Embed Size (px)
Citation preview

28 JOGNN © 2007, AWHONN, the Association of Women’s Health, Obstetric and Neonatal Nurses
Objective : To construct a substantive theory of postpartum fatigue.
Design : Grounded theory. Setting : Participants were recruited in the hos-
pital after delivery and interviewed in their homes. Participants : Thirteen primiparae ( n = 5) and
multiparae ( n = 8) women between 2 and 5 weeks postpartum from diverse ethnic, age, obstetric, and fi nancial contexts were theoretically sampled.
Results : Persevering was the central human process around which the grounded theory emerged. The process of persevering was explained through the relationships of infl uencing factors, postpartum fatigue, coping techniques, self-transcendence, and caregiving. Participants persevered in caregiving of infants and older children in spite of an overwhelm-ing desire to rest and sleep using self-identifi ed cop-ing techniques in combination with the belief that their children brought purpose and meaning to their lives.
Conclusions : The theory “ Persevering Through Postpartum Fatigue ” contributes a more complete un-derstanding of the complex phenomenon of postpar-tum fatigue as it is expressed in the everyday lives of women during the postpartum period. The results may be used to develop and implement health- promoting nursing interventions to reduce postpartum fatigue and its health-related consequences. JOGNN, 36, 28-37; 2007. DOI: 10.1111/J.1552-6909.2006.00116.x
Keywords : Grounded theory — Maternal-infant sleep pattern confl ict — Persevering — Postpartum fatigue — Self-transcendence
Accepted: November 2006
Postpartum fatigue (PPF) is a predominant concern of women after childbirth ( Kline, Martin, & Deyo,
1998; Mercer, 1986; Troy, 2003 ). When ongoing and unrelieved, PPF can have untoward effects on maternal health, functional status, and infant development, de-lay maternal return of functional status, and promote early weaning from breastfeeding ( McVeigh, 2000; Parks, Lenz, Milligan, & Han, 1999; Pugh & Milligan, 1998; Tulman & Fawcett, 1988; Tulman, Fawcett, Groblewski, & Silverman, 1990 ). Postpartum fatigue is a health-related pattern defi ned in the literature as an overwhelming sense of exhaustion and decreased ca-pacity for physical and mental work following child-birth ( Parks et al., 1999; Rubin, 1984 ; Troy).
Especially important to the health of women and families is the growing evidence linking PPF and postpartum depression (PPD). Fatigue is a symptom of PPD, a diagnostic criterion of PPD as well as a major feature of the depressive experience ( American Psychiatric Association, 1994; Beck, 2006 ). Recently, two studies reported that fatigue at days 7 and 14 after delivery predicted depressive symptoms at 28 days after delivery ( Bozoky & Corwin, 2002; Corwin, Brownstead, Barton, Heckard, & Morin, 2005 ). Given the close relationship between PPF and PPD, combined with the evidence that an estimated 10% to 43% of women develop PPD, a better understand-ing of PPF has the potential to translate into interven-tions aimed at reducing the severity and incidence of PPD through targeted PPF-reducing interventions ( Baker et al., 2005; Berenson, Breitkopf, & Wu, 2003 ; Foss, 2001; Goyal, Murphy, & Cohen, 2006; Logsdon, Wisner, & Pinto-Foltz, 2006 ).
Although women often believe that PPF is a temporary condition that will lessen when everyday routines are reestablished, empirical evidence suggests the contrary ( Milligan, Lenz, Parks, Pugh, & Kitzman, 1997 ). In general, PPF does not signifi cantly improve
CLINICAL RESEARCH
Persevering Through Postpartum Fatigue Jennifer Runquist

January/February 2007 JOGNN 29
over the fi rst 6 weeks after delivery ( Troy, 2003 ). Instead, PPF either becomes progressively worse through the fourth week after delivery or remains stable at levels noted shortly after delivery ( Bozoky & Corwin, 2002; Troy & Dalgas-Pelish, 2003 ). Moreover, Parks et al. (1999) noted that PPF may continue into the second year after delivery in more than half of women.
Postpartum fatigue is a complex phenomenon theorized to change in relation to numerous physical, psychological, and situational variables ( Milligan et al., 1997 ). A solid grasp of factors that can contribute to and effectively reduce PPF continues to elude researchers. Part of the phenomenon ’ s complexity arises from the dynamic nature of PPF. The onset or amelioration of PPF can be rapid or insidious, and PPF can worsen, improve, or even com-pletely abate in a matter of hours or days.
Identifi cation of PPF ’ s health-related consequences arose out of research that examined how fatigue changed across weeks and months ( Lee & Zaffke, 1999; Parks et al., 1999; Troy & Dalgas-Pelish, 2003 ). Research on PPF has pre-dominantly measured either the incidence of PPF or the symptoms and severity of PPF over single time points rang-ing from twice-a-day measures to weekly/monthly mea-sures over the fi rst postpartum year. Yet, researchers still do not fi rmly grasp the factors that contribute to changes in PPF across time. This knowledge gap must be bridged in order to eventually develop interventions that can effec-tively respond to the dynamic nature of the phenomenon.
Since the literature has identifi ed PPF as a process- oriented phenomenon (e.g., changing in relation to factors over time; Milligan et al., 1997 ), the purpose of this study was to examine the everyday process of PPF through de-velopment of a substantive theory. This study assumed that the most effective means for studying the complex and everyday process of PPF was to interview women ex-periencing the phenomenon. As a result, this study began with two primary research questions: (a) how do women describe their experience of PPF and (b) how do women manage in their everyday lives while fatigued?
Methods
Research Design Scholars have identifi ed the need for methodologies
that can accommodate the complexity of PPF ( Parks et al., 1999 ). As a result, grounded theory was chosen because this methodology offered the benefi t of a process-oriented methodological approach that could accommodate and capture everyday complexities of phenomena ( Glaser, 1992; Glaser & Strauss, 1967 ).
Procedure Prior to recruitment and data collection, approval to
conduct the study was obtained from the hospital and
university institutional review boards. Study participants were recruited from an inpatient postpartum nursing unit at a regional academic medical center in the southwest Uni-ted States. Using the principles of theoretical sampling ( Glaser & Strauss, 1967 ), initial participant recruitment was directed toward obtaining participants who represented a wide range of ethnic, social, economic, health, and obstet-ric contexts. As data analysis continued, participants were recruited based upon the needs of the emerging theory.
After orienting nurses on the postpartum unit to the study, the researcher informed staff nurses of particular characteristics needed of potential participants (e.g., cesar-ean, vaginal delivery; primiparous, multiparous). Staff nurses having patients with those characteristics would then ask those patients at an appropriate time for permis-sion to be approached by the researcher. When a potential participant expressed interest in the study and permission to approach was obtained, the researcher then reviewed the criteria required for inclusion in the study. Inclusion criteria were as follows: at least 18 years old, able to read and write English, living in or near a particular city in Arizona, birthed a healthy infant in the previous 4 days, able to be contacted by home or cell phone, and reported no ongoing treatment for a mental health or substance abuse problem. Upon meeting the inclusion criteria, the purpose of the study was explained to the participant. Then, informed consent was obtained, followed by demo-graphic and contact information.
Study participants were telephoned 1 to 2 weeks after delivery to schedule an interview at a place of the partici-pant ’ s choosing (12 interviewed in their home, 1 inter-viewed at a coffee shop). Interviews took place between 2 and 5 weeks after delivery ( M = 3.6 weeks, SD = .81) when PPF is known to be an ongoing and intense feature of post-partum life ( Mercer, 1986; Troy, 2003 ).
A semistructured interview schedule guided the investi-gator during the audiotaped interviews, which lasted be-tween 15 and 60 minutes ( M = 38 minutes, SD = 11). Questions on the interview guide were modifi ed three times based on the needs of the ongoing data analysis. Some questions were kept through all three iterations (e.g., What is it like to have fatigue with a newborn baby? What makes your fatigue worse/better? How does being fatigued change you?). Some questions were added to fur-ther explore emerging concepts (e.g., How does your body/mind feel when you are tired? How do you feel about your baby/about yourself when fatigued?). Some questions were deleted when they did not yield data relevant to the analysis (e.g., Is there anything that could have helped to decrease your fatigue?). Field notes of observations were recorded immediately after leaving the interview. Interviews were transcribed by the investigator. Transcription accu-racy was checked by a colleague who read randomly chosen transcripts while listening to the audiotape. Participant con-fi dentiality was ensured through use of pseudonyms.

30 JOGNN Volume 36, Number 1
Data Analysis The data were analyzed using the constant compara-
tive method in which the analysis begins with coding of the fi rst transcript and ends with the generation of the grounded theory ( Glaser, 1992 ). This method uses a sys-tematic process of continuously comparing each piece of data (e.g., words, lines, phrases) with every other piece of data to identify concepts, concept properties and de-limiters, and eventually relationships among concepts, which generate a theory that is “ grounded ” in the data (Glaser). Data analysis is an iterative process that occurs simultaneously with participant recruitment and data collection.
As the analysis proceeded, participants were sampled for their ability to contribute to a comprehensive understand-ing of the phenomenon. For example, women with more than two children were sampled at one point to better un-derstand the fatigue process in women with more than two children. Data analysis continued until redundancy emerged at which point the data appeared theoretically saturated because no new concepts or relationships related to the theory emerged with further interviews ( Glaser, 1992 ).
Careful attention was paid to establishing rigor through the criteria of credibility, transferability, dependability, and confi rmability ( Lincoln & Guba, 1985 ). A few of the strategies used to enhance the trustworthiness of the fi nd-ings included member checking (i.e., asking participants for feedback on emerging hypotheses), peer debriefi ng (i.e., regular discussions of emerging results with an expe-rienced grounded theorist), a refl exive journal, and an in-dependent confi rmability audit (where a grounded theorist colleague not involved in the study reviewed all coding, abstracting, and tracked decisions and documentation).
Results
Sample Thirteen women were interviewed. Theoretical satura-
tion (i.e., repetition of all relevant concepts and categories) was obtained at 10 participants, and 3 additional partici-pants were interviewed to ensure redundancy and thickness of the data ( Glaser & Strauss, 1967 ). Seventeen women originally consented to participate, but 4 were lost to fol-low-up. In the fi nal sample ( n = 13), participants varied in age from 19 to 41 years ( M = 29.1, SD = 7.5) and ethnically refl ected the local geography (Caucasian = 46%; Hispanic = 38%; African American = 8%; Native American = 8%). Years of education varied from 12 to 22 years ( M = 14, SD = 3). Sixty-nine percent ( n = 9) were married. Thirty-one percent ( n = 4) were single where two participants lived with their boyfriends, and two participants reported no partner. Additionally, 69% gave birth vaginally and 31% operatively. Five participants (39%) were primiparous, four participants had two children (including the infant), two
participants had three children, and two participants had four children. Eight (62%) participants breastfed their infants, three (23%) bottle-fed, and two (15%) breast- and bottle-fed. Financially, the sample reported being not at all comfortable ( n = 2), somewhat comfortable ( n = 8), very comfortable ( n = 2), and extremely comfortable ( n = 1).
To better understand participants ’ health context, partici-pants were asked if they had any health problems. Seven (54%) participants reported no health problems before, dur-ing, or after the pregnancy. However, six women experienced one or more health problems including obesity, gestational diabetes, prophylactic therapy for past pulmonary embo-lisms, severe nausea in pregnancy, chronic coccyx pain after a second-trimester car accident, chronic constipation, and an emergent 7-day postpartum rehospitalization for life-threat-ening fl uid buildup in the chest cavity of unknown etiology.
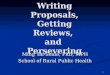
Grounded Theory Model: “ Persevering Through PPF ”
Figure 1 illustrates the grounded theory titled “ Perse-vering Through PPF ” that emerged from participants ’ ac-counts of PPF. The theory has fi ve major concepts (PPF, infl uencing factors, coping techniques, self-transcendence, and caregiving). Persevering is the human process that in-tegrated the theory ’ s concepts across time ( Fagerhaugh, 1986 ). Each major concept will be discussed in turn fol-lowed by the persevering process.
“ Postpartum fatigue changes everything. It changes your mood, your happiness level. It
changes everything. ”
Postpartum Fatigue . Postpartum fatigue emerged as an overwhelmingly negative, distressing, subjective experi-ence that changed every aspect of participants ’ lives.
It changes everything. It changes your mood, your hap-piness level. It changes everything (Maria). Seems like everything. How you feel is different. How you dress is different ‘ cause you don ’ t, don ’ t want to get dressed. I think eh, when you ’ re not getting enough sleep it really affects every part of you. Your mind isn ’ t right (Janet).
Not a single participant said PPF had any positive ben-efi t in their life. Postpartum fatigue was distressing and made relationships with others and everyday tasks more diffi cult. “ I just think that you know it really does put a strain on relationships ” (Monica). “ You just feel helpless I think when you ’ re tired ” (Kari). “ I think it ’ s the worst type of fatigue, because you don ’ t see an end to it ” (Kari).

January/February 2007 JOGNN 31
PPF was operationalized by four integrated dimensions: mental, physical, stress-worry, and frustration. Each di-mension had particular manifestations that distinguished each from the others. When fatigued, participants reported experiencing manifestations in multiple dimensions.
In the mental dimension, PPF included negative self-perceptions, irritable, cranky mood, and a reduced ability to pay attention due to a slowing down of the mind, lack of focus, or unsteady or rambling thoughts.
Just rambling, like nothing ’ s steady. Nothing is, noth-ing is, nothing is straight. Just seems like everything ’ s just a blur. That ’ s how it feels (Janet). You don ’ t have no focus on anything (Janet).
Participants ’ negative perceptions were directed toward themselves, not their infants. “ I feel like I ’ m failing [my children] somehow. Uh, I, I don ’ t think of them as so much a burden as I feel like you know, I, I ’ m more of a disap-pointment to myself than I am feeling that they ’ re a burden ” (Monica).
Several physical manifestations collapsed into the cate-gories of body soreness, body aches, and weakness. Pain was a component of each of these categories. Participants said that body soreness and body aches occurred in rela-tion to either particular body parts (e.g., the back) or to whole-body soreness or aching. Weakness was a lack of feeling strong or feeling like the body would give in if pushed too far. “ Like you could just feel like you just push through yourself that ’ s how weak you be ” (Janet).
The stress-worry dimension was a prominent and unique component of PPF. Stress-worry (and also the frustration dimension discussed later) was placed in a category separate
from the mental dimension for two reasons: (a) the intense distress experienced with stress-worry and its ubiquitous occurrence in participants when fatigued meant stress-worry emerged as a defi ning feature of PPF and (b) the relationship that stress-worry had with PPF was different from the mental dimension.
Stress-worry referred to how participants felt stress pre-dominantly in the form of worry over identifi ed stressors (e.g., cleaning, cooking, infant care, visitors). Worry was continuous in nature and often manifested most intensely when participants wished to fall asleep. Participants were kept awake “ worrying ” about all that they had not ac-complished or still remained to be accomplished.
When you ’ re fatigued and you ’ re forced to lay down and all you do is think about what you have to do so it ’ s kind of like no matter how much you want to rest you ’ re still you know, feeling like you ’ re helpless or out of control (Monica).
Both the stress-worry and frustration dimensions (discussed next) had a distinctly cyclical relationship with fatigue. Stress-worry, for participants who experienced this, increased fatigue severity and worsening fatigue increased stress-worry.
If you ’ re feeling that stress all the time, sort of that anxiety, it, it really does sap you and make you more tired … it defi nitely one has to do with the other. It ’ s kind of a vicious cycle (Linda).
The same cycling occurred in the frustration dimension where frustration increased fatigue and fatigue increased frustration.
FIGURE 1 Persevering Through Postpartum Fatigue.

32 JOGNN Volume 36, Number 1
I can ’ t let go of things even though I ’ m fatigued. You ’ d think I could say oh, I ’ m just too tired to do that I can ’ t do it, but instead I get frustrated right? I ’ m too tired to do it, but I wanna do it (Kari).
Whereas stress-worry was manifested in response to stressors, frustration was manifested in response to being unable to carry something through. What participants most wanted and could not obtain was uninterrupted sleep. When participants became frustrated, they re-ported being bothered by the littlest of irritants and lacked patience.
I don ’ t have any patience. I can ’ t keep a little bit of the patience. It ’ s just like (exasperated ah!) (Cathy).
When fatigued, participants stated that it was easier to take out their frustrations on family members because they did not possess their usual level of patience. Maria describes the diffi culty she faces relating to her 2 year old when fatigued.
… and then little kids are little kids and you just get so overwhelmed and it ’ s like “ don ’ t do that! ” And you try not to scream and be impatient, but sometimes its hard (Maria).
Infl uencing Factors . There were three groups of fac-tors that infl uenced PPF: (a) maternal-infant sleep pattern confl ict, (b) infant characteristics, and (c) fatigue limiting factors. The dissonance or confl ict between the mother ’ s and infant ’ s sleep patterns emerged as the foremost infl u-ence on PPF for both primipara and multipara partici-pants; however, fi rst-time mothers were surprised by the degree of disruption to their sleep patterns.
I think what I ’ ve been fi nding most fatiguing is not sleep-ing in long blocks. It ’ s the 1½ hours here, another hour and a half. I really want my 5 hours at a time (Kari).
Infant characteristics were behaviors of the infant that tended to either improve or worsen PPF. For instance, characteristics that improved PPF included having a “ good ” infant, which participants defi ned as an infant who was content or one who fell asleep quickly after wak-ing to eat. Infant characteristics that worsened PPF in-cluded infants who took 60 minutes to eat, infants who fell asleep while eating, infants who slept in short intervals (i.e., 1-3 hours), and infants who seemed gassy, colicky, or generally discomforted and cried for hours at a time.
So last night I got 2 hours of sleep (Kari). He can cry 8 hours straight and not sleep (Kari). We were just so tired, it was 2 in the morning. He ’ d be crying since 8 (Kari).
Fatigue limiting factors represented a group of fi ve fac-tors that appeared to limit PPF. First, participants who
had prior infant experience (particularly fi rst-time moth-ers) seemed more adept at caring for an infant and were less distressed at having an infant who required constant caregiving.
When I was about 15 my mom had a baby. So we were always around. I actually, I ’ m handling, I ’ m handling it OK, being a new mother ‘ cause I would take care of my little brother. We were always there (Elisa).
Second, the availability of instrumental support, e.g., practical assistance with infant care ( Finfgeld-Connett, 2005 ) was particularly important to participants ’ abilities to both cope with the fatigue and limit the cycle of wors-ening fatigue. Third, having multiple diverse sources of information (such as family, friends, health care profes-sionals, books, Internet; not just 10 expert baby books) of which participants could ask questions and receive advice seemed to limit PPF, especially for fi rst-time mothers.
And I don ’ t, I don ’ t really have too much questions, because my mom, my sister the, that nurse and the In-ternet. Those things help me a lot (Elena).
Fourth, when fatigued, the ability to “ let go ” and not worry about undone tasks was a factor that limited PPF.
And then with the baby I don ’ t really care too much about the house you know, I go slow, slow and I don ’ t care if it ’ s, you know messy or not (Elena).
Conversely, PPF was worse in participants who were either unable to set aside nonessential tasks or worried constantly about tasks if they did set them aside.
I feel a lot more fatigued and overwhelmed if I ’ m you know, thinking OK I gotta get this done, I gotta do this (Linda).
Finally, in this study, a number of participants (both primipara and multipara) expressed surprise and distress over the length of the postpartum healing process. They had expected to be “ up and running ” at a prepregnant level of functional status 3 to 7 days after delivery.
I mean giving birth also makes you really tired after a couple of days, a little bit stressed like I said, because you ’ re trying to do the same things you used to do be-fore and you have to take time to recover (Elisa).
The distress created by the expectation that they should have already recovered affected multiple PPF dimensions. First, these unrealistic expectations contributed to stress, and participants worried about not having fully healed yet. Second, participants felt frustrated over not having fully recovered from childbirth, believing the reason was some personal defi cit or fault.

January/February 2007 JOGNN 33
I ’ m more of a disappointment to myself than I am feeling that they ’ re a burden, you know what I mean. It ’ s like I should be able to do whatever (Linda).
Additionally, these unrealistic expectations worsened participants ’ self-perception, which worsened PPF by compelling participants to try harder and fi ght the fatigue more.
I feel like I can ’ t do everything I want to do. Like um, incapable of um, of handling things the way I usually do, so I guess I kinda feel like um, a little disappointed in myself (Lilia).
Women who had realistic expectations of how long it takes to resume daily activities after childbirth spoke of respecting the needs of their bodies and minds to heal. These participants tended to have better fatigue experiences compared to women with unrealistic expecta-tions about the postpartum healing process.
I don ’ t really care too much about the house you know, I go slow, slow and I don ’ t care if it ’ s, you know messy or not (Elena).
Coping Techniques . Participants identifi ed a variety of techniques they used to manage their fatigue. In the model ( Figure 1 ), these techniques, identifi ed by participants as “ coping techniques ” interfaced between PPF and the infl uencing factors. Coping techniques generally fell into one of two categories based on their intended effect: (a) techniques that directly functioned to temporarily reduce PPF manifestations and (b) techniques that indirectly affected PPF by changing some aspect of the infl uencing factors. Techniques such as drinking coffee, showering, or conserving energy by withdrawing from family were employed in response to an immediate need to reduce perception of fatigue but did not actually address the need for sleep.
I try and stay away from everybody … like last night I was real tired I just try and stay away from everybody ‘ cause I don ’ t wanna make anybody feel uncomfortable and I don ’ t want ‘ em all to be pitying to you, so I stay away from everybody (Janet).
Techniques such as getting the baby into a routine, in-creasing the amount of time between infant feedings, or going to bed early were attempts to change the infl uencing factors such as infant characteristics, or reducing the maternal-infant sleep pattern confl ict.
I tried to get him in a pattern where I would, he would be falling asleep, I would just try to keep him awake to keep fi nishing to get full completely before he fell, fell asleep. That way I could have more rest (Lilia).
Self-Transcendence . In the nursing literature, self- transcendence refers to an ever-present capacity to grasp perspectives that exceed everyday confi nes and limitations ( Reed, 1991, 2003 ). A broadened life perspective facili-tates a person ’ s ability to fi nd meaning and purpose in life and is often more apparent during times of heightened vul-nerability ( Reed, 2003 ). In this study, self-transcendence was a salient element of the persevering process that inter-faced between PPF and caregiving. When fatigued, partici-pants reported feeling an overwhelming need to rest and sleep. However, the caregiving demands of the infant and older children competed with the participants ’ ability to act on feeling the need to rest and sleep. In these instances, participants called upon an inner resource to enable them to persevere with caregiving. Participants found the strength to persevere through a belief that their children brought purpose and meaning to their lives.
I just realize that his needs are more important than mine and I ’ ll fi nd another time to sleep. It ’ s just kind of a understanding of what ’ s more important is probably the way I cope with it (Ann).
Concurrently, infants and other children were perceived by the participants to be vulnerable. This vulnerability, manifested by the need for continuous caregiving, com-pelled the women to persevere in spite of fatigue.
My kids motivate me. Obviously I have to take care of them. They can ’ t take care of themselves. And I, I just know I have to, I have to be here for my family. That ’ s my motivation. To keep going (Susan).
Caregiving . Caregiving was both implicit to the perse-vering process and the outcome of the persevering process. Caregiving included care of infants and older children as well as the maintenance of those everyday household re-sponsibilities that facilitated ongoing childcare (e.g., food preparation for older children). Participants did not ex-pand upon these three facets of caregiving, nor was care-giving self-directed. Caregiving was couched in terms of others ’ needs, and participants minimized their own needs, especially for sleep and self-care, in order to keep up with the caregiving demands of their children.
Participants minimized their own needs, especially for sleep and self-care, in order to keep up with the caregiving demands
of their children.

34 JOGNN Volume 36, Number 1
Participants identifi ed caregiving as the dominant focus at this time in their lives, and all decisions were evaluated within the context of providing ongoing care to the infant and older children. Caregiving was a paradox, being dif-fi cult and challenging, yet also enjoyable and meaningful. Postpartum fatigue made caregiving more diffi cult.
I have to get up and make sure his diaper is changed and he ’ s clean and he ’ s taken care of and that can be hard when you can barely keep your eyes open (Ann).
Within the context of PPF, relationships with people other than the infant and older children (e.g., spouses, ex-tended family) moved into the background of participants ’ attention because participants gave priority to their care-giving responsibilities. Relationships with other persons became a priority when those relationships could facilitate a reduction of PPF (e.g., providing childcare so the par-ticipant could nap). In Janet ’ s scenario, she moved from her boyfriend ’ s apartment back into her mother ’ s house because her mother could help her develop a routine.
That ’ s why I ’ m here at my mom ’ s ‘ cause she ’ s helping me to get that stuff together (Janet).
The process of persevering . Persevering integrated all aspects of the model and explained how women continued caring for their infants in the face of ongoing PPF. Perse-vering was an implicit and continuously ongoing feature of participants ’ lives within the PPF process.
I know I need to attend to his needs no matter how tired I am. I have to get up and feed him (Ann).
I just kind of deal with it and just say OK it ’ s just a little bit longer I take like every hour at a time and I go from there (Maria).
Perseverance is a steady persistence in adhering to a course of action, belief, or purpose (Editors of the Ameri-can Heritage Dictionaries, 2000 ). In this study, all par-ticipants adhered to the action, belief, and purpose of continuing to care for their infants and older children in spite of all but the most debilitating fatigue (i.e., physical or mental shutdown).
I think if I got ill. If I got real sick I ’ d probably stop and take a rest. Take a, take a look at the situation again. But with me for some reason it always takes something drastic to happen before you know, I ’ ll actually rest (Susan).
This study reformulated persevering from a basic social psychological process (a concept arising out of the socio-logical tradition) into a “ human process ” (Reed & Runquist, in press). Labeling persevering as a human process better represents the process of PPF as a nursing concept by
embracing the social, physical, mental, spiritual, and health-related processes involved with PPF.
Summary of the Model “ Persevering Through PPF ” The process of persevering was explained through rela-
tionships among infl uencing factors, PPF, coping techniques, caregiving, and self-transcendence. Participants identifi ed three groups of factors as having the most infl uence on PPF across the fi rst 5 weeks after delivery. These infl uencing fac-tors functioned to either improve or worsen PPF. Postpar-tum fatigue was characterized by four dimensions (mental, physical, stress-worry, and frustration) each of which had empirical, context-dependent manifestations. Profound negative feelings and an overwhelming need to rest and sleep brought on by PPF were offset by the use of coping techniques and self-transcendence, which enabled women to persevere in the provision of care to their children.
Discussion and Implications
The theory generated in this study provides a fi rst glimpse at the everyday process of PPF from the point of view of women experiencing the phenomenon. The theory lends support to the existing evidence of PPF as a multidi-mensional, complex, dynamic, and context-dependent concept that manifests negative effects in women ’ s mental, physical, and social health. The fi ndings of this study also extend nursing ’ s understanding of PPF in a number of areas that have potential for future intervention development. For instance, Rogan, Shmied, Barclay, Everitt, and Wyllie ’ s (1999) grounded theory study of fi rst-time mothers reported that infant behavior, social support, and previous infant experience all mediated the process of becoming a mother. These factors were identifi ed in the current study but more specifi cally linked to PPF as infl uences (both positive and negative) as well as avenues for interventions for managing or limiting PPF severity.
While the results of this study need further refi nement, evaluation, and extension, there are basic nursing inter-ventions identifi ed from the results of this study that can translate to the postpartum bedside, community-based maternal and pediatric care settings, and prenatal and postpartum educational settings. For example, nurses should teach women and their families about a mother ’ s basic need for rest and sleep after childbirth, develop real-istic expectations for themselves, and strategize with fami-lies about how to create social support systems that meet mothers ’ needs within the postpartum period.
A number of the PPF manifestations identifi ed by par-ticipants in this study are supported in prior literature on motherhood experience ( Barclay, Everitt, Rogan, Shmied, & Wyllie, 1997; Martell, 2001; Mercer, 1986; Rubin, 1984 ). Postpartum fatigue manifestations such as painful ach-ing, self-doubt, continuous worry, losing patience, and rambling thoughts (i.e., reduced focus or attention) are

January/February 2007 JOGNN 35
potential “ red fl ags ” for women to self-identify when they are entering the vicious cycle of worsening fatigue and need to seek help from support networks to rest.
However, most of the PPF manifestations are subjective and not necessarily visible to family members, often lead-ing women to suffer in silence using coping techniques such as drinking coffee that help them get through the day but do not actually address the problem that a woman ’ s basic human need for sleep and rest is not being met. As demonstrated by the complexity of PPF noted in this study ’ s model, simply teaching about PPF manifestations would not be an effective intervention without also exam-ining the woman ’ s environmental context and society ’ s social construction of motherhood.
In today ’ s environment, motherhood ideology ( Koniak-Griffi n, Logsdon, Hines-Martin, & Turner, 2006; Wearing, 1984 ) remains a strong infl uence on women as evidenced by a number of the participants in this study believing they could “ do it all, ” often only days after giving birth. As well, women live in a context that does not provide infor-mation about the postpartum healing process nor the amount of time and rest that healing requires ( Kline et al., 1998 ). Instead, media, health care, and pregnancy experts sensationalize birth to such a degree that what comes after the birth is anticlimactic, manageable, and believed to be easy or natural ( Speier, 2001 ; Technical Working Group, World Health Organization, 1999; Woolett & Parr, 1997 ). As nurses at the bedside, in the community, and in clinics, we have the opportunity to teach women and families how their lives will change after childbirth and the amount of time, energy, and kinds of support they will need not only those fi rst weeks after delivery but also that fi rst year after delivery. Giving women permission to ask for help in this “ do-it-all ” society can be empowering.
However, nurses must also teach families that the post-partum period is a vulnerable time for women in which women who are accustomed to “ doing it all ” may not re-alize they are exhausted or “ on the edge. ” Nurses should promote family communication on planning for frequent, planned activities that give the mother respite from her caregiving responsibilities so that she can not only have knowledge about realistic expectations about the postpar-tum healing process but also the tools that enable her to apply that knowledge to her everyday life.
Nurses should promote family communication on planning for frequent,
planned activities that give new mothers respite from their caregiving responsibilities.
Comparison of PPF With the Existing Theoretical Literature
The theory generated from the results of this study di-verges from the existing PPF literature in two signifi cant ways: (a) the characterization of PPF ’ s dimensions, and (b) how PPF changes. Lenz and Pugh (2003) identify PPF ’ s dimensions as timing, intensity, quality, and distress, which arise out of their conceptualization of PPF as a symptom. In this study, participants did not conceptualize their fatigue as a symptom but instead identifi ed the dimensions of PPF as physical, mental, stress-worry, and frustration. These dimen-sions were operationalized in terms of context-dependent manifestations (e.g., body soreness, decreased attention), which could possibly serve as empirical indicators of PPF in the future. Postpartum fatigue was the pattern constructed from the constellation of manifestations within each of the four PPF dimensions. The second major difference with the literature related to changes in PPF. Lenz and Pugh theorized that variations in PPF occur based on the dimensions of tim-ing, intensity, quality, and distress. However, in this grounded theory, participants perceived that the infl uencing factors (i.e., maternal-infant sleep pattern confl ict, infant character-istics, and fatigue limiting factors) and coping techniques changed the dimensions and manifestations of PPF.
This study adds to the existing literature on self- transcendence. Self-transcendence has most often been de-scribed within illness and end-of-life contexts and diffi cult life circumstances such as homelessness ( Coward, 2005; Runquist & Reed, in press; Upchurch & Mueller, 2005 ). Spirituality and self-transcendence within childbearing contexts are most often discussed in relation to the birth experience ( Budin, 2001 ). This is the fi rst published study to identify self-transcendence as a salient element of a postpartum health-related pattern such as PPF. Self- transcendence arises partly out of a developmental paradigm ( Reed, 1991 ). As a source of resilience during developmen-tally related life transitions such as adolescence and older age, self-transcendence may have applicability to broader postpartum phenomena and motherhood experience.
Limitations
This study examined PPF over the fi rst 5 weeks after delivery. As a result, caution should be used when evaluat-ing the usefulness of the theory beyond 5 weeks as the postpartum period is a time of accelerated change. Some aspects of the theory may retain usefulness given that PPF has been documented as long as 18 months after delivery ( Parks et al., 1999 ); however, it is likely that parts of the theory such as infl uencing factors and PPF manifestations will change as time passes. Likewise, the transferability of the theory beyond the participant ’ s characteristics and con-texts should be undertaken with caution, especially given the highly individualized, context-dependent nature of PPF. An additional limitation of this study was the inclusion of

36 JOGNN Volume 36, Number 1
participants who had both chronic and acute health condi-tions that could impact their fatigue experience separate from the childbirth and postpartum experience. In partic-ular, one participant reported being on prophalyxis anti-coagulation therapy for a history of pulmonary embolism, and one participant reported emergent hospitalization af-ter delivery for fl uid in her chest cavity.
Implications for Nursing Research
The theory “ Persevering Through PPF ” provides a more explanatory view of PPF. As an initial grounded theory, further investigation should take place in populations in different geographic, ethnic, social, age (including adoles-cents), and obstetric contexts to identify its usefulness and further refi ne its components. Additionally, with evidence linking PPF and PPD, this grounded theory provides initial insight into identifying what it is about PPF that changes women ’ s risk for depressive symptoms (e.g., basic need for sleep not being met). Concepts such as maternal-infant sleep pattern confl ict have the potential to be developed into measures and tested for their relationship to depres-sive symptomatology and infant outcomes. Likewise, qualitative investigations comparing the fatigue process across time in women with and without depressive symp-tomatology could further elucidate how PPF can be dif-ferentiated from PPD.
Finally, these results arose out of the voices of diverse postpartum women and refl ect their own priorities, needs, and goals. This study has identifi ed avenues for the future development of interventions that have the potential to be responsive and useful for women arising out of diverse contexts. Future studies on PPF should continue to strive for inclusion of diverse mothering experiences in order to capture a grounded and rich understanding of the phenomenon.
Acknowledgement
The author thanks Dr. Pamela G. Reed, College of Nursing, University of Arizona, and Drs. Karen Morin, Rachel Schiffman, and Teresa Johnson at the University of Wisconsin-Milwaukee.
REFERENCES
American Psychiatric Association . ( 1994 ). Diagnostic and statis-tical manual of mental disorders: DSM-IV . Washington, DC : Author .
Baker , L . , Cross , S . , Greaver , L . , Wei , G . , Lewis , R . , & Healthy Start CORPS . ( 2005 ). Prevalence of postpartum depres-sion in a Native American population . Maternal and Child Health Journal , 9 , 21 - 25 .
Barclay , L . , Everitt , L . , Rogan , F . , Shmied , V . , & Wyllie , A . ( 1997 ). Becoming a mother — An analysis of women ’ s
experience of early motherhood . Journal of Advanced Nursing , 25 , 719 - 728 .
Beck , C . T . ( 2006 ). Postpartum depression: It isn ’ t just the blues . American Journal of Nursing , 106 , 40 - 51 .
Berenson , A . B . , Breitkopf , C . R . , & Wu , Z . H . ( 2003 ). Repro-ductive correlates of depressive symptoms among low- income minority women . Obstetrics & Gynecology , 102 , 1310 - 1325 .
Bozoky , I . , & Corwin , E . J . ( 2002 ). Fatigue as a predictor of postpartum depression . Journal of Obstetric, Gynecologic, and Neonatal Nursing , 31 , 436 - 443 .
Budin , W . C . ( 2001 ). Birth and death: Opportunities for self-transcendence . Journal of Perinatal Education , 10 , 38 - 42 .
Corwin , E . J . , Brownstead , J . , Barton , N . , Heckard , S . , & Morin , K . ( 2005 ). The impact of fatigue on the development of postpartum depression . Journal of Obstetric, Gynecologic, and Neonatal Nursing , 34 , 577 - 586 .
Coward , D . D . ( 2005 ). Transcending breast cancer: Making meaning from diagnosis and treatment . Journal of Holistic Nursing , 23 , 264 - 83 .
Editors of the American Heritage Dictionaries . ( Eds .). ( 2000 ). American Heritage Dictionary ( 4th ed .). Boston : Houghton Miffl in .
Fagerhaugh , S . Y . ( 1986 ). Analyzing data for basic social pro-cesses . In W . C . Chenitz & J . M . Swanson ( Eds .), From practice to grounded theory: Qualitative research in nurs-ing ( pp . 133 - 145 ). Menlo Park, CA : Addison-Wesley .
Finfgeld-Connett , D . ( 2005 ). Clarifi cation of social support . Journal of Nursing Scholarship , 37 , 4 - 9 .
Foss , G . F . ( 2001 ). Maternal sensitivity, posttraumatic stress, and acculturation in Vietnamese and Hmong mothers . Maternal Child Nursing , 26 , 257 - 263 .
Glaser , B . G . ( 1992 ). Basics of grounded theory analysis . Mill Valley, CA : Sociology Press .
Glaser , B . G . , & Strauss , A . L . ( 1967 ). The discovery of grounded theory . Chicago : Adline .
Goyal , D . , Murphy , S . O . , & Cohen , J . ( 2006 ). Immigrant Asian Indian women and postpartum depression . Journal of Ob-stetric, Gynecologic, and Neonatal Nursing , 35 , 98 - 104 .
Kline , C . R . , Martin , D . P . , & Deyo , R . A . ( 1998 ). Health con-sequences of pregnancy and childbirth as perceived by women and clinicians . Obstetrics & Gynecology , 92 , 842 - 848 .
Koniak-Griffi n , D . , Logsdon , M . C . , Hines-Martin , V . , & Turner , C . C . ( 2006 ). Contemporary mothering in a di-verse society . Journal of Obstetric, Gynecologic, and Neonatal Nursing , 35 , 671 - 678 .
Lenz , E . R . , & Pugh , L . C . ( 2003 ). The theory of unpleasant symptoms . In M . J . Smith & P . R . Liehr ( Eds .), Middle range theory for nursing ( pp . 69 - 90 ). New York : Springer .
Lee , K. A ., & Zaffke , M . ( 1999 ). Longitudinal changes in fatigue and energy during pregnancy and the postpartum period . Journal of Obstetric , Gynecologic , and Neonatal Nursing 28 , 183 - 191 .
Lincoln , Y . S . , & Guba , E . G . ( 1985 ). Naturalistic inquiry . New York : Sage .
Logsdon , M . C . , Wisner , K . L . , & Pinto-Foltz , M . D . ( 2006 ). The impact of postpartum depression on mothering . Journal of Obstetric, Gynecologic, and Neonatal Nursing , 35 , 652 - 658 .

January/February 2007 JOGNN 37
McVeigh , C . A . ( 2000 ). Investigating the relationship between satisfaction with social support and functional status after childbirth . MCN, American Journal of Maternal Child Nursing , 25 , 25 - 30 .
Martell , L . K . ( 2001 ). Heading toward the new normal: A con-temporary postpartum experience . Journal of Obstetric, Gynecologic, and Neonatal Nursing , 30 , 496 - 506 .
Mercer , R . T . ( 1986 ). First-time motherhood: Experiences from teens to forties . New York : Springer .
Milligan , R . , Lenz , E . R . , Parks , P . L . , Pugh , L . D . , & Kitzman , H . ( 1997 ). Postpartum fatigue: Clarifying a concept . In A . G . Gift ( Ed .), Clarifying concepts in nursing research ( pp . 97 - 109 ). New York : Springer .
Parks , P . L . , Lenz , E . R . , Milligan , R . A . , & Han , H . ( 1999 ). What happens when fatigue lingers for 18 months after delivery? Journal of Obstetric, Gynecologic, and Neonatal Nursing , 28 , 87 - 93 .
Pugh , L . C . , & Milligan , R . A . ( 1998 ). Nursing intervention to increase duration of breastfeeding . Applied Nursing Research , 11 , 190 - 194 .
Reed , P . G . ( 1991 ). Self-transcendence and mental health in the oldest-old adults . Nursing Research , 40 , 5 - 11 .
Reed , P . G . ( 2003 ). The theory of self-transcendence . In M . J . Smith & P . R . Liehr ( Eds .), Middle range theory for nurs-ing ( pp . 145 - 166 ). New York : Springer .
Reed , P . G . , & Runquist , J . J . (in press) . Methodological reformu-lation of grounded theory: From basic social process to human-environmental process . Nursing Science Quarterly .
Rogan , F . , Shmied , V . , Barclay , L . , Everitt , L . , & Wyllie , A . ( 1997 ). Becoming a mother — Developing a new theory of early motherhood . Journal of Advanced Nursing , 25 , 877 - 85 .
Rubin , R . ( 1984 ). Maternal identity and the maternal experi-ence . New York : Springer .
Runquist , J . J . , & Reed , P . G . ( in press ). Self-transcendence and well-being in homeless adults . Journal of Holistic Nursing .
Speier , D . ( 2001 ). Becoming a mother . Journal of the Associa-tion for Research on Mothering , 3 , 7 - 18 .
Technical Working Group, World Health Organization . ( 1999 ). Postpartum care of the mother and newborn: A practical guide . Birth , 26 , 255 - 258 .
Troy , N . W . ( 2003 ). Is the signifi cance of postpartum fatigue being overlooked in the lives of women? MCN, American Journal of Maternal Child Nursing , 28 , 252 - 257 .
Troy , N . W . , & Dalgas-Pelish , P . ( 2003 ). The effectiveness of a self-care intervention for the management of postpartum fatigue . Applied Nursing Research , 16 , 38 - 45 .
Tulman , L . , & Fawcett , J . ( 1988 ). Return of functional ability after childbirth . Nursing Research , 37 , 77 - 81 .
Tulman , L . , Fawcett , J . , Groblewski , L . , & Silverman , L . ( 1990 ). Changes in functional status after childbirth . Nursing Research , 39 , 70 - 75 .
Upchurch , S . , & Mueller , W . H . ( 2005 ). Spiritual infl uences on ability to engage in self-care activities among older African Americans . International Journal of Aging & Human Development , 60 , 77 - 94 .
Wearing , B . ( 1984 ). The ideology of motherhood . London : George Allen & Unwin .
Woolett , A . , & Parr , M . ( 1997 ). Psychological tasks for women and men in the postpartum . Journal of Reproductive & Infant Psychology , 15 , 159 - 183 .
Jennifer Runquist, PHD, RN, is an assistant professor in the College of Nursing, University of Wisconsin — Milwaukee.
Address for correspondence : Jennifer Runquist, PHD, RN, College of Nursing, University of Wisconsin — Milwaukee. PO BOX 413, Milwaukee, WI 53201. E-mail: [email protected] .