Embed Size (px)
Citation preview

Peroneal tendofascial flap: a new fascial flap for Achilles tendon coverage, apreliminary report
Ashraf Hussein ElGhamry
Plastic Surgery Unit, Department of Surgery, Fayoum School of Medicine, Cairo University, Egypt
SUMMARY. The tendons of the both peroneus longus and brevis muscles lie in the lateral compartment of the leg,enclosed in a fascial sheath. This sheath has been dissected off the tendons in three cases and opened longitudinallyforming a sheet of vascularised fascia proximally based and continuous with the peroneal muscles. These sheets of6 £ 12 cm dimensions have been successfully transposed with split skin graft to cover an exposed Achilles tendon.In another case, the peroneus brevis muscle and the opened fascial sheath of the peroneus longus tendon forming onesheet was used to cover a defect over the Achilles tendon 10 cm above the heel. This ‘tenofascial flap’ offers regionaltissue to solve the difficult lower third leg defects especially those of Achilles tendon exposure, as it is thin, pliable,allows gliding of the tendon underneath it and vascular enough to sustain a durable skin graft. q 2003 The BritishAssociation of Plastic Surgeons. Published by Elsevier Science Ltd. All rights reserved.
Keywords: peroneal, Achilles tendon, fascial flaps, adipofascial flap.
The leg is composed of three compartments. The lateralor peroneal one contains two muscles; the peroneuslongus is superficial and higher than the peroneus brevis.Its muscle fibres end at the beginning of the lower thirdof leg with a tendon passing vertically downward behindthe lateral malleolus to be inserted in the medial aspectof the foot. The peroneus brevis muscle is the deeperand lower muscle, hence its muscle fibres reach thelower third of the leg and its tendon continues deep tothat of peroneus longus behind the lateral malleolus tobe inserted in the lateral aspect of the foot. The two per-oneal tendons are enclosed in a fascial sheath part ofwhich contains synovium, which start approximately4 cm proximal to the lateral malleolus and end at a simi-lar distance distally. The sheath is single proximally andbecomes doubled distally.1
The exposed Achilles tendon following trauma, infec-tion and failed repair often poses a problem for the plas-tic surgeon. Regional tissue especially vascularisedfascial flaps is not always available to cover the exposedtendon. Many authors use free microvascular fascialflaps to cover this region.2,3 This paper present a fascialflap dissected off the peroneal tendons and used tocover an exposed Achilles tendon in four cases, with suc-cessful outcome.
Patients and methods
Four cases with chronic ulcers over the Achilles tendonwere treated in the year 2000. Table 1 illustrates thecases.
284
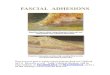
Figure 1—Pre-operative photo of post-traumatic ulcer over the tendoAchilles 3 cm above the heel.
British Journal of Plastic Surgery (2003), 56, 284–288q 2003 The British Association of Plastic Surgeons. Published by Elsevier Science Ltd. All rights reserved.doi:10.1016/S0007-1226(03)00116-4

Surgical technique
1. Debridement of the ulcer including excision of all thefibrous tissue and release of the Achilles tendon (Fig. 1).
2. Vertical skin incision at the lateral edge of thedefect running up or downwards according to the site ofthe ulcer, over the peroneus longus tendon, 1–2 cmbehind the lateral malleolus.
3. The deep fascia is opened in the incision line open-ing the peroneal compartment.
4. Release of the peroneal retinaculum with care not toinjure the fascia over the tendons.
5. Dissection of the fascial flap:(A) In three cases. Collar incision in the synovial
sheath around the peroneal tendon at the tip of the lateralmalleolus.
Splitting the tendon sheath deep to the peroneus brevistendon, then dissection of the tendon sheath off theperoneal tendons, as one sheet continues from distal toproximal till the muscle fibres of the peroneus brevismuscle are reached, and are separated from the tendonin its lowermost fibres.
Now, the tendon sheath is dissected and split to form asheet of vascularised fascia proximally pedicled withdimensions 6 £ 12 cm as shown in Figure 2.
The flap of ‘peroneal tendofascia’ is transposed tocover the exposed Achilles tendon as shown in Figure 3.
Split thickness skin graft was used to cover the fasciawith successful outcome as shown in Figures 4 and 5.
(B) In the fourth case, the defect is higher than theprevious cases as it lies 10 cm above the heel (Fig. 6).
After debridement and opening the peroneal compart-ment, dissection of the flap started at the same point bycutting the peroneus brevis tendon and its sheath, whilethe sheath of the peroneus longus only was cut.
Proximal dissection was continued by dissecting the
Table 1 Summary of cases and results
NoAge(yr) Aetiology
Site ofulcera
(cm)
Sizeofdefect Flap composition Results
1 22 Trauma 3 6 £ 9 PTFF of PB andPL tendon
Success
2 30 Trauma 4 6 £ 8 PTFF of PB andPL tendon
Success
3 15 Trauma 2 5 £ 6 PTFF of PB andPL tendon
Success
4 18 Post-burn 10 7 £ 13 PB muscle andPTFF of PL ten-don
Success
PB, peroneus brevis; PL, peroneus longus; PTFF peroneal tendofascialflap.a Distance between lower edge of defect to upper border of the heel.
Figure 2—Intra-operative photo showing the peroneal tendofascial flapof both peroneal tendons spreaded before transposition.
Figure 3—The fascial flap transposed to cover the Achilles tendon andperoneal tendons. Addison’s forceps is shown to pass deep to the flapbefore the last suture.
Peroneal tendofascial flap: a new fascial flap for Achilles tendon coverage 285

tendon sheath of peroneus longus alone but attached asone sheet with peroneus brevis muscle which was separ-ated from the periosteum of the fibula till the mid leg.
Now, a flap composed of peroneus brevis muscle andperoneal longus tendofascia is transposed to cover theexposed Achilles tendon as shown in Figure 7.
Results
In the four cases, the fascial flap survived completelyand the skin graft has taken.
The cases have been followed up for at least sixmonths for the durability of the skin graft and motilityof the ankle joint. Results are very promising as nobreakdown of the skin graft had been noticed, also allthe cases were ambulant two weeks after surgery withfull range of movement along the follow-up period.
Discussion
The tendons of the peroneus longus and peroneus brevismuscles pass vertically downwards in the lower third ofthe lateral compartment of the leg, enclosed in a fascialsheath, the lower part of it contains synovium whichsplits into two separate sheathes distal to the lateral
malleolus. The blood supply of this fascial and synovialsheath seems to come from the muscle proximally as itis continuous with its outer fascia and muscle fibres andthe author did not notice any significant vessel cut duringdissection of the four cases. In this work, the describedfascial sheath was dissected off the tendon and openedlongitudinally forming a sheet of vascularised fasciaproximally based and of 6 £ 12 dimensions. This fascialflap had been transferred to cover an exposed Achillestendon with split skin graft over it with good results. Ina higher and larger defect over the Achilles tendon, aflap of vascularised tissue of 7 £ 13 composed of pero-neous brevis muscle and split fascial sheath of peroneuslongus tendon has been transposed and covered withsplit thickness skin graft resulting in complete healingof the ulcer. This fascial flap to the best of my knowl-edge was not described before and we refer to it as a per-oneal tendofascial flap.
Dissection of this flap was easy with constantanatomy. Although this fascial flap is thin, it is vascularand strong enough to offer durable, sound coverage ofthe Achilles tendon without any functional motor deficitas proved during the follow-up period.
Fascial flaps are preferred in coverage of the Achillestendon because they are pliable and thin, yet largeenough to be wrapped completely around the tendon
Figure 4—Post-operative photo (6 ms) showing complete healing withgraft take.
Figure 5—Post-operative photo showing normal foot eversion andflexion.
Figure 6—Pre-operative photo of ulcer in post-burn scar over theAchilles tendon 10 cm above the heel.
286 British Journal of Plastic Surgery

and interposed between it and the ankle joint ifnecessary.2 Regional tissue is often insufficient to coversmall defects over an exposed desiccated tendon.2,3
Turnover distally based adipofascial flaps based on per-forators of the posterior tibial or peroneal vessels arethe available local fascial cover for Achilles tendon.4
The aetiology behind tendon exposure either trauma,infection or burn may destroy the distal perforatorsaround the tendon, hence directing the surgeon to usefree microvascular fascial flap. This paper presents alocal fascial flap expanding the armamentarium of thereconstructive surgeon to use local tissues to cover an
Figure 7—(A–C) These diagrams illustrate the standard method of raising the flap described and transposing the fascial and synovial flap. (D) Showsthe flap transposed with the peroneus brevis muscle (see text).
Peroneal tendofascial flap: a new fascial flap for Achilles tendon coverage 287

exposed Achilles tendon with the following advantages:
(1) Minimal donor site morbidity as it lies within thevicinity of the defect (Fig. 8)
(2) Ideal tissue for tendon coverage as it is originally atendon sheath and proved to be a durable cover(Fig. 9)
(3) Highly dependable vascularity with constant bloodsupply
(4) Easy dissection and short operative time(5) It lies in a deeper anatomical plane to that of both
the fasciocutaneous and adipofascial flaps, as aresult, it is not affected in most of the cases by thefactors exposing the tendon.
(6) It can cover wide defects (7–8 cm in breadth) whencombined with the peroneus brevis muscle whichdoes not exceed 4 cm in breadth when used alone5
Finally, this peroneal tendofascial flap can theoreti-cally rotate anteriorly to cover defects located in theanterolateral aspect of the lower third of the leg.
Conclusion
The tendon sheath of both peroneal tendons in the lateralcompartment of the leg was dissected off the tendonsfrom distal at the lateral malleolus to proximal, resultingin vascularised fascial flap used to cover an exposedAchilles tendon in three cases and combined with pero-neus brevis muscle in the fourth case. This fascial flap‘peroneal tendofascial flap’ has the advantages of beingthin, pliable, resilient, well vascularised to offer durableskin graft, easily dissected in short operative time andhas constant proximal blood supply usually not affectedby the various aetiologist factors exposing the tendoAchilles. This new flap may increase the capability ofthe reconstructive surgeon to cover the difficult lowerthird leg defects by regional tissue.
References
1. Williami PL, Lawrence HB, Martin MB, et al. Gray’s Anatomy, 35ed. New York: Churchill Livingstone; 1995. p. 856.
2. Upton J, Tracy MB, Steven LS, et al. Fascial flap coverage ofAchilles tendon defects. Plast Reconstr Surg 1995;95:1056–61.
3. Lee JW, Yu JC, Shieh SJ, et al. Reconstruction of the Achilles ten-don and overlying soft tissue using anterolateral thigh free flap.Br J Plast Surg 2000;53:574–7.
4. Galumbeck M, Lawrence B. Colen: coverage of the lower leg.Rotational flaps. Orthop Clin N Am 1993;V24:473–9.
5. Mathes BJ, Nahai F, Reconstructive Surgery: Principles, Anatomyand Technique, V3. New York: Churchill Livingstone; 1997. p.1444.
The Authors
Ashraf Hussein ElGhamry MD, Lecturer of General and PlasticSurgery, Fayoum School of Medicine
Batal El Salam Street, Fayoum, Egypt
Paper received 23 November 2001.Accepted 15 April 2003.
Figure 8—Early post-operative result (2 week) showing complete grafttake and donor site incision.
Figure 9—Post-operative result (6 ms) showing durable cover.
288 British Journal of Plastic Surgery