Embed Size (px)
Citation preview

Perinatal Confidential Enquiry -Congenital Diaphragmatic Hernia
December 2014
Maternal, Newborn and Infant Clinical Outcome Review Programme

Perinatal Confidential Enquiry -Congenital Diaphragmatic Hernia
December 2014
Department of Health Sciences University of Leicester 22-28 Princess Road West Leicester, LE16TP
Maternal, Newborn and Infant Clinical Outcome Review Programme
David J Field, Pauline S Hyman-Taylor, Carole M Bacon and Elizabeth S Draper

Design by: Sarah Chamberlain and Andy Kirk
Cover artist: Tana West
Printed by: University of Leicester Print Services
This report should be cited as:
Field D, Hyman-Taylor P, Bacon C and Draper ES on behalf of MBRRACE-UK. Perinatal Confidential Enquiry – Congenital Diaphragmatic Hernia. Leicester: The Infant Mortality and Morbidity Group, Department of Health Sciences, University of Leicester.2014.
© 2014 The Infant Mortality and Morbidity Studies, Department of Health Sciences, University of Leicester
Perinatal Confidential Enquiry 2014 i
Foreword
I am delighted to be able to write the foreword of this Perinatal Confidential Enquiry into the care fetuses and babies with congenital diaphragmatic hernia (CDH). Whilst recognising the central issue of outcomes for the babies, the report rightly places considerable emphasis on parental counselling and experience throughout the whole journey; from antenatal diagnosis, through impact of problems in access to intensive care cots to palliative care.
Although CDH may be deemed to be a relatively uncommon occurrence, the findings of this report are of considerable generalisable importance. Firstly, the complex nature of the condition, and its high mortality and morbidity, provide one the most sensitive ‘litmus’ tests of the integrity, leadership and effective functioning of the large multi-disciplinary teams that are needed to manage it. Secondly, the enquiry provides an in-depth and thorough evaluation of the potentially sub-optimal care which can result from specialist services being delivered on too many sites and in the absence of a networked approach.
Children and their families have the right to expect the same excellent standard of care, regardless of where they live across the UK. Despite the fact that a high level of senior input was provided in most cases, the report highlights inconsistencies across different centres and an inadequate evidence base underpinning many aspects of both obstetric and neonatal care. The commitment of those delivering care across the UK cannot be questioned, but nonetheless, variation in healthcare is almost inevitably the enemy of the good. Hence the recommendations of the authors for focusing care in a limited number of centres, with the establishment of clinical networks, is a logical and persuasive conclusion.
I congratulate the MBRRACE-UK team on the thoroughness of the report, and strongly commend it to all those concerned with producing best possible outcomes for some of our sickest babies, including both commissioners and providers of specialist neonatal services, as well as policy-makers, researchers and relevant voluntary sector groups. It makes compelling and thought-provoking reading.
Dr Hilary CassPresident, RCPCH


Perinatal Confidential Enquiry 2014
Contents
Foreword .............................................................................................................. i
Executive Summary ........................................................................................... 5Background...............................................................................................................5Congenital diaphragmatic hernia ..............................................................................5The Confidential Enquiry Process ............................................................................5
Cases ................................................................................................................................6
Summary grading system results ......................................................................................6
Key findings ........................................................................................................ 7
Recommendations ............................................................................................. 7
Acknowledgements ............................................................................................ 8Members of the MBRRACE-UK collaboration: ..................................................................8
Members of the Leicester based MBRRACE-UK team: ....................................................8
Members of the Oxford based MBRRACE-UK team: ........................................................8
MBRRACE-UK Congenital Diaphragmatic Hernia Topic Expert Group members: ..........9
MBRRACE-UK congenital diaphragmatic hernia confidential enquiry panel members: ...9
Other agencies involved: .................................................................................................10
The Maternal, Newborn and Infant Clinical Outcome Review Independent Advisory Group: ...............................................................................................................10
Healthcare Quality Improvement Partnership: ................................................................11
MBRRACE-UK Third Sector Stakeholder Group and Representatives who Attended Meetings: ..................................................................................................12
MBRRACE-UK Royal College and Professional Association Stakeholder Group and Representatives who Attended Meetings: ................................................................12
Funding ...........................................................................................................................12
Main report of the Confidential Enquiry ......................................................... 13Background.............................................................................................................13Topic Choice ...........................................................................................................13Congenital Diaphragmatic Hernia (CDH)................................................................14The Confidential Enquiry Process ..........................................................................14
Topic Expert group ..........................................................................................................15
Case note acquisition ......................................................................................................16
Reviewers ........................................................................................................................16
Case review panel meetings ...........................................................................................17
Findings from panel reviews ...................................................................................17Details of cases reviewed ................................................................................................17
Panel findings in relation to care .....................................................................................18

Perinatal Confidential Enquiry 2014
Themes ...................................................................................................................29Summary based on standards of care grading system ...................................................32
Parental perspectives .............................................................................................33
Lay report of the Confidential Enquiry ........................................................... 34In brief .....................................................................................................................34Background.............................................................................................................34What is congenital diaphragmatic hernia (CDH)?...................................................35What does the review look at?................................................................................35What did they find? .................................................................................................35
What was considered to be good care? ..........................................................................36
What was considered to be poor care? ...........................................................................36
What do parents think? ...........................................................................................36What are the recommendations following the review? ...........................................37Further reading .......................................................................................................37
References ........................................................................................................ 38
Appendices ....................................................................................................... 39Appendix 1 – Consensus statement from the Topic Expert group ..........................39
Guidelines for judging/grading of cases for review for: ..................................................39
2014 Perinatal Confidential Enquiry into Congenital Diaphragmatic Hernia ..................39
Appendix 2: Instructions for Trusts / Boards regarding the anonymisation of notes and document checklist ............................................................................44
2014 Confidential Enquiry into Congenital Diaphragmatic Hernia ..................................44
Anonymisation of Notes Guidance Document ................................................................44
Document checklist.................................................................................................46Appendix 3: Training materials for assessors including instructions for access to the on-line case review system and confidentiality agreements ............48Appendix 4: Assessment documentation used by panels ......................................54

Perinatal Confidential Enquiry 2014 5
Executive Summary
BackgroundThe contract for the Maternal Neonatal and Infant (MNI)CORP was awarded to MBRRACE-UK by the Healthcare Quality Improvement Partnership (HQIP) on 30th May 2012. MBRRACE-UK is a collaboration led from the National Perinatal Epidemiology Unit in Oxford with members from the Universities of Leicester, who lead the perinatal aspects of the work, Liverpool and Birmingham and University College London, as well a general practitioner from Oxford, and Sands, the stillbirth and neonatal death charity.
This report is based on the findings of first perinatal Confidential Enquiry process run by the MBRRACE-UK team and focusses on the care of fetuses and babies with congenital diaphragmatic hernia.
Congenital diaphragmatic herniaCongenital diaphragmatic hernia (CDH) occurs in approximately 1 in 3000–4000 live births, and is associated with a high overall mortality and a high rate of morbidity amongst survivors. Estimates of the number of cases in the UK vary but it is likely that there are between 200 and 300 new cases annually. Of these up to 70% are likely to be diagnosed antenatally as part of routine screening. Up to a third of all UK cases end in either a spontaneous loss during the pregnancy or an elective termination.
The Confidential Enquiry ProcessA stratified random sample of cases was selected by UK country, timing of diagnosis (antenatal or postnatal) and pregnancy outcome (classified as: termination of pregnancy, stillbirth, neonatal death or survival to discharge). Cases were reviewed by confidential enquiry panels using a standardised methodology. Cases for review were identified from an existing epidemiological study of CDH cases born in UK during 2009 and 2010. As there were no national or international standards that related to the whole care pathway for CDH, criteria to judge the quality of care were established by consensus with the help of a Topic Expert Group (TEG). This was a multidisciplinary group comprising experts from the relevant clinical specialties and a patient representative from the charity CDH UK. The group utilised a consensus approach to identify components of good practice in relation to each of the following aspects of the care pathway:
• Diagnosis Screening and Delivery Issues
• Resuscitation
• Early after-care
• Surgery and post-operative care
• Palliative care issues – either antenatal or postnatal where appropriate
• Long-term outcome
Perinatal Confidential Enquiry 20146
Confidential enquiry panels were made up of specialists from all of the relevant disciplines. They considered the care provided to each of the selected cases in relation to the whole care pathway using the following criteria:
• Grade 1: Good care; no improvements identified
• Grade 2: Improvements in care identified which would have made no difference to outcome
• Grade 3: Improvements in care identified which may have made a difference to outcome
The overall grade of the quality of care provision for each case reflected the worst grade awarded to that case for any aspect of the pathway of care. In addition reviewers were asked specifically to flag immediately any cases which met HQIP’s cause for concern criteria in relation to very poor or negligent care.
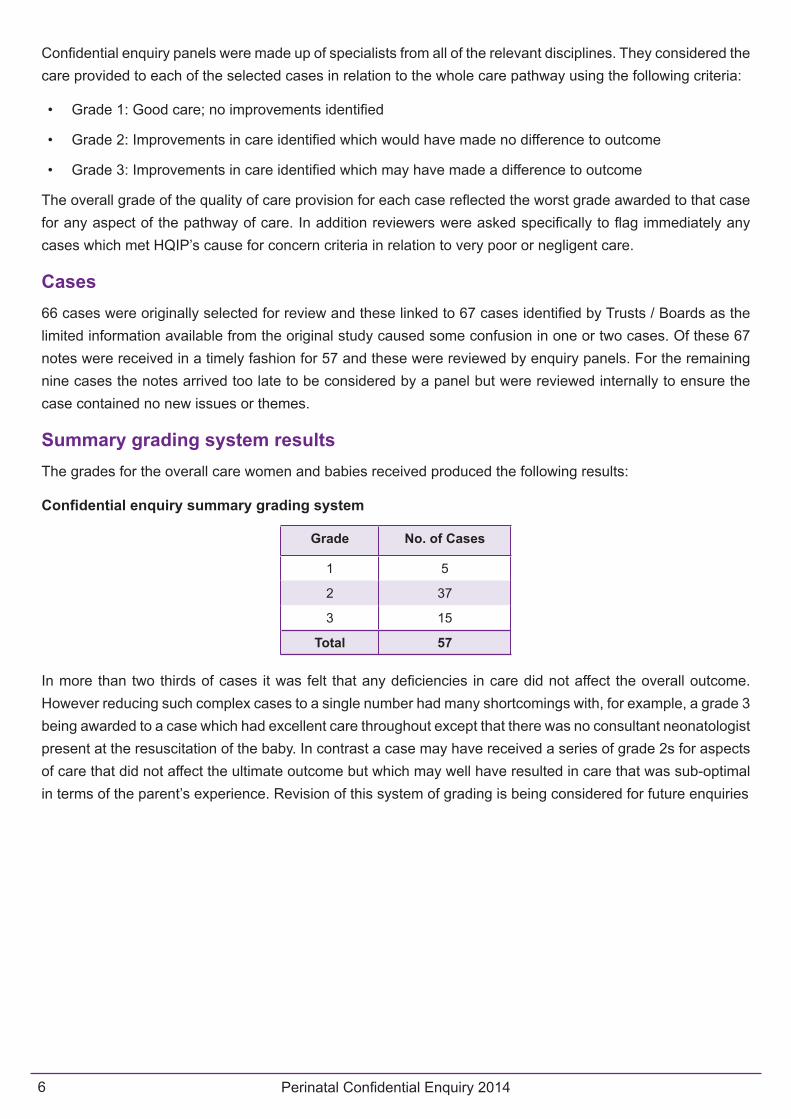
Cases66 cases were originally selected for review and these linked to 67 cases identified by Trusts / Boards as the limited information available from the original study caused some confusion in one or two cases. Of these 67 notes were received in a timely fashion for 57 and these were reviewed by enquiry panels. For the remaining nine cases the notes arrived too late to be considered by a panel but were reviewed internally to ensure the case contained no new issues or themes.
Summary grading system resultsThe grades for the overall care women and babies received produced the following results:
Confidential enquiry summary grading system
Grade No. of Cases
1 5
2 37
3 15
Total 57
In more than two thirds of cases it was felt that any deficiencies in care did not affect the overall outcome. However reducing such complex cases to a single number had many shortcomings with, for example, a grade 3 being awarded to a case which had excellent care throughout except that there was no consultant neonatologist present at the resuscitation of the baby. In contrast a case may have received a series of grade 2s for aspects of care that did not affect the ultimate outcome but which may well have resulted in care that was sub-optimal in terms of the parent’s experience. Revision of this system of grading is being considered for future enquiries

Perinatal Confidential Enquiry 2014 7
Key findings
• In most parts of the UK the services provided for CDH were not patient-centred however alternative models providing a clear care pathway for CDH cases were identified (for example: http://www.nsd.scot.nhs.uk/services/nmcn/cdh.html).
• There was enormous variation across UK in terms of how a women and babies diagnosed with CDH were managed particularly in relation to cases diagnosed antenatally.
• There was a lack of consistency in the information provided antenatally and postnatally regarding prognosis both in terms of content and also how the information was provided.
• Many aspects of obstetric, neonatal and surgical care remain without an adequate evidence base.
• Although access to neonatal intensive care cots / surgical cots was not a common problem in the few cases where there was difficulty it caused great distress.
• Follow up arrangements showed very marked differences between centres.
• Documentation of certain aspects of care was frequently poor.
• Despite the variation in practice most cases received a high level of senior input throughout their course.
Recommendations
Perinatal Confidential Enquiry 20148
Acknowledgements
It is with grateful thanks that the MBRRACE-UK collaboration would like to acknowledge the contribution of the many healthcare professionals and staff from the health service and other organisations who were involved in the notification of cases, the provision of data and the assessment of individual cases. Without the generous contribution of their time and expertise it would not have been possible to produce this report. It is only through this national collaborative effort that it has been possible to conduct this confidential enquiry and to continue the UK tradition of national self-audit to improve care for women, babies and their families in the future.
We would particularly like to thank all MBRRACE-UK Lead Reporters and other staff in Trusts and Health Boards across the UK without whom information about cases would not have been available to enable the enquiry to be conducted.
Members of the MBRRACE-UK collaboration: - Jenny Kurinczuk, Professor of Perinatal
Epidemiology, Director, National Perinatal Epidemiology Unit, Lead MBRRACE-UK, University of Oxford
- Marian Knight, Professor of Maternal and Child Population Health, NIHR Research Professor and Honorary Consultant in Public Health, Maternal Programme Lead for MBBRACE-UK, University of Oxford
- Elizabeth Draper, Professor of Perinatal and Paediatric Epidemiology, Perinatal Programme Co-lead for MBBRACE-UK, University of Leicester
- David Field, Professor of Neonatal Medicine, Perinatal Programme Co-lead for MBBRACE-UK, University of Leicester
- Charlotte Bevan, Senior Research and Prevention Officer, Sands
- Peter Brocklehurst, Professor of Women’s Health, Director of the UCL EGA Institute for Women’s Health
- Ron Gray, Associate Professor, National Perinatal Epidemiology Unit, University of Oxford
- Sara Kenyon, Reader in Evidence Based Maternity Care, University of Birmingham
- Bradley Manktelow, Senior Research Fellow, University of Leicester
- Jim Neilson, Professor of Obstetrics & Gynaecology, University of Liverpool
- Maggie Redshaw, Senior Research Fellow and Social Scientist, National Perinatal Epidemiology Unit, University of Oxford
- Janet Scott, Head of Research and Prevention, Sands
- Judy Shakespeare, Retired General Practitioner, Oxford
- Lucy Smith, Research Fellow, University of Leicester
Members of the Leicester based MBRRACE-UK team: - Pauline Hyman-Taylor, Perinatal Programme
Manager and Research Fellow
- Carol Bacon, Clinical Advisor,
- Alun Evans, Medical Statistician
- Janet Hood, Administrative Support
- Caroline Ellershaw, Administrative Support
- Hollie Burton, Administrative Support
- Helen Jukes Administrative Support
Members of the Oxford based MBRRACE-UK team: - Sarah Lawson, Head of IT and Information
Security, NPEU
- Peter Smith, Programmer and Data Manager
- Carl Marshall, Programmer
- Lucila Canas Bottos, Programmer

Perinatal Confidential Enquiry 2014 9
MBRRACE-UK Congenital Diaphragmatic Hernia Topic Expert Group members: - Pamela Boyd, Neonatal Nurse, Aneurin Bevan
Health Board
- Jonathan Coutts, Consultant Neonatal and Respiratory Paediatrician, NHS Greater Glasgow and Clyde
- David Crabbe, Consultant Paediatric Surgeon, The Leeds Teaching Hospital NHS Trust
- Carl Davis, Consultant Paediatric Surgeon, NHS Greater Glasgow and Clyde
- Alan Fenton, Consultant Neonatologist, The Newcastle upon Tyne Hospitals NHS Foundation Trust
- Jane Herod, Consultant Anaesthetist, Great Ormond Street Hospital for Children NHS Foundation Trust
- David Howe, Consultant in Maternal Fetal Medicine, University Hospital Southampton NHS Foundation Trust
- Alyson Hunter, Consultant in Maternal Fetal Medicine, Belfast Health and Social Care Trust
- Paul Losty, Professor of Paediatric Surgery, Alder Hey Childrens Hospital NHS Foundation Trust, University of Liverpool
- Karen Luyt, Consultant Neonatologist, University Hospitals of Bristol NHS Foundation Trust
- Tim Overton, Consultant in Maternal Fetal Medicine, University Hospitals of Bristol NHS Foundation Trust
- Nadia Permalloo, Midwife, National Quality Assurance Manager, UK National Screening Committee, Public Health England
- Beverley Power, Lay Member, CDH UK
- Coralie Rogers, Midwife, Birmingham Women’s Hospital NHS Foundation Trust
- Ann Tonks, Project Manager, West Midlands Congenital Anomaly Register
- Juliet Wolfe Barry, Consultant Paediatric Anaesthetist, Leeds Teaching Hospitals NHS Trust
MBRRACE-UK congenital diaphragmatic hernia confidential enquiry panel members: - Roshan Adappa, Neonatologist, Cardiff and Vale
University Health Board
- Nargis Ahmad, Anaesthetist, Great Ormond Street Hospital for Children NHSFT
- Joseph Aquilina, Lead Clinician Fetal Medicine CAG, Barts Health NHS Trust
- Sybil Barr, Neonatologist, Cardiff and Vale University Health Board
- Kathryn Beardsall, Neonatologist, Cambridge University Hospitals NHS Foundation Trust
- Ravindra Bhat, Neonatologist, King’s College Hospital NHS Foundation Trust
- Therese Bourne, Midwife, The Whittington Hospital NHS Trust
- Lydia Bowden, Neonatologist, The Pennine Acute Hospitals NHS Trust
- Pamela Boyd, Neonatal Nurse, Aneurin Bevan Health Board
- Sue Calder, Maternity Education Team Leader, Midwife/Supervisor of Midwives, Barking Havering & Redbridge University Hospitals NHS Trust
- Helen Cameron, Obstetrician, City Hospitals Sunderland NHS Foundation Trust
- Philip Chetcuti, Neonatologist, The Leeds Teaching Hospitals NHS Trust
- Simon Clarke, Paediatric Surgeon, Chelsea and Westminster Hospitals NHS Foundation Trust
- Jonathan Coutts, Consultant Neonatal and Respiratory Paediatrician, NHS Greater Glasgow & Clyde
- David Crabbe, Paediatric Surgeon, The Leeds Teaching Hospitals NHS Trust
- Carl Davis, Paediatric Surgeon, NHS Greater Glasgow & Clyde
- Medhat Ezzat, Neonatologist, NHS Grampian
- Alan Fenton, Neonatologist, The Newcastle upon Tyne Hospitals NHS Foundation Trust
- Tracey Glanville, Maternal & Fetal Medicine Specialist, The Leeds Teaching Hospitals NHS Trust

Perinatal Confidential Enquiry 201410
- Sundeep Harigopal, Neonatologist, The Newcastle upon Tyne Hospitals NHS Foundation Trust
- Jane Herod, Anaesthetist, Great Ormond Street Hospital for Children NHS Foundation Trust
- Janet Herrod, Obstetrician, Mid Staffordshire NHS Foundation Trust
- Karen Hoover, Advanced Neonatal Nurse Practitioner, Brighton and Sussex University Hospitals NHS Trust
- David Howe, Maternal & Fetal Medicine Specialist, University Hospital Southampton NHS Foundation Trust
- Bryony Jones, Maternal & Fetal Medicine Specialist, Imperial College NHS Trust
- Andrena Kelly, Neonatal Nurse, NHS Greater Glasgow & Clyde
- Sarah Kenyon, Reader in Evidence Based Medicine, University of Birmingham
- Manjiri Khare, Maternal & Fetal Medicine Specialist, University Hospitals of Leicester NHS Trust
- Morag Liddell, Senior Chargel Nurse, NHS Greater Glasgow & Clyde,
- Paul Losty, Professor of Paediatric Surgery, Alder Hey Childrens Hospital NHS Foundation Trust, University of Liverpool
- Karen Luyt, Neonatologist, University Hospitals of Bristol NHS Foundation Trust
- Nancy Mackeith, Midwife, Barts Health NHS Trust
- Bill Martin, Maternal & Fetal Medicine Specialist, Birmingham Women’s NHS Foundation Trust
- Alan Mathers, Obstetrician, NHS Greater Glasgow & Clyde
- Majella McCullagh, Paediatric Surgeon, Belfast Health & Social Care Trust and South Eastern Health and Social Care Trust
- Penny Mc Parland, Obstetrician, University Hospitals of Leicester NHS Trust
- Anthony Moriarty, Anaesthetist, Birmingham Children’s Hospital NHS Foundation Trust
- Sandeep Motiwale, Paediatric Surgeon, Nottingham University Hospitals NHS Trust
- Padma Munjuluri, Maternal & Fetal Medicine Specialist, Bradford Teaching Hospitals NHS Foundation Trust
- Raji Parasuraman, Maternal & Fetal Medicine Specialist, University Hospital Southampton NHS Foundation Trust
- Andy Petros, Anaesthetist, Great Ormond Street Hospital for Children NHS Foundation Trust
- Cathy Roberts, Obstetrician, Homerton University Hospital NHS Foundation Trust
- Coralie Rogers, Midwife, Birmingham Women’s NHS Foundation Trust
- Stephen Wardle, Neonatologist, Nottingham University Hospitals NHS Trust
- Helen Whapshott, Midwife, Frimley Park Hospital NHS Foundation Trust
- Melissa Whitworth, Obstetrician, Central Manchester and Manchester Children’s University Hospitals NHS Foundation Trust
- Juliet Wolfe-Barry, Anaesthetist, Doncaster and Bassetlaw Hospitals NHS Foundation Trust
Other agencies involved: - Northern Ireland Maternal and Child Health, NSC
Public Health Agency: Heather Reid, Joanne Gluck, Malcolm Buchanan
- UK Obstetric Surveillance System: Melanie Workman, Maureen Frostick, Anne Smith, Patsy Spark
- British Association of Paediatric Surgeons Congenital Anomalies Surveillance System: Melanie Workman, Maureen Frostick, Anne Smith, Patsy Spark
The Maternal, Newborn and Infant Clinical Outcome Review Independent Advisory Group: - Catherine Calderwood (Chair), National Clinical
Director for Maternity and Women’s Health for NHS England and Medical Advisor for Women and Children’s Health for the Scottish Government
- Janice Allister, General Practitioner, Peterborough David Bogod, Consultant Anaesthetist, at Nottingham University Hospitals NHS Trust (member of the IAG until March 2014)

Perinatal Confidential Enquiry 2014 11
- Zoe Boreland, Midwifery and Children’s advisor, Northern Ireland Department of Health, Social Services and Public Safety (member of the IAG from September 2014)
- Cath Broderick, Lay Representative (member of the IAG from October 2013)
- Roch Cantwell, Consultant Psychiatrist, Southern General Hospital, Glasgow (member of the IAG until March 2013)
- Richard Cooke, Professor of Neonatal Medicine, Liverpool Women’s Hospital NHS Foundation Trust (member of the IAG until October 2012)
- Andy Cole, Chief Executive, Bliss (member of the IAG until March 2014)
- Jacqueline Cornish, National Clinical Director Children, Young People and Transition to Adulthood, NHS England (member of the IAG from March 2014)
- Phillip Cox, Consultant Perinatal Pathologist, Birmingham Women’s Hospital
- Polly Ferguson, Welsh Government (member of the IAG until March 2013)
- Roshan Fernando, Consultant Anaesthetist and Honorary Senior Lecturer, University College London Hospitals NHS Foundation Trust (member of the IAG from September 2014)
- Melissa Green, Interim Chief Executive, Bliss (member of the IAG from September 2014)
- David James, Clinical Co-director at the National Collaborating Centre for Women’s and Children’s Health
- Helen Dolk, Professor of Perinatal Epidemiology, Director of the Centre for Maternal, Fetal and Infant Research, Institute for Nursing Research, University of Ulster
- Alan Fenton, Consultant in Neonatal Medicine, Newcastle upon Tyne (member of the IAG from March 2014)
- Bryan Gill, Consultant in Neonatal Medicine and Medical Director, Leeds (member of the IAG until March 2014)
- Mervi Jokinen, Practice and Standards Development Adviser, Royal College of Midwives
- Jim Livingstone, Northern Ireland Department of Health, Social Services and Public Safety (member of the IAG until March 2013)
- Heather Livingston, Northern Ireland Department of Health, Social Services and Public Safety (member of the IAG until March 2014)
- Heather Mellows, Professional Advisor in Obstetrics, Department of Health (England) (member of the IAG until March 2013)
- Liz McDonald, Consultant Perinatal Psychiatrist and Clinical Lead for Perinatal Psychiatry, East London Foundation Trust (member of the IAG from October 2013)
- Edward Morris, Consultant in Obstetrics and Gynaecology, Norfolk & Norwich University Hospital and Honorary Senior Lecturer, University of East Anglia
- Heather Payne, Senior Medical Officer for Maternal and Child Health, Welsh Government
- Nim Subhedar, Consultant Neonatologist, Liverpool Women’s Hospital NHS Foundation Trust (member of the IAG from October 2013)
- Michele Upton, Patient Safety Domain, NHS England (member of the IAG from September 2014)
- Jason Waugh, Consultant and Lead for Obstetric Medicine, Newcastle Upon Tyne.
- David Williams, Consultant Obstetric Physician, The Institute for Women’s Health, University College London Hospital
Healthcare Quality Improvement Partnership: - Jenny Mooney, Business Manager, Clinical
Outcome Review Programmes (to May 2014), Director of Operations, National Clinical Audit and Patient Outcome Programmes
- Lorna Pridmore, Clinical Outcome Review Programmes Facilitator

Perinatal Confidential Enquiry 201412
MBRRACE-UK Third Sector Stakeholder Group and Representatives who Attended Meetings: - Jane Abbott, Bliss
- Beverley Beech, AIMS
- Jenny Chambers, OC Support
- Jane Denton, Multiple Birth Foundation
- Jane Fisher, ARC
- Pauline Hull, electivecesarean.com
- Penny Kerry, Miscarriage Association
- Beckie Lang, Health Campaigns Tommy’s
- Neil Long, Sands
- Sarah McMullen, NCT
- Jane Plumb, Group B Strep Support
- Andrea Priest, Best Beginnings
- Gwynne Rayns, NSPCC
- Jean Simons, Lullaby Trust (formerly FSID)
- Cheryl Titherly, ARC
- Maureen Treadwell, Birth Trauma Association
MBRRACE-UK Royal College and Professional Association Stakeholder Group and Representatives who Attended Meetings: - Carmel Bagness, Royal College of Nursing
- Patrick Cadigan, Royal College of Physicians
- Hilary Cass, Royal College of Paediatrics and Child Health
- Paul Clyburn, Obstetric Anaesthetists Association & Royal College of Anaesthetists
- Sanjeev Deshpande, British Association of Perinatal Medicine
- Denise Evans, Neonatal Nurses Association
- Roshan Fernando, Obstetric Anaesthetists Association & Royal College of Anaesthetists
- Jacque Gerrard, Royal College of Midwives
- Steve Gould, British and Irish Paediatric Pathology Association
- Diane Hulbert, College of Emergency Medicine
- Hannah Knight, Royal College of Obstetricians and Gynaecologists
- Sarah Johnson, Royal College of Obstetricians and Gynaecologists
- Lucy Mackillop, Royal College of Physicians
- Lisa Nandi, British Association of Perinatal Medicine
- Lesley Page, Royal College of Midwives
- David Richmond, Royal College of Obstetricians and Gynaecologists
- Jane Sandall, British Maternal Fetal Medicine Society
- Neil Sebire, Royal College of Pathologists
- Lorraine Tinker, Royal College of Nursing
FundingThe Maternal, Newborn and Infant Clinical Outcome Review programme, delivered by MBRRACE-UK, is commissioned by the Healthcare Quality Improvement Partnership (HQIP) on behalf of NHS England, NHS Wales, the Health and Social care division of the Scottish government, the Northern Ireland Department of Health, Social Services and Public Safety (DHSSPS), the States of Jersey, Guernsey, and the Isle of Man.
Perinatal Confidential Enquiry 2014 13
Main report of the Confidential Enquiry
BackgroundThe programme of national confidential enquiries into perinatal deaths commenced in 1993 with the establishment of the Confidential Enquiry into Stillbirth and Deaths in Infancy (CESDI) to address the relatively high stillbirth and infant mortality rates in the UK through mortality surveillance and confidential enquiries. Re-structuring of commissioning and funding led to organisational changes with the process being run by the Confidential Enquiries into Maternal and Child Health (CEMACH) from 2003 to 2008 and subsequently the Centre for Maternal and Child Enquiries (CMACE) in 2009. During 2009 commissioning of CMACE came under the auspices of the National Patient Safety Agency as one of the three national confidential enquiries along with the National Confidential Enquiry into Patient Outcome and Death (NCEPOD) dealing with surgical and medical cases and the National Confidential Inquiry for Suicides and Homicides by those with a mental illness who have had previous secondary care contact (NCISH).
In 2010 further changes led to the requirement, under European procurement legislation, that all three programmes were open to competitive tender. The programmes were also renamed the Clinical Outcome Review Programmes (CORPs). The contract for the Maternal Neonatal and Infant Clinical Outcome Review Programme (MNI-CORP) was awarded to MBRRACE-UK by the Healthcare Quality Improvement Partnership (HQIP) on 30th
May 2012. MBRRACE-UK is a collaboration led from the National Perinatal Epidemiology Unit at the University of Oxford with members from the Universities of Leicester, who lead the perinatal aspects of the work, Liverpool and Birmingham and University College London, as well a general practitioner from Oxford, and Sands, the stillbirth and neonatal death charity. Of note under the new
arrangements for the MNI-CORP the confidential enquiries have been extended to include cases of serious morbidity as well as deaths.
This report is based on the findings of the first perinatal Confidential Enquiry run by the MBRRACE-UK team and focuses on the care of fetuses and babies with congenital diaphragmatic hernia.
Topic ChoiceHQIP have developed a standard process for choosing topics for confidential enquiry to be run by the Clinical Outcome Review Programmes and this is normally completed in the year prior to any enquiry taking place. However given the time needed to complete the organisational change following the award of the MNI-CORP to MBRRACE-UK there was inadequate time to carry out this process for this first enquiry. In addition, there was no up to date database from which cases could be sampled. Therefore, in order to complete the enquiry in a timely manner it was necessary to consider topics for which an appropriate sampling frame of cases was already available.
The British Association of Paediatric Surgeons Congenital Anomalies Surveillance System (BAPS-CASS), in association with the United Kingdom Obstetric Surveillance System (UKOSS) carried out a UK wide epidemiological study of cases of congenital diaphragmatic hernia (CDH) during 2009 and 2010. Although the information available with which to identify these cases was very limited, as data are collected anonymously through these systems, this study offered a starting point for the sampling of cases for the enquiry process. More importantly CDH has a high rate of both mortality and morbidity and its management involves a whole range of clinical staff including midwives, obstetricians, radiologists, neonatologists, neonatal nurses, paediatric intensive care doctors and nurses, paediatric surgeons, anaesthetists and pathologists. Furthermore CDH

Perinatal Confidential Enquiry 201414
had not been the subject of a confidential enquiry by any of the predecessor organisations. This option was presented to the Independent Advisory Group for the MNI-CORP (http://www.hqip.org.uk/independent-advisory-group-for-the-corp-maternal-infant-perinatal-programme/) who supported the choice.
Congenital Diaphragmatic Hernia (CDH)Congenital diaphragmatic hernia (CDH) occurs in approximately 1 in 3000–4000 live births, with a high overall mortality despite continuing advances in prenatal diagnosis and postnatal management. Estimates of the number of new cases occurring each year in the UK vary and are particularly affected by whether an antenatal or postnatal population or both is used for the estimate. Based on published data it is likely that there are between 200 and 300 cases in the UK each year (1,2) Of these up to 70% are likely to be diagnosed antenatally as part of routine screening. Up to a third of all UK cases end in either a spontaneous loss during the pregnancy or an elective termination (1,2). Mortality prior to surgery is substantial and deaths following surgery also occur. CDH survivors experience significant pulmonary, gastrointestinal, cardiac, and neurologic morbidities. A significant number show evidence of neurocognitive delay (NCD), hearing impairment, and behavioural disorders at follow-up (3).
CDH results from a failure of normal development of the diaphragm during the first trimester and is categorized into three broad types of defect:
1. Complete absence of the diaphragm, which is rare, but the most severe with the worst prognosis.
2. Failure of normal development of the diaphragm anteriorly, seen in only ~2% of cases.
3. Failure of the diaphragm to close posteriorly - the most common type of defect - 85% of which are left sided, 10% right sided and 5% bilateral.
Eventration of the diaphragm is often considered as part of the range of CDH pathology. However this results from a failure of muscle development in the primitive diaphragm and is not a true hernia: as such these cases were not considered in this confidential enquiry.
CDH can occur as part of a syndrome (e.g. Fryn’s syndrome) or in association with a chromosomal anomaly (e.g. Trisomy 13 or 18) and in these circumstances the reported overall prognosis is worse. In terms of the effect on the developing cardiorespiratory system, compression of both lungs during pregnancy results in hypoplasia especially in the lung on the affected side. In the most severe cases, cardiac function can also be compromised in utero. After delivery gaseous distension of gut in the chest can result in further cardiorespiratory compromise. Pulmonary hypoplasia and poor oxygenation following delivery commonly result in a failure of normal adaptation to extra uterine life with persistent pulmonary hypertension of the newborn. By contrast in more mildly affected cases cardiopulmonary development and function may be sufficient to enable normal extra uterine adaptation with presentation at a later stage.
Within the UK delivery of these babies can occur in any of the estimated more than 300 plus delivery units (4) and, when not diagnosed in the antenatal period, in babies born at home. However for cases with an antenatal diagnosis delivery normally occurs in a hospital setting that has neonatal intensive care facilities on site. Surgery can occur in one of the 27 paediatric surgical centres, sites most of which are co-located with the delivery unit and neonatal intensive care service.
The Confidential Enquiry ProcessA confidential enquiry is a process of systematic, multi-disciplinary, anonymous case review (5) and for the purpose of the CDH enquiry focussed on the cases identified by the BAPS-CASS / UKOSS study of affected births in 2009 and 2010. Given
Perinatal Confidential Enquiry 2014 15
resource constraints and the qualitative nature of the enquiry process a sample of between 65 and 70 cases was felt to be of adequate size to ensure theme saturation. A stratified random sample, by UK country, timing of diagnosis (antenatal or postnatal) and pregnancy outcome (classified as: termination of pregnancy, stillbirth, neonatal death or survival to discharge) was selected in autumn 2013. In the final sample of 67 cases (based on the information collected by the BAPS-CASS/UKOSS study) 46 were male and 21 female, 47/67 were antenatally diagnosed and pregnancy outcomes comprised: 6 terminations of pregnancy, 2 stillbirths, 17 neonatal deaths and 42 surviving children.
The aims of the confidential enquiry were:
1. To assess the quality of care provision across the UK for pregnancies affected by CDH.
2. To assess the quality of care provision across the UK for babies presenting antenatally or postnatally with a diagnosis of CDH.
3. To identify aspects of sub-optimal care and excellent practice.
4. To review how closely the care provided across the UK mapped to consensus views of best practice (in 2009/2010) identified by the Topic Expert Group (see below).
5. To identify any recurring themes for potential improvement in relation to the care provided.
Confidential enquiries focus on care quality with a particular emphasis on aspects which were suboptimal in order to inform future practice and improvements in care. For the MNI-CORP we adopted the following criteria to summarise the assessment of the quality of care provided for individual cases:
◦ Grade 1: Good care; no improvements identified
◦ Grade 2: Improvements in care* identified which would have made no difference to outcome
◦ Grade 3: Improvements in care* identified which may have made a difference to outcome
(*Improvements in care should be interpreted to include adherence to guidelines, where these exist and have not been followed, as well as other improvements which would normally be considered part of good care, where no formal guidelines exist.)
• In addition reviewers were asked specifically to flag immediately any cases which met HQIP’s cause for concern criteria. The HQIP protocol defines “Identified Causes for Concern” as follows: Death (child or adult) attributable to abuse or neglect, in any setting, but no indication of cross agency involvement (i.e. no mention of safeguarding, social services, police or LSCB).
• Staff member displaying:
◦ Abusive behaviour (including allegations of sexual assault)
◦ Serious professional misconduct
◦ Dangerous lack of competency
But not clear if incident has been reported to senior staff
• Standards in care that indicate a dysfunctional or dangerous department or organisation, or grossly inadequate service provision.
Topic Expert groupA Topic Expert Group (TEG) was convened to steer the enquiry. This was a multidisciplinary group comprising experts from the relevant clinical specialties and a patient representative from the charity CDH UK (see Appendix 1). A review of the literature failed to identify a robust evidence base or established care pathway in relation to the

Perinatal Confidential Enquiry 201416
management of CDH. Therefore, the group utilised a consensus approach to identify aspects of good practice in relation to each of the following aspects of the care pathway:
• Diagnosis Screening and Delivery Issues
• Resuscitation
• Early after-care
• Surgery and post-operative care
• Palliative care issues – either antenatal or postnatal where appropriate
• Long-term outcome
The document produced is included in Appendix 1 and formed the framework against which cases were assessed.
Case note acquisitionData on cases included in the BAPS-CASS/UKOSS study contained no personal identifiers which complicated the process of case identification. The information available to identify cases was limited to the hospital providing care, the name of the person reporting the case and the date of operation or death. With changes in personnel in hospitals this led to significant problems in identifying the correct case in some hospitals in order to acquire a copy of the notes for the enquiry process. Initial points of contact were the person who notified the case to the BAPS-CASS /UKOSS studies (many of whom had left the hospital by the time of this contact) and the local MBRRACE-UK lead. Whilst some teams responded promptly others were reluctant to collaborate. In these latter cases we subsequently approached the local quality managers and this significantly improved the compliance of Trusts/Health Boards with our request. As a last resort, in a small number of cases, we approached the Chief Executive to facilitate the process.
Once cases were identified our initial request to the local teams was for relevant sections of the notes to be copied, anonymised and then supplied to the MBRRACE-UK office in Leicester. Clear instructions were provided on how to complete this process as
per our standard protocol (5,6) –see also Appendix 2. However the lengthy nature of many of the notes and the time consuming nature of anonymisation meant that many Trusts / Health Boards were reluctant to take on this task and with limited prior experience those who did attempt the anonymisation process found it very difficult. Permission was therefore sought and obtained from the Confidentiality Advisory Group for copies of the records to be sent prior to anonymisation which was then carried out in the secure Leicester MBRRACE-UK office following prescribed information governance guidelines. Cases were anonymised by redaction of the case and family identifiers, hospital and clinician names. The type and grade of staff that made a particular entry was retained for enquiry purposes. Clearly the notes of the cases selected varied greatly in complexity as they included children who survived after a prolonged hospital stay and other cases where, after diagnosis, the family chose a termination. Once notes were received and reviewed it was possible to establish in which cases the mother and or child had been cared for in an additional hospital(s) which then triggered a request for these extra records.
Northern Ireland has different data protection arrangements from the rest of the UK and as such there is no mechanism for the export out of Northern Ireland of identifiable data without consent. As a consequence the Northern Ireland Maternal and Child Health (NIMACH) office within the Health and Social Care Public Health Agency were responsible for obtaining the records of identified cases and individual parental consent.
All records were reviewed in Leicester prior to assessment by panel members. This allowed notes to be prepared in a logical order, completeness to be checked and any documentation not needed as part of the review process to be removed.
ReviewersThe care pathway for CDH involves a large multidisciplinary team of health professionals, especially for those babies who survive, including midwives, obstetricians, fetal medicine specialists,

Perinatal Confidential Enquiry 2014 17
neonatologists, paediatric intensivists, neonatal nurses, paediatric surgeons, and paediatric anaesthetists. Representatives from all these specialties were needed for the confidential enquiry panels. Approaches were made to the relevant Colleges and specialty groups with requests that they advertise for panel assessors amongst their members. Those who expressed interest were asked to provide a brief summary of their experience to ensure that they had the relevant background and were in good standing with relevant College/professional organisation.
All those who were accepted as potential assessors were asked to join a training session in the form of a virtual meeting with a video demonstration of the secure on-line viewing system through which notes could be accessed and an explanation of the review process. This session was accessed remotely and lasted approximately one hour (See Appendix 3).
Case review panel meetingsThe enquiry process commenced once the notes for an individual case had been checked and confirmed as complete. The relevant records were then uploaded and made available for viewing via the MBRRACE-UK secure web-based high compliance system. Panel members logged in to the system using a secure username and password to access the specific case notes they had been allocated and were asked to review each case ahead of the panel meeting.
Panel meetings were planned as face-to-face discussions lasting up to six hours. They were all held at a venue in the Midlands to provide ease of access to members from around the UK. Details of the meeting and access to the cases were provided 3-4 weeks in advance in order that panel members were able to review and evaluate the allocated cases, up to 9 cases per panel, prior to the meeting.
In total 8 panels were held. To ensure standardisation of the process each panel was chaired by either David Field or Elizabeth Draper, members of the MBRRACE-UK team. The composition of the panel
otherwise reflected the nature of the cases to be reviewed (e.g. for cases ending in termination no paediatric surgeon was needed). Each case was discussed in turn commencing with an overview by a panel member who had been allocated as lead for the case in advance. This was followed by a general discussion where aspects of poor care or particularly good care were highlighted. In addition recurring themes were also noted. At the end of this discussion the Chair and a member of the MBRRACE-UK team both completed an assessment form based on the consensus reached by the panel. The individual assessment forms completed by each panel member were also collected.
We attempted to ensure that cases were always reviewed by panel members who had no personal involvement in the case. Unfortunately due to the time delay between the cases and the panel reviews a number of staff had changed posts and therefore this was not achieved in a small number of cases. Panel members were asked to notify the chair when this occurred and similarly if they recognised the provenance of a case or the identity of an individual involved in the care despite the anonymising process.
Findings from panel reviews
Details of cases reviewedA total of 66 potential cases were originally identified for confidential review from the BAPS-CASS / UKOSS data base. However the limited information available about the identification of each case generated 67 potential cases all of whom were considered for inclusion in the enquiry process cases.
Requests for notes began in September 2013. In order to meet HQIP’s reporting timetable it was necessary to complete the enquiry process by the end of July 2014. Notes relating to the whole care pathway were identified and retrieved for 54 cases and for part of the care pathway for a further 3 and these 57 were reviewed by panels.

Perinatal Confidential Enquiry 201418
Of the remaining cases selected as part of the sample: in 1 case consent was not provided (this was a necessary step just in Northern Ireland), records for 1 case, from Kings College Hospital, were not provided as they appeared to have been lost and in 8 cases the records were received too late for the enquiry process i.e. they arrived during July 2014. These ’late’ cases were reviewed by the in-house clinical team and appeared to provide no issues or themes that had not already been highlighted. As a result they were not subject to panel review and did not contribute to the numbers of specific events referred to later in the report.
Although cases were sampled on the basis of the various diagnostic categories reported to the BAPS-CASS / UKOSS studies (often based on an antenatal diagnosis) some of these proved to be incorrect when the notes were reviewed by the panels. This difference might have been because of difficulties in identifying the correct case in the hospital that originally referred the case or simply because updated information about the diagnosis may not have been supplied to the anomalies register. The final combination of cases that were reviewed at a panel (from either full or partial records) was as follows:
• Antenatally diagnosed and died either as a termination of pregnancy or a stillbirth, n=7.
• Antenatally diagnosed and survived, n=23. This included:
◦ two sets of twins where one twin was diagnosed with CDH and survived and the other twin was unaffected;
◦ two cases where the initial (antenatal) diagnosis of CDH proved to be incorrect.
• Antenatally diagnosed and born alive but died prior to their initial discharge from hospital, n=15.
• Postnatally diagnosed cases all of whom survived, n=12.
It is important to note that termination of pregnancy for fetal anomaly is not offered in Northern Ireland.
Panel findings in relation to careThe panel findings are presented based on the various aspects of care highlighted as important by the topic expert group at the start of the confidential enquiry process. The selected enquiry panel cases, chosen to encompass all types of presentation, were not necessarily representative of the total CDH population in the UK and hence the findings focus on themes rather than proportions.
Screening and Diagnosis Issues
The Topic Expert Group (TEG) identified the following areas of practice which they felt panel members should consider when reviewing cases:
a) Was screening carried out at the appropriate time?
b) Did the mother of the child decline screening, or book into antenatal care late in the pregnancy? Was referral appropriate and timely (taking into account geographical location)?
c) Was counselling documented as regards content and with the appropriate multidisciplinary team?
d) Was there evidence that the counselling was provided in a way to meet the mother’s / family’s needs including, if appropriate, access to a multidisciplinary team?
e) Was sufficient time given for the decision-making process?
These issues were assessed for the 45 cases where antenatal diagnosis of CHD was made. In all cases where antenatal detection did not occur, screening had taken place.
Although, in general, there was compliance with the recommendations of the Fetal Anomaly Screening Programme (FASP) and the TEG’s recommendations regarding good practice in relation to this aspect of the pathway, there was significant variation. The TEG recognised that the FASP guidelines of screening between 18+0 and 20+6 were released in 2010 i.e. part way through the period from which cases were selected but nonetheless this was felt to represent a good standard against which to compare

Perinatal Confidential Enquiry 2014 19
what actually took place. In fact the initial anomaly screening scan occurred outside the recommended window in just 2 cases. Delayed scans had potentially important implications for parents in terms of decision making regarding whether to terminate the pregnancy. Although it might seem that CDH is a sufficiently severe anomaly to qualify for late termination after the 24 week limit specified in the abortion legislation, this was not the universal view of the obstetricians / fetal medicine specialists who took part in the panels.
Documentation around the counselling process was often not detailed and hence it was difficult for panels to accurately determine the information given to parents. Whilst some women were offered a confirmatory scan, often in a different hospital, very quickly after an initial abnormality was suspected this was not always the case with, at worst, confirmation of diagnosis made at 31 weeks gestation i.e. several weeks after the provisional diagnosis. It was clear that some of the variation observed was the result of where the woman lived and the accessibility of a specialist / specialist centre capable of carrying out the confirmatory scan. However once a firm diagnosis was made it became apparent that the counselling offered in different centres varied markedly. In some settings couples had the opportunity to meet all of the members of the multidisciplinary team at the same appointment. In other units, this opportunity was much more piecemeal with each specialist being seen on a different occasion and sometimes in different locations. Panel members expressed differing views on the acceptability of this variation in practice. They considered the inconvenience and financial implications of multiple visits for parents versus the ability to have additional time to assimilate information. However it was clear that the counselling offered reflected the local policy rather than an attempt to meet individual needs. We came across no examples of the use of telemedicine where geography made repeated visits to the referral centre particularly difficult.
There was significant variation in terms of the prognostic information provided and there appears to have been little appreciation, by some of those providing counselling, of the risk of long term neurodevelopmental problems in these children. In a number of cases the panel felt that the counselling gave an over optimistic view of the child’s likely course and prognosis. In three cases diagnosed antenatally, neonatal counselling was provided immediately prior to delivery. Most counselling appeared to have been delivered by a consultant but occasionally it was delivered by a trainee.
The guidance document produced by the TEG contained one aspect of practice where no consensus could be reached regarding best practice and this related to the use of antenatal measures to predict outcome. Until recently these have been based on ultrasound measurements of, for example, lung to head ratio and whether the liver had moved into the chest. There was disagreement between TEG members about the extent to which these measures were meaningful and reproducible outside specific centres. More recently it has been suggested that fetal MRI scanning might provide greater precision. It became clear at the panel meetings that measures of severity were used infrequently - in only 4 out of the 23 cases diagnosed antenatally who survived. However, in these four cases it formed a major feature of the counselling as recorded in the notes.
There were two cases where the antenatal diagnosis of CDH made on ultrasound was wrong (cystic adenomatoid malformation; major hiatus hernia – a late diagnosis).
In one further case a diagnosis on ultrasound of absent ductus venosus was diagnosed as a Morgagni (anterior) CDH at 17 days of postnatal age. In this case it was felt that fetal MRI may well have allowed a precise diagnosis at a much earlier point. Similarly MRI might have prevented the offer of a termination (that was not accepted) in an antenatally diagnosed CDH that proved ultimately to be a benign cystic lesion.

Perinatal Confidential Enquiry 201420
Delivery issues
Issues relating to delivery identified by the topic expert group were:
a) Where was the baby delivered?
b) Was the baby born in the planned place of delivery?
c) At what gestation was the baby delivered?
d) Was it a planned delivery?
e) Was labour induced?
f) Who was responsible for the baby’s care and treatment?
The pattern of care that emerged in terms of delivery for the babies in which an antenatal diagnosis had occurred again reflected a lack of agreement amongst the wider clinical community in terms of what constituted best practice and there was
substantial variation. Whilst there was a clear, and appropriate, reluctance to intervene in a way that led to a premature birth and only four cases were delivered by planned caesarean section (although here there were multiple indications and not just the presence of a CDH), planning around delivery showed no consistent approach. (See Tables 1 and 2)
There was no obvious or measurable effect on the babies’ condition at birth as a result of this variation but it did mean that the timing of delivery could not be planned. Of the antenatally detected cases in which the pregnancy continued 14/38 (approximately a third) delivered between 20.00hrs and 08.00hrs (i.e. outside the routine attendance hours for a neonatal consultant in most Trusts / Health Boards and the evening handover round) see Table 3: Delivery times for antenatally detected cases. None of the deliveries occurred on Saturday or Sunday.

Perinatal Confidential Enquiry 2014 21
Tabl
e 1:
Ant
enat
ally
dia
gnos
ed C
DH
cas
es w
ho s
urvi
ved
– de
liver
y an
d ne
onat
al m
anag
emen
t sum
mar
y
No
Del
iver
y Pl
anD
eliv
ery
Out
com
eP
Bic
arb
Surf
acta
ntH
FOV
NO
Dop
Dob
Adr
enal
ine
Hco
rtEC
HO
ECM
OC
omm
ents
1IO
L 38
/40
twin
Twin
1 u
naffe
cted
SV
D
Twin
2 C
DH
EM
CS
√√
√√
√√
2IO
L39/
40E
MC
S√
√√
√√
√√
3IO
L38/
40S
VD
√√
√
4IO
L39/
40Ve
ntou
se√
√√
RS
V IM
M
5IO
LS
VD
33/4
0√
√√
√
6IO
LE
MC
S30
/40
FE
TO E
XIT
√√
√R
SV
IMM
7E
lect
ive
CS
SV
D37
/40
√√
√√
√R
SV
IMM
8IO
LS
VD
39/4
0√
√√
√√
√√
RS
V IM
M
9IO
LS
VD
√√
√
√
√√
10E
lect
ive
CS
Ele
ctiv
e C
S 3
8/40
√√
11U
ncle
arE
MC
S39
/40
√ √
√√
√
12IO
LS
VD
√
√√
√√
13IO
LE
MC
S P
ET
32/4
0√
√√
√√
√√
14IO
LS
VD
39/
40√
No
CD
H o
n x-
ray
Ext
ubat
ed√
Cys
tic lu
mp
i.e. n
ot C
DH
15C
DH
@36
/40
SV
D 3
7/40
√H
iatu
s H
erni
a i.e
. not
CD
H
16E
lect
ive
CS
Ele
ctiv
e C
S 3
5/40
PE
T√
√√
√√
√√
-
17IO
LE
MC
S 3
9/40
√√
√
18IO
LS
VD
√
√
19IO
LS
VD
√
√√
√√
√
20E
lect
ive
CS
39/
40E
lect
ive
CS
39/
40√
√√
√
21IO
LS
VD
39/
40√
√√
√√
22E
lect
ive
CS
tw
ins
EM
CS
34/
40 (a
bnor
mal
D
oppl
er’s
)√
√√
√√
√√
√
23IO
LS
VD
√√
Key
IOL
= in
duct
ion
of la
bour
; CS
= ca
esar
ean
sect
ion;
SV
D =
Spo
ntan
eous
ver
tex
deliv
ery;
EM
CS
= E
mer
genc
y ca
esar
ean
sect
ion;
P =
Par
alys
ed;
Bic
arb
= b
icar
bona
te;
HFO
V =
ven
tilat
ion
usin
g os
cilla
tion;
NO
= n
itric
oxi
de; D
op =
Dop
amin
e; D
ob =
Dob
utam
ine;
H
cort
= H
ydro
corti
sone
; E
CH
O =
Pre
-ope
rativ
e he
art s
can;
E
CM
O =
ext
ra
corp
orea
l mem
bran
e ox
ygen
atio
n.
RS
V IM
M –
Imm
unis
atio
n ag
ains
t Res
pira
tory
Syn
cytia
l Viru
s; F
ETO
– F
etos
copi
c Tr
ache
al O
cclu
sion
; P
ET
– P
re e
clam
psia
toxa
emia
Perinatal Confidential Enquiry 201422
Tabl
e 2:
Ant
enat
ally
di
agno
sed
CD
H c
ases
who
die
d –
deliv
ery
and
neon
atal
man
agem
ent s
umm
ary
No
Del
iver
y Pl
anD
eliv
ery
Out
com
eP
BIc
arb
Surf
acta
ntH
FVO
NO
Dop
Dob
Adr
enal
ine
Cor
tison
eEC
HO
ECM
OD
ied
& C
omm
ents
1IO
LS
VD
T√
√√
√√
√√
√ la
rge
PD
AC
onsi
dere
d bu
t fel
t to
be
too
unst
able
2 da
ys
2IO
LS
VD
T+6
√√
√√
√√
√√
Con
side
red
but f
elt
to b
e to
o un
stab
le≤2
4hrs
3P
ET
32/4
0E
MC
S√
√√
√√
√√
√4
days
Tris
omy
13 +
Im
perfo
rate
anu
s
4IO
LS
VD
37/4
0√
√√
√√
17 h
rs
5IO
L S
VD
38/4
0√
√√
√√
pros
tinC
onsi
dere
d bu
t fel
t to
be
too
unst
able
19hr
s
6IO
L /P
ET
EM
CS
30/
40
√√
√√
√√
ò
24hr
s
7IO
LFo
rcep
s 38
/40
√√
√√
ò
24hr
s
8IO
LS
VD
39/
40√
√√
√7
days
Hyp
opla
stic
L H
eart
9IO
L S
VD
37/4
0√
√√
48H
rs H
ypop
last
ic L
Hea
rt
10IO
LS
VD
term
√√
√√
≤24h
rs
11IO
L/P
ET
EM
CS
34/4
0√
√√
√√
≤24h
rs
12IO
LE
MC
S T
erm
√√
√√
√√
√C
DH
suc
cess
fully
repa
ired
Die
d ag
e 31
day
s
13IO
LS
VD
35/4
0√
√√
ò2
4hrs
FE
TO
14E
lect
ive
CS
Ele
ctiv
e C
S38
/40
√√
√√
√48
hrs
15IO
L S
VD
Ter
m√
√√
Not
m
entio
ned
Acc
epte
d &
tra
nsfe
rred
but
not
su
itabl
e on
arr
ival
in
EC
MO
cen
tre
Hea
d s
can
IVH
++
fixed
dila
ted
pupi
ls≤2
4hrs
of
age
Key
IOL
= in
duct
ion
of la
bour
; CS
= ca
esar
ean
sect
ion;
SV
D =
Spo
ntan
eous
ver
tex
deliv
ery;
EM
CS
= E
mer
genc
y ca
esar
ean
sect
ion;
P =
Par
alys
ed;
Bic
arb
= b
icar
bona
te;
HFO
V =
ven
tilat
ion
usin
g os
cilla
tion;
NO
= n
itric
oxi
de; D
op =
Dop
amin
e; D
ob =
Dob
utam
ine;
H
cort
= H
ydro
corti
sone
; E
CH
O =
Pre
-ope
rativ
e he
art s
can;
E
CM
O =
ext
ra
corp
orea
l mem
bran
e ox
ygen
atio
n.;
IV
H =
intra
vent
ricul
ar h
aem
orrh
age

Perinatal Confidential Enquiry 2014 23
Table 3: Delivery times for antenatally detected casesTime of day - Arrows show the 08.00hr to 20.00hr optimal*
Delivery time (hr)
Cas
e nu
mbe
r
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 241 *
2 3 * 4 * 5 6 * 7 8 * 9 *
10 * 11 12 * 13 * 14 15 * 16 * 17 * 18 * 19 * 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38
39 40
Legend:-
BLACK = Surviving children
GREEN = Neonatal deaths
BLUE = Stillbirths
*Optimal refers to the TEG’s view of the timing of delivery most likely to relate to the immediate availability of senior staff and facilities

Perinatal Confidential Enquiry 201424
Panel members identified various factors that impacted on the actual timing of delivery such as the day and time chosen for induction, specialist staff availability, neonatal cots availability and (where surgery took place on a separate site) surgical cot availability. A clear example of the potential impact of the nature and timing of delivery in relation to any prior planning can be seen in Vignette 1.
Vignette 1
A young primigravida was found to have a fetus with an abnormality in the chest on her anomaly screening ultrasound. Two MRI scans were performed subsequently to confirm the diagnosis of CDH and a third was planned. Detailed discussions regarding delivery options took place and a plan was made regarding induction near term. However whilst an inpatient at 35 weeks of gestation, as a result of hypertension, the woman went into spontaneous labour on the antenatal ward and arrived on labour ward just in time for the delivery. The baby subsequently did well.
Resuscitation Issues
Issues highlighted by the topic expert group for review in relation to resuscitation were:
a) Who was involved in the emergency care of the baby?
b) Were they appropriately qualified/experienced?
c) What evidence is available to demonstrate what attempts were made to avoid lung injury?
d) Was there adequate communication with parents regarding the baby’s condition?
In the majority of cases resuscitation was well managed and led by a consultant. However in those cases that delivered outside of the normal attendance hours for a consultant, the team attending the delivery was generally less comprehensive in its make up than for deliveries during the working day. Where a consultant was at home at the time of an ’out of hours’ delivery, in most cases they attended in person within 30 minutes. There were seven occasions when the panel considered that
those present for the resuscitation of the baby were insufficiently experienced and the composition of the team was felt to be inadequate.
In terms of the approach to resuscitation in the absence of clear evidence to support particular measures it was difficult to make definitive judgements about the competence and/or practice of staff during resuscitation. Of the antenatally detected cases thought to be affected by CDH all, except one, were electively paralysed and ventilated at birth as part of resuscitation. These measures are designed to both gain control of ventilation and prevent gaseous distension of the bowel. Although widely used, this practice is not universally accepted. (The one case that was not treated in this way proved not to have CDH). An approach to resuscitation that aimed to provide “lung protection” was generally not apparent from the records although it is possible that the teams felt that such measures were inherent in their approach. Instead the focus appeared to be one of achieving adequate stabilisation of the baby.
In 25 cases the panel considered that some aspect of the overall resuscitation was inadequate. However in nine cases this related to some aspect of inadequate documentation and in seven cases to the absence of a consultant neonatologist at the time of delivery. In general there was good communication with the family around the time of the child’s delivery and initial assessment and stabilisation. This included those cases where the baby clearly did not respond to resuscitation.
Early After-Care (i.e. 1-48 hours post-delivery) Issues
1) Antenatally detected cases born alive
Issues highlighted by the topic expert group for review in relation to early after-care were:
a) What measures were taken to assess/monitor, the severity of the condition?
b) Were the care options discussed with the baby’s parents? By whom?

Perinatal Confidential Enquiry 2014 25
This proved to be a difficult aspect of care for the panels to assess both because of the lack of relevant evidence to guide practice and the great diversity that emerged in the approaches taken by the various clinical teams. However the care was certainly consultant-led in the majority of cases and consultant delivered in many.
There was commonality of view around the need to ensure an adequate systemic blood pressure although the approach to doing this varied markedly. In most cases any intervention was informed by an early cardiac scan which was documented in all cases, except one, who achieved initial stabilisation. Many units used inotropic drugs in the form of Dopamine and Dobutamine early in the course of the baby’s treatment , while in a small number of centres other inotropes were used, such as Milrinone. Fluid boluses were used commonly and their use to support blood pressure seemed to outweigh any concerns about ’fluid overload’. There
was no sense of a standard regime, again almost certainly a reflection of an absence of evidence to guide management.
Ventilator management showed similar marked variation both in terms of the type of ventilator employed (high frequency vs time cycled pressure limited) and also the blood gas targets. However given the relatively small number of cases reviewed overall the number where a ’lung protection strategy’ could be employed as opposed to cases where the priority was to find a ventilator strategy that would keep the baby alive meant that it was generally difficult to judge the clinicians preferred aims in terms of their ventilation strategy. Four of the cases reviewed were considered to have received sub-optimal care related to the ventilation techniques adopted and the lack of an effective lung protective strategy.
Attempts to manage the pulmonary hypertension that commonly complicates cases of CDH showed the most variation of all. Examples of the measures used are included in Table 4.
Table 4: Examples of therapeutic inconsistency
Therapeutic measure Evidence and panel comments
Use of nitric oxide to produce pulmonary arteriolar vasodilatation.
Some evidence suggests nitric oxide may be harmful in CDH. However the evidence from trials is very limited and evidence from
basic science regarding how nitric oxide works does support its use. Nitric oxide use occurred frequently in the cases reviewed.
Use of sodium bicarbonate to control acidosis
Acidosis tends to encourage pulmonary arteriolar vasoconstriction and hence there is some physiological evidence to support the principle
of trying to reduce any on-going acidosis. However the use of sodium bicarbonate has no effect on any underlying problems producing
acidosis and its use normally results in further accumulation of carbon dioxide. Use of sodium bicarbonate was supported by some panel
members and rejected by others.
The use of Prostin (prostaglandin) to maintain the patency of the ductus
arteriosus to prevent, in the presence of severe pulmonary hypertension,
overload of the right ventricle.
Physiologically sound and used in some major centres / reported in case series but not supported by strong clinical evidence. Used in two of the
cases reviewed.
Changes to ventilation
In a high proportion of cases, in the face of deterioration, different modes of ventilation were tried. Evidence of likely benefit is lacking
and there was no coherent approach in terms of the nature and order of the ventilator modes employed.
Perinatal Confidential Enquiry 201426
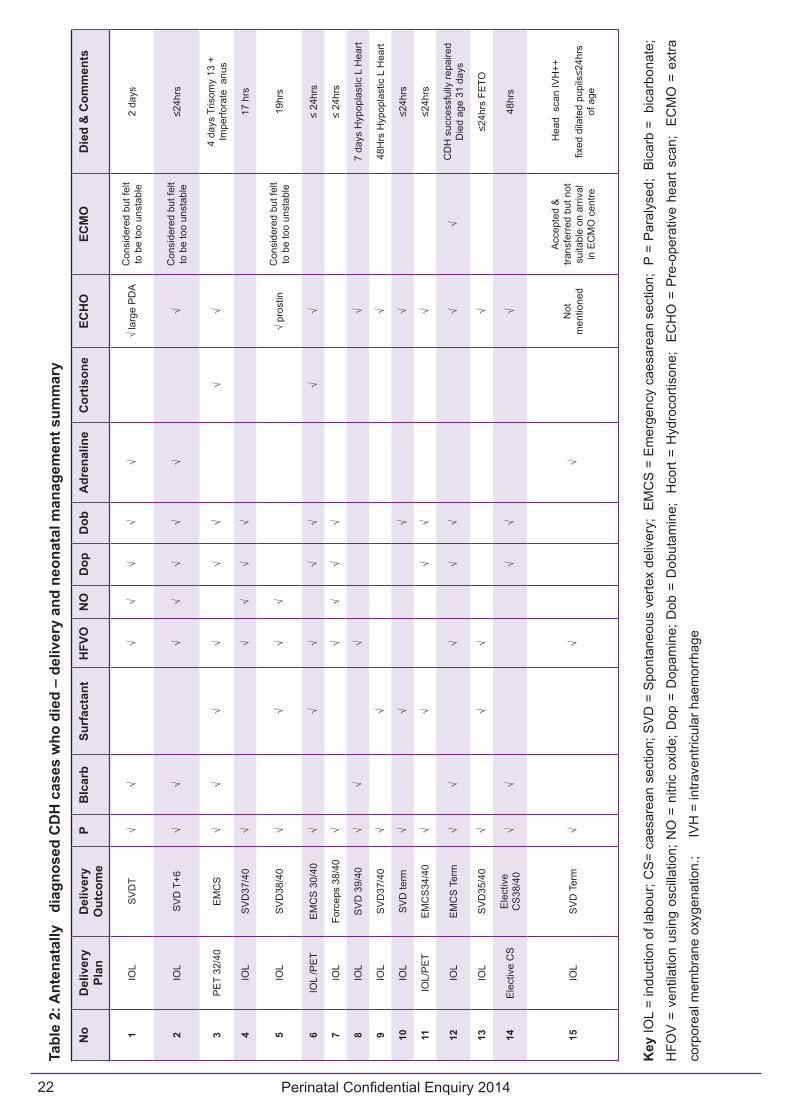
Table 1 and table 2 illustrate more generally the variation in practice for the treatment of babies with CDH. Each row of the tables denotes a case reviewed during the course of the enquiry. The use of some of the more common interventions is then shown in a series of columns. Although this demonstrates variation in the treatments used there was in addition, variation in terms of under what circumstances these interventions were used and for how long.
The use of ECMO in babies with CDH is well described in the literature and although it is used commonly in some major centres / case series around the world there is no clear evidence that it alters the course of an individual case. Of the reviewed CDH cases born alive ECMO was used in a total of two cases and in a third case transfer for ECMO occurred but on arrival the baby’s condition was felt to be too poor to initiate ECMO. Its use appeared to be more readily considered when it was available locally. Of the 15 cases that died after birth, ECMO was documented as being considered in 3 further cases. Reasons for not referring for ECMO included the baby being too ill to move or being considered to have such severe pulmonary hypoplasia that it was incompatible with life. In the cases where ECMO was considered but felt to be inappropriate the reason for the clinical team’s decision, based on the records, was shared with the parents in two out of three cases.
On a small number of occasions babies diagnosed antenatally required transfer having been delivered away from the intended unit. Some babies delivered in units without neonatal surgery available on site and required transfer after delivery. Such transfers were not always straightforward with significant delays in an appropriate bed becoming available in three cases where the baby was in a neonatal intensive care unit awaiting a cot for surgery (See vignette 2). There was no clear evidence that this impacted on the child’s eventual outcome although it did cause distress to the parents (documented in the notes). All postnatal transfers of antenatally diagnosed cases, when they did occur, appear to have been carried out by an appropriate transport team.
Vignette 2
This case involved a young woman, with a concealed pregnancy who booked for antenatal care at 31 weeks of gestation, at her local district general hospital, supported by her parents, a community midwife and her social worker, where her baby was diagnosed with CDH. She was immediately referred to her local tertiary unit. She self-referred to the tertiary centre at 36 weeks of gestation where her baby was delivered by category 1 emergency caesarean section. The baby was admitted to the neonatal unit within 15 minutes of delivery, intubated, nasogastric tube inserted and ventilated. The baby’s condition was considered stable within 24 hours but the baby then spent 6 days in intensive care waiting for a surgical bed at the local children’s surgical unit. It became apparent after 5 days that a surgical cot would not be available locally and staff looked for a cot elsewhere. A surgical cot was offered in the third unit that they tried, but transfer was delayed until the following morning to avoid a late night transfer in cold weather.
Once the baby was admitted to the surgical unit, there was a further 5 day delay before surgical intervention took place despite clear documentation that the baby’s condition was stable. Post-surgical care was uneventful and the baby was transferred back into the care of the staff at the local District General Hospital at 4 weeks of age.
2) CDH cases presenting postnatally
Issues highlighted by the topic expert group for review in relation to early after-care were:
• Where applicable the care should be provided in accordance with the same principles as for antenatally detected cases.
This group of cases demonstrated the diagnostic difficulties that can be associated with CDH.
In these cases the clinical management was generally good once the correct diagnosis was made. However prior to this point there were a number of examples where the lack of a diagnosis or misdiagnosis led to inappropriate counselling or investigations. For

Perinatal Confidential Enquiry 2014 27
example a prolonged hospital stay and multiple investigations (including two bronchoscopies) were carried out in a child with persistent tachypnoea who was later found to have the rare anterior form of CDH on MRI.
These are difficult cases and they occur only rarely. None of this group underwent an antenatal MRI scan and it is unclear whether its use was indicated or would have led to a precise diagnosis at an earlier point.
The lack of planning in postnatally diagnosed cases resulted in two significant problems relating to transfer following the diagnosis. In one case a transport team was simply not available out of hours and hence the child had a protracted stay at a non-specialist unit (see Vignette 3). In a second case the child was transferred from A&E to the tertiary centre simply accompanied by his father.
Vignette 3
A primigravid mother, with an unremarkable antenatal history and normal antenatal scans and serology delivered at 40+5 weeks of gestation in her local District General Hospital. The child developed a degree of respiratory distress and was rapidly diagnosed to have a large congenital diaphragmatic hernia. The baby was efficiently paralysed, intubated, ventilated and stabilised by three hours of age. Transfer to the local specialist centre was requested but the transport team were “not available” as the transfer was requested after 20.00 hours and therefore the child had to remain at the hospital of birth until the next day when transfer did occur with successful surgery on day 5 after birth.
Surgery and Post-operative Care Issues
Issues highlighted by the topic expert group for review in relation to Surgery and Post-operative Care were:
a) Was the baby in a stable condition and suitable for surgery?
b) Who provided the peri-operative care?
c) Were they appropriately qualified/experienced?
d) Was the care provided to the correct standard and in the safest way possible?
Of the total group of 57 cases reviewed, 34 underwent surgery for CDH. In general this aspect of the care pathway met the expectations of the topic expert group although judging the prior experience of the surgical team was not possible. Surgery was delayed in two of the cases reviewed after the child had been admitted to a surgical cot, because of problems of staff or theatre availability.
In all antenatally diagnosed cases the decision to operate coincided with signs of improved stability in the baby. Timing of surgery was, as a result, able to be planned by the surgical team and took place between 8am and 8pm (standard working hours for the surgical team) in all cases where an operation was performed for CDH.
End of Life / Palliative Care Issues
CDH is a condition associated with high rates of mortality and long-term disability. Some parents opt not to continue a pregnancy once the diagnosis is made, whilst for other children it is only after birth that it becomes clear that the condition is so severe that the child cannot be stabilised. As a result there are multiple circumstances where issues of counselling, managing and supporting parents in such decisions might occur. The topic expert group identified aspects of care that they felt should be considered in relation to end of life /palliative care whenever it occurred in the care pathway, which were:
a) Were the parents sufficiently well-informed to enable them to make a decision based on what they knew and wanted for their baby?
b) Were all possible options explained?
c) Were discussion and psychosocial support for parents provided and well-documented in the case notes?
d) Was follow-up psychosocial care provided for the parents following their baby’s death?

Perinatal Confidential Enquiry 201428
The panel discussions generally reflected two points in the care pathway:
• Counselling and support in relation to a decision to terminate the pregnancy.
• Counselling and support in relation to a decision to re-orientate care to a palliative approach at any time after delivery had occurred.
1. Early intervention:
For cases of termination of pregnancy (TOP) following an antenatal diagnosis of CDH, the documentation of the process of counselling and support for those parents who decided to terminate a pregnancy was often vague. Of course the extent to which individual women or couples agonised over such a decision and the amount of information they felt they needed to make their decision is likely to have been extremely variable. Generally such detail was not apparent from the records. In some cases (for example where CDH was part of a trisomy such as Edward’s syndrome) the prognosis was undoubtedly bleak for any live born child. In cases of apparently isolated CDH the variation in the counselling referred to above, particularly regarding the likely outcome for the baby (see Diagnosis and Screening,) will clearly have had an effect on the decisions regarding whether to continue a pregnancy made by some women / couples.
Some panel members debated whether offering termination of pregnancy as an option after 24 weeks of gestation was acceptable given the predicted rate of survival is 50%.
In one particular case, poor counselling and subsequent support following a decision to opt for a termination of the pregnancy was highlighted by panel members as resulting in care of such poor quality, as to cause significant and avoidable distress (Vignette 4).
Vignette 4
Having been informed she was carrying a child diagnosed with CDH and Edward’s syndrome at 22 weeks of gestation, a woman was admitted to a District General Hospital at 34+1 week’s gestation with vaginal bleeding and in pain with a provisional diagnosis of a small placental abruption. Her case notes highlight that she was known to be socially isolated with young children, no family nearby and a husband who worked away from home.
There was no evidence in her case notes to suggest a holistic approach to her antenatal care or that a senior clinician had adopted a leadership role for her clinical management. A plan of care was made but not followed. Lack of resources “the unit was very busy” was recorded as the reason for the standard of care provided.
Bleeding and in pain she was left inappropriately unattended on an antenatal ward . There was no documented patient advocacy from midwifery staff and her case notes created the impression of a lack of compassion in the approach of the clinical team. The woman delivered a stillborn child and went home the next day.
There was no documented offer of a post mortem examination, the opportunity to create mementos, no documented offer of bereavement care, and no documented follow-up provision.
The woman did not attend her 6 week follow-up appointment and became pregnant the following year, and annotations to her case notes recorded that she had still not dealt with the death of her child from the previous pregnancy.
In only a small number of cases that were reviewed the pregnancy was terminated. As such, it was not possible to reach a conclusion concerning the overall quality of the psychological support provided in the short and medium term. However, there was no clear sense of a ’normal care pathway’ that included this type of support for women / couples who took this decision.
Perinatal Confidential Enquiry 2014 29
2. Decision-making phase post-delivery –
where, after delivery, the clinical team felt that there was no reasonable possibility of long-term survival, communication and decision making were generally well documented and involved almost exclusively the direct involvement of a consultant. Clearly it was more straightforward to counsel and make decisions regarding a child who could be assessed in their own right in terms of their condition instead of what might take place – the situation with antenatal counselling. Nonetheless this aspect of care appears to have been generally well done. In terms of subsequent support for families this was less well documented and often it was not clear who was to provide this care or where e.g. specialist centre, local neonatal service, or GP.
Long-term Outcome Issues
Issues highlighted by the topic expert group for review in relation to long-term outcome were:
a) Was follow-up care provided?
b) Who provided the follow-up care?
c) Was it individualised to the care needs of the child?
d) Where was it documented?
As with all aspects of care in relation to CDH the follow- up arrangements showed marked variation in the scope and duration of the care provided and currently there appears to be no agreed UK policy for the long-term care of these children and three cases reviewed during the course of the enquiry, appeared to have received sub-optimal or no follow-up care. Two babies were discharged home inappropriately early and required readmission shortly afterwards.
In one of the cases reviewed, a post-natal meeting with parents resulted in a change in policy in the unit concerned. This was highlighted as an example of good practice.
There is good evidence that children with CDH have a high rate of neurodevelopmental problems as well as problems associated with their surgery such as hiatus hernia. Although there is no relevant national
standard the approach to the need for and extent of long term follow-up was surprising with some children discharged by the age of one year if they seemed well and were thriving. By contrast, in other parts of the UK follow-up was provided in a specialist multidisciplinary clinic and continued throughout childhood.
Post mortems
In four of the five pregnancies that ended in termination reviewed by the panels consent was given for a post-mortem examination but in only one of the fifteen babies who died after being born alive. Two additional sets of case notes, in which the outcome was termination, arrived after the deadline for panel review and in one of these a post mortem examination also took place. The exact reason for this different pattern between terminations and postnatal deaths was not clear but the particularly low rate amongst the postnatal deaths was felt to be surprising. In those babies who underwent post-mortem the quality was felt to be good and the subsequent follow up and counselling was also well done by appropriate specialists.
ThemesIt was clear from the cases reviewed that CDH commanded significant time and input from the full range of senior clinicians represented on the panels i.e. midwives, obstetricians, fetal medicine specialists, neonatologists, paediatric intensivists, neonatal nurses, paediatric surgeons, and paediatric anaesthetists. There was no sense that the severity and complexity of the condition was not appreciated. However the low annual total number of cases means that for any one Trust / Health Board experience of the condition is limited. Similarly for the individual surgeon, anaesthetist or intensivist their personal experience could easily be limited to around one case a year unless a local arrangement focuses experience on individuals with a special interest and we identified no evidence of this. In most parts of the UK there was no evidence of a specific pathway for women / couples whose baby

Perinatal Confidential Enquiry 201430
has been identified with CDH and this has major implications for the way in which they receive their care. Essentially the package of care is not centred on the patient but instead the various components are assembled each time they are needed and this was reflected in many of the themes that emerged from the panel reviews.
Antenatal counselling (organisation)
The arrangements for parents to receive detailed counselling normally involved a visit to a specialist centre which, in some parts of UK, required a significant journey. In some centres it was possible to see all of the relevant specialists at the same visit either together or separately and this must be considered the standard that should be offered to parents. This approach was certainly not available for many women / couples. The use of telemedicine might have reduced the need for travel but in the cases we reviewed there was no evidence of the use of this approach.
Antenatal counselling (content)
It was clear from the records that the information given regarding prognosis in individual cases differed quite markedly. In terms of key issues such as the chances of survival and risk of long term developmental problems it appeared that, in a number of cases, there had not been adequate emphasis regarding the risks of an adverse outcome. This lack of consistency was compounded by the use of scan measures of severity (whose accuracy, reproducibility and validity appears to remain uncertain) in a few centres and not at all in others.
In two of the cases there was sufficient detail in the record for panel members to describe the process of counselling as “inappropriate” and “lacking compassion”.
Aspects of the counselling provided for a number of cases were commended by the panel. This included, in particular cases, the care by Consultant Obstetricians and Neonatologists, Community and Bereavement Midwives; the provision of appropriate written information, early referral to CDH UK and
other third sector organisations for additional support as well as the opportunity to create memories and mementos.
The role of fetal intervention (in utero measures intended to improve outcome) and MRI
Two cases were offered fetal intervention (tracheal occlusion - one resulting in neonatal death, the second child survived) and just four cases underwent fetal MRI (in one patient two separate MRIs, with a third planned at the time of delivery). There appeared to be no clear rationale for using either intervention and in none of these cases were the patients enrolled into a research project. Research to firmly establish the value (or not) of fetal intervention and MRI is required and panel discussions certainly identified a small number of cases who might well have benefitted from an in-utero MRI.
Approach to delivery
Six of the cases reviewed were planned to be delivered by caesarean section (although the indications were not solely based on the presence of CDH). A number of other babies did deliver by emergency caesarean section generally after an induction of labour. There was a complete lack of consistency in the approach to the timing of delivery with some cases being induced near term and others being left to go into spontaneous labour. Whilst in some cases there was clearly careful consideration of the gestation at which delivery should occur by contrast there was no evidence that there was similar consideration given to the time of day that the delivery should take place. Although almost all antenatally diagnosed cases were delivered in a fetal medicine setting, it seems self-evident that the resilience of the service to deliver safely and stabilise what is typically a very sick baby is much more limited when delivery occurs ’out of hours’. However it would be wrong to assume that planned caesarean section would automatically produce the best outcome for mother and baby. Issues of the timing and nature of delivery merit urgent evaluation in order to both standardise and optimise these elements of care for CDH cases.

Perinatal Confidential Enquiry 2014 31
Access to a neonatal cot
In terms of the cases reviewed the package of care was affected by a lack of an appropriate neonatal cot on five occasions. In these five cases induction was delayed as a result. In one notable case a baby required transfer after delivery from the neonatal intensive care unit to another hospital, in the same city, for surgery. Once the baby was in a stable condition, lack of a surgical cot led to a delay of several days before the surgery could take place (see Vignette 2). Although it is not possible to guarantee the consistent availability of a cot either for neonatal care or surgery ’open ended delays’ (with the induction or transfer being reviewed daily for more than one day) are not acceptable.
Approach to care after birth
It was probably amongst the group of babies who had a sustained period of care on the neonatal unit that variation in practice was seen most starkly. Most of these babies ran a very challenging course requiring a great deal of intervention and there was, in the vast majority of cases, clear evidence of consultant led care and in many cases consultant delivered care. There were very few cases where a panel felt this aspect of care was poor however the rationale for particular approaches or therapeutic choices showed great variation or was simply not clear. The use of ECMO provides an example with one or two centres clearly considering this as a routinely available treatment option whilst in other centres it was seen only as a rescue treatment that was considered for babies in extremis.
Follow up
Again parents will have experienced very different approaches to follow up depending upon where they lived and the service available either locally or in their nearest specialist centre. It would seem sensible that a service specification should make clear a core follow up process with the intention of identifying problems at an early stage and facilitating involvement of appropriate allied health professionals
such as physiotherapists and dieticians as necessary. This might also include access to appropriate advice re risks in future pregnancies.
Psychological support
The need for psychological support for parents was a potential consideration at various stages in the care pathway: following antenatal diagnosis, a decision to terminate the pregnancy, when the baby was extremely ill on the neonatal unit and following a postnatal death. Even when it was clear that a need for psychological support had been identified, in general, such support did not seem to be readily available.
Documentation
A common finding in national audits is a lack of adequate documentation around certain key aspects of care. This was also true of certain aspects of the CDH confidential enquiry particularly regarding decisions to terminate a pregnancy. Inadequate documentation was reported by panel members in 17 (30%) of the cases reviewed. There were instances of omissions where care was not documented adequately, or there was no evidence to support the fact it had been provided. There were also examples (10) of both inappropriate documentation and or incorrect information recorded. This included a missing consent form, a missing anaesthetic record, an inappropriate standardised letter sent to the mother in the postnatal period, and three separate cases of important inaccuracies recorded in the medical notes: 1. A misdiagnosis of CDH which continued into the discharge letter, 2. Documentation of a history of mental health problems that related to another patient, 3. Documentation of a history of drug abuse and this too related to a different patient. By contrast discussions to re-orientate care taken on the neonatal unit were generally well documented.
Leadership
In 16 of the cases reviewed, leadership issues were considered to have negatively influenced the standard of care provided at some point in the baby’s course. Lack of consultant grade input and
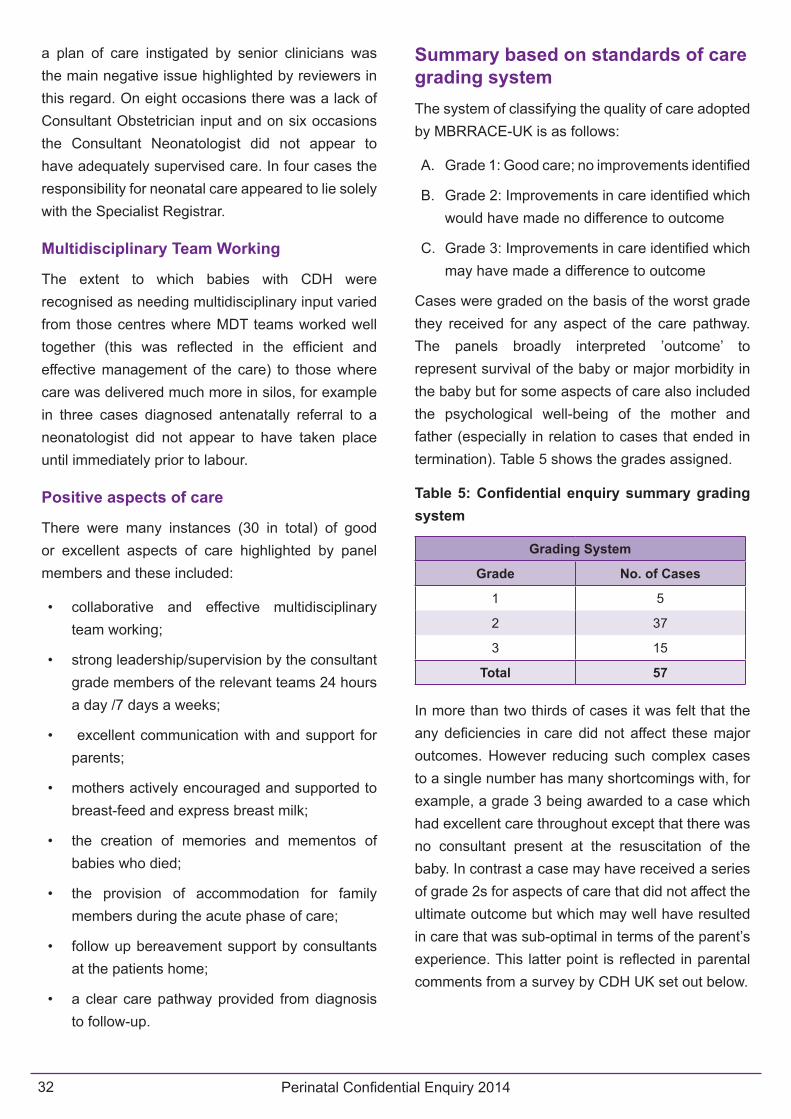
Perinatal Confidential Enquiry 201432
a plan of care instigated by senior clinicians was the main negative issue highlighted by reviewers in this regard. On eight occasions there was a lack of Consultant Obstetrician input and on six occasions the Consultant Neonatologist did not appear to have adequately supervised care. In four cases the responsibility for neonatal care appeared to lie solely with the Specialist Registrar.
Multidisciplinary Team Working
The extent to which babies with CDH were recognised as needing multidisciplinary input varied from those centres where MDT teams worked well together (this was reflected in the efficient and effective management of the care) to those where care was delivered much more in silos, for example in three cases diagnosed antenatally referral to a neonatologist did not appear to have taken place until immediately prior to labour.
Positive aspects of care
There were many instances (30 in total) of good or excellent aspects of care highlighted by panel members and these included:
• collaborative and effective multidisciplinary team working;
• strong leadership/supervision by the consultant grade members of the relevant teams 24 hours a day /7 days a weeks;
• excellent communication with and support for parents;
• mothers actively encouraged and supported to breast-feed and express breast milk;
• the creation of memories and mementos of babies who died;
• the provision of accommodation for family members during the acute phase of care;
• follow up bereavement support by consultants at the patients home;
• a clear care pathway provided from diagnosis to follow-up.
Summary based on standards of care grading systemThe system of classifying the quality of care adopted by MBRRACE-UK is as follows:
A. Grade 1: Good care; no improvements identified
B. Grade 2: Improvements in care identified which would have made no difference to outcome
C. Grade 3: Improvements in care identified which may have made a difference to outcome
Cases were graded on the basis of the worst grade they received for any aspect of the care pathway. The panels broadly interpreted ’outcome’ to represent survival of the baby or major morbidity in the baby but for some aspects of care also included the psychological well-being of the mother and father (especially in relation to cases that ended in termination). Table 5 shows the grades assigned.
Table 5: Confidential enquiry summary grading system
Grading System
Grade No. of Cases
1 5
2 37
3 15
Total 57
In more than two thirds of cases it was felt that the any deficiencies in care did not affect these major outcomes. However reducing such complex cases to a single number has many shortcomings with, for example, a grade 3 being awarded to a case which had excellent care throughout except that there was no consultant present at the resuscitation of the baby. In contrast a case may have received a series of grade 2s for aspects of care that did not affect the ultimate outcome but which may well have resulted in care that was sub-optimal in terms of the parent’s experience. This latter point is reflected in parental comments from a survey by CDH UK set out below.

Perinatal Confidential Enquiry 2014 33
Whilst the scoring system did provide a broad assessment of the overall package of care our experience of using this particular grading system has led us to consider some important refinements for enquiries starting after January 2015. In particular we will consider the overall outcome for the mother and baby separately. Secondly we will add a fourth category “Improvements in care identified which would have made a difference to outcome”
Parental perspectivesOne particular limitation of this enquiry was the need to use cases from 2009 and 2010. However the main charity in the UK focused on CDH (CDH UK http://www.cdhuk.org.uk) as part of the Topic Expert Group discussions arranged, in 2013, to poll their members regarding their own experiences of using the services for CDH. The questions asked were:
• Is there any aspect of your antenatal care during your pregnancy that you were unhappy with?
• Is there anything relating to the birth of your baby that you were unhappy with?
• Is there anything relating to your postnatal care that you were unhappy with?
• Is there anything that you feel would have helped to improve your care and overall experience?
They received 115 responses and from these the following themes and comments emerged:
A. Aspects of care that parents were unhappy with:
Antenatal care - these included a perceived lack of communication and understanding of NHS staff of the condition, feeling unsupported and afraid, being treated insensitively by staff.
Intrapartum care - NHS facilities perceived as being ill-equipped and under resourced, lack of staff, lack of cots.
Postnatal care - lack of support, lack of knowledge (staff), loss of continuity of care
B. Suggested Improvements to care:
• More information about CDH and its implications.
• The opportunity to talk to other parents early on and later.
• Access to details of support groups and written information when needed.
• Perceptions of the need for increased knowledge of doctors and nurses other than those in tertiary centres
• Desire for more follow-up – counselling, support, information.
Like the confidential enquiry process this survey can only provide a snapshot of care from the perspective of families who are CDH UK members and responded to the survey. Although the questions asked sought information which focused on negative experiences and gaps in provision it is important to note that many of the comments reflect a lack of consistency in approach and provision which was in accord with the review panel findings. Therefore, there is no suggestion that the issues raised by the review of cases from 2009 and 2010 have been resolved in the interim. On the contrary they appear to remain entirely relevant.

Perinatal Confidential Enquiry 201434
Lay report of the Confidential Enquiry
The lay report was produced by Christine Whitehouse on behalf of:
SANDS - Charlotte Bevan
Bliss - Melissa Green
CDH UK - Beverley Power
MBRRACE-UK: Elizabeth Draper, David Field, Pauline Hyman-Taylor, Jenny Kurinczuk
In briefIn the UK today, almost one in every 100 babies is stillborn or dies soon after birth. Up to 100 women die every year during or just after pregnancy. These figures are unusually high for a developed country. A team of academics, clinicians and charity representatives called MBRRACE-UK has been asked by the NHS to look at why this is so, and how care for mothers and babies can be improved.
In the first of a series of Confidential Enquiries, MBRRACE-UK examined congenital diaphragmatic hernia (CDH), an uncommon and complex condition which is not well understood. They identified many instances of excellent care, with teams of specialists, led by a consultant, working well together and offering solid support to parents throughout the process, from diagnosis to follow-up care. But they also found examples of poor and unacceptable care, where parents received no or inadequate counselling, where documents were inaccurate or missing, or where life-saving surgery had to be delayed because not enough special cots were available.
As a result of the enquiries, MBRRACE-UK recommended that in future a package of care should be tailored to the mother and baby’s medical and surgical needs, and offered at a small number of centres staffed by dedicated teams of specialists from obstetricians and neonatal nurses to psychologists and social workers
BackgroundEvery day in the UK 17 families are devastated by the death of their baby shortly before or soon after birth. Some of these deaths could be avoided. The NHS has recognised that improvements are needed in the health and care of women and their babies throughout the UK, and so it collects information about those who die or are born very sick every year to identify patterns in illness and disease in order to work out the best way to deliver care. This work is carried out by MBRRACE-UK, a team of academics and clinicians, a GP and representatives from the charity Sands.
MBRRACE-UK also conducts what are called Confidential Enquiries. These are an opportunity to gain a fuller picture of what happens when a particular illness occurs and how it might be treated or even prevented in the future. In a Confidential Enquiry, a panel of experts meets to look in detail at a sample of case notes (e.g. maternity records, referral letters and investigations such as scans, X-rays or a post-mortem examination) of mothers or babies who have died and to ask: did the mother or baby receive the right care, and how could it have been better?
For the 2015 report, MBRRACE decided to focus on the care of unborn and newborn babies with congenital diaphragmatic hernia (CDH). Relatively little is known about the best way to care for babies with CDH, and many either do not survive or survive with serious long-term health problems. At the moment they have to be monitored, cared for and treated by a large number of people.

Perinatal Confidential Enquiry 2014 35
What is congenital diaphragmatic hernia (CDH)?CDH occurs when the baby’s diaphragm (a thin sheet of muscle that separates the heart and lungs from the stomach and helps us to breathe) does not develop properly. This means that the stomach and other organs such as the liver and intestines may push into the chest cavity. This can affect how lungs develop and grow, making breathing difficult or, in some cases, impossible.
There are up to 300 cases of CDH in the UK every year. Most cases (around 70%) are diagnosed before birth by ultrasound scan performed during pregnancy. Of these, one in three mothers will either miscarry or choose not to continue the pregnancy.
Of all pregnancies affected by CDH, up to half of babies will die. Those that survive may experience a number of ongoing issues with their health, some mild and some severe. These could include problems with their lungs, stomachs and hearts. A child with CDH who survives could have learning difficulties, hearing impairment and behavioural disorders as they grow up. How well the baby is likely to do will depend on: whether the baby is born prematurely (before 37 weeks); how big the hernia is; whether there are other birth defects or genetic problems; and how badly the development of the lungs has been affected.
What does the review look at?Over the course of a year a panel of experts met to discuss 57 cases of CDH which were diagnosed in 2009 and 2010. (A representative from the charity CDH UK was present at the first consultation to establish how the enquiry would be conducted and how cases would be chosen, reviewed and graded.) This number, though small, included cases which were diagnosed before and after birth, and those with a range of different outcomes. This provided a ‘snapshot’ of CDH across the UK.
The panel considered the quality of care given to each of the 57 babies with CDH throughout the seven stages of what is known as the ‘care pathway’: screening for CDH and diagnosis; delivery of the baby; resuscitation; early after-care (up to 48 hours after the baby is delivered); surgery and post-operative care; palliative care (specialised care for people with serious illnesses or who may die); and long-term care (care for surviving babies into childhood). They graded the cases into:
1. Good care, no improvements identified (five cases fell into this category)
2. Improvements in care identified, would have made no difference to outcome (37 cases)
3. Improvements in care identified, may have made a difference to outcome (15 cases).
Even if just one aspect of the care was considered poor, the case was given the lowest grade:
A 28-year-old first-time mother, who had had normal scans, gave birth to a full-term baby boy at her local hospital. He had difficulty breathing, was diagnosed as having a large hernia, and was ventilated and stabilised within three hours. Transfer to a specialist unit was requested but as it was after 8pm, a suitable team was not available so the boy had to wait until the next day. When he was five days old, he was operated on successfully. Although the care was generally excellent and the baby survived, the fact that there was no suitable team available to transfer him when the diagnosis was first made affected the grading of the case (3).
What did they find?Mothers and babies with CDH could start their care in any one of 300 hospitals around the UK and have their specialist care in one of 27 centres. This means that neither individual consultants nor individual hospital trusts get much experience treating mothers and babies with CDH. In fact doctors may only see one or two cases a year, and sometimes may not treat a case for several years. So generally there is no specific pathway of care that is followed each time a baby is diagnosed with CDH.

Perinatal Confidential Enquiry 201436
Also, there hasn’t been much scientific evidence developed around what is the best care for babies with CDH. This evidence would form the basis of guidelines, policies and practices that could be used nationally or even internationally to make sure every baby got consistently good care.
What was considered to be good care?The panel found many examples of good or excellent care, which included:
• A clear pathway from diagnosis to follow-up
• Teams of people from different specialties working well together, led by consultants who were available round-the-clock
• Excellent communication with and support for parents, e.g. encouraging mothers to breastfeed/express milk and giving families somewhere to stay during acute care, and
• Follow-up bereavement support at the parents’ home, helping them to create memories and mementoes of their baby.
What was considered to be poor care?• Sometimes counselling and support was only
available at a specialist centre. At other times the wrong information was given. In a rare case, no psychological support was offered:
A woman diagnosed as carrying a child with CDH was transferred to her district hospital at 34 weeks, because she was bleeding and in pain. After being poorly looked after for 12 hours, she was sent home a day after delivering a stillborn girl. A plan of care was not followed and a lack of resources - “the unit was very busy” - was blamed.
• The care mothers and babies received wasn’t consistent, with some receiving special treatment and others not. These include: surgery on the baby when still inside the womb (using a technique called FETO which encourages the baby’s lungs to grow by putting a small balloon into the windpipe before birth); and ECMO (a
machine which does the work of a baby’s lungs and heart, breathing and delivering oxygen into the blood).
• There sometimes wasn’t enough thought given to the time of day that the mother should give birth: delivering and stabilising a very sick baby is much more difficult overnight or at weekends when some important members of the team may not be available.
• There were not always enough special cots. This is particularly upsetting, when parents don’t know from one day to the next when a cot will be available. It means that induction (when labour is brought on with the use of drugs) and even life-saving surgery may have to wait for several days:
A young girl, diagnosed as carrying a baby with CDH at 31 weeks, gave birth to a boy at 37 weeks in her local hospital. He spent six days in intensive care waiting for a bed at the local children’s surgical unit. He then had to wait another five days for surgery.
• Follow-up care was patchy and regular follow-up care after the baby went home from hospital often depended on where parents lived and whether they had access to specialists such as dieticians who advise on feeding and nutrition or physiotherapists who help with the baby’s development.
• Important documents were incomplete or missing. Some sets of notes contained very little detail, particularly concerning a decision to end a pregnancy. Others records referred to the wrong patient or provided information insensitively.
What do parents think?This Confidential Review looked at cases from 2009 and 2010. To check whether or not the issues raised in the panel reviews were still relevant, CDH UK asked its members about their experiences of care in 2013. From 115 responses, the charity found that little had changed in three to four years: parents felt

Perinatal Confidential Enquiry 2014 37
that before birth, staff did not understand CDH and therefore did not support them or communicate well or sensitively about it; during birth, there were too few staff or resources such as cots; and after birth, there was a lack of knowledge in the non-specialist centres as well as lack of support and coordination of care after the baby was taken home or after bereavement.
What are the recommendations following the review?The Confidential Enquiry recommended that the service be more patient-centred i.e. a package of care should be tailored according to the mother and baby’s medical and surgical needs, rather than put together, sometimes hastily, depending on what resources are available.
This will involve changing the way care is delivered. This should be at a smaller number of centres which are run by clinical networks (teams of people with very specialist expertise e.g. obstetricians with particular experience of dealing with CDH) to manage the care of very ill babies.
While having a smaller number of centres with dedicated services will mean some parents will have to travel longer distances than they currently do, it will make it easier to:
• Include all important elements of care, such as counselling and psychological support (especially for decisions about ending a pregnancy so parents can make an informed choice).
• Agree on the best way to manage the care and treatment of babies diagnosed with CDH and how to handle late termination of pregnancy and set UK-wide standards.
• Produce a national ‘information sheet’ with clear and consistent information about CDH.
• Keep track of the correct and complete documentation of each case of CDH.
• Bring researchers together to work on scientific studies so that approaches to the care of babies with the condition can become more based on good-quality evidence.
• Make sure all cases of CDH are recorded and followed up properly on a proposed NHS register, which will give researchers a single, reliable source of information from which to learn more about trends in conditions where there is a problem about how the baby develops in the womb, such as CDH, across the UK.
CDH UK also made some recommendations:
• there should be more information about CDH and its implications
• parents should have opportunities to talk to other parents
• parents should be given written information and details of support groups
• doctors and nurses other than those in specialist centres need better knowledge of CDH, and
• there should be better coordinated follow-up care.
Further readingTo read the full report, MBRRACE-UK 2013/2014 Perinatal Confidential Enquiry – Congenital Diaphragmatic Hernia (CDH), to read more about the involvement of patients and the public in decisions about services, and to find out about the topics for confidential enquiries that MBRRACE will cover, see www.npeu.ox.ac.uk/MBRRACE-UK

Perinatal Confidential Enquiry 201438
References
1) Stege G, Fenton A, Jaffray B. Nihilism in the 1990s: The true mortality of congenital diaphragmatic hernia. Pediatrics. 2003 Sep;112(3 Pt 1):532-5.
2) Wright JC, Budd JL, Field DJ, Draper ES. Epidemiology and outcome of congenital diaphragmatic hernia: a 9-year experience. Paediatr Perinat Epidemiol. 2011 Mar;25(2):144-9.
3) Wynn J, Aspelund G, Zygmunt A, et al. Developmental outcomes of children with congenital diaphragmatic hernia: a multicenter prospective study. J Pediatr Surg. 2013 Oct;48(10):1995-2004. doi: 10.1016/j.jpedsurg.2013.02.041.
4) National Audit Office. Maternity Services. London 2013. http://www.nao.org.uk/wp-content/uploads/2013/11/10259-001-Maternity-Services-Book-1.pdf
5) Draper ES, Kurinczuk JJ, Lamming CR, Clarke M, James D, Field DJ. A confidential enquiry into cases of neonatal encephalopathy: Clinical governance in practice. Archives of Disease in Childhood 2002; 87:F176-F180
6) Lindquist A, Kurinczuk J, Redshaw M, Knight M. Experiences, utilisation and outcomes of maternity care in England among women from different socio-economic groups: findings from the 2010 National Maternity Survey. BJOG. 2014 Sep 17. doi: 10.1111/1471-0528.13059. [Epub ahead of print]
Perinatal Confidential Enquiry 2014 39
Appendices
Appendix 1 – Consensus statement from the Topic Expert group
Guidelines for judging/grading of cases for review for:
2014 Perinatal Confidential Enquiry into Congenital Diaphragmatic Hernia The following document represents the views of an “expert panel” representing a range of specialisms (see Appendix 1) who met to outline an appropriate care pathway for babies diagnosed with congenital diaphragmatic hernia either before or after delivery. The document is meant to guide those who review the selected cases in judging / grading the various aspects of care provided using the following system:
It is not possible to grade the presence or absence of good clinical practice markers in isolation. The markers of good clinical care set out below need to be graded within the clinical context of each individual case. What might not have influenced outcome in one case might well do so in another. How each is graded will depend on the assessor’s clinical interpretation of how the various aspects of care were delivered in relation to the circumstances of the particular case being reviewed.
CLINICAL CARE ISSUES TO BE ASSESSED
1. Screening and Diagnosis Issues
Was screening carried out at the appropriate time?
Did the mother of the child decline screening, or book into antenatal care late in the pregnancy? Was referral appropriate and timely (taking into account geographical location)?
Was counselling documented as regards content and with the appropriate multidisciplinary team?
Was there evidence that the counselling was provided in a way to meet the mother’s / family’s needs including, if appropriate, access to a multidisciplinary team?
Was sufficient time given for the decision-making process?
1.1 Good clinical practice would include:
• An ultra-sound scan at 18+0 - 20+6 weeks gestation.
• The parents of the child should have been offered invasive testing for chromosome anomalies
• If the diagnosis of CDH was suspected on a screening scan the mother should have been seen by a clinician able to confirm and discuss the diagnosis in more detail (obstetrician with an interest in antenatal diagnosis, radiologist with an interest or fetal medicine consultant). This review should have included specialist scanning to exclude other congenital anomalies. Depending on local facilities this might have been by a clinician within the same hospital, in which case they should have been seen within three days, or they might have been referred to a fetal medicine centre in which case they should have been seen within 5 days of referral.

Perinatal Confidential Enquiry 201440
• Once the diagnosis was confirmed the parents should have been offered an opportunity to meet the MDT in the relevant tertiary centre who would be providing care for the baby. The MDT team should have provided written and verbal information to parents.
• Some women will have chosen not to continue a pregnancy based on the diagnosis alone whilst others will have wished to delay such a decision until they had had an opportunity to seek further information and counselling including on some occasions the MDT. Adequate time should have been given for the parents to consider the option of termination of pregnancy following diagnosis and/or their meeting with the MDT. The choice made by parents should have been supported by the MDT.
• Information should have been provided to enable access to alternative sources of support, e.g. CDH UK, Antenatal Results & Choices (ARC), HealthTalkOnline, etc.
1.2 Issues lacking consensus
• The panel were divided in relation to the value of antenatal measurements of severity.
2. Delivery issues
Where was the baby delivered?
Was the baby born in the planned place of delivery?
At what gestation was the baby delivered?
Was it a planned delivery?
Was labour induced?
Who was responsible for the baby’s care and treatment?
2.1 Good clinical practice would include:
• Delivery should have been carefully planned to take account of maturity (> 38 weeks gestation), immediate access to specialist neonatal support and the distance of the mother’s home from the specialist centre. Timing of delivery should also have taken account of availability of appropriate MDT members. If delivery was by planned CS ideally this should not have occurred before 39 weeks.
• Planned delivery should have taken place in a tertiary centre, with a Level 3 Neonatal Intensive Care Unit with Neonatal Surgery available on site or affiliated and 24 hour access to a paediatric cardiology specialist.
• A Consultant Neonatologist should have been present at the delivery
• In the case of post-natal diagnosis: timely referral and transfer to a tertiary neonatal surgery centre with the appropriate transport team should have occurred.
3. Resuscitation Issues
Who was involved in the emergency care of the baby?
Were they appropriately qualified/experienced?
What evidence is available to demonstrate attempts were made to avoid lung injury?
Was there adequate communication with parents regarding the baby’s condition?

Perinatal Confidential Enquiry 2014 41
3.1 Good clinical practice would include:
• Resuscitation should have been Consultant led, supported by an adequate team.
• Prompt transfer from labour ward to NICU after initial stabilisation should have taken place.
• For babies diagnosed antenatally, there should have been immediate endotracheal intubation, IV access and early passage of an oro/naso-gastric tube.
• There should be evidence in the records of a lung protective ventilation strategy
• There should be clear evidence of early communication with parents whilst in the delivery room, documented in the case notes and parents given an opportunity to see and touch their baby before transfer to NICU, where appropriate.
4. Early After-Care (i.e. 1-48 hours post-delivery) Issues
What measures were taken to assess/monitor, the severity of the condition?
Were the care options discussed with the baby’s parents? By whom?
4.1 Good clinical practice would include:
• There should be evidence of the early institution of full invasive monitoring including invasive arterial monitoring and central venous access.
• Echocardiogram (together with a specialist cardiac assessment) and a head ultrasound scan should have been performed as soon as possible.
• Pulmonary hypertension should have been adequately assessed and managed/treated.
• A lung protective ventilation strategy should have been used and documented.
• Careful consideration should have been given to fluid management to minimise the adverse effects of 3rd spacing.
• Inotropic support should have been initiated early where indicated to achieve Systemic BP at least that appropriate for gestational age.
• If cardiac output was poor, in the presence of evidence of pulmonary hypertension, Prostin might have been considered to maintain ductal flow and offload the RV if deemed appropriate by echocardiography findings
• Any transfer to the surgical unit should have been by a designated, appropriately trained, transport team.
• In cases where the baby could be adequately stabilised and the degree of pulmonary hypoplasia was felt to be compatible with long term survival Extracorporeal Membrane Oxygenation (ECMO) should have been considered, and the case discussed with an ECMO Centre. Following discussion with an ECMO Centre, the case for/against ECMO should have been discussed with parents. The reasons for its use, its limitations and why it was/was not advisable for the treatment of their baby should have been documented.
4.2 Late Presentation of CDH:
• The care should be provided in accordance with the principles described above where applicable.
Perinatal Confidential Enquiry 201442
5. Surgery and Post-operative Care Issues
Was the baby in a stable condition and suitable for surgery?
Who provided the peri-operative care?
Were they appropriately qualified/experienced?
Was the care provided to the correct standard and in the safest way possible?
5.1 Good clinical practice would include:
• The timing of surgery should have been based on whether the baby’s condition was sufficiently stable using protective ventilation modes and on moderate/minimal inotropic support, with evidence of resolving/resolved pulmonary hypertension.
• The surgery should have been timed to occur in normal working hours (8am to 8pm).
• The same intensive care unit should have provided both pre-operative and immediate post-operative care.
• Surgery should have been Consultant delivered, with an experienced specialist paediatric anaesthetist present.
• If transferred to theatre for surgical repair, the baby should have continued to receive the same level of support during transport as in the NICU and the transport team should have been appropriately experienced.
• The baby should have been transported on a ventilator (not hand-bagged), CO2 should have been monitored during transfer and surgery and the use of nitrous oxide avoided.
6. Palliative Care Issues
Were the parents sufficiently well-informed to enable them to make a decision based on what they knew and wanted for their baby?
Were all possible options explained?
Were discussion and psychosocial support for parents provided and well-documented in the case notes?
Was follow-up psychosocial care provided for the parents following the baby’s death?
6.1 Early intervention: Termination of pregnancy (TOP)
6.1.1 Good clinical practice would include:
• Information on methods of termination and bereavement (such as that from ARC) should have been provided to parents
• The case notes should provide evidence that there was provision of information for parents for whom English was not their first language
• Fetocide should have been offered if appropriate
• Counselling should have been offered by the MDT team if requested by the family.
• Parents should have been referred to alternative sources of information and support (e.g. CDH UK, ARC, HealthTalkOnline, etc.)
• A post-mortem should have been offered and this discussion should have been documented
• Counselling should have been offered at 3 months post-termination

Perinatal Confidential Enquiry 2014 43
6.2 Decision-making phase post delivery
6.2.1 Good clinical practice would include:
• The reorientation of care should have been discussed in cases where:
◦ There was a failure to stabilise the patient in a situation where ECMO was not appropriate or declined,
◦ The presence of other major congenital anomalies and/or severe intracranial haemorrhage was not compatible with survival with an acceptable quality of life.
• Any decision to re-orientate care should have been supported by the relevant MDT and this should have been documented.
• There should have been documentation of a discussion with the family regarding reorientation of care. This discussion should have been led by a Consultant.
• The options for palliative care should have been explained to parents and documented in the case notes.
• The wishes of the family should have been documented in the case notes.
• A private space should have been provided for parents and their baby.
• Evidence of follow-up should have been documented in the case notes (and, where appropriate a discussion of the post-mortem results).
• Bereavement follow-up should have been offered <7 weeks after death
7. Long-term Outcome Issues
Was follow-up care provided?
Who provided the follow-up care?
Was it individualised to the care needs of the child?
Where was it documented?
7.1 Good clinical practice would include:
• Pre-discharge, all babies should have received all relevant newborn screening and immunisations
• Follow-up care should have been provided tailored to the needs of the individual child (this might have included access to dietetics, neurodevelopmental physiotherapy, SALT, Paediatric Surgeon, Neonatologist and other relevant clinical specialties).
• Details of these arrangements should have been provided in the discharge summary and clinic letters.
Perinatal Confidential Enquiry 201444
Appendix 2: Instructions for Trusts / Boards regarding the anonymisation of notes and document checklist
2014 Confidential Enquiry into Congenital Diaphragmatic Hernia
Anonymisation of Notes Guidance Document • Do not use a black felt tip or marker pen which may dry out eventually and allow the underlying text
to become clearly visible again, often seeping through to the back of the page and sometimes through to several pages. This is particularly a problem with double sided photocopies.
• Photocopy the original case notes. Please work with and return an anonymised copy of the case notes
• The best method for anonymisation of notes is to use a correction roller – this has been provided. Please use on the copied notes.
• Before starting, check that all the pages are present for each section of the notes & in date order. Please number the pages sequentially, (in the bottom right hand corner of each page), to facilitate the discussion of the case. A code has been allocated for each case. Please mark the maternal and baby notes appropriately e.g. M001 and B001. The appropriate numbering convention for each case will be sent to you by the MBRRACE-UK team. A list of the required notes for each case has been provided. Please ensure identifiers are not visible.
• In order to limit the amount of photocopying and anonymisation necessary for the enquiry, for those cases who survive for more than 28 days, please provide information up to and including 28 days old. If following review a key element of care is deemed to be missing from the information provided: we will contact you to request further details.
• Please ensure all of the staff names and information are removed and replaced with the job title or grade so that the notes make sense and it is possible to tell who wrote what.
• Please ensure all of the identifiers are removed from the notes this includes the Trust’s header/footer/address/logo.
• Please remove less obvious identifiers such as contact numbers for local support services etc. so that it is not possible to identify the region where the case occurred.
• Please remove staff initials from drug charts/NNU & PICU charts/early warning charts.
• Please do not use white stickers which are difficult to cut to size and so often obscure some of the written content as well as the identifier.
• During the copying/scanning, leave out any blank pages – (the notes contain a standard set of papers not all of which are needed by all patients.) Do not copy sheets of hospital identification labels. Do not collect growth charts unless specifically requested.
Please ensure that the following are blanked to ensure complete anonymisation
• Patient and parents first and family names, even when referred to only by their first names. If the baby, parents or siblings are referred to by name, you will need to substitute as appropriate i.e. patient, mother, sister etc.;
• The hospital identification number;
Perinatal Confidential Enquiry 2014 45
• The patient’s NHS number;
• The patient’s/parents address and telephone numbers;
• All staff names, including initials. Status of staff to be substituted where possible;
• All details of hospital name, addresses and phone/fax numbers printed on all stationary;
• Laboratory numbers that are assigned to individual patients;
• Blanking of the information has to be absolute. Check that this is satisfactory early on in the process by scanning sheets to avoid having to repeat the work. Please use the correction rollers provided.
• You will have to read through the notes and have some understanding of the clinical picture. Some staff refer to patients, parents and other professionals by name. First & family names must all be masked. Patients being referred to other hospitals must have the name of the new hospital masked.
• Please write over the correction tape where necessary in order to make it clear to the confidential enquiry panel the status of the professionals providing care. Many, but not all, professionals indicate their status after signing entries in the notes. In this case you only need to blank the name and signature. However, if they have not done so, you will need to write in their status i.e. Consultant, ANNP, Dr, Nurse, Health Professional, etc. as appropriate. This will also apply to professionals named who are working in other Trusts – usually in the context of a baby being referred to another unit. If another hospital is named, you will need to mask it and write over it the status of the care that that particular hospital provides i.e. Level 3 Neonatal Services etc. Neonatal Transport Teams will need to be anonymised – names of the team substituted by professional status and the actual name of the Transport Service substituted by Neonatal Transport Team or Service. It needs to be clear that this has been inserted by the anonymiser i.e. use a different colour/capital letters.
• Signature sheets are included in some notes. They will be useful to the person doing the anonymisation, but they do not need to be sent to the enquiry team.

Perinatal Confidential Enquiry 201446
Document checklistPlease supply the following documents. Where a document is not available, please give the reason why and where relevant, inform us of the person we should contact to request this information. You may use the notes section overleaf to record this information if necessary.
Document checklist Please supply the following documents. Where a document is not available, please give the reason why and where relevant, inform us of the person we should contact to request this information. You may use the notes section overleaf to record this information if necessary. Information Attached
(please tick √)
Reason if not attached
Hospital Maternity Records include fluid and drug charts, test results, antenatal and discharge summaries and printed output from electronic records systems
Women’ hand-‐held maternity notes
Written communications include correspondence and referral letters
GP records
Evidence of screening for congenital anomaly e.g. Ultrasound scan, cardiac assessment, MRI etc.
Obstetric case notes
MDT meeting records
Fetal medicine case notes
X-‐rays and scans

Perinatal Confidential Enquiry 2014 47
Document checklistPlease supply the following documents. Where a document is not available, please give the reason why and where relevant, inform us of the person we should contact to request this information. You may use the notes section overleaf to record this information if necessary.
Document checklist Please supply the following documents. Where a document is not available, please give the reason why and where relevant, inform us of the person we should contact to request this information. You may use the notes section overleaf to record this information if necessary. Information Attached
(please tick √)
Reason if not attached
Hospital Maternity Records include fluid and drug charts, test results, antenatal and discharge summaries and printed output from electronic records systems
Women’ hand-‐held maternity notes
Written communications include correspondence and referral letters
GP records
Evidence of screening for congenital anomaly e.g. Ultrasound scan, cardiac assessment, MRI etc.
Obstetric case notes
MDT meeting records
Fetal medicine case notes
X-‐rays and scans
Laboratory reports include haematology, virology, bacteriology and microbiology reports
Delivery case notes including details of resuscitation attempts
Neonatal case notes including blood gases, measurements of blood pressure, drug charts
Operation notes (including anaesthetic record)
Discharge summary
Outpatient clinic records and correspondence
Local hospital review, local enquiry or critical incident report (if available)
Please use this space to record any additional information

Perinatal Confidential Enquiry 201448
Appendix 3: Training materials for assessors including instructions for access to the on-line case review system and confidentiality agreementsGuidance and training document for case review panel members (including Topic Expert Group membership and case evaluation form)
MBRRACE-UK 2014 Perinatal Confidential Enquiry into Congenital Diaphragmatic Hernia
Case review panel member guidance and training
Thank you for agreeing to take part in the confidential enquiry into congenital diaphragmatic hernia (CDH). The purpose of the enquiry is to look at quality of care identifying aspects of both good practice and aspects where there is a need for improvement. By way of preparation for the process this document sets out the key steps in the process and the general principles that will be applied. In addition you will also be invited to join a telephone conference which will go over these issues again, provide an opportunity for you to ask any questions about parts of the process that are not clear and explain how to access the cases on-line.
Preparation for the enquiry process
The cases to be reviewed have been drawn from an existing epidemiological study based on the whole of the UK. From this study 66 cases have been selected to form the basis of the confidential enquiry and have been chosen to represent both a geographical spread across UK and the full range of outcomes associated with CDH. The notes of the selected cases have been anonymised both in terms of the hospitals and clinicians involved although entries in the notes should record the type and grade of staff who made the entry. Clearly the notes of the cases selected vary greatly in complexity as they include children who survived after a prolonged hospital stay and other cases where after diagnosis the family chose a termination. In relation to the former types of case we have limited the neonatal records to the first month of life as it is the package of care we wish to examine rather than a particular outcome. This variation in case type will influence the number of cases that can be discussed at any one assessment meeting but we will aim to balance the work out between our groups of assessors
As there are currently no NICE guidelines or other established standards for the care of infants with CDH, a consensus “optimal” care pathway has been agreed by a Topic Expert Group convened to steer the enquiry (a multidisciplinary group comprising of clinical experts and a patient representative (see Appendix 1). The aim of this document is to provide a framework against which cases can be assessed and a copy of the document is attached as a separate document).
The assessment process
You will be asked whether you can attend an assessment panel on a particular date and once it is clear that a full multidisciplinary team can be convened (joining by telephone will not be acceptable) all the members of the assessment team will receive a confirmed date and venue (we will do our best to make travel arrangements as easy as possible). The meeting will generally last the whole day. Each meeting will comprise a maximum of 12 panel members of mixed specialty and will be chaired by one of the MBRRACE-UK team.

Perinatal Confidential Enquiry 2014 49
Approximately one month ahead of the meeting you will be given access to the notes of the cases to be discussed on that day. As indicated above the number of cases to be discussed will vary depending on complexity. You will be asked to read all of the cases and “score” the care. In addition one or perhaps two cases will be identified for which you will be asked to lead the presentation at the face to face consensus meeting.
When you attend case review panel consensus meetings the Chair (neutral) will re-iterate the principles of the process and answer any questions prior to the start of the meeting. During the course of the case review panel meetings each case will be discussed with the aim of resolving any differences of opinion about the standard of care provided. At the end of each discussion a confidential enquiry case summary form based on the panel view will be completed. The final consensual assessment of each case will be collated by the MBRRACE-UK team.
Access to case notes
All details of allocated cases (surveillance data, case notes, post-mortem report and any local review) will be available for viewing only via a secure online high compliance system. Full details for accessing the anonymised notes via the case viewer will be provided to each case reviewer in an email (Appendix 3), as well as an invitation to join a live online demonstration of the system before the review process begins. Please note: all users of the MBRRACE-UK system are required to complete and return our confidentiality statement and declaration of interest form before access is granted to view the selected cases (see Appendix 4 and 5).
Panel members will access the case notes they have been allocated on-line and assess each case using the standard form. As a case review panel member you will be sent paper copies of the assessment forms by the MBRRACE-UK office and instructed to complete the forms for each case allocated for review. These will be collected at the panel meeting following the discussion of each case.
Anonymisation of cases
All cases will be supplied in an anonymised format and no attempt should be made to try to identify the identity of cases, individuals or hospitals.
Assessment form
We have developed a form to support the review process (Appendix 2). The assessment form asks the reviewer to consider a series of steps on the care pathway from diagnosis to discharge / death which map to the various headings on the document produced by the expert panel. It comprises questions about the quality of care at each stage using a grading system (see below) but also includes free text boxes for reviewer’s opinions or other points they wish to raise. Not all cases will be relevant to all steps on the pathway e.g. terminations will not require the neonatal sections to be completed.
Categorisation of cases
For each aspect of care along the pathway reviewers will be asked to grade the care into one of the following three categories:
• Good care; no improvements identified
• Improvements in care* identified which would have made no difference to outcome
• Improvements in care* identified which may have made a difference to outcome

Perinatal Confidential Enquiry 201450
(*Improvements in care should be interpreted to include adherence to guidelines, where these exist and have not been followed, as well as other improvements which would normally be considered part of good care, where no formal guidelines exist.)
At the end of the discussion of each case at the, a summary score will be determined for inclusion in the final report.
Please note that whilst the aim of the enquiry is to focus on quality of care HQIP has specific guidance that applies in any case where any deficiencies in care are of a more serious nature:
HQIP Cause for Concern Guidance
• Death (child or adult) attributable to abuse or neglect, in any setting, but no indication of cross agency involvement (i.e. no mention of safeguarding, social services, police or LSCB).
• Staff member displaying:
◦ Abusive behaviour (including allegations of sexual assault)
◦ Serious professional misconduct
◦ Dangerous lack of competency
◦ But not clear if incident has been reported to senior staff
• Standards in care that indicate a dysfunctional or dangerous department or organisation, or grossly inadequate service provision.
Cases felt to fulfil these criteria must be notified separately and urgently.

Perinatal Confidential Enquiry 2014 51
The MBRRACE-UK web-based data entry system is available for the 2013 Perinatal Confidential Enquiry (CDH) Case Review. The MBRRACE-UK web address is: www.mbrrace.ox.ac.uk
• If you are already registered on the MBRRACE-UK system as a reporter then please continue to use your current login.
¾ Once you login then please select the Maternal Deaths option and then Case Assessment. Select a case and click on the View Case Notes button. You will then see the case notes displayed.
¾ Please note that you will not be able to view the case notes if we have not yet received a signed copy of the Confidentiality Statement and Declaration of Interest form from you.
• Once you have reviewed a case please complete a copy of the attached MBRRACE-UK Case Evaluation Form (Appendix 2).
• Please bring all completed case evaluation forms with you to the panel review meeting.
If you have requested that we contact you using a “home” email address we will endeavour to ensure that we send out a brief notification to your home address when a new case is available for you to review. Please do not use your home e-mail address to correspond with us about a case or to send documents to us.
• If you are a new user to the system your username is your registered email address that you have supplied us with. This will be either, your NHS Trust, nhs.net or University email address.
To log in for the first time, enter your username, leave the password field blank, then click ‘request a new activation code’. You will then need to enter your username again and click ‘request’. You will receive the code via email, which you then use as the password when logging in. You will then be prompted to change your password.
The rules for passwords are:
• Maximum length of 20 and a minimum length of 8
• No dictionary words longer than three characters
• At least 1 number and 4 letters
• The letters must be mixed case
• Special characters from the list $@#+![]
• Special characters are not required but may be included
• Different to the last five passwords
Now please follow the instructions for registered users on the previous page
If you need any further assistance the team will be happy to answer any queries and can be contacted by email: [email protected] or by telephone: 0116 252 5425/5408

Perinatal Confidential Enquiry 201452
Confidentiality Statement - Confidential Enquiry Panel Assessors
MBRRACE-UK is a collaboration led from the NPEU, University of Oxford who was appointed by the Healthcare Quality Improvement Partnership (“HQIP”) to deliver the national Maternal, Newborn and Infant Clinical Outcome Review Programme, including the Confidential Enquiry into Perinatal Mortality and Morbidity. The MBRRACE-UK collaborators are delighted that you have agreed to act as an MBRRACE-UK Confidential Enquiry Panel Assessor.
The appointment requires you to review case studies and to provide your written findings, conclusions and recommendations in relation to your assessment of the case. Accordingly, your appointment will involve the disclosure to you, both directly and indirectly, of confidential case materials in a variety of forms and media. In consideration of the opportunity to be involved in this project as an MBRRACE-UK Confidential Enquiry Panel Assessor, please read the terms set out below, and confirm your agreement to these terms by signing the enclosed duplicate where indicated.
In my role as an MBRRACE-UK assessor I declare that:
• I undertake not to make or keep an electronic or paper copy of the case materials with which I am provided for the purposes of MBRRACE-UK confidential enquiries.
• I will only discuss the details of any individual case (findings, conclusions and recommendations) which I assess in my role as an MBRRACE-UK assessor with other MBRRACE-UK assessors and members of the MBRRACE-UK team unless otherwise specifically authorised to do so by the MBRRACE-UK Perinatal Lead Prof Elizabeth Draper.
• I will at all times keep completely confidential any information relating to the review of individual cases, discussions with other MBRRACE-UK panel assessors and MBRRACE-UK team members, and any other aspects of my role as an MBRRACE-UK panel assessor.
• Should I recognise a case from my clinical work, medico-legal work or some other set of circumstances I will immediately stop reviewing the case and declare this prior knowledge to the MBRRACE-UK Perinatal Lead Prof Elizabeth Draper, or to the MBRRACE-UK Lead Prof Jenny Kurinczuk. I understand that depending upon the circumstances it may be necessary to reallocate the case.
• Having reviewed an individual case for the purposes of the MBRRACE-UK confidential enquiries should I encounter this case at any point in the future in relation to medico-legal work or any other similar work, that I will declare a conflict of interest and withdraw from that work thereby ensuring that I do not make use of any privileged information arising from my involvement in MBRRACE-UK for any other purposes and that all such activities are kept completely separate and confidential.
• In the course of my work for MBRRACE-UK that I understand that I am bound by my usual professional code of conduct.
• I understand that this agreement will extend in perpetuity beyond my tenure as an MBRRACE-UK panel assessor.
Name: …………………………………………………………………………………………..
Signature: ………………………………………………………………………………………
Date: _____/_____/_____
Perinatal Confidential Enquiry 2014 53
MBRRACE-UK Confidential Enquiry Panel Assessor - Declaration of Relevant Interests Form
Name:
Relevant paid interests (it is not necessary to disclose the amount):
Other relevant interests (e.g. membership of organisations or unpaid work):
Relevant interests of the panel assessor personal partner and other close family members:
Is there any other information which would be deemed reasonable for the MBRRACE-UK team to be informed of that could give rise to a conflict or perceived conflict of interest with the MBRRACE-UK Confidential Enquiry work?
I have declared above all current, relevant interests and I will identify any future interests to the MBRRACE-UK team if and when they arise.
Signed ………………….………..………………….
Name…………………………………………………
Date ………………………………………………….

Perinatal Confidential Enquiry 201454
Appendix 4: Assessment documentation used by panels
Case num
ber:
MBR
RACE
-‐UK 20
14 Perinatal Con
fidentia
l Enq
uiry– Co
ngenita
l Diaph
ragm
atic Hernia
Sub-
optim
al c
are
O: N
o su
b-op
timal
car
e
1:
Min
or s
ubop
timal
car
e
2: S
igni
fican
t sub
optim
al c
are
3:
Maj
or s
ubop
timal
car
e
Rel
evan
ce o
f gra
de o
f car
e to
ou
tcom
e
O: N
ot re
leva
nt
1:
Pos
sibl
y re
leva
nt
2:
Pro
babl
y re
leva
nt
3: A
lmos
t cer
tain
ly re
leva
nt
Wha
t:
R:
Failu
re to
reco
gnis
e pr
oble
m
A:
Failu
re to
act
app
ropr
iate
ly
C
: C
omm
unic
atio
ns fa
ilure
S:
Fa
ilure
to s
uper
vise
H
: A
ny la
ck o
f hum
an re
sour
ce
E: A
ny la
ck o
r fai
lure
of e
quip
men
t
O
: O
ther
(ple
ase
spec
ify)
Who
:
Type
of H
ealth
Pro
fess
iona
l or c
arer
in
volv
ed (e
.g. G
P, H
ospi
tal M
idw
ife,
Obs
tetri
cian
, par
ents
). If
mor
e th
an
one
pers
on fo
r thi
s fa
ctor
, writ
e on
se
para
te li
nes.
No:
Diagn
osis and
scree
ning
issues
Plea
se re
fer t
o “G
uide
lines
for j
udgi
ng/g
radi
ng o
f cas
es fo
r rev
iew
” do
cum
ent
Sub-
optim
al
care
Rel
evan
ce o
f gr
ade
of c
are
to o
utco
me
Wha
t
Who
Gra
de o
f St
aff
Locu
m
Yes/
No
1.
2.
3.
4.

Perinatal Confidential Enquiry 2014 55
Case num
ber:
MBR
RACE
-‐UK 20
14 Perinatal Con
fidentia
l Enq
uiry– Co
ngenita
l Diaph
ragm
atic Hernia
(*Im
provem
ents in
care shou
ld be interpreted to in
clud
e ad
herence to guide
lines, w
here th
ese exist a
nd have no
t been follo
wed
, as w
ell a
s other im
provem
ents which
wou
ld normally be considered
part o
f goo
d care (see con
sensus docum
ent), w
here no form
al guide
lines exist.)
Sub-
optim
al c
are
O: N
o su
b-op
timal
car
e
1:
Min
or s
ubop
timal
car
e
2: S
igni
fican
t sub
optim
al c
are
3:
Maj
or s
ubop
timal
car
e
Rel
evan
ce o
f gra
de o
f car
e to
ou
tcom
e
O: N
ot re
leva
nt
1:
Pos
sibl
y re
leva
nt
2:
Pro
babl
y re
leva
nt
3: A
lmos
t cer
tain
ly re
leva
nt
Wha
t:
R:
Failu
re to
reco
gnis
e pr
oble
m
A:
Failu
re to
act
app
ropr
iate
ly
C
: C
omm
unic
atio
ns fa
ilure
S:
Fa
ilure
to s
uper
vise
H
: A
ny la
ck o
f hum
an re
sour
ce
E: A
ny la
ck o
r fai
lure
of e
quip
men
t
O
: O
ther
(ple
ase
spec
ify)
Who
:
Type
of H
ealth
Pro
fess
iona
l or c
arer
in
volv
ed (e
.g. G
P, H
ospi
tal M
idw
ife,
Obs
tetri
cian
, par
ents
). If
mor
e th
an o
ne
pers
on fo
r thi
s fa
ctor
, writ
e on
sep
arat
e lin
es.
No:
Delivery issues
Plea
se re
fer t
o “G
uide
lines
for j
udgi
ng/g
radi
ng o
f cas
es fo
r rev
iew
” do
cum
ent
Sub-
optim
al
care
Relevance
of
grad
e of
care to
ou
tcom
e
Wha
t Who
Grade
of
Staff
Locum
Yes/No
1.
2.
3.
4.
Perinatal Confidential Enquiry 201456
Case num
ber:
MBR
RACE
-‐UK 20
14 Perinatal Con
fidentia
l Enq
uiry– Co
ngenita
l Diaph
ragm
atic Hernia
(*Im
provem
ents in
care shou
ld be interpreted to includ
e ad
herence to guide
lines, w
here th
ese exist a
nd have no
t been follo
wed
, as w
ell a
s other im
provem
ents which
wou
ld normally be considered
part o
f goo
d care (see con
sensus docum
ent), w
here no form
al guide
lines exist.)
Sub-
optim
al c
are
O: N
o su
b-op
timal
car
e
1:
Min
or s
ubop
timal
car
e
2: S
igni
fican
t sub
optim
al c
are
3:
Maj
or s
ubop
timal
car
e
Rel
evan
ce o
f gra
de o
f car
e to
ou
tcom
e
O: N
ot re
leva
nt
1:
Pos
sibl
y re
leva
nt
2:
Pro
babl
y re
leva
nt
3: A
lmos
t cer
tain
ly re
leva
nt
Wha
t:
R:
Failu
re to
reco
gnis
e pr
oble
m
A:
Failu
re to
act
app
ropr
iate
ly
C
: C
omm
unic
atio
ns fa
ilure
S:
Fa
ilure
to s
uper
vise
H
: A
ny la
ck o
f hum
an re
sour
ce
E: A
ny la
ck o
r fai
lure
of e
quip
men
t
O
: O
ther
(ple
ase
spec
ify)
Who
:
Type
of H
ealth
Pro
fess
iona
l or c
arer
in
volv
ed (e
.g. G
P, H
ospi
tal M
idw
ife,
Obs
tetri
cian
, par
ents
). If
mor
e th
an o
ne
pers
on fo
r thi
s fa
ctor
, writ
e on
sep
arat
e lin
es.
No:
Re
suscitation
Plea
se re
fer t
o “G
uide
lines
for j
udgi
ng/g
radi
ng o
f cas
es fo
r rev
iew
” do
cum
ent
Sub-
optim
al
care
Rel
evan
ce o
f gr
ade
of c
are
to
outc
ome
Wha
t
Who
G
rade
of
Staf
f
Locu
m
Yes/
No
1.
2.
3.
4.

Perinatal Confidential Enquiry 2014 57
Case num
ber:
MBR
RACE
-‐UK 20
14 Perinatal Con
fidentia
l Enq
uiry– Co
ngenita
l Diaph
ragm
atic Hernia
(*Im
provem
ents in
care shou
ld be interpreted to in
clud
e ad
herence to guide
lines, w
here th
ese exist a
nd hav
e no
t been follo
wed, a
s well a
s other im
provem
ents which
wou
ld normally be considered
part o
f goo
d care (see con
sensus docum
ent), w
here no form
al guide
lines exist.)
Sub-
optim
al c
are
O: N
o su
b-op
timal
car
e
1:
Min
or s
ubop
timal
car
e
2: S
igni
fican
t sub
optim
al c
are
3:
Maj
or s
ubop
timal
car
e
Rel
evan
ce o
f gra
de o
f car
e to
ou
tcom
e
O: N
ot re
leva
nt
1:
Pos
sibl
y re
leva
nt
2:
Pro
babl
y re
leva
nt
3: A
lmos
t cer
tain
ly re
leva
nt
Wha
t:
R:
Failu
re to
reco
gnis
e pr
oble
m
A:
Failu
re to
act
app
ropr
iate
ly
C
: C
omm
unic
atio
ns fa
ilure
S:
Fa
ilure
to s
uper
vise
H
: A
ny la
ck o
f hum
an re
sour
ce
E: A
ny la
ck o
r fai
lure
of e
quip
men
t
O
: O
ther
(ple
ase
spec
ify)
Who
:
Type
of H
ealth
Pro
fess
iona
l or c
arer
in
volv
ed (e
.g. G
P, H
ospi
tal M
idw
ife,
Obs
tetri
cian
, par
ents
). If
mor
e th
an o
ne
pers
on fo
r thi
s fa
ctor
, writ
e on
sep
arat
e lin
es.
No:
Ea
rly aftercare (i.e. 24-‐48
hou
rs post-‐de
livery)
Plea
se re
fer t
o “G
uide
lines
for j
udgi
ng/g
radi
ng o
f cas
es fo
r rev
iew
” do
cum
ent
Sub-
optim
al
care
Rel
evan
ce o
f gr
ade
of c
are
to
outc
ome
Wha
t
Who
G
rade
of
Staf
f
Locu
m
Yes/
No
1.
2.
3.
4.

Perinatal Confidential Enquiry 201458
Case num
ber:
MBR
RACE
-‐UK 20
14 Perinatal Con
fidentia
l Enq
uiry– Co
ngenita
l Diaph
ragm
atic Hernia
(*Im
provem
ents in
care shou
ld be interpreted to in
clud
e ad
herence to guide
lines, w
here th
ese exist a
nd hav
e no
t been follo
wed, a
s well a
s other im
provem
ents which
wou
ld normally be considered
part o
f goo
d care (see con
sensus docum
ent), w
here no form
al guide
lines exist.)
Sub-
optim
al c
are
O: N
o su
b-op
timal
car
e
1:
Min
or s
ubop
timal
car
e
2: S
igni
fican
t sub
optim
al c
are
3:
Maj
or s
ubop
timal
car
e
Rel
evan
ce o
f gra
de o
f car
e to
ou
tcom
e
O: N
ot re
leva
nt
1:
Pos
sibl
y re
leva
nt
2:
Pro
babl
y re
leva
nt
3: A
lmos
t cer
tain
ly re
leva
nt
Wha
t:
R:
Failu
re to
reco
gnis
e pr
oble
m
A:
Failu
re to
act
app
ropr
iate
ly
C
: C
omm
unic
atio
ns fa
ilure
S:
Fa
ilure
to s
uper
vise
H
: A
ny la
ck o
f hum
an re
sour
ce
E: A
ny la
ck o
r fai
lure
of e
quip
men
t
O
: O
ther
(ple
ase
spec
ify)
Who
:
Type
of H
ealth
Pro
fess
iona
l or c
arer
in
volv
ed (e
.g. G
P, H
ospi
tal M
idw
ife,
Obs
tetri
cian
, par
ents
). If
mor
e th
an o
ne
pers
on fo
r thi
s fa
ctor
, writ
e on
sep
arat
e lin
es.
No:
Su
rgery an
d po
st-‐ope
rative
care
Plea
se re
fer t
o “G
uide
lines
for j
udgi
ng/g
radi
ng o
f cas
es fo
r rev
iew
” do
cum
ent
Sub-
optim
al
care
Rel
evan
ce o
f gr
ade
of c
are
to
outc
ome
Wha
t
Who
G
rade
of
Staf
f
Locu
m
Yes/
No
1.
2.
3.
4.

Perinatal Confidential Enquiry 2014 59
Case num
ber:
MBR
RACE
-‐UK 20
14 Perinatal Con
fidentia
l Enq
uiry– Co
ngenita
l Diaph
ragm
atic Hernia
(*Im
provem
ents in
care shou
ld be interpreted to in
clud
e ad
herence to guide
lines, w
here th
ese exist a
nd hav
e no
t been follo
wed, a
s well a
s other im
provem
ents which
wou
ld normally be considered
part o
f goo
d care (see con
sensus docum
ent), w
here no form
al guide
lines exist.)
Sub-
optim
al c
are
O: N
o su
b-op
timal
car
e
1:
Min
or s
ubop
timal
car
e
2: S
igni
fican
t sub
optim
al c
are
3:
Maj
or s
ubop
timal
car
e
Rel
evan
ce o
f gra
de o
f car
e to
ou
tcom
e
O: N
ot re
leva
nt
1:
Pos
sibl
y re
leva
nt
2:
Pro
babl
y re
leva
nt
3: A
lmos
t cer
tain
ly re
leva
nt
Wha
t:
R:
Failu
re to
reco
gnis
e pr
oble
m
A:
Failu
re to
act
app
ropr
iate
ly
C
: C
omm
unic
atio
ns fa
ilure
S:
Fa
ilure
to s
uper
vise
H
: A
ny la
ck o
f hum
an re
sour
ce
E: A
ny la
ck o
r fai
lure
of e
quip
men
t
O
: O
ther
(ple
ase
spec
ify)
Who
:
Type
of H
ealth
Pro
fess
iona
l or c
arer
in
volv
ed (e
.g. G
P, H
ospi
tal M
idw
ife,
Obs
tetri
cian
, par
ents
). If
mor
e th
an o
ne
pers
on fo
r thi
s fa
ctor
, writ
e on
sep
arat
e lin
es.
No:
Pa
lliative Ca
re Issues
Plea
se re
fer t
o “G
uide
lines
for j
udgi
ng/g
radi
ng o
f cas
es fo
r rev
iew
” do
cum
ent
Sub-
optim
al
care
Rel
evan
ce o
f gr
ade
of c
are
to
outc
ome
Wha
t
Who
G
rade
of
Staf
f
Locu
m
Yes/
No
1.
2.
3.
4.

Perinatal Confidential Enquiry 201460
Case num
ber:
MBR
RACE
-‐UK 20
14 Perinatal Con
fidentia
l Enq
uiry– Co
ngenita
l Diaph
ragm
atic Hernia
(*Im
provem
ents in
care shou
ld be interpreted to in
clud
e ad
herence to guide
lines, w
here th
ese exist a
nd hav
e no
t been follo
wed, a
s well a
s other im
provem
ents which
wou
ld normally be considered
part o
f goo
d care (see con
sensus docum
ent), w
here no form
al guide
lines exist.)
Sub-
optim
al c
are
O: N
o su
b-op
timal
car
e
1:
Min
or s
ubop
timal
car
e
2: S
igni
fican
t sub
optim
al c
are
3:
Maj
or s
ubop
timal
car
e
Rel
evan
ce o
f gra
de o
f car
e to
ou
tcom
e
O: N
ot re
leva
nt
1:
Pos
sibl
y re
leva
nt
2:
Pro
babl
y re
leva
nt
3: A
lmos
t cer
tain
ly re
leva
nt
Wha
t:
R:
Failu
re to
reco
gnis
e pr
oble
m
A:
Failu
re to
act
app
ropr
iate
ly
C
: C
omm
unic
atio
ns fa
ilure
S:
Fa
ilure
to s
uper
vise
H
: A
ny la
ck o
f hum
an re
sour
ce
E: A
ny la
ck o
r fai
lure
of e
quip
men
t
O
: O
ther
(ple
ase
spec
ify)
Who
:
Type
of H
ealth
Pro
fess
iona
l or c
arer
in
volv
ed (e
.g. G
P, H
ospi
tal M
idw
ife,
Obs
tetri
cian
, par
ents
). If
mor
e th
an o
ne
pers
on fo
r thi
s fa
ctor
, writ
e on
sep
arat
e lin
es.
No:
Lo
ng te
rm outcome
Plea
se re
fer t
o “G
uide
lines
for j
udgi
ng/g
radi
ng o
f cas
es fo
r rev
iew
” do
cum
ent
Sub-
optim
al
care
Rel
evan
ce o
f gr
ade
of c
are
to
outc
ome
Wha
t
Who
G
rade
of
Staf
f
Locu
m
Yes/
No
1.
2.
3.
4.

Perinatal Confidential Enquiry 2014 61
Case Eva
luation Fo
rm
MB
RR
AC
E-U
K 2
014
Per
inat
al C
onfid
entia
l Enq
uiry
– C
onge
nita
l Dia
phra
gmat
ic H
erni
a
Cas
e nu
mbe
r:
Ove
rall Gr
ade
Gra
de o
f car
e
1: G
ood
care
; no
impr
ovem
ents
iden
tifie
d
2: Im
prov
emen
ts in
car
e* id
entif
ied
whi
ch w
ould
hav
e m
ade
no d
iffer
ence
to o
utco
me
3: I
mpr
ovem
ents
in c
are*
iden
tifie
d w
hich
may
hav
e m
ade
a di
ffere
nce
to o
utco
me
Sum
mar
y co
mm
ents
:

MBRRACE-UK
Department of Health Sciences University of Leicester 22-28 Princess Road West Leicester, LE1 6TP
Tel: +44-116 252 5425
Email: [email protected]
Web: www.npeu.ox.ac.uk/mbrrace-uk