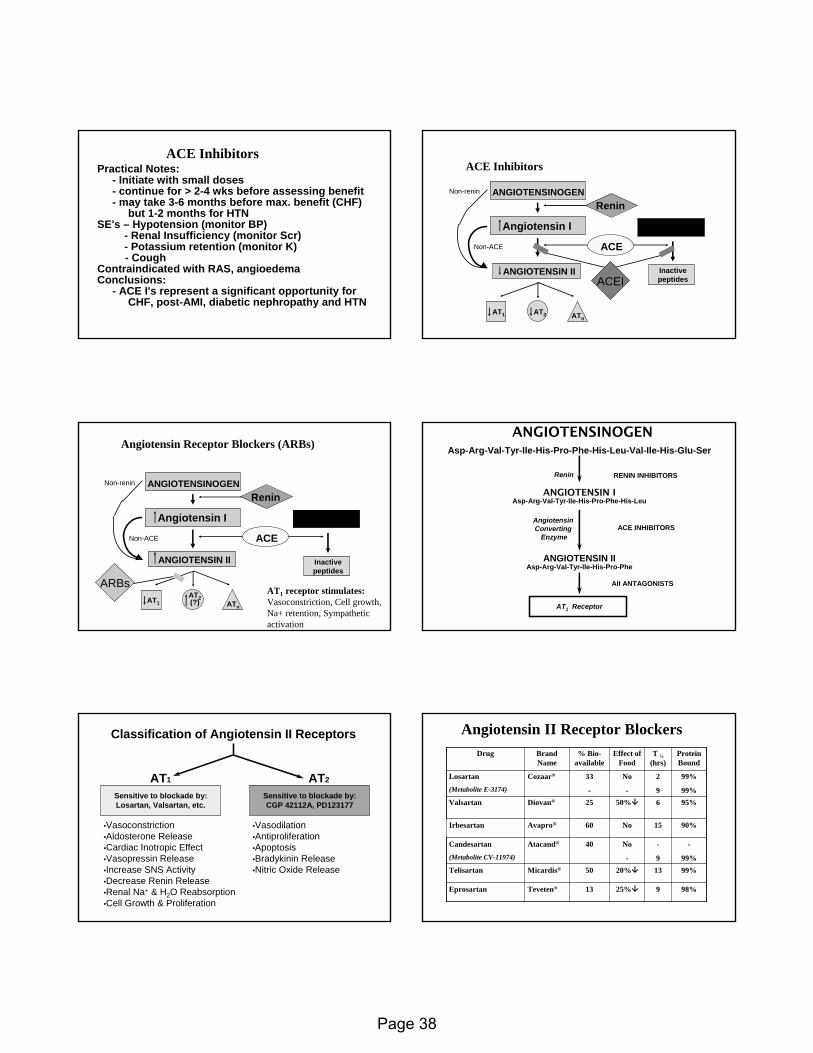
ACE InhibitorsACE InhibitorsPractical Notes:Practical Notes:
-- Initiate with small dosesInitiate with small doses-- continue for > 2continue for > 2--4 wks before assessing benefit4 wks before assessing benefit-- may take 3may take 3--6 months before max. benefit (CHF)6 months before max. benefit (CHF)
but 1but 1--2 months for HTN2 months for HTNSE'sSE's –– Hypotension (monitor BP)Hypotension (monitor BP)
-- Renal Insufficiency (monitor Renal Insufficiency (monitor ScrScr))-- Potassium retention (monitor K)Potassium retention (monitor K)-- CoughCough
Contraindicated with RAS, Contraindicated with RAS, angioedemaangioedemaConclusions:Conclusions:
-- ACE ACE I'sI's represent a significant opportunity forrepresent a significant opportunity forCHF, postCHF, post--AMI, diabetic nephropathy and HTN AMI, diabetic nephropathy and HTN
ACE InhibitorsACE Inhibitors
ANGIOTENSINOGEN
Angiotensin I
ANGIOTENSIN II Inactivepeptides
Renin
ACE
Non-renin
Non-ACE
Bradykinin
ACEI
AT1 AT2 ATn
Angiotensin Receptor Blockers (ARBs)Angiotensin Receptor Blockers (ARBs)
ANGIOTENSINOGEN
Angiotensin I
ANGIOTENSIN II Inactivepeptides
Renin
ACE
Non-renin
Non-ACE
Bradykinin
AT1AT2(?) ATn
ARBsAT1 receptor stimulates:Vasoconstriction, Cell growth, Na+ retention, Sympathetic activation
ANGIOTENSINOGENANGIOTENSINOGEN
ANGIOTENSIN I
ANGIOTENSIN II
Asp-Arg-Val-Tyr-Ile-His-Pro-Phe-His-Leu-Val-Ile-His-Glu-Ser
Asp-Arg-Val-Tyr-Ile-His-Pro-Phe-His-Leu
Asp-Arg-Val-Tyr-Ile-His-Pro-Phe
Angiotensin Converting
Enzyme
Renin
AT1 Receptor
RENIN INHIBITORS
ACE INHIBITORS
AII ANTAGONISTS
Classification of Angiotensin II Receptors
Sensitive to blockade by:Losartan, Valsartan, etc.
AT2AT1
Sensitive to blockade by:CGP 42112A, PD123177
•Vasoconstriction•Aldosterone Release•Cardiac Inotropic Effect•Vasopressin Release•Increase SNS Activity•Decrease Renin Release•Renal Na+ & H2O Reabsorption•Cell Growth & Proliferation
•Vasodilation•Antiproliferation•Apoptosis•Bradykinin Release•Nitric Oxide Release
Angiotensin II Receptor BlockersAngiotensin II Receptor Blockers
98%98%9925%25%1313TevetenTeveten®®EprosartanEprosartan
99%99%131320%20%5050MicardisMicardis®®TelisartanTelisartan
--
99%99%
--
99
NoNo
--
4040AtacandAtacand®®CandesartanCandesartan
(Metabolite CV(Metabolite CV--11974)11974)
90%90%1515NoNo6060AvaproAvapro®®IrbesartanIrbesartan
95%95%6650%50%2525DiovanDiovan®®ValsartanValsartan
99%99%
99%99%
22
99
NoNo
--
3333
--
CozaarCozaar®®LosartanLosartan
(Metabolite E(Metabolite E--3174)3174)
Protein Protein BoundBound
T T ½½(hrs)(hrs)
Effect of Effect of FoodFood
% Bio% Bio--availableavailable
Brand Brand NameName
DrugDrug
Page 38
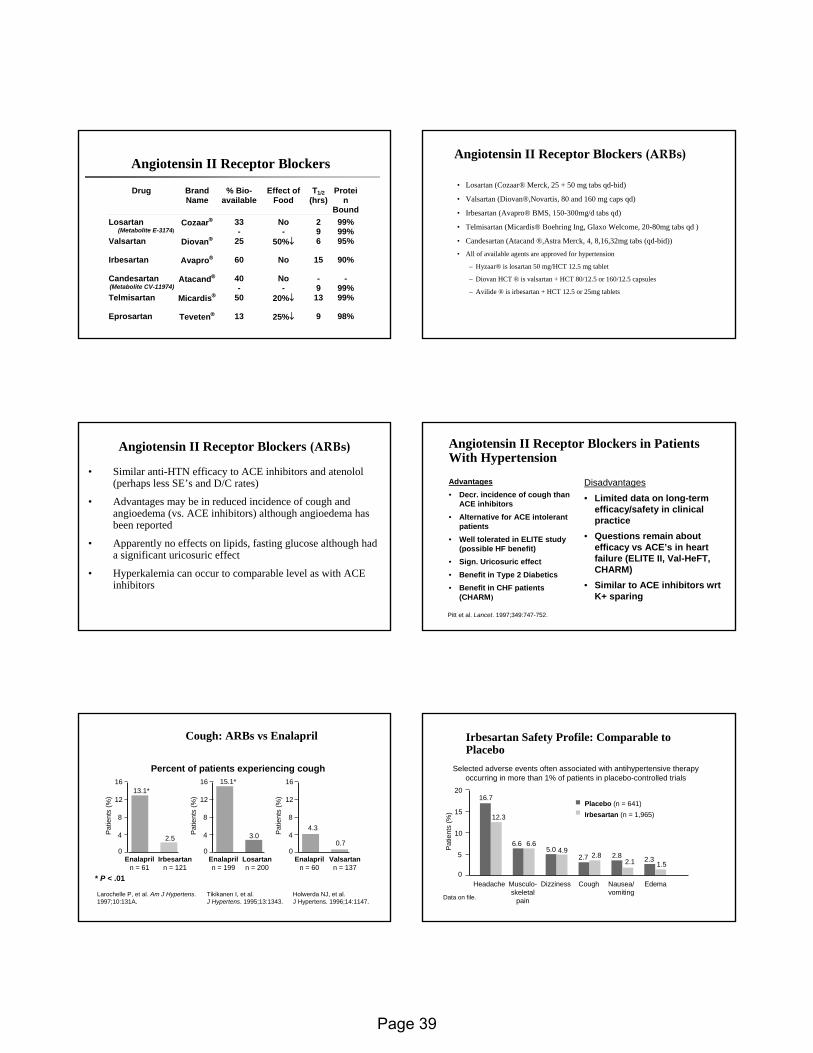
Angiotensin II Receptor BlockersAngiotensin II Receptor Blockers
Drug Brand Name
% Bio- available
Effect of Food
T1/2 (hrs)
Protein
BoundLosartan
(Metabolite E-3174) Cozaar® 33
- No -
2 9
99% 99%
Valsartan Diovan® 25 50%↓ 6 95%
Irbesartan Avapro® 60 No 15 90%
Candesartan (Metabolite CV-11974)
Atacand® 40 -
No -
- 9
- 99%
Telmisartan Micardis® 50 20%↓ 13 99%
Eprosartan Teveten® 13 25%↓ 9 98%
Angiotensin II Receptor Blockers Angiotensin II Receptor Blockers (ARBs)(ARBs)
• Losartan (Cozaar® Merck, 25 + 50 mg tabs qd-bid)
• Valsartan (Diovan®,Novartis, 80 and 160 mg caps qd)
• Irbesartan (Avapro® BMS, 150-300mg/d tabs qd)
• Telmisartan (Micardis® Boehring Ing, Glaxo Welcome, 20-80mg tabs qd )
• Candesartan (Atacand ®,Astra Merck, 4, 8,16,32mg tabs (qd-bid))
• All of available agents are approved for hypertension
– Hyzaar® is losartan 50 mg/HCT 12.5 mg tablet
– Diovan HCT ® is valsartan + HCT 80/12.5 or 160/12.5 capsules
– Avilide ® is irbesartan + HCT 12.5 or 25mg tablets
Angiotensin II Receptor Blockers Angiotensin II Receptor Blockers (ARBs)(ARBs)
• Similar anti-HTN efficacy to ACE inhibitors and atenolol (perhaps less SE’s and D/C rates)
• Advantages may be in reduced incidence of cough and angioedema (vs. ACE inhibitors) although angioedema has been reported
• Apparently no effects on lipids, fasting glucose although had a significant uricosuric effect
• Hyperkalemia can occur to comparable level as with ACE inhibitors
Angiotensin II Receptor Blockers in Patients Angiotensin II Receptor Blockers in Patients With HypertensionWith Hypertension
Pitt et al. Pitt et al. LancetLancet. 1997;349:747. 1997;349:747--752.752.
AdvantagesAdvantages• Decr. incidence of cough than
ACE inhibitors• Alternative for ACE intolerant
patients • Well tolerated in ELITE study
(possible HF benefit)• Sign. Uricosuric effect• Benefit in Type 2 Diabetics• Benefit in CHF patients
(CHARM)
DisadvantagesDisadvantages
• Limited data on long-term efficacy/safety in clinical practice
• Questions remain about efficacy vs ACE’s in heart failure (ELITE II, Val-HeFT, CHARM)
• Similar to ACE inhibitors wrtK+ sparing
Cough: ARBs Cough: ARBs vsvs EnalaprilEnalapril
Percent of patients experiencing cough16
12
8
4
0
16
12
8
4
0
16
12
8
4
00.7
4.33.0
15.1*13.1*
2.5
Pat
ient
s (%
)
Pat
ient
s (%
)
Pat
ient
s (%
)
Enalapriln = 61
Irbesartann = 121
Enalapriln = 199
Losartann = 200
Enalapriln = 60
Valsartann = 137
* P < .01
Larochelle P, et al. Am J Hypertens.1997;10:131A.
Tikikanen I, et al.J Hypertens. 1995;13:1343.
Holwerda NJ, et al.J Hypertens. 1996;14:1147.
Irbesartan Safety Profile: Comparable to Irbesartan Safety Profile: Comparable to PlaceboPlacebo
20
15
10
5
0
16.7
Pat
ient
s (%
)
Headache
Placebo (n = 641)Irbesartan (n = 1,965)
Data on file.
Selected adverse events often associated with antihypertensive therapyoccurring in more than 1% of patients in placebo-controlled trials
12.3
6.6 6.65.0 4.9
2.7 2.8 2.82.1 2.3
1.5
Musculo-skeletal
pain
Dizziness Cough Nausea/vomiting
Edema
Page 39
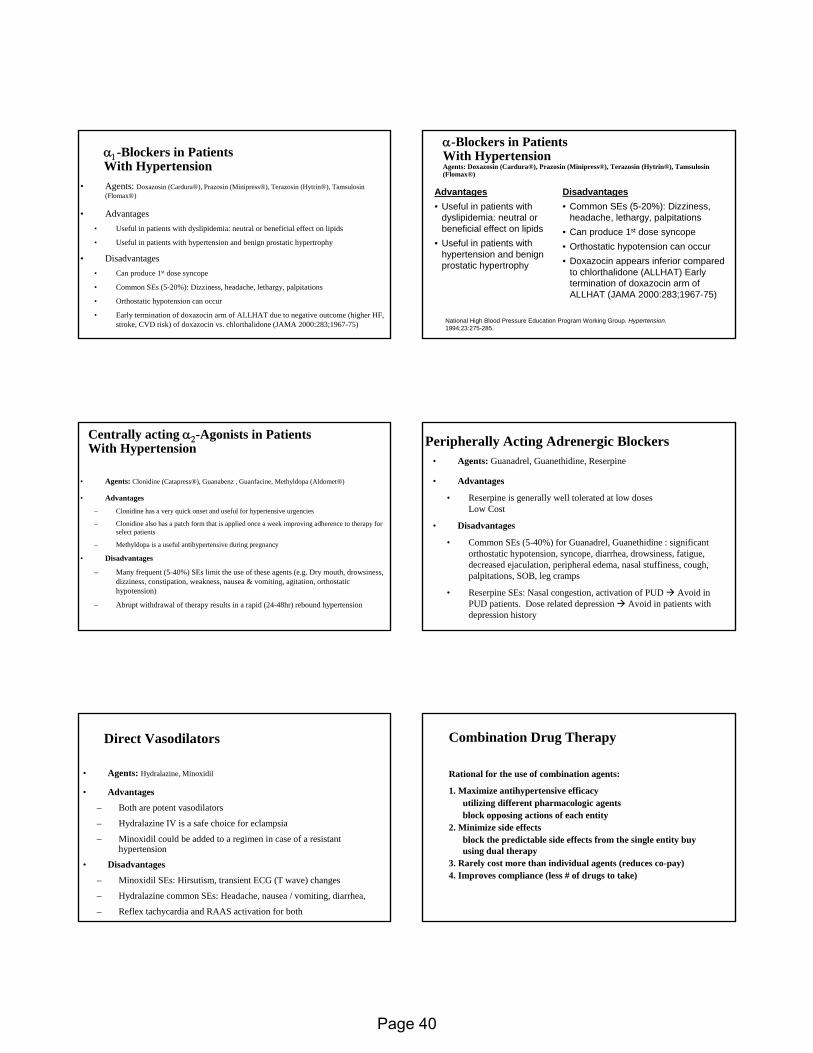
αα11--Blockers in Patients Blockers in Patients With HypertensionWith Hypertension
•• Agents: Agents: DoxazosinDoxazosin ((CarduraCardura®), ®), PrazosinPrazosin ((MinipressMinipress®), ®), TerazosinTerazosin ((HytrinHytrin®), ®), TamsulosinTamsulosin((FlomaxFlomax®)®)
•• AdvantagesAdvantages• Useful in patients with dyslipidemia: neutral or beneficial effect on lipids
• Useful in patients with hypertension and benign prostatic hypertrophy
•• DisadvantagesDisadvantages• Can produce 1st dose syncope
• Common SEs (5-20%): Dizziness, headache, lethargy, palpitations
• Orthostatic hypotension can occur
• Early termination of doxazocin arm of ALLHAT due to negative outcome (higher HF, stroke, CVD risk) of doxazocin vs. chlorthalidone (JAMA 2000:283;1967-75)
αα--Blockers in Patients Blockers in Patients With HypertensionWith HypertensionAgents: Agents: DoxazosinDoxazosin ((CarduraCardura®), ®), PrazosinPrazosin ((MinipressMinipress®), ®), TerazosinTerazosin ((HytrinHytrin®), ®), TamsulosinTamsulosin((FlomaxFlomax®)®)
AdvantagesAdvantages• Useful in patients with
dyslipidemia: neutral or beneficial effect on lipids
• Useful in patients with hypertension and benign prostatic hypertrophy
DisadvantagesDisadvantages• Common SEs (5-20%): Dizziness,
headache, lethargy, palpitations• Can produce 1st dose syncope• Orthostatic hypotension can occur• Doxazocin appears inferior compared
to chlorthalidone (ALLHAT) Early termination of doxazocin arm of ALLHAT (JAMA 2000:283;1967-75)
National High Blood Pressure Education Program Working Group. National High Blood Pressure Education Program Working Group. Hypertension. Hypertension. 1994;23:2751994;23:275--285.285.
Centrally acting Centrally acting αα22--Agonists in Patients Agonists in Patients With HypertensionWith Hypertension
•• Agents: Agents: Clonidine (Clonidine (CatapressCatapress®), ®), GuanabenzGuanabenz , , GuanfacineGuanfacine, Methyldopa (, Methyldopa (AldometAldomet®)®)
•• AdvantagesAdvantages
– Clonidine has a very quick onset and useful for hypertensive urgencies
– Clonidine also has a patch form that is applied once a week improving adherence to therapy for select patients
– Methyldopa is a useful antihypertensive during pregnancy
•• DisadvantagesDisadvantages
– Many frequent (5-40%) SEs limit the use of these agents (e.g. Dry mouth, drowsiness, dizziness, constipation, weakness, nausea & vomiting, agitation, orthostatic hypotension)
– Abrupt withdrawal of therapy results in a rapid (24-48hr) rebound hypertension
Peripherally Acting Adrenergic BlockersPeripherally Acting Adrenergic Blockers•• Agents: Agents: Guanadrel, Guanethidine, ReserpineGuanadrel, Guanethidine, Reserpine
•• AdvantagesAdvantages
• Reserpine is generally well tolerated at low dosesLow Cost
•• DisadvantagesDisadvantages
• Common SEs (5-40%) for Guanadrel, GuanethidineGuanadrel, Guanethidine : significant orthostatic hypotension, syncope, diarrhea, drowsiness, fatigue,decreased ejaculation, peripheral edema, nasal stuffiness, cough, palpitations, SOB, leg cramps
• Reserpine SEs: Nasal congestion, activation of PUD Avoid in PUD patients. Dose related depression Avoid in patients with depression history
Direct VasodilatorsDirect Vasodilators
•• Agents: Agents: Hydralazine, MinoxidilHydralazine, Minoxidil
•• AdvantagesAdvantages
– Both are potent vasodilators
– Hydralazine IV is a safe choice for eclampsia
– Minoxidil could be added to a regimen in case of a resistant hypertension
•• DisadvantagesDisadvantages
– Minoxidil SEs: Hirsutism, transient ECG (T wave) changes
– Hydralazine common SEs: Headache, nausea / vomiting, diarrhea,
– Reflex tachycardia and RAAS activation for both
Combination Drug TherapyCombination Drug Therapy
Rational for the use of combination agents:
1. Maximize antihypertensive efficacyutilizing different pharmacologic agentsblock opposing actions of each entity
2. Minimize side effectsblock the predictable side effects from the single entity buy using dual therapy
3. Rarely cost more than individual agents (reduces co-pay)4. Improves compliance (less # of drugs to take)
Page 40
Summary by Drug ClassSummary by Drug Class• Diuretics:
- Supported by JNC 7 and evidence (SHEP, STOP-HTN ALLHAT etc.)• Beta-Blockers
- Supported by JNC VI and evidence (SHEP, STOP-HTN etc.)- Supported by evidence of co-morbidities (AMI, CHF)
• ACE Inhibitors: - Supported by ADA Guidelines (general for Diabetics) and Evidence (HOPE, AASK)
• Calcium Channel Blockers- Supported by Evidence (Syst-Eur, Syst- China, ASCOT-BPL)
• ARBs:- Supported by guidelines (ADA for type 2 diabetics with microalbuminuria-IDNT, IRMA 2, RENAAL), Alternative to ACE inhibitors for CHF (if intolerant to ACE I’s, some comparative HTN data with b-blockers-LIFE)
• Others:- alpha blockers (not for HTN only- ALLHAT)
Essentials of Hypertension:Essentials of Hypertension:SummarySummary
• Fundamental basis for aggressive management of blood pressure is established
• Guidelines for selection of drug classes must be considered as guide for most patients
• Special populations (Elderly, Diabetics) may require specific approaches with multiple drugs
• Too many patients are less than optimally managed for hypertension and other risk factors for CVD
Page 41
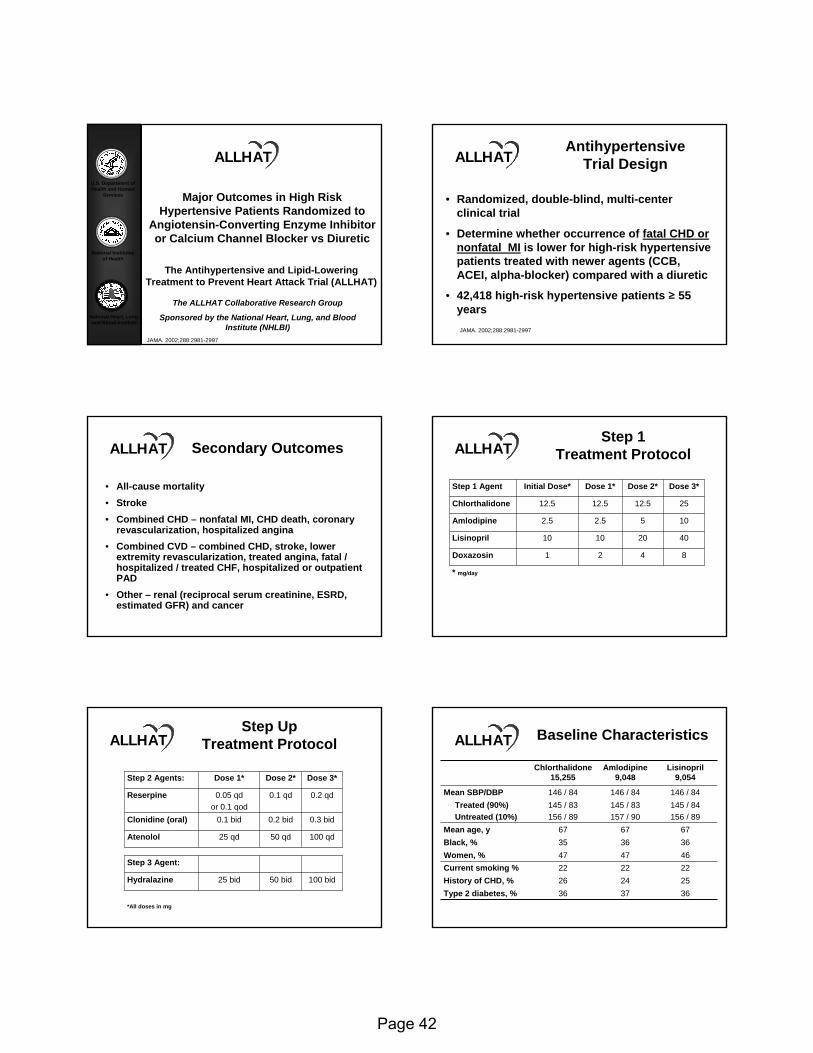
U.S. Department of Health and Human
Services
National Institutes of Health
National Heart, Lung, and Blood Institute
Major Outcomes in High Risk Hypertensive Patients Randomized to
Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic
The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT)
The ALLHAT Collaborative Research Group
Sponsored by the National Heart, Lung, and Blood Institute (NHLBI)
ALLHAT
JAMA. 2002;288:2981-2997
AntihypertensiveTrial Design
• Randomized, double-blind, multi-center clinical trial
• Determine whether occurrence of fatal CHD or nonfatal MI is lower for high-risk hypertensive patients treated with newer agents (CCB, ACEI, alpha-blocker) compared with a diuretic
• 42,418 high-risk hypertensive patients ≥ 55 years
ALLHAT
JAMA. 2002;288:2981-2997
Secondary Outcomes
• All-cause mortality• Stroke• Combined CHD – nonfatal MI, CHD death, coronary
revascularization, hospitalized angina• Combined CVD – combined CHD, stroke, lower
extremity revascularization, treated angina, fatal / hospitalized / treated CHF, hospitalized or outpatient PAD
• Other – renal (reciprocal serum creatinine, ESRD, estimated GFR) and cancer
ALLHATStep 1
Treatment Protocol
8421Doxazosin
* mg/day
40201010Lisinopril
1052.52.5Amlodipine
2512.512.512.5Chlorthalidone
Dose 3*Dose 2*Dose 1*Initial Dose*Step 1 Agent
ALLHAT
100 bid50 bid25 bidHydralazine
*All doses in mg
Step 3 Agent:
100 qd50 qd25 qdAtenolol
0.3 bid0.2 bid0.1 bidClonidine (oral)
0.2 qd0.1 qd0.05 qdor 0.1 qod
Reserpine
Dose 3*Dose 2*Dose 1*Step 2 Agents:
ALLHATStep Up
Treatment Protocol Baseline Characteristics
145 / 84156 / 89
145 / 83157 / 90
145 / 83156 / 89
Treated (90%)Untreated (10%)
372422473667
146 / 84
Amlodipine 9,048
146 / 84146 / 84Mean SBP/DBP
3636Type 2 diabetes, %2526History of CHD, %2222Current smoking %4647Women, %3635Black, %6767Mean age, y
Lisinopril 9,054
Chlorthalidone 15,255
ALLHAT
Page 42
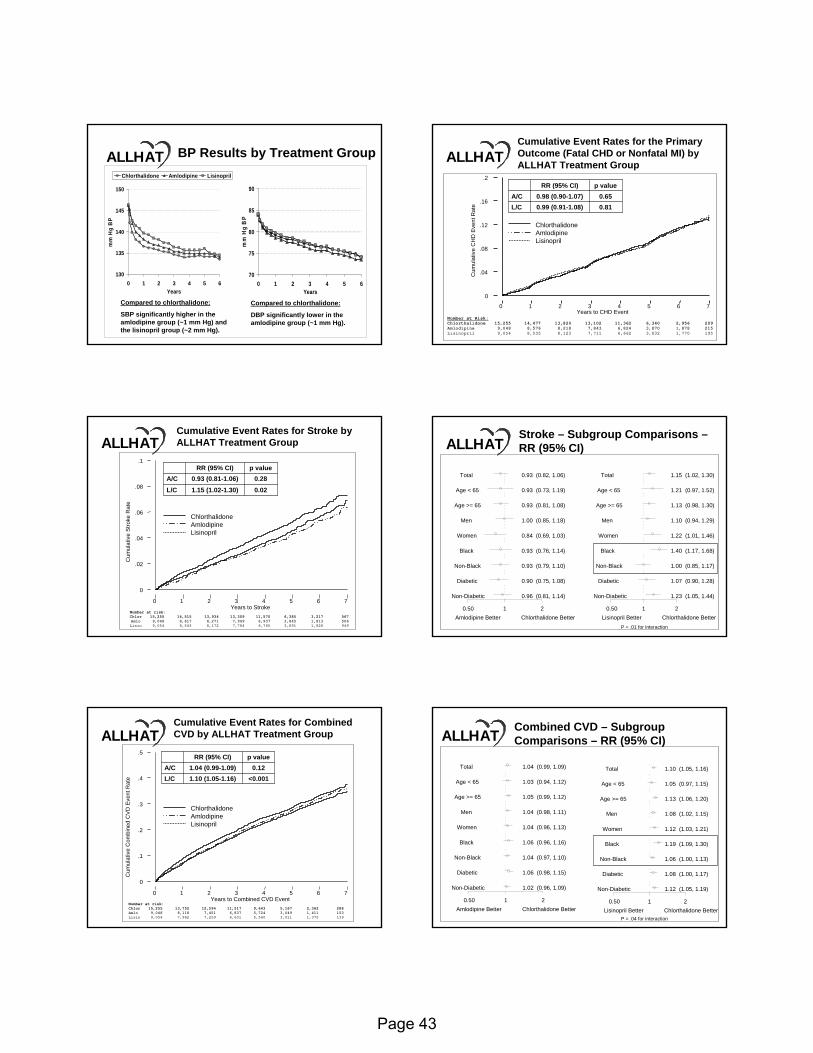
BP Results by Treatment Group
130
135
140
145
150
0 1 2 3 4 5 6Years
mm
Hg
BP
Chlorthalidone Amlodipine Lisinopril
Compared to chlorthalidone:
SBP significantly higher in the amlodipine group (~1 mm Hg) and the lisinopril group (~2 mm Hg).
70
75
80
85
90
0 1 2 3 4 5 6Years
mm
Hg
BP
Compared to chlorthalidone:
DBP significantly lower in the amlodipine group (~1 mm Hg).
ALLHAT
Years to CHD Event0 1 2 3 4 5 6 7
Cum
ulat
ive
CH
D E
vent
Rat
e
0
.04
.08
.12
.16
.2
Number at Risk:Chlorthalidone 15,255 14,477 13,820 13,102 11,362 6,340 2,956 209 Amlodipine 9,048 8,576 8,218 7,843 6,824 3,870 1,878 215 Lisinopril 9,054 8,535 8,123 7,711 6,662 3,832 1,770 195
Cumulative Event Rates for the Primary Outcome (Fatal CHD or Nonfatal MI) by ALLHAT Treatment Group
0.810.99 (0.91-1.08)L/C0.650.98 (0.90-1.07)A/C
p valueRR (95% CI)
ALLHAT
ChlorthalidoneAmlodipineLisinopril
Cum
ulat
ive
Stro
ke R
ate
Years to Stroke0 1 2 3 4 5 6 7
0
.02
.04
.06
.08
.1
Number at risk: Chlor 15,255 14,515 13,934 13,309 11,570 6,385 3,217 567 Amlo 9,048 8,617 8,271 7,949 6,937 3,845 1,813 506 Lisin 9,054 8,543 8,172 7,784 6,765 3,891 1,828 949
Cumulative Event Rates for Stroke by ALLHAT Treatment Group
0.021.15 (1.02-1.30)L/C0.280.93 (0.81-1.06)A/C
p valueRR (95% CI)
ALLHAT
ChlorthalidoneAmlodipineLisinopril
Stroke – Subgroup Comparisons –RR (95% CI)
Amlodipine Better Chlorthalidone Better0.50 1 2
Non-Diabetic 0.96 (0.81, 1.14)
Diabetic 0.90 (0.75, 1.08)
Non-Black 0.93 (0.79, 1.10)
Black 0.93 (0.76, 1.14)
Women 0.84 (0.69, 1.03)
Men 1.00 (0.85, 1.18)
Age >= 65 0.93 (0.81, 1.08)
Age < 65 0.93 (0.73, 1.19)
Total 0.93 (0.82, 1.06)
Lisinopril Better Chlorthalidone Better0.50 1 2
Non-Diabetic 1.23 (1.05, 1.44)
Diabetic 1.07 (0.90, 1.28)
Non-Black 1.00 (0.85, 1.17)
Black 1.40 (1.17, 1.68)
Women 1.22 (1.01, 1.46)
Men 1.10 (0.94, 1.29)
Age >= 65 1.13 (0.98, 1.30)
Age < 65 1.21 (0.97, 1.52)
Total 1.15 (1.02, 1.30)
ALLHAT
P = .01 for interaction
Cum
ulat
ive
Com
bine
d C
VD
Eve
nt R
ate
Years to Combined CVD Event0 1 2 3 4 5 6 7
0
.1
.2
.3
.4
.5
Number at risk: Chlor 15,255 13,752 12,594 11,517 9,643 5,167 2,362 288 Amlo 9,048 8,118 7,451 6,837 5,724 3,049 1,411 153 Lisin 9,054 7,962 7,259 6,631 5,560 3,011 1,375 139
Cumulative Event Rates for Combined CVD by ALLHAT Treatment Group
<0.0011.10 (1.05-1.16)L/C0.121.04 (0.99-1.09)A/C
p valueRR (95% CI)
ALLHAT
ChlorthalidoneAmlodipineLisinopril
Combined CVD – Subgroup Comparisons – RR (95% CI)
Amlodipine Better Chlorthalidone Better0.50 1 2
Non-Diabetic 1.02 (0.96, 1.09)
Diabetic 1.06 (0.98, 1.15)
Non-Black 1.04 (0.97, 1.10)
Black 1.06 (0.96, 1.16)
Women 1.04 (0.96, 1.13)
Men 1.04 (0.98, 1.11)
Age >= 65 1.05 (0.99, 1.12)
Age < 65 1.03 (0.94, 1.12)
Total 1.04 (0.99, 1.09)
Lisinopril Better Chlorthalidone Better0.50 1 2
Non-Diabetic 1.12 (1.05, 1.19)
Diabetic 1.08 (1.00, 1.17)
Non-Black 1.06 (1.00, 1.13)
Black 1.19 (1.09, 1.30)
Women 1.12 (1.03, 1.21)
Men 1.08 (1.02, 1.15)
Age >= 65 1.13 (1.06, 1.20)
Age < 65 1.05 (0.97, 1.15)
Total 1.10 (1.05, 1.16)
ALLHAT
P = .04 for interaction
Page 43
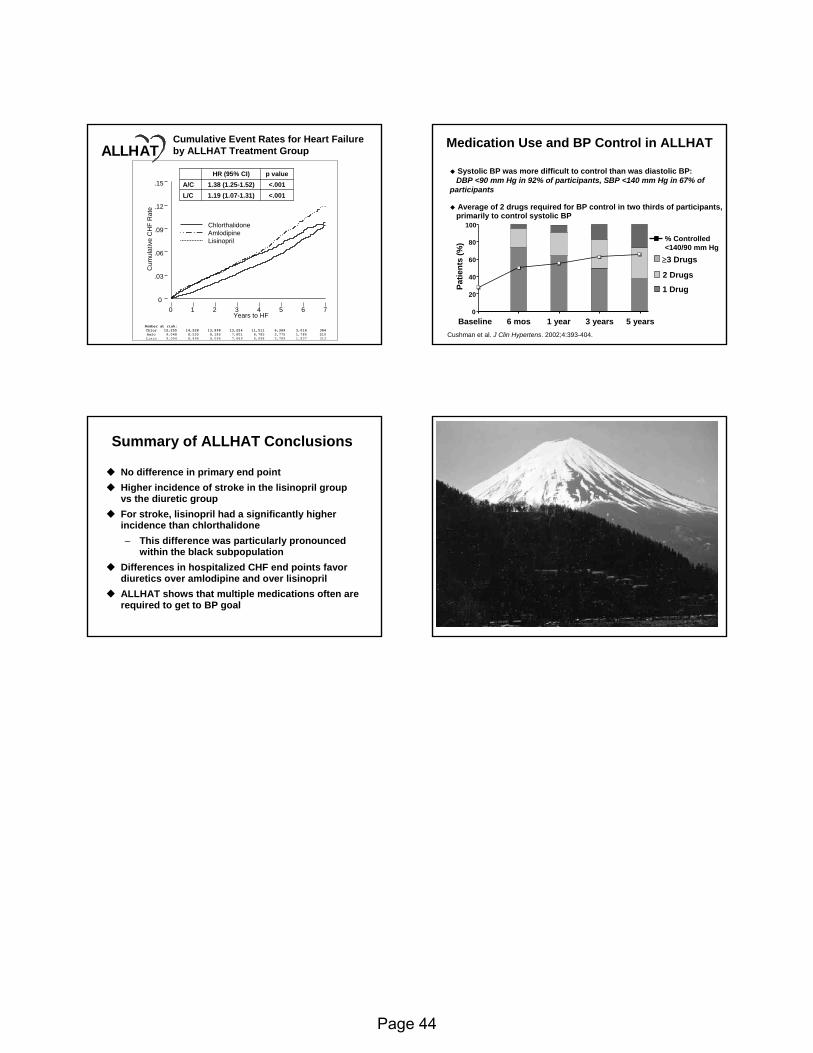
Cum
ulat
ive
CH
F R
ate
Years to HF0 1 2 3 4 5 6 7
0
.03
.06
.09
.12
.15
Cumulative Event Rates for Heart Failure by ALLHAT Treatment Group
<.0011.19 (1.07-1.31)L/C<.0011.38 (1.25-1.52)A/C
p valueHR (95% CI)
ALLHAT
ChlorthalidoneAmlodipineLisinopril
Number at risk: Chlor 15,255 14,528 13,898 13,224 11,511 6,369 3,016 384 Amlo 9,048 8,535 8,185 7,801 6,785 3,775 1,780 210 Lisin 9,054 8,496 8,096 7,689 6,698 3,789 1,837 313
Medication Use and BP Control in ALLHAT
Cushman et al. Cushman et al. J J ClinClin HypertensHypertens. 2002;4:393. 2002;4:393--404. 404.
BaselineBaseline 6 6 mosmos 1 year1 year 3 years3 years 5 years5 years
1 Drug1 Drug2 Drugs2 Drugs
≥≥3 Drugs3 Drugs
% Controlled <140/90 mm Hg
Patie
nts
(%)
Patie
nts
(%)
0
20
40
60
80
100
Systolic BP was more difficult to control than was diastolic BP:Systolic BP was more difficult to control than was diastolic BP:DBP <90 mm Hg in 92% of participants, SBP <140 mm Hg in 67% oDBP <90 mm Hg in 92% of participants, SBP <140 mm Hg in 67% of f
participantsparticipants
Average of 2 drugs required for BP control in two thirds of partAverage of 2 drugs required for BP control in two thirds of participants, icipants, primarily to control systolic BPprimarily to control systolic BP
Summary of ALLHAT Conclusions
No difference in primary end pointNo difference in primary end pointHigher incidence of stroke in the Higher incidence of stroke in the lisinoprillisinopril group group vsvs the diuretic groupthe diuretic groupFor stroke, For stroke, lisinoprillisinopril had a significantly higher had a significantly higher incidence than chlorthalidoneincidence than chlorthalidone– This difference was particularly pronounced
within the black subpopulation Differences in hospitalized CHF end points favor Differences in hospitalized CHF end points favor diuretics over amlodipine and over diuretics over amlodipine and over lisinoprillisinoprilALLHAT shows that multiple medications often are ALLHAT shows that multiple medications often are required to get to BP goalrequired to get to BP goal
Page 44
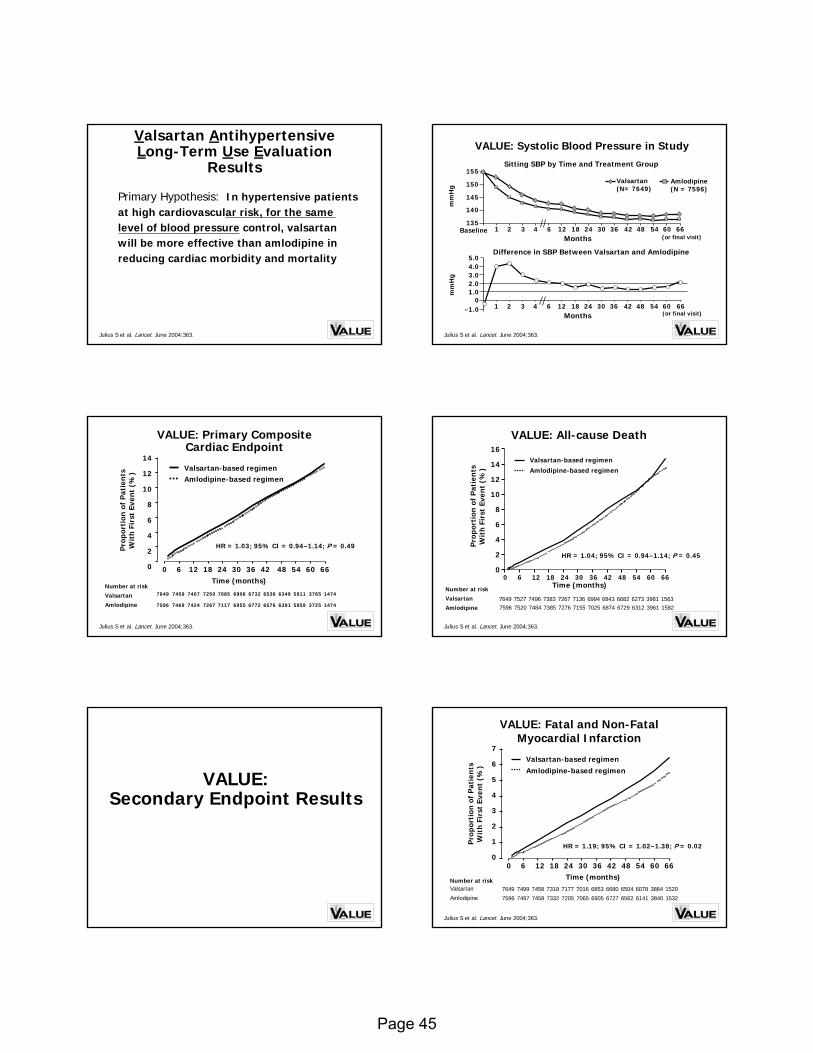
Primary Hypothesis: In hypertensive patients at high cardiovascular risk, for the same level of blood pressure control, valsartanwill be more effective than amlodipine in reducing cardiac morbidity and mortality
Valsartan Antihypertensive Long-Term Use Evaluation
ResultsResults
Julius S et al. Lancet. June 2004;363.
VALUE: Systolic Blood Pressure in Study
Julius S et al. Lancet. June 2004;363.
Valsartan (N= 7649)
Amlodipine (N = 7596)
135
140
145
150
155
mm
Hg
Months
Sitting SBP by Time and Treatment Group
Baseline 1 24 482 3 4 6 12 18 30 36 42 54 60 66
01.02.03.04.0
1 24 48
mm
Hg
2 3 4 6 12 18 30 36 42 54 60 66Months
5.0Difference in SBP Between Valsartan and Amlodipine
–1.0
(or final visit)
(or final visit)
VALUE: Primary Composite Cardiac Endpoint
14
12
10
8
6
4
2
0
Time (months)0 6 12 18 24 30 36 42 48 54 60 66
Pro
por
tion
of
Pat
ien
ts
Wit
h F
irst
Eve
nt
(%) Valsartan-based regimen
Amlodipine-based regimen
HR = 1.03; 95% CI = 0.94–1.14; P = 0.49
Julius S et al. Lancet. June 2004;363.
Number at risk
Valsartan
Amlodipine 7596
7649
7469
7459
7424
7407
7267
7250
7117
7085
6772
6732
6955
6906
6576
6536
5959
5911
3725
3765
1474
1474
6391
6349Number at risk
Valsartan
Amlodipine 75967649
75207527
74847496
73857383
72767267
70256994
71557136
68746843
63126273
39613981
15821563
67296682
VALUE: All-cause Death
Time (months)0 6 12 18 24 30 36 42 48 54 60 66
Pro
por
tion
of
Pat
ien
ts
Wit
h F
irst
Eve
nt
(%)
16
14
12
10
8
6
4
2
0
Valsartan-based regimenAmlodipine-based regimen
HR = 1.04; 95% CI = 0.94–1.14; P = 0.45
Julius S et al. Lancet. June 2004;363.
VALUE:VALUE:Secondary Endpoint ResultsSecondary Endpoint Results
Time (months)Number at riskValsartan
Amlodipine 7596
7649
7497
7499
7458
7458
7332
7319
7205
7177
6905
6853
7065
7016
6727
6680
6141
6078
3840
3864
1532
1520
6562
6504
Pro
por
tion
of
Pat
ien
ts
Wit
h F
irst
Eve
nt
(%)
7
6
5
4
3
2
1
0
VALUE: Fatal and Non-FatalMyocardial Infarction
0 6 12 18 24 30 36 42 48 54 60 66
Valsartan-based regimenAmlodipine-based regimen
HR = 1.19; 95% CI = 1.02–1.38; P = 0.02
Julius S et al. Lancet. June 2004;363.
Page 45
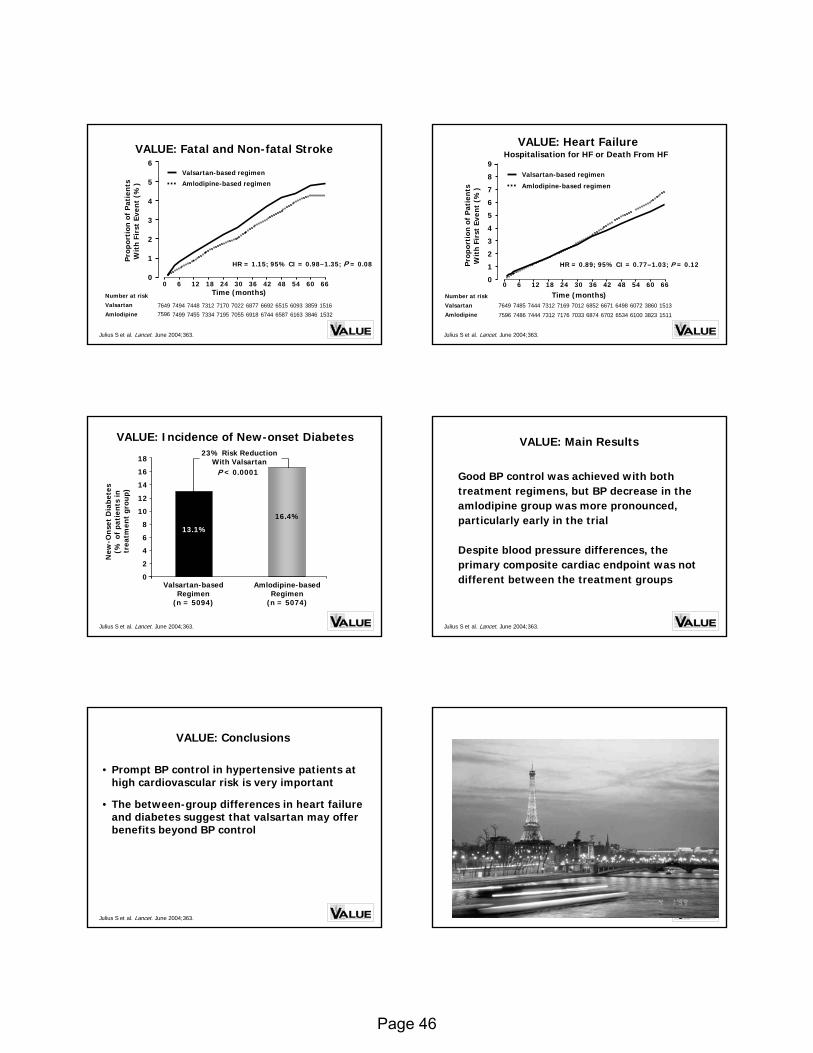
VALUE: Fatal and Non-fatal Stroke
Julius S et al. Lancet. June 2004;363.
Number at risk
Valsartan
Amlodipine 75967649
7499
7494
7455
7448
7334
7312
7195
7170
6918
6877
7055
7022
6744
6692
6163
6093
3846
3859
1532
1516
6587
6515
6
5
4
3
2
1
0
Time (months)0 6 12 18 24 30 36 42 48 54 60 66
Pro
por
tion
of
Pat
ien
ts
Wit
h F
irst
Eve
nt
(%)
Valsartan-based regimen
Amlodipine-based regimen
HR = 1.15; 95% CI = 0.98–1.35; P = 0.08
Number at risk
Valsartan
Amlodipine 7596
7649
7486
7485
7444
7444
7312
7312
7176
7169
6874
6852
7033
7012
6702
6671
6100
6072
3823
3860
1511
1513
6534
6498
VALUE: Heart Failure
Time (months)0 6 12 18 24 30 36 42 48 54 60 66
9
8
7
6
5
4
3
2
1
0
Valsartan-based regimen
Amlodipine-based regimen
HR = 0.89; 95% CI = 0.77–1.03; P = 0.12Pro
por
tion
of
Pat
ien
ts
Wit
h F
irst
Eve
nt
(%)
Julius S et al. Lancet. June 2004;363.
Hospitalisation for HF or Death From HF
VALUE: Incidence of NewVALUE: Incidence of New--onset Diabetesonset Diabetes
New
-On
set
Dia
bete
s (%
of
pati
ents
in
trea
tmen
t gr
oup)
Julius S et al. Lancet. June 2004;363.
0
2
4
6
8
10
12
14
Valsartan-based Regimen
(n = 5094)
Amlodipine-based Regimen
(n = 5074)
13.1%
16.4%
23% Risk Reduction With Valsartan
16
18
P < 0.0001 Good BP control was achieved with both treatment regimens, but BP decrease in the amlodipine group was more pronounced, particularly early in the trial
Despite blood pressure differences, the primary composite cardiac endpoint was not different between the treatment groups
VALUE: Main Results
Julius S et al. Lancet. June 2004;363.
• Prompt BP control in hypertensive patients at high cardiovascular risk is very important
• The between-group differences in heart failure and diabetes suggest that valsartan may offer benefits beyond BP control
VALUE: Conclusions
Julius S et al. Lancet. June 2004;363.
Page 46
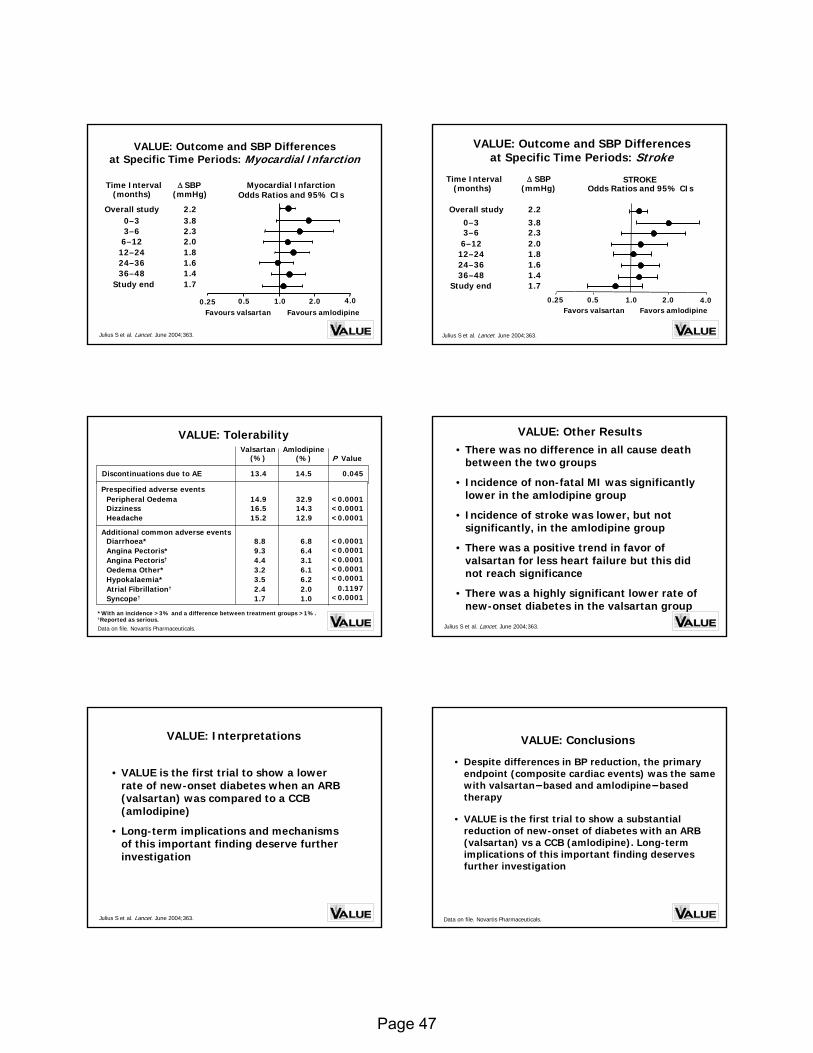
VALUE: Outcome and SBP Differencesat Specific Time Periods: Myocardial Infarction
Time Interval(months)
Overall study
Study end
1.0 2.00.5
Myocardial InfarctionOdds Ratios and 95% CIs
∆ SBP(mmHg)
1.41.61.82.0
3.8
1.7
2.2
2.3
4.00.25
36–4824–3612–246–12
0–33–6
Favours amlodipineFavours valsartan
Julius S et al. Lancet. June 2004;363.
VALUE: Outcome and SBP Differencesat Specific Time Periods: Stroke
Odds Ratios and 95% CIs
Favors valsartan Favors amlodipine1.0 2.00.5
Time Interval(months)
Overall study
36–4824–3612–246–12
0–3
Study end
∆ SBP(mmHg)
1.41.61.82.0
3.8
1.7
2.2
3–6 2.3
0.25 4.0
Julius S et al. Lancet. June 2004;363.
STROKE
VALUE: TolerabilityVALUE: Tolerability
*With an incidence >3% and a difference between treatment groups >1%.†Reported as serious.
P Value(%)(%)
0.045
<0.0001<0.0001<0.0001
2.02.4Atrial Fibrillation†
1.01.7Syncope†
6.23.5Hypokalaemia*
Prespecified adverse events
6.49.3Angina Pectoris*3.14.4Angina Pectoris†
6.13.2Oedema Other*
6.88.8Diarrhoea*Additional common adverse events
14.513.4
12.915.2Headache14.316.5Dizziness32.914.9Peripheral Oedema
Amlodipine Valsartan
Data on file. Novartis Pharmaceuticals.
Discontinuations due to AE
<0.0001<0.0001<0.0001
0.1197<0.0001<0.0001
<0.0001
• There was no difference in all cause death between the two groups
• Incidence of non-fatal MI was significantly lower in the amlodipine group
• Incidence of stroke was lower, but not significantly, in the amlodipine group
• There was a positive trend in favor of valsartan for less heart failure but this did not reach significance
• There was a highly significant lower rate of new-onset diabetes in the valsartan group
VALUE: Other Results
Julius S et al. Lancet. June 2004;363.
• VALUE is the first trial to show a lower rate of new-onset diabetes when an ARB (valsartan) was compared to a CCB (amlodipine)
• Long-term implications and mechanisms of this important finding deserve further investigation
VALUE: Interpretations
Julius S et al. Lancet. June 2004;363.
• Despite differences in BP reduction, the primary endpoint (composite cardiac events) was the same with valsartan−based and amlodipine−basedtherapy
• VALUE is the first trial to show a substantial reduction of new-onset of diabetes with an ARB (valsartan) vs a CCB (amlodipine). Long-term implications of this important finding deserves further investigation
VALUE: Conclusions
Data on file. Novartis Pharmaceuticals.
Page 47
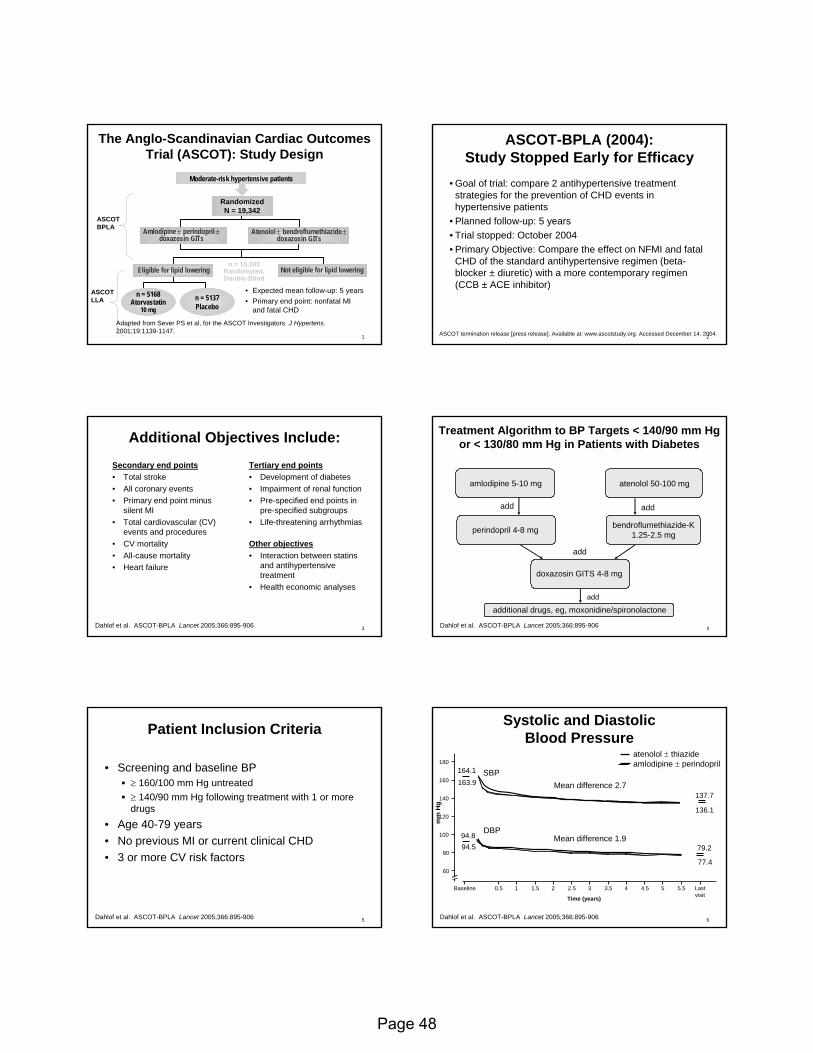
1
• Expected mean follow-up: 5 years• Primary end point: nonfatal MI
and fatal CHD
The AngloThe Anglo--Scandinavian Cardiac Outcomes Scandinavian Cardiac Outcomes Trial (ASCOT): Study DesignTrial (ASCOT): Study Design
Adapted from Sever PS et al, for the ASCOT Investigators. J Hypertens. 2001;19:1139-1147.
n = 5168Atorvastatin
10 mg
n = 5137Placebo
n = 10,305Randomized, Double-Blind
RandomizedN = 19,342
Amlodipine± perindopril±doxazosin GITs
Moderate-risk hypertensive patients
Eligible for lipid lowering Not eligible for lipid lowering
Atenolol± bendroflumethiazide±doxazosin GITs
ASCOT BPLA
ASCOTLLA
2
ASCOTASCOT--BPLA (2004): BPLA (2004): Study Stopped Early for EfficacyStudy Stopped Early for Efficacy
• Goal of trial: compare 2 antihypertensive treatment strategies for the prevention of CHD events in hypertensive patients
• Planned follow-up: 5 years• Trial stopped: October 2004• Primary Objective: Compare the effect on NFMI and fatal
CHD of the standard antihypertensive regimen (beta-blocker ± diuretic) with a more contemporary regimen (CCB ± ACE inhibitor)
ASCOT termination release [press release]. Available at: www.ascotstudy.org. Accessed December 14, 2004.
3
Additional Objectives Include:Additional Objectives Include:Secondary end points• Total stroke• All coronary events• Primary end point minus
silent MI• Total cardiovascular (CV)
events and procedures• CV mortality• All-cause mortality• Heart failure
Tertiary end points• Development of diabetes• Impairment of renal function• Pre-specified end points in
pre-specified subgroups• Life-threatening arrhythmias
Other objectives• Interaction between statins
and antihypertensive treatment
• Health economic analyses
Dahlof et al. ASCOT-BPLA Lancet 2005;366:895-906 4
amlodipine 5-10 mg atenolol 50-100 mg
perindopril 4-8 mg bendroflumethiazide-K1.25-2.5 mg
doxazosin GITS 4-8 mg
add
add add
additional drugs, eg, moxonidine/spironolactoneadd
Treatment Algorithm to BP Targets < 140/90 mm Hg Treatment Algorithm to BP Targets < 140/90 mm Hg or < 130/80 mm Hg in Patients with Diabetesor < 130/80 mm Hg in Patients with Diabetes
Dahlof et al. ASCOT-BPLA Lancet 2005;366:895-906
5
Patient Inclusion CriteriaPatient Inclusion Criteria
• Screening and baseline BP ≥ 160/100 mm Hg untreated≥ 140/90 mm Hg following treatment with 1 or more drugs
• Age 40-79 years • No previous MI or current clinical CHD• 3 or more CV risk factors
Dahlof et al. ASCOT-BPLA Lancet 2005;366:895-906 6
Systolic and Diastolic Systolic and Diastolic Blood PressureBlood Pressure
mm
Hg
60
80
100
120
140
160
180
Time (years)
Baseline 0.5 1 1.5 2 2.5 3 3.5 4 4.5 5 5.5
atenolol ± thiazideamlodipine ± perindopril
137.7
136.1
79.2
77.4
Mean difference 1.9
Last visit
Mean difference 2.7SBP
DBP
163.9164.1
94.894.5
Dahlof et al. ASCOT-BPLA Lancet 2005;366:895-906
Page 48
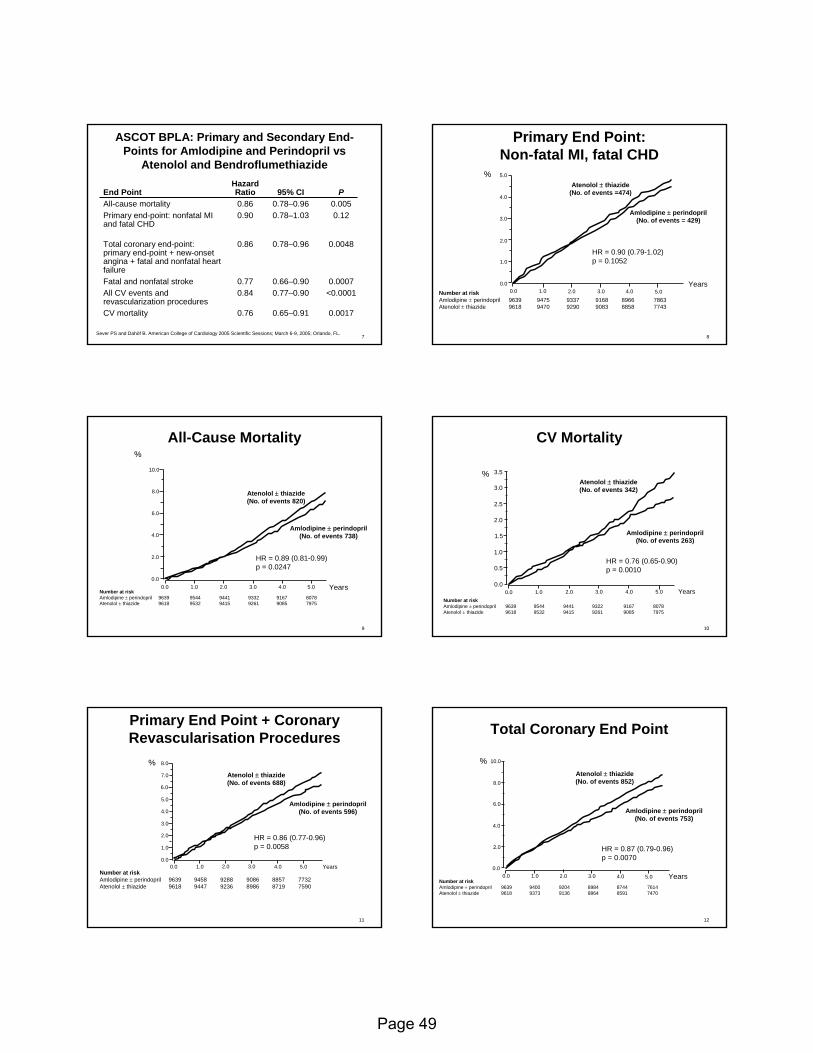
7Sever PS and Dahöf B. American College of Cardiology 2005 Scientific Sessions; March 6-9, 2005; Orlando, FL.
0.00170.65–0.910.76CV mortality
<0.00010.77–0.900.84All CV events and revascularization procedures
0.00070.66–0.900.77Fatal and nonfatal stroke
0.00480.78–0.960.86Total coronary end-point: primary end-point + new-onset angina + fatal and nonfatal heart failure
0.120.78–1.030.90Primary end-point: nonfatal MI and fatal CHD
0.0050.78–0.960.86All-cause mortalityP95% CI
Hazard RatioEnd Point
ASCOT BPLA: Primary and Secondary EndASCOT BPLA: Primary and Secondary End--Points for Amlodipine and Points for Amlodipine and PerindoprilPerindopril vs vs
AtenololAtenolol and and BendroflumethiazideBendroflumethiazide
8
Number at riskAmlodipine ± perindopril 9639 9475 9337 9168 8966 7863Atenolol ± thiazide 9618 9470 9290 9083 8858 7743
0.0 1.0 2.0 3.0 4.0 5.0Years0.0
1.0
2.0
3.0
4.0
5.0
HR = 0.90 (0.79-1.02)p = 0.1052
Atenolol ± thiazide(No. of events =474)
Amlodipine ± perindopril(No. of events = 429)
%
Primary End Point: Primary End Point: NonNon--fatal MI, fatal CHDfatal MI, fatal CHD
9
AllAll--Cause Mortality Cause Mortality
Number at riskAmlodipine ± perindopril 9639 9544 9441 9332 9167 8078Atenolol ± thiazide 9618 9532 9415 9261 9085 7975
0.0 1.0 2.0 3.0 4.0 5.0 Years0.0
2.0
4.0
6.0
8.0
10.0
HR = 0.89 (0.81-0.99)p = 0.0247
%
Amlodipine ± perindopril(No. of events 738)
Atenolol ± thiazide(No. of events 820)
10
CV MortalityCV Mortality
Number at riskAmlodipine ± perindopril 9639 9544 9441 9322 9167 8078Atenolol ± thiazide 9618 9532 9415 9261 9085 7975
0.0 1.0 2.0 3.0 4.0 5.0 Years0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
Amlodipine ± perindopril(No. of events 263)
Atenolol ± thiazide(No. of events 342)
HR = 0.76 (0.65-0.90)p = 0.0010
%
11
Number at riskAmlodipine ± perindopril 9639 9458 9288 9086 8857 7732Atenolol ± thiazide 9618 9447 9236 8986 8719 7590
%
0.0 1.0 2.0 3.0 4.0 5.0 Years0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
HR = 0.86 (0.77-0.96)p = 0.0058
Atenolol ± thiazide(No. of events 688)
Amlodipine ± perindopril(No. of events 596)
8.0
Primary End Point + CoronaryPrimary End Point + CoronaryRevascularisationRevascularisation ProceduresProcedures
12
Number at riskAmlodipine ± perindopril 9639 9400 9204 8984 8744 7614Atenolol ± thiazide 9618 9373 9136 8864 8591 7470
Years0.0 1.0 2.0 3.0 4.0 5.00.0
2.0
4.0
6.0
8.0
10.0
Amlodipine ± perindopril(No. of events 753)
Atenolol ± thiazide(No. of events 852)
HR = 0.87 (0.79-0.96)p = 0.0070
%
Total Coronary End Point Total Coronary End Point
Page 49
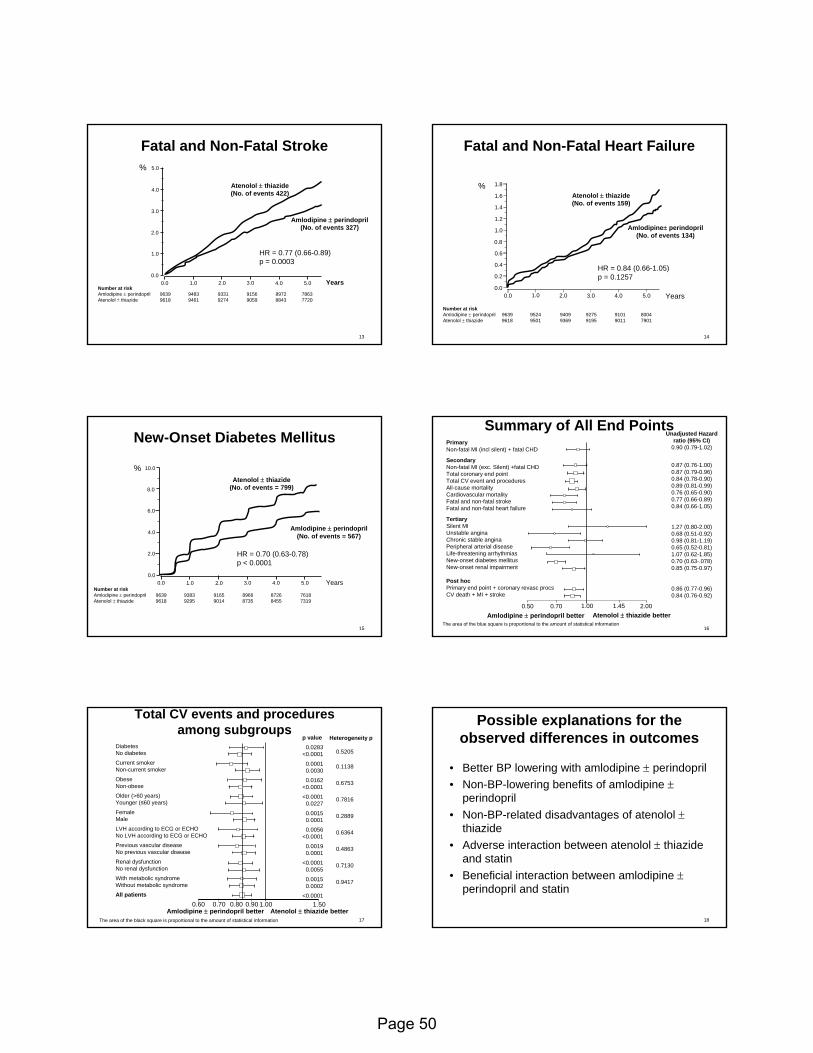
13
Fatal and NonFatal and Non--Fatal Stroke Fatal Stroke
Number at riskAmlodipine ± perindopril 9639 9483 9331 9156 8972 7863Atenolol ± thiazide 9618 9461 9274 9059 8843 7720
0.0 1.0 2.0 3.0 4.0 5.0 Years0.0
1.0
2.0
3.0
4.0
5.0
Amlodipine ± perindopril(No. of events 327)
Atenolol ± thiazide(No. of events 422)
HR = 0.77 (0.66-0.89)p = 0.0003
%
14
Fatal and NonFatal and Non--Fatal Heart FailureFatal Heart Failure
Number at riskAmlodipine ± perindopril 9639 9524 9409 9275 9101 8004Atenolol ± thiazide 9618 9501 9369 9195 9011 7901
0.0 1.0 2.0 3.0 4.0 5.00.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
1.6
HR = 0.84 (0.66-1.05)p = 0.1257
Amlodipine± perindopril(No. of events 134)
Atenolol ± thiazide(No. of events 159)
%
Years
1.8
15
NewNew--Onset Diabetes Mellitus Onset Diabetes Mellitus
Number at riskAmlodipine ± perindopril 9639 9383 9165 8966 8726 7618Atenolol ± thiazide 9618 9295 9014 8735 8455 7319
0.0 1.0 2.0 3.0 4.0 5.0 Years0.0
2.0
4.0
6.0
8.0
10.0
Amlodipine ± perindopril(No. of events = 567)
Atenolol ± thiazide(No. of events = 799)
HR = 0.70 (0.63-0.78)p < 0.0001
%
16
Summary of All End PointsSummary of All End Points
The area of the blue square is proportional to the amount of statistical informationAmlodipine ± perindopril better Atenolol ± thiazide better
0.50 0.70 1.00 1.45
PrimaryNon-fatal MI (incl silent) + fatal CHD
SecondaryNon-fatal MI (exc. Silent) +fatal CHDTotal coronary end pointTotal CV event and proceduresAll-cause mortalityCardiovascular mortalityFatal and non-fatal strokeFatal and non-fatal heart failure
TertiarySilent MIUnstable anginaChronic stable anginaPeripheral arterial diseaseLife-threatening arrhythmiasNew-onset diabetes mellitusNew-onset renal impairment
Post hocPrimary end point + coronary revasc procsCV death + MI + stroke
2.00
Unadjusted Hazard ratio (95% CI)
0.90 (0.79-1.02)
0.87 (0.76-1.00)0.87 (0.79-0.96)0.84 (0.78-0.90)0.89 (0.81-0.99)0.76 (0.65-0.90)0.77 (0.66-0.89)0.84 (0.66-1.05)
1.27 (0.80-2.00)0.68 (0.51-0.92)0.98 (0.81-1.19)0.65 (0.52-0.81)1.07 (0.62-1.85)0.70 (0.63-.078)0.85 (0.75-0.97)
0.86 (0.77-0.96)0.84 (0.76-0.92)
17
0.60 0.70 0.80 0.90 1.00 1.50
The area of the black square is proportional to the amount of statistical information
Amlodipine ± perindopril better Atenolol ± thiazide better
DiabetesNo diabetes
Current smokerNon-current smoker
ObeseNon-obese
Older (>60 years)Younger (≤60 years)
FemaleMale
LVH according to ECG or ECHONo LVH according to ECG or ECHO
Previous vascular diseaseNo previous vascular disease
Renal dysfunctionNo renal dysfunction
With metabolic syndromeWithout metabolic syndrome
All patients
p value0.0283
<0.0001
0.00010.0030
0.0162<0.0001
<0.00010.0227
0.00150.0001
0.0056<0.0001
0.00190.0001
<0.00010.0055
0.00150.0002
<0.0001
Heterogeneity p
0.5205
0.1138
0.6753
0.7816
0.2889
0.6364
0.4863
0.7130
0.9417
Total CV events and procedures Total CV events and procedures among subgroupsamong subgroups
18
Possible explanations for the Possible explanations for the observed differences in outcomesobserved differences in outcomes
• Better BP lowering with amlodipine ± perindopril• Non-BP-lowering benefits of amlodipine ±
perindopril• Non-BP-related disadvantages of atenolol ±
thiazide• Adverse interaction between atenolol ± thiazide
and statin• Beneficial interaction between amlodipine ±
perindopril and statin
Page 50

19
Final conclusionsFinal conclusions
• Amlodipine ± perindopril based therapy confers an advantage over atenolol ± thiazide based therapy on all major CV end points, all-cause mortality and new-onset diabetes
• Irrespective of the reasons for benefit, the standard regimen of beta-blocker ± thiazide should not be preferred to the amlodipine ±perindopril regimen for most patients
Page 51

1
LIFEBackground/Rationale
– No specific drug treatment in hypertension has shown unique benefit over another
– LVH is a strong and independent risk factor– Angiotensin II is an important growth factor and
linked to mortality– Purpose: To determine if the selective AT1-
receptor blockade (losartan) is potentially more effective than atenolol in reversing LVH and CV morbidity and mortality beyond BP lowering
Dahl f B, et al. Lancet 2002;359:995-1003..
2
9193 men and women with Hypertension and LVHTitration target: BP < 140/90 mmHg
Losartan 50 mg(n=4605)
Atenolol 50 mg(n=4588)
+ HCTZ 12.5 mg
LIFEStudy Dosing Design
Losartan 100 mg+ HCTZ 12.5 mg
Month 2
Month 4
Losartan 100 mg+ HCTZ 12.5 - 25 mg
+ others*
Month 6
+ HCTZ 12.5 mg
Atenolol 100 mg+ HCTZ 12.5 mg
Atenolol 100 mg+ HCTZ 12.5 - 25 mg
+ others*
* Excluding ACEIs, A-II antagonists, -blockers
DahlDahl f B, et al.f B, et al. Lancet 2002;359:995Lancet 2002;359:995--1003.1003.
3
• SBP (baseline) 174.3 174.5
• SBP (follow-up) 144.1 145.4
• DBP (baseline) 97.9 97.7
• DBP (follow-up) 81.3 80.9
LIFEBlood Pressure:
Baseline & Follow-up (mean 4.8 yrs)
LosartanLosartan AtenololAtenolol(n=4605) (n=4588)
DahlDahl f B, et al.f B, et al. Lancet 2002;359:995Lancet 2002;359:995--1003.1003.
4
LIFEPrimary Composite Outcome*
* CV Mortality, All Stroke, All MI
Time (months)Time (months)
P ro p
orti o
n o f
pat
ient
s wi th
P r
o por
ti on
o f p
atie
nts w
i th
fi rs t
ev e
n t (%
)fi r
s t e
v en t
(%)
0 0
44
10101212
00 66 1212 1818 2424 3030 3636 4242 4848 5454 6060 6666
AtenololAtenolol
Intention to TreatIntention to Treat
Adjusted Risk Reduction 13.0%, pAdjusted Risk Reduction 13.0%, p = 0.021= 0.02122
8 8 LosartanLosartan
Unadjusted Risk Reduction 14.6%, p = 0.009Unadjusted Risk Reduction 14.6%, p = 0.009
66
14141616
DahlDahl f B, et al.f B, et al. Lancet 2002;359:995Lancet 2002;359:995--1003.1003.
5
LIFE StudyDiabetes Substudy
• Patients: 9,195 men and women with hypertension (160-200/95-115 mm Hg), ECG signs of LVH and type 2 DM, aged 55-80 years
• Mean age: 67.4; BP: 176/97 mm Hg; BP goal <140/90 mm Hg• Drug therapy:
– 586 randomized to losartan +/-HCTZ, mean BP at end of follow-up: 146/79 mm Hg
– 609 randomized to atenolol +/- HCTZ, mean BP at end of follow-up: 148/79 mm Hg
• Primary endpoints: CV morbidity and mortality (CV death, stroke, MI) 4.7-year mean follow-up
Lindholm LH, et al. Lancet. 2002; 359:1004-1010.
6
LIFE Diabetes SubstudyResults
Endpoint Events per 1000 Patient-YearsLosartan Atenolol % Reduction
Primary composite 39.2 53.6 24*CV mortality 13.6 21.8 37*MI 15.2 18.7 17Stroke 19.0 24.5 21Total Mortality 22.5 37.2 39*Heart Failure Admit 11.8 20.7 45*
*P<0.05.
Lindholm LH, et al. Lancet. 2002; 359:1004-1010.
Page 52
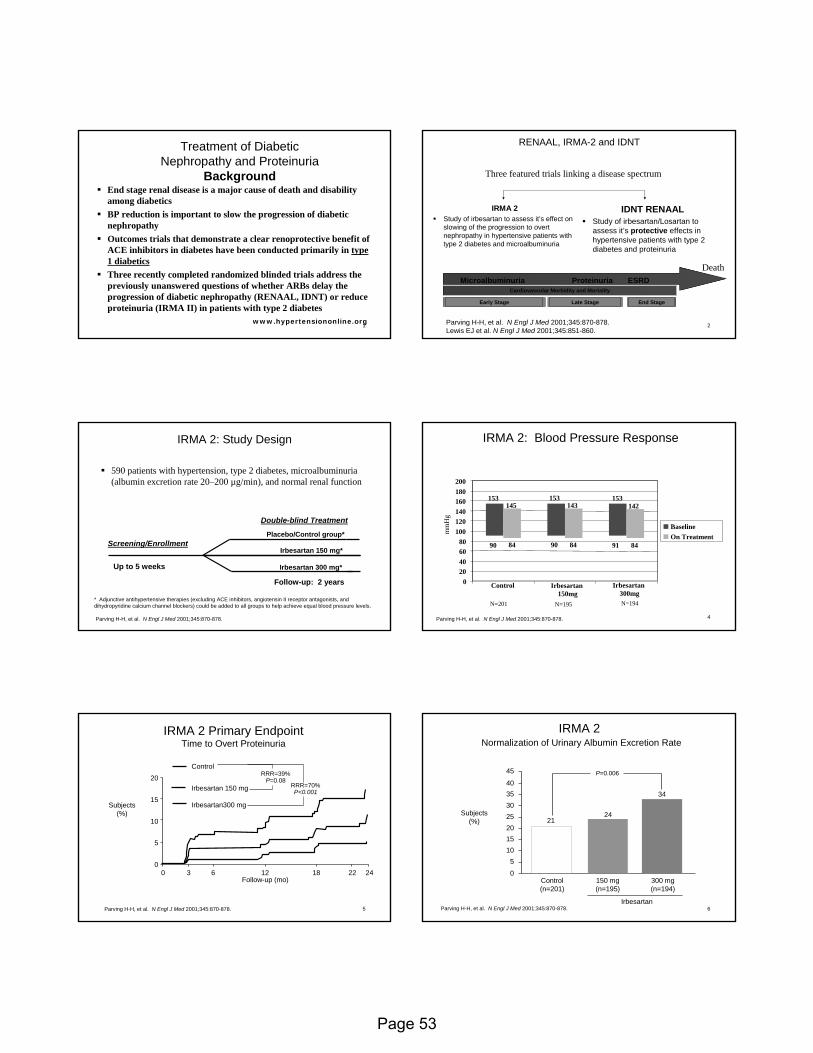
1
Treatment of Diabetic Treatment of Diabetic Nephropathy and ProteinuriaNephropathy and Proteinuria
BackgroundBackgroundEnd stage renal disease is a major cause of death and disabilityamong diabeticsBP reduction is important to slow the progression of diabetic nephropathyOutcomes trials that demonstrate a clear renoprotective benefit of ACE inhibitors in diabetes have been conducted primarily in type 1 diabeticsThree recently completed randomized blinded trials address the previously unanswered questions of whether ARBs delay the progression of diabetic nephropathy (RENAAL, IDNT) or reduce proteinuria (IRMA II) in patients with type 2 diabetes
www.hypertensiononline.org 2
RENAAL, IRMARENAAL, IRMA--2 and IDNT2 and IDNT
IRMA 2Study of irbesartan to assess it’s effect on slowing of the progression to overt nephropathy in hypertensive patients with type 2 diabetes and microalbuminuria
IDNT RENAALStudy of irbesartan/Losartan to assess it’s protective effects in hypertensive patients with type 2 diabetes and proteinuria
Three featured trials linking a disease spectrum
Microalbuminuria Proteinuria ESRDCardiovascular Morbidity and Mortality
Early Stage Late Stage
Death
End Stage
Parving H-H, et al. N Engl J Med 2001;345:870-878.Lewis EJ et al. N Engl J Med 2001;345:851-860.
Double-blind Treatment
Up to 5 weeks
Screening/EnrollmentIrbesartan 150 mg*
Irbesartan 300 mg*
Follow-up: 2 years
Placebo/Control group*
IRMA 2: Study DesignIRMA 2: Study Design
590 patients with hypertension, type 2 diabetes, microalbuminuria (albumin excretion rate 20–200 µg/min), and normal renal function
* Adjunctive antihypertensive therapies (excluding ACE inhibitors, angiotensin II receptor antagonists, and dihydropyridine calcium channel blockers) could be added to all groups to help achieve equal blood pressure levels.
Parving H-H, et al. N Engl J Med 2001;345:870-878. 4
IRMA 2: Blood Pressure ResponseIRMA 2: Blood Pressure Response
020406080
100120140160180200
Control Irbesartan150mg
BaselineOn Treatment
84
153 153145 143 142
90 84 90 84 91
153
Irbesartan300mg
N=201 N=195 N=194
mm
Hg
Parving H-H, et al. N Engl J Med 2001;345:870-878.
5
0
5
10
15
20
0 3 6 12 18 22 24Follow-up (mo)
Subjects(%)
IRMA 2 Primary EndpointIRMA 2 Primary EndpointTime to Overt ProteinuriaTime to Overt Proteinuria
Parving H-H, et al. N Engl J Med 2001;345:870-878.
Control
Irbesartan 150 mg
Irbesartan300 mg
RRR=39%P=0.08
RRR=70%P<0.001
6
IRMA 2IRMA 2Normalization of Urinary Albumin Excretion RateNormalization of Urinary Albumin Excretion Rate
35
45
40
3025201510
50
Subjects(%)
Control(n=201)
150 mg(n=195)
300 mg(n=194)
Irbesartan
24
34
21
P=0.006
Parving H-H, et al. N Engl J Med 2001;345:870-878.
Page 53
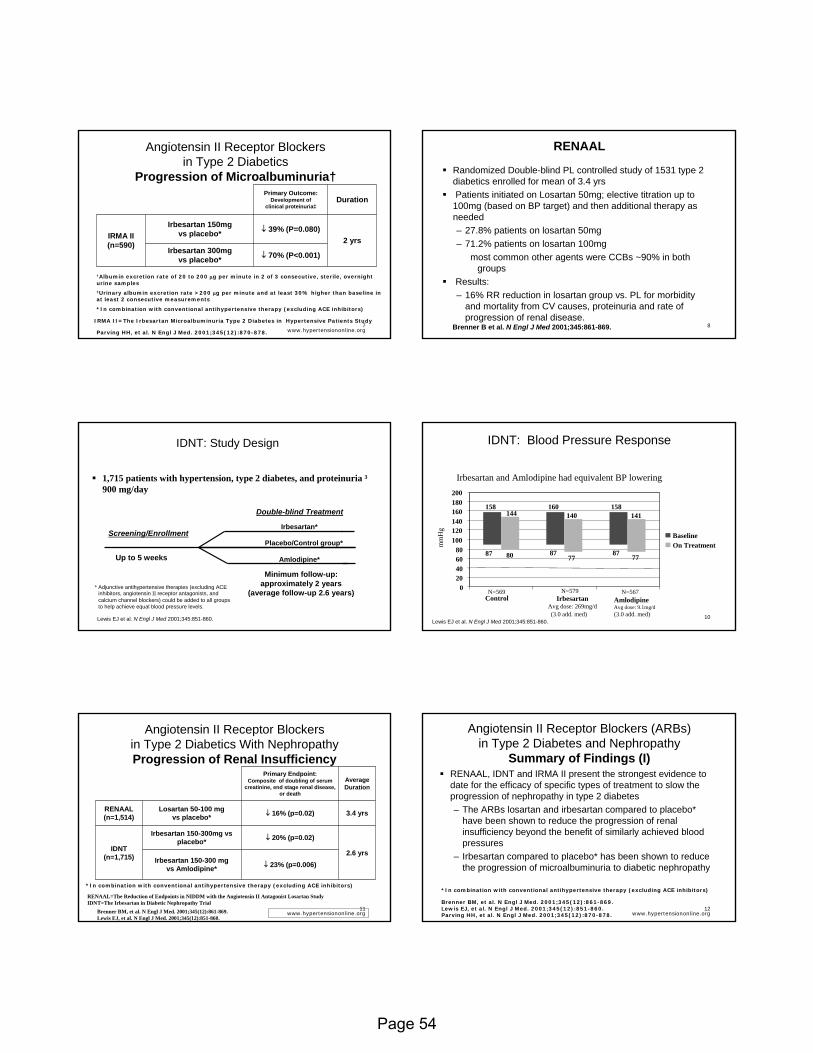
7
Angiotensin II Receptor Blockers Angiotensin II Receptor Blockers in Type 2 Diabeticsin Type 2 Diabetics
Progression of Progression of MicroalbuminuriaMicroalbuminuria††
2 yrsIrbesartan 300mg
vs placebo*
Irbesartan 150mg vs placebo*
DurationPrimary Outcome:
Development of clinical proteinuria‡
↓ 39% (P=0.080)IRMA II (n=590)
↓ 70% (P<0.001)
†Albumin excretion rate of 20 to 200 µg per minute in 2 of 3 consecutive, sterile, overnight urine samples‡Urinary albumin excretion rate >200 µg per minute and at least 30% higher than baseline in at least 2 consecutive measurements
*In combination with conventional antihypertensive therapy (excluding ACE inhibitors)
Parving HH, et al. N Engl J Med. 2001;345(12):870-878.
IRMA II=The Irbesartan Microalbuminuria Type 2 Diabetes in Hypertensive Patients Study
www.hypertensiononline.org8
RENAALRENAAL
Randomized Double-blind PL controlled study of 1531 type 2 diabetics enrolled for mean of 3.4 yrsPatients initiated on Losartan 50mg; elective titration up to
100mg (based on BP target) and then additional therapy as needed– 27.8% patients on losartan 50mg– 71.2% patients on losartan 100mg
most common other agents were CCBs ~90% in both groups
Results:– 16% RR reduction in losartan group vs. PL for morbidity
and mortality from CV causes, proteinuria and rate of progression of renal disease.
Brenner B et al. N Engl J Med 2001;345:861-869.
IDNT: Study DesignIDNT: Study Design
1,715 patients with hypertension, type 2 diabetes, and proteinuria ³ 900 mg/day
Double-blind Treatment
Up to 5 weeks
Screening/EnrollmentPlacebo/Control group*
Amlodipine*
Minimum follow-up: approximately 2 years
(average follow-up 2.6 years)
Irbesartan*
* Adjunctive antihypertensive therapies (excluding ACE inhibitors, angiotensin II receptor antagonists, and calcium channel blockers) could be added to all groups to help achieve equal blood pressure levels.
Lewis EJ et al. N Engl J Med 2001;345:851-860. 10
IDNT: Blood Pressure ResponseIDNT: Blood Pressure Response
020406080
100120140160180200
Control
BaselineOn Treatment
77
160 158144 140 141
87 80 8777
87
158
Irbesartan and Amlodipine had equivalent BP lowering
N=569 N=579 N=567
mm
Hg
IrbesartanAvg dose: 269mg/d
AmlodipineAvg dose: 9.1mg/d(3.0 add. med)(3.0 add. med)
Lewis EJ et al. N Engl J Med 2001;345:851-860.
11
Angiotensin II Receptor Blockers Angiotensin II Receptor Blockers in Type 2 Diabetics With Nephropathyin Type 2 Diabetics With NephropathyProgression of Renal InsufficiencyProgression of Renal Insufficiency
Irbesartan 150-300 mgvs Amlodipine*
Irbesartan 150-300mg vsplacebo*
Losartan 50-100 mg vs placebo* 3.4 yrsRENAAL
(n=1,514)
↓ 23% (p=0.006)2.6 yrs
↓ 20% (p=0.02)IDNT
(n=1,715)
↓ 16% (p=0.02)
Average Duration
Primary Endpoint:Composite of doubling of serum
creatinine, end stage renal disease, or death
*In combination with conventional antihypertensive therapy (excluding ACE inhibitors)
RENAAL=The Reduction of Endpoints in NIDDM with the Angiotensin II Antagonist Losartan StudyIDNT=The Irbesartan in Diabetic Nephropathy Trial
Brenner BM, et al. N Engl J Med. 2001;345(12):861-869. Lewis EJ, et al. N Engl J Med. 2001;345(12):851-860.
www.hypertensiononline.org12
Angiotensin II Receptor Blockers (ARBs) Angiotensin II Receptor Blockers (ARBs) in Type 2 Diabetes and Nephropathyin Type 2 Diabetes and Nephropathy
Summary of Findings (I)Summary of Findings (I)RENAAL, IDNT and IRMA II present the strongest evidence to date for the efficacy of specific types of treatment to slow theprogression of nephropathy in type 2 diabetes– The ARBs losartan and irbesartan compared to placebo*
have been shown to reduce the progression of renal insufficiency beyond the benefit of similarly achieved blood pressures
– Irbesartan compared to placebo* has been shown to reduce the progression of microalbuminuria to diabetic nephropathy
Brenner BM, et al. N Engl J Med. 2001;345(12):861-869. Lewis EJ, et al. N Engl J Med. 2001;345(12):851-860.Parving HH, et al. N Engl J Med. 2001;345(12):870-878.
*In combination with conventional antihypertensive therapy (excluding ACE inhibitors)
www.hypertensiononline.org
Page 54
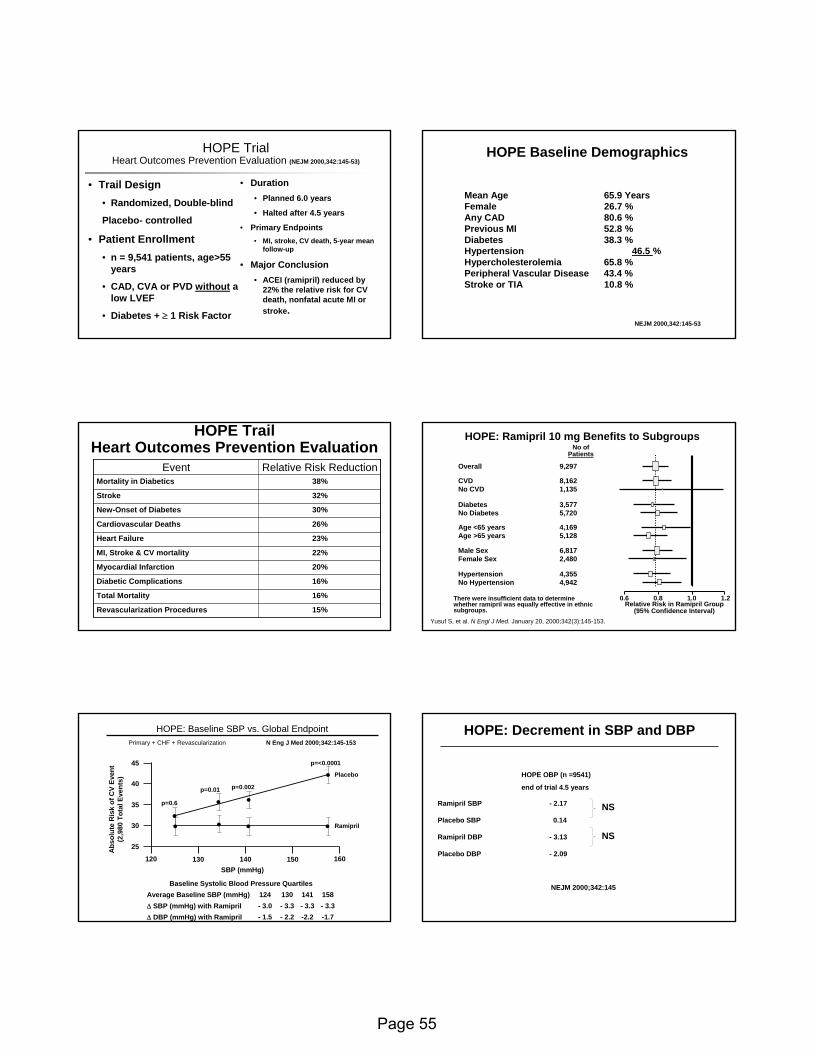
HOPE TrialHOPE TrialHeart Outcomes Prevention Evaluation Heart Outcomes Prevention Evaluation (NEJM 2000,342:145-53)
• Trail Design• Randomized, Double-blind
Placebo- controlled
• Patient Enrollment• n = 9,541 patients, age>55
years
• CAD, CVA or PVD without a low LVEF
• Diabetes + ≥ 1 Risk Factor
• Duration• Planned 6.0 years
• Halted after 4.5 years
• Primary Endpoints• MI, stroke, CV death, 5-year mean
follow-up
• Major Conclusion• ACEI (ramipril) reduced by
22% the relative risk for CV death, nonfatal acute MI or stroke.
HOPE Baseline Demographics
Mean Age 65.9 Years Female 26.7 %Any CAD 80.6 % Previous MI 52.8 % Diabetes 38.3 % Hypertension 46.5 % Hypercholesterolemia 65.8 % Peripheral Vascular Disease 43.4 % Stroke or TIA 10.8 %
NEJM 2000,342:145-53
HOPE TrailHOPE TrailHeart Outcomes Prevention EvaluationHeart Outcomes Prevention Evaluation
15%15%Revascularization ProceduresRevascularization Procedures
16%16%Total MortalityTotal Mortality
16%16%Diabetic ComplicationsDiabetic Complications
20%20%Myocardial InfarctionMyocardial Infarction
22%22%MI, Stroke & CV mortalityMI, Stroke & CV mortality
23%23%Heart FailureHeart Failure
26%26%Cardiovascular DeathsCardiovascular Deaths
30%30%NewNew--Onset of DiabetesOnset of Diabetes
32%32%StrokeStroke
38%38%Mortality in DiabeticsMortality in DiabeticsRelative Risk ReductionRelative Risk ReductionEventEvent
HOPE: Ramipril 10 mg Benefits to SubgroupsHOPE: Ramipril 10 mg Benefits to Subgroups
There were insufficient data to determine There were insufficient data to determine whether ramipril was equally effective in ethnic whether ramipril was equally effective in ethnic subgroups.subgroups.
OverallOverall 9,2979,297
CVDCVD 8,1628,162No CVDNo CVD 1,1351,135
Age <65 yearsAge <65 years 4,1694,169Age >65 yearsAge >65 years 5,1285,128
Male SexMale Sex 6,8176,817Female SexFemale Sex 2,4802,480
HypertensionHypertension 4,3554,355No HypertensionNo Hypertension 4,9424,942
DiabetesDiabetes 3,5773,577No DiabetesNo Diabetes 5,7205,720
No ofNo ofPatientsPatients
0.60.6 0.80.8 1.01.0 1.21.2Relative Risk in Ramipril GroupRelative Risk in Ramipril Group
(95% Confidence Interval)(95% Confidence Interval)Yusuf S, et al. N Engl J Med. January 20, 2000;342(3):145-153.
-1.7-2.2- 2.2- 1.5∆ DBP (mmHg) with Ramipril- 3.3- 3.3- 3.3- 3.0∆ SBP (mmHg) with Ramipril158141130124Average Baseline SBP (mmHg)
Baseline Systolic Blood Pressure Quartiles
•
•••
Placebo
•• • • Ramipril
SBP (mmHg)
25
30
35
40
45
120 160140 150130
Abs
olut
e R
isk
of C
V Ev
ent
(2,9
80 T
otal
Eve
nts)
HOPE: Baseline SBP vs. Global EndpointPrimary + CHF + Revascularization N Eng J Med 2000;342:145-153
p=0.6
p=0.01 p=0.002
p=<0.0001
HOPE: Decrement in SBP and DBPHOPE: Decrement in SBP and DBP
HOPE OBP (n =9541)
end of trial 4.5 years
Ramipril SBP - 2.17
Placebo SBP 0.14
Ramipril DBP - 3.13
Placebo DBP - 2.09
NEJM 2000;342:145NEJM 2000;342:145
NS
NS
Page 55
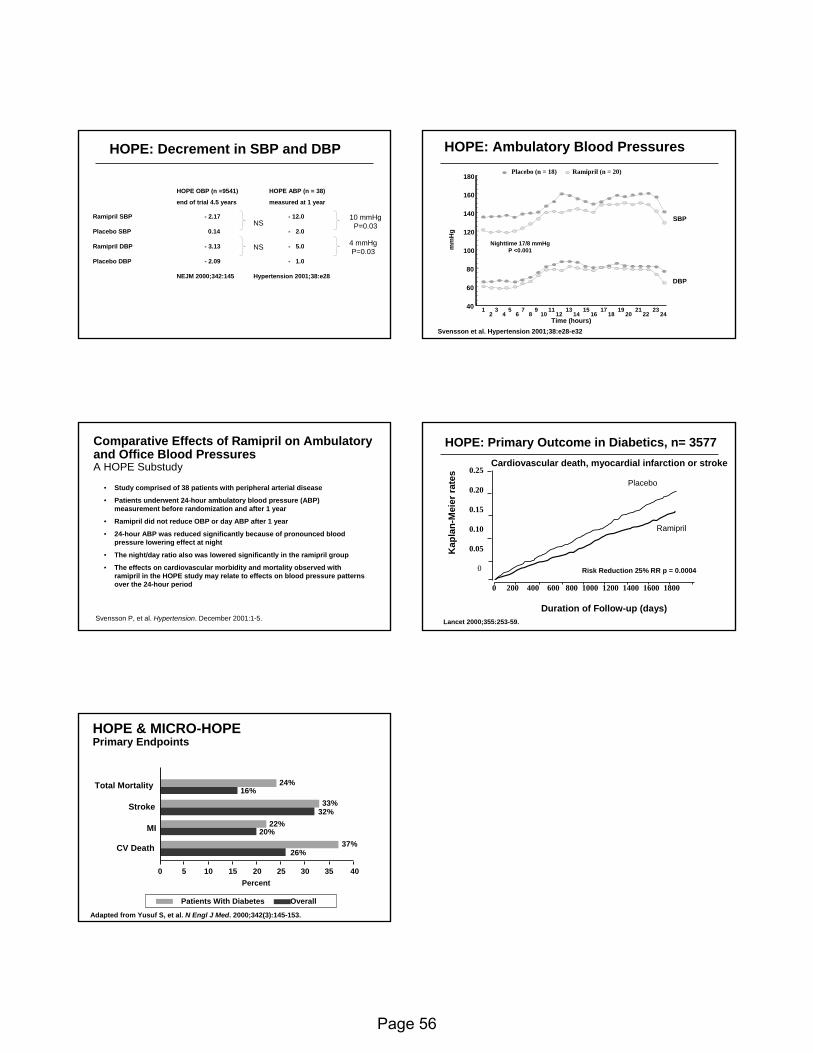
HOPE OBP (n =9541) HOPE ABP (n = 38)
end of trial 4.5 years measured at 1 year
Ramipril SBP - 2.17 - 12.0
Placebo SBP 0.14 - 2.0
Ramipril DBP - 3.13 - 5.0
Placebo DBP - 2.09 - 1.0
NEJM 2000;342:145 Hypertension 2001;38:e28NEJM 2000;342:145 Hypertension 2001;38:e28
NS
NS
10 mmHgP=0.03
4 mmHgP=0.03
HOPE: Decrement in SBP and DBPHOPE: Decrement in SBP and DBP HOPE: Ambulatory Blood PressuresHOPE: Ambulatory Blood Pressures
Svensson et al. Hypertension 2001;38:e28Svensson et al. Hypertension 2001;38:e28--e32e32Time (hours)
40
60
80
100
120
140
160
180
mm
Hg
1 3 5 7 9 11 13 15 17 19 21 232 4 6 8 10 12 14 16 18 20 22 24
Placebo (n = 18) Ramipril (n = 20)
DBP
SBP
Nighttime 17/8 mmHgP <0.001
Comparative Effects of Ramipril on Ambulatory Comparative Effects of Ramipril on Ambulatory and Office Blood Pressuresand Office Blood PressuresA HOPE SubstudyA HOPE Substudy
• Study comprised of 38 patients with peripheral arterial disease
• Patients underwent 24-hour ambulatory blood pressure (ABP) measurement before randomization and after 1 year
• Ramipril did not reduce OBP or day ABP after 1 year
• 24-hour ABP was reduced significantly because of pronounced blood pressure lowering effect at night
• The night/day ratio also was lowered significantly in the ramipril group
• The effects on cardiovascular morbidity and mortality observed with ramipril in the HOPE study may relate to effects on blood pressure patterns over the 24-hour period
Svensson P, et al. Hypertension. December 2001:1-5.Duration of Follow-up (days)
Kap
lan-
Mei
er ra
tes
HOPE: Primary Outcome in Diabetics, n= 3577
0.25
0.20
0.15
0.10
0.05
0
Placebo
0 200 400 600 800 1000 1200 1400 1600 1800
Lancet 2000;355:253Lancet 2000;355:253--59.59.
Risk Reduction 25% RR p = 0.0004
Cardiovascular death, myocardial infarction or stroke
Ramipril
HOPE & MICROHOPE & MICRO--HOPEHOPEPrimary EndpointsPrimary Endpoints
CV DeathCV Death
MIMI
StrokeStroke
Total MortalityTotal Mortality 24%24%16%16%
33%33%32%32%
22%22%20%20%
37%37%26%26%
00 55 1010 1515 2020 2525 3030 3535 4040
Patients With Diabetes Overall Patients With Diabetes Overall
PercentPercent
Adapted from Yusuf S, et al. N Engl J Med. 2000;342(3):145-153.
Page 56
Reviewed: 12/19/2005
PHAR 6122 Cardiovascular Section
Robert J. Straka, Pharm.D. FCCP Pharmacotherapeutic Issues with Managing Hypercholesterolemia
Spring 2006
Objectives After attending lecture and reading the required material, the learner will be able to: 1. Describe the basic pathophysiology of atherosclerosis. 2. Describe and explain fully each of the risk factors for developing atherosclerotic
coronary vascular disease (ASCVD). 3. Discuss current NCEP (ATP III) and updated treatment guidelines for patients
with hyperlipidemia and newer landmark studies which may modify your approach to such patients
4. Outline the major classes of drugs used to treat hyperlipidemia with special
emphasis on differentiating between, HMG-CoA reductase inhibitors, niacin formulations, fibrates, and bile acid sequestrants, cholesterol absorption inhibitors in regards to:
a. MOA
b. Effects on lipid profile c. Dosing d. Common or serious adverse effects e. Special considerations for their use f. Place in treating a specific patient with a dyslipidemia
5. Indicate the drug of choice and an appropriate general dosage range for a given
patient and be able to select an alternative if the initial drug is inadequate or intolerable.
6. Demonstrate the ability to design a treatment plan to initiate drug and non-drug
treatment of hyperlipidemic patient, select, monitor and titrate appropriate drug therapy. Calculate 10-year CHD risk, select target LDL, HDL and non-HDL goals. Be able to recommend responsible actions to take to avoid drug interactions or managing adverse reactions to lipid lowering agents.
Page 57
Reviewed: 12/19/2005
PHARM 6122 Cardiovascular Section
Robert J. Straka, Pharm.D. Ischemic Heart Disease – Chronic Stable Angina
Spring 2006
Objectives
After attending lecture and reading the required material, the student will be able to: Angina: 1. Be able to contrast and compare chronic stable angina, Prinzmetal's or variant angina,
and unstable angina with respect to presentation, pathophysiology, and approach to treatment.
2. Describe and define the determinants of myocardial oxygen consumption. 3. Be able to list and explain the risk factors for coronary heart disease (CHD). Drug Therapy: 1. Demonstrate a detailed understanding of the clinical effects and differences between
the currently available nitroglycerin products. 2. Provide a review of the issues surrounding the problem of nitrate tolerance, with
emphasis on the mechanism, evaluation for, and strategies for its prevention. 4. Demonstrate a detailed understanding of the clinical effects, prioritizing for use, and
indications of the currently available calcium channel blockers and beta-blockers. 4. Demonstrate knowledge of basic monitoring parameters in assessing efficacy and
toxicity of calcium channel blockers, beta blockers, nitrates and antiplatelet therapy. 5. Given a patient case, construct a treatment plan including the selection of the
appropriate medication, dose, monitoring parameters, and patient instructions.
Page 58
Reviewed: 12/19/2005
Phar 6122 Cardiovascular Section
Robert J. Straka, Pharm.D. Pathophysiology and Therapy of Acute Coronary Syndromes (including
STEMI, non-STEMI and Unstable Angina) Spring 2006
Objectives
After attending lecture and reading the required material, the student will be able to: 1. Describe the clinical signs and symptoms of a patient experiencing a myocardial
infarction and be able to distinguish them from other acute coronary syndromes (unstable angina or non-STEMI)
2. Recommend drug therapy for a suspected ST-segment elevation MI (STEMI) or non-
STEMI or Unstable Angina (UA) for a patient based on an understating of: a. mechanisms of action b. usual dosing c. expected outcome d. common or serious adverse effects e. drug interactions
f. therapeutic efficacy
3. Describe the role of the ECG (interpreting changes), cardiac enzymes, and clinical presentation in the diagnosis of a patient with a suspected STEMI or non-STEMI or UA.
4. Explain the role of beta-blocking agents, ACE Inhibitors, lytics, anticoagulants,
aspirin and other antiplatelet agents in the treatment of each of these Acute Coronary Syndromes (ACS’s) and how the features of those agents may be exploited to achieve the optimal outcome for a given patient.
5. Contrast and compare the thrombolytics available for the treatment of a patient with
an ACS with regards to the mechanism of action, dose, advantages, disadvantages, contraindications, cost, side effect profiles, length of therapy and expected outcomes.
Page 59
Last Reviewed: 12/19/2005
Phar 6122 Cardiovascular Section
Robert J. Straka, Pharm.D. Antithrombotic Agents
Spring 2006
Objectives
Upon completion of this lecture, students should be able to:
1. Describe the mechanism of action of aspirin, thienopyridines, and glycoprotein IIB/IIIA receptor antagonists and direct thrombin inhibitors.
2. Describe the physiologic process of coagulation. 3. Discuss dosing, monitoring and adverse effects of the most common anticoagulation
drugs, namely heparin and warfarin and how to reverse their effects. 4. Outline the indications or roles for antithrombotic agents for specific cardiovascular
disorders such as acute myocardial infarction, angina and atrial fibrillation for primary and secondary prevention of coronary events.
Page 60
Reviewed: 12/19/2005
Phar 6122 Cardiovascular Section
Robert Straka, Pharm.D. Chronic Heart Failure
And Acute Heart Failure
Spring 2006
Lecture Objectives for Both Acute and Chronic Heart Failure
Lectures: After attending lecture and reading the recommended literature, the learner will be able to: 1) Appreciate the basic pathophysiology of CHF and be able to describe the role of the RAA
system in this syndrome. 2) Define the following terms: Preload, Afterload, and Wall tension 3) List the major therapeutic goals of treating chronic heart failure (CHF) and the signs and
symptoms of CHF in the cardiac patient. Distinguish between left ventricular systolic and diastolic dysfunction.
4) Describe the NYHA functional classification system for CHF patients and be able to relate
these to the newer “stages” adopted by AHA/ACC. You should also be able to contrast these to the “Forrester Classification” of patients with acute heart failure.
5) Be able to describe the major objectives, general study design, number of patients, the
therapies evaluated, overall outcomes, (significance) and conclusions of the major trials evaluating drug therapy of CHF identified as landmark trials in class.
6) Be able to develop a reasonable treatment plan for the management of a patient in need of
acute therapy to manage CHF based on data presented to you in a case format and evaluate and recommend pharmacotherapy management for the patient being followed for chronic HF. (Both Acute and Chronic HF)
7) Understand how the following hemodynamic parameters are measured, their normal values,
and their importance in monitoring the patient with CHF: RAP, CVP, CO, CI, PAP,UO, SV and PCWP. (Acute HF lectures)
Page 61
Reviewed: 12/19/2005
Phar 6122 Cardiovascular Section
Robert Straka, Pharm.D.
Acute Heart Failure Spring 2006
Objectives
After attending lecture and reading the recommended literature, the student will be able to: 1) Describe the basic pathophysiology of acute heart failure. 2) Define the following terms: Preload, Afterload, and Wall tension 3) Demonstrate an understanding of how the following hemodynamic parameters are
measured, their normal values, and their importance in monitoring the patient with heart failure: RAP, CVP, CO, CI, PAP,UO, SV and PCWP.
4) Develop a reasonable treatment plan and monitoring parameters for the management of a
patient in acute heart failure.
Page 62
Reviewed: 12/19/2005
PHAR 6122 Cardiovascular Section
Pulmonary Embolism & Deep Vein Thrombosis
Spring 2006
Objectives
After attending this lecture and reading the required material, the student will be able to: 1. Describe the risk factors associated with the development of pulmonary embolism
(PE) and deep vein thrombosis (DVT). 2. Demonstrate an understanding of the pathophysiology of PE and DVT. 3. Recognize clinical presentation of PE and DVT and differentiate between the
available objective tests used to make the diagnosis. 4. Describe the therapeutic role of unfractionated heparin, low molecular weight
heparin, and warfarin in PE/DVT in regards to dosing, length of therapy, and monitoring.
5. Describe the role of thrombolytics in treating PE/DVT, specifically, when lytics are
indicated, dosing, duration of treatment, and monitoring. 6. Discuss in what type of patients DVT prophylaxis is necessary and be familiar with
available options.
Page 63

Page 64
Appendix A
Phar 6122: Pathophysiology and Pharmacotherapy of Cardiovascular Disorders
Spring 2006 Web Exercise
The following exercise is designed to expose the student to just a few of the numerous web sites that may be helpful during and beyond this course, and to acquaint students with retrieving Adobe® Portable Document Format (PDF) file articles from the world wide web. Please work independently in answering the five questions below. Although this will not be graded, completion of the exercise will be required to receive a final grade in this course. Please submit it to the cardiovascular TA at the end of class on Monday JANUARY 30, 2006. Name (Please Print):____________________________ 1) Site: Homepage for Phar 6122--Cardiology Assignment: Locate the calcium channel blocker table and list the agent(s) that should be adjusted in patients with renal failure. Agents: ____________________________________________________________________________________________ 2) Site: The official National “American Heart Association (AHA)” Homepage (http://www.americanheart.org)
• Assignment: Go to the “Scientific Statements and Practice Guidelines” area. Look at the ACC/AHA 2004 Practice Guidelines for the Management of Patients With ST-Elevation Myocardial Infarction--Full Text
• Note: You can find this by going first to “Science & Professional” link on the left hand side of the homepage. On the pull-down list click “My American Heart for Professionals” link, then click the upper tab for “Practice Guidelines”. You will see “Statements and Guidelines” and under this heading click the “Topic List” which will lead to cardiovascular areas to search for the relevant guideline.
Print off page 5 of this PDF document (HyperText Markup Language [HTML] version is does not work) and write out, in the space below, the Classifications I, II, IIa, IIb, III used to describe the levels of evidence used in AHA/ACC documents to qualify a recommendation.
I
II
IIa
IIb III
3) Use your access to Lexi-Comp (either website or PDA database) clinical software to answer the following question. What is the maximum dose per day for ezetimibe (Zetia™). (Use Lexi-Drugs installed book if using a PDA)? Answer: ______________________ 4) Site: The official “theheart.org” Homepage Assignment: Register yourself on the “theheart.org” website. 5) Site: Obtain PDF electronic journal articles online from the U of M Bio-Medical Library (Instructions on Webpage: http://www.courses.ahc.umn.edu/pharmacy/5822/InstructionsforJournalsonWeb.pdf). Assignment: Use the guide to search online for and print ONLY the abstract (1st page, p.1495) from the ASCOT-BPLA trial (Dahlof, B, et al. Prevention of cardiovascular events with an antihypertensive regimen of amlodipine adding perindopril as required versus atenolol adding bendroflumethiazide as required, in the Anglo-Scandinavian Cardiac Outcomes Trial-Blood Pressure Lowering Arm (ASCOT-BPLA): a multicentre randomized controlled trial. Lancet 2005;366:895-906). You Must Print the PDF page. The Free Text, HTML format, or the page from the website itself will not be acceptable. Only PDF pages handed in will count for your completion of this exercise. Staple the PDF printout of the abstract to back of this page.





























