Embed Size (px)
Citation preview

CentralBringing Excellence in Open Access
JSM Foot and Ankle
Cite this article: Sagar R, Challa S (2017) Pathology and Diagnosis of Nocardiosis. JSM Foot Ankle 2(5): 1040.
*Corresponding authorSundaram Challa, Department of Pathology, Nizam’s Institute of Medical Sciences Hyderabad, Telangana, India, Tel: 09849496333; Email:
Submitted: 09 November 2017
Accepted: 28 November 2017
Published: 30 November 2017
ISSN: 2475-9112
Copyright© 2017 Challa et al.
OPEN ACCESS
Keywords•Nocardiosis•Risk factors•Pathogenesis•Pathology•Diagnosis
Review Article
Pathology and Diagnosis of NocardiosisRadha Sagar1 and Sundaram Challa2*1Department of Pathology, Kaloji Narayana Rao University of Health Sciences, India2Department of Pathology, Nizam’s Institute of Medical Sciences, India
Abstract
Nocardia is a gram positive aerobic filamentous bacteria which is weakly acid fast. It is an opportunistic infection. But its incidence in immunocompetent people is ion the rise. It is ubiquitous and the mode of entry is either by direct implantation through skin or by inhalation. The risk factors include immunosuppression in organ transplant recipients, rheumatic diseases, human immunodeficiency virus infection. Infection can be localized to one organ or can be disseminated. Lung is the commonest organ involved, followed by brain and skin. The pathogenesis is due to deficiency of cell mediated immunity. Identification of the organism is the main stay for diagnosis. The size of the granule, suppurative inflammation, Splendore-Hopple phenomenon, weak acid fastness and thin branching filaments on silver stain help in making the diagnosis on histopathology. The organisms can be readily grown in aerobic media. Polymerase chain reaction and 16SrDNA sequencing are the molecular methods for demonstration of Nocardia. High index of clinical suspicion and rapid diagnosis are the key factors for better patient outcome. This review focuses on the pathogenesis, pathology and diagnosis.
ABBREVIATIONSHSCT: Hematopoietic Stem Cell Transplantation; CMV:
Cytomegalovirus; HIV: Human Immunodeficiency Virus; CNS: Central Nervous System; BAL: Bronchoalveolar Lavage; CSF: Cerebrospinal Fluid; FNAC: Fine Needle Aspiration Cytology; H&E: Hematoxylin and Eosin; ZN: Zeihl-Neelsen; PCR: Polymerase Chain Reaction
INTRODUCTION Nocardia species are gram positive bacteria that belong to
the genus of Nocardia, family of Nocardiaceae, and suborder of “aerobic actinomycetes”. Nocardia species are ubiquitous in the environment and are present in soil, decomposing vegetable matter, organic substances and water. More than 50 species of Nocardia are identified but most of the human infections are caused by Nocardia asteroides complex, which are a group of bacteria with a heterozygous pattern of antimicrobial drug susceptibilities [1]. Nocardia species have wide geographic distribution depending on the prevailing environmental conditions. These infections may be localized or disseminated and are more common and generally more serious in severely immunocompromised and debilitated patients. Nocardiaspecies are the most common cause of actinomycotic mycetoma in India [2,3].
PATHOGENESISRisk factors
Nocardia is usually an opportunistic pathogen but can cause disease even in healthy hosts. Persons with depressed immunity
are at high risk of developing the infection. The risk factors include individuals on treatment for lymphoma and other malignancies, recipients of solid organ transplants (especially lung followed by heart, small bowel, kidney and liver) and allogenic hematopoietic stem cell transplants (HSCT), patients receiving long term treatment with steroids or other immunosuppressive agents, alcoholism and retroviral infection [4]. In organ transplant patients, the frequency of nocardial infection is reported to be 0.6%-3% and the cause is immunosuppression. Use of Azathioprine and prednisone has a higher risk than cyclosporine and prednisone [5]. In a case control study of 5126 cases of solid organ transplantation, Nocardia infection was highest in the lungs, followed by heart, small intestine, kidney and liver transplants [4]. In autoimmune and rheumatic disorders, long term and high dose use of corticosteroids and concomitant use of immunosuppressant’s along with pre-existing pulmonary diseases and diabetes mellitus are reported to be the most common risk factors [6].
Associated conditions
The infection can also occur as a co-infection with tuberculosis or cytomegalovirus (CMV) infection and in patients with human immunodeficiency virus (HIV) infection. Association with co-morbidities like diabetes mellitus, chronic alcoholism, pulmonary obstructive disease, structural lung abnormalities, pneumoconiosis and bronchiectasis are reported [7].
Route of entry
The infection usually occurs as an opportunistic infection in immunosupressed individuals, especially in those with

CentralBringing Excellence in Open Access
Challa et al. (2017)Email:
JSM Foot Ankle 2(5): 1040 (2017) 2/5
deficiency of cell mediated immune response. However, it can also occur in immunocompetent individuals, usually by traumatic implantation or contamination with soil.
The infection is acquired primarily by inhalation of the bacillus from the environment, from where it spreads hematogenously to other organs and tissues [8,9]. The infection is also acquired by inoculation after trauma or following surgery. The most common site of involvement is lung, followed by central nervous system (CNS), skin and soft tissues.
Disseminated nocardiosis occurs by hematogeneousa spread and is defined as infection in more than one body location. Disseminated nocardiosis can invade any organ but commonly involves lungs, CNS, eyes, kidneys, skin, subcutaneous tissue and bone. Heart valves, liver, spleen, adrenal glands, thyroid gland, and other organs are rarely infected [7,10]. No person to person transmission is reported.
Factors related to host-pathogen interaction: The host-pathogen interactions were studied extensively both in-vitro and in-vivo. Both cell mediated and humoral mediated immunity were implicated in the pathogenesis; however, cell mediated immunity is crucial in limiting the infection. The entry of the organism activates innate immunity and neutrophils provide the first line of defense. Local macrophages get activated and enter the site of inflammation. Both neutrophils and macrophages engulf the organisms by complement mediated phagocytosis and try to limit the infection. Neutrophils predominate in the early lesions of nocardiosis. However, degranulation and adherence of neutrophils to the organism, and engulfment by macrophages fail to kill the organisms [11]. These processes limit the spread of infection until a specific cell-mediated response can occur. A population of immune primed T cells enhances phagocytosis, stimulates cellular response, and may induce direct cytotoxicity to the bacteria [12,13].The role of humoral mediated immunity is limited; antibodies have been shown to enhance phagocytosis and the microbicidal activity of activated macrophages in experimental models [14].
Immune T cells effectively clear Nocardia organisms from the lung and prevent extra-pulmonary dissemination. Corticosteroids impair the lymphocyte function. Diseases with impairment of cell mediated immunity facilitate disease progression.
Nocardia species possess multiple mechanisms to overcome the immune response of the host. Certain species such as N. brasiliensis, are more commonly found in the immunocompetent individuals whereas species such as Nocardia farcinica, Nocardia nova, and Nocardia cyriacigeorgica mostly affect immunosuppressed individuals [3]. The virulence of the organism dictates the pathogen-phagocyte interaction and is attributed to the complex cell wall glycolipids. These interactions inhibit phagosome - lysosome fusion and decrease lysosomal enzyme activity in macrophages, neutralize phagosomal acidification, and resist the oxidative killing mechanisms of phagocytes. The virulence of the strain, the growth phase of nocardia, adaptation of the organism to the microenvironment facilitates the organisms to survive within macrophages as facultative intracellular pathogens and evade host defenses [3, 13, 15]. In the chronic disease, neutrophils and macrophages fail to generate a burst of
oxidative metabolism during phagocytosis, thus impairing the intracellular killing [13].
Nocardiosis of Lung
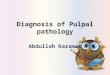
Pulmonary nocardiosis is the most common manifestation of nocardial infection. Involvement of lung occurs in 70% of all cases [16]. Nocardia asteroids are the most common organism though nine species have been associated with human disease [17]. Eighty eight percent of patients have one of the predisposing factors and 10-20% of patients have no preexisting illness or immunosuppression [18]. Patil et al., reported pulmonary nocardiosis in immunocompetent patients [19]. Pulmonary nocardiosis can occasionally occur through gastrointestinal tract especially through appendix rarely pulmonary infection follows dental procedures or peri odontal infection. Symptoms include cough, fever, dyspnea, chest pain, weight loss and hemoptysis. It can present as an acute, sub-acute or chronic disease with remissions and exacerbations. There is usually a delay in diagnosis due to lack of clinical suspicion and nonspecific features at presentation. Isolated pleural involvement is rare and presents with effusion and empyema [15, 19, 20]. Lung involvement can be a part of disseminated nocardiosis. Radiologically, pulmonary nocardiosis presents mainly as multiple pulmonary nodules (Figure 1A), consolidations, and cavity bilaterally in both immunocompromised and immunocompetent patients [21]. Other findings include bronchiectasis, pleural thickening, ground glass opacity, mass-like consolidation, intrathoracic lymphadenopathy, pleural effusion, reticular infiltration and pericardial effusion [21]. CT scan is more sensitive and shows lesions earlier than the plain chest radiograph.
Nocardiosis of CNS
The most common extra pulmonary site for Nocardiosis is CNS [13]. It is uncommon but clinically important disease as it is associated with high mortality. It accounts for 15-50% of nocardiosis and 2% of brain abscesses [8,22,23]. It can affect the brain or spinal cord. It occurs along with pulmonary disease or as isolated disease. It usually occurs in immunosuppressed individuals. The presentation is usually with headache, nausea, vomiting, focal neurological deficit and seizures or as cord compression. Radiological features are nonspecific and may involve brain or cord as parenchymal lesions. Multifocal ring-enhancing lesions are the dominant features of brain [8,9]. The most common pathology is single or multiple brain abscess and
Figure 1a Computed tomography chest showing bilateral multiple nodules in lung parenchyma.

CentralBringing Excellence in Open Access
Challa et al. (2017)Email:
JSM Foot Ankle 2(5): 1040 (2017) 3/5
the other pathologies include meningitis or granuloma [8,22,24-27].
Nocardiosis of skin and subcutaneous tissues: Cutaneous nocardiosis usually occurs in immunocompetent individuals. N. brasiliensis is the most common species isolated from the majority (approximately 80%) of cases, though the disease can be caused by any species [28]. The infection is most common in individuals from rural areas in developing countries, attributed to minor localized trauma due to walking barefoot. Foot is the most common site of infection, followed by hand, neck and face [24,29]. The disease may be subdivided into four clinical types: mycetoma, lymphocutaneous infection, superficial skin infection and secondary cutaneous involvement with disseminated disease [30]. Mycetoma is a chronic, localized, slowly progressive, painless infection with tumefaction, subcutaneous nodules, destructive granulomata, and formation of intermittent fistulas with pus. In lymphocutaneous form, the spread is beyond the cutaneous focus to involve the regional lymphatics and results in regional lymphadenopathy. This form of the disease is referred to as the lymphocutaneous syndrome or the sporotrichoid form of cutaneous nocardiosis [30]. In one-third of cases, the disease may progress to form lymphatic abscesses. Superficial skin infection is characterized by cellulitis with erythema, pain and swelling. There may be ulceration and abscess formation. Cutaneous nocardiosis secondary to disseminated disease occurs in immunocompromised individuals and associated with high mortality [30,31]. Radiological investigations with conventional radiography, ultrasonography and magnetic resonance imaging are required to assess extent of soft tissue involvement and bone involvement, especially in mycetoma.
Disseminated Nocardiosis
It is a life threatening infection, occurring in severely immunocompromised individuals and associated with high mortality. It is an endogenous infection with primary focus usually in lung and rarely from skin. CNS involvement is the most common and serious complication, though any organ may be involved [15,29].
DIAGNOSISNocardiosis is difficult to diagnose clinically, radiologically,
and histopathologically. Routine hematological investigations may reveal leukocytosis with neutrophilia. There will be an increase in inflammatory markers. Radiological features are variable, nonspecific and depend on the site (s) of involvement. In patients with suspected nocardial infection and a compatible clinical picture, a definitive diagnosis usually depends on the demonstration of the organisms in smears or sections examined microscopically together with isolation and identification by microbiologic culture [7]. The specimens for laboratory evaluation include sputum, bronchialoalveolar lavage (BAL) fluid, exudate, cerebrospinal fluid (CSF) or material obtained by fine needle aspiration cytology (FNAC) and biopsy [15,30].
Direct microscopy
It is the most important method for the diagnosis. The material received is spread on glass slide and examined microscopically. Granules or clumps of organisms are crushed between glass
slides and the morphology is observed. Nocardia species are gram-positive and the filaments are thin, long and branch at right angles. The organisms are gram positive and weakly acid fast. Hence, Gram’s stain and modified Kinyoun acid-fast stain are to be done when nocardia infection is suspected clinically. The filaments have a beaded appearance on microscopy [15,30].
Culture studies
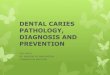
Nocardia species are aerobic and grow on blood agar or saborauds agar. However, growth on blood agar may be slow, and incubation for periods longer than 48 h is usually necessary. As cultures enter the stationary phase, the filaments tend to fragment into coccobacillary forms. The culture shows dry granular wrinkled yellowish white colonies of Nocardia asteroids (Figure 1B). The growth of nocardia in culture should always be correlated with clinical picture as nocardia can colonise in healthy individuals in respiratory tract [15,30].
PATHOLOGYThe biopsy sections stained with hematoxylin and eosin
Figure 1b Culture media showing dry granular wrinkled yellowish white colonies of Nocardia asteroids.
Figure 1c Photomicrograph showing grains with peripheral intense eosinophilic material, Splendore-Hoeppli phenomenon. (Hematoxylin & eosin x 200).

CentralBringing Excellence in Open Access
Challa et al. (2017)Email:
JSM Foot Ankle 2(5): 1040 (2017) 4/5
(H&E), usually show abscess with predominant neutrophilic infiltrate. A few foreign body giant cells, lymph mononuclear cells and rarely a granuloma formation may be seen, especially in mycetoma of cutaneous nocardiosis. The granules of nocardia are white and small, measuring 0.5 to 1µm in diameter. In mycetoma, compact granules are formed, similar to those observed for the anaerobic actinomycetes. Rarely, the grains show peripheral intense eosinophilic material, representing Splendore-Hoeppli phenomenon. H&E shows the tissue reaction and the grains but the filamentous nature of the bacteria is not appreciated. Nocardia microorganisms are filamentous rods that show right-angled branching both in culture and in tissues. The filaments are gram positive and stained with Brown & Brenn (equivalent of gram stain) stain on tissue sections. The filaments are weakly acid fast and are stained with the modified Kinyoun or the Fite-Faraco staining methods. Gomori’s methenamine silver stain also delineates the filaments [15,30] (Figure 1 C-E).
Differential diagnosis
Nocardia species need to be differentiated from actinomycetes and mycobacteria. Actinomycetes are also gram positive but are not acid fast. Actinomycetes grow under anaerobic conditions in culture, whereas Nocardia grow under aerobic conditions. Mycobacteria are acid fast and resist decolorization with 20% sulfuric acid on Zeihl-neelsen (ZN) stain, whereas Nocardia are weakly acid fast with 1% sulfuric acid. The weak acid fastness and beaded appearance on microscopy, differentiate Nocardia from mycobacteria.
Molecular methods
Identification of species of Nocardia is important as epidemiologic subtypes, virulence and antimicrobial susceptibility differ amongst the species. Identification of Nocardia species by polymerase chain reaction (PCR) and 16SrDNA sequencing are very accurate methods of diagnosis [32].
CONCLUSIONWith the increase in the number of patients receiving
immunosuppressive treatment for malignancies and various autoimmune and rheumatological diseases, awareness about Nocardia being a possible pathogen is important. Prompt diagnosis is important for early institution of appropriate antimicrobial therapy and favorable outcome.
REFERENCES1. Wallace RJ, Steele LC, Sumter G, Smith JM. Antimicrobial susceptibility
patterns of Nocardia asteroides. Antimicrob Agents Chemother. 1988; 32: 1776-1779.
2. Chaudhuri BN, Maiti PK, Sil J. Antibiotic sensitivity patterns of actinomycetes isolated from patients of actinomycetoma. Indian J Med Res. 1997; 105: 162-166.
3. Relhan V, Mahajan K, Agarwal P, Garg VK. Mycetoma: An Update. Indian J Dermatol. 2017; 62: 332-340.
4. Peleg AY, Husain S, Qureshi ZA. Risk factors, clinical characteristics, and outcome of Nocardia infection in organ transplant recipients: a matched case-control study. Clin Infect Dis. 2007; 44: 1307-1314.
5. Roberts SA, Franklin JC, Mijch A, Spelman D. Nocardia infection in heart-lung transplant recipients at Alfred Hospital, Melbourne, Australia, 1989-1998. Clin Infect Dis. 2000; 31: 968-972.
6. Yamagata M, Hirose K, Ikeda K, Nakajima H. Clinical Characteristics of Nocardia Infection in Patients with Rheumatic Diseases. Clin Dev Immunol. 2013; 818654.
7. Wilson JW. Nocardiosis: updates and clinical overview. Mayo Clin Proc. 2012; 87: 403-407.
8. Zakaria A, Elwatidy S, Elgamal E. Nocardia brain abscess: severe CNS infection that needs aggressive management; case report. Acta Neurochir (Wien). 2008; 1097-1111.
9. Kranick SM, Zerbe CS. Case report from the NIH Clinical Center: CNS nocardiosis. J Neurovirol. 2013; 19: 505-507.
10. Yu Kurahara, Kazunobu Tachibana, Kazunari Tsuyuguchi, Masanori Akira, Katsuhiro Suzuki Seiji Hayashi. Pulmonary nocardiosis: A clinical analysis of 59 cases. Respiratory investigation. 2014; 52: 160-166.
11. Ekizlerian SM, Brandão Filho SL, Tincani I, Alves LM, Silva CL. Studies on the pathogenesis of actinomycotic mycetoma in animals injected
Figure 1d Acid fast filamentous bacteria with beaded appearance (Modified Kinyoun stain x200).
Figure 1e Thin filamentous, branching bacteria (Gomori’s methenamine silver stain x 200).

CentralBringing Excellence in Open Access
Challa et al. (2017)Email:
JSM Foot Ankle 2(5): 1040 (2017) 5/5
Sagar R, Challa S (2017) Pathology and Diagnosis of Nocardiosis. JSM Foot Ankle 2(5): 1040.
Cite this article
with fractions isolated from Nocardia brasiliensis. Br J Exp Pathol. 1987; 68: 115-123.
12. Deem RL, Doughty FA, Beaman BL. Immunologically specific direct T lymphocyte-mediated killing of Nocardia asteroides. J Immunol. 1983; 130: 2401-2406.
13. Beaman BL, Beaman L. Nocardia species: host-parasite relationships. Clin Microbiol Rev. 1994; 7: 213-264.
14. Davis-Scibienski C, Beaman BL. Interaction of alveolar macrophages with Nocardia asteroides: immunological enhancement of phagocytosis, phagosome-lysosome fusion, and microbicidal activity. Infect Immun. 1980; 30: 578-587.
15. Patil NP, Nadkarni NJ, Sharma NR. Nocardiosis: clinical and pathological aspects. In: Poblet Martinez E, ed. Histopathology: Reviews and Recent Advances. 2012. Infect Immun. 1980; 30: 578-587.
16. Vohra P, Sharma M, Yadav A, Chaudhary U. Nocardiosis: A review of clinic-microbiological features. Int J Life ScBt Pharma Res. 2013; 2: 20-29.
17. Zaatreh M, Alabulkarim W. Images in clinical medicine. Disseminated central nervous system nocardiosis. N Eng. J Med. 2006; 354: 2082.
18. Yang M, Xu M, Wei W, Gao H, Zhang X, Zhao H, et al. Clinical findings of 40 patients with nocardiosis: A retrospective analysis in a tertiary hospital. Exp Ther Med. 2014; 8: 25-30.
19. Patil MCS, Varghese J, Rajagopalan N. A fatal case of pulmonary nocardiosis. BMJ Case Reports. 2012.
20. Gowrinath K, Das S, Ranjitham M, Sekhar U, Thanasekaraan V. Nocardial hydropneumothorax. Indian J Chest Dis Allied Sci. 2004; 46: 51-53.
21. Mehrian P, Esfandiari E, Karimi MA, Memari B. Computed Tomography Features of Pulmonary Nocardiosis in Immunocompromised and Immunocompetent Patients. Pol J Radiol. 2015; 80: 13-17.
22. Chedid MB, Chedid MF, Porto NS, Severo CB, Severo LC. Nocardial infections: report of 22 cases. Rev Inst Med Trop Sao Paulo. 2007; 49: 239-246.
23. Anagnostou T, Arvanitis M, Kourkoumpetis TK, Desalermos A, Carneiro HA, Mylonakis E. Nocardiosis of the central nervous system: experience from a general hospital and review of 84 cases from the literature. Medicine (Baltimore). 2014; 93: 19-32.
24. Lakshmi V, Sundaram C, Meena AK, Murthy JM. Primary cutaneous nocardiosis with epidural abscess caused by Nocardia brasiliensis: a case report. Neurol India. 2002; 50: 90-92.
25. Sundaram C, Lakshmi V. Pathogenesis and pathology of brain abscess. Indian J Pathol Microbiol. 2006; 49: 317-326.
26. Lakshmi V, Umabala P, Anuradha K, Padmaja K, Padmasree C, Rajesh A, et al. Microbiological Spectrum of Brain Abscess at a Tertiary Care Hospital in South India: 24-Year Data and Review. Pathology Res Int. 2011; 583139.
27. Nalini A, Saini J, Mahadevan A. Central nervous system norcardiosis with granulomatous pachymeningitis and osteomyelitis of skull vault. Indian J Pathol Microbiol. 2014; 57: 332-334.
28. Maraki S, Chochlidakis S, Nioti E, Tselentis Y. Primary lymphocutaneous nocardiosis in an immunocompetent patient. Ann. Clin. Microbiol. Antimicrob. 2004; 3: 24-28.
29. McNeil MM, Brown JM. The medically important aerobic actinomycetes: epidemiology and microbiology. Clin Microbiol Rev. 1994; 7: 357-417.
30. Brown-Elliott BA, Brown JM, Conville PS, Wallace RJ. Clinical and Laboratory Features of the Nocardia spp. Based on Current Molecular Taxonomy. Clin Microbiol Rev. 2006; 19: 259-282.
31. Kalb RE, Kaplan MH, Grossman ME. Cutaneous nocardiosis. Case reports and review. J Am Acad Dermatol. 1985; 13: 125-133.
32. Antimicrobe.