Embed Size (px)
DESCRIPTION
Hyperthyroidim and Hypothyroidism
Citation preview
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 1/97
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 2/97
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 3/97
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 4/97
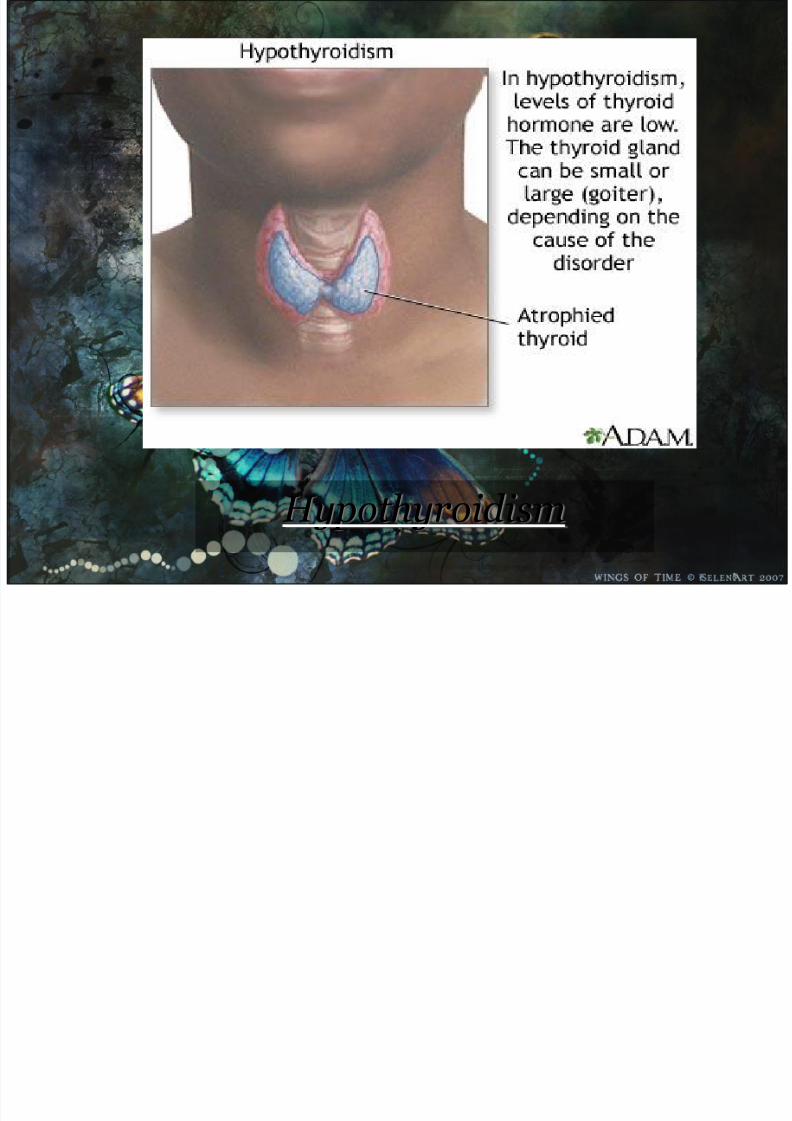
the disease state in humans and in vertebratescaused by insufficient production of thyroid
hormone by the thyroid gland.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 5/97
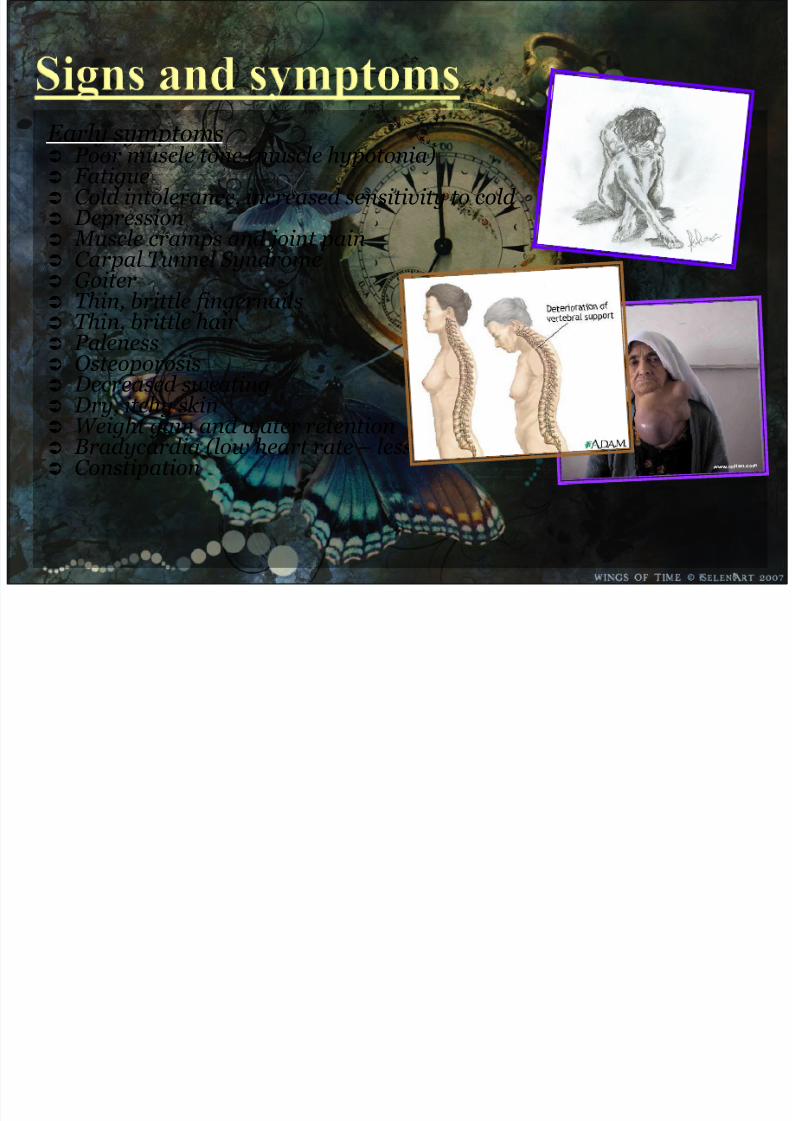
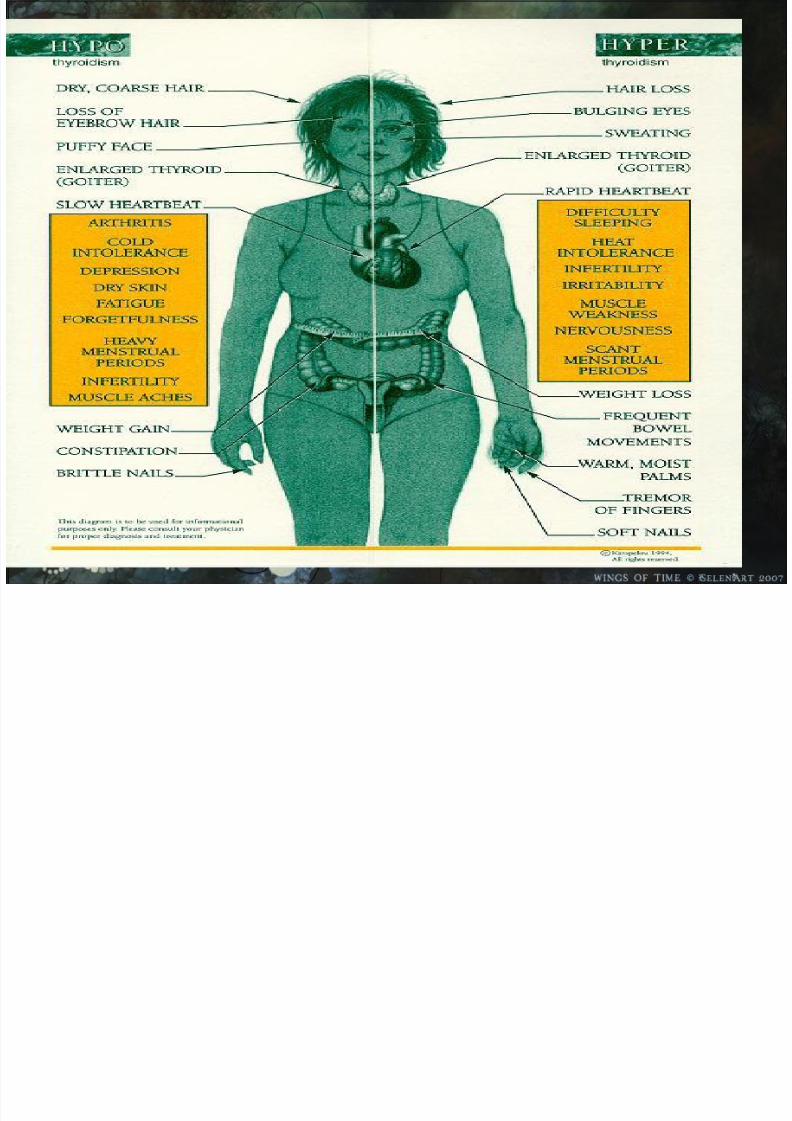
Early symptoms Poor muscle tone (muscle hypotonia) Fatigue Cold intolerance, increased sensitivity to cold Depression Muscle cramps and joint pain Carpal Tunnel Syndrome Goiter Thin, brittle fingernails Thin, brittle hair Paleness Osteoporosis Decreased sweating
Dry, itchy skin Weight gain and water retention Bradycardia (low heart rate – less than sixty beats per minute) Constipation
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 6/97
Late symptoms Slow speech and a hoarse, breaking voice –
deepening of the voice can also be noticed
Dry puffy skin, especially on the face Thinning of the outer third of the eyebrows (sign of
Hertoghe) Abnormal menstrual cycles
Low basal body temperature
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 7/97
Less common symptoms Impaired memory Impaired cognitive function (brain fog) and
inattentiveness A slow heart rate with ECG changes including low
voltage signals. Diminished cardiac output and decreased contractility.
Reactive (or post-prandial) hypoglycemia Sluggish reflexes Hair loss Anemia caused by impaired haemoglobin synthesis
(decreased EPO levels), impaired intestinal iron and folate absorption or B12 deficiency from perniciousanemia
Difficulty swallowing
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 8/97
About three percent of the general population ishypothyroidic. Factors such as iodine deficiency orexposure to Iodine-131 can increase that risk. There are anumber of causes for hypothyroidism. Iodine deficiency is
the most common cause of hypothyroidism worldwide. Iniodine-replete individuals hypothyroidism is generallycaused by Hashimoto's thyroiditis, or otherwise as aresult of either an absent thyroid gland or a deficiency in
stimulating hormones from the hypothalamus or pituitary.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 9/97
Thyroid hormone replacement therapy generallymaintains normal thyroid hormone levels unless
treatment is interrupted or discontinued.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 10/97
II. ANATOMY
&PHYSIOLOGY
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 11/97
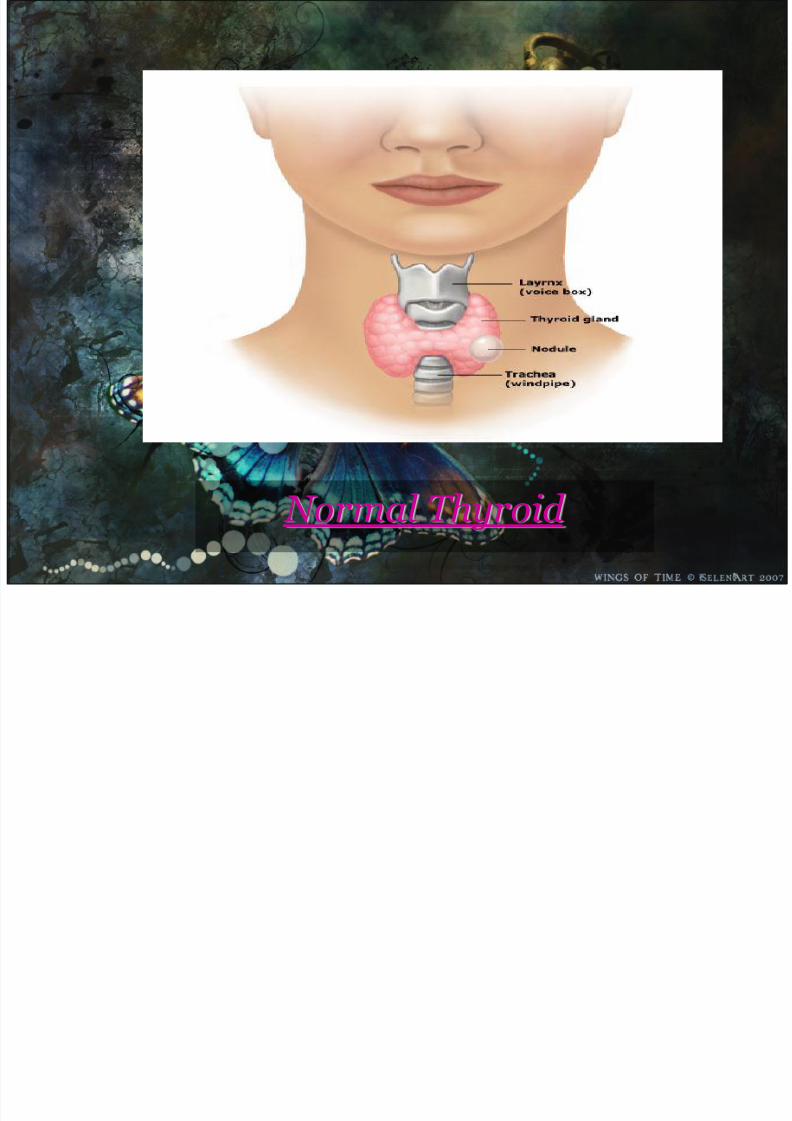
The thyroid glands are found on the trachea.The main hormone produced is called thyroxine. This hormone controls the growth
and development of animals. Iodine isrequired for its production.
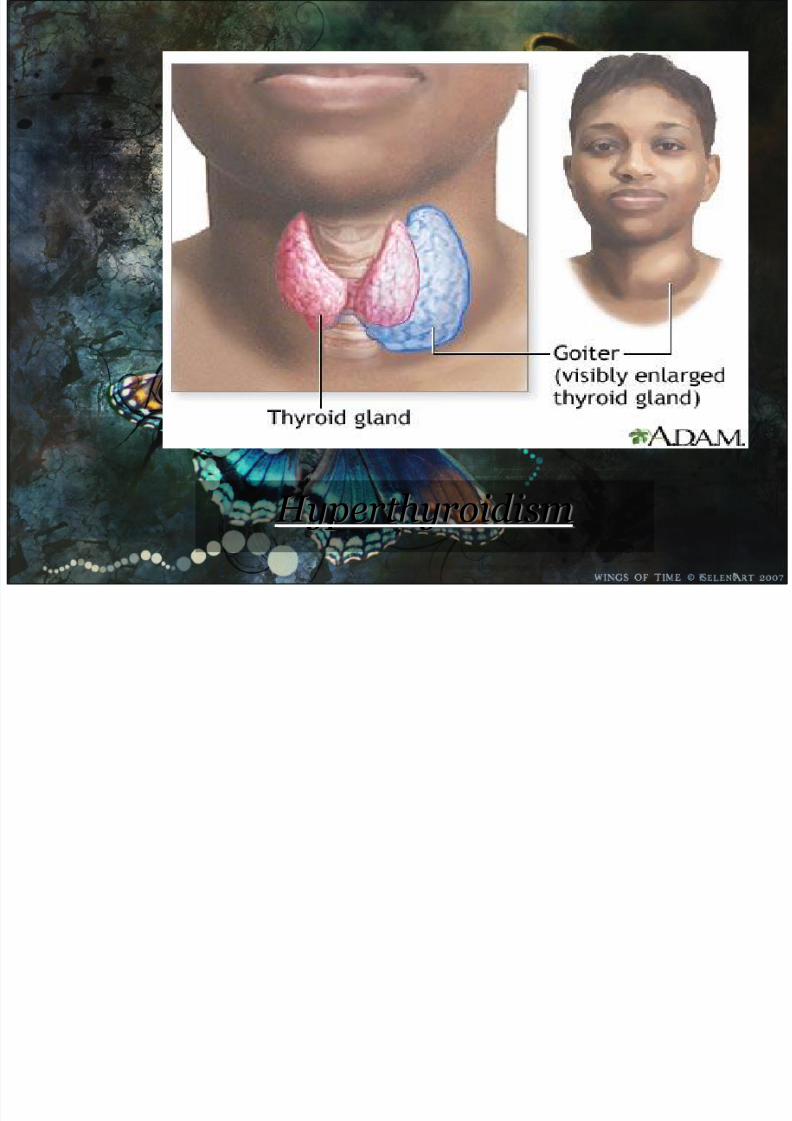
Lack of thyroxine causes deformation and retardation. The glands swell if not enoughhormone is produced – this is called goitre inhumans.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 12/97
These are located on either side of the thyroid. They produce two hormones: Parathormone and Calcitonin.These hormones control the level of calcium,magnesium and phosphate in the body.
Thymus
A very small gland located on the neck. Has someinvolvement in the production of lymphocytes, whichare involved in immune response.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 13/97
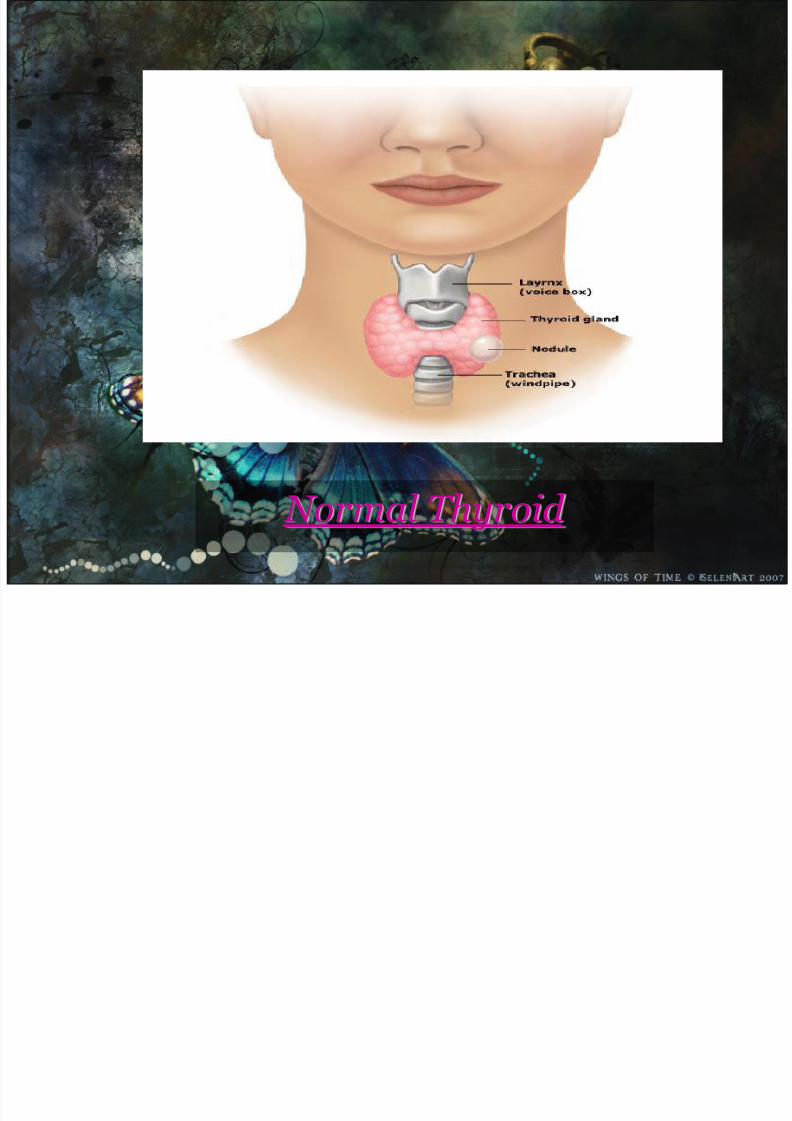
Normal Thyroid
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 14/97
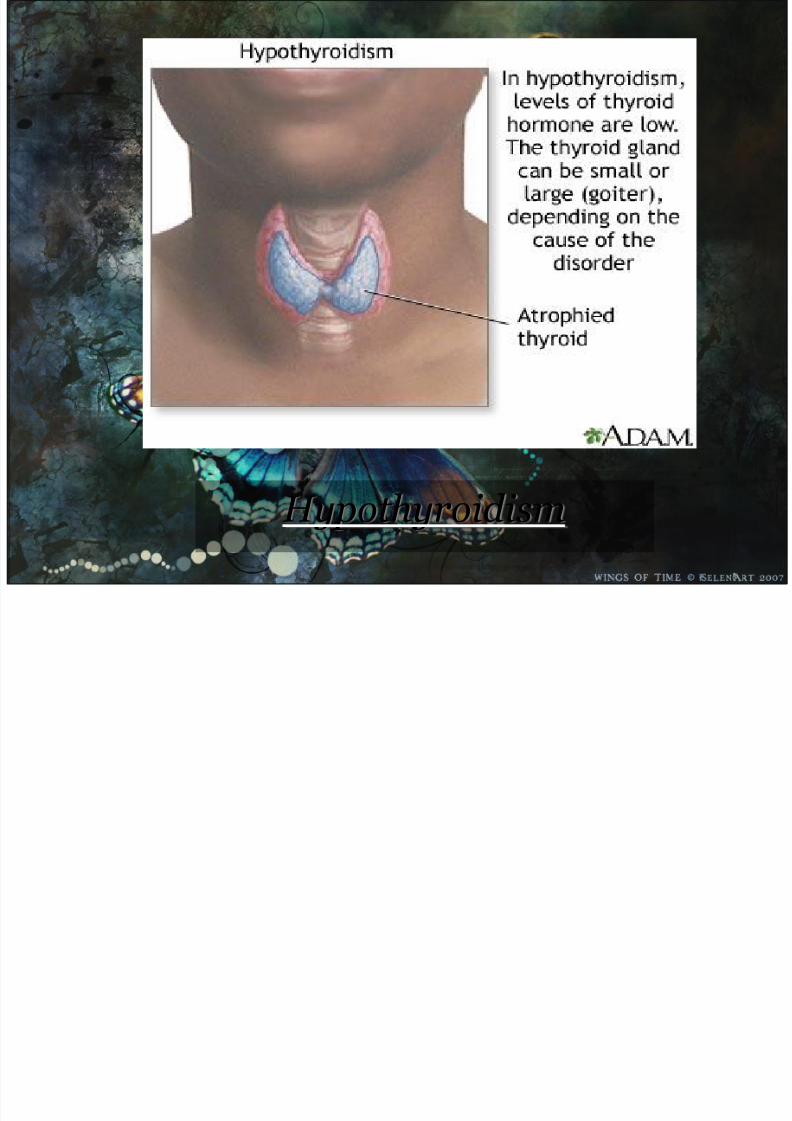
Hypothyroidism
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 15/97
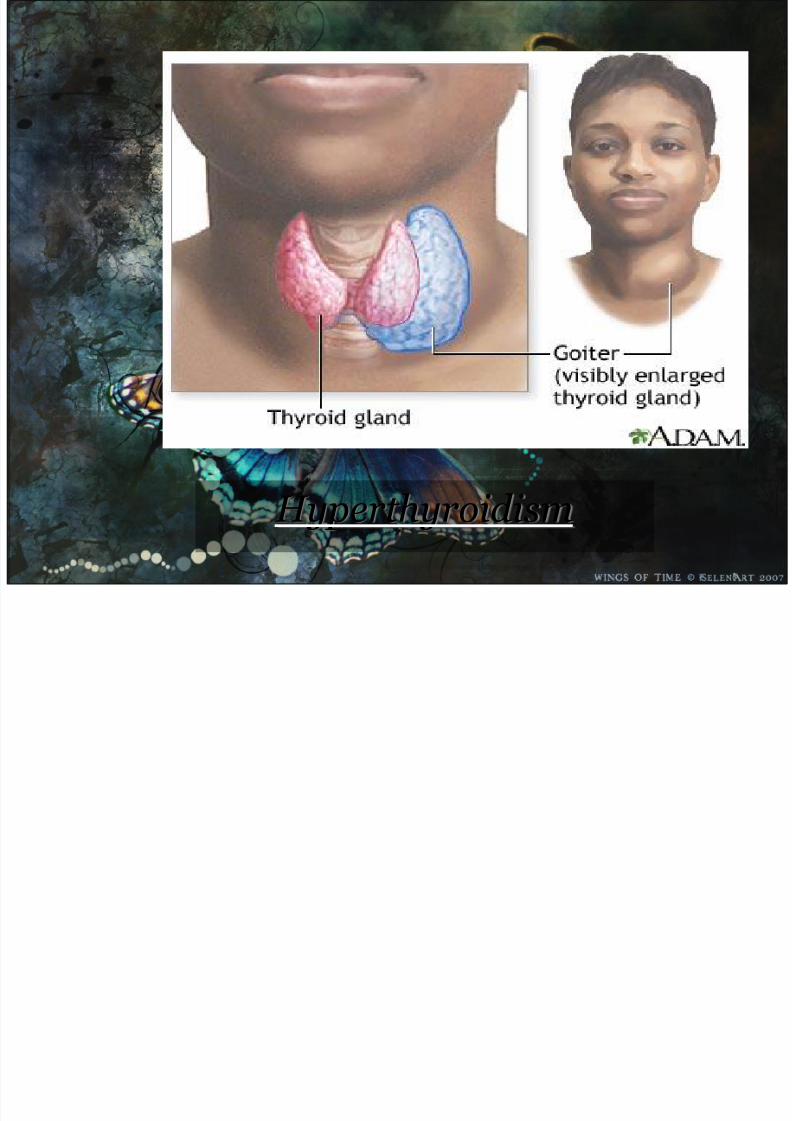
Hyperthyroidism
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 16/97
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 17/97
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 18/97
IV. NURSING DIAGNOSIS
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 19/97
Imbalanced Nutrition: More than Body Requirementsrelated to a slowed metabolic rate resulting in weight gain
Activity Intolerance related to weakness and apathysecondary to a decreased metabolic rate resulting in anincreased heart rate and shortness of breath with activity
Constipation related to decreased peristalsis secondary toslowed metabolic rate and activity intolerance, resultingin decreased frequency of stools and painful defecation
Hypothermia related to slowed metabolic rate resultingin subnormal body temperature
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 20/97
V. NURSING INTERVENTIONS
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 21/97
The patient with hypothyroidism experiencesdecreased energy and moderate to severelethargy. As a result, the risk for
complications from immobility increases. A major role of the nurse is assisting with
care and hygiene while encouraging the patient to participate in activities within established tolerance levels to prevent the complications of immobility.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 22/97
The nurse closely monitors the patients ital signsand cognitive level to detect the following:
Deterioration of physical and mental status
Signs and symptoms indicating that treatment has resulted in the metabolic rate exceeding theability of the cardiovascular and pulmonarysystems to respond.
Continued limitations or complications of myxedema
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 23/97
The patient often experiences chilling and extreme intolerance to cold, even if the
room feels comfortable or hot to others. Extra clothing and blankets are provided, and the patient is protected from drops
Use of heating pads and electric blanket is
avoided because of the risk of peripheral vasodilation, further loss of body heat, and vascular collapse.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 24/97
The patient with moderate to severehypothyroidism may experience severeemotionally actions to changes in appearance
and body image and the frequent delay indiagnosis. As hypothyroidism is treated successfully and symptoms subside, the patient may experience depression and guilt as a result of the progression and severity of symptoms that occurred.
The nurse informs the patient and family that the symptoms and inability to recognize them
are common and part of the disorder itself.

7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 25/97
Because most hypothyroidism treatment takes place at home, the patient and familyrequire information and instruction that will enable them to monitor the patients condition
and response to therapy. The nurse instructs the patient about the
desired actions and side effects of meditations about how and when to take
prescribe medications. The nurse provides written instructions and
guidelines for the patient and family.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 26/97
The patient with hypothyroidism and myxedema need considerable follow-upand healthcare.
Assistance the nurse reinforces theimportance of continued thyroid hormonereplacement and periodic follow-up and instructs the patient and family members
about the signs of over medication and under medication.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 27/97
V. MEDICATIONS
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 28/97
Hypothyroidism is traditionally treated with thyroid hormone replacement therapy (either synthetic ornatural). Thyroid replacement therapy could includetaking levothyroxine (T 4 ), liothyronine (T 3 ), or acombination product that contains both T 4 and T 3. All o
these treatments work in the body like thyroxine, thehuman hormone that is normally produced by thethyroid gland, and subsequently converted to T 3, theactive hormone.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 29/97
The purpose of treatment is to replace the thyroid hormonethat is lacking. Levothyroxine is the most commonly used medication. Doctors will prescribe the lowest dose that effectively relieves symptoms and brings the TSH level to anormal range. If you have heart disease or you are older,your doctor may start with a very small dose.
Lifelong therapy is required unless you have a conditioncalled transient viral thyroiditis.
You must continue taking your medication even when your
symptoms go away. When starting your medication, yourdoctor may check your hormone levels every 2 - 3 months. After that, your thyroid hormone levels should bemonitored at least every year.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 30/97
Do NOT stop taking the medication when you feel better.Continue taking the medication exactly as directed by yourdoctor.
If you change brands of thyroid medicine, let your doctorknow. Your levels may need to be checked.
Some dietary changes can change the way your bodyabsorbs the thryoid medicine. Talk with your doctor if youare eating a lot of soy products or a high-fiber diet.
Thryoid medicine works best on an empty stomach and when taken 1 hour before any other medications. Do NOT take thyroid hormone with calcium, iron, multivitamins,alumin hydroxide antacids, colestipol, or other medicinesthat bind bile acids, or fiber supplements.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 31/97
MEDICAL MANAGEMENT
(HYPOTHYROIDISM)
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 32/97
Treatment
Treating Overt Hypothyroidism.
Patients with overt hypothyroidism, indicated by clearsymptoms and blood tests that show high TSH (generally10 mU/L and above) and low thyroxine (T4) levels, must have thyroid replacement therapy.
Treating Subclinical or Mild Hypothyroidism.
Considerable debate exists about whether to treat patients with subclinical hypothyroidism (slightly higherthan normal TSH levels, normal thyroxine levels, and noobvious symptoms). Some doctors opt for treatment and others opt for simply monitoring patients.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 33/97
It is not clear if the benefits of treating subclinical hypothyroidismoutweigh the risks and potential complications. Doctors who do not advocate treatment argue that thyroid levels can vary widely, and
subclinical hypothyroidism may not persist. In such cases,overtreatment leading to hyperthyroidism is a real risk.
There is reasonable evidence and consensus to recommend treatment for subclinical hypothyroidism in the presence of other factors, including:
High total or LDL cholesterol levels Blood tests that show autoantibodies indicating a future risk for Hashimoto's thyroiditis or other forms of other autoimmune hypothyroidism Blood tests that show TSH levels greater than 10 mU/LGoiter Pregnancy
Female infertility associated with subclinical hypothyroidism
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 34/97
Treatment is optional in patients with subclinical hypothyroidism who have no obvious symptoms and normal cholesterol levels. Some doctors feel that treating
this group of patients will prevent progression to overt hypothyroidism and future heart disease, as well asincrease a patient's sense of well-being. However, theevidence to support treatment of this patient group is not nearly as strong. Many doctors recommend against
treatment and suggest that these patients should simplyhave lab tests every 6 - 12 months.
Suppressive Thyroid Therapy.
Suppressive thyroid therapy involves takinglevothyroxine in doses that are high enough to blockthe production of natural TSH but too low to causehyperthyroid symptoms. It may be used for patientswith large goiters or thyroid cancer.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 35/97
Treatment of Special Cases
Treating the Elderly and Patients with Heart Disease.
Thyroid dysfunction is common in elderly patients, with most having subclinical hypothyroidism. There is no evidence that this condition poses any great harm in this population, and most doctors recommend treating only high-risk patients.
Elderly patients, particularly people with heart conditions,usually start with very low doses of thyroid replacement,since thyroid hormone may cause angina or even a heart attack. Patients who have heart disease must take lower-than-average maintenance doses. Doctors do not recommend treatment for subclinical hypothyroidism in most elderly patients with heart disease. Such patients should be closelymonitored, however.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 36/97
Treating Newborns and Infants with Hypothyroidism. Babies born with hypothyroidism (congenital hypothyroidism) should be treated with levothyroxine(T4) as soon as possible to prevent complications. Earlytreatment can help improve IQ and other developmental
factors. However, even with early treatment, mild problems in mental functioning may last into adulthood. In general, children born with milder forms of hypothyroidism will fare better than those who have
more severe forms.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 37/97
Treatment During Pregnancy and for Postpartum Thyroiditis. Women who have hypothyroidism before becoming pregnant
may need to increase their dose of levothyroxine during pregnancy. Women who are first diagnosed with overthypothyroidism during pregnancy should be treated immediately, with quick acceleration to therapeutic levels.
Although not well proven, doctors often recommend treating patients diagnosed with subclinical hypothyroidism while pregnant. There are no risks to the developing baby when the pregnant woman takes appropriate doses of thyroid hormones.The pregnant woman with hypothyroidism should be monitored
regularly and doses adjusted as necessary. If postpartumthyroiditis develops after delivery, any thyroid medicationshould be reduced or temporarily stopped during this period.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 38/97
Treatment of Hypothyroidism and Iodide Deficiency.
People who are iodide deficient may be able to betreated for hypothyroidism simply by using iodized salt.In addition to iodized salt, seafood is a good source.Except for plants grown in iodine-rich soil, most other
foods do not contain iodine. The current RDA for iodideis 150 micrograms for both men and women, with anupper limit of 1,100 micrograms to avoid thyroid injury.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 39/97
Hyperthyroidism
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 40/97
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 41/97
Hyperthyroidism is the term for overactive tissue withinthe thyroid gland, resulting in overproduction and thus an
excess of circulating free thyroid hormones: thyroxine (T 4 ),triiodothyronine(T 3 ), or both. Thyroid hormone isimportant at a cellular level, affecting nearly every type of tissue in the body.
Thyroid hormone functions as a stimulus to metabolismand is critical to normal function of the cell. In excess, it both overstimulates metabolism and exacerbates the effect of the sympathetic nervous system, causing "speeding up" of various body systems and symptoms resembling an
overdose of epinephrine (adrenaline). These include fast heart beat and symptoms of palpitations, nervous systemtremor and anxiety symptoms, digestive systemhypermotility (diarrhea), and weight loss.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 42/97
weight loss (often accompanied by an increased
appetite) anxiety intolerance to heat hair loss
muscle aches weakness fatigue hyperactivity Irritability Apathy depression polyuria and sweating.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 43/97
The major causes in humans are:Graves' disease (the most common etiology with 70-
80%) Toxic thyroid adenoma
Toxic multinodular goitre
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 44/97
Hyperthyroidism is generally treatable and carriesa good prognosis. Most patients lead normal lives
with proper treatment. Thyroid storm, however, canbe life threatening and can lead to heart, liver, orkidney failure.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 45/97
II. ANATOMY
&PHYSIOLOGY
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 46/97
The thyroid glands are found on the trachea.The main hormone produced is called thyroxine. This hormone controls the growth
and development of animals. Iodine isrequired for its production.
Lack of thyroxine causes deformation and retardation. The glands swell if not enoughhormone is produced – this is called goitre inhumans.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 47/97
These are located on either side of the thyroid. They produce two hormones: Parathormone and Calcitonin.These hormones control the level of calcium,magnesium and phosphate in the body.
Thymus
A very small gland located on the neck. Has someinvolvement in the production of lymphocytes, whichare involved in immune response.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 48/97
Normal Thyroid
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 49/97
Hypothyroidism
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 50/97
Hyperthyroidism
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 51/97
III. PATHOPHYSIOLOGY
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 52/97
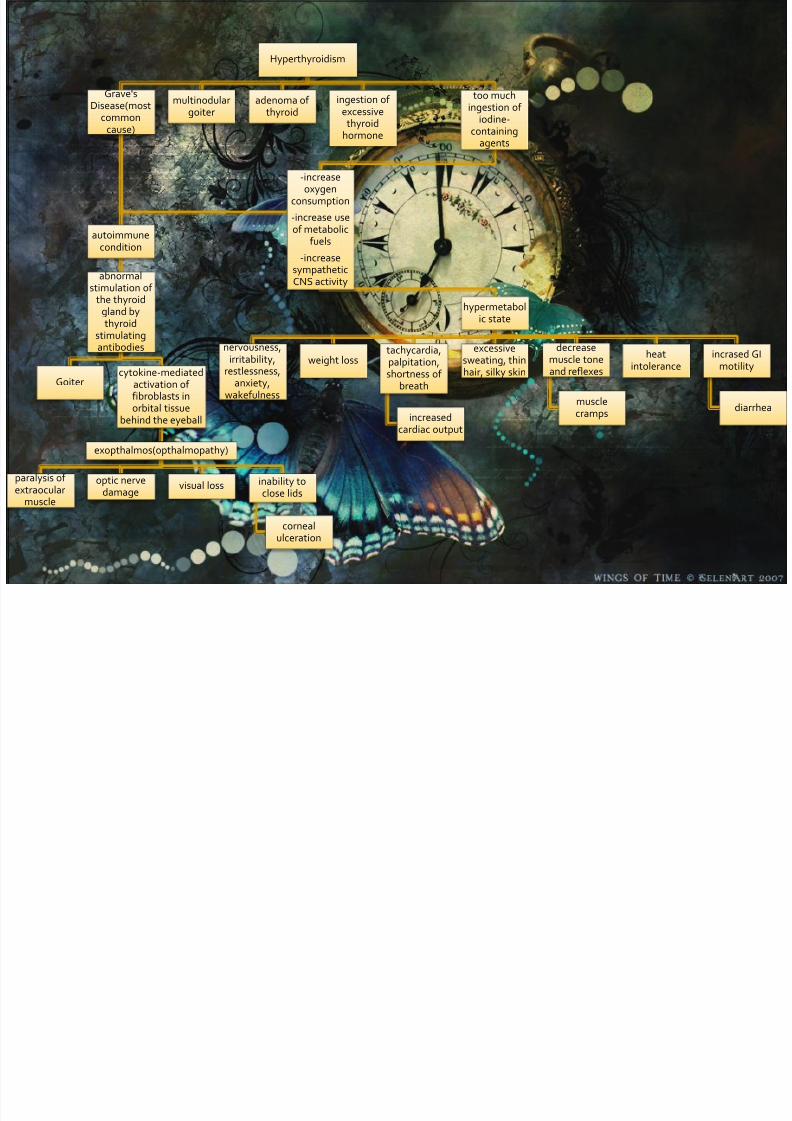
Hyperthyroidism
Grave'sDisease(most
commoncause)
autoimmunecondition
abnormalstimulation of
the thyroidgland bythyroid
stimulatingantibodies
Goitercytokine-mediated
activation of fibroblasts inorbital tissue
behind the eyeball
exopthalmos(opthalmopathy)
paralysis of extraocular
muscle
optic nervedamage
visual loss inability toclose lids
cornealulceration
multinodulargoiter
adenoma of thyroid
ingestion of excessive
thyroidhormone
too muchingestion of
iodine-containing
agents
-increaseoxygen
consumption
-increase useof metabolic
fuels
-increasesympathetic
CNS activity
hypermetabolic state
nervousness,irritability,
restlessness,anxiety,
wakefulness
weight losstachycardia,palpitation,shortness of
breath
increasedcardiac output
excessivesweating, thinhair, silky skin
decreasemuscle toneand reflexes
musclecramps
heatintolerance
incrased GImotility
diarrhea
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 53/97
IV. NURSING DIAGNOSIS
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 54/97
Imbalanced Nutrition: Less than Body Requirementsrelated to accelerated metabolic rate resulting in weight loss and decreased energy levels
Activity Intolerance related to exhaustion secondary toaccelerated metabolic rate resulting in inability to performactivity without shortness of breath and significant increases in heart rate
Hyperthermia related to accelerated metabolic rateresulting in fever, diaphoresis, and reported heat intolerance
Impaired Social Interaction related to extreme agitation,hyperactivity, and mood swings resulting in inability torelate effectively with others

7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 55/97
V. NURSING INTERVENTIONS
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 56/97
Rapid movement of food through thegastrointestinal tract may result tonutritional imbalance and further
weight loss. Highly seasoned foods and stimulants
such as coffee, tea, cola, and alcohol arediscouraged to reduce the area.
High calorie, high protein foods areencouraged.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 57/97
The patient needs reassurance that the emotional reactions being experience are a result of thedisorder and that with effective treatment thosesymptoms will be controlled.
Use a calm, unhurried approach with the patient.
Stressful experiences are minimized; therefore,if hospitalized, the patient is not placed in aroom with very ill or talkative patients.
The environment is kept quite and uncluttered.
The nurse encourages relaxing activities if theydo not overestimate the patient.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 58/97
The patient is likely to experience changes inappearance, appetite and weight.
The nurse conveys and understanding of the patients concern about these problems and assists
the patient to develop effective coping strategies. If changes in appearance are very disturbing to
patient, mirrors maybe covered or removed.
The nurse reminds the family members and
personnel to avoid bringing these changes to the patient’s attention.
The nurse explains to the patient and family that most of these changes are expected to disappearwith effective treatment.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 59/97
The patient finds a normal roomtemperature too warm because of an
exaggerated metabolic rate and increased heat production.
The nurse maintains the environment at a
cool, comfortable temperature and changes bedding and clothing as needed.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 60/97
The nurse closely monitors the patient with
hyperthyroidism for signs and symptomsthat maybe indicative of thyroid storm. Anti-thyroid medications maybe prescribe to
reduce thyroid hormone levels.
Propranolol and digitalis maybe prescribe totreat cardiac symptoms.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 61/97
The nurse teaches the patient how and when to take prescribe medication, and provides instructionsabout the essential role of the medication and broader therapeutic plan.
The nurse provides a written plan for the patient touse at home
The nurse identifies adverse effects that should bereported if they occur.
The nurse also advises the patient to avoid stressful situations that may precipitate thyroid storm.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 62/97
The nurse reinforces to the patient and familythe importance of long-term follow-up becauseof the risk for hypothyroidism afterthyroidectomy or treatment with anti-thyroid
medications or radioactive iodine.The nurse also assesses the patient for changes
indicating return to normal thyroid function and signs and symptoms of hyperthyroidism and
hypothyroidism.The nurse reminds the patients and family about
the importance of health promotion activitiesand recommended health screening.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 63/97
VI. MEDICAL MANAGEMENT
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 64/97
Radioiodine is considered the treatment of choice forhyperthyroidism, but in some situations, methimazole
therapy is preferred, such as in cats with pre-existingrenal insufficiency.
Methimazole blocks thyroid hormone synthesis, and controls hyperthyroidism in more than 90% of cats that tolerate the drug. Unfavorable outcomes are usually dueto side effects such as gastrointestinal (GI) upset, facial
excoriation, thrombocytopenia, neutropenia, or liverenzyme elevations; warfarin-like coagulopathy ormyasthenia gravis have been reported but are rare.
S i l P d
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 65/97
Surgical Procedure Surgery - this involves surgically removing thethyroid gland (thyroidectomy). It may be an option for patients who cannot tolerate anti-thyroid medications,or those who do not wish to receive radioactive iodinetherapy. Patients will subsequently require thyroxinetreatment to make sure their blood levels of thyroid
hormones are adequate.
The operative procedure to treat hyperthyroidism isknown as a near total thyroidectomy
It is performed under general anesthesia.
The surgeon makes an incision in the skin lines acrossthe front of the neck and carefully exposes the thyroid gland.
Precautions are taken to identify, isolate, and protect
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 66/97
fy, , pimportant structures in the area of the thyroid gland. Twoare particularly important:
1. The laryngeal nerve, which is vital for the proper function of the larynx or voice box, iscarefully identified and protected from traumaduring this procedure.
2. The four small parathyroid glands, which areembedded in thyroid tissue and produce ahormone necessary for maintenance of blood calcium levels, are also identified and preserved.
Most of the thyroid gland is removed.
The surgeon usually leaves about 3 to 8 grams, which isless the 0.3 ounces of thyroid tissue.
The procedure generally takes several hours.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 67/97
The incision usually heals well and is usually not evennoticeable
Surgical Care
Thyroidectomy is no longer the recommended first-linetherapy for hyperthyroid Graves disease. However, a recent retrospective cohort
studyjavascript:showcontent('active','references'); showed that one-third of all patients electing surgery as definitivemanagement did so without a specific indication, and the patient satisfaction with the decision for surgery asdefinitive management of Graves disease was high. Surgeryis a safe alternative therapeutic option in patients who arenoncompliant with or cannot tolerate antithyroid drugs,have moderate-to-severe ophthalmopathy, have largegoiters, or refuse or cannot undergo radioiodine therapy.
Thyroidectomy may be appropriate in the presence of a
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 68/97
Thyroidectomy may be appropriate in the presence of athyroid nodule that is suggestive of carcinoma.
In certain cases (eg, in pregnant patients with severe
hyperthyroidism), thyroidectomy may be indicated becauseradioactive iodine and antithyroid medications may becontraindicated.
It generally is reserved for patients with large goiters
with or without compressive symptoms. It also may be indicated in patients who refuseradioiodine as definitive therapy or in those in whom theuse of antithyroid drugs and/or radioiodine does not control hyperthyroidism.
Surgery provides rapid treatment of Graves diseaseand permanent cure of hyperthyroidism in most patients,and it has "negligible mortality and acceptable
morbidity" by experienced surgeons.
Ophthalmopathy
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 69/97
Ophthalmopathy
Near-total thyroidectomy has little, if any, effect on the course of
ophthalmopathy.
If ophthalmopathy is severe but inactive, orbital decompressionmay be performed. Reducing proptosis and decompressing the
optic nerve can be achieved by transantral orbital decompression.The major adverse effect is postoperative diplopia, which maynecessitate a second surgery on the extraocular muscles to correctthe problem.
Rehabilitative (extraocular muscle or eyelid) surgery is oftenneeded. Eyelid surgery (eg, severance of the Müller muscle, scleral or palatal graft insertion) can be performed to improve exposurekeratitis.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 70/97
VII. MEDICATIONS
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 71/97
Hyperthyroidism can be treated using medicine,radiation, or surgery. Many factors, such as the person's
age and the severity and type of hyperthyroidism, areimportant in determining which treatment is best. The
two main types of medicines used to treat hyperthyroidism are antithyroid drugs and beta-
blockers.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 72/97
Antithyroid drugs, such as methimazole (MMI orTapazole) and propylthiouracil (PTU), work bydecreasing the production of thyroid hormone. Both are very effective, but methimazole isgenerally preferred because of a rare risk of serious side effects with PTU. The illustrationshows that some hormone is made, but the thyroid
becomes much less efficient. When taken faithfully, these drugs are usually very effective incontrolling hyperthyroidism within a few weeks.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 73/97
For pregnant women, PTU is the preferred drug during the first trimester. After the first trimester, methimazole is preferred.
For patients with sustained forms of
hyperthyroidism, such as Graves' disease or toxic nodular
goiter, anti-thyroid medications are often
used. The goal with this form of drug therapyis to prevent the thyroid from producinghormones.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 74/97
Very rarely, patients treated with these medicationscan develop liver inflammation or a deficiency of white blood cells therefore, patients takingantithyroid drugs should be aware that they must stop their medication and call their doctor promptly
if they develop yellowing of the skin, a high fever, orsevere sore throat. The main shortcoming of antithyroid drugs is that the underlyinghyperthyroidism often comes back after they arediscontinued. For this reason, many patients withhyperthyroidism are advised to consider atreatment that permanently prevents the thyroid gland from producing too much thyroid hormone.
Cont’d
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 75/97
Rash itching or fever (but these are
uncommon)
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 76/97
MMI is usually preferred over PTU because it reverses hyperthyroidism more quickly and has fewer side effects. MMI requires an
average of 6 weeks to lower T4 levels tonormal and is often given before radioactiveiodine treatment. MMI can be taken once perday.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 77/97
PTU blocks the conversion of T4 to T3 in non-thyroid tissue, but it does not reverse
hyperthyroidism as rapidly as MMI. PTU must be taken two to three times per the day.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 78/97
PTU used to be the drug of choice during pregnancybecause it is thought to have a lower risk of causingbirth defects. But experts now recommend that PTU be
given during the first trimester only. This is becausethere have been rare cases of liver damage in peopletaking PTU. After the first trimester, women should switch to methimazole for the rest of the pregnancy.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 79/97
Beta-blockers, such as atenolol, are oftenstarted as soon as the diagnosis of hyperthyroidism is made. While beta-blockersdo not reduce thyroid hormone production,
they can control many of the bothersomesymptoms, such as rapid heart rate, tremors,anxiety, and heat intolerance. Once thehyperthyroidism is under control (byantithyroid drugs, surgery, or radioactiveiodine), the beta-blocker is stopped.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 80/97
Destroying the thyroid with radiation, called radioiodine ablation, is a permanent way toresolve hyperthyroidism. The amount of radiationused is small and does not cause cancer. This is themost widely used treatment in the United States.
Radioiodine is given in liquid or capsule form, and it works by attacking and destroying much of thethyroid tissue. This takes about 6 to 18 weeks. People with severe symptoms, older adults, and people with heart problems should first be treated
with an antithyroid drug to control symptoms. Most patients who receive radioiodine develophypothyroidism and need to take thyroid hormonesupplements for the rest of their lives.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 81/97
Sometimes, after apparently successful treatment,the condition returns and further treatment isneeded.
About 20 percent of those who use radioiodinetreatment require a second dose. These peopleusually have severe hyperthyroidism or a verylarge goiter.
Occasionally, people whose hyperthyroidism iscaused by Graves' disease may find that their eyesymptoms worsen after therapy.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 82/97
People who undergo this therapy should avoid close physical contact, especially with youngchildren and pregnant women, for three toseven days after treatment because of the possibility of exposing them to low doses of radiation. This can be difficult for parents of young children. Patients will need to see their
clinician on a regular basis after treatment tohave thyroid hormone levels checked and monitor for hypothyroidism or recurrent hyperthyroidism.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 83/97
VIII. DIAGNOSTIC
PROCEDURES
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 84/97
Hypo t h y r o i d i sm
&
Hype r t h y r o i d i sm
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 85/97
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 86/97
The TSH (or Thyroid Stimulating Hormone) assay has been recognized as
an exquisitely sensitive indicator of thyroid status.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 87/97
The T4 (or Thyroxin) assay complements
the TSH assay, and is used to confirm athyroid disorder when suggested by anabnormal TSH.
The T3 (or Triiodothyronine) assay is
another assay which is used in thediagnosis of thyroid disorders.
T3
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 88/97
The T3 Resin Uptake assay is used in calculatingthe Free Thyroxin Index (FTI).
Autoantibodies of clinical interest in thyroid disease include thyroid-stimulating antibodies
(TSAb), TSH receptor-binding inhibitoryimmunoglobulins (TBII), antithyroglobulinantibodies (Anti-Tg Ab) and the antithyroid peroxidase antibody (Anti-TPO Ab).
Other Tests
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 89/97
Similar in its use for evaluating a breast
mass, ultrasound can be used to assess athyroid nodule.
Fine Needle Aspiration (FNA) has becomethe single-most important step in theevaluation of a thyroid nodule.
Fine Needle Aspiration
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 90/97
The thyroid glands' ability to concentrate iodineand certain radioactive isotopes has beenexploited in a nuclear imaging technique knownas the thyroid scan.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 91/97
X. DIET
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 92/97
No foods have been shown in clinical studies toimprove or worsen the symptoms of
hyperthyroidism. However, that doesn't meanyou shouldn't pay attention to what you eat. Ahealthy, well-balanced diet is important forthose with hyperthyroidism -- both during and after treatment. It should include things likeruits, vegetables, and lean proteins, with limited
amounts of foods high in fat and cholesterol.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 93/97
Healthcare providers generally advise their patients to follow good dietary habits followingtreatment for hyperthyroidism. The reason isthat considerable weight gain is common withthis condition. One study showed an averageweight gain of about 12 pounds (5.4 kg) in people followed for up to two years after
hyperthyroidism treatment.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 94/97
Graves' disease
Preexisting obesity Previous weight loss as a result of
hyperthyroidism
Hypothyroidism following treatment.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 95/97
The good news is that research has also shownthat this weight gain can be minimized by following sensible dietary habits. If you have anoveractive thyroid, you should strive to eat awell-balanced diet and control your weight.
A well-balanced diet can help you feel betterand can be a positive step in dealing with
hyperthyroidism. It can also help decrease yourchances of developing heart disease or certaintypes of cancer.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 96/97
Eat a heart-healthy diet. This diet should include foodssuch as:
Fruits, vegetables, grains, and fat-free or low-fat milk and milk products
Lean meats, poultry, fish, beans, eggs, and nuts. Limit foods with saturated fats, trans fats, cholesterol,
sodium (salt), and added sugars.
Get regular physical activity for at least 30 minutes aday on most days of the week.
Limit your intake of alcohol.
7/15/2019 Pathophysiology of Hyperthyroidism
http://slidepdf.com/reader/full/pathophysiology-of-hyperthyroidism-563280be738e6 97/97
END
-To God be the Glory-






![Pathophysiology: Heart Failure - Columbia University Heart Failure ... – TPR = [MAP - CVP] / CO, and ... – Anemia – Systemic arteriovenous fistulas – Hyperthyroidism](https://img.dokumen.tips/doc/110x75/5aa356057f8b9ab4208e3286/pathophysiology-heart-failure-columbia-heart-failure-tpr-map-cvp.jpg)