Embed Size (px)
Citation preview

Performance of strabismic subjects using a validatedsurgical training module: A pilot studyGerard P. Barry, MD,a John W. Simon, MD,a David Auringer,b Ward Dunnican, MD,c andJitka Zobal-Ratner, MDa
PURPOSE To compare the performance of patients with strabismus to that of age-matched controls in
Author affiliations: aDepartmenYork; bAlbany Medical College,Medical College, Albany, New Y
Presented at the 35th AnnualOphthalmology and Strabismus,
Financial support: There is noThis study was conducted at thSubmitted October 7, 2008.Revision accepted May 2, 200Reprint requests: John W. Sim
Ophthalmology, Albany Medical(email: [email protected]).
Copyright � 2009 by the AmStrabismus.
1091-8531/2009/$36.00 1
doi:10.1016/j.jaapos.2009.05
350
a validated surgical training module.
METHODS A prospective experimental study was conducted of 14 adult patients with strabismus since
childhood and absent stereopsis and of 14 age-matched controls with normal stereopsis.Each participant received instruction in the task of peg transfer on a validated surgicaltraining device and then completed 10 consecutive timed trials. The means of the best 5scores were compared using the 2-sample Wilcoxon rank-sum test.RESULTS The average age of cases was 34.8 years (range, 15-51 years) compared with 37.8 years
(range, 14-56 years) for controls. The scores for the strabismic patients ranged from50.8 to 151.4 seconds, with a mean of 82.5 � 26.7 seconds. Controls ranged from 43.2to 129 seconds, with a mean of 64.7 � 23.9 seconds. The Wilcoxon rank-sum test showedsignificantly better performance among controls (p 5 0.022).CONCLUSIONS Patients with strabismus performed more poorly than did age-matched controls in this
model of hand-eye coordination. However, there was significant overlap between groupsand several patients with strabismus performed better than the mean of the control group.Further investigation is required to elucidate the impact of strabismus on surgical perform-ance. ( J AAPOS 2009;13:350-353)Childhood strabismus affects approximately 3% ofthe population.1-3 Patients with constant devia-tions typically have poor stereopsis. Even after
surgery to improve their ocular alignment, tests of binocu-larity, including stereopsis and Worth 4-Dot fusion, oftenshow that they continue to function monocularly.4-9
Similarly, people with poor vision in one eye typicallylack stereopsis.
We have often wondered whether people without stere-opsis can become effective surgeons. Anecdotal reportssuggest they indeed can,10 but very little has been pub-lished comparing the performance of people with and with-out stereopsis on fine-motor tasks.11 We undertook sucha comparison using a validated surgical training module.
t of Ophthalmology, Albany Medical College, Albany, NewAlbany, New York; and cDepartment of Surgery, AlbanyorkMeeting of the American Association for PediatricSan Francisco, California, April 17-21, 2009.financial conflict of interest to report.e Albany Medical Center in Albany, New York.
9.on, MD, Professor and Chair, Department of
College, 1220 New Scotland Rd., Slingerlands, NY 12159
erican Association for Pediatric Ophthalmology and
0.002
Subjects and Methods
This study, which was approved by the Albany Medical Center
Institutional Review Board, conformed to the requirements of the
U.S. Health Insurance Portability and Accountability Act.
Informed consent was obtained for all participants. Fourteen adult
patients with strabismus (cases) were recruited from our practices.
An equal number of age-matched controls were recruited from their
families and from the community. All patients with strabismus had
undergone eye muscle surgery in childhood and all but one had
a repeat procedure in adulthood. None had measurable stereopsis
using Randot circles (Stereo Optical Co., Inc., Chicago, IL), and
all had Worth-4 Dot (Reichert Ophthalmic; Leica Inc., Buffalo,
NY) suppression at distance and near. Their clinical findings are
summarized in (e-Supplement 1, available at jaapos.org). All normal
controls had 20/30 or better visual acuity in each eye, normal ocular
motility and alignment, and at least 60 arcsec of stereopsis. Their
clinical findings are summarized in (e-Supplement 2, available at
jaapos.org). No participant had any previous medical or surgical
training.
The device (Figure 1; USSC Laptrainer; U.S. Surgical Corpo-
ration, Norwalk, CT) and validated training task we used have
been described elsewhere.12 In brief, a laparoscopic trainer box
with 2 sets of 6 pegs on a board includes 2 trocars with grasping
instruments, which can be used to transfer disks from one peg
to another. Subjects were instructed to grasp each disk from the
first set using the left-handed instrument, to transfer it to the right
hand, and then to place it onto the corresponding peg from the
second set. The process was then repeated until all 6 disks were
transferred, and was then reversed. Subjects were first given
Journal of AAPOS
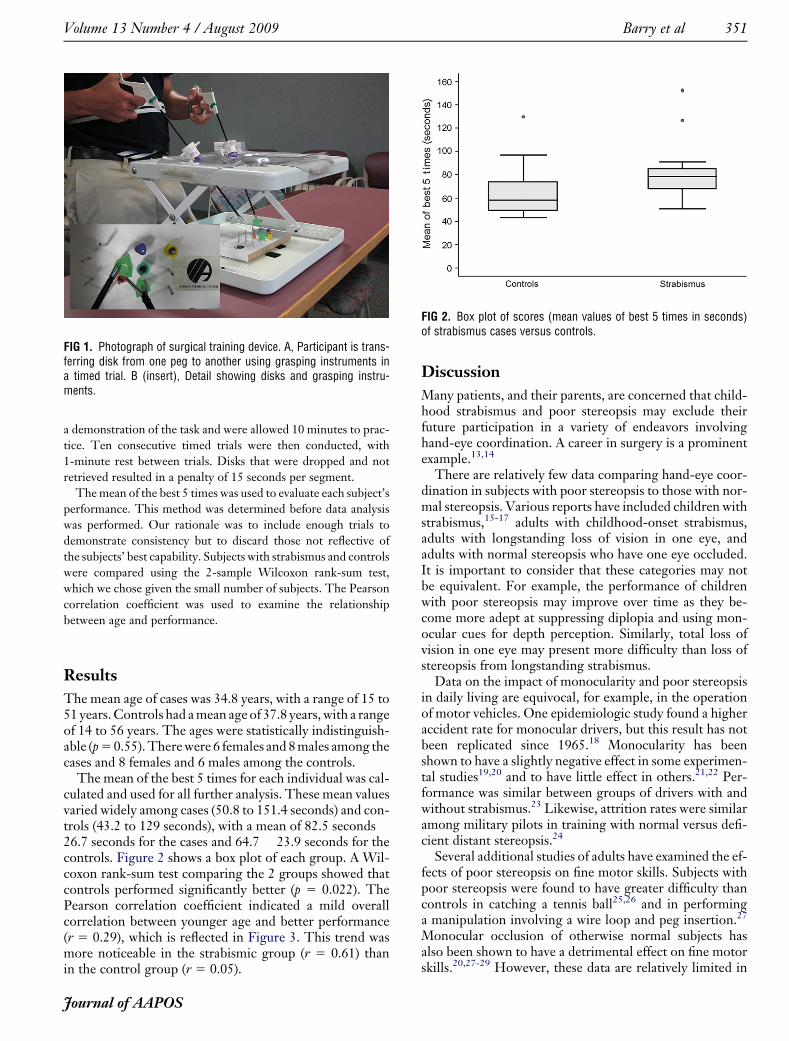
FIG 1. Photograph of surgical training device. A, Participant is trans-ferring disk from one peg to another using grasping instruments ina timed trial. B (insert), Detail showing disks and grasping instru-ments.
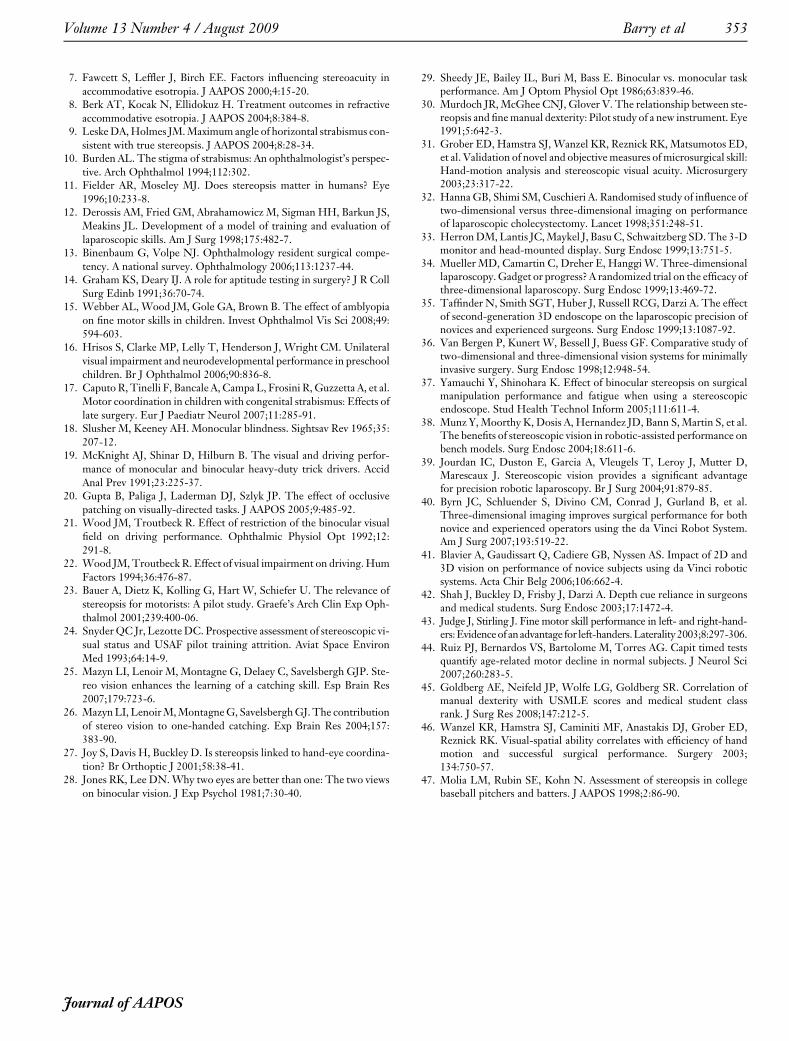
FIG 2. Box plot of scores (mean values of best 5 times in seconds)of strabismus cases versus controls.
Volume 13 Number 4 / August 2009 Barry et al 351
a demonstration of the task and were allowed 10 minutes to prac-
tice. Ten consecutive timed trials were then conducted, with
1-minute rest between trials. Disks that were dropped and not
retrieved resulted in a penalty of 15 seconds per segment.
The mean of the best 5 times was used to evaluate each subject’s
performance. This method was determined before data analysis
was performed. Our rationale was to include enough trials to
demonstrate consistency but to discard those not reflective of
the subjects’ best capability. Subjects with strabismus and controls
were compared using the 2-sample Wilcoxon rank-sum test,
which we chose given the small number of subjects. The Pearson
correlation coefficient was used to examine the relationship
between age and performance.
Results
The mean age of cases was 34.8 years, with a range of 15 to51 years. Controls had a mean age of 37.8 years, with a rangeof 14 to 56 years. The ages were statistically indistinguish-able (p 5 0.55). There were 6 females and 8 males among thecases and 8 females and 6 males among the controls.
The mean of the best 5 times for each individual was cal-culated and used for all further analysis. These mean valuesvaried widely among cases (50.8 to 151.4 seconds) and con-trols (43.2 to 129 seconds), with a mean of 82.5 seconds �26.7 seconds for the cases and 64.7 � 23.9 seconds for thecontrols. Figure 2 shows a box plot of each group. A Wil-coxon rank-sum test comparing the 2 groups showed thatcontrols performed significantly better (p 5 0.022). ThePearson correlation coefficient indicated a mild overallcorrelation between younger age and better performance(r 5 0.29), which is reflected in Figure 3. This trend wasmore noticeable in the strabismic group (r 5 0.61) thanin the control group (r 5 0.05).
Journal of AAPOS
Discussion
Many patients, and their parents, are concerned that child-hood strabismus and poor stereopsis may exclude theirfuture participation in a variety of endeavors involvinghand-eye coordination. A career in surgery is a prominentexample.13,14
There are relatively few data comparing hand-eye coor-dination in subjects with poor stereopsis to those with nor-mal stereopsis. Various reports have included children withstrabismus,15-17 adults with childhood-onset strabismus,adults with longstanding loss of vision in one eye, andadults with normal stereopsis who have one eye occluded.It is important to consider that these categories may notbe equivalent. For example, the performance of childrenwith poor stereopsis may improve over time as they be-come more adept at suppressing diplopia and using mon-ocular cues for depth perception. Similarly, total loss ofvision in one eye may present more difficulty than loss ofstereopsis from longstanding strabismus.
Data on the impact of monocularity and poor stereopsisin daily living are equivocal, for example, in the operationof motor vehicles. One epidemiologic study found a higheraccident rate for monocular drivers, but this result has notbeen replicated since 1965.18 Monocularity has beenshown to have a slightly negative effect in some experimen-tal studies19,20 and to have little effect in others.21,22 Per-formance was similar between groups of drivers with andwithout strabismus.23 Likewise, attrition rates were similaramong military pilots in training with normal versus defi-cient distant stereopsis.24
Several additional studies of adults have examined the ef-fects of poor stereopsis on fine motor skills. Subjects withpoor stereopsis were found to have greater difficulty thancontrols in catching a tennis ball25,26 and in performinga manipulation involving a wire loop and peg insertion.27
Monocular occlusion of otherwise normal subjects hasalso been shown to have a detrimental effect on fine motorskills.20,27-29 However, these data are relatively limited in

FIG 3. Linear plot of age versus score (mean values of best 5 times inseconds), showing moderate correlation among strabismus cases andvery little correlation among controls.
352 Barry et al Volume 13 Number 4 / August 2009
scope and conclusions drawn regarding the functional im-pairment caused by decreased stereopsis have varied.
Two studies have examined the relationship betweenstereopsis and surgical performance in adults. In a letterto the editor in 1991, Murdoch and colleagues30 describeda new instrument to assess fine manual dexterity. Theytested several groups, including adult subjects with normal,reduced, and absent stereopsis. Compared with controls,the group with absent stereopsis performed more poorly,whereas the group with reduced stereopsis performed sim-ilarly, but with wider variation in scores. Grober and col-leagues31 found no correlation between microsurgicalperformance and stereoacutiy, measured with a nonstan-dard technique. Individual stereoacuity measurementswere not given and all subjects were surgical residentswith apparently normal vision.
Our results indicate that strabismus patients with mini-mal or absent stereopsis indeed did perform more poorlythan normal controls. However, there was substantial over-lap between the 2 groups, and more variation was notedwithin each group than between the 2 groups. It is note-worthy that several of the subjects with strabismus werequite adept at performing the task and had scores consider-ably better than the mean of the normal controls.
We acknowledge that there are limitations inherent in thissmall, pilot study. We considered only patients with child-hood-onset strabismus who had no stereopsis. We did notstudy patients with partial binocularity, such as monofixa-tion syndrome, who might have performed better.30 Wechose to study a simple surgical training module, ratherthan a computerized microsurgical simulator, because ithas been well validated in previous studies and because it isbased on a truly 3-dimensional surgical task applicable tosurgery in general.12 The effect of stereopsis on other surgi-cal training models may differ.32-41 Also, we did not examinethe learning curve in patients with strabismus. Perhaps pa-tients with strabismus could achieve scores similar to normalsubjects after an appropriate learning period.
Surgeons in different fields may be affected differently bylack of stereopsis. Surgeons adept at endoscopic proce-dures, performed monocularly, have shown greater adapta-tion to a nonstereoscopic environment than medicalstudent controls.42 Ophthalmology, on the other hand, isunusual among surgical fields in that stereopsis may bebeneficial in the clinical examination. Assessing cup/diskratio and retinal elevation might be more difficult fortrainees with poor stereopsis.
Stereopsis is only one of many factors involved in hand-eye coordination. Studies have correlated dexterity withleft-handedness, age, medical student class rank, U.S.Medical License Examination scores, and tests of ‘‘visual-spatial ability’’ that do not actually involve stereopsis.43-46
Experience has frequently been found to represent themost important factor.35,46
A variety of anecdotal reports suggests that individualswith strabismus or poor binocularity can still excel at visu-ally demanding tasks. Babe Ruth is widely believed to havebeen blind in one eye from anisometropic amblyopia(plano right eye, 16.00 sphere left eye).47 Wesley Walker,a former all-pro National Football League wide receiver,was also blind in one eye.47
Despite the statistical difference between patients withstrabismus and controls, our experience suggests thatsome individuals with poor stereopsis are able to performquite well on a specific surgical task. Further investigationis warranted to further elucidate the practical impact ofstrabismus on surgical performance.
Literature Search
A MEDLINE search of the literature was performed usingthe terms binocularity OR stereopsis AND dexterity OR finemotor. A total of 1,810 items were reviewed. All articles ofinterest were available in English.
Acknowledgments
We thank Ashar Ata for his help with statistical analysis and the SightSociety of Northeastern New York for their financial support.
References
1. The Multi-ethnic Pediatric Eye Disease Study Group. Prevalence ofamblyopia and strabismus in African American and Hispanic childrenages 6 to 72 months. The Multi-ethnic Pediatric Eye Disease Study.Ophthalmology 2008;115:1229-36.
2. Govindan BA, Mohney BG, Diehl NN, Burke JP. Incidence and typesof childhood exotropia: A population-based study. Ophthalmology2005;112:104-8.
3. Greenberg AE, Mohney BG, Diehl NN, Burke JP. Incidence andtypes of childhood esotropia: A population-based study. Ophthalmol-ogy 2007;114:170-74.
4. Birch EE, Stager DR Sr. Long-term motor and sensory outcomes af-ter early surgery for infantile esotropia. J AAPOS 2006;10:409-13.
5. Saunders RA, Trivedi RH. Sensory results after lateral rectus musclerecession for intermittent exotropia operated before two years of age.J AAPOS 2008;12:132-5.
6. Uretmen O, Kose S, Oztas Z, Egrilmez S. Factors influencing ster-eoacuity in refractive accommodative esotropia. Can J Ophthalmol2007;42:600-04.
Journal of AAPOS
Volume 13 Number 4 / August 2009 Barry et al 353
7. Fawcett S, Leffler J, Birch EE. Factors influencing stereoacuity inaccommodative esotropia. J AAPOS 2000;4:15-20.
8. Berk AT, Kocak N, Ellidokuz H. Treatment outcomes in refractiveaccommodative esotropia. J AAPOS 2004;8:384-8.
9. Leske DA, Holmes JM. Maximum angle of horizontal strabismus con-sistent with true stereopsis. J AAPOS 2004;8:28-34.
10. Burden AL. The stigma of strabismus: An ophthalmologist’s perspec-tive. Arch Ophthalmol 1994;112:302.
11. Fielder AR, Moseley MJ. Does stereopsis matter in humans? Eye1996;10:233-8.
12. Derossis AM, Fried GM, Abrahamowicz M, Sigman HH, Barkun JS,Meakins JL. Development of a model of training and evaluation oflaparoscopic skills. Am J Surg 1998;175:482-7.
13. Binenbaum G, Volpe NJ. Ophthalmology resident surgical compe-tency. A national survey. Ophthalmology 2006;113:1237-44.
14. Graham KS, Deary IJ. A role for aptitude testing in surgery? J R CollSurg Edinb 1991;36:70-74.
15. Webber AL, Wood JM, Gole GA, Brown B. The effect of amblyopiaon fine motor skills in children. Invest Ophthalmol Vis Sci 2008;49:594-603.
16. Hrisos S, Clarke MP, Lelly T, Henderson J, Wright CM. Unilateralvisual impairment and neurodevelopmental performance in preschoolchildren. Br J Ophthalmol 2006;90:836-8.
17. Caputo R, Tinelli F, Bancale A, Campa L, Frosini R, Guzzetta A, et al.Motor coordination in children with congenital strabismus: Effects oflate surgery. Eur J Paediatr Neurol 2007;11:285-91.
18. Slusher M, Keeney AH. Monocular blindness. Sightsav Rev 1965;35:207-12.
19. McKnight AJ, Shinar D, Hilburn B. The visual and driving perfor-mance of monocular and binocular heavy-duty trick drivers. AccidAnal Prev 1991;23:225-37.
20. Gupta B, Paliga J, Laderman DJ, Szlyk JP. The effect of occlusivepatching on visually-directed tasks. J AAPOS 2005;9:485-92.
21. Wood JM, Troutbeck R. Effect of restriction of the binocular visualfield on driving performance. Ophthalmic Physiol Opt 1992;12:291-8.
22. Wood JM, Troutbeck R. Effect of visual impairment on driving. HumFactors 1994;36:476-87.
23. Bauer A, Dietz K, Kolling G, Hart W, Schiefer U. The relevance ofstereopsis for motorists: A pilot study. Graefe’s Arch Clin Exp Oph-thalmol 2001;239:400-06.
24. Snyder QC Jr, Lezotte DC. Prospective assessment of stereoscopic vi-sual status and USAF pilot training attrition. Aviat Space EnvironMed 1993;64:14-9.
25. Mazyn LI, Lenoir M, Montagne G, Delaey C, Savelsbergh GJP. Ste-reo vision enhances the learning of a catching skill. Esp Brain Res2007;179:723-6.
26. Mazyn LI, Lenoir M, Montagne G, Savelsbergh GJ. The contributionof stereo vision to one-handed catching. Exp Brain Res 2004;157:383-90.
27. Joy S, Davis H, Buckley D. Is stereopsis linked to hand-eye coordina-tion? Br Orthoptic J 2001;58:38-41.
28. Jones RK, Lee DN. Why two eyes are better than one: The two viewson binocular vision. J Exp Psychol 1981;7:30-40.
Journal of AAPOS
29. Sheedy JE, Bailey IL, Buri M, Bass E. Binocular vs. monocular taskperformance. Am J Optom Physiol Opt 1986;63:839-46.
30. Murdoch JR, McGhee CNJ, Glover V. The relationship between ste-reopsis and fine manual dexterity: Pilot study of a new instrument. Eye1991;5:642-3.
31. Grober ED, Hamstra SJ, Wanzel KR, Reznick RK, Matsumotos ED,et al. Validation of novel and objective measures of microsurgical skill:Hand-motion analysis and stereoscopic visual acuity. Microsurgery2003;23:317-22.
32. Hanna GB, Shimi SM, Cuschieri A. Randomised study of influence oftwo-dimensional versus three-dimensional imaging on performanceof laparoscopic cholecystectomy. Lancet 1998;351:248-51.
33. Herron DM, Lantis JC, Maykel J, Basu C, Schwaitzberg SD. The 3-Dmonitor and head-mounted display. Surg Endosc 1999;13:751-5.
34. Mueller MD, Camartin C, Dreher E, Hanggi W. Three-dimensionallaparoscopy. Gadget or progress? A randomized trial on the efficacy ofthree-dimensional laparoscopy. Surg Endosc 1999;13:469-72.
35. Taffinder N, Smith SGT, Huber J, Russell RCG, Darzi A. The effectof second-generation 3D endoscope on the laparoscopic precision ofnovices and experienced surgeons. Surg Endosc 1999;13:1087-92.
36. Van Bergen P, Kunert W, Bessell J, Buess GF. Comparative study oftwo-dimensional and three-dimensional vision systems for minimallyinvasive surgery. Surg Endosc 1998;12:948-54.
37. Yamauchi Y, Shinohara K. Effect of binocular stereopsis on surgicalmanipulation performance and fatigue when using a stereoscopicendoscope. Stud Health Technol Inform 2005;111:611-4.
38. Munz Y, Moorthy K, Dosis A, Hernandez JD, Bann S, Martin S, et al.The benefits of stereoscopic vision in robotic-assisted performance onbench models. Surg Endosc 2004;18:611-6.
39. Jourdan IC, Duston E, Garcia A, Vleugels T, Leroy J, Mutter D,Marescaux J. Stereoscopic vision provides a significant advantagefor precision robotic laparoscopy. Br J Surg 2004;91:879-85.
40. Byrn JC, Schluender S, Divino CM, Conrad J, Gurland B, et al.Three-dimensional imaging improves surgical performance for bothnovice and experienced operators using the da Vinci Robot System.Am J Surg 2007;193:519-22.
41. Blavier A, Gaudissart Q, Cadiere GB, Nyssen AS. Impact of 2D and3D vision on performance of novice subjects using da Vinci roboticsystems. Acta Chir Belg 2006;106:662-4.
42. Shah J, Buckley D, Frisby J, Darzi A. Depth cue reliance in surgeonsand medical students. Surg Endosc 2003;17:1472-4.
43. Judge J, Stirling J. Fine motor skill performance in left- and right-hand-ers: Evidence of an advantage for left-handers. Laterality 2003;8:297-306.
44. Ruiz PJ, Bernardos VS, Bartolome M, Torres AG. Capit timed testsquantify age-related motor decline in normal subjects. J Neurol Sci2007;260:283-5.
45. Goldberg AE, Neifeld JP, Wolfe LG, Goldberg SR. Correlation ofmanual dexterity with USMLE scores and medical student classrank. J Surg Res 2008;147:212-5.
46. Wanzel KR, Hamstra SJ, Caminiti MF, Anastakis DJ, Grober ED,Reznick RK. Visual-spatial ability correlates with efficiency of handmotion and successful surgical performance. Surgery 2003;134:750-57.
47. Molia LM, Rubin SE, Kohn N. Assessment of stereopsis in collegebaseball pitchers and batters. J AAPOS 1998;2:86-90.
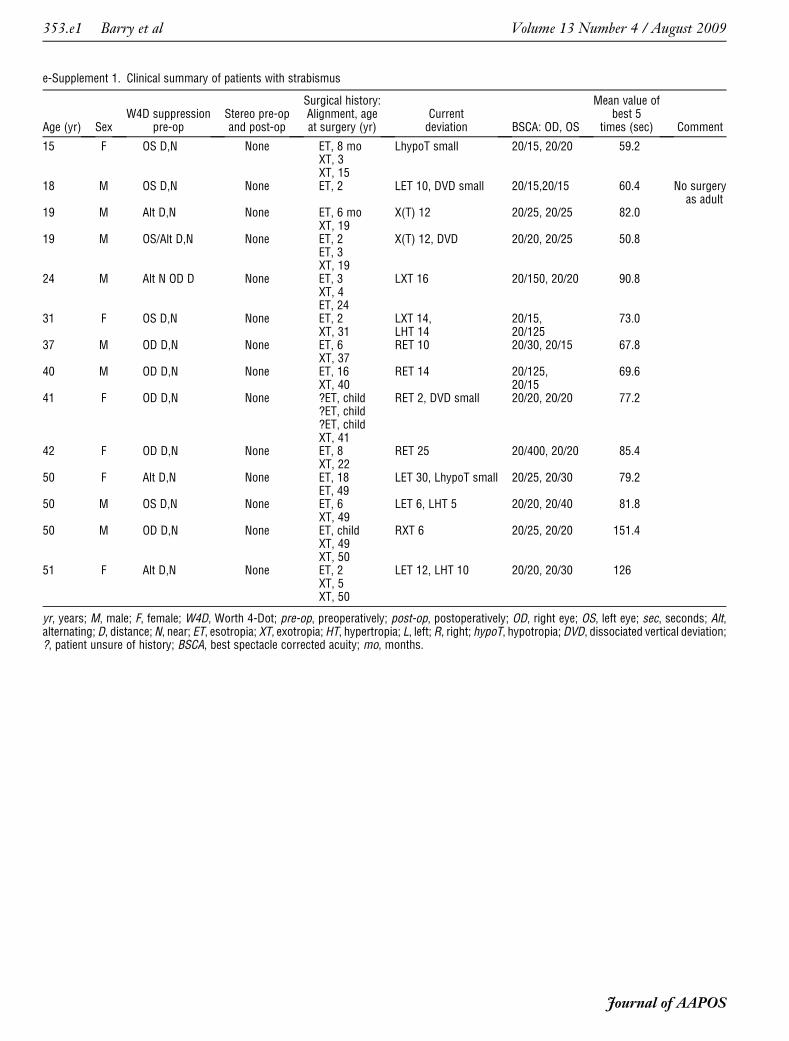
e-Supplement 1. Clinical summary of patients with strabismus
Age (yr) SexW4D suppression
pre-opStereo pre-opand post-op
Surgical history:Alignment, ageat surgery (yr)
Currentdeviation BSCA: OD, OS
Mean value ofbest 5
times (sec) Comment
15 F OS D,N None ET, 8 mo LhypoT small 20/15, 20/20 59.2XT, 3XT, 15
18 M OS D,N None ET, 2 LET 10, DVD small 20/15,20/15 60.4 No surgeryas adult
19 M Alt D,N None ET, 6 mo X(T) 12 20/25, 20/25 82.0XT, 19
19 M OS/Alt D,N None ET, 2 X(T) 12, DVD 20/20, 20/25 50.8ET, 3XT, 19
24 M Alt N OD D None ET, 3 LXT 16 20/150, 20/20 90.8XT, 4ET, 24
31 F OS D,N None ET, 2 LXT 14, 20/15, 73.0XT, 31 LHT 14 20/125
37 M OD D,N None ET, 6 RET 10 20/30, 20/15 67.8XT, 37
40 M OD D,N None ET, 16 RET 14 20/125, 69.6XT, 40 20/15
41 F OD D,N None ?ET, child RET 2, DVD small 20/20, 20/20 77.2?ET, child?ET, childXT, 41
42 F OD D,N None ET, 8 RET 25 20/400, 20/20 85.4XT, 22
50 F Alt D,N None ET, 18 LET 30, LhypoT small 20/25, 20/30 79.2ET, 49
50 M OS D,N None ET, 6 LET 6, LHT 5 20/20, 20/40 81.8XT, 49
50 M OD D,N None ET, child RXT 6 20/25, 20/20 151.4XT, 49XT, 50
51 F Alt D,N None ET, 2 LET 12, LHT 10 20/20, 20/30 126XT, 5XT, 50
yr, years; M, male; F, female; W4D, Worth 4-Dot; pre-op, preoperatively; post-op, postoperatively; OD, right eye; OS, left eye; sec, seconds; Alt,alternating; D, distance; N, near; ET, esotropia; XT, exotropia; HT, hypertropia; L, left; R, right; hypoT, hypotropia; DVD, dissociated vertical deviation;?, patient unsure of history; BSCA, best spectacle corrected acuity; mo, months.
Journal of AAPOS
353.e1 Barry et al Volume 13 Number 4 / August 2009
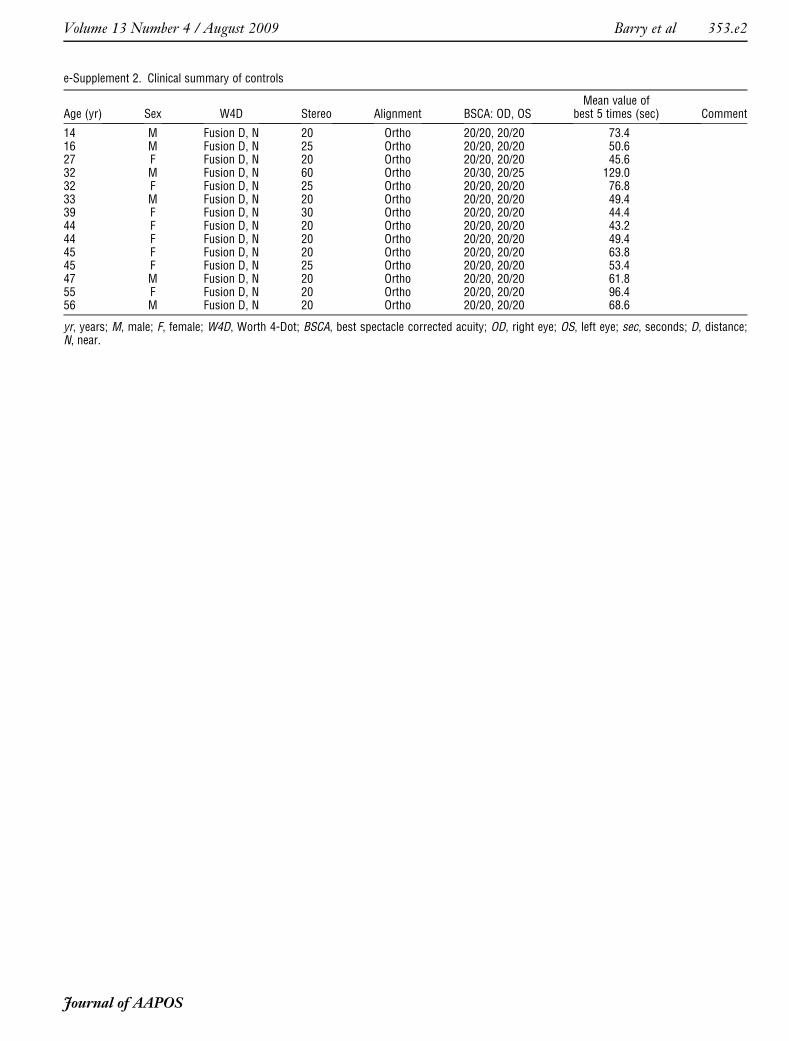
e-Supplement 2. Clinical summary of controls
Age (yr) Sex W4D Stereo Alignment BSCA: OD, OSMean value of
best 5 times (sec) Comment
14 M Fusion D, N 20 Ortho 20/20, 20/20 73.416 M Fusion D, N 25 Ortho 20/20, 20/20 50.627 F Fusion D, N 20 Ortho 20/20, 20/20 45.632 M Fusion D, N 60 Ortho 20/30, 20/25 129.032 F Fusion D, N 25 Ortho 20/20, 20/20 76.833 M Fusion D, N 20 Ortho 20/20, 20/20 49.439 F Fusion D, N 30 Ortho 20/20, 20/20 44.444 F Fusion D, N 20 Ortho 20/20, 20/20 43.244 F Fusion D, N 20 Ortho 20/20, 20/20 49.445 F Fusion D, N 20 Ortho 20/20, 20/20 63.845 F Fusion D, N 25 Ortho 20/20, 20/20 53.447 M Fusion D, N 20 Ortho 20/20, 20/20 61.855 F Fusion D, N 20 Ortho 20/20, 20/20 96.456 M Fusion D, N 20 Ortho 20/20, 20/20 68.6
yr, years; M, male; F, female; W4D, Worth 4-Dot; BSCA, best spectacle corrected acuity; OD, right eye; OS, left eye; sec, seconds; D, distance;N, near.
Journal of AAPOS
Volume 13 Number 4 / August 2009 Barry et al 353.e2





























