Embed Size (px)
Citation preview

Patients’ Attitudes About Autonomy andConfidentiality in Genetic Testing forBreast-Ovarian Cancer Susceptibility
Judith L. Benkendorf,1* Jeri E. Reutenauer,2 Chanita A. Hughes,2 Nadine Eads,3 Jan Willison,2Madison Powers,4 and Caryn Lerman2
1Division of Genetics, Department of Obstetrics and Gynecology, Georgetown University Medical Center,Washington, DC
2Lombardi Cancer Center, Georgetown University Medical Center, Washington, DC3Washington Cancer Institute, Washington Hospital Center, Washington, DC4Kennedy Institute of Ethics, Georgetown University, Washington, DC
The identification of BRCA1 and BRCA2,two breast-ovarian cancer susceptibilitygenes, has brought many ethical and so-cial issues to the forefront. This paperpresents the results of a survey assessingthe attitudes of 238 unaffected first-degreerelatives of women with breast or ovariancancer regarding the ethical issues of au-tonomy and confidentiality as they relate toBRCA1/2 testing. Baseline knowledge aboutBRCA1/2 and ethnic and psychosocial char-acteristics of our study population were ex-amined to determine their association withwomen’s attitudes. The majority of women(86–87%) felt that health care providersshould not disclose the results of genetictests for breast-ovarian cancer susceptibil-ity to insurance companies or employerswithout written consent; however, only 56–57% felt that written consent should be re-quired for a spouse or immediate family toreceive this information. Ninety-eight per-cent of the women surveyed agreed that ge-netic testing for breast-ovarian cancer riskshould be voluntary. Likewise, most women(95%) agreed that a person should be able tohave genetic testing against a doctor’s rec-ommendation and 88% of the women sur-veyed agreed that parents should be able toconsent to genetic susceptibility testing onbehalf of their minor children. African
American women were less concerned thanCaucasian women about the protection ofconfidentiality in families, they were morelikely to agree that an individual should stillhave access to testing when their physiciansrecommended against it, and they weremore supportive of parents’ rights to con-sent to genetic predisposition testing on be-half of their minor children. Women withcoping styles characterized by higher opti-mism were more likely to favor access to ge-netic testing when a physician recom-mended against it, and to support parents’rights to consent to testing of their minorchildren. Therefore, the setting and mannerin which genetic counseling and testing aredelivered must be appropriately tailored toreflect these attitudinal differences andpreferences. Am. J. Med. Genet. 73:296–303,1997. © 1997 Wiley-Liss, Inc.
KEY WORDS: autonomy; confidentiality;BRCA1/2 testing; patients’ at-titudes
INTRODUCTION
With the rapid elucidation of the molecular basis ofmany common diseases of adulthood, such as diabetes,Alzheimer disease, and some forms of cancer, individu-als will have the option of being tested for a wide rangeof genetic predispositions. Two breast-ovarian cancersusceptibility genes, BRCA1 and BRCA2, have beenisolated [Miki et al., 1994; Wooster et al., 1995]. Pres-ently, genetic tests for hereditary breast and ovariancancer are being transferred from the laboratory benchto the clinical research arena [Lerman et al., 1996]. Asthese tests are integrated into routine patient care, itwill be of paramount importance for potential consum-ers to consider the social and ethical ramifications of
Contract grant sponsor: National Institute of Mental Healthand National Human Genome Research Institute, NIH; Contractgrant number: RO1MH/HG54435.
*Correspondence to: Judith L. Benkendorf, M.S., Division ofGenetics, Department of Obstetrics and Gynecology (3PHC),Georgetown Medical Center, 3800 Reservoir Road, NW, Washing-ton, DC 20007.
Received 26 February 1997; Accepted 1 August 1997
American Journal of Medical Genetics 73:296–303 (1997)
© 1997 Wiley-Liss, Inc.

testing prior to consenting to have testing performed.Health professionals must appreciate these nuances oftesting in order to elicit informed consent.
DNA-based genetic predisposition testing differsfrom many other forms of medical testing and screen-ing because the results reflect potential future illnessand carry implications for the health of related familymembers [President’s Commission, 1983]. Hence, theethical principle of respect for autonomy and duties toprotect confidentiality, intrinsic to the practice of mod-ern medicine, are cast in a new light.
In the context of BRCA1/2 predisposition testing, theprinciple of autonomy reflects an individual’s right tochoose: 1) whether or not to receive information aboutpersonal risk status; 2) whether or not to be tested; 3)with whom tests results will be shared; and 4) who hasthe authority, within a family as well as in society, todisclose these results [Andrews et al., 1994; Powers,1994]. Implicit in respecting an individual’s right tomake these types of decisions are duties to ensure thevoluntariness of testing and to protect against un-wanted and unauthorized disclosures of genetic infor-mation [Murray, 1992; Andrews et al., 1994; NationalSociety of Genetic Counselors, Inc., 1992]. These dutiesare presently viewed as critical to the informed consentprocess for genetic testing [Andrews et al., 1994]. Inaddition, patients’ rights to exercise parental au-tonomy in obtaining tests for their minor children andtheir rights to obtain testing for themselves over theobjections of their physicians are included in the scopeof autonomy rights.
At a time when there is little published consensusamongst professionals (ethicists, geneticists, and themedical community) about issues such as access totesting, disclosure of test results, and the testing ofminors, we sought the opinions of potential consumersof genetic testing for hereditary breast-ovarian cancersusceptibility who had enrolled in our hereditarybreast-ovarian cancer education and counseling pro-gram. This study had two key objectives. The first wassimply to describe levels of agreement vs. disagreementwith statements reflecting these ethical issues of au-tonomy and confidentiality in a sample of women rep-resentative of those who may seek BRCA1/2 testing inthe future. The second objective was to identify char-acteristics of these women that correlated with particu-lar attitudes. Toward this end, we examined sociode-mographic and medical factors, prior exposure to ge-netic testing, baseline knowledge, and personalityfactors. With an increased understanding of the factorsand experiences that shape counseling participants’ at-titudes about ethical issues, we will be better able toaddress these issues in the informed consent processand to tailor education and counseling approaches toindividual needs.
MATERIALS AND METHODSParticipants
Eligible subjects were women aged 18–75 with atleast one first-degree relative (FDR) with breast and/orovarian cancer, and no personal history of cancer.
Procedures
Two mechanisms were used to recruit subjects intothe program. Patient-referred subjects were recruitedthrough contact with their relative affected with eitherbreast or ovarian cancer. Affected index patients wereidentified through patient lists at the Georgetown Uni-versity Medical Center (GUMC) and the WashingtonHospital Center (WHC). They were contacted by tele-phone to ask permission to invite their unaffectedFDRs to participate in the study. Letters of introduc-tion describing the program were mailed to unaffectedFDRs of the index patients who granted permission. Ifthey did not wish to participate, the FDRs were in-structed to call a local telephone number. Those whodid not ‘‘opt-out’’ were contacted for the interview de-scribed below. The second recruitment mechanism wasby self-referral. Women were informed about the pro-gram either by their physicians or through brochureslocated in cancer centers, obstetrics and gynecology de-partments, and genetics clinics. Eligible women wereinstructed to complete either the self-referral form or tocontact the research assistant directly.
Both patient-referred and self-referred subjects werecontacted to participate in a 20-min baseline telephoneinterview to assess sociodemographics, family history,genetic testing exposure, and knowledge about BRCA1testing. This structured interview was administered bya research assistant, using a computer-assisted tele-phone interviewing (CATI) system. The response rateto the baseline interview was 82%. Following the inter-view, consenting subjects were invited to attend an in-dividual educational session with a nurse educator orgenetic counselor about the natural history of breastand ovarian cancers, cancer risk factors, preventionand screening guidelines, hereditary cancers, andBRCA1 testing. Seventy-one percent of the women whoaccepted the invitation completed the education ses-sion. As described in a previous report, nonparticipantswere more likely to have less education, to be unmar-ried, to be African American, and to have only one rela-tive affected with breast cancer [Lerman et al., 1997].Self-referred women were significantly more likely toparticipate than patient-referred women (76% vs. 52%;P < .001).
In the waiting room prior to the education session,informed consent was obtained. At the same time, par-ticipants were asked to complete a set of self-reportquestionnaires which included measures of genetictesting attitudes and personality. The present paperfocuses on the data collected during the baseline inter-view and previsit assessments (i.e., prior to geneticseducation and counseling).
Measures
The following measures were ascertained during thebaseline interview and the previsit assessments.
Predictor Variables
Sociodemographics. Variables included ethnic-ity, age, marital status, education level, employmentstatus, and health insurance status.
Attitudes About BRCA1/2 Testing 297
Familial risk. Variables included number of FDRsaffected with breast cancer (0, 1, or 2+) and number ofFDRs with ovarian cancer (0, 1, or 2+).
Genetic testing exposure. Variables includedprevious use of genetic testing or counseling by thepatient or her spouse, such as chorionic villus sam-pling, amniocentesis, maternal serum marker screen-ing, Tay-Sachs or sickle-cell screening, and cancer riskassessment based on family history (yes or no), andhow much the participant read or heard about genetictesting for inherited disease (1, almost nothing; 2, alittle bit; 3, a fair amount; and 4, a lot) and about ge-netic testing for cancer (1, almost nothing; 2, a little bit;3, a fair amount; and 4, a lot).
Psychological Factors
Knowledge. Knowledge about genetic testing forinherited susceptibility to breast and ovarian cancerwas assessed with an 11-item true-false scale devel-oped as part of a core set of instruments for the Na-tional Human Genome Research Institute Cancer Ge-netic Studies Consortium [Measurement Task Force,1995]. One point was given for each correct answer.
Optimism. Dispositional optimism was measuredusing the brief Life Orientation Test (LOT) [Scheier etal., 1994]. The brief LOT is a 10-item Likert-style ques-tionnaire that measures the level of optimism in one’soutlook on life. Respondents are asked to rate how
much they agree or disagree (i.e., 0, strongly disagree;1, disagree; 2, neutral; 3, agree; and 4, strongly agree)with items such as ‘‘in uncertain times, I usually expectthe best’’ and ‘‘I hardly ever expect things to go myway.’’ An optimism score is created by summing sixitems; a higher score indicates a more optimistic out-look. This scale had good internal consistency (Cron-bach’s alpha 4 .89).
Information-seeking. Information-seeking cop-ing style was assessed by the Miller Behavioral StyleScale (MBSS) [Miller, 1980]. The MBSS describes fourhypothetical threatening situations and asks respon-dents to choose the coping responses that are charac-teristic of how they would respond in that situation. Aninformation-seeking, or ‘‘monitoring,’’ score is calcu-lated by summing the number of monitoring items en-dorsed. The monitoring subscale had good internal con-sistency (Cronbach’s alpha 4 .72).
Outcome Variable: Attitudes About EthicalIssues in Genetic Testing
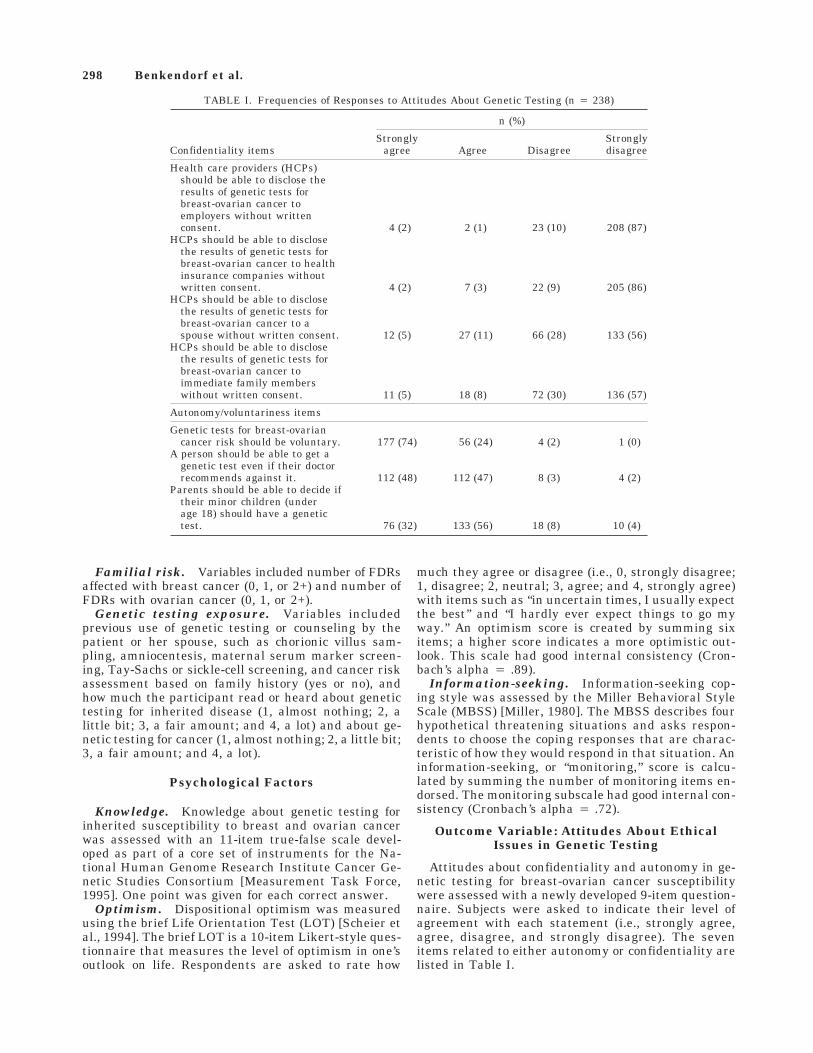
Attitudes about confidentiality and autonomy in ge-netic testing for breast-ovarian cancer susceptibilitywere assessed with a newly developed 9-item question-naire. Subjects were asked to indicate their level ofagreement with each statement (i.e., strongly agree,agree, disagree, and strongly disagree). The sevenitems related to either autonomy or confidentiality arelisted in Table I.
TABLE I. Frequencies of Responses to Attitudes About Genetic Testing (n 4 238)
Confidentiality items
n (%)
Stronglyagree Agree Disagree
Stronglydisagree
Health care providers (HCPs)should be able to disclose theresults of genetic tests forbreast-ovarian cancer toemployers without writtenconsent. 4 (2) 2 (1) 23 (10) 208 (87)
HCPs should be able to disclosethe results of genetic tests forbreast-ovarian cancer to healthinsurance companies withoutwritten consent. 4 (2) 7 (3) 22 (9) 205 (86)
HCPs should be able to disclosethe results of genetic tests forbreast-ovarian cancer to aspouse without written consent. 12 (5) 27 (11) 66 (28) 133 (56)
HCPs should be able to disclosethe results of genetic tests forbreast-ovarian cancer toimmediate family memberswithout written consent. 11 (5) 18 (8) 72 (30) 136 (57)
Autonomy/voluntariness items
Genetic tests for breast-ovariancancer risk should be voluntary. 177 (74) 56 (24) 4 (2) 1 (0)
A person should be able to get agenetic test even if their doctorrecommends against it. 112 (48) 112 (47) 8 (3) 4 (2)
Parents should be able to decide iftheir minor children (underage 18) should have a genetictest. 76 (32) 133 (56) 18 (8) 10 (4)
298 Benkendorf et al.

Data Analysis
Descriptive statistics were generated to characterizethe sample in terms of sociodemographics, family his-tory, genetic testing exposure, and psychological vari-ables. Frequencies were generated for attitudes aboutgenetic testing items. T-tests and chi-square tests ofassociation were conducted to identify factors associ-ated with attitudes about genetic testing. Logistic re-gression modeling was performed to identify factorshaving independent associations with attitude outcomevariables.
RESULTSSample Characteristics
The sample consisted of 238 women. Seventy-six per-cent of the sample were Caucasian women; 18% of thesample were African American women. The other 6%were excluded for the purposes of this analysis. Themean age of the sample was 44 (range, 22–75). Themajority of the sample were married (67%), had edu-cation beyond high school (90%), were employed (72%),and had health insurance (92%). The majority ofwomen in this sample had one FDR affected withbreast or ovarian cancer (90%); the rest had two ormore affected FDRs.
Attitudes About Genetic Testing
The pattern of responses to genetic testing attitudeitems is shown in Table I. The vast majority of womenfelt that the results of genetic tests should be kept con-fidential from insurers and employers. For instance,86–87% percent of the sample disagreed strongly withthe statements that health care providers should beable to disclose the results of genetic tests for breast-ovarian cancer risk to health insurance companies or toemployers without written consent. Fewer women (56–57%) disagreed strongly with the statements thathealth care providers should be able to disclose theresults of genetic tests to immediate family members orto spouses without written consent. The vast majority
of women agreed strongly that genetic tests for breast-ovarian cancer risk should be voluntary (74%). Most ofthe women agreed that one should be able to get agenetic test even if one’s doctor recommends against it;however, only 48% strongly agreed with this state-ment. Most of the women agreed that parents shouldbe able to decide if their minor children should have agenetic test (32% agreed strongly and 56% agreed).
Factors Associated With Attitudes AboutGenetic Testing
Three attitude items were selected for further analy-sis, based on variability in the distribution of re-sponses: 1) individuals should be able to get a genetictest even if their doctor recommends against it; 2) par-ents should be able to decide if their minor children(under age 18) should have a genetic test; and 3) healthcare providers should be able to disclose the results ofgenetic tests for breast-ovarian cancer to immediatefamily members without written consent. Because ofthe skewed distribution, these items were recoded as‘‘agree/disagree strongly’’ vs. ‘‘else.’’ Demographic, fa-milial, knowledge, and personality variables associatedsignificantly with each of these three attitudes areshown in Tables II–IV.
Several factors were associated with attitudes aboutthe need for physician recommendation for genetictesting. Significantly fewer white women than AfricanAmerican women strongly agreed that a person shouldbe able to get a genetic test, even if their doctor hadrecommended against it (43% vs. 63%, P < .05). Womenwith more exposure to genetic testing for cancer sus-ceptibility (heard a fair amount/a lot) were more likelythan women with less exposure (heard nothing/a little)to strongly agree with this statement (59% vs. 42%, P <.05). Older women and women with more exposure togenetic testing for inherited disease (heard a fairamount/a lot) were more likely to agree strongly thatgenetic testing should be available against a doctor’srecommendation, but this was not statistically signifi-cant (P < .10). In addition, women who strongly agreedthat genetic testing should be available against a doc-
TABLE II. Sociodemographic Factors Associated With Genetic Testing Attitudes
Predictor variable Category
Providers discloseto family,% stronglydisagree
Test against doctor’srecommendation,% strongly agree
Parents decide if minorchildren to be tested,
% strongly agree
Race African American 49 63* 56*White 58 43 24
Age 18–34 50 34** 21**35–49 61 51 3150+ 60 53 40
Marital status Married 59 50 31Not married 56 43 32
Education level øHigh school 45 38 32>High school 60 49 31
Employment status Employed 60 47 31Not employed 53 50 32
Health insurance status Yes 59 48 32No 33 33 22
*P < .05.**P < .10.
Attitudes About BRCA1/2 Testing 299

tor’s recommendation had higher optimism and moni-toring scores. Factors not associated with agreeing thatgenetic testing should be available, even when a phy-sician recommends against it, included marital status,educational level, employment status, health insur-ance status, number of FDRs with breast or ovariancancer, previous use of genetic testing, and baselineknowledge. In the logistic regression model, the follow-ing variables had independent associations: race (OR,0.41; CI, 0.20, 0.84); exposure to cancer genetics (OR,2.40; CI, 1.32, 4.37); optimism (OR, 1.88; CI, 1.07, 3.30);and monitoring (OR, 2.37; CI, 1.34, 4.20).
Race and age were related to attitudes about genetictesting of minor children. Significantly fewer whitethan African American women strongly agreed thatparents should be able to decide if minor children aretested (24% vs. 56%, P < .05). Age was also associatedwith attitudes about genetic testing of minor children,although this was not significant (P < .10). Olderwomen were more likely to agree strongly that parentsshould be able to decide if minor children are tested.Women who strongly agreed that parents should beable to decide if minor children are tested had signifi-cantly higher optimism scores than women whoagreed, disagreed, or strongly disagreed (P < .05). Fac-tors not associated with attitudes about testing chil-dren included marital status, educational level, em-ployment status, health insurance status, number ofFDRs with breast or ovarian cancer, use and exposureto genetic testing, a monitoring coping style, andbaseline knowledge. Race was the only factor indepen-dently associated with this attitude in the multivari-able model (OR, 0.21; CI, 0.11, 0.42).
With regard to attitudes about providers disclosinggenetic test results to immediate family members, onlyknowledge had a marginal association. Women who
had higher knowledge scores were more likely tostrongly disagree that test results could be disclosed tofamily members. No other demographic, risk, or expo-sure variables related to this attitude.
DISCUSSION
The results of this study demonstrated general con-sensus among the women surveyed with regard to theissues of autonomy and confidentiality in genetic test-ing for breast-ovarian cancer risk. Overall, mostwomen felt that the results of genetic testing should bekept confidential. Levels of agreement that genetic testresults could be released without written consent in-creased with the intimacy of the relationship to thethird party. Women were more lenient about the re-lease of test results to their immediate families (44%)and spouses (43%) than they were about the disclosureof their test results to health insurance companies(14%) and employers (13%). This is consistent with aprevious survey regarding genetic testing for occupa-tional susceptibility which suggests that people aremore likely to trust physicians with such sensitive in-formation, as opposed to employers or insurers [Wertzand Fletcher, 1989]. This may be due to heightenedpublic awareness of the potential for discrimination inthe procurement or retention of employment or insur-ance as a result of genetic testing [Hudson et al., 1995].The relatively greater willingness to allow family mem-bers and spouses access to this informaiton withoutwritten consent may be out of a desire to promote thewell-being of their families [American Society of Hu-man Genetics/ACMG Report, 1995]. While the publicmay not be well-informed about the myriad intrafamil-ial issues surrounding genetic predisposition testingand the potential of this information to exacerbate ex-
TABLE III. Risk and Exposure Factors Associated With Genetic Testing Attitudes
Predictor variable Category
Providers discloseto family,% stronglydisagree
Test against doctor’srecommendation,% strongly agree
Parents decide if minorchildren to be tested,
% strongly agree
Number of first-degree relatives 0/1 57 47 30with cancer 2+ 50 60 37
Previous use of genetic testing Yes 68 63 37No 57 46 31
Exposure to information about Nothing/a little 55 43* 29testing for inherited disease A fair amount/a lot 65 56 37
Exposure to information about Nothing/a little 59 42** 28testing for cancer A fair amount/a lot 57 59 38
*P < .10.**P < .05.
TABLE IV. Psychoeducational Factors Associated With Genetic Testing Attitudes
Predictor variable
Disclose to familyTest against doctor’s
recommendationParents decide if minor
children to be tested
Strongly disagree Else Strongly agree Else Strongly agree Else
Optimism, mean (SD) 17.4 (3.8) 16.6 (4.5) 17.6* (4.2) 16.5 (3.9) 17.8* (3.7) 16.6 (4.2)Monitoring, mean (SD) 9.6 (2.7) 9.7 (2.6) 10.1* (2.7) 9.3 (2.6) 9.5 (2.6) 9.7 (2.7)Knowledge, mean (SD) 6.1** (2.0) 5.6 (2.2) 5.8 (2.0) 5.9 (2.1) 5.9 (1.9) 5.9 (2.1)
*P < .05.**P < .10.
300 Benkendorf et al.

isting family dynamics [Biesecker et al., 1993], partici-pants with higher baseline knowledge were marginallymore likely to favor disclosure to immediate familywithout written consent. This is the opposite of whatmight have been expected, and will be discussed fur-ther. Tension often exists between respecting the pri-vacy of the individual being tested and the responsibil-ity to warn other family members of potential geneticrisks [Murray, 1992; Andrews et al., 1994]. Addition-ally, both positive and negative test results can createfeelings of shame, guilt, anxiety, and depression [Bie-secker et al., 1993], making those receiving test resultsvery vulnerable at a time when they are also beingasked to be the gatekeepers of information for theirrelatives.
The vast majority of respondents agreed that genetictests for breast-ovarian cancer risk should be volun-tary. This finding is not surprising, and reflects thehigh premium our society places on autonomy in healthcare decision making. However, in our sample therewas some divergence of opinion with regard to access togenetic testing when a physician has recomendedagainst it, and with regard to parents’ rights to decideif their minor children (under 18 years) should have agenetic test.
African American respondents were more likely thanwhite respondents to strongly agree that a personshould be able to get a genetic test even if her doctorrecommends against it. Historically, in African Ameri-can women, the underutilization of routine breast can-cer screening modalities, such as mammography,breast self-examinations, and clinical breast examina-tions, has been attributed to physician failure to rec-ommend screening [Burack and Ling, 1989; Fletcher etal., 1993]. Distrust of the medical community may alsoplay a role in shaping African American women’s atti-tudes about obtaining testing against their doctors’ rec-ommendations. Unethical medical studies conductedon African Americans have resulted in a mistrust of themedical community [Gamble, 1993]. Furthermore,Baker and Cook [1983] reported that in the event ofserious illness, African American women between ages27–55 years are more likely to consult family membersand friends than the professional health care system.Given these experiences, African American womenmay feel the need to be more proactive in accessinghealth services [Baker and Cook, 1983].
Women with more exposure to genetic testing forcancer were more likely to strongly agree that an indi-vidual should have access to a genetic test even if herphysician recommends against it. In fact, in some casesthey may be more familiar with genetic testing thantheir physicians! This is consistent with prior researchshowing that women with more prior knowledge aboutamniocentesis were more likely to have made decisionsabout testing prior to a genetic counseling visit [Rapp,1993]. Those with little or no prior exposure or knowl-edge based their decisions on the information theywere presented in the genetic counseling session. Thus,the less exposure individuals have and the less ac-quainted they are with the salient issues surroundinggenetic screening and testing decisions, the more likely
they are to be influenced by a perceived recommenda-tion from a health care provider.
Additionally, women with higher optimism andmonitoring coping styles were more likely to stronglyagree that a person should be able to get a genetic testeven if her doctor recommends against it. Since opti-mists expect positive outcomes [Scheier and Carver,1992], they maintain a feeling of competence and con-trol [Stubblefield, 1995]. Therefore, they may be morecomfortable with autonomy in their genetic testing de-cisions, irrespective of their physician’s recommenda-tion. In addition, monitors are information seekers[Miller, 1995] who may be motivated to pursue genetictesting, even against their physicians’ recommenda-tions, because of their desire for this information. Thedesire for testing in this group is noteworthy and clini-cally relevant in that it is independent of family his-tory, which actually dictates the magnitude of geneticrisk and the likelihood of a positive test result.
In addition to deciding for themselves whether or notto pursue genetic testing, adults have the authority tomake medical decisions on behalf of their children. Tra-ditionally, these have been decisions in which the im-mediate benefit to the child is well-accepted. There isan ongoing debate about whether parents should havethe right to decide for their minor children about ge-netic predisposition testing for an adult–onset disorder,such as breast or ovarian cancer [American Society ofHuman Genetics/ACMG Report, 1995; Clayton, 1995],in which there is no immediate medical harm to beaverted. Thus, it is not surprising that differences inopinion were found in our sample.
Attitudes about testing minor children were associ-ated with ethnic background and optimism. The Afri-can American women in our sample were more likelythan white women to agree strongly that parentsshould be able to decide whether to test their minorchildren for genetic predisposition to breast-ovariancancer (56% vs. 24%, respectively). Although this issuehas not been previously addressed in the literature,one could speculate that the strong matriarchal role inthe African American culture may underpin the con-cept of parental consent for genetic testing of minorchildren. The belief that parents should be able to de-cide about genetic testing for minor children was alsoassociated with optimistic personality. Since optimistsgenerally anticipate that their actions will result inpositive outcomes [Scheier and Carver, 1992], theymay believe that authorizing genetic testing for theirminor children will be beneficial. Optimists may notrealize the potential negative implications of makinggenetic testing decisions for their children, such as ad-verse effects on family relationships and their chil-dren’s future right not to know their genetic statuses.
A number of factors were not associated with atti-tudes about disclosure to family members without writ-ten consent, access to testing against physicians’ rec-ommendations, and testing minor children. For ex-ample, while exposure to information about testing forhereditary breast-ovarian cancer susceptibility waspositively related to the belief that one should be ableto be tested against a physician’s recommendation, itwas unrelated to attitudes about disclosure to family or
Attitudes About BRCA1/2 Testing 301

testing children. This is somewhat surprising, sinceone would expect that women exposed to more infor-mation would be more aware of potential adverse con-sequences of testing children or of disclosure of testresults to family members without written consent. Itis possible that information exposure was predomi-nantly through the media as opposed to through genet-ics professionals. Further research should evaluatemore specifically the various sources of informationand their impact on testing attitudes and behaviors.
This study has some limitations. The sample wasprimarily middle class and white. Although AfricanAmerican women comprised 18% of the sample, therewere too few representatives of other ethnic groups toinclude them in the analysis. Therefore, while oursample may be somewhat representative of the popu-lation of women in this metropolitan urban area inter-ested in hereditary breast-ovarian cancer susceptibilitytesting, the results may not be applicable to the generalpopulation. Because self-referred women were morelikely than patient-referred women to attend the edu-cation session, our sample may also be more character-istic of individuals who keep appointments. Anotherlimitation of the study is that the questionnaire wasonly administered prior to the educaiton intervention.Women’s attitudes may change significantly as a resultof pretest education and counseling [Lerman et al.,1997].
Ninety percent of the participants in this study hadonly one FDR with breast or ovarian cancer. The ma-jority will therefore not be appropriate candidates forgenetic testing for BRCA1/2 mutations, in spite of rep-resenting a group of women most likely to present toprimary care physicians requesting testing. Hence, ourfindings may not be generalizable to women from he-reditary breast-ovarian cancer families. Examinationof attitudes about autonomy and confidentiality in ge-netic susceptibility testing for hereditary cancer, andthe correlation of those attitudes with sociodemo-graphic, medical, and personality factors, prior expo-sure to gentic testing, and baseline knowledge in thislatter group of individuals, are areas for future work.Likewise, future studies should query about patients’willingness to disclose results of genetic tests for cancersusceptibility to another physician or health profes-sional without written consent, a situation frequentlyencountered by genetic counselors and physicians. Fi-nally, two of the autonomy items in our questionnaire(‘‘A person should be able to get a genetic test even iftheir doctor recommends against it,’’ and ‘‘Parentsshould be able to decide if their minor children (underage 18) should have a genetic test’’) did not specify thatthe question referred to genetic testnig for breast-ovarian cancer susceptibility. While it was assumedthat participants would have answered these questionsin the context of genetic testing for breast-ovarian can-cer, their responses may in fact reflect attitudes aboutgenetic tests in general.
Despite these limitations, this is one of the first re-ported studies of consumers’ attitudes about issues ofautonomy and confidentiality with regard to geneticsusceptibility testing for heterditary breast-ovariancancer. We have demonstrated that patients not only
have concrete points of view about these social andethical issues, but also that their attitudes vary withethnic, educational, and psychosocial factors. Whileprofessionals still debate the very dilemmas we sur-veyed, it is clear that the public is capable of consider-ing these complex issues; their perspectives and atti-tudes should be represented as practice guidelines andlegislative proposals emerge.
Ethnic differences influence the ways in which con-fidentiality and autonomy are valued within families.In addition, life experience, exposure to and knowledgeabout breast and ovarian cancer, and susceptibilitytesting all play important roles in shaping individualattitudes. Personality and coping style may also influ-ence individual preferences. Therefore, it is of the ut-most importance to be cognizant of these potential, in-dividual differences when tailoring and eliciting in-formed consent for this, and other, hereditary diseasepredisposition testing.
Genetic susceptibility testing for common adult-onset disorders will afford each member of society thepotential to become a consumer of genetic services.During this critical time, as newly developed testingcapabilities for hereditary breast-ovarian cancer sus-ceptibility cross over from the research arena to clinicalpractice, the health care community must work to-gether to establish well-grounded models for the safe,effective delivery of genetic susceptibility tests. Thesemodels must address the characteristics and attitudesof the breadth of consumers within the population atlarge.
ACKNOWLEDGMENTS
The authors thank the following individuals for theircontributions to this study: Barbara Biesecker, DonaldHadley, Beth Peshkin, and June Peters, for their as-sistance with protocol development; David Main, An-dres Gomez-Caminero, and Margaret Reed, for statis-tical programming; Rachel Manassan, Jennifer Rocca,Kristin Willard, and Dara Ganoczy, for telephone in-terviewing; Drs. James Barter, Susan Honing, andClaudine Isaacs, the physicians and nurses in the De-partment of Obstetrics and Gynecology at GeorgetownUniversity Medical Center, and Drs. Marc Boisvert,Lisa Boyle, Mark Buchly, Lawrence Lessin, and JohnMcKnight at the Washington Hospital Center, for pa-tient referrals and their support. Finally, we are grate-ful to all of the women who gave their time and par-ticipated in our clinical trial of pretest education andcounseling. This research was supported by grantRO1MH/HG54435, from the National Institute of Men-tal Health and the National Human Genome ResearchInstitute, NIH.
REFERENCES
American Society of Human Genetics/ACMG Report (1995): Points to con-sider: Ethical, legal and psychological implications of genetic testing inchildren and adolescents. Am J Hum Genet 57:1223–1241.
Andrews LB, Fullarton JE, Holtzman NA, Motulsky AG (eds) (1994): ‘‘As-sessing Genetic Risks: Implications for Health and Social Policy.’’Washington, DC: National Academy Press, pp 14–28.
302 Benkendorf et al.
Baker A, Cook GS (1983): Stress, adaptation and the black individual. JNurs Educ 22:237–242.
Biesecker BB, Boehnke M, Calzone K, Markel DS, Garber JE, Collins FS,Weber BL (1993): Genetic counseling for families with inherited sus-ceptibility to breast and ovarian cancer. JAMA 269:1970–1974.
Burack RC, Ling J (1989): The acceptance and completion of mammogra-phy in older black women. Am J Public Health 79:721–726.
Clayton EW (1995): Removing the shadow of the law from the debate aboutgenetic testing of children. Am J Med Genet 57:630–634.
Fletcher SW, Black W, Harris R, Rimer BK, Shapiro S (1993): Report of theInternational Workshop on Screening for Breast Cancer. JNCI 85:1664–1656.
Gamble VN (1993): A legacy of mistrust: African Americans and medicalresearch. Am J Prevent Med 9:35–38.
Hudson KL, Rothenberg KH, Andrews LB, Kahn MJE, Collins FS (1995):Genetic discrimination and health insurance: An urgent need for re-form. Science 270:391–393.
Lerman C, Narod S, Schulman K, Hughes C, Gomez-Caminero A, BonneyG, Gold K, Trock B, Main D, Lynch J, Fulmore C, Snyder C, Lemon S,Conway T, Tonin P, Lenoir G, Lynch H (1996): BRCA1 testing in fami-lies with hereditary breast-ovarian cancer: A prospective study of pa-tient decision making and outcomes. JAMA 275:1885–1892.
Lerman CE, Biesecker BB, Benkendorf JL, Kerner J, Gomez-Caminero A,Hughes C, Reed MM (1997): Controlled trial of pre-test education ap-proaches to enhance informed decision-making for BRCA1 gene test-ing. JNCI 89:148–157.
Measurement Task Force (1995): Cancer Genetics Studies Consortium,National Human Genome Research Institute, Ethical, Legal and SocialImplications Program.
Miki Y, Swensen J, Shattuck-Eidens D, Futreal PA, Harshman K, Tavit-gian S, Lui Q, Cochran C, Bennett LM, Ding W (1994): A strong can-didate for the breast-ovarian cancer susceptibility gene BRCA1. Sci-ence 266:67–71.
Miller S (1995): Monitoring versus blunting style of coping with cancerinfluence the information patients want and need about their disease.Cancer 76:167–177.
Miller SM (1980): Monitoring and blunting: Validation of a questionnaireto assess styles of information-seeking under threat. J Pers Soc Psychol52:345–353.
Murray TH (1992): The human genome project and genetic testing: Ethicalimplications. In the American Association for the Advancement of Sci-ence: ‘‘The Genome, Ethics and the Law: Issues in Genetic Testing.’’Washington, DC. American Association for the Advancement of SciencePress, pp 49–78.
National Society of Genetic Counselors, Inc. (1992): National Society ofGenetic Counselors Code of Ethics. J Genet Counsel 1:41–43.
Powers M (1994): Privacy and the control of the genetic information. InFrankel M, Teich A (eds): ‘‘The Genetic Frontier: Ethics, Law, andPolicy.’’ Washington, DC: American Association for the Advancement ofScience Press, pp 77–100.
President’s Commission for the Study of Ethical Problems in Medicine andBiomedical and Behavioral Research (1983): ‘‘Screening and Counsel-ing for Genetic Conditions.’’ Washington, DC: U.S. Government, pp1–86.
Rapp R (1993): Amniocentesis in sociocultural perspective. J Genet Coun-sel 2:183–196.
Scheier MF, Carver CS (1992): Effects of optimism on psychological andphysical well-being: Theoretical overview and empirical update. CognTher Res 16:201–228.
Scheier MF, Carver CS, Bridges MW (1994): Distinguishing optimism fromneuroticism (and trait anxiety, self-mastery, and self-esteem): A re-evaluation of the Life Orientation Test. J Pers Soc Psychol 67:1063–1078.
Stubblefield C (1995): Optimism: A determinant of health behavior. NursForum 30:19–24.
Wertz DC, Fletcher JC (1989): An international survey of attitudes ofmedical geneticists toward mass screening and access to results. PublicHealth Rep 104:35–44.
Wooster R, Bignell G, Lancaster J, Swift S, Seal S, Mangion J, Collins N(1995): Identification of the breast cancer susceptibility gene BRCA2.Nature 378:789–792.
Attitudes About BRCA1/2 Testing 303