-
8/4/2019 pedia cardio
1/95
PEDIATRIC CARDIOVASCULAR
DISORDERS
Mr. Erwin U. Imperio
-
8/4/2019 pedia cardio
2/95
VARIATIONS FROM THE ADULT
Fetal Circulation
Characteristics:
Placenta is the source of oxygen for the fetus
Fetal lungs receive
-
8/4/2019 pedia cardio
3/95
-
8/4/2019 pedia cardio
4/95
NORMAL CIRCULATORY CHANGES AT
BIRTH
When the umbilical cord is clamped or
severed, the blood supply from the placenta is
cut-off, and oxygenation must then take place
in the newborns lungs
As the lungs expand with the air, the
pulmonary artery pressure decreases and
circulation lungs increases
-
8/4/2019 pedia cardio
5/95
STRUCTURAL CHANGES
DUCTUS VENOSUS
After the umbilical cord is severed, flow to the
ductus venosus decreases, and eventually ceases
Constricts within 3-7 days after birth
Becomes ligamentum venosum
-
8/4/2019 pedia cardio
6/95
STRUCTURAL CHANGES
FORAMEN OVALE
Functional closure occurs when:
Pressure in the LA exceeds pressure in the right
Expansion of PA causes a drop in PA pressure and RA
and RV pressure
Increased pulmonary blood flow to the LA and aortic
pressure = increased LA and LV pressure
Anatomical closure occurs:
Within 1st week after birth with the deposit of fibrin
-
8/4/2019 pedia cardio
7/95
STRUCTURAL CHANGES
DUCTUS ARTERIOSUS
Increase aortic blood flow = increase aortic pressure =decrease
right-to-left shunt
Increase pulmonary blood flow = increase arterialoxygen =
vasoconstriction within hours of birth
Functional closure occurs:
24 hours after birth when vasoconstriction causes cessationof
blood flow
Anatomical closure: 1-3 weeks when there is growth of fibrous
tissue in the
lumen of ductus arteriosus
-
8/4/2019 pedia cardio
8/95
ABNORMAL CIRCULATORY PATTERNS
AFTER BIRTH
This may happen as a result of abnormal
openings between pulmonary and systemic
circulations
-
8/4/2019 pedia cardio
9/95
ASSESSMENT
Family History : genetic problems
Pregnancy History:
Rubella
Viral infections
Medications
X-ray exposure
Alcohol ingestion
Cigarette smoking
-
8/4/2019 pedia cardio
10/95
ASSESSMENT
Childs health history
Presenting problem
Feeding problems
Failure to thrive
Respiratory difficulties
Color changes
Activity intolerance
Past medical history
Rheumatic fever
-
8/4/2019 pedia cardio
11/95
ASSESSMENT
Physical Examination
Plot height and weight
Measure VS (especially BP and RR)
Inspect for chest enlargement Inspect for presence of
cyanosis
Inspect for clubbing of finger
Observe for distended neck veins Palpate/percuss quality and
symmetry of pulses,
size of liver and spleen, presence of thrill
-
8/4/2019 pedia cardio
12/95
ASSESSMENT
Physical Examination
Auscultate for abnormal heart sounds / murmurs
Innocent: no anatomic or physiologic abnormality
Functional: no anatomic defect, but may be caused by a
physiologic abnormality
Organic: caused by structural abnormality
-
8/4/2019 pedia cardio
13/95
LABORATORY / DIAGNOSTIC TESTS
CXR
MRI
ECG Hematologic testing
-
8/4/2019 pedia cardio
14/95
LABORATORY / DIAGNOSTIC TESTS
Cardiac Catheterization
Access: femoral vein
Nursing Care: Pre-test
Prepare child based on developmental level Administer
medications as ordered
Nursing Care: Post-test
Check extremity distal to the catheterization site for:
Color Temperature
Pulse
Capillary refill
-
8/4/2019 pedia cardio
15/95
LABORATORY / DIAGNOSTIC TESTS
Cardiac Catheterization
Nursing Care: Post-test
Keep extremity distal to the catheterization site
extended for 6 hours
Check pressure dressing over catheterization site for
bleeding
-
8/4/2019 pedia cardio
16/95
NURSING DIAGNOSIS
Altered growth and development: failure tothrive
High risk for injury: physiologic
Activity intolerance Altered nutrition: less than body
requirements Fear/anxiety: child and family
Risk for infection Decreased cardiac output Fluid volume
excess
-
8/4/2019 pedia cardio
17/95
PLANNING AND IMPLEMENTATION
Tissue will be adequately oxygenated
Child will achieve normal growth and
development milestones
Child will be free from symptoms of
complications of heart disease
Parents will understand childs condition
-
8/4/2019 pedia cardio
18/95
CARE OF A PEDIATRIC CLIENT WITH
CONGENITAL HEART DISEASE
-
8/4/2019 pedia cardio
19/95
BLOOD CIRCULATION
-
8/4/2019 pedia cardio
20/95
FIRST CLASSIFICATION
ACYANOTIC
Left-to-right shunts
Oxygenated tounoxygenated blood
CYANOTIC
Right-to-left shunts
Deoxygenated tooxygenated blood
-
8/4/2019 pedia cardio
21/95
SECOND CLASSIFICATION
Increased pulmonary blood flow
Ventricular Septal Defect
(VSD)
Atrial Septal Defect (ASD)
Atrioventricular canal defect
Patent Ductus Arteriosus
(PDA)
Decreased pulmonary blood flow
Tricuspid Atresia
Tetralogy of Fallot
-
8/4/2019 pedia cardio
22/95
SECOND CLASSIFICATION
Mixed blood flow
Transposition of the great
arteries
Total anomalous pulmonary
venous return
Truncus arteriosus
Hypoplastic left heartsyndrome
Obstruction to blood flow
Pulmonary stenosis
Aortic stenosis Coarctation of the aorta
-
8/4/2019 pedia cardio
23/95
INCREASED PULMONARY BLOOD
FLOW
-
8/4/2019 pedia cardio
24/95
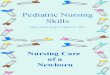
VENTRICULAR SEPTAL DEFECT
ILLUSTRATION description
Opening present in the
septum between two
ventricles
Left-to-right shunt
(acyanotic)
Results into RV hypertrophy
-
8/4/2019 pedia cardio
25/95
ATRIAL SEPTAL DEFECT
ILLUSTRATION description
Opening present between
two atria
Left-to-right shunt
(acyanotic)
Results into RV hypertrophy
-
8/4/2019 pedia cardio
26/95
ATRIOVENTRICULAR SEPTAL DEFECT
ILLUSTRATION description
Endocardial cushion
defect
Left-to-right shunt
Blood may flow between all
four heart chambers
Seen in 50% of children withDown Syndrome
Leads to RV hypertrophy
-
8/4/2019 pedia cardio
27/95
PATENT DUCTUS ARTERIOSUS (PDA)
Patent ductus arteriosus description
Results from failure to close
at birth
Left-to-right shunt
Leads to RV hypertrophy
-
8/4/2019 pedia cardio
28/95
ASSESSMENT FINDINGS
CHF:
Tachypnea, tachycardia
Hepatomegaly
Feeding difficulties
FTT
Activity intolerance
-
8/4/2019 pedia cardio
29/95
MANAGEMENT
CONGENITAL HEART DEFECTS
VSD
MEDICAL
CHF Management
Digoxin and diuretics
Avoid oxygen
Increase caloric intake
Infective endocarditis
prophylaxis 6 months aftersurgery / ventricular device
occluder
-
8/4/2019 pedia cardio
30/95
MANAGEMENT
CONGENITAL HEART DEFECTS
VSD
SURGICAL
Cardiac catheterization for
placement of ventricular
occlusion
Usually repaired after age 1
Approaches:
One-stage
Patch closure
Two-stages
PA banding to restrict
pulmonary blood flow
Patch close of VSD, removal
of PA banding
-
8/4/2019 pedia cardio
31/95
MANAGEMENT
CONGENITAL HEART DEFECTS
ASD
MEDICAL
CHF Management
Digoxin and diuretics
Infective endocarditis
prophylaxis 6 months after
surgery / atrial device
occluder
-
8/4/2019 pedia cardio
32/95
MANAGEMENT
CONGENITAL HEART DEFECTS
ASD
SURGICAL
Cardiac catheterization for
placement of atrial
occlusion
Primary repair: suture
closure of ASD
Patch repair of ASD
-
8/4/2019 pedia cardio
33/95
MANAGEMENT
CONGENITAL HEART DEFECTS
PDA
MEDICAL
CHF Management
Digoxin and diuretics
Infective endocarditis
prophylaxis 6 months after
surgery coil occlusion
-
8/4/2019 pedia cardio
34/95
MANAGEMENT
CONGENITAL HEART DEFECTS
PDA
SURGICAL
Cardiac catheterization
Small PDAs; coil occlusion
Large PDAs: closure device
PDA ligation
-
8/4/2019 pedia cardio
35/95
DISORDERS WITH OBSTRUCTION TO
BLOOD FLOW
-
8/4/2019 pedia cardio
36/95
PULMONARY STENOSIS
ILLUSTRATION description
Inability of RV to evacuate
blood by way of PA
Results into RV hypertrophy
-
8/4/2019 pedia cardio
37/95
AORTIC STENOSIS
ILLUSTRATION description
Inability of LV to evacuate
blood by way of aortic valve
Results into LV hypertrophy
-
8/4/2019 pedia cardio
38/95
COARCTATION OF THE AORTA
ILLUSTRATION description
Narrowing of the lumen of
the aorta due to a
constricting band
Two locations:
Preductal (bet. subclavian
artery and ductus arteriosus)
Postductal (distal to ductusarteriosus)
Results into increase BP
proximal to coarctation and
decrease distal to it
-
8/4/2019 pedia cardio
39/95
ASSESSMENT FINDINGS
Pulmonary Stenosis
Hypoxia
Tachypnea
RV failure
Activity intolerance
-
8/4/2019 pedia cardio
40/95
ASSESSMENT FINDINGS
Aortic Stenosis
Severe CHF
Tachypnea
Faint peripheral pulses, poor perfusion, poor
capillary refill, cool skin
Poor feeding
Activity intolerance
-
8/4/2019 pedia cardio
41/95
ASSESSMENT FINDINGS
Coarctation of the Aorta
Hypertesion in the upper extremities, with absent
or weak femoral pulses
Nosebleeds
Headaches
Leg cramps
-
8/4/2019 pedia cardio
42/95
MANAGEMENT
CONGENITAL HEART DEFECTS
Pulmonary Stenosis
MEDICAL
PGE1 infusion
Intubation and ventilation
Inotropics
Infective endocarditis
prophylaxis
-
8/4/2019 pedia cardio
43/95
MANAGEMENT
CONGENITAL HEART DEFECTS
Pulmonary Stenosis
SURGICAL
Balloon pulmonary
valvuloplasty
Valvotomy or valvectomy
-
8/4/2019 pedia cardio
44/95
MANAGEMENT
CONGENITAL HEART DEFECTS
Aortic Stenosis
MEDICAL
PGE1 infusion
Intubation and ventilation
Inotropics
Infective endocarditis
prophylaxis
-
8/4/2019 pedia cardio
45/95
MANAGEMENT
CONGENITAL HEART DEFECTS
Aortic Stenosis
SURGICAL
Cardiac catheterization
Aortic balloon valvuloplasty
Aortic balloon angioplasty
Valvotomy
-
8/4/2019 pedia cardio
46/95
MANAGEMENT
CONGENITAL HEART DEFECTS
Coarctation of the Aorta
MEDICAL
PGE1 infusion
Intubation and ventilation
Infective endocarditis
prophylaxis
Anticongestive therapy
-
8/4/2019 pedia cardio
47/95
MANAGEMENT
CONGENITAL HEART DEFECTS
Coarctation of the Aorta
SURGICAL
Balloon angioplasty
End-to-end anastomosis
-
8/4/2019 pedia cardio
48/95
DISORDERS WITH MIXED BLOOD
FLOW
-
8/4/2019 pedia cardio
49/95
TRANSPOSITION OF GREAT ARTERIES
ILLUSTRATION description
Aorta rises from the RV
instead of the left
Pulmonary artery arises
from the LV instead of right
TOTAL ANOMALOUS PULMONARY
-
8/4/2019 pedia cardio
50/95
TOTAL ANOMALOUS PULMONARY
VENOUS RETURN
ILLUSTRATION description
PV returns to the Ra or the
superior vena cava instead
of the LA
-
8/4/2019 pedia cardio
51/95
TRUNCUS ARTERIOSUS
ILLUSTRATION description
ONE major trunk arises
from the LV and RV in place
of separate aorta and
pulmonary artery vessels
-
8/4/2019 pedia cardio
52/95
ASSESSMENT FINDINGS
Transposition of Great Arteries
Cyanosis
Tachypnea
CHF
Feeding difficulties
-
8/4/2019 pedia cardio
53/95
ASSESSMENT FINDINGS
Total Anomalous Pulmonary Venous Return
Cyanostic
Activity intolerance
Signs of RSHF
-
8/4/2019 pedia cardio
54/95
ASSESSMENT FINDINGS
Truncus Arteriosus
Cyanotic
-
8/4/2019 pedia cardio
55/95
MANAGEMENT
CONGENITAL HEART DEFECTS
Transposition of great
arteries
MEDICAL
PGE1 infusion
Anticongestive drugs
Intubation and ventilation
Inotropics
Infective endocarditis
prophylaxis
-
8/4/2019 pedia cardio
56/95
MANAGEMENT
CONGENITAL HEART DEFECTS
Transposition of great
arteries
SURGICAL
Procedure of choice:
Arterial switch operation
Aorta and PA are switched
back to their anatomically
correct ventricle
-
8/4/2019 pedia cardio
57/95
MANAGEMENT
CONGENITAL HEART DEFECTS
Total anomalous pulmonary
venous return
MEDICAL
PGE1 infusion
Anticongestive drugs
Intubation and ventilation
Inotropics
Infective endocarditis
prophylaxis
-
8/4/2019 pedia cardio
58/95
MANAGEMENT
CONGENITAL HEART DEFECTS
Total anomalous pulmonary
venous return
SURGICAL
Reimplantation of the
pulmonary veins into the
left atrium
-
8/4/2019 pedia cardio
59/95
MANAGEMENT
CONGENITAL HEART DEFECTS
Truncus arteriosus
MEDICAL
PGE1 infusion
Anticongestive drugs
Intubation and ventilation
Inotropics
Infective endocarditis
prophylaxis
-
8/4/2019 pedia cardio
60/95
MANAGEMENT
CONGENITAL HEART DEFECTS
Truncus arteriosus
SURGICAL
Grafting to separate aorta
and pulmonary artery
-
8/4/2019 pedia cardio
61/95
DISORDERS WITH DECREASED
PULMONARY BLOOD FLOW
-
8/4/2019 pedia cardio
62/95
TRICUSPID ATRESIA
ILLUSTRATION description
Tricuspid valve completely
closed = no blood flow from
the RA to the RV
Blood bypasses the lungs
(crosses from foramen ovale
to LA)
-
8/4/2019 pedia cardio
63/95
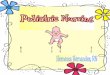
TETRALOGY OF FALLOT
ILLUSTRATION description
FOUR anomalies present
-
8/4/2019 pedia cardio
64/95
ASSESSMENT FINDINGS
Tricuspid Atresia
Cyanosis
Tachypnea
Feeding difficulties
-
8/4/2019 pedia cardio
65/95
ASSESSMENT FINDINGS
Tetralogy of Fallot
Cyanosis
Polycythemia
Activity intolerance
Squatting
Hypercyanotic spells Tet spells
Occurs in the morning soon after awakening, during orafter:
crying, feeding, painful procedures
Characterized by: tachypnea, irritability, increasing
cyanosis, flaccidity and loss of consciousness
-
8/4/2019 pedia cardio
66/95
MANAGEMENT
CONGENITAL HEART DEFECTS
Tricuspid Atresia
MEDICAL
PGE1 infusion
Anticongestive drugs
Intubation and ventilation
Inotropics
Infective endocarditis
prophylaxis
-
8/4/2019 pedia cardio
67/95
MANAGEMENT
CONGENITAL HEART DEFECTS
Tricuspid atresia
SURGICAL
First surgery: neonate
Blalock-Taussig shunt (shunt
bet. aorta and PA)
Pulmonary artery band
Second surgery: 6-9 months
End-to-end anastomosis
Third surgery: 18 months-3yrs
IVC to PA connection
-
8/4/2019 pedia cardio
68/95
MANAGEMENT
CONGENITAL HEART DEFECTS
Tetralogy of Fallot
MEDICAL
Positioning (knee-chest)
Morphine sulfate
Beta-blockers
-
8/4/2019 pedia cardio
69/95
MANAGEMENT
CONGENITAL HEART DEFECTS
Tetralogy of Fallot
SURGICAL
Blalock-Taussig procedure
Brock procedure (full repair)
-
8/4/2019 pedia cardio
70/95
ACQUIRED HEART DISEASE
-
8/4/2019 pedia cardio
71/95
Congestive Heart Failure (CHF)
-
8/4/2019 pedia cardio
72/95
DESCRIPTION
Occurs when CO cannot meet metabolic
demands of the body
-
8/4/2019 pedia cardio
73/95
ASSOCIATED FACTORS
CHDs
Acquired heart disease: myocarditis,
cadiomyopathy, acute rheumatic fever
Anemia
Iatrogenic fluid overload
-
8/4/2019 pedia cardio
74/95
CLASSIFICATIONS
Right-sided
Left-sided
-
8/4/2019 pedia cardio
75/95
ASSESSMENT FINDINGS
LEFT-SIDED
Pulmonary congestion
Tachypnea
Cyanosis
Cough
Crackles
RIGHT-SIDED
Systemic venous congestion
Hepatomegaly
Peripheral edema: scrotal and
orbital
Weight gain
Decreased urine output
-
8/4/2019 pedia cardio
76/95
MANAGEMENT
Diuretics
Digoxin
ACE inhibitors
Beta-adrenergic blockers
Inotropics
-
8/4/2019 pedia cardio
77/95
NURSING DIAGNOSES
Decreased Cardiac Output related to myocardialdysfunction
Excess fluid volume related to decreased cardiac
contractility and decreased excretion from the kidney Impaired
gas exchange related to pulmonary venous
congestion
Activity intolerance
Risk for infection related to pulmonary congestion
Imbalanced Nutrition: Less Than Body Requirements
related to increased metabolic demands with
decreased caloric intake
-
8/4/2019 pedia cardio
78/95
NURSING INTERVENTIONS
Improving Myocardial Efficiency
Administer Digoxin as prescribed
Measure HR, hold if HR < 90 bpm
Check MOST RECENT potassium level, hold if < 3.5 Report signs
of digoxin toxicity:
Vomiting
Nausea
Visual changes Bradycardia
-
8/4/2019 pedia cardio
79/95
NURSING INTERVENTIONS
Improving Myocardial Efficiency
Administer afterload reduction medications as
prescribed
Measure BP before and after giving meds, hold if lowBP and
notify the physician
Observe for signs of hypotension:
Dizziness
Light-headedness Sncope
-
8/4/2019 pedia cardio
80/95
NURSING INTERVENTIONS
Maintaining Fluid and Electrolyte Balance
Administer diuretics as prescribed
Obtain daily weights
Keep strict I&O monitoring Monitor serum potassium
(potassium supplements as
needed)
Sodium restriction
Fluid restriction
S G O S
-
8/4/2019 pedia cardio
81/95
NURSING INTERVENTIONS
Relieving Respiratory Distress
Administer oxygen as prescribed
Elevate HOB
NURSING INTERVENTIONS
-
8/4/2019 pedia cardio
82/95
NURSING INTERVENTIONS
Promoting Activity Tolerance
Organize nursing care
Respond efficiently to a crying infant
Provide small, frequent feedings
NURSING INTERVENTIONS
-
8/4/2019 pedia cardio
83/95
NURSING INTERVENTIONS
Decreasing Risk of Infection
Ensure good hand washing by everyone
Avoid exposure to all children or caretakers
Monitor signs of infection: fever, cough, runnynose, diarrhea,
vomiting
NURSING INTERVENTIONS
-
8/4/2019 pedia cardio
84/95
NURSING INTERVENTIONS
Providing Adequate Nutrition
Provide nutritious foods that the child likes
High calorie snack
EVALUATION
-
8/4/2019 pedia cardio
85/95
EVALUATION
HR within normal range
No unexpected weight gain
Clear lungs
Participates in quiet diversional activities
No signs and symptoms of infection
Adequate intake of small, frequent feedings
-
8/4/2019 pedia cardio
86/95
Acute Rheumatic Fever
DESCRIPTION
-
8/4/2019 pedia cardio
87/95
DESCRIPTION
Acute autoimmune disease that occurs as asequeale of GABHS
infection
ASSESSMENT
-
8/4/2019 pedia cardio
88/95
ASSESSMENT
Major
Carditis
Polyarhtritis
Chorea
Erythema marginatum
Subcutaneous nodules
ASSESSMENT
-
8/4/2019 pedia cardio
89/95
ASSESSMENT
Minor
Arthralgia
Fever
Laboratory abnormalities: elevated ESR, WBC, C-reactive protein
positive
ECG changes prolonged PR interval
MANAGEMENT
-
8/4/2019 pedia cardio
90/95
MANAGEMENT
Antibiotics (penicillin/erythromycin)
Oral salicylates (aspirin)
Corticosteroids
Diazepam or other neurologic agents
Bed rest
NURSING DIAGNOSIS
-
8/4/2019 pedia cardio
91/95
NURSING DIAGNOSIS
Decreased Cardiac Output related to carditis
Acute and Chronic Pain related to arthritis
Risk for injury related to chorea
NURSING INTERVENTIONS
-
8/4/2019 pedia cardio
92/95
NURSING INTERVENTIONS
Improving Cardiac Output
Explain to the child and family the need for bed
rest
Organize nursing care Administer course of antibiotics as
prescribed
Administer meds for CHF as directed
NURSING INTERVENTIONS
-
8/4/2019 pedia cardio
93/95
NURSING INTERVENTIONS
Relieving Pain
Administer anti-inflammatory medication,
analgesics, and antipyretics
Monitor for signs of aspirin toxicity Tinnitus, nausea and
vomiting, headache
Monitor for signs of corticosteroid use
Weight gain, rounded face, decrease resistance to infection
Administer with food
NURSING INTERVENTIONS
-
8/4/2019 pedia cardio
94/95
NURSING INTERVENTIONS
Protecting the Child with Chorea
Use padded side rails
Assist with feeding
Avoid the use of straw and sharp utensils
Administer phenobarbital or other neurologic
agents as prescribed
EVALUATION
-
8/4/2019 pedia cardio
95/95
EVALUATION
HR within normal range
Compliant with anti-inflammatory therapy
Feeds self, washes face and hands, and
ambulates without injury