Embed Size (px)
DESCRIPTION
vujhhnnn
Citation preview

7/16/2019 Pathology Lab v Diffuse and Multinodular Goiter.
http://slidepdf.com/reader/full/pathology-lab-v-diffuse-and-multinodular-goiter 1/18
PATHOLOGY LAB V-DIFFUSE AND MULTINODULAR GOITER .
Arben Santo.
CASE OUTLINE.
Case Presentation: Aina H.
Nontoxic goiter Dyshormonogenetic goiter Toxic multinodular goiter
Endemic goiter
OBJECTIVES.
After completing this module the student
will be able to:
1. Define “goiter” and explain the principlesof classification of goiters into simple
(nontoxic) and toxic, diffuse and
multinodular 2. Explain the principle of classification of
goiters into sporadic and endemic types
3. Describe the gross and histopathologic
findings of diffuse and multinodular goiters
4. Describe the clinical and radiological
findings in nontoxic goiters
5. Describe the pathogenesis of nontoxicgoiters6. Describe the etiology, pathogenesis,
pathology and clinical characteristics
of dyshormonogenetic goiter 7. Describe pathological and clinical
features of toxic multinodular goiters
REFERENCES.1. Robbins and Cotran Pathologic Basis of
Disease, 8th
edition, p. 1116-1118
2. Loyd RV, Douglas BR, and Young WF,Atlas of nontumor pathology: Endocrine
diseases. Armed Forces Institute of
Pathology, Washington, DC, 2002
CASE PRESENTATION: AINA H. Aina, a 50-year-old female Cambodian refugee, presents with enlargement of a longstandingneck mass. Physical examination reveals a multinodular thyroid gland, all of which moves with
swallowing. There is a dominant, left-lobe, 6-cm nodule, which the patient said had enlarged
abruptly 10 days before. Her thyroid gland extends below the sternal notch into the anterior
mediastinum, so the inferior portion is not palpable. A fine-needle aspiration smear of the left-lobe mass shows evidence of a hemorrhagic colloid cyst. The patient is taken to surgery because
of her sensation oflaryngeal compression, and a total thyroidectomy is performed. The
pathologist notes a multinodular goiter and confirms the large hemorrhagic cyst, but also findsa solid 2.5-cm nodule in the mediastinal portion of the thyroid gland. This mass is partially
encapsulated, but enlarged follicular cells forming small follicles are seen to penetrate the
capsuleand to invade vascular channels around the nodule. The cells have round, euchromaticnuclei without inclusions, grooves, or papillae. A definitive diagnosis of follicular thyroid
carcinoma complicating a multinodular goiter was made.
The patient does not return for follow-up visits until one year later, when she notes pain in
her left humerus. On x-ray studies, a lytic lesion is found, as are several small nodules in thelungs. Her TSH (thyroid-stimulating hormone, thyrotropin) level is markedly elevated.
DEFINITIONS.
1. Goiter.
7/16/2019 Pathology Lab v Diffuse and Multinodular Goiter.
http://slidepdf.com/reader/full/pathology-lab-v-diffuse-and-multinodular-goiter 2/18
The term goiter is nonspecific and refers simply to an enlargement of the thyroid gland. Goiters
have a variety of etiologies ranging from inflammatory diseases (thyroiditis), non-neoplastic
enlargements (Graves disease), and neoplasms (thyroid adenoma or carcinoma). The presence of a goiter does not reflect the functional activity of the gland which can range from euthyroid to
hyperthyroid and hypothyroid states. Thyroid function may be normal (simple or nontoxic
goiter), overactive (toxic goiter), or underactive (hypothyroid goiter).A goiter may extend into the retrosternal space, with or without substantial anterior enlargement.Because of the anatomic relationship of the thyroid gland to the trachea, larynx, superior and
inferior laryngeal nerves, and esophagus, abnormal growth may cause a variety of compressive
syndromes.
2. Nontoxic goiter.
Nontoxic or simple goiter may be defined as any thyroid enlargement that is not associated with
hyperthyroidism or hypothyroidism and that does not result from inflammation (thyroiditis) or
neoplasia (thyroid adenoma or carcinoma).The term is usually restricted to the form that occurssporadically, i.e., in regions that are not the locus of endemic goiter . Although useful in
indicating the presence of the characteristics just noted, the term simple goiter can be a result of
different underlying abnormalities.The simple or nontoxic goiter may be diffuse or multinodular , but a diffuse goiter often evolves
into a nodular goiter.
Nontoxic goiters are characterized by diffuse hyperplasia of the thyroid gland and colloid
accumulation. Thyroid hyperplasia often results from disturbances of the feedback system inwhich decreased production of thyroid hormone can lead to increased production of thyrotropin-
releasing hormone (TRH) from the hypothalamus and thyroid stimulating hormone (TSH) from
the pituitary. TSH stimulates hyperplasia of the thyroid gland, leading to enlargement of thegland. 3. Toxic goiter. Toxic goiter is a goiter that is associated with hyperthyroidism. Examples of toxic goiters include
toxic multinodular goiter, and toxic thyroid adenoma. 4. Endemic goiter. Endemic goiter is defined as thyroid enlargement that occurs in more than 10% of a population,
and sporadic goiter is a result of environmental or genetic factors that do not affect the general population.
EPIDEMIOLOGY. Sporadic goiter is the most common cause of nontoxic goiter in the United States. The incidence
of sporadic nontoxic goiter has been estimated in North America at approximately 5%. Sporadic
diffuse nontoxic goiters are seen most frequently between 10 and 20 years of age. Nontoxic
multinodular goiters are usually seen in persons after 30 years of age. Generally, thedevelopment of palpable thyroid nodules and goiter progressively increases with age. The
prevalence of palpable nodules is approximately 5-6% in people aged 60 years, but on autopsy
and ultrasonographic imaging findings, the incidence of small, nonpalpable nodules approaches
50% in people aged 60 years.Sporadic goiter is more common in women than in men. The female-to-male ratio is 4:1.
ETIOLOGY.
7/16/2019 Pathology Lab v Diffuse and Multinodular Goiter.
http://slidepdf.com/reader/full/pathology-lab-v-diffuse-and-multinodular-goiter 3/18
The cause of sporadic goiter sporadic goiter is usually unknown. Causes of sporadic goiter
development can be quite variable.
1. Iodine deficiency.Goiter formation occurs with moderately deficient iodine intake of less than 50 microgram/day.
Severe iodine deficiency associated with intake of less than 25 microgram/day is associated with
hypothyroidism and cretinism.2. Goitrogens.Chemically-induced goiters may result from consumption of goitrogens. Goitrogens are
substances that suppress the function of the thyroid gland by interfering with iodine uptake,
which can, as a result, cause an enlargement of the thyroid, i.e., a goiter. There are various typesof goitrogens.
(A) Goitrogenic foods.
There are two general categories of foods that interfere with thyroid gland function: soybean-
related foods and cruciferous vegetables.Soybean-related foods. The soybean (Glycine max) is a species of legume native to Southeastern
Asia. Included in the category of soybean-related foods are soybeans themselves as well as soy
extracts, and foods made from soy, including soymilk, tofu and tempeh. It is the isoflavones insoy that have been associated with decreased thyroid hormone output. Isoflavones are naturally-
occurring substances that belong to the flavonoid family of nutrients. Isoflavones like genistein
appear to reduce thyroid hormone output by blocking activity of the enzyme thyroid
peroxidase (which is responsible for adding iodine onto the thyroid hormones).Cruciferous vegetables. A second category of foods associated with disrupted thyroid hormone
production is the cruciferous food family. Foods belonging to this family are called "crucifers,"
and include broccoli, cauliflower, Brussels sprouts, cabbage, mustard, rutabagas, kohlrabi, andturnips. Isothiocyanates are the category of substances in crucifers that have been associated with
decreased thyroid function. Like the isoflavones, isothiocyanates appear to reduce thyroid
function by blocking thyroid peroxidase.
Most goitrogens are inactivated with heat, but there is some evidence that isoflavones in soy arenot heat inactivated.
(B) Chemical goitrogens. Many drugs and environmental agents behave as goitrogens. The
following drugs have goitrogenic effects: propylthiouracil (used to treat hyperthyroidism,including Graves disease), lithium (used to treat bipolar disorder), phenylbutazone (used as
analgesic and antipyretic), aminoglutethimide (used to suppress adrenal function in Cushing
syndrome), iodine-containing expectorants (used to reduce chest congestion).The following environmental agents have goitrogenic effects: phenolic and phthalate ester
derivatives and resorcinol found downstream of coal and shale mines.
3. Dyshormonogenesis. Dyshormonogenetic goiter is a type of goiter resulting from enzyme defects in thyroid hormonesynthesis. Most cases are familial and inherited as autosomal recessive conditions.
4. Childhood head and neck radiation. Radiation exposure during childhood results goiter. CLINICAL PRESENTATION. Sporadic goiters are generally asymptomatic and found either by a clinician's physical
examination or by the patient's observation of neck enlargement (cosmetic disfigurement).
7/16/2019 Pathology Lab v Diffuse and Multinodular Goiter.
http://slidepdf.com/reader/full/pathology-lab-v-diffuse-and-multinodular-goiter 4/18
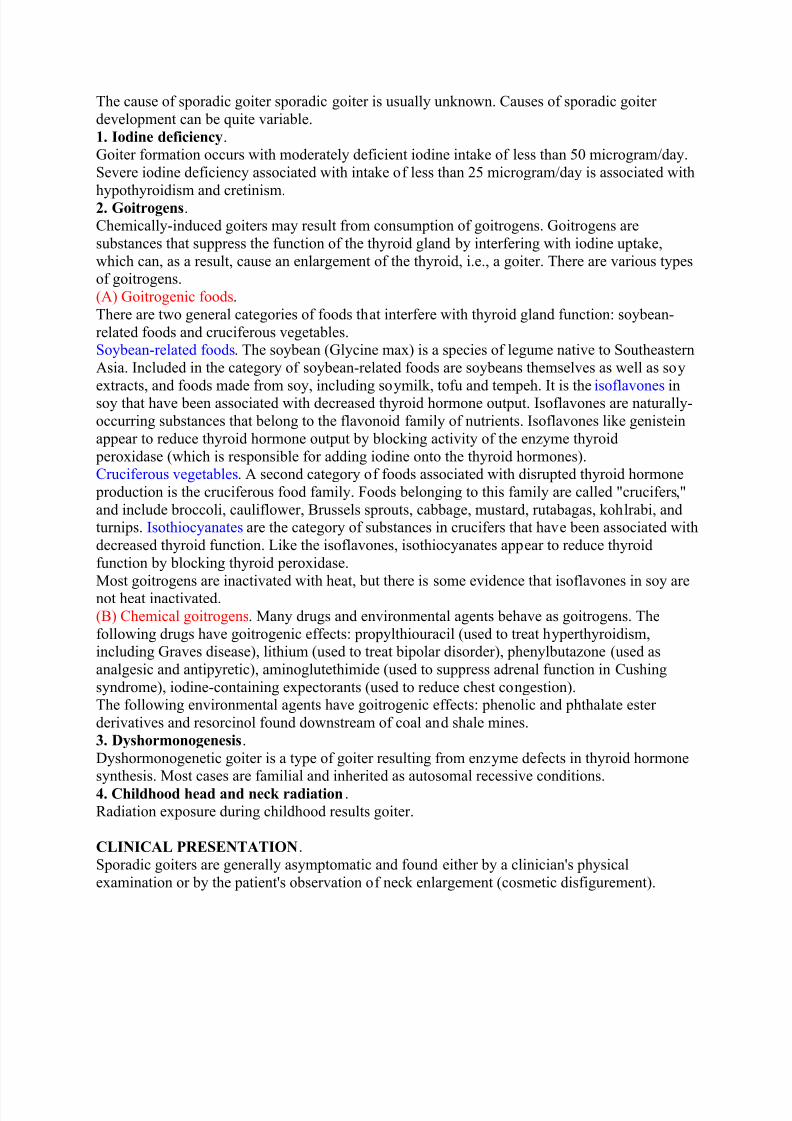
Occasionally, the goiter may produce symptoms caused by pressure on anterior neck structures
(neck discomfort). Large goiters may displace or compress the neck organs including the trachea
(wheezing, cough), the esophagus (dysphagia), and the recurrent laryngeal nerve (hoarseness,although this sign is usually more diagnostic of a thyroid carcinoma).
7/16/2019 Pathology Lab v Diffuse and Multinodular Goiter.
http://slidepdf.com/reader/full/pathology-lab-v-diffuse-and-multinodular-goiter 5/18
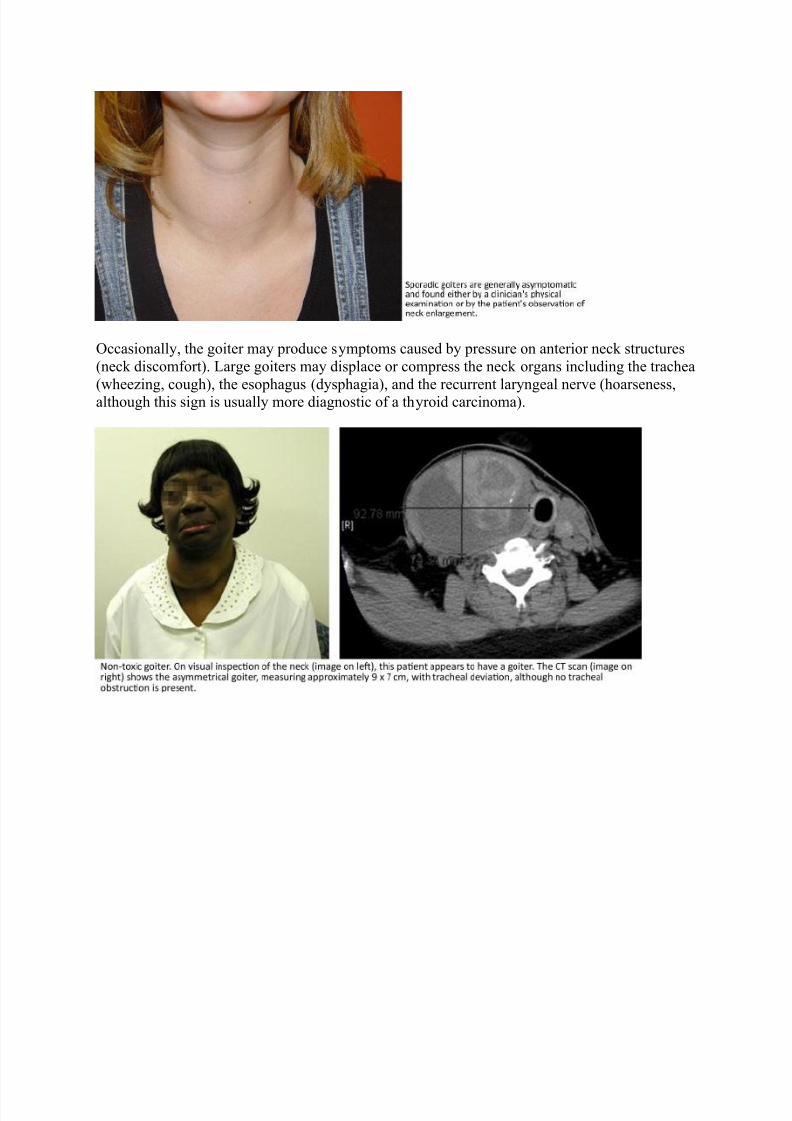
Rarely, the obstruction can be dangerous because of narrowing of the trachea and thedevelopment of tracheitis with edema and tracheomalacia, leading to severe narrowing of theairway with serious obstruction resulting in a respiratory emergency.
Sometimes, mechanical obstruction may result in superior vena cava syndrome, with
engorgement of facial and neck veins from narrowing of the thoracic inlet.
LABORATORY FINDINGS.
Thyroid function tests should be obtained, though the results of these are usually normal. Initial
screening should include TSH. Determination of serum TSH will distinguish nontoxic goitersfrom toxic goiters. In the absence of symptoms of hyper or hypothyroidism further testing is not
required. If the TSH is low, measurement of serum free thyroxine (free T4) and total
triiodothyronine (T3) is used to confirm the diagnosis of hyperthyroidism (i.e., toxic goiter).
IMAGING.
1. Ultrasonography.
High resolution ultrasonography is the imaging method of choice in the evaluation of thyroidgland morphology in goiters. This technique is capable of establishing goiter size and detecting
nodules as small as 0.3 cm in diameter, which means that it can differentiate diffuse goiters from
multinofular goiters.
2. CT scanning.
CT scanning is more precise. It can be used to delineate size and goiter extent. CT scanning does
a much better job than ultrasonography in determining the effect of the goitrous thyroid gland on
nearby structures.2. Scintigraphic thyroid scanning with (
123iodine or
99m technetium).
Thyroid scintigraphy is not routinely indicated in the assessment of diffuse goiter. The
radioactive iodine uptake is usually normal in diffuse goiter. Thyroid scintigraphy allows thediagnosis of multinodular goiter and helps in the identifying the function of a thyroid nodule (hot
nodule or cold nodule).
MORPHOLOGY.
7/16/2019 Pathology Lab v Diffuse and Multinodular Goiter.
http://slidepdf.com/reader/full/pathology-lab-v-diffuse-and-multinodular-goiter 6/18
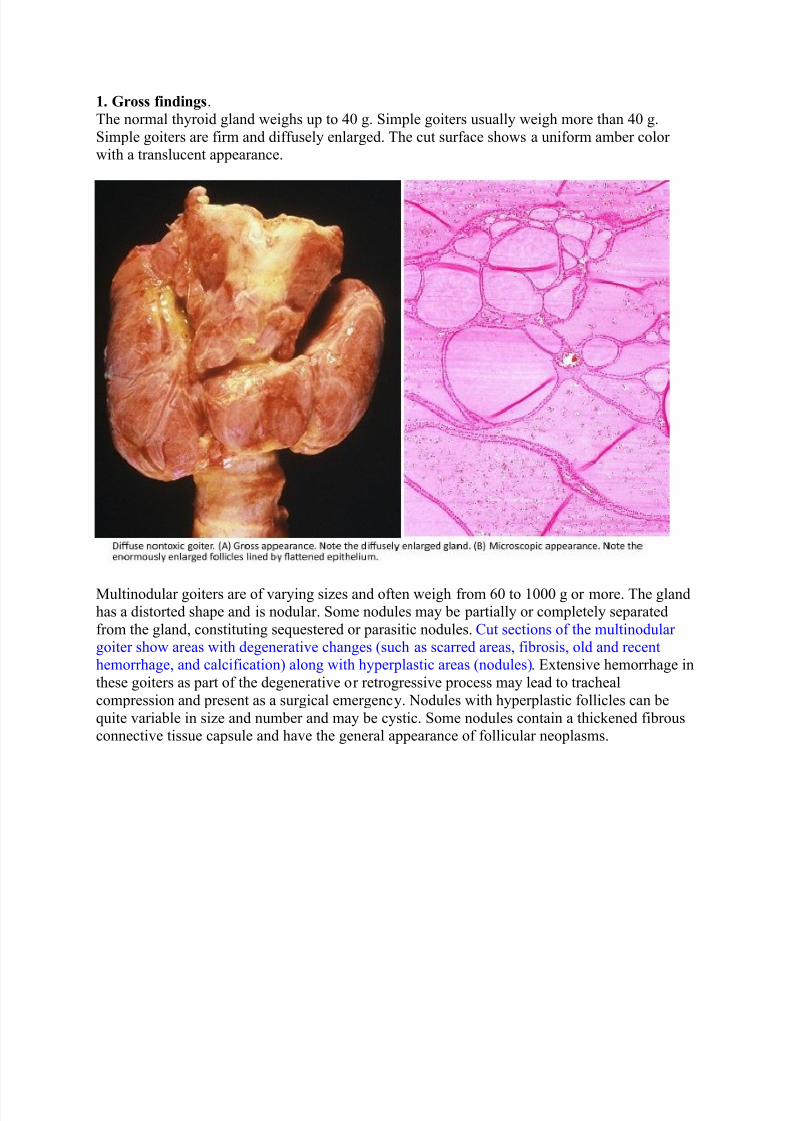
1. Gross findings.
The normal thyroid gland weighs up to 40 g. Simple goiters usually weigh more than 40 g.
Simple goiters are firm and diffusely enlarged. The cut surface shows a uniform amber color with a translucent appearance.
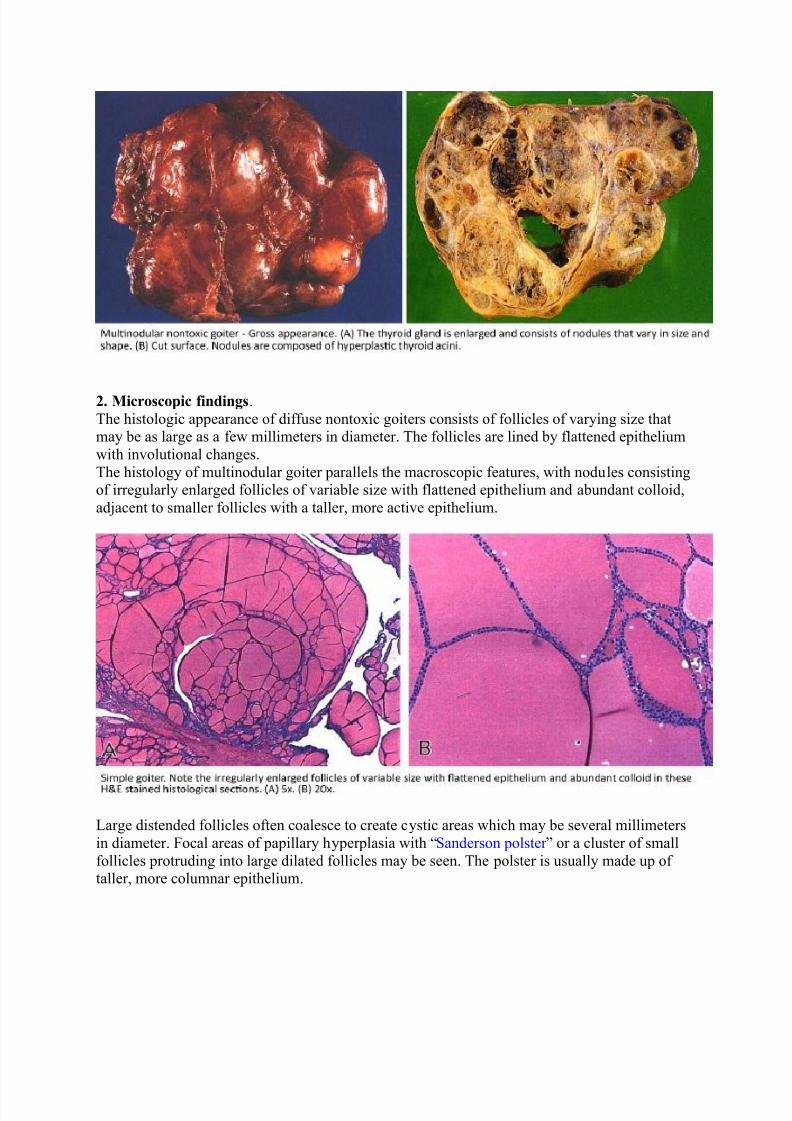
Multinodular goiters are of varying sizes and often weigh from 60 to 1000 g or more. The glandhas a distorted shape and is nodular. Some nodules may be partially or completely separated
from the gland, constituting sequestered or parasitic nodules. Cut sections of the multinodular goiter show areas with degenerative changes (such as scarred areas, fibrosis, old and recenthemorrhage, and calcification) along with hyperplastic areas (nodules). Extensive hemorrhage in
these goiters as part of the degenerative or retrogressive process may lead to tracheal
compression and present as a surgical emergency. Nodules with hyperplastic follicles can be
quite variable in size and number and may be cystic. Some nodules contain a thickened fibrousconnective tissue capsule and have the general appearance of follicular neoplasms.
7/16/2019 Pathology Lab v Diffuse and Multinodular Goiter.
http://slidepdf.com/reader/full/pathology-lab-v-diffuse-and-multinodular-goiter 7/18
2. Microscopic findings.
The histologic appearance of diffuse nontoxic goiters consists of follicles of varying size thatmay be as large as a few millimeters in diameter. The follicles are lined by flattened epithelium
with involutional changes.
The histology of multinodular goiter parallels the macroscopic features, with nodules consistingof irregularly enlarged follicles of variable size with flattened epithelium and abundant colloid,
adjacent to smaller follicles with a taller, more active epithelium.
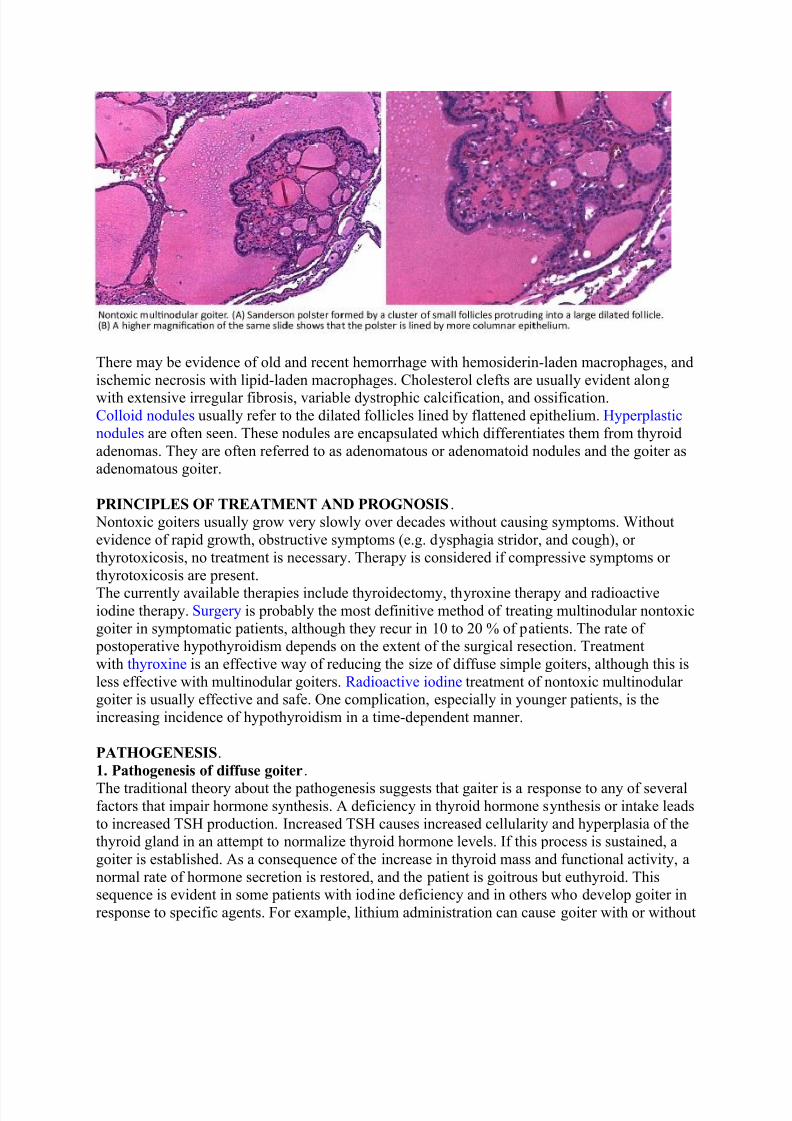
Large distended follicles often coalesce to create cystic areas which may be several millimeters
in diameter. Focal areas of papillary hyperplasia with “Sanderson polster ” or a cluster of small
follicles protruding into large dilated follicles may be seen. The polster is usually made up of taller, more columnar epithelium.
7/16/2019 Pathology Lab v Diffuse and Multinodular Goiter.
http://slidepdf.com/reader/full/pathology-lab-v-diffuse-and-multinodular-goiter 8/18
There may be evidence of old and recent hemorrhage with hemosiderin-laden macrophages, and
ischemic necrosis with lipid-laden macrophages. Cholesterol clefts are usually evident along
with extensive irregular fibrosis, variable dystrophic calcification, and ossification.Colloid nodules usually refer to the dilated follicles lined by flattened epithelium. Hyperplastic
nodules are often seen. These nodules are encapsulated which differentiates them from thyroid
adenomas. They are often referred to as adenomatous or adenomatoid nodules and the goiter asadenomatous goiter.
PRINCIPLES OF TREATMENT AND PROGNOSIS. Nontoxic goiters usually grow very slowly over decades without causing symptoms. Without
evidence of rapid growth, obstructive symptoms (e.g. dysphagia stridor, and cough), or
thyrotoxicosis, no treatment is necessary. Therapy is considered if compressive symptoms or
thyrotoxicosis are present.
The currently available therapies include thyroidectomy, thyroxine therapy and radioactiveiodine therapy. Surgery is probably the most definitive method of treating multinodular nontoxic
goiter in symptomatic patients, although they recur in 10 to 20 % of patients. The rate of postoperative hypothyroidism depends on the extent of the surgical resection. Treatment
with thyroxine is an effective way of reducing the size of diffuse simple goiters, although this is
less effective with multinodular goiters. Radioactive iodine treatment of nontoxic multinodular goiter is usually effective and safe. One complication, especially in younger patients, is the
increasing incidence of hypothyroidism in a time-dependent manner.
PATHOGENESIS.
1. Pathogenesis of diffuse goiter.
The traditional theory about the pathogenesis suggests that gaiter is a response to any of severalfactors that impair hormone synthesis. A deficiency in thyroid hormone synthesis or intake leads
to increased TSH production. Increased TSH causes increased cellularity and hyperplasia of thethyroid gland in an attempt to normalize thyroid hormone levels. If this process is sustained, a
goiter is established. As a consequence of the increase in thyroid mass and functional activity, a
normal rate of hormone secretion is restored, and the patient is goitrous but euthyroid. Thissequence is evident in some patients with iodine deficiency and in others who develop goiter in
response to specific agents. For example, lithium administration can cause goiter with or without
7/16/2019 Pathology Lab v Diffuse and Multinodular Goiter.
http://slidepdf.com/reader/full/pathology-lab-v-diffuse-and-multinodular-goiter 9/18
hypothyroidism. Goiter (if early) regresses when iodine is administered (if iodine deficiency is
the cause), when lithium or another offending agent is withdrawn, or if suppressive doses of
exogenous thyroid hormone are administered.In most patients with diffuse nontoxic goiter, however, no extrinsic goitrogenic factor can be
identified. As a consequence, the cause may be some intrinsic, probably inborn, abnormality in
thyroid hormone synthesis akin to those that produce goitrous hypothyroidism.This concept of the pathogenesis of nontoxic goiter is inconsistent with the fact that the serumTSH concentration is normal in most patients with nontoxic goiter. This can be explained with
the fact that goitrogenic stimulus has been present in the past but may no longer be detectable at
the time of study, so the residual normal TSH concentration can maintain but not initiate thegoiter. A second possibility is that the increase in serum TSH concentration is significant but too
small to be detected by the immunoassay methods now available.
2. Pathogenesis of multinodular goiter.
(A) Why a long-standing nontoxic goiter becomes nodular? The concept of areas of hyperplasiacoupled with areas of involution. In the pathogenesis of simple and multinodular goiters, it is
assumed that there is initially diffuse hyperplasia which becomes nodular with increasing size,
fibrosis, and distortion of the vascular supply of the thyroid gland. But we don’t know why along-standing nontoxic goiter becomes nodular and develops anatomic and functional
heterogeneity and functional autonomy. These characteristics have been assumed to result from
either prolonged hyperstimulation by TSH or repeated cycles of hyperstimulation and involution.
Hyperstimulation or cycles of hyperstimulation and involution could lead to the emergence of areas of hyperplasia, possibly associated with functional autonomy, coupled with areas of
involution (exhaustion atrophy), the whole made more heterogeneous by localized hemorrhage,
fibrosis, and sometimes calcification.(B) Microheterogeneity of structure and function within the goitrous thyroid gland. Another
pathogenetic concept is the microheterogeneity of structure and function within the goitrous
thyroid gland. Heterogeneity may result from clonal differences among the cells that give rise to
thyroid follicles, some being more and some less responsive to external stimulation by TSH andsome being autonomous at the outset. This concept implies that the anatomic and functional
heterogeneity within the thyroid at the outset of the disease is exaggerated by prolonged
stimulation.(C) Polyclonality. Studies involving X-chromosome inactivation analysis have revealed that both
monoclonal and polyclonal nodules coexist within the same gland. Polyclonality implies
multicellular origin due to the proliferation of a group of cells, whereas a monoclonal tumor isthought to be formed by an expansion of a single cell. In multinodular glands, one or more than
one nodule could be monoclonal, the remainder of nodules being polyclonal.
(D) The biologic continuum between hyperplastic nodules and follicular adenomas. Hyperplastic
nodules can evolve into follicular adenomas. There is a biologic continuum between hyperplasticnodules and follicular adenomas. Monoclonal adenomas within hyperplastic thyroid glands may
reflect a stage in progression along the hyperplasia-neoplasia spectrum; accumulation of multiple
somatic mutations may subsequently confer a selective growth advantage to this single cell.
(E) Autonomous hyperfunction leads to thyrotoxicosis. Ultimately, autonomous hyperfunctionmay be sufficient to produce thyrotoxicosis, or thyrotoxicosis may supervene when the patient is
exposed to an iodine load. For this reason, patients with nontoxic multinodular goiter should not
be given medications that contain iodine and should be observed after radiologic procedures thatinvolve administration of iodinated contrast media

7/16/2019 Pathology Lab v Diffuse and Multinodular Goiter.
http://slidepdf.com/reader/full/pathology-lab-v-diffuse-and-multinodular-goiter 10/18
DEFINITION.These familial goiters develop because of an inherited defect in the metabolism of thyroid
hormone. There are several major biodefects which lead to decreased thyroid hormone synthesis.
The resultant alterations in thyroid gland homeostasis, disturbance of the feedback system, andchronic TSH stimulation lead to enlarged thyroid glands or goiters. The defect is usually
transmitted as an autosomal recessive trait and is a cause of cretinism and hypothyroidism. The
goiter is usually not present at birth but appears later in life.
EPIDEMIOLOGY.
Dyshormonogenetic goiters are rare, with a prevalence of 1 in 30,000 to 50,000 live births in
North America and Europe. It is the second most frequent cause of permanent congenital
hypothyroidism after thyroid dysgenesis (i.e. thyroid aplasia and hypoplasia).
ETIOLOGY.
The following is a short list of possible inherited anomalies: (a) TSH receptor abnormalitiesassociated with lack of responsiveness to TSH, (b) impaired ability to uptake iodide, (c)
organification defect, i.e. inability to add iodine to thyroglobulin which is a critical step in
generating thyroid hormone, (d) Pendred syndrome which is a familial organification defectassociated with congenital deafness, (e) thyroglobulin defect which is inability to form or
degrade thyroglobulin, and (f) deiodinase defect which leads to impairment in the activation of
thyroid hormones.
CLINICAL FINDINGS.
The clinical presentation depends on the severity of the inborn error. A severe defect will lead toneonatal or congenital hypothyroidism, goiter, mental retardation, and growth abnormalities(cretinism). Milder defects will present later in life (adolescence or young adulthood) as goiter
and minimal (if any) thyroid dysfunction. Laboratory evaluation for inborn errors of thyroid
metabolism is complex and extensive.
7/16/2019 Pathology Lab v Diffuse and Multinodular Goiter.
http://slidepdf.com/reader/full/pathology-lab-v-diffuse-and-multinodular-goiter 11/18
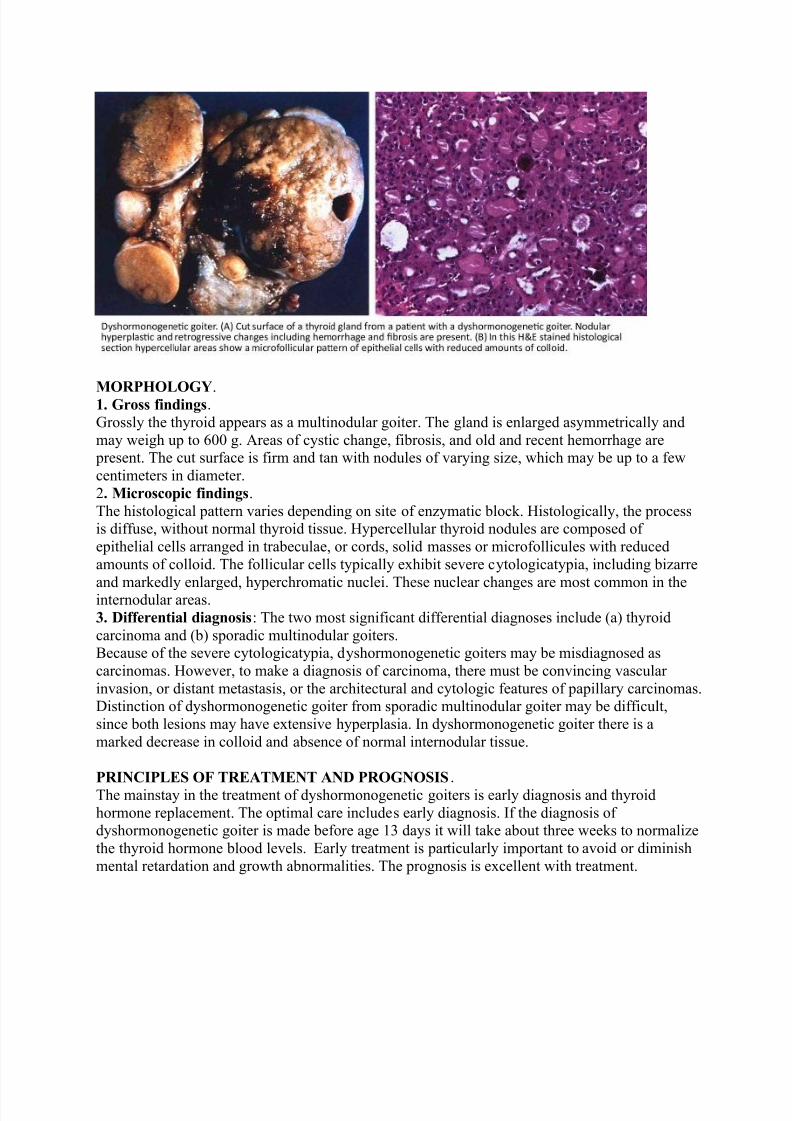
MORPHOLOGY.1. Gross findings.
Grossly the thyroid appears as a multinodular goiter. The gland is enlarged asymmetrically and
may weigh up to 600 g. Areas of cystic change, fibrosis, and old and recent hemorrhage are present. The cut surface is firm and tan with nodules of varying size, which may be up to a few
centimeters in diameter.
2. Microscopic findings.
The histological pattern varies depending on site of enzymatic block. Histologically, the processis diffuse, without normal thyroid tissue. Hypercellular thyroid nodules are composed of
epithelial cells arranged in trabeculae, or cords, solid masses or microfollicules with reduced
amounts of colloid. The follicular cells typically exhibit severe cytologicatypia, including bizarre
and markedly enlarged, hyperchromatic nuclei. These nuclear changes are most common in theinternodular areas.
3. Differential diagnosis: The two most significant differential diagnoses include (a) thyroid
carcinoma and (b) sporadic multinodular goiters.Because of the severe cytologicatypia, dyshormonogenetic goiters may be misdiagnosed as
carcinomas. However, to make a diagnosis of carcinoma, there must be convincing vascular
invasion, or distant metastasis, or the architectural and cytologic features of papillary carcinomas. Distinction of dyshormonogenetic goiter from sporadic multinodular goiter may be difficult,
since both lesions may have extensive hyperplasia. In dyshormonogenetic goiter there is a
marked decrease in colloid and absence of normal internodular tissue. PRINCIPLES OF TREATMENT AND PROGNOSIS.
The mainstay in the treatment of dyshormonogenetic goiters is early diagnosis and thyroid
hormone replacement. The optimal care includes early diagnosis. If the diagnosis of dyshormonogenetic goiter is made before age 13 days it will take about three weeks to normalize
the thyroid hormone blood levels. Early treatment is particularly important to avoid or diminish
mental retardation and growth abnormalities. The prognosis is excellent with treatment.
7/16/2019 Pathology Lab v Diffuse and Multinodular Goiter.
http://slidepdf.com/reader/full/pathology-lab-v-diffuse-and-multinodular-goiter 12/18
DEFINITION.This is a condition in which hyperthyroidism arises in a multinodular goiter, usually of
longstanding duration. One or several nodules in a multinodular goiter develop autonomous
function. Toxic multinodular goiter represents a spectrum of disease ranging from a singlehyperfunctioning nodule (toxic adenoma) within a multinodular thyroid to a gland with multiple
areas of hyperfunction. Autonomous hyperactivity is conferred by somatic mutations of the TSH
receptor in some nodules of multinodular goiters. Autonomously functioning nodules may
become toxic., especially when nodules are larger than 2.5 cm in diameter. Signs and symptomsof toxic nodular goiter are similar to those of other types of hyperthyroidism.
EPIDEMIOLOGY. Toxic multinodular goiter accounts for approximately 15-30% of cases of hyperthyroidism in the
United States, second only to Graves disease. Most patients with toxic nodular goiter are older than 50 years. Toxic multinodular goiter occurs 3 to 4 times more commonly in women than in
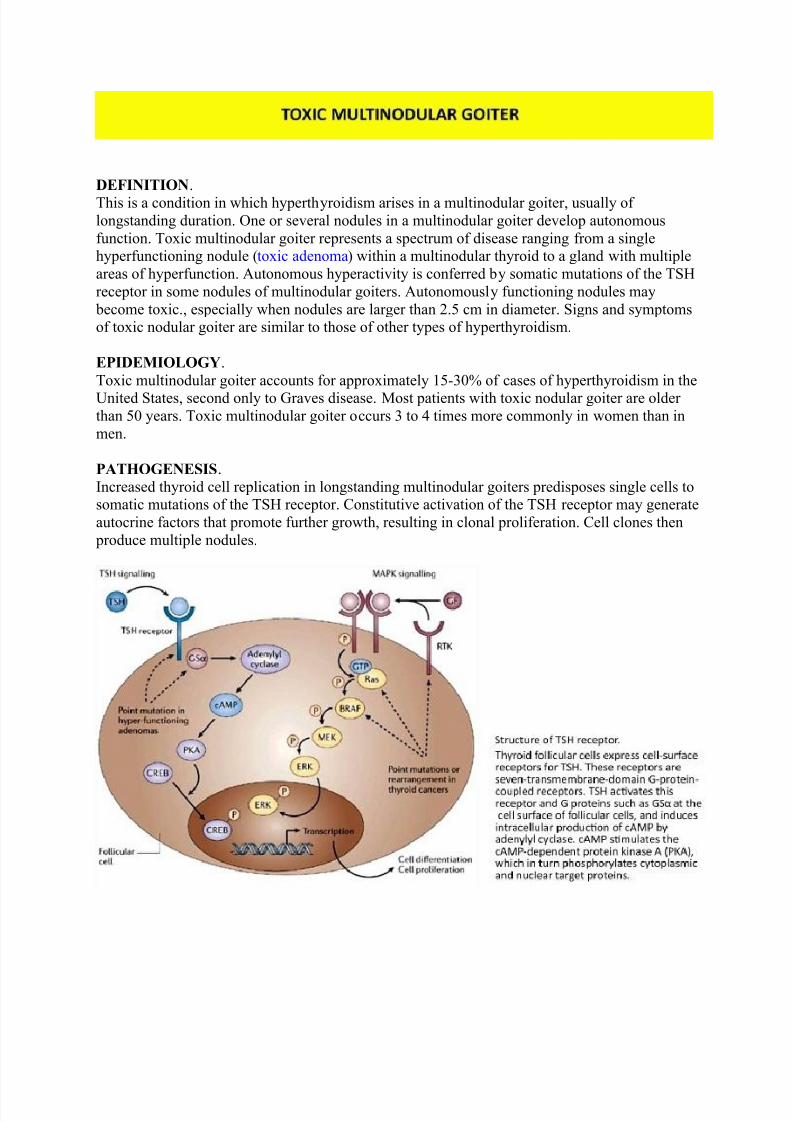
men. PATHOGENESIS. Increased thyroid cell replication in longstanding multinodular goiters predisposes single cells tosomatic mutations of the TSH receptor. Constitutive activation of the TSH receptor may generate
autocrine factors that promote further growth, resulting in clonal proliferation. Cell clones then
produce multiple nodules.
7/16/2019 Pathology Lab v Diffuse and Multinodular Goiter.
http://slidepdf.com/reader/full/pathology-lab-v-diffuse-and-multinodular-goiter 13/18
The TSH receptor is a member of the G protein-coupled receptor superfamily of membrane
proteins and is coupled to the GS alpha protein. Somatic mutations of the TSH receptors and GS
alpha protein confer constitutive activation to the cyclic adenosine monophosphate (cAMP)cascade of the inositol phosphate pathways. These mutations may be responsible for functional
autonomy of the thyroid in 20-80% of cases.
These mutations are found in autonomously functioning solitary thyroid nodules within amultinodular gland. Nonfunctioning thyroid nodules within the same gland lack these mutations.The reported frequency of these mutations varies widely, ranging from 10-80%.
CLINICAL PRESENTATION. Most patients with toxic multinodular goiter present with symptoms typical of hyperthyroidism,
including heat intolerance, atrial fibrillation or tachycardia, tremor, weight loss, hunger, and
frequent bowel movements. Some patients are asymptomatic or have minimal symptoms and are
incidentally found to have hyperthyroidism during routine screening. The most commonlaboratory finding is a suppressed TSH with normal free thyroxine (T4) levels.
Signs found on physical examination include tachycardia, hyperkinesis, moist, smooth skin,
tremor, proximal muscle weakness and brisk deep tendon reflexes.
LABORATORY STUDIES.
Thyroid function tests.
Evidence of hyperthyroidism must be present in order to consider a diagnosis of toxic nodular
goiter. TSH assays are generally the best initial screening tool for hyperthyroidism. Patients withtoxic multinodular goiter will have suppressed TSH levels.
The overproduction of thyroid hormone in toxic multinodular goiter is usually less than in
Graves disease. The serum T3 and T4 concentrations may be only slightly increased while
suppressed TSH may be the only early manifestation of this condition. Free T4 levels may beelevated or within the reference range. Note that even when the total T3 and T4 levels are within
the reference range they are higher than the normal range for a particular individual.
IMAGING.
1. Nuclear scintigraphy.
Nuclear scans should be performed on patients with biochemical hyperthyroidism. Nuclear medicine scans can be performed with radioactive iodine (
123I) or with technetium-99m (
99m Tc).
In patients with toxic nodular goiter, the scan results usually reveal patchy uptake, with areas of
increased uptake (hot nodules) and decreased uptake (cold nodules).
2. Ultrasonography.Ultrasonography is able delineate discrete nodules that are not palpable during thyroid
examination. Ultrasonography is helpful when correlated with nuclear scans to determine the
functionality of nodules. Cold nodules should be considered for fine-needle aspiration biopsy
prior to definitive treatment of a toxic multinodular goiter.
7/16/2019 Pathology Lab v Diffuse and Multinodular Goiter.
http://slidepdf.com/reader/full/pathology-lab-v-diffuse-and-multinodular-goiter 14/18
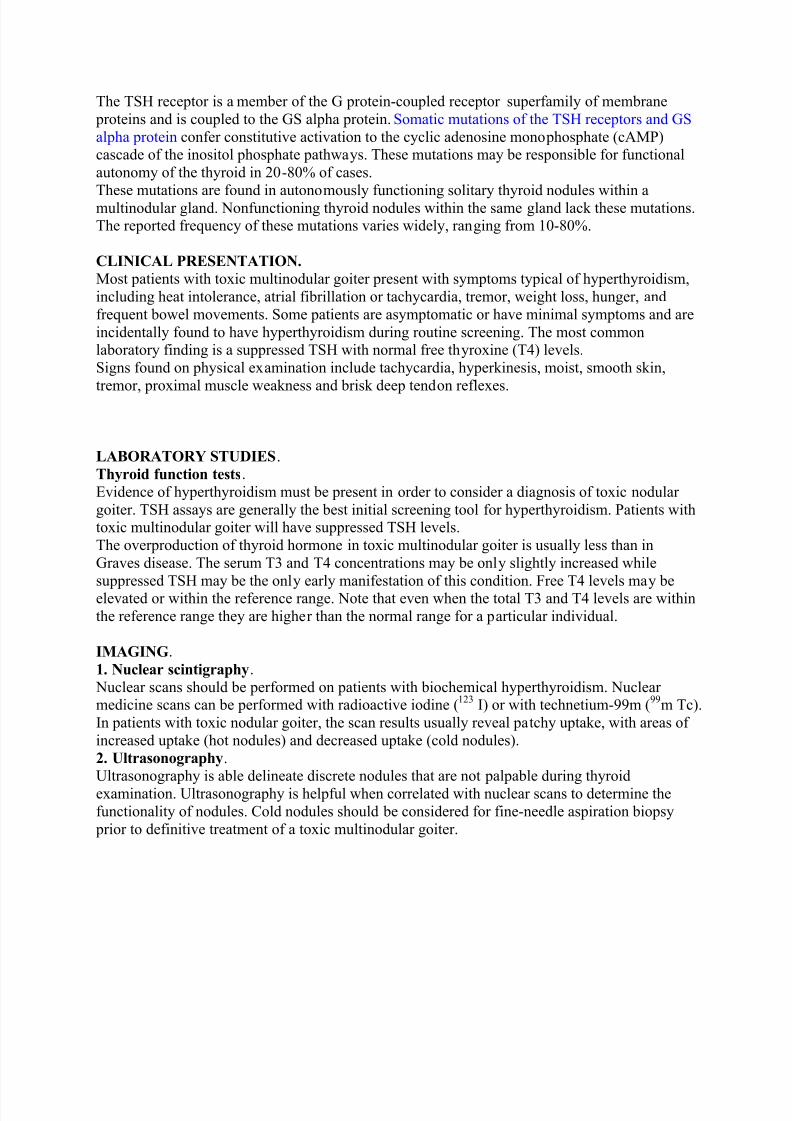
MORPHOLOGY.
The gross and histologic appearance of a toxic multinodular goiter and a nontoxic multinodular goiter overlap. Distinguishing these two entities without clinical correlation and imaging studies
may be difficult.
PRICIPLES OF TREATMENT AND PROGNOSIS.
Patients with toxic multinodular goiter who have autonomously functioning nodules should be
treated definitely with radioactive iodine or surgery. The treatment of choice is radioactive iodine.
Patients with obstructive syndromes are usually treated with surgery, especially when there isdanger of further obstruction from the temporary thyroid enlargement that radioactive iodine
treatment sometimes produces.
DEFINITION. Goiter is conveniently referred to as endemic when it occurs in more than 10% of the population
in a defined area with iodine-poor soil. It is the chief consequence of iodine deficiency, resulting
from either low iodine intake.
AREAS OF IODINE DEFICIENCY.
1. Worldwide.
Worldwide, the soil in large geographic areas is deficient in iodine. About 29% of the world’s population, living in approximately 130 countries, is estimated to live in areas of deficiency
Historically, endemic goiters have developed in geographic areas such as the mountainous
regions of South America (Andes), Europe (Alps) and Asia (Himalayas). The use of the term“iodine deficiency disorder ” emphasizes the results of iodine deficiency on mental and physical

7/16/2019 Pathology Lab v Diffuse and Multinodular Goiter.
http://slidepdf.com/reader/full/pathology-lab-v-diffuse-and-multinodular-goiter 15/18
development. The incidence of endemic goiter and cretinism decreases markedly when iodine is
introduced into the diet as a supplement.
2. United States. Normal dietary iodine intake is 100-150 microgram/day. In the United States, iodine has been
voluntarily supplemented in table salt (70 microgram/g). In the early 1900s, the Great Lakes,
Appalachian, and northwestern regions of the United States were endemic regions for iodinedeficiency disorder , but since the iodization of salt and other foods in the 1920s, dietary iodinelevels generally have been adequate.
CLINCAL MANIFESTATIONS.
Affected patients from geographic regions where iodine deficiency disorders are endemic
manifest with goiter, symptoms and signs of hypothyroidism. Cretinism and mental retardationas the most extreme manifestation of iodine deficiency disorders are frequent in the endemic
areas.
MORPHOLOGY.
The macroscopic and microscopic findings in endemic goiters are similar to those
of multinodular goiters, with multiple nodules in a background of degenerative changesincluding fibrosis, old and recent hemorrhage, and dystrophic calcification. The histologic
picture is variable-sized follicles, with thin follicular cells in dilated colloid follicles admixed
with smaller follicles lined by columnar epithelium.
PRINCIPLES OF TREATEMENT.
Long-term dietary iodine replacement at levels recommended by the Institute of Medicine and
WHO may decrease the size of iodine-deficient goiters in very young children and pregnant
women and is indicated for all patients with iodine deficiency. Generally, long-standing goitersassociated with iodine deficiency disorder respond with only small amounts of shrinkage after
iodine supplementation, and patients are at risk for developing hyperthyroidism. Patients do not
routinely require specific therapy unless the goiter is large enough to cause compressivesymptoms.
7/16/2019 Pathology Lab v Diffuse and Multinodular Goiter.
http://slidepdf.com/reader/full/pathology-lab-v-diffuse-and-multinodular-goiter 16/18
1.
A 34-year-old woman, gravida 3, para 2,presented with polyhydramnios andpremature labor during the 32nd week
of gestation. Her thyroid function andthyroid antibodies were normal, her history revealed no exposure togoitrogens. Fetal ultrasounddemonstrated a bilobed symmetricanterior neck mass measuring 4.0 x 8.0cm. It caused hyperextension of thehead and polyhydramnios, makingspontaneous delivery impossible. Fetalblood sampling revealed severehypothyroidism with a serum total
thyroxine (T4) of 2.4 mcg/dL (normal: 3-16) and a thyroid-stimulating hormone(TSH) of 200 micro-U/mL (normal: 3-14)so that 250 micro-g L-thyroxine wereinjected intraamniotically.Hypothyroidism had improved at 36weeks with a total thyroxineof 4.3mcg/dL and a TSH of 80 micro-U/mL. Atthis time 200 mg L-thyroxine wereinjected into the umbilical vein. Theprocedure was repeated at 37 weekswith another 100 micro-g L-thyroxine.Thyroid function had improved further.Total thyroxine was 6.3 mcg/dL, andTSH was 36.6 micro-U/mL. The goiter was reduced to 4.2 x 5.1 cm so that amale infant with a small goiter was bornby uncomplicated vaginal delivery at 39weeks and 6 days. Molecular geneticstudies revealed that the infant had ahomozygous mutation of the thyroidperoxidase gene. Thyroid peroxidasegene abnormalities are known to giverise to organification defects, i.e. inabilityto add iodine to thyroglobulin which is acritical step in generating thyroidhormone. This infant’s goiter can mostlikely classified as:
Dyshormonogenetic
Sporadic
Endemic
Toxic
2.
All of the following clinical findings arecorrect concerning simple non-toxicgoiter except:
Neck discomfort
Venous engorgement
Dysphagia
Male predominance
Peak incidence during adolescenceand early adult years
3.
A 22 –year old woman was referred byher family physician to the Departmentof Endocrinology because of a largethyroid, but no clinical or biochemicalsigns of thyroid dysfunction. The patienthad no major focal, nor major cosmeticproblems. The thyroid enlargementappeared at her first pregnancy. At thetime of referral TSH was 2.23 micro-U/L(normal: 2 –10) and thus TSH was notsuppressed, total thyroxine (T4) was 8mcg/dL (normal: 5-12) and total tri-iodothyronine (T3) was 163 ng/dL(normal: 70 –205). A nuclear thyroidscintigraphy showed a diffuse,homogenous and equal uptake in both
lobes. Both the right and the left lobewere considerably enlarged, measuring6 x 10 cm. No hypo-functioning ‘cold’nodules were identified and thus no fineneedle aspiration was performed. Whichof the following is the most likelydiagnosis?
7/16/2019 Pathology Lab v Diffuse and Multinodular Goiter.
http://slidepdf.com/reader/full/pathology-lab-v-diffuse-and-multinodular-goiter 17/18
Papillary carcinoma of thyroid
Normal thyroid
Hashimoto thyroiditis
Diffuse non-toxic goiter
Graves disease
4.
An 86-year-old man presents with largegoiter on April 2009. He reported weightloss of 10 pounds over the last year,fatigue, and an irregular heart rate over the last 2 years. Physical examinationshowed a bilaterally enlarged 100 g,asymmetric and nodular thyroid gland. Areview of his records from the past 15years shows that on January 1995 hehad a diffuse goiter that was only slightlyenlarged, at 40 g. He denies a history of head and neck radiation. His freethyroxine (T4) index has beenincreasing slowly, and his thyroid-stimulating hormone (TSH) level hasfallen progressively from 2.5 U/mL 15years ago to his recent value of 0.4U/mL (reference range is 0.5-5.5 U/mL).Which of the following is the most likelydiagnosis?
Nontoxic multinodular goiter
Papillary carcinoma of the thyroid
Graves disease
Toxic multinodular goiter
Diffuse nontoxic goiter
5.
All of the following elements of thetraditional theory about thepathogenesis of simple non-toxic goiter are correct except:
Hyperplastic thyroid produceshormone in excess leading tosymptoms of thyrotoxicosis.
Thyroid hyperplasia restoreshormone secretion to the normal
level.
Insufficient iodine intake is at theroot of the problem.
Insufficient iodine intake bringsabout increased production of thyroid stimulating hormone (TSH).
Increased TSH induces hyperplasiaand enlargement of the thyroidgland with increase in functional
activity. 6.
Endemic goiter is an enlargement of thethyroid gland that occurs in more than10% of a population of a geographicregion secondary to iodine deficiency.
False
True
7.
The term goiter refers to: Any enlargement of the thyroidassociated with inflammatorydiseases
Any enlargement of the thyroidregardless of etiology
Enlargement of the thyroid
secondary to Graves disease
Any enlargement of the thyroidassociated with neoplasticdiseases
Enlargement of the thyroidsecondary to the ingestion of goitrogens
7/16/2019 Pathology Lab v Diffuse and Multinodular Goiter.
http://slidepdf.com/reader/full/pathology-lab-v-diffuse-and-multinodular-goiter 18/18
8.
A 55-year-old woman who reportsshortness of breath on exertion isreferred to Policlinico Di Monza (Torino,
Italy) for evaluation of a neck mass. Shewas born and raised in northern Italy, anarea of endemic goiter. She has been ingood health until he noted recentshortness of breath, stridor, and coughon climbing stairs; she reports difficultyswallowing solid food because it sticksin his mid neck during a swallow. Onphysical examination, she has nocyanosis, no cough, and no wheezing.Her respiratory rate is 15 breaths per
minute. The trachea is deviated to theleft, with an enlarged thyroid about 6times normal size. The thyroid is firm,with an irregular surface and withevidence of nodules. Upon raising her
arms, her face turns red and her external jugular veins fill with blood.Laboratory studies show a referencerange thyroid-stimulating hormone(TSH) and free thyroxine (T4) level.
Which of the following is the most likelydiagnosis? Papillary carcinoma of the thyroid
Thyroid adenoma
Diffuse nontoxic goiter
Toxic multinodular goiter
Non-toxic multinodular goiter


















![Riedel’s thyroiditis presenting as large retropharyngeal ... · in literature are multinodular goiters[2,8,9] with one large study failing to mention the pathology of the goiter.[3]](https://img.dokumen.tips/doc/110x75/5b6a1e7a7f8b9af6098bb781/riedels-thyroiditis-presenting-as-large-retropharyngeal-in-literature.jpg)










