Embed Size (px)
DESCRIPTION
Pedia Tickler
Citation preview
THE SEVEN HABITS OF HIGHLY EFFECTIVE PEOPLE
by Stephen R. Covey
Habit 1: Be Proactive•Ability to control one’s environment, rather that have it control you.•Taking initiative doesn’t mean being aggressive, it means recognizing your responsibility to make things happen
Habit 2: Begin with the end in mind•The habit of personal leadership•Lead oneself towards what you consider your aims•Based on imagination – the ability to envision, to see the potential, to create with our minds what we cannot at present see with our eyes
Habit 3: Put First Things First•The habit of personal management•Create a clear, mutual understanding of what needs to be accomplished, focusing on what, not how; results not methods•Spend time. Be patient. Visualize the desired result
Habit 4: Think Win-Win•The habit of interpersonal relationship•Achievements are largely dependent on co- operative efforts with others•Agreements or solutions are mutually beneficial & satisfying
Habit 5: Seek first to understand and then to be understood
•The habit of communication•Diagnose before you prescribe•Simple, effective & essential in developing & maintaining positive relationships in all aspects of life
Habit 6: Synergize•The habit of creative cooperation•“the whole is greater than the sum of its parts”•See good & potential in other person’s contribution
Habit 7: Sharpen the saw•The habit self-renewal, of continuous improvement•Circles & embodies all other habits
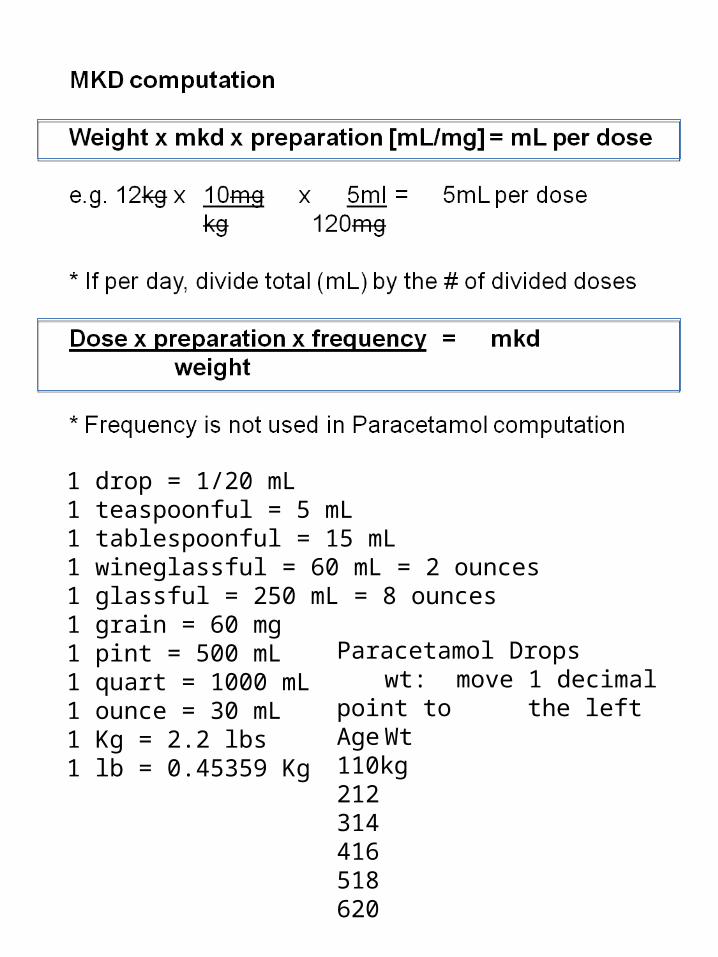
1 drop = 1/20 mL1 teaspoonful = 5 mL1 tablespoonful = 15 mL1 wineglassful = 60 mL = 2 ounces1 glassful = 250 mL = 8 ounces1 grain = 60 mg1 pint = 500 mL1 quart = 1000 mL1 ounce = 30 mL1 Kg = 2.2 lbs1 lb = 0.45359 Kg
Paracetamol Dropswt: move 1 decimal point to
the leftAge Wt110kg212314416518620


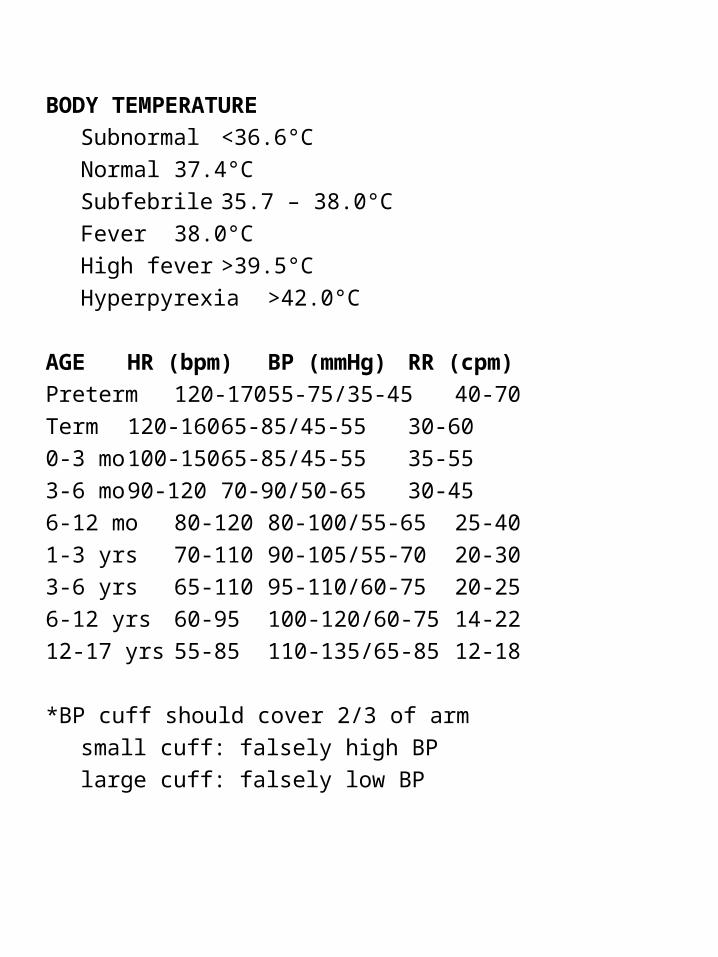
BODY TEMPERATURE
Subnormal <36.6°C
Normal 37.4°C
Subfebrile 35.7 – 38.0°C
Fever 38.0°C
High fever >39.5°C
Hyperpyrexia >42.0°C
AGE HR (bpm) BP (mmHg) RR (cpm)
Preterm 120-170 55-75/35-45 40-70
Term 120-160 65-85/45-55 30-60
0-3 mo 100-150 65-85/45-55 35-55
3-6 mo 90-120 70-90/50-65 30-45
6-12 mo 80-120 80-100/55-65 25-40
1-3 yrs 70-110 90-105/55-70 20-30
3-6 yrs 65-110 95-110/60-75 20-25
6-12 yrs 60-95 100-120/60-75 14-22
12-17 yrs 55-85 110-135/65-85 12-18
*BP cuff should cover 2/3 of arm
small cuff: falsely high BP
large cuff: falsely low BP
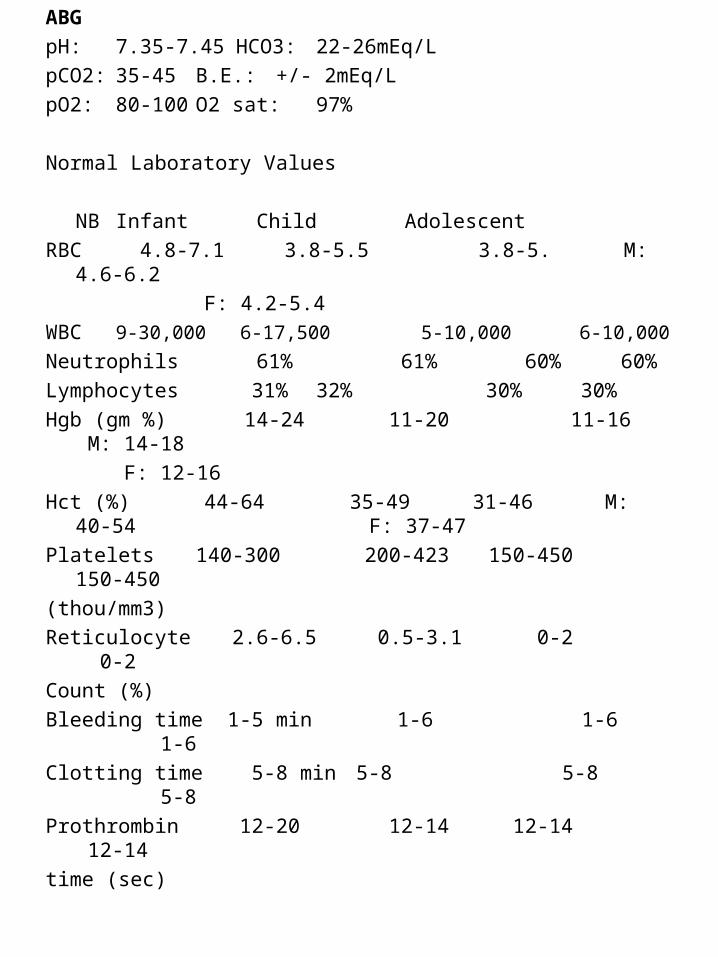
ABG
pH: 7.35-7.45 HCO3: 22-26mEq/L
pCO2: 35-45 B.E.: +/- 2mEq/L
pO2: 80-100 O2 sat: 97%
Normal Laboratory Values
NB Infant Child Adolescent
RBC 4.8-7.1 3.8-5.5 3.8-5. M: 4.6-6.2
F: 4.2-5.4
WBC 9-30,000 6-17,500 5-10,000 6-10,000
Neutrophils 61% 61% 60% 60%
Lymphocytes 31% 32% 30% 30%
Hgb (gm %) 14-24 11-20 11-16 M: 14-18
F: 12-16
Hct (%) 44-64 35-49 31-46 M: 40-54 F: 37-47
Platelets 140-300 200-423 150-450 150-450
(thou/mm3)
Reticulocyte 2.6-6.5 0.5-3.1 0-2 0-2
Count (%)
Bleeding time 1-5 min 1-6 1-6 1-6
Clotting time 5-8 min 5-8 5-8 5-8
Prothrombin 12-20 12-14 12-14 12-14
time (sec)

BMI
Asian Caucasian
Underweight <18.5 <18.5
Normal 18.5 – 22.9 18.5 – 24.9
Overweight ≥ 23.0 25 – 29.9
at risk 23 – 24.9
Obese I 25 – 29.9 30 – 39.9
Obese II ≥ 30 >40
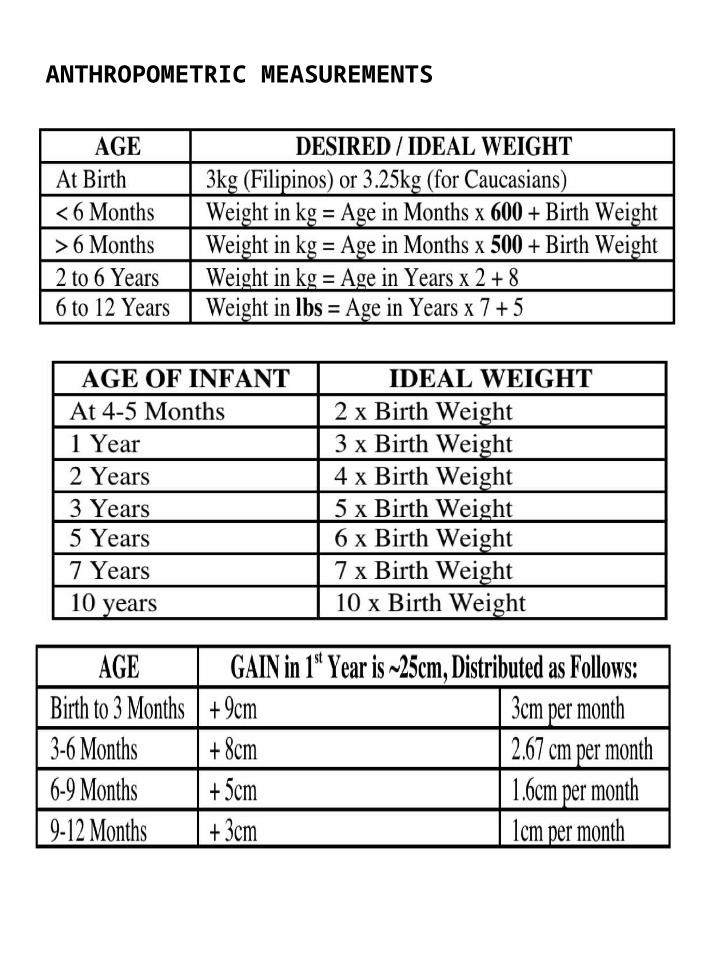
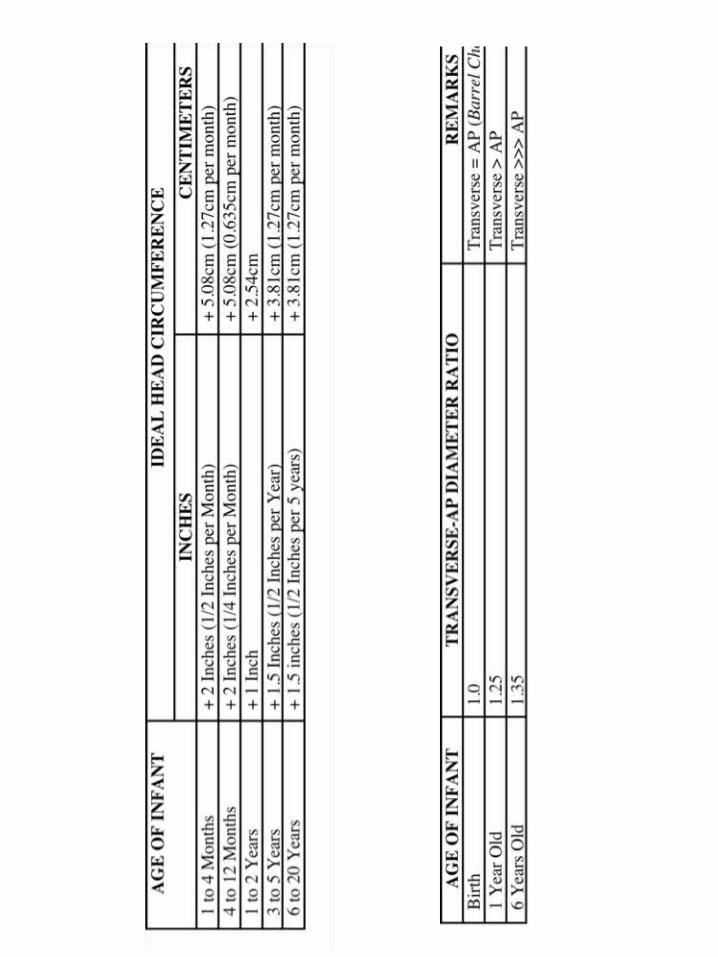
ANTHROPOMETRIC MEASUREMENTS
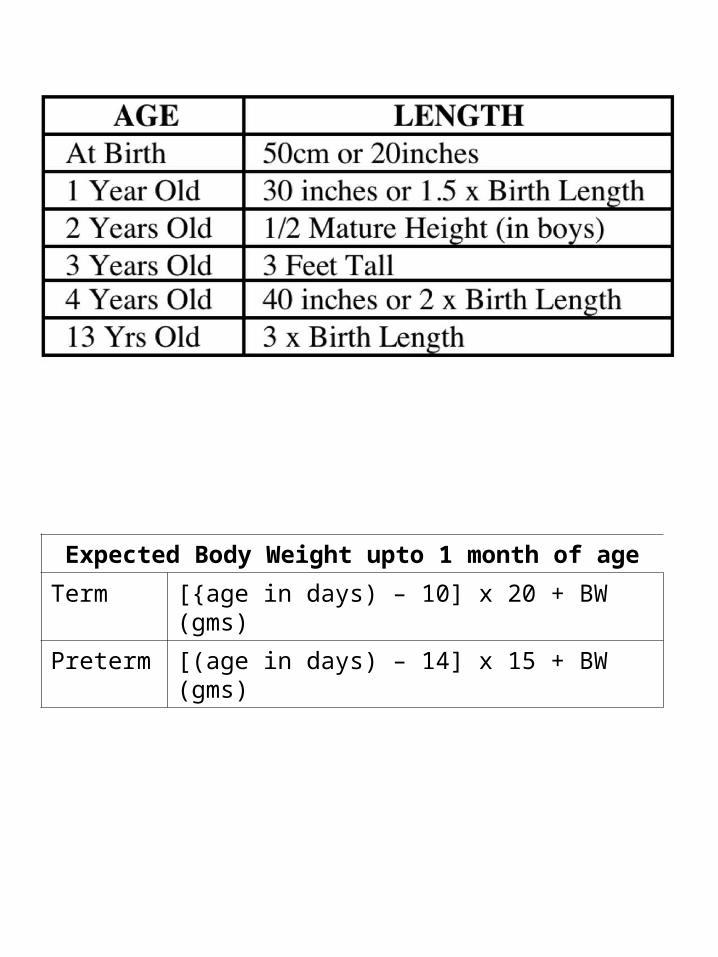
Expected Body Weight upto 1 month of age
Term [{age in days) – 10] x 20 + BW (gms)
Preterm [(age in days) – 14] x 15 + BW (gms)

APG
AR
GCS
SCO
RIN
G
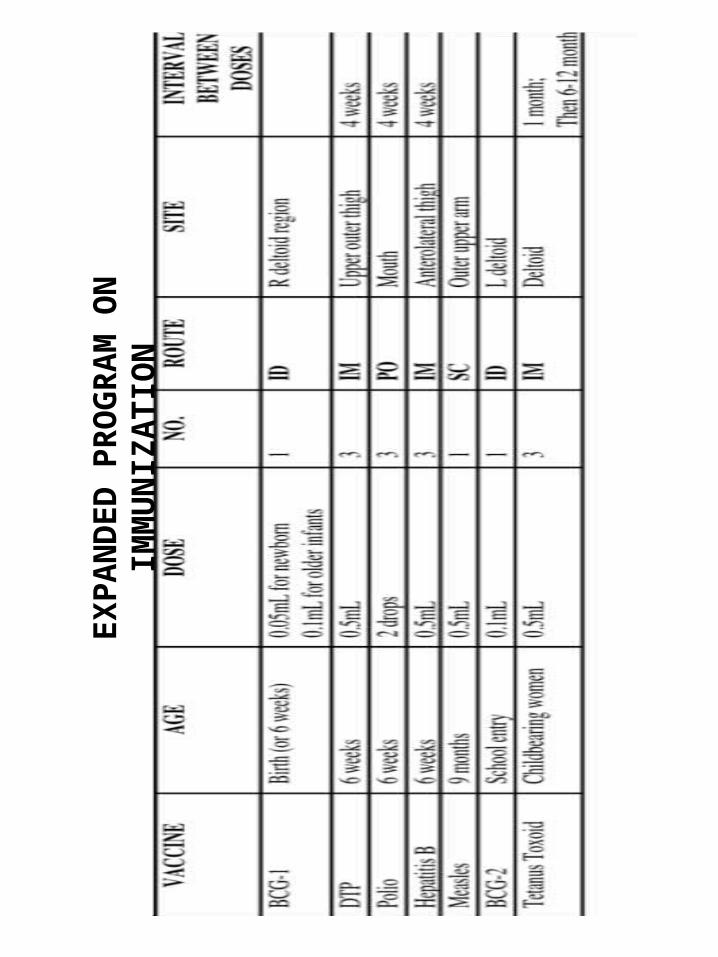
EXPA
ND
ED P
ROG
RAM
ON
IM
MU
NIZ
ATIO
N
ACUTE DIARRHEA (at least 3x BM in 24 hrs)
4 Major Mechanisms
1. Poorly absorbed osmotically active substances in lumen
2. Intestinal ion secretion (increased) or decreased absorption
3. Outpouring into the lumen of blood, mucus
4. Derangement of intestinal motility
Rotaviral AGE (vomiting first then diarrhea)
ingestion of rotavirus rotavirus in intestinal villi destruction of villi
(secretory diarrhea absorption, secretion) AGE
Assessment of dehydration (skin pinch test)
(+) if > 2 seconds
no dehydration if skin tenting goes back immediately

Etiology of AGE
Bacteria Viruses
Aeromonas Astroviruses
Bacillus cereus Caloviruses
Campylobacter jejuni Norovirus
Clostridium perfringens Enteric adenoviruses
Clostridium difficile Rotavirus
Escherichia coli Cytomegalovirus
Plesiomonas shigelbides Herpes simplex virus
Salmonella
Shigella
Staphylococcus aureus
Vibrio cholerae 01 & 0139
Vibrio parahaemolyticus
Yersinia enterocolitica
Parasites
Balantidium coli
Blastocyctis hominis
Cryptosporidium
Giardia lamblia
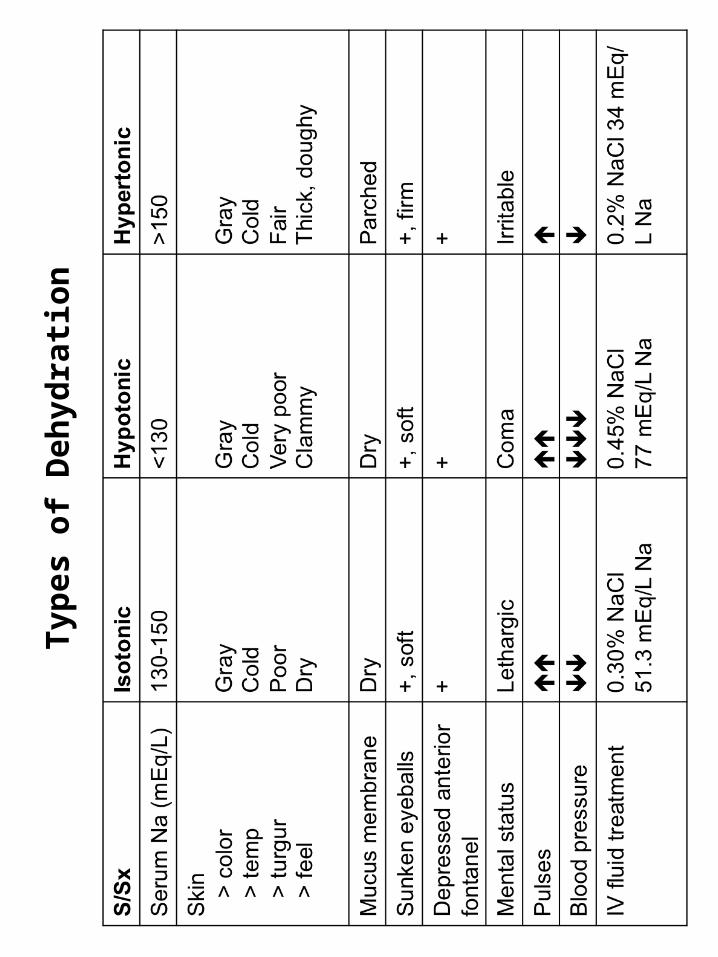
Type
s of
Deh
ydra
tion
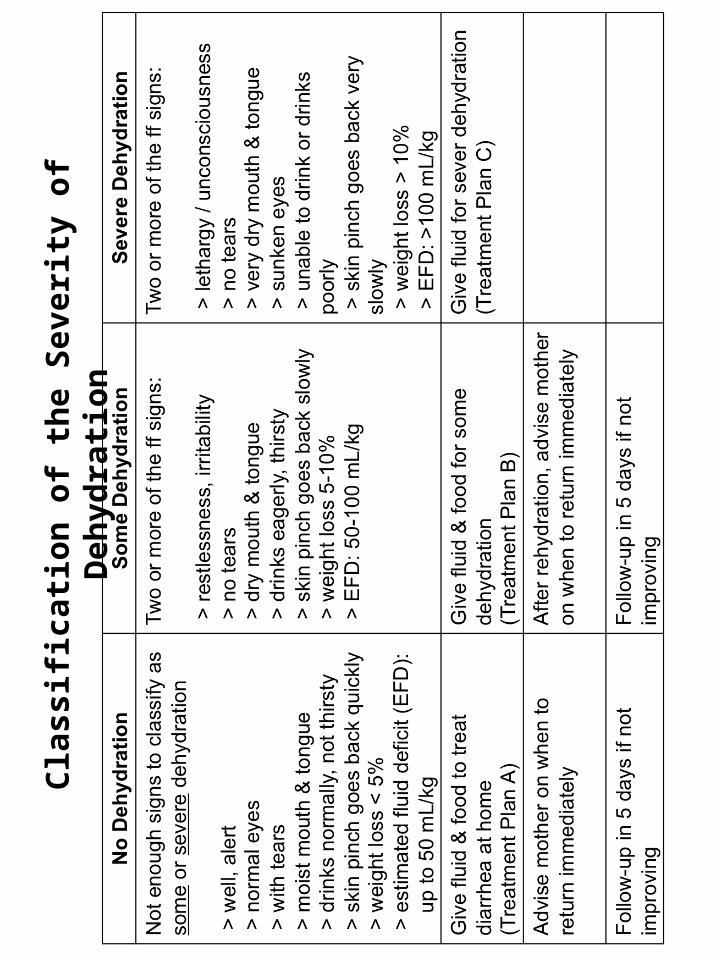
Clas
sific
ation
of t
he S
ever
ity o
f Deh
ydra
tion
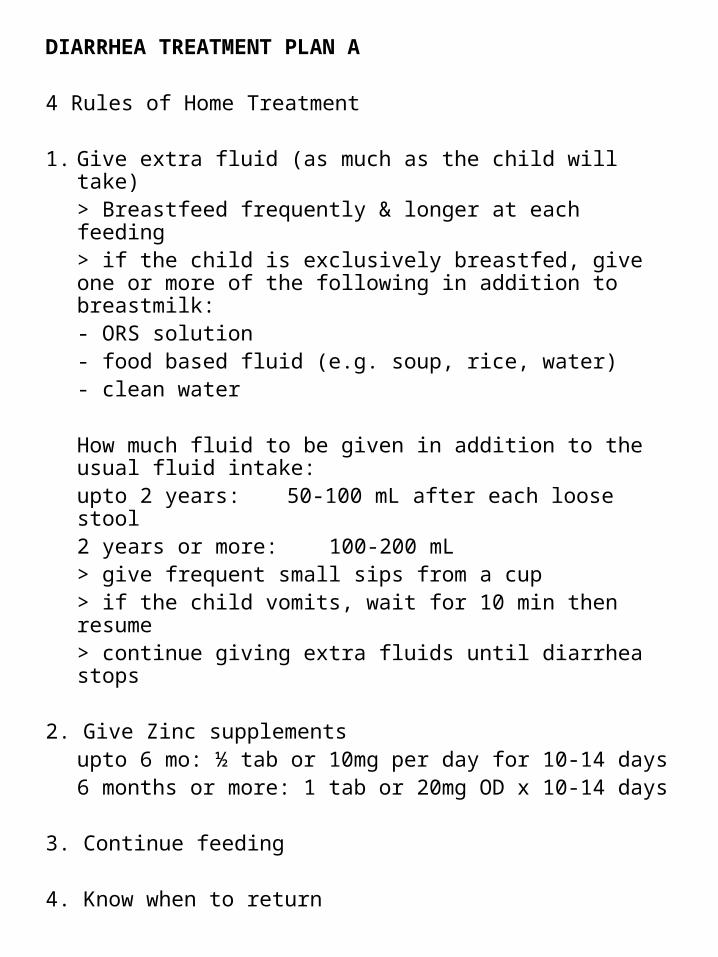
DIARRHEA TREATMENT PLAN A
4 Rules of Home Treatment
1. Give extra fluid (as much as the child will take)> Breastfeed frequently & longer at each feeding> if the child is exclusively breastfed, give one or more of the following in addition to breastmilk:
- ORS solution- food based fluid (e.g. soup, rice, water)- clean water
How much fluid to be given in addition to the usual fluid intake:upto 2 years: 50-100 mL after each loose stool2 years or more: 100-200 mL
> give frequent small sips from a cup> if the child vomits, wait for 10 min then
resume> continue giving extra fluids until diarrhea
stops
2. Give Zinc supplementsupto 6 mo: ½ tab or 10mg per day for 10-14 days6 months or more: 1 tab or 20mg OD x 10-14 days
3. Continue feeding
4. Know when to return
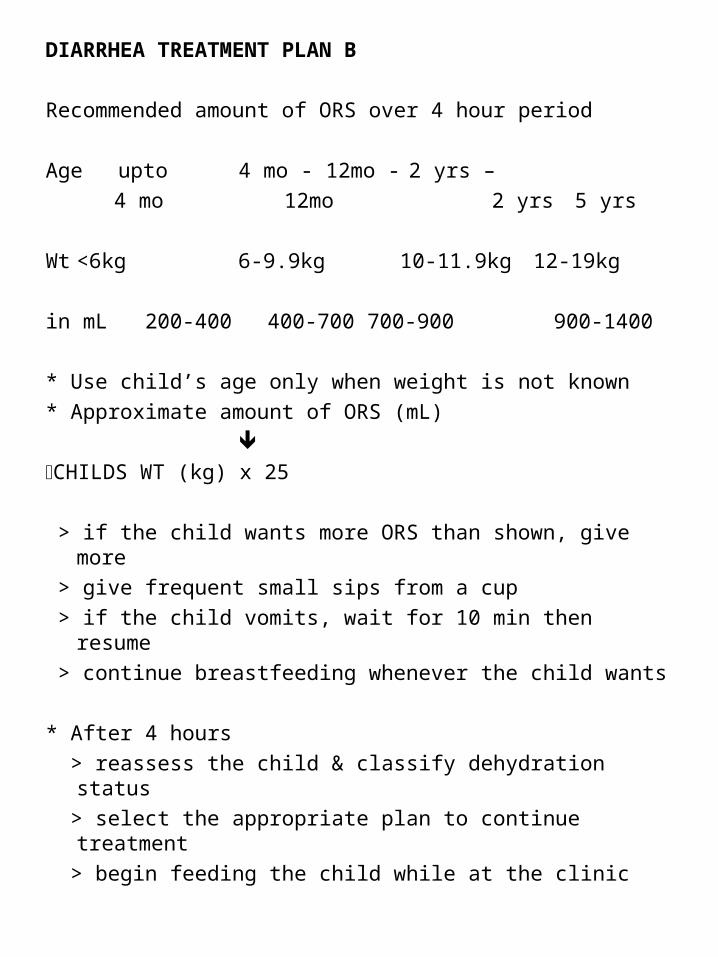
DIARRHEA TREATMENT PLAN B
Recommended amount of ORS over 4 hour period
Age upto 4 mo - 12mo - 2 yrs –
4 mo 12mo 2 yrs 5 yrs
Wt <6kg 6-9.9kg 10-11.9kg 12-19kg
in mL 200-400 400-700 700-900 900-1400
* Use child’s age only when weight is not known
* Approximate amount of ORS (mL)
CHILDS WT (kg) x 25
> if the child wants more ORS than shown, give more
> give frequent small sips from a cup
> if the child vomits, wait for 10 min then resume
> continue breastfeeding whenever the child wants
* After 4 hours
> reassess the child & classify dehydration status
> select the appropriate plan to continue treatment
> begin feeding the child while at the clinic

DIARRHEA TREATMENT PLAN C
Treat severe dehydration QUICKLY!
> start IV fluid immediately
> if the child can drink, give ORS by mouth while the IV drip is being set up
> give 100mL/kg Lactated Ringer’s solution
Age First give Then give
30mL/kg in: 70mL/kg in:
Infants 1 hour* 5 hours
(<12mo)
Children 30 min* 2 ½ hours
(12mo-5yrs)
* Repeat once if radial pulse is very weak or not detectable
> reassess the child every 15-30 min. if dehydration is not improving, give IV fluid more rapidly
> also give ORS (~5mL/kg/hr) as soon as the child can drink [usually after 3-4 hours in infants; 1-2 hours in children]
> reassess after 6 hrs (infant) & 3 hrs (child)
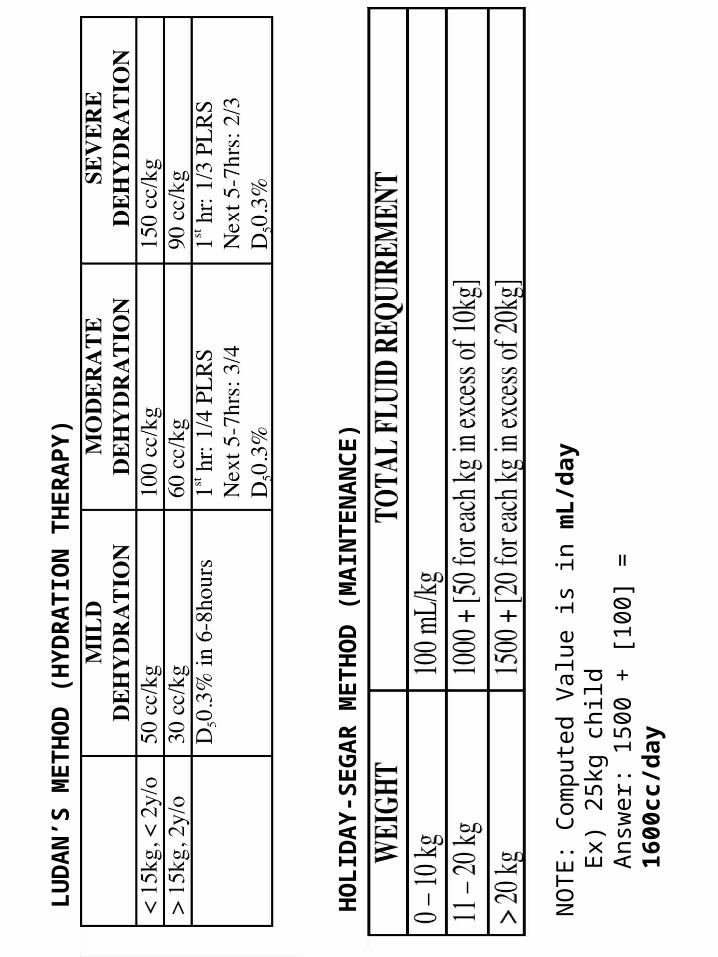
LU
DA
N’S
ME
TH
OD
(H
YD
RA
TIO
N T
HE
RA
PY
)
HO
LID
AY
-SE
GA
R M
ET
HO
D (
MA
INT
EN
AN
CE
)
NO
TE
: C
ompu
ted
Val
ue is
in m
L/d
ayE
x) 2
5kg
child
Ans
wer
: 15
00 +
[10
0] =
160
0cc/
day
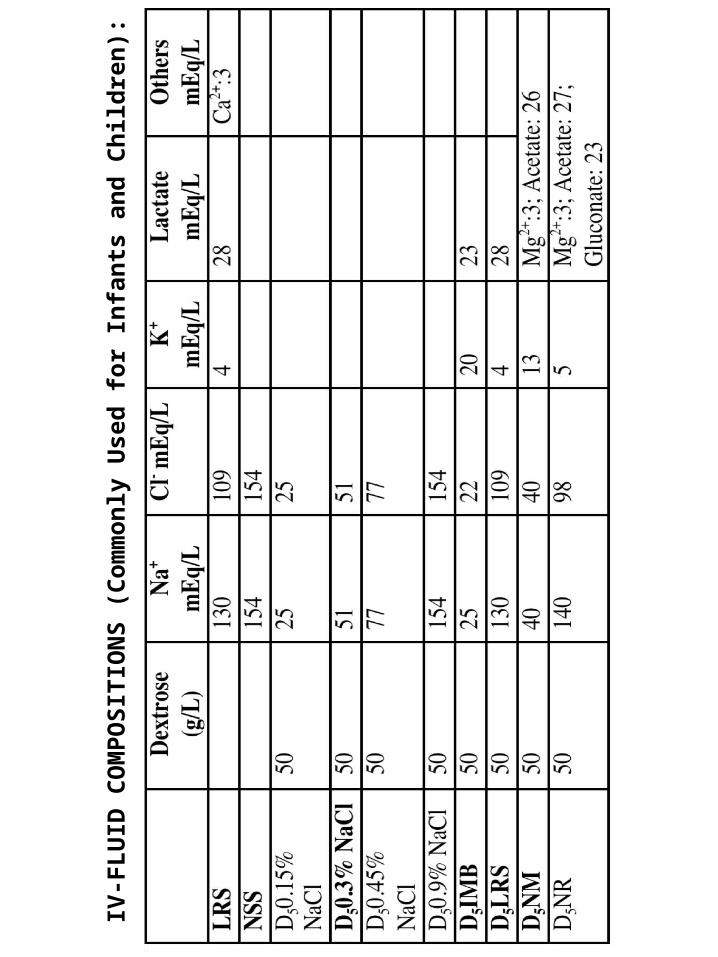
IV-F
LU
ID C
OM
PO
SIT
ION
S (
Co
mm
on
ly U
sed
fo
r In
fan
ts a
nd
Ch
ild
ren
):
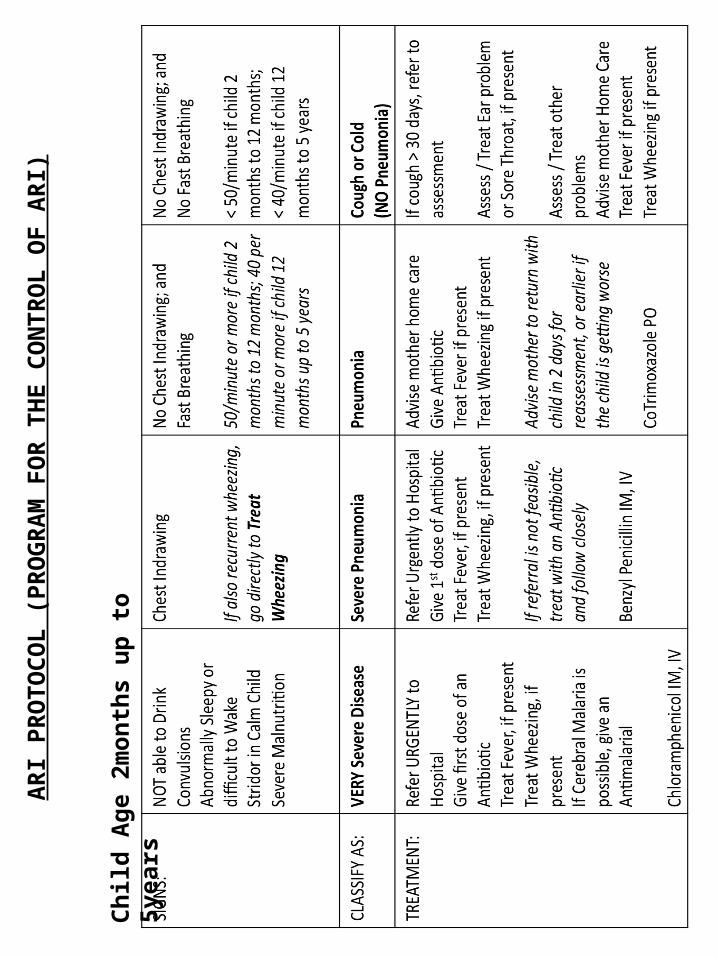
ARI P
ROTO
COL
(PRO
GRA
M F
OR
THE
CON
TRO
L O
F AR
I)
Ch
ild
Ag
e 2m
on
ths
up
to
5ye
ars
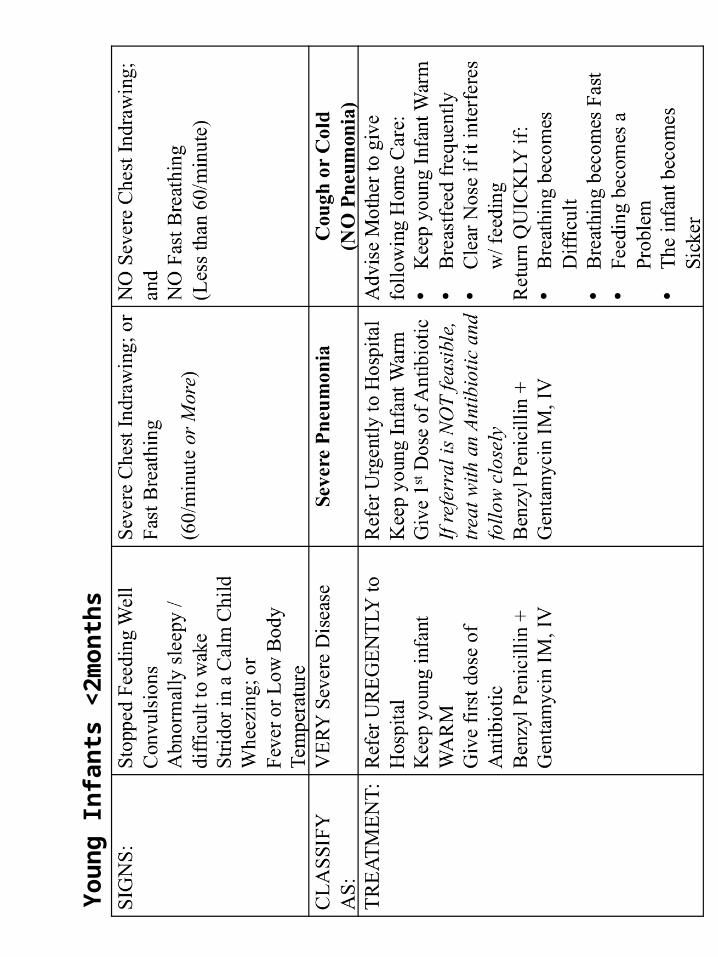
Yo
un
g I
nfa
nts
<2m
on
ths
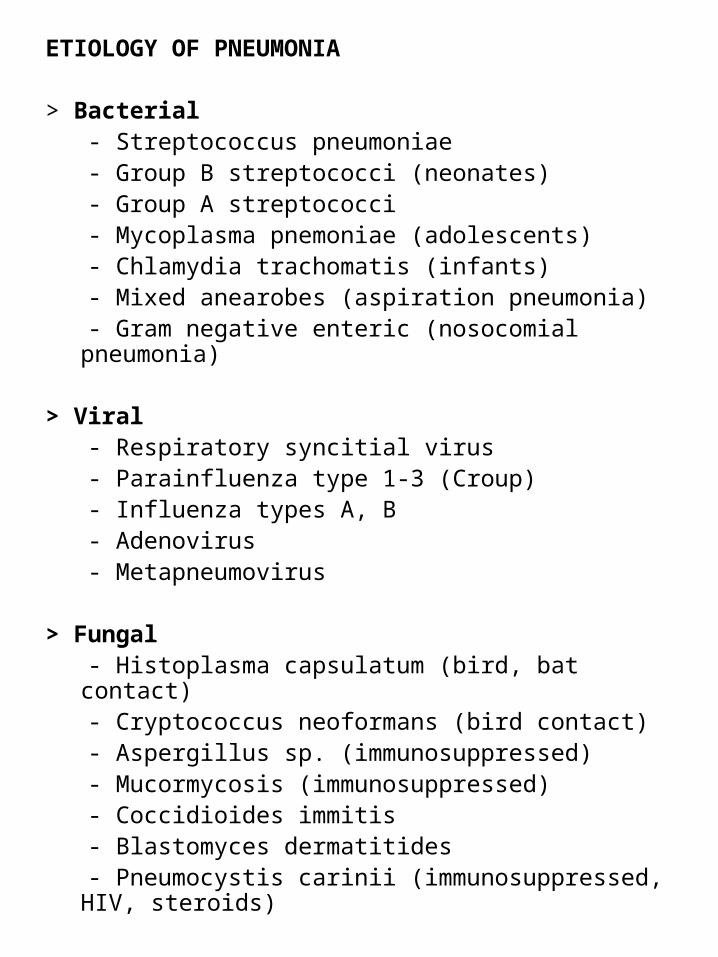
ETIOLOGY OF PNEUMONIA
> Bacterial - Streptococcus pneumoniae - Group B streptococci (neonates) - Group A streptococci - Mycoplasma pnemoniae (adolescents) - Chlamydia trachomatis (infants) - Mixed anearobes (aspiration pneumonia) - Gram negative enteric (nosocomial pneumonia)
> Viral - Respiratory syncitial virus - Parainfluenza type 1-3 (Croup) - Influenza types A, B - Adenovirus - Metapneumovirus
> Fungal - Histoplasma capsulatum (bird, bat contact) - Cryptococcus neoformans (bird contact) - Aspergillus sp. (immunosuppressed) - Mucormycosis (immunosuppressed) - Coccidioides immitis - Blastomyces dermatitides - Pneumocystis carinii (immunosuppressed, HIV,
steroids)
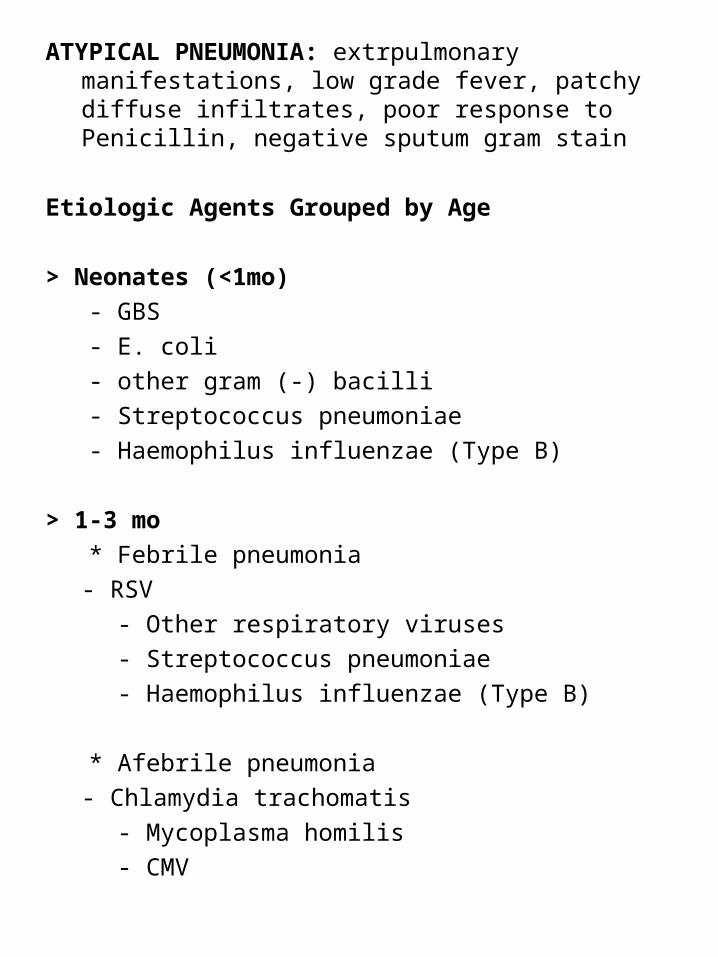
ATYPICAL PNEUMONIA: extrpulmonary manifestations, low grade fever, patchy diffuse infiltrates, poor response to Penicillin, negative sputum gram stain
Etiologic Agents Grouped by Age
> Neonates (<1mo)
- GBS
- E. coli
- other gram (-) bacilli
- Streptococcus pneumoniae
- Haemophilus influenzae (Type B)
> 1-3 mo
* Febrile pneumonia
- RSV
- Other respiratory viruses
- Streptococcus pneumoniae
- Haemophilus influenzae (Type B)
* Afebrile pneumonia
- Chlamydia trachomatis
- Mycoplasma homilis
- CMV
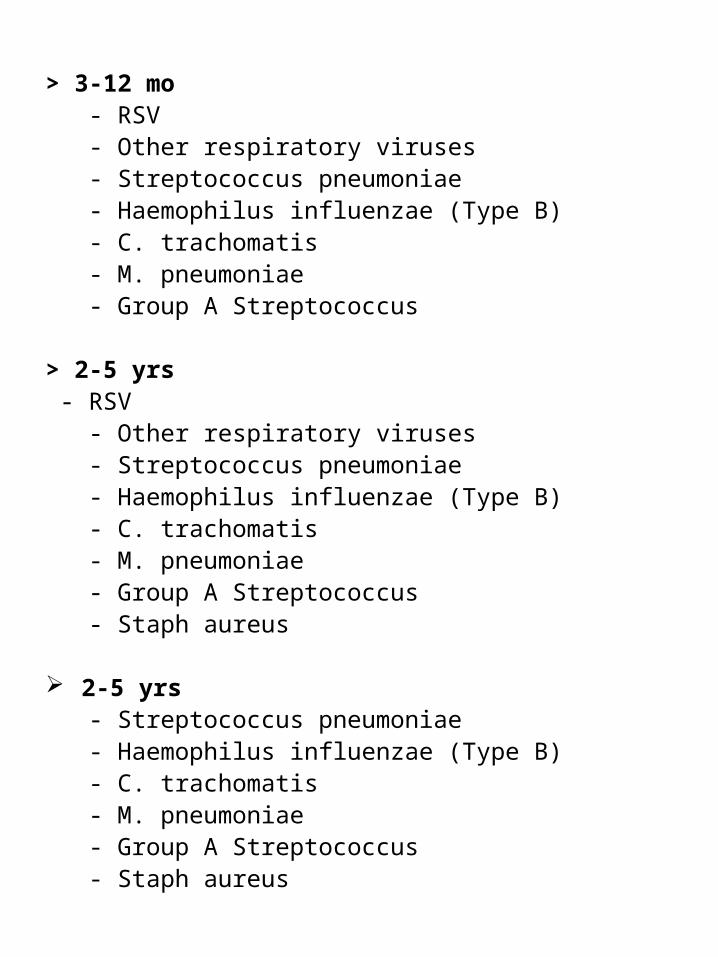
> 3-12 mo - RSV - Other respiratory viruses - Streptococcus pneumoniae - Haemophilus influenzae (Type B) - C. trachomatis - M. pneumoniae - Group A Streptococcus
> 2-5 yrs - RSV - Other respiratory viruses - Streptococcus pneumoniae - Haemophilus influenzae (Type B) - C. trachomatis - M. pneumoniae - Group A Streptococcus - Staph aureus
2-5 yrs - Streptococcus pneumoniae - Haemophilus influenzae (Type B) - C. trachomatis - M. pneumoniae - Group A Streptococcus - Staph aureus

Den
gu
e P
ath
op
hys
iolo
gy
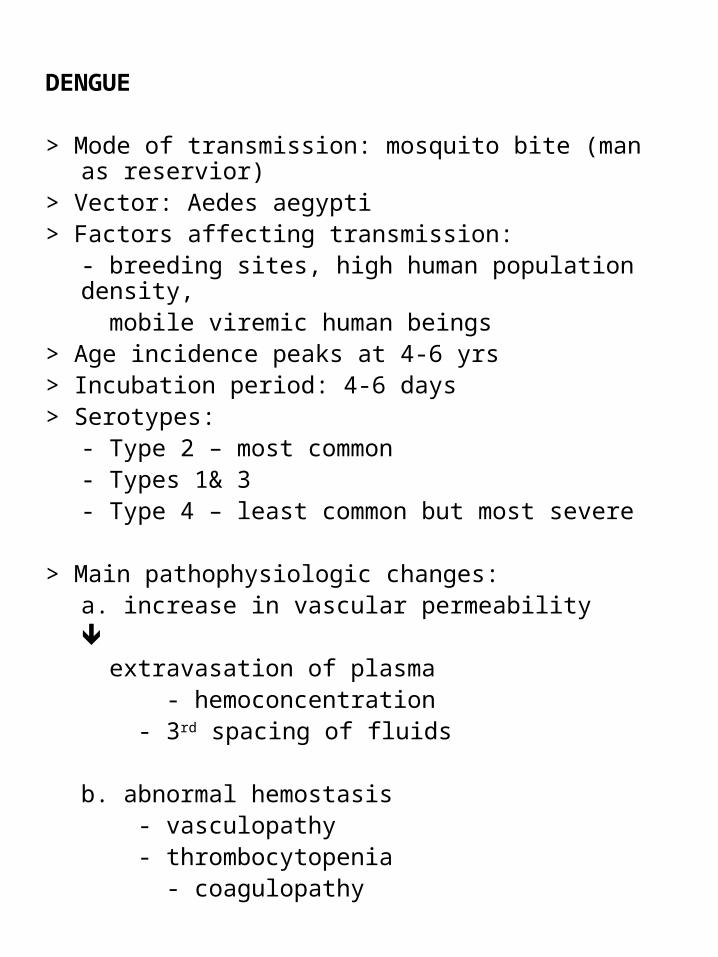
DENGUE
> Mode of transmission: mosquito bite (man as reservior)> Vector: Aedes aegypti> Factors affecting transmission:
- breeding sites, high human population density, mobile viremic human beings
> Age incidence peaks at 4-6 yrs> Incubation period: 4-6 days> Serotypes:
- Type 2 – most common- Types 1& 3- Type 4 – least common but most severe
> Main pathophysiologic changes:a. increase in vascular permeability
extravasation of plasma
- hemoconcentration - 3rd spacing of fluids
b. abnormal hemostasis - vasculopathy - thrombocytopenia
- coagulopathy
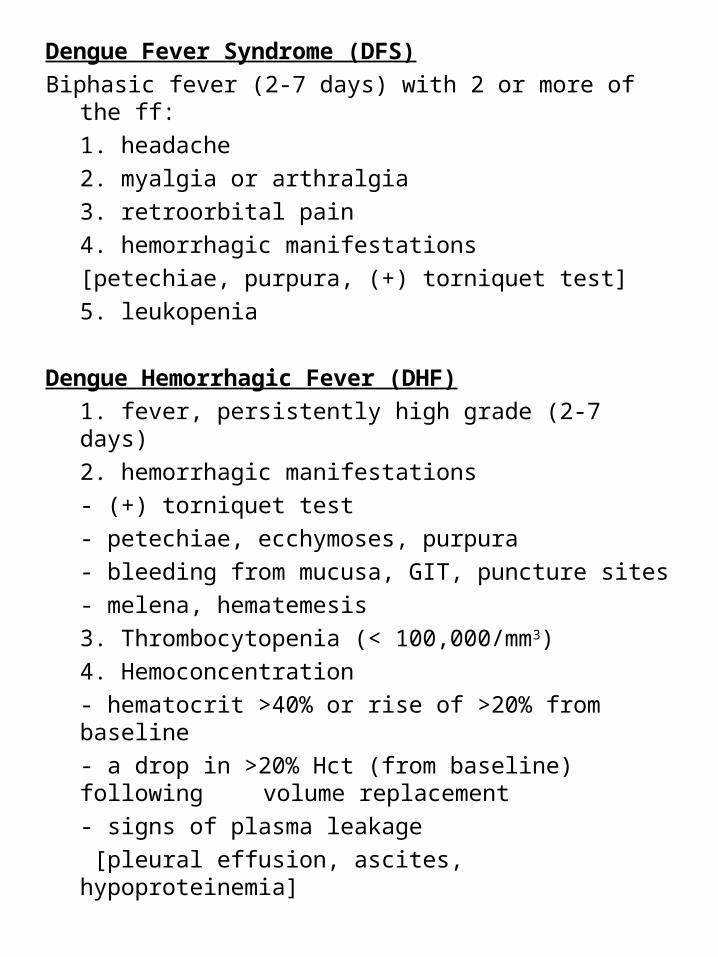
Dengue Fever Syndrome (DFS)
Biphasic fever (2-7 days) with 2 or more of the ff:
1. headache
2. myalgia or arthralgia
3. retroorbital pain
4. hemorrhagic manifestations
[petechiae, purpura, (+) torniquet test]
5. leukopenia
Dengue Hemorrhagic Fever (DHF)
1. fever, persistently high grade (2-7 days)
2. hemorrhagic manifestations
- (+) torniquet test
- petechiae, ecchymoses, purpura
- bleeding from mucusa, GIT, puncture sites
- melena, hematemesis
3. Thrombocytopenia (< 100,000/mm3)
4. Hemoconcentration
- hematocrit >40% or rise of >20% from baseline
- a drop in >20% Hct (from baseline) following volume replacement
- signs of plasma leakage
[pleural effusion, ascites, hypoproteinemia]
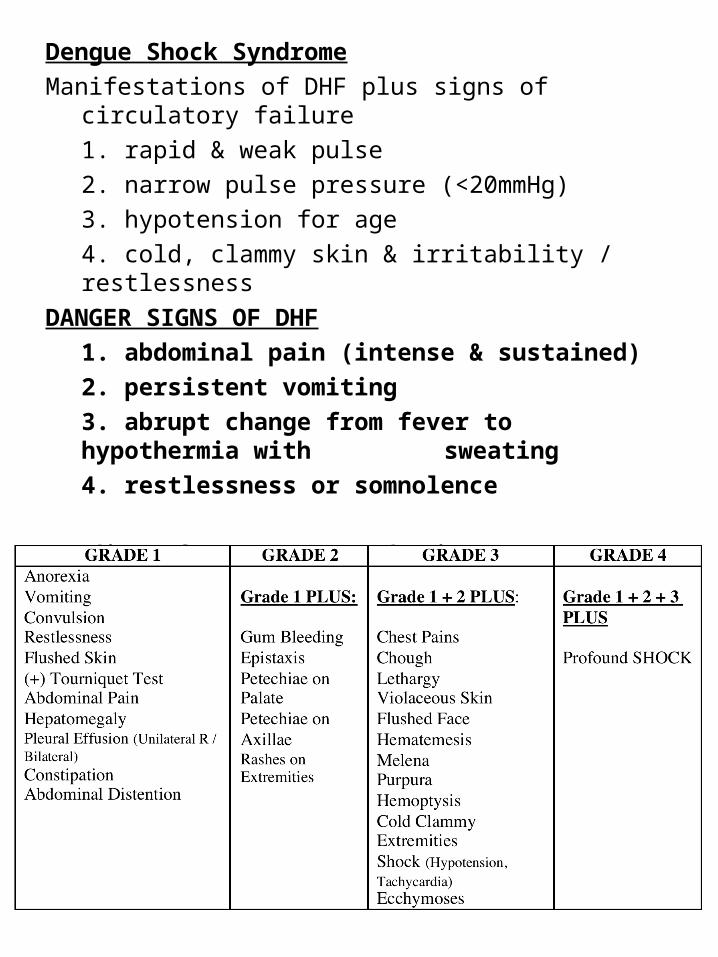
Dengue Shock Syndrome
Manifestations of DHF plus signs of circulatory failure
1. rapid & weak pulse
2. narrow pulse pressure (<20mmHg)
3. hypotension for age
4. cold, clammy skin & irritability / restlessness
DANGER SIGNS OF DHF
1. abdominal pain (intense & sustained)
2. persistent vomiting
3. abrupt change from fever to hypothermia with sweating
4. restlessness or somnolence
Grading of Dengue Hemorrhagic Fever

Torniquet Test: SBP + DBP = mean BP for 5 minutes
2
if ≥20 petechial rash per sq. inch on antecubital fossa
(+) test
Herman’s Rash:
> usually appears after fever lysed
> initially appears on the lower extremities
> not a common finding among dengue patients
> “an island of white in an ocean of red”
Recommended Guidelines for Transfusion:
Transfuse:
- PC < 100,000 with signs of bleeding
- PC < 20,000 even if asymptomatic
- use FFP if without overt bleeding
- FWB in cases with overt bleeding or signs of hypovolemia
> if PT & PTT are abnormal: FFP
> if PTT only: cryprecipitate
Leukopenia in dengue: probable etiology is Pseudomonas
therefore: give Meropenem or Ceftazidime
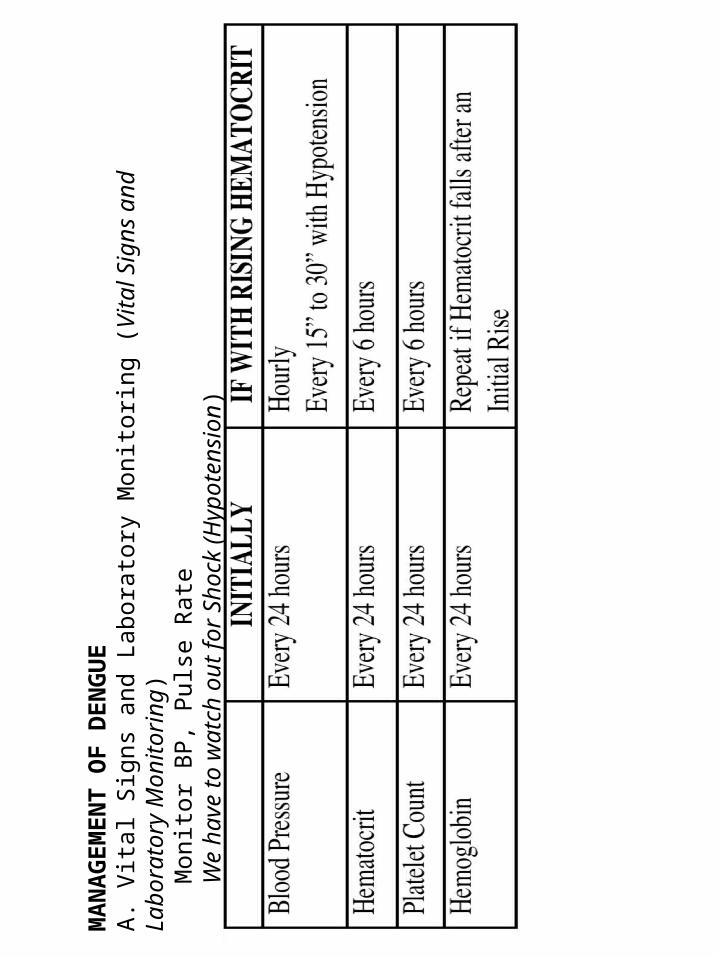
MA
NA
GE
ME
NT
OF
DE
NG
UE
A.
Vita
l Sig
ns a
nd L
abor
ator
y M
onito
ring
(Vita
l Sig
ns a
nd L
abor
ator
y M
onito
ring)
Mon
itor
BP
, P
ulse
Rat
eW
e ha
ve t
o w
atch
out
for
Sho
ck (
Hyp
oten
sion
)
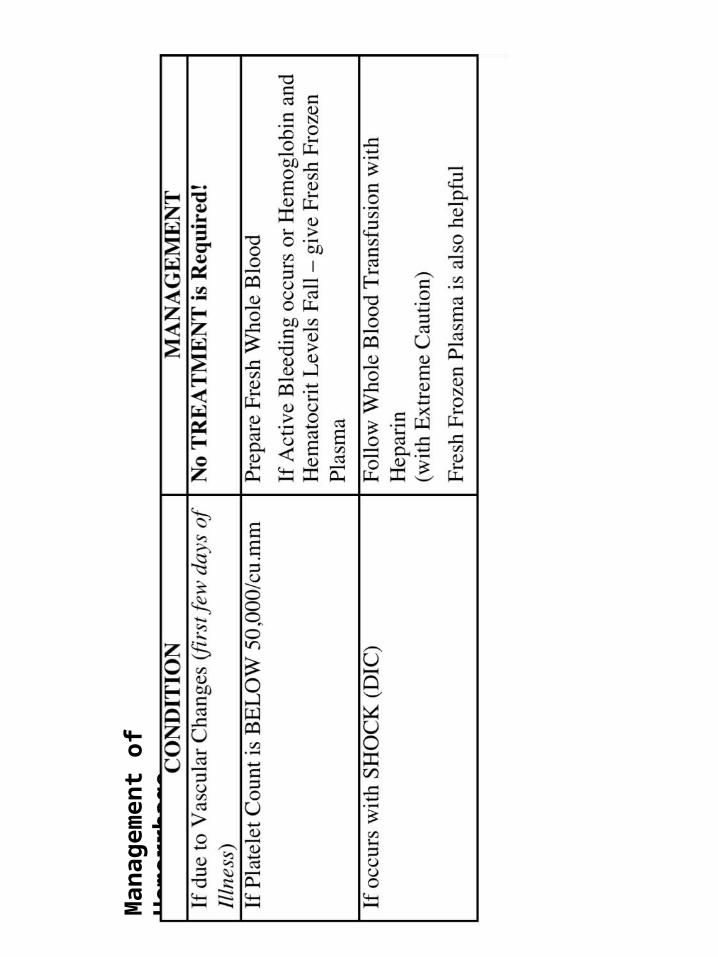
Man
agem
ent o
f Hem
orrh
age
URINARY TRACT INFECTION
Suggestive UTI:
- Pyuria: WBC ≥ 5/HPF or 10mm3
- Absence of pyuria doesn’t rule out UTI
- Pyuria can be present w/o UTI
Presumptive UTI:
- (-) urine culture
- lower colony counts may be due to:
* overhydration
* recent bladder emptying
* previous antibiotic intake
Proven or Confirmed UTI:
- (+) urine culture ≥ 100,000 cfu/mL urine of a single organism
- multiple organisms in culture may indicate a contaminated sample
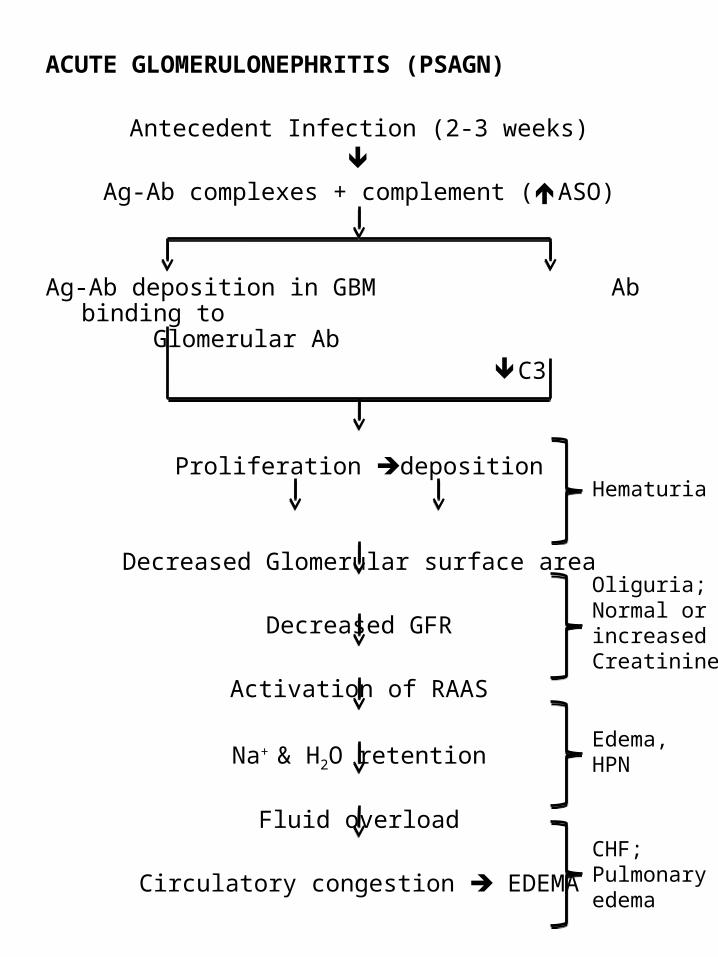
ACUTE GLOMERULONEPHRITIS (PSAGN)
Antecedent Infection (2-3 weeks)
Ag-Ab complexes + complement (ASO)
Ag-Ab deposition in GBM Ab binding to Glomerular Ab
C3
Proliferation deposition
Decreased Glomerular surface area
Decreased GFR
Activation of RAAS
Na+ & H2O retention
Fluid overload
Circulatory congestion EDEMA
Hematuria
Oliguria;Normal or increased Creatinine
Edema,HPN
CHF;Pulmonary edema
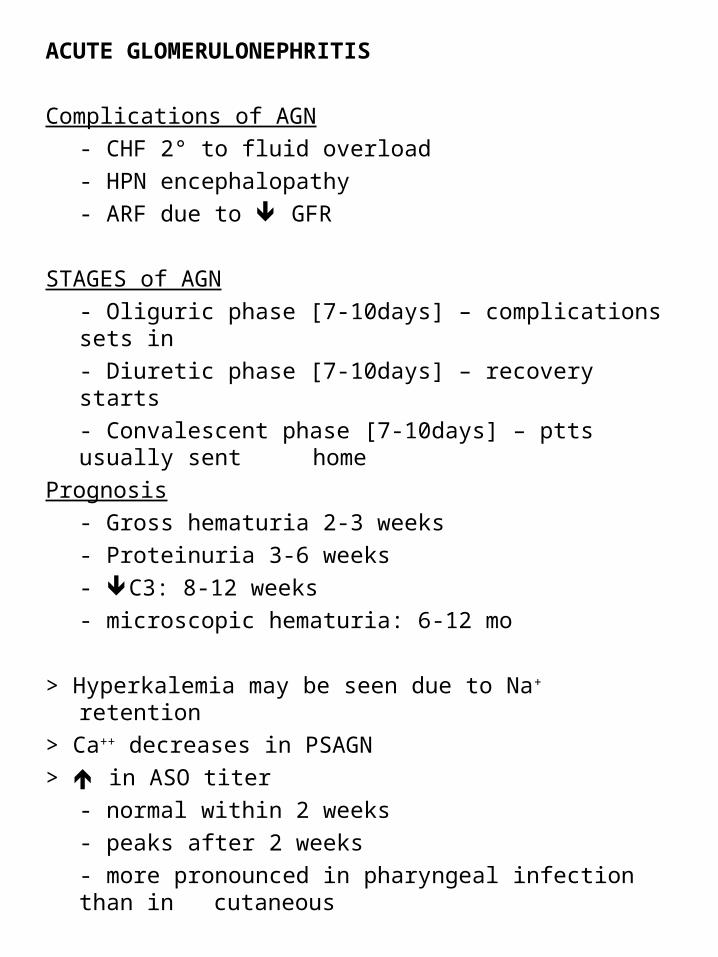
ACUTE GLOMERULONEPHRITIS
Complications of AGN
- CHF 2° to fluid overload
- HPN encephalopathy
- ARF due to GFR
STAGES of AGN
- Oliguric phase [7-10days] – complications sets in
- Diuretic phase [7-10days] – recovery starts
- Convalescent phase [7-10days] – ptts usually sent home
Prognosis
- Gross hematuria 2-3 weeks
- Proteinuria 3-6 weeks
- C3: 8-12 weeks
- microscopic hematuria: 6-12 mo
> Hyperkalemia may be seen due to Na+ retention
> Ca++ decreases in PSAGN
> in ASO titer
- normal within 2 weeks
- peaks after 2 weeks
- more pronounced in pharyngeal infection than in cutaneous
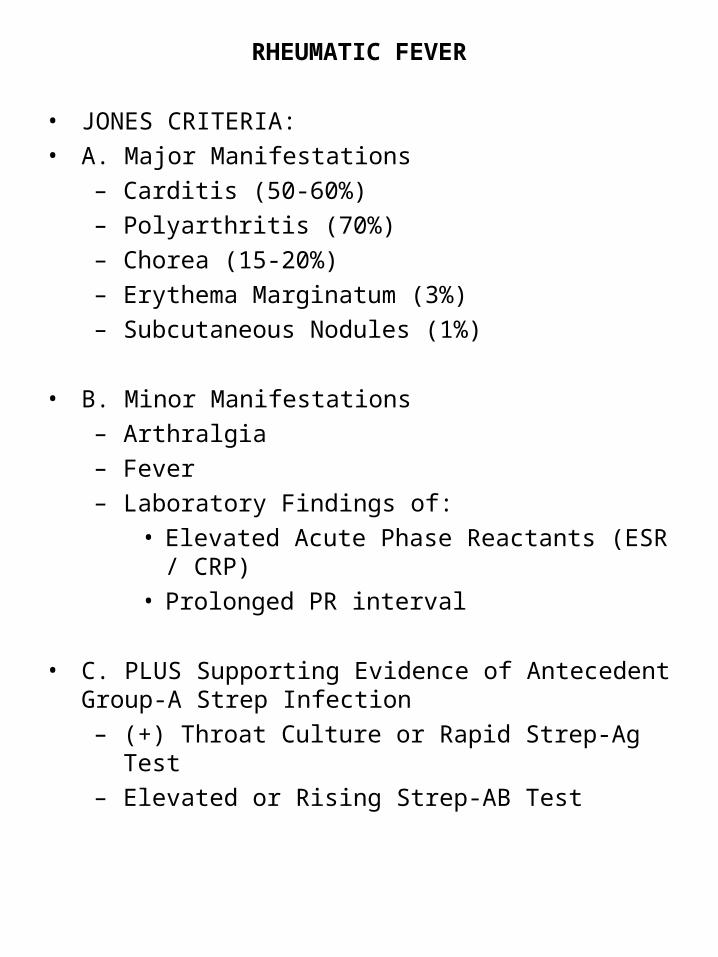
RHEUMATIC FEVER
• JONES CRITERIA:
• A. Major Manifestations
– Carditis (50-60%)
– Polyarthritis (70%)
– Chorea (15-20%)
– Erythema Marginatum (3%)
– Subcutaneous Nodules (1%)
• B. Minor Manifestations
– Arthralgia
– Fever
– Laboratory Findings of:
• Elevated Acute Phase Reactants (ESR / CRP)
• Prolonged PR interval
• C. PLUS Supporting Evidence of Antecedent Group-A Strep Infection
– (+) Throat Culture or Rapid Strep-Ag Test
– Elevated or Rising Strep-AB Test
TREATMENT OF RHEUMATIC FEVER
• A. Antibiotic Therapy
– 10 days of Oral Penicillin or Erythromycin
– IM Injection of Benzethine Penicillin
• **NOTE: Sumapen = Oral Penicillin!
• B. Anti-Inflammatory Therapy
• 1. Aspirin (if Arthritis, NOT Carditis)
• Acute: 100mg/kg/day in 4 doses x 3-5days
• Then, 75mg/kg/day in 4 doses x 4 weeks
• 2. Prednisone
• 2mg/kg/day in 4 doses x 2-3weeks
• Then, 5mg/24hrs every 2-3 days
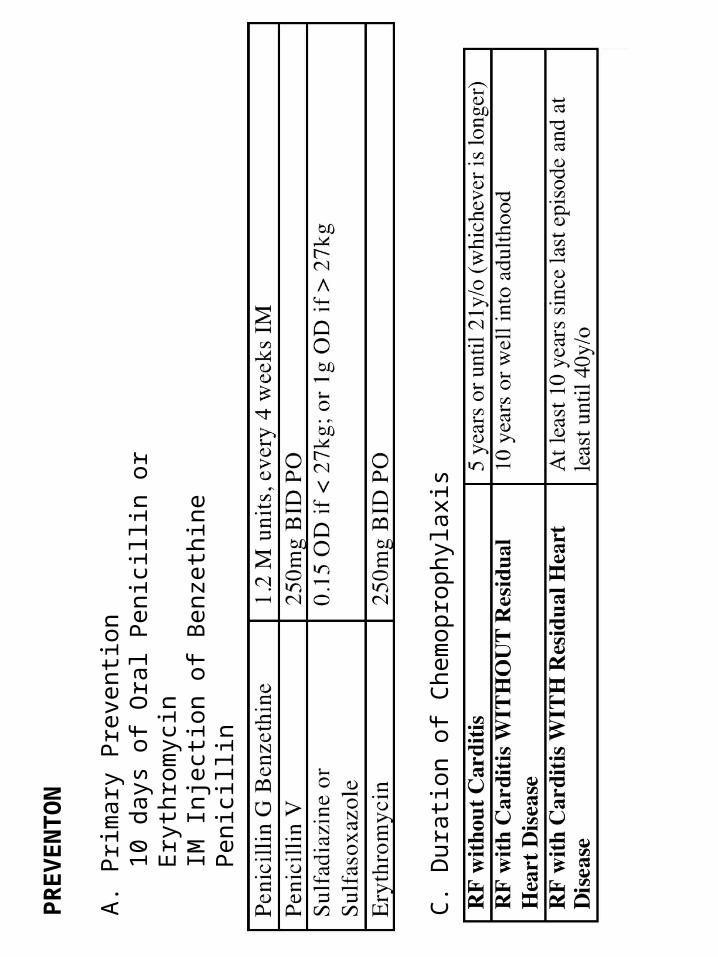
PR
EV
EN
TO
N
A.
Prim
ary
Pre
vent
ion
10 d
ays
of O
ral P
enic
illin
or
Ery
thro
myc
inIM
Inj
ectio
n of
Ben
zeth
ine
Pen
icill
in
B.
Sec
onda
ry P
reve
ntio
n
C.
Dur
atio
n of
Che
mop
roph
ylax
is
KAWASAKI DISEASE
CDC-CRITERIA FOR DIAGNOSIS: ADOPTED FROM KAWASAKI (ALL SHOULD BE PRESENT)
A) HIGH Grade Fever (>38.5 Rectally) PRESENT for AT LEAST 5-days without other Explanation
“High Grade Fever of at least 5 days”
DOES NOT Respond to any kind of Antibiotic!
B) Presence of 4 of the 5 Criteria:
1) Bilateral CONGESTION of the Ocular Conjunctiva (seen in 94%)
2) Changes of the Lips and Oral Cavity (At least ONE)
3) Changes of the Extremities (At least ONE)
4) Polymorphous Exanthem (92%)
5) Cervical Adenopathy = Non-Suppurative Cervical Adenopathy (should be >1.5cm) in 42%
KAWASAKI DISEASE
HARADA Criteria
- used to determine whether IVIg should be given
- assessed within 9 days from onset of illness
1. WBC > 12,000
2. PC <350,000
3. CRP > 3+
4. Hct <35%
5. Albumin <3.5 g/dL
6. Age 12 months
7. Gender: male
•IVIg is given if ≥ 4 of 7 are fulfilled
•If < 4 with continuing acute symptoms, risk score must be reassessed daily
TREATMENT: Currently Recommended Protocol:
A. IV-Immunoglobulin
2g/kg Regimen Infusion EQUALLY Effective in Prevention of Aneurysms and Superior to 4-day Regimen with respect to Amelioration of Inflammation as measured by days of Fever, ESR, CRP, Platelet Count, Hgb, and Albumin.
NOTE: There is a TIME FRAME of 10 days
B. Aspirin
HIGH Dose ASA (80-100mg/kg/day divided q 6h) should be given Initially in Conjunction with IV-IG
THEN
Reduced to Low Dose Aspirin (3-5mg/kg/day)
AND
Continued until Cardiac Evaluation COMPLETED
(approximately 1-2 months AFTER Onset of Disease)
SEIZURES
> Seizures: sudden event caused by abrupt, uncontrolled, hypersynchronous discharges of neurons
> Epilepsy: tendency for recurrent seizures that are unprovoked by an immediate cause
> Status epilepticus: >30min or back-to-back w/o return to baseline
> Etiology:
- V ascular : AVM, stroke, hemorrhage
- I nfections : meningitis, encephalitis
- T raumatic :
- A utoimmune : SLE, vasculitis, ADEM
- M etabolic : electrolyte imbalance
- I diopathic : “idiopathic epilepsy”
- N eoplastic : space occupying lesion
- S tructural : cortical malformation, prior stroke
- S yndrome : genetic disorder
TYPES OF SEIZURES
A. Partial Seizures (Focal / Local)
– Simple Partial
– Complex Partial (Partial Seizure + Impaired Consciousness)
– Partial Seizures evolving to Tonic-Clonic Convulsion)
B. Generalized Seizures
– Absence (Petit mal)
– Myoclonic
– Clonic
– Tonic
– Tonic-Clonic
– Atonic
SIMPLE FEBRILE SEIZURE vs. COMPLEX FEBRILE SEIZURE
Febrile Seizure: “A seizure in association with a febrile illness in the absence of a CNS infection or acute electrolyte imbalance in children older than 1 month of age without prior afebrile seizures”
CLASSIFICATION BY CAUSE
A. Acute Symptomatic (shortly after an acute insult)
– Infection
– Hypoglycemia, low sodium, low calcium
– Head trauma
– Toxic ingestion
B. Remote Symptomatic
– Pre-existing brain abnormality or insult
– Brain injury (head trauma, low oxygen)
– Meningitis
– Stroke
– Tumor
– Developmental brain abnormality
C. Idiopathic
– No history of preceding insult
– Likely “genetic” component
SIMPLE FEBRILE SEIZURE
A. Criteria for an SFS
– < 15 minutes
– Generalized-tonic-clonic
– Fever > 100.4 rectal to 101 F (38 to 38.4 C)
– No recurrence in 24 hours
– No post-ictal neuro abnormalities (e.g. Todd’s paresis)
– Most common 6 months to 5 years
– Normal development
– No CNS infection or prior afebrile seizures
B. Risk Factors
– Febrile seizure in 1st/2nd degree relative
– Neonatal nursery stay of >30 days
– Developmental delay
– Height of temperature
C. Risk Factors for Epilepsy (2 to 10% will go on to have epilepsy)
– Developmental delay
– Complex FS (possibly > 1 complex feature)
– 5% > 30 mins => _ of all childhood status
– Family History of Epilepsy
– Duration of fever
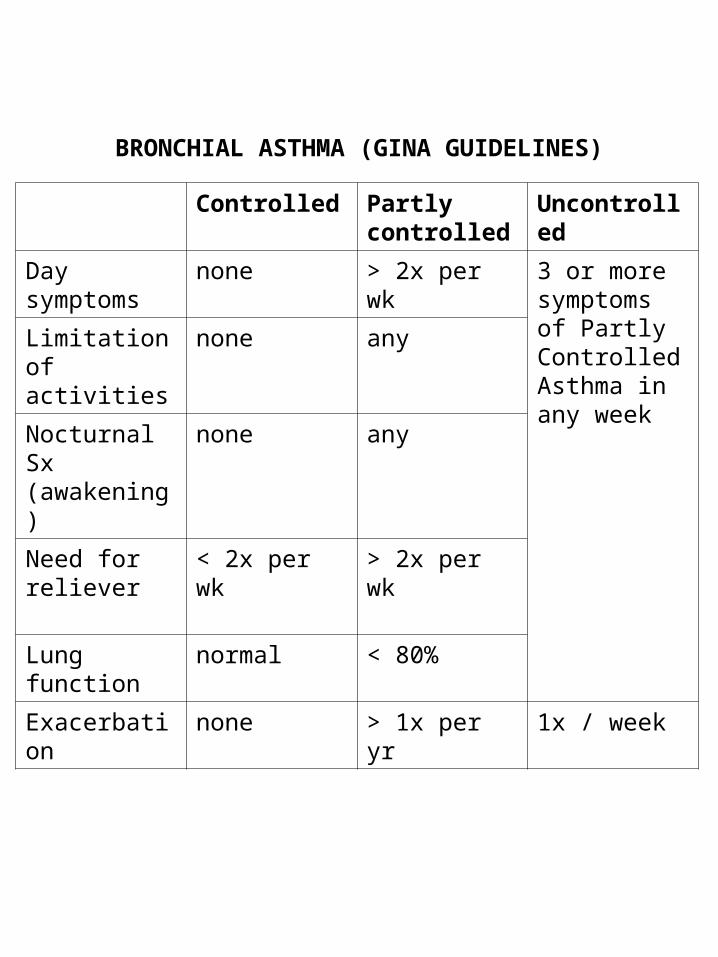
BRONCHIAL ASTHMA (GINA GUIDELINES)
Controlled Partly controlled
Uncontrolled
Day symptoms
none > 2x per wk 3 or more symptoms of Partly Controlled Asthma in any week
Limitation of activities
none any
Nocturnal Sx (awakening)
none any
Need for reliever
< 2x per wk > 2x per wk
Lung function normal < 80%
Exacerbation none > 1x per yr 1x / week
Tuberculosis (Treatment)I. Pulmonary TB
A. Fully susceptible M. tuberculosis, no history of previous anti-TB drugs, low local persistence of primary resistance to Isoniazid (H)
2HRZ OD then 4HR OD or 3x/wk DOT
B. Microbial susceptibility unknown or initial drug resistance suspected (e.g. cavitary), previous anti-TB use, close contact w/ resistant source case or living in high areas w/ high pulmonary resistance to H.
2HRZ + E/S OD, then 4 HR + E/S OD or 3x/wekk DOT
I. Extrapulmonary TB
Same in PTB
For severe life threatening disease (e.g. miliary, meningitis, bone, etc)
☤ 2HRZ + E/S OD, then 10HR + E/S OD or 3x/wk DOT
H.E.A.D.S.S.S.Home Environment☤ With whom does the adolescent live?☤ Any recent changes in the living situation?☤ How are things among siblings?☤ Are parents employed?☤ Are there things in the family he/she wants to change?
Employment and Education☤ Currently at school? Favorite subjects?☤ Patient performing academically?☤ Have been truant/expelled from school?☤ Problems with classmates/teachers?☤ Currently employed?☤ Future education/employment goals?
Activities☤ What he/she does in spare time?☤ Patient does for fun?☤ Whom does patient spend spare time?☤ Hobbies, interests, close friends?
H.E.A.D.S.S.S.Drugs☤ Used tobacco/alcohol/steroids?☤ Illicit drugs? Frequency? Amount? Affected daily activiities?☤ Still using? Friends using/selling?
Sexual activities☤ Sexual orientation?☤ GF/BF? Typical date?☤ Sexually active? When started? # of persons?
Contraceptives? Pregnancies? STDs?
Suicide/Depression☤ Ever sad/tearful/unmotivated/hopeless?☤ Thought of hurting self/others?☤ Suicide plans?
Safety☤ Use seatbelts/helmets?☤ Enter into high risk situations?☤ Member of frat/sorority/orgs?☤ Firearm at home?
Respiratory Distress Syndrome(Hyaline Membrane Disease)
☤ Male, preterm, low BW, maternal DM, & perinatal asphyxia☤ Corticosteroids:
• most successful method to induce fetal lung maturation• Administered 24-48 hours before delivery decrease incidence
of RDS• Most effective before 34 weeks AOG
☤ Microscopically: diffuse atelectasis, eosinophilic membrane
Pathophysiology:1. Impaired/delayed surfactant synthesis & secretion2. V/Q (ventilation/perfusion) imbalance due to deficiency of
surfactant and decreased lung compliance3. Hypoxemia and systemic hypoperfusion4. Respiratory and metabolic acidosis5. Pulmonary vasoconstriction6. Impaired endothelial &epithelial integrity7. Proteinous exudate8. RDS
Respiratory Distress Syndrome(Hyaline Membrane Disease)
Clinical Features:1. Tachypnea, nasal flaring, subcostal and intercostal
retractions, cyanosis, grunting2. Pallor – from anemia, peripheral vasoconstriction3. Onset – within 6 hours of life
Peak severity – days 2-3Recovery – 72 hours
Retractions:☤ Due to (-) intrapleural pressure produced by interaction b/w
contraction of diaphragm & other respiratory muscles and mechanical properties of the lungs & chest wall
Nasal flaring:☤ Due to contraction of alae nasi muscles leading to marked reduction
in nasal resistanceGrunting:☤ Expiration through partially closed vocal cordsInitial expiration: glottis closedlungs w/ gasinc. transpulmo P w/o
airflowLast part of expiration: gas expelled against partially closed cordsCyanosis:☤ Central – tongue & mnucosa (imp. Indicator of impaired gas
exchange); depends on total amount of desaturated Hgb

F.R.I.C.H.M.O.N.D.
☤Fluids
☤Respiration
☤ Infection
☤Cardiac
☤Hematologic
☤Metabolic☤Output & Input [cc/kg/h] N: 1-2
☤Neuro
☤Diet




























