Embed Size (px)
DESCRIPTION
pendarahan
Citation preview
Perdarahan ObstetrikPerdarahan Obstetrik
Dwi NurrianaDwi Nurriana
INTRODUCTIONINTRODUCTION
OBSTERICS IS “ OBSTERICS IS “ BLOODY BUSINESSBLOODY BUSINESS”” US : 17% DIRECT CAUSE OF MATERNAL US : 17% DIRECT CAUSE OF MATERNAL
DEATHSDEATHS UK: MAJOR FACTOR FOR MATERNAL DEATHSUK: MAJOR FACTOR FOR MATERNAL DEATHS DEVELOPING COUNTRIES : ALMOST HALF OF DEVELOPING COUNTRIES : ALMOST HALF OF
POSTPARTUM DEATHS.POSTPARTUM DEATHS.
CAUSES AND PREDISPOSING CAUSES AND PREDISPOSING FACTORSFACTORS
ABNORMAL PLACENTATIONABNORMAL PLACENTATION TRAUMA DURING LABOUR AND DELIVERYTRAUMA DURING LABOUR AND DELIVERY SMALL MATERNAL BLOOD VOLUMESMALL MATERNAL BLOOD VOLUME UTERINE ATONYUTERINE ATONY COAGULATION DEFECTS- INTENSIFY OTHER COAGULATION DEFECTS- INTENSIFY OTHER
CAUSESCAUSES OTHER FACTORSOTHER FACTORS
ANTEPARTUMANTEPARTUM POSTPARTUMPOSTPARTUM
TRIMESTER 1TRIMESTER 1 TRIMESTER 2TRIMESTER 2 TRIMESTER 3TRIMESTER 3 POSTPARTUMPOSTPARTUM
TRIMESTER 1TRIMESTER 1
THREATENED ABORTIONTHREATENED ABORTION HYDATIDIFORM MOLEHYDATIDIFORM MOLE BLIGHTED OVUMBLIGHTED OVUM DEATH CONCEPTUSDEATH CONCEPTUS ECTOPIC PREGNANCYECTOPIC PREGNANCY
TRIMESTER 2TRIMESTER 2
THREATENED ABORTIONTHREATENED ABORTION ECTOPIC PREGNANCYECTOPIC PREGNANCY DEATH CONCEPTUSDEATH CONCEPTUS
TRIMESTER 3TRIMESTER 3
PLACENTA PREVIAPLACENTA PREVIA PLACENTAL ABRUPTIONPLACENTAL ABRUPTION VASA PREVIAVASA PREVIA UTERINE RUPTUREUTERINE RUPTURE
POSTPARTUMPOSTPARTUM
UTERINE ATONYUTERINE ATONY REST OF PLACENTAEREST OF PLACENTAE LACERATIONLACERATION COAGULOPATHYCOAGULOPATHY UTERINE INVERSIONUTERINE INVERSION UTERINE RUPTUREUTERINE RUPTURE

ObjectivesObjectives– DefinitionDefinition
– EtiologyEtiology
– Risk FactorsRisk Factors
– PreventionPrevention
– ManagementManagement
Postpartum Hemorrhage

PPH on bed and floor 2000ml
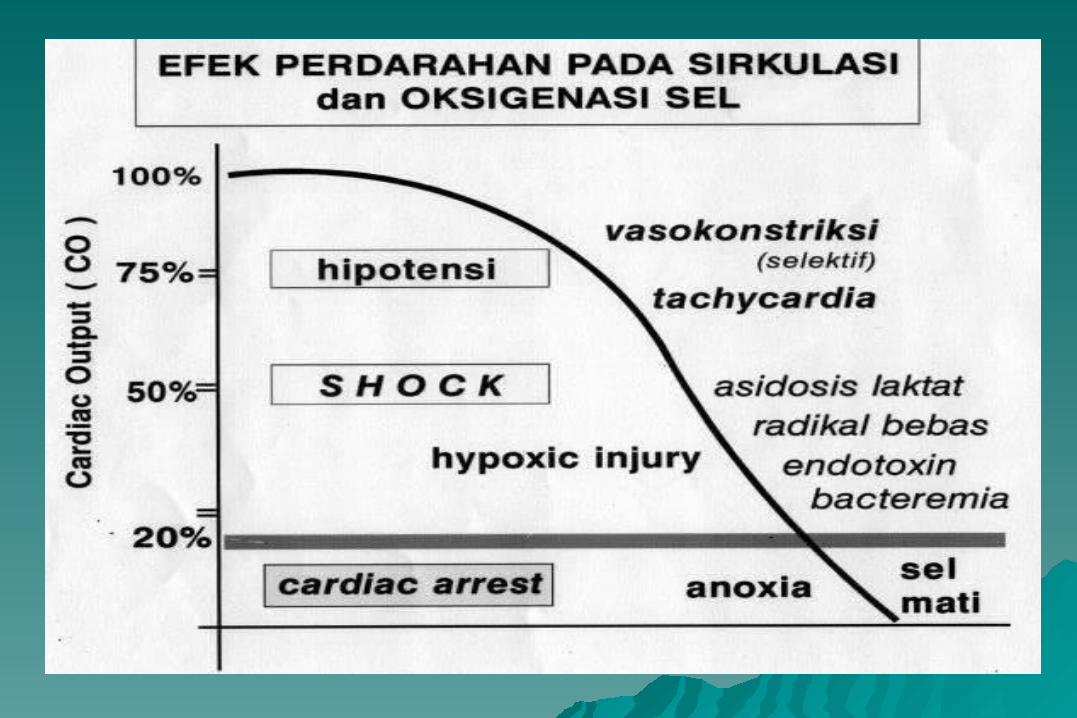
-70%
-60%
-50%
-40%
-30%
-20%
-10%
0%
10%
20%
anaesthetist obstetrician gynae nurse midwife theatre nurse HCA

PPH on bed only 1000ml
-30%
-20%
-10%
0%
10%
20%
30%
40%
anaesthetist obstetrician gynae nurse midwife theatre nurse HCA
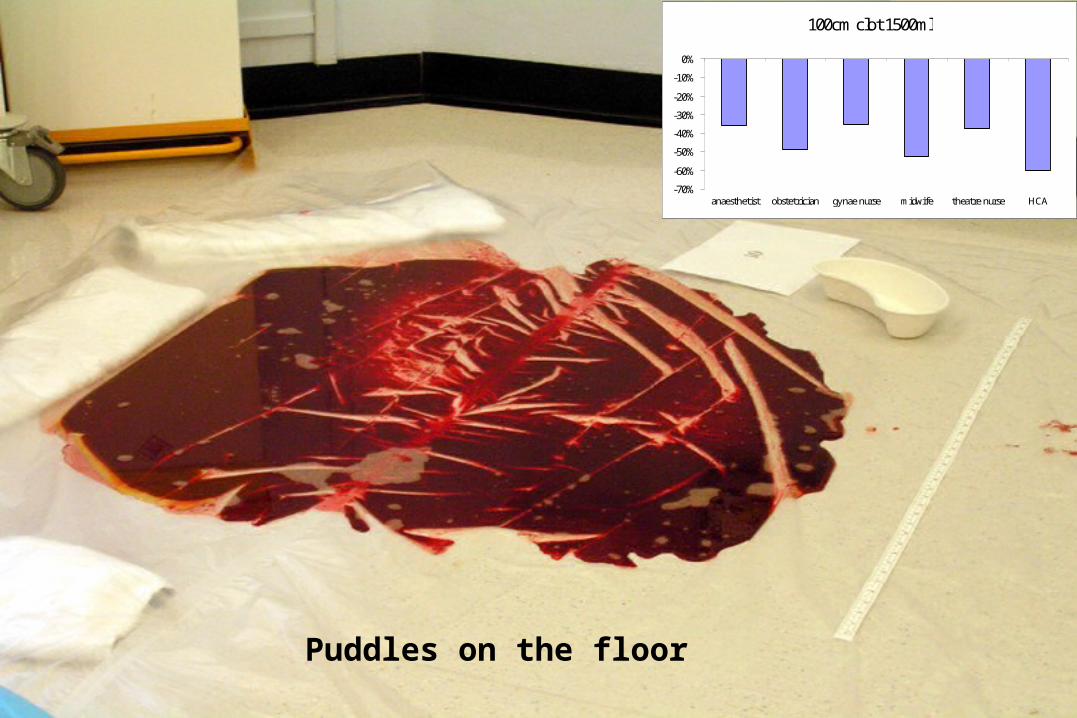
100cm clot 1500ml
-70%
-60%
-50%
-40%
-30%
-20%
-10%
0%
anaesthetist obstetrician gynae nurse midwife theatre nurse HCA
Puddles on the floor
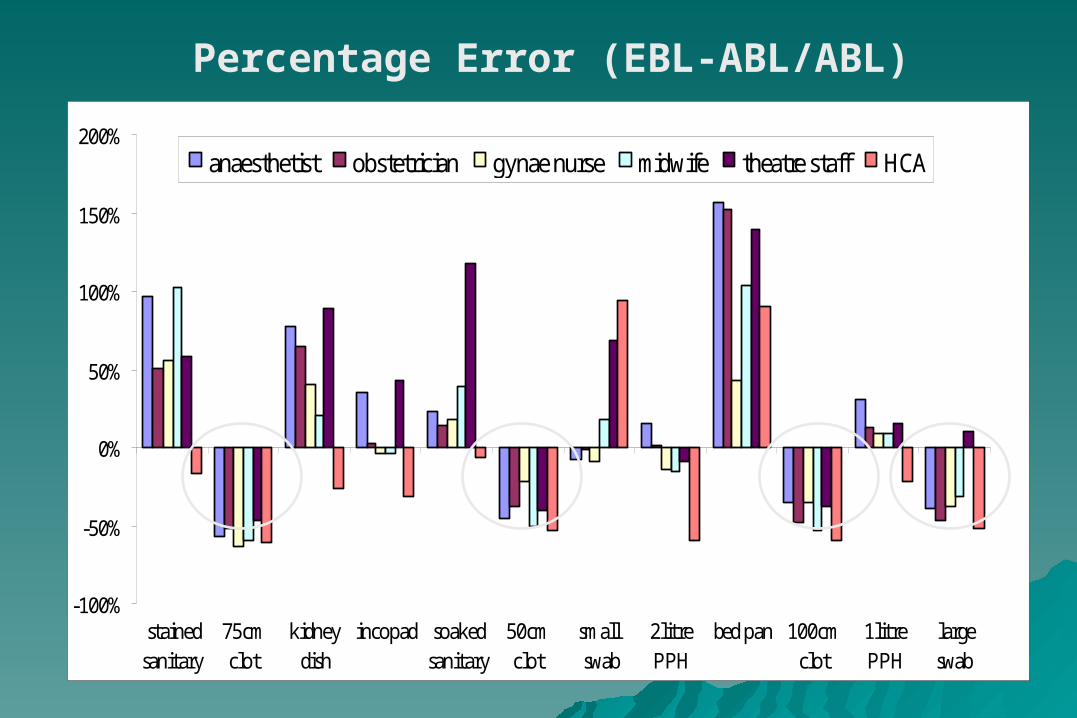
-100%
-50%
0%
50%
100%
150%
200%
stainedsanitary
75cmclot
kidneydish
incopad soakedsanitary
50cmclot
small swab
2litrePPH
bed pan 100cmclot
1litrePPH
largeswab
anaesthetist obstetrician gynae nurse midwife theatre staff HCA
Percentage Error (EBL-ABL/ABL)

Revealed bleeding….Revealed bleeding….
Traditional DefinitionTraditional Definition
– blood loss of > 500 mL following vaginal deliveryblood loss of > 500 mL following vaginal delivery– blood loss of > 1000 mL following cesarean blood loss of > 1000 mL following cesarean
deliverydelivery
Functional DefinitionFunctional Definition– any blood loss that has the potential to produce any blood loss that has the potential to produce
or produces hemodynamic instabilityor produces hemodynamic instability
IncidenceIncidence– about 5% of all deliveriesabout 5% of all deliveries
Postpartum Hemorrhage
Etiology of Postpartum Etiology of Postpartum HemorrhageHemorrhage
TToneone - uterine atony- uterine atony
TTissueissue - retained tissue/clots- retained tissue/clots
TTraumarauma - laceration, rupture, - laceration, rupture, inversioninversion
TThrombinhrombin - coagulopathy- coagulopathy
Postpartum Hemorrhage
Risk Factors for PPH - AntepartumRisk Factors for PPH - Antepartum
– previous PPH or manual removal previous PPH or manual removal
– placental abruption, especially if concealedplacental abruption, especially if concealed
– intrauterine fetal demiseintrauterine fetal demise
– placenta previaplacenta previa
– gestational hypertension with proteinuriagestational hypertension with proteinuria
– overdistended uterus (e.g. twins, overdistended uterus (e.g. twins,
polyhydramnios)polyhydramnios)
– pre-existing maternal bleeding disorderpre-existing maternal bleeding disorder
(e.g. ITP)(e.g. ITP)
Postpartum Hemorrhage
Risk Factors for PPH - IntrapartumRisk Factors for PPH - Intrapartum
– operative delivery - cesarean or assisted operative delivery - cesarean or assisted
vaginalvaginal
– prolonged labourprolonged labour
– rapid labourrapid labour
– induction or augmentationinduction or augmentation
– chorioamnionitischorioamnionitis
– shoulder dystociashoulder dystocia
– internal podalic version and extraction of internal podalic version and extraction of
second twinsecond twin
– acquired coagulopathy (e.g. HELLP, DIC)acquired coagulopathy (e.g. HELLP, DIC)
Postpartum Hemorrhage
Risk Factors for PPH - Risk Factors for PPH - PostpartumPostpartum– lacerations or episiotomylacerations or episiotomy
– retained placenta/placental retained placenta/placental
abnormalitiesabnormalities
– uterine ruptureuterine rupture
– uterine inversionuterine inversion
– acquired coagulopathy (e.g. DIC)acquired coagulopathy (e.g. DIC)
Postpartum Hemorrhage
PreventionPrevention
– be preparedbe prepared– active management of the third stageactive management of the third stage
prophylactic oxytocin with delivery or with prophylactic oxytocin with delivery or with delivery of anterior shoulderdelivery of anterior shoulder– 10 U IM or 5 U IV bolus 10 U IM or 5 U IV bolus – 20 U/L N/S IV run rapidly20 U/L N/S IV run rapidly
early cord clamping and cuttingearly cord clamping and cutting gentle cord traction with suprapubic gentle cord traction with suprapubic
countertractioncountertraction
Postpartum Hemorrhage
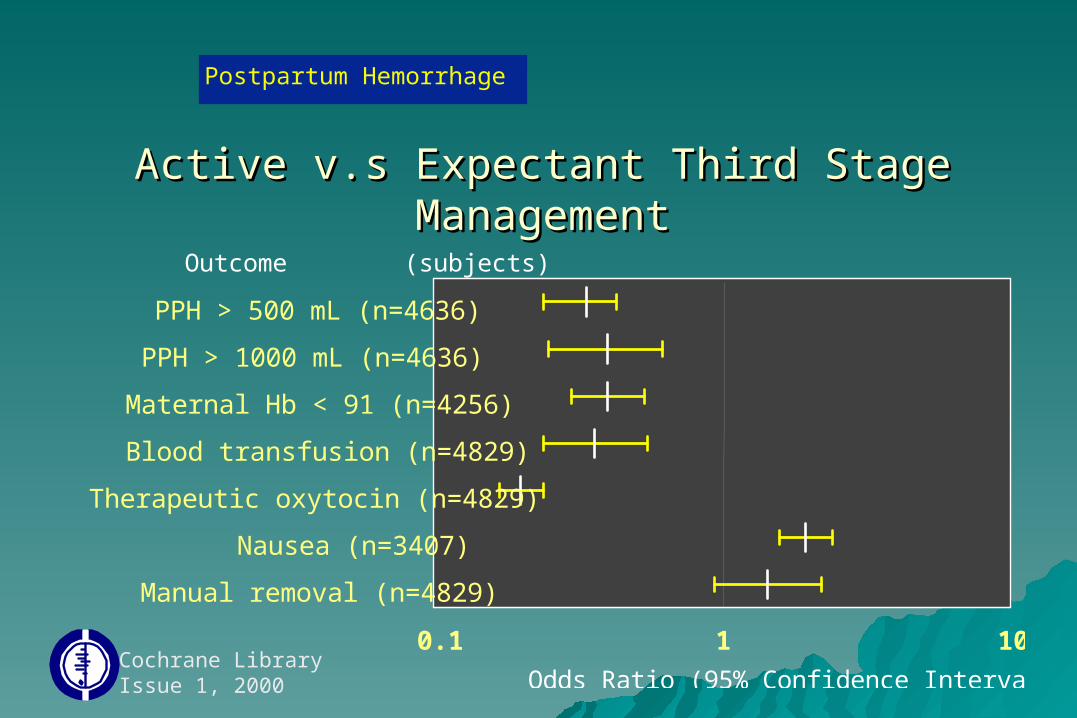
Active v.s Expectant Third Stage Active v.s Expectant Third Stage ManagementManagement
Cochrane LibraryIssue 1, 2000
PPH > 500 mL (n=4636)
PPH > 1000 mL (n=4636)
Maternal Hb < 91 (n=4256)
Blood transfusion (n=4829)
Therapeutic oxytocin (n=4829)
Nausea (n=3407)
Manual removal (n=4829)
0.1 1 10
Odds Ratio (95% Confidence Interval)
Outcome (subjects)
Postpartum Hemorrhage
Diagnosis - Is this a PPH?Diagnosis - Is this a PPH?– consider risk factorsconsider risk factors
– observe vaginal lossobserve vaginal loss
– express blood from vagina following C/Sexpress blood from vagina following C/S– REMEMBERREMEMBER
blood loss is consistently underestimatedblood loss is consistently underestimated ongoing trickling can lead to significant blood ongoing trickling can lead to significant blood
lossloss blood loss is generally well tolerated to a blood loss is generally well tolerated to a
pointpoint
Postpartum Hemorrhage
Diagnosis - What is the Diagnosis - What is the cause?cause?– assess the fundusassess the fundus
– inspect the lower genital tractinspect the lower genital tract
– explore the uterusexplore the uterus retained placental fragmentsretained placental fragments uterine ruptureuterine rupture uterine inversionuterine inversion
– assess coagulationassess coagulation
Postpartum Hemorrhage
ABCAA= airway= airwayBB= breathing= breathingCC= circulation= circulation
PostpartumHemorrhage
Management - Management - ABCABC’s’s– talk to and observe patienttalk to and observe patient
– large bore IV access (16 large bore IV access (16
gauge)gauge)
– crystalloid - lots!crystalloid - lots!
– CBCCBC
– cross-match and typecross-match and type
– get HELP!get HELP!
Postpartum Hemorrhage
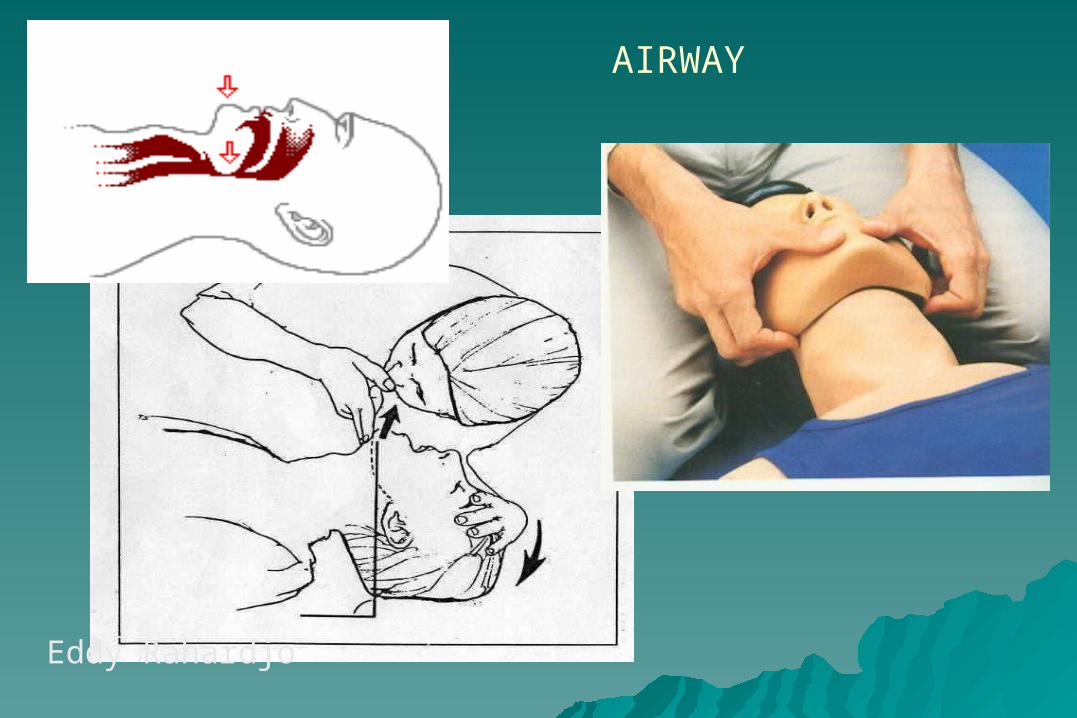
AIRWAY
Eddy Rahardjo
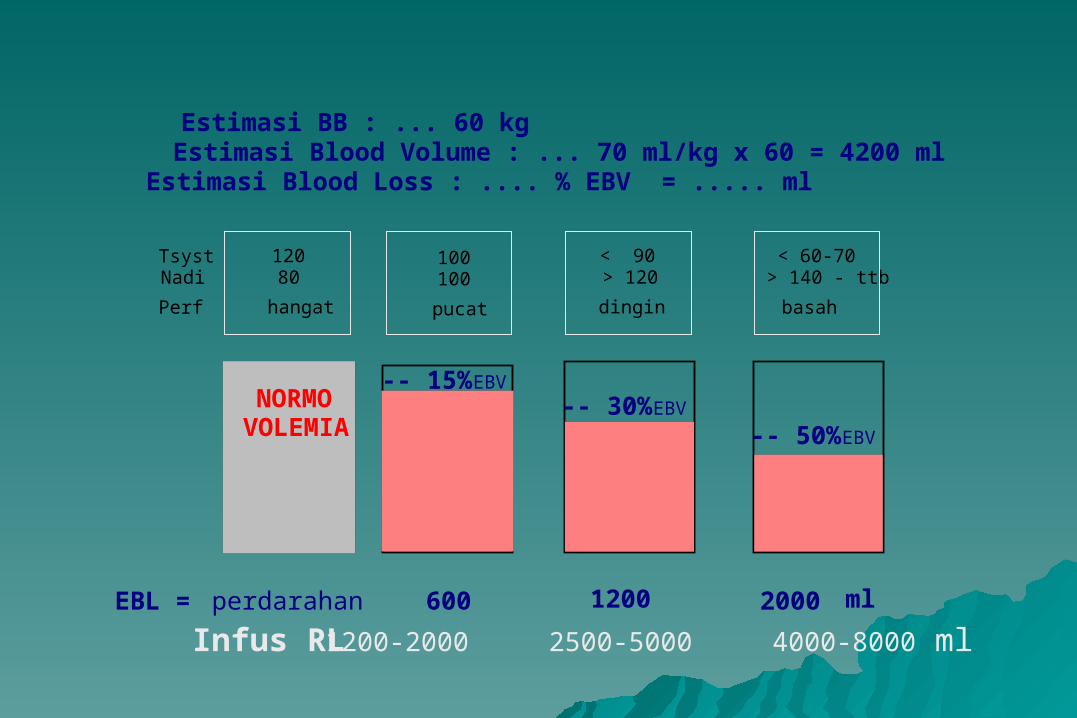
Estimasi BB : ... 60 kgEstimasi Blood Volume : ... 70 ml/kg x 60 = 4200 mlEstimasi Blood Loss : .... % EBV = ..... ml
NORMOVOLEMIA
-- 30% EBV-- 15% EBV
-- 50% EBV
TsystNadi
Perf
120 80
hangat
100100
pucat
< 90> 120
dingin
< 60-70> 140 - ttb
basah
EBL = perdarahan 600 1200 2000 ml
Infus RL 1200-2000 2500-5000 4000-8000 ml
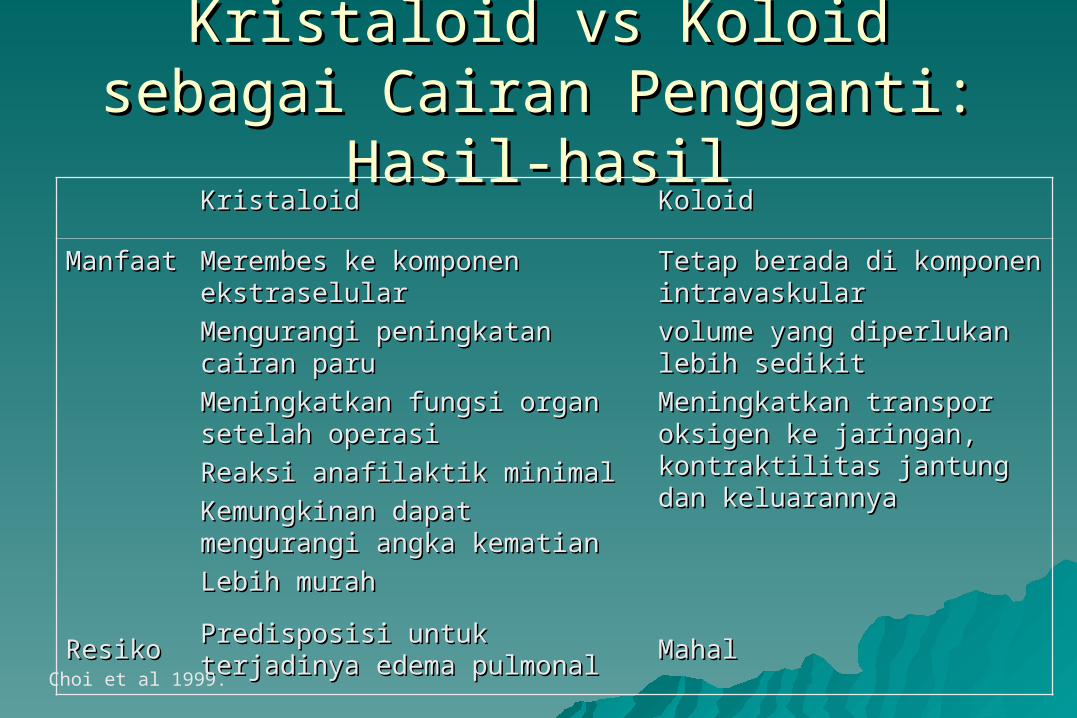
Kristaloid vs Koloid sebagai Cairan Kristaloid vs Koloid sebagai Cairan Pengganti: Hasil-hasilPengganti: Hasil-hasil
KristaloidKristaloid KoloidKoloid
Manfaat Manfaat Merembes ke komponen Merembes ke komponen ekstraselularekstraselular
Mengurangi peningkatan cairan Mengurangi peningkatan cairan paruparu
Meningkatkan fungsi organ Meningkatkan fungsi organ setelah operasi setelah operasi
Reaksi anafilaktik minimalReaksi anafilaktik minimal
Kemungkinan dapat Kemungkinan dapat mengurangi angka kematian mengurangi angka kematian
Lebih murahLebih murah
Tetap berada di komponen Tetap berada di komponen intravaskularintravaskular
volume yang diperlukan volume yang diperlukan lebih sedikitlebih sedikit
Meningkatkan transpor Meningkatkan transpor oksigen ke jaringan, oksigen ke jaringan, kontraktilitas jantung dan kontraktilitas jantung dan keluarannyakeluarannya
ResikoResiko Predisposisi untuk terjadinya Predisposisi untuk terjadinya edema pulmonaledema pulmonal MahalMahal
Choi et al 1999.
Kristaloid vs Koloid sebagai Cairan Kristaloid vs Koloid sebagai Cairan Pengganti: KesimpulanPengganti: Kesimpulan
Kristaloid merupakan pilihan pertama Kristaloid merupakan pilihan pertama untuk digunakan, karena:untuk digunakan, karena:– Lebih amanLebih aman– Lebih murahLebih murah– Lebih mudah didapatkanLebih mudah didapatkan
Management Management - - Assess the Assess the fundusfundus
– simultaneous with ABC ’ssimultaneous with ABC ’s
– atony is the leading cause of PPHatony is the leading cause of PPH
– if boggy if boggy bimanual massage bimanual massage rules out uterine inversionrules out uterine inversion may feel lower tract injurymay feel lower tract injury evacuate clot from vagina and/or cervixevacuate clot from vagina and/or cervix may consider manual exploration at this may consider manual exploration at this
timetime
Postpartum Hemorrhage
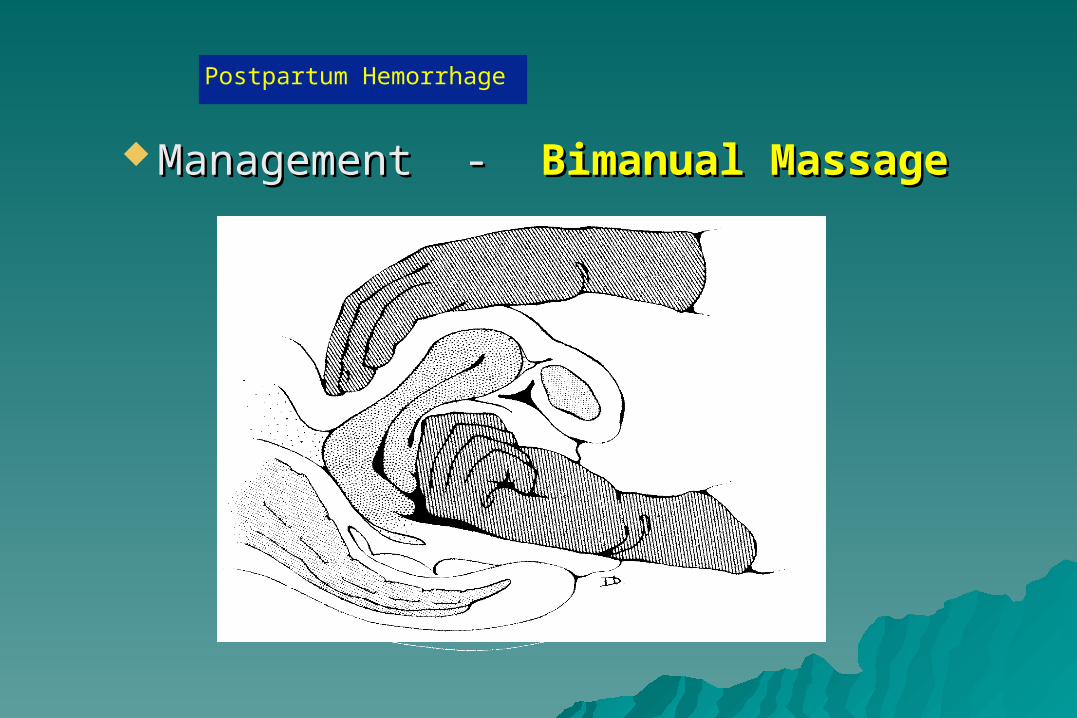
Management - Management - Bimanual MassageBimanual Massage
Postpartum Hemorrhage
Management Management - - OxytocinOxytocin
– 5 units IV bolus5 units IV bolus
– 20 units per L N/S IV wide open20 units per L N/S IV wide open
– 10 units intramyometrial given 10 units intramyometrial given
transabdominallytransabdominally
Postpartum Hemorrhage
Management Management --ManualExplorationManualExploration– if no response to bimanual massage if no response to bimanual massage
and oxytocin then proceed to and oxytocin then proceed to exploration exploration
– manual exploration will:manual exploration will: rule out uterine inversionrule out uterine inversion palpate cervical injurypalpate cervical injury remove retained placenta or clot from remove retained placenta or clot from
uterusuterus rule out uterine rupture or dehiscencerule out uterine rupture or dehiscence
Postpartum Hemorrhage
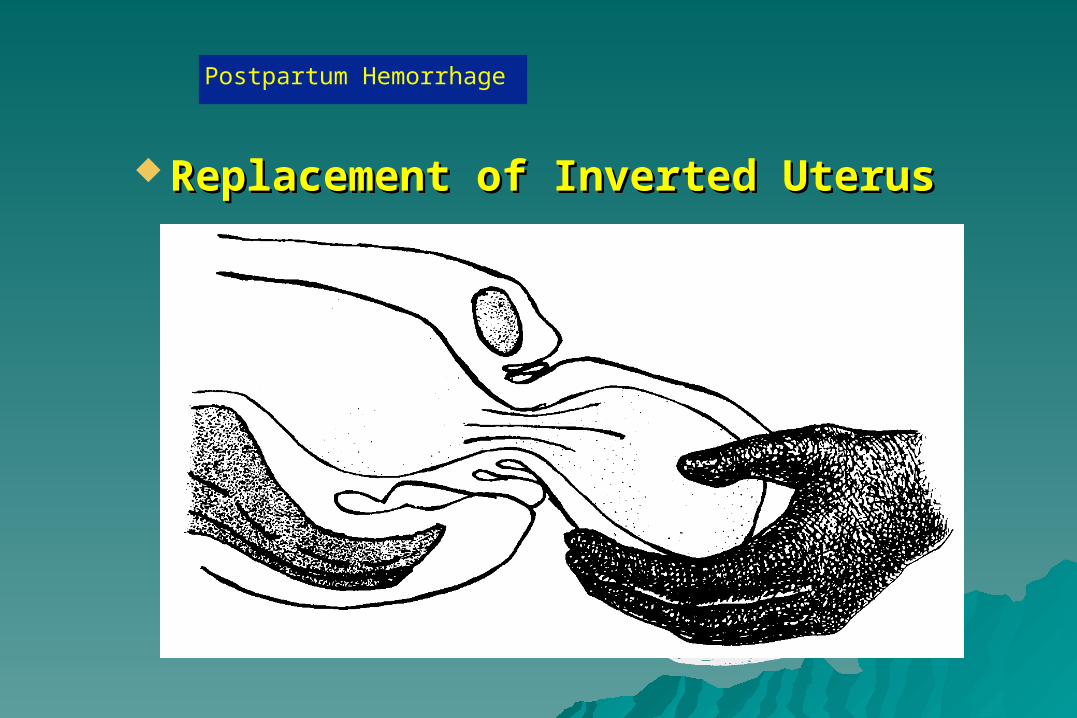
Replacement of Inverted UterusReplacement of Inverted Uterus
Postpartum Hemorrhage
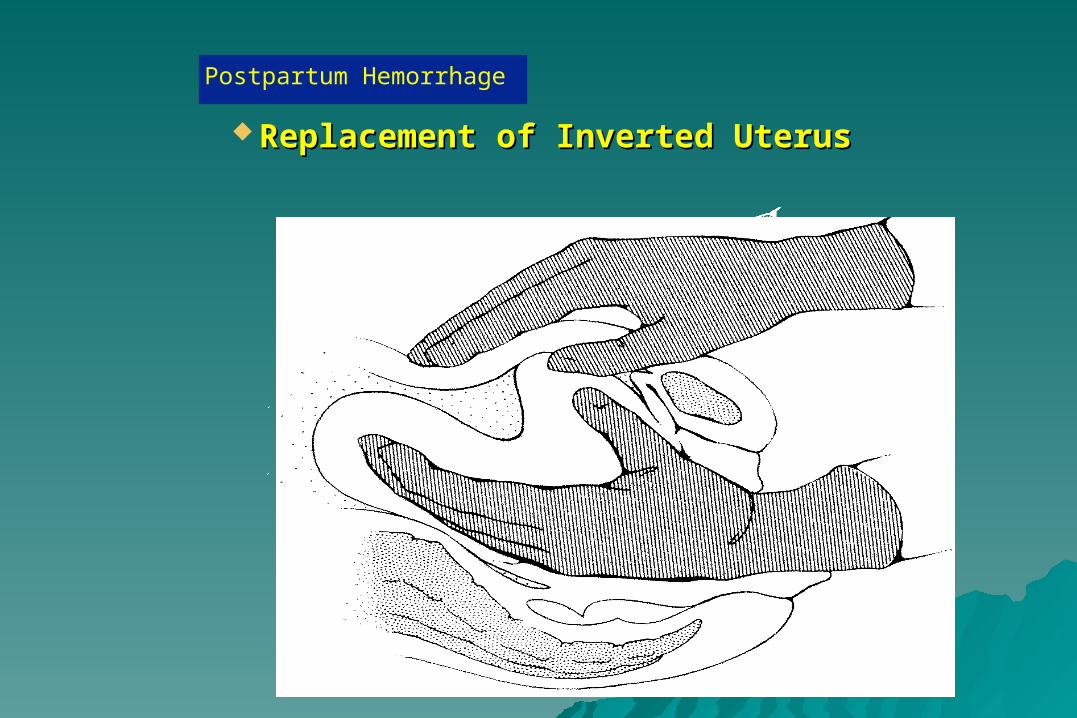
Replacement of Inverted UterusReplacement of Inverted Uterus
Postpartum Hemorrhage
Management Management - Additional Uterotonics - Additional Uterotonics– ergotamine - caution in hypertensionergotamine - caution in hypertension
0.25 mg IM or 0.125 mg IV0.25 mg IM or 0.125 mg IV maximum dose 1.25 mgmaximum dose 1.25 mg
– Hemabate (carboprost) - asthma is relative Hemabate (carboprost) - asthma is relative contraindicationcontraindication
15 methyl-prostaglandin F215 methyl-prostaglandin F2 0.25 mg IM or intramyometrial0.25 mg IM or intramyometrial Maximum dose 2 mgMaximum dose 2 mg
– Cytotec (misoprostol) - caution in asthmaCytotec (misoprostol) - caution in asthma 400 mg pr or po400 mg pr or po
Postpartum Hemorrhage
Management - Bleeding with firm Management - Bleeding with firm uterusuterus
– explore the lower genital tractexplore the lower genital tract
– requirementsrequirements -- appropriate analgesiaappropriate analgesia
-- good exposure and good exposure and lightinglighting
– appropriate surgical repairappropriate surgical repair- - may temporize with may temporize with
packingpacking
Postpartum Hemorrhage
Management - Continued uterine bleedingManagement - Continued uterine bleeding
– possible coagulopathy - INR, PTT, TCT, fibrinogenpossible coagulopathy - INR, PTT, TCT, fibrinogen
– if coagulation is abnormal:if coagulation is abnormal: correct with clotting factors, plateletscorrect with clotting factors, platelets
– if coagulation is normal:if coagulation is normal: prepare for O.R. (may consider embolization)prepare for O.R. (may consider embolization) rule out uterine rupture, inadequate incision repairrule out uterine rupture, inadequate incision repair consider uterine/hypogastric ligation, hysterectomyconsider uterine/hypogastric ligation, hysterectomy
Postpartum Hemorrhage
Management - ABC ’sManagement - ABC ’s
ENSURE that you are always ENSURE that you are always ahead with yourahead with your resuscitation!!!!resuscitation!!!!
– consider need for Foley catheter, CVP, arterial consider need for Foley catheter, CVP, arterial line, etcline, etc
– consider need for more expert helpconsider need for more expert help
Postpartum Hemorrhage


B-Lynchmethode
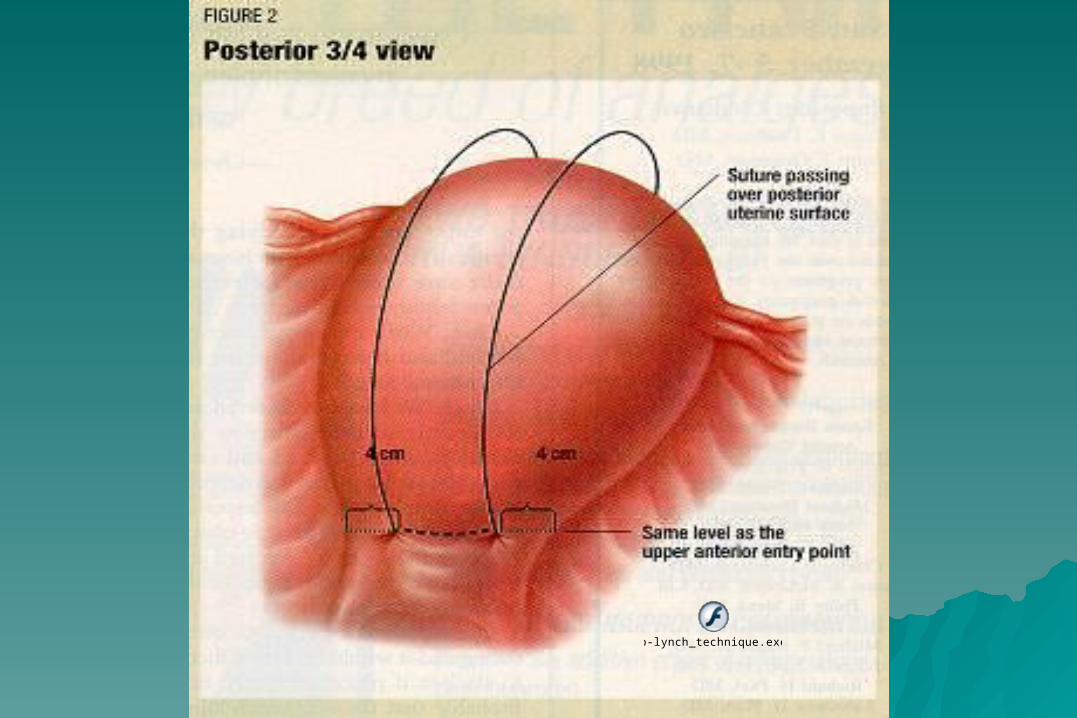
b-lynch_technique.exe
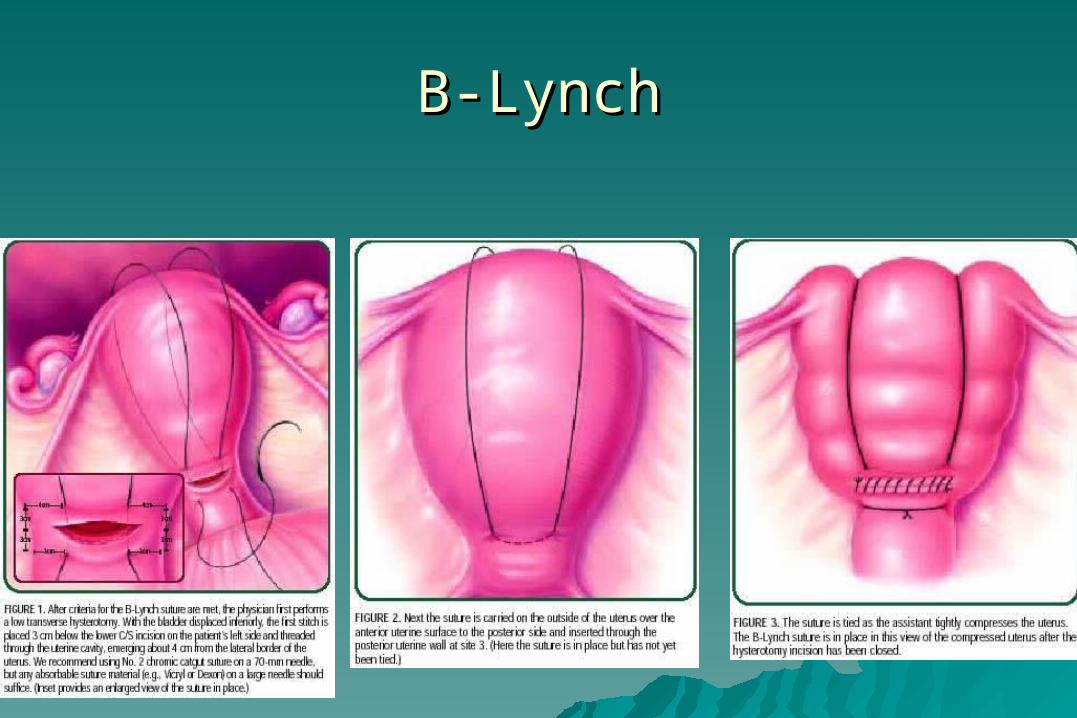
B-LynchB-Lynch
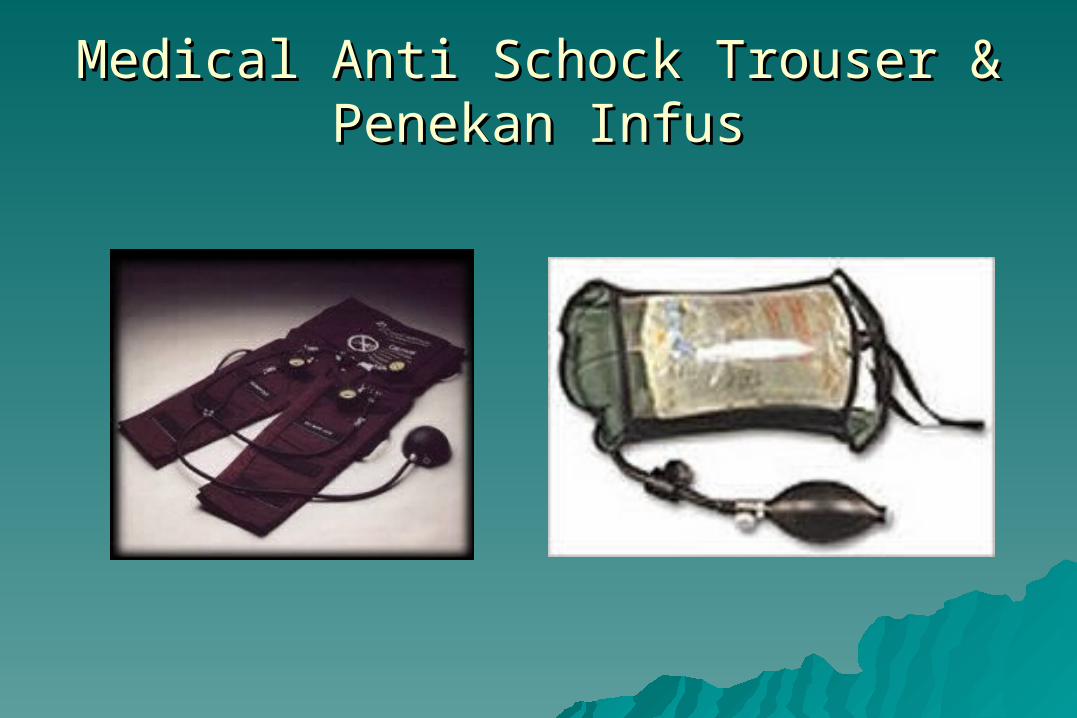
Medical Anti Schock Trouser & Medical Anti Schock Trouser & Penekan InfusPenekan Infus
ConclusionsConclusions
– be preparedbe prepared– practice preventionpractice prevention– assess the lossassess the loss– assess maternal statusassess maternal status– resuscitate vigorously and resuscitate vigorously and
appropriatelyappropriately– diagnose the causediagnose the cause– treat the causetreat the cause
Postpartum Hemorrhage
Management - EvolutionManagement - Evolution
PanicPanicHysterectomy
PitocinProstaglandinsHappiness
Postpartum Hemorrhage

Thank YouThank You
Postpartum Hemorrhage











![[SriMO2016] Referensi Genitouro-Reproduksi (Obstetrik)](https://img.dokumen.tips/doc/110x75/577c856d1a28abe054bd1b55/srimo2016-referensi-genitouro-reproduksi-obstetrik.jpg)

















