Embed Size (px)
Citation preview

doi:10.1016/S0360-3016(03)00120-2
CLINICAL INVESTIGATION Breast
PARTIAL BREAST BRACHYTHERAPY AFTER LUMPECTOMY: LOW-DOSE-RATE AND HIGH-DOSE-RATE EXPERIENCE
DOUGLAS W. ARTHUR, M.D.,* DERRICK KOO, M.D.,* ROBERT D. ZWICKER, PH.D.,†
SHIDONG TONG, PH.D.,* HARRY D. BEAR, M.D., PH.D.,‡ BRIAN J. KAPLAN, M.D.,‡
BRIAN D. KAVANAGH, M.D.,§ LAUREL A. WARWICKE, M.D.,* DIANE HOLDFORD, R.N.,*CYRUS AMIR, PH.D.,¶ KELLIE J. ARCHER, PH.D.,¶ AND RUPERT K. SCHMIDT-ULLRICH, M.D.*
Departments of *Radiation Oncology and¶Biostatistics, and‡Division of Surgical Oncology, Virginia Commonwealth UniversityMedical College of Virginia Campus, Richmond, VA;†Department of Radiation Oncology, University of Kentucky, Lexington,
KY; §Department of Radiation Oncology, University of Colorado Health Science Center, Denver, CO
Purpose: The use of partial breast brachytherapy (PBB) after lumpectomy for selected patients with early-stagebreast cancer reduces the adjuvant radiotherapy treatment time to<1 week. Despite the advantages ofaccelerated treatment, maintaining an acceptable cosmetic outcome is important. In a cohort of patients whoreceived low-dose-rate (LDR) or high-dose-rate (HDR) PBB after lumpectomy, the clinical characteristics andtreatment parameters were analyzed to identify predictors for an unfavorable cosmetic outcome.Methods and Materials: Early-stage breast cancer patients with clear resection margins and 0–3 positive lymphnodes were eligible for PBB. Uniform guidelines for target definition and brachytherapy catheter placement wereapplied. The HDR PBB dose was 34 Gy in 10 fractions within 5 days, and the LDR dose was 45 Gy given at arate of 50 cGy/h. The end points included incidence of radiation recall reaction, telangiectasias, and cosmetic-altering fibrosis.Results: Between 1995 and 2000, 44 patients with early-stage breast cancer received PBB without adjuvantexternal beam radiotherapy after lumpectomy (31 HDR PBB, 13 LDR PBB). After a median follow-up of 42months (range 18–86), all patients remained locally controlled. The overall rate of good/excellent cosmeticoutcome was 79.6% overall and 90% with HDR PBB. Radiation recall reactions occurred in 43% of patients (6of 14) who received adriamycin. LDR PBB and adriamycin were significant predictors for late unfavorablecosmetic changes in univariate analysis (p � 0.003 andp � 0.005, respectively).Conclusion: Although a high rate of local control and good/excellent cosmetic outcome is provided with HDRPBB, the risk of unfavorable cosmetic changes when treated with both LDR PBB and adriamycin is noteworthy.This suggests that HDR PBB is preferred in patients for whom adriamycin is indicated. © 2003 Elsevier Inc.
Brachytherapy, Breast cancer, Breast-conserving therapy, Accelerated partial breast irradiation.
INTRODUCTION
Breast-conserving treatment (BCT), characteristically con-sisting of whole breast radiotherapy (RT) after lumpectomy,is known to yield equivalent local control rates to that ofmastectomy and has been accepted as an appropriate localtreatment option for selected early-stage breast cancer pa-tients (1–6). Despite this equivalence, many patients whoare appropriate for BCT do not pursue this approach as aresult of personal choice, physician preference, or the in-ability to complete 6 weeks of daily RT as a result oflogistical barriers(7–9). In response, interest has beengrowing in accelerating the delivery of radiation to over-
come these obstacles and therefore providing additionalwomen with the option of BCT.
A review of the past treatment experience with BCTrevealed that the overwhelming majority of in-breast fail-ures were in the immediate vicinity of the lumpectomycavity (10–13). Failures elsewhere in the breast are foundwith extended follow-up in only 1–3% of patients(10–13).The failures beyond the lumpectomy cavity occur withequal frequency in both patients treated with lumpectomyonly and patients treated with lumpectomy and whole breastRT. This finding suggests that the impact of whole breastRT on reducing the in-breast failure rate is only at the siteof initial involvement and that equivalent local control rates
Reprint requests to: Douglas W. Arthur, M.D., Department ofRadiation Oncology, Medical College of Virginia Hospitals ofVirginia Commonwealth University, P.O. Box 980058, Richmond,VA 23298-0058. Tel: (804) 828-7232; Fax: (804) 828-6042;E-mail: [email protected]
Presented at the 43rd Annual Meeting of the American Societyof Therapeutic Radiology and Oncology, November 4–8, 2001,San Francisco, CA.
Received Jun 14, 2002, and in revised form Oct 3, 2002.Accepted for publication Jan 8, 2003.
Int. J. Radiation Oncology Biol. Phys., Vol. 56, No. 3, pp. 681–689, 2003Copyright © 2003 Elsevier Inc.
Printed in the USA. All rights reserved0360-3016/03/$–see front matter
681
can be achieved with partial breast RT. Two to 5-yearfollow-up data are now being reported for PBB from severalinstitutions suggesting equivalent safety and efficacy com-pared with whole breast RT (14–18). Additionally, severaldifferent methods of accelerated breast RT have been de-scribed, including both catheter- and balloon-based brachy-therapy delivering treatment within 4–5 days and intraop-erative treatment delivering RT entirely at the time oflumpectomy (19–23). We report an analysis of our initialexperience with PBB after lumpectomy for selected early-stage breast cancer patients. Patient characteristics and treat-ment parameters were evaluated in relationship to treatmentoutcome, with particular emphasis on the assessment ofcosmetic results and the identification of risk factors foradverse cosmetic changes.
METHODS AND MATERIALS
Patient selectionBetween 1995 and 2000, 44 women were treated with
PBB as the only method of adjuvant RT after surgery forearly-stage breast cancer. With institutional review boardapproval, this treatment experience was reviewed to evalu-ate the relationship of treatment parameters to outcome. Theintent of patient selection for this procedure was to includeonly those patients for whom the clinical, mammographic,and pathologic features of their presenting lesions suggestedthat the region of greatest risk of in-breast failure was mostlikely confined to the area of lumpectomy. Patient selectioncriteria were predetermined and prospectively applied. Ini-tially, noninvasive disease was included. This was laterrevised to only include invasive disease. All 44 patientspresented with clinical and mammographic evidence ofunifocal disease, underwent lumpectomy, and were histo-logically proven to have breast cancer. Patient and treatmentcharacteristics are listed in Table 1. The primary lesionremoved was required to be unifocal and �4 cm in greatestdimension with negative microscopic margins (defined asno tumor involving the inked resection margin). Patientswith evidence of an extensive intraductal component werenot included. Patients who had Stage NX with a risk ofaxillary metastasis of �5% were included. Initially, axillarydissection was necessary and patients with up to 1–3 posi-tive lymph nodes without evidence of extracapsular exten-sion were allowed. However, following reports regardingthe potential benefit of chest wall RT in node-positivewomen, this policy was changed to include node-negativewomen only (24, 25). Additionally, patients determined tobe node negative by sentinel node evaluation were laterincluded as the reliability of the sentinel node procedurewas accepted.
Surgery and pathologic evaluationThe surgical aspect of treatment consisted of lumpectomy
and axillary nodal evaluation by Level I–II dissection orsentinel lymph node procedure. The goal of lumpectomywas to remove the index lesion with a margin of normal
breast tissue while conserving the breast with an acceptablecosmetic outcome. India ink was used to coat the lumpec-tomy specimen surface, and the specimen was subsequentlyprocessed for disease identification and determination ofmargin status. If malignant cells did not extend to the inkedsurface, the margin status was considered negative. Thenegative margin status was then further characterized with ameasurement, in millimeters, of the closest extent of malig-nant cells to the inked specimen surface. Most patientscompleted axillary nodal evaluation with Level I-II axillarydissection or negative sentinel node dissection. All patho-logic data were reviewed in the Department of Pathology,Virginia Commonwealth University Medical College ofVirginia Campus. Five patients were clinically node nega-tive and did not undergo surgical lymph node evaluation.Three of these five had a limited risk of lymph node in-volvement, two of them (both age �75 years) had primarylesions �1 cm in size and one had ductal carcinoma in situ.The two additional patients had undergone prior axillary
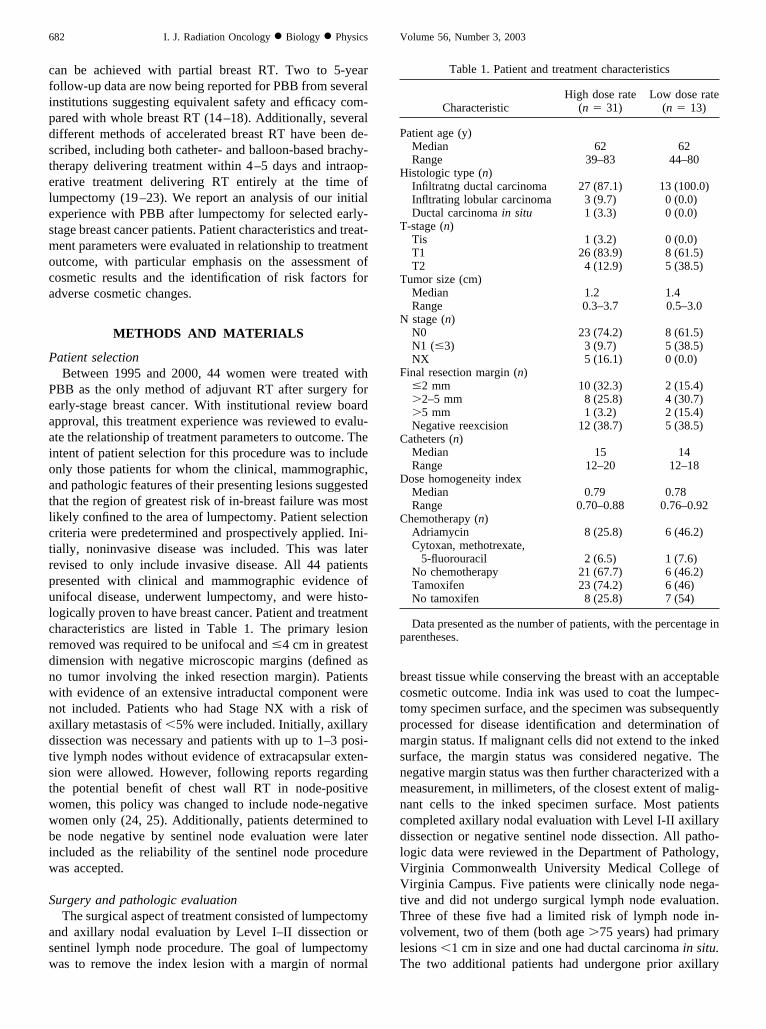
Table 1. Patient and treatment characteristics
CharacteristicHigh dose rate
(n � 31)Low dose rate
(n � 13)
Patient age (y)Median 62 62Range 39–83 44–80
Histologic type (n)Infiltratng ductal carcinoma 27 (87.1) 13 (100.0)Infltrating lobular carcinoma 3 (9.7) 0 (0.0)Ductal carcinoma in situ 1 (3.3) 0 (0.0)
T-stage (n)Tis 1 (3.2) 0 (0.0)T1 26 (83.9) 8 (61.5)T2 4 (12.9) 5 (38.5)
Tumor size (cm)Median 1.2 1.4Range 0.3–3.7 0.5–3.0
N stage (n)N0 23 (74.2) 8 (61.5)N1 (�3) 3 (9.7) 5 (38.5)NX 5 (16.1) 0 (0.0)
Final resection margin (n)�2 mm 10 (32.3) 2 (15.4)�2–5 mm 8 (25.8) 4 (30.7)�5 mm 1 (3.2) 2 (15.4)Negative reexcision 12 (38.7) 5 (38.5)
Catheters (n)Median 15 14Range 12–20 12–18
Dose homogeneity indexMedian 0.79 0.78Range 0.70–0.88 0.76–0.92
Chemotherapy (n)Adriamycin 8 (25.8) 6 (46.2)Cytoxan, methotrexate,
5-fluorouracil 2 (6.5) 1 (7.6)No chemotherapy 21 (67.7) 6 (46.2)Tamoxifen 23 (74.2) 6 (46)No tamoxifen 8 (25.8) 7 (54)
Data presented as the number of patients, with the percentage inparentheses.
682 I. J. Radiation Oncology ● Biology ● Physics Volume 56, Number 3, 2003

dissections for preexisting disease; one with early-stagebreast cancer treated 10 years before with lumpectomy andno adjuvant breast RT and one with soft-tissue sarcoma ofthe upper arm.
Systemic therapyRecommendations regarding systemic therapy were left
to the discretion of the medical oncologist involved in eachcase. The initiation of all systemic treatment was withheldfor the first 2 weeks after the completion of brachytherapy.Fourteen patients received adriamycin-based chemotherapy,8 of whom also received tamoxifen. Three patients receiveda combination of cytoxan, methotrexate, and 5-fluorouracilchemotherapy, 21 received tamoxifen only, and 6 patientsdid not receive any additional systemic therapy.
Brachytherapy—catheter placementThe aim of catheter placement was to ensure homoge-
neous dose delivery to the target volume. The catheterplacement techniques were identical regardless of dose rate.The target volume was defined as the lumpectomy cavityplus a 2-cm margin, except where these target dimensionswere limited by the extent of breast tissue (i.e., chest walland skin). Our preference was to place catheters after reviewof the final pathology report, allowing us to determine theappropriateness of breast brachytherapy and avoid unnec-essary catheter placement. Therefore, catheters were placedat the time of lumpectomy in only 1 case. In this case,surgical clips were placed after lumpectomy. Under directvisualization of the open lumpectomy cavity, the skin wasmarked to reflect the extent of the cavity. Button-endedcatheters were then placed with a free-hand technique byfirst placing a series of metal trocars into position. Eachtrocar was then used as a guide and a button-ended after-loading catheter pulled into position. Once all the catheterswere appropriately placed, the wound was closed and theposition of the catheters secured with a stabilizing button. Inthe remaining cases, the catheters were placed with a closedcavity and, in most cases, surgical clips were placed at thetime of breast-conserving surgery, thus delineating thelumpectomy cavity. In those cases in which surgical clipswere not placed, radiopaque marker seeds placed with ul-trasound guidance around the lumpectomy cavity served toidentify the cavity. Catheter placement was initially per-formed in the ambulatory surgical suite under conscioussedation. Fluoroscopy provided visualization of the surgicalclips/marker seeds and guidance of free-hand catheterplacement. The catheter placement procedure was latermoved to our department where use of the CT simulator hasallowed fluoroscopic and CT-guided catheter placement.Catheters were placed at 1–1.5-cm intervals with an inter-planar separation individually determined for each caseusing an algorithm to ensure homogeneous dose coverage ofthe target (26, 27).
Brachytherapy—dosimetry and treatment deliveryDosimetric planning was initiated after acquisition of
orthogonal film radiographs of the implant. The locations ofthe surgical clips/marker seeds were digitized into the plan-ning system to represent the lumpectomy cavity, and thetarget was extrapolated from these points. Two-dimensionaltreatment planning was completed with the Theraplan sys-tem for the 13 patients treated with LDR brachytherapy. Forthe 31 patients treated with HDR brachytherapy, cases wereeither planned with the Nucletron Planning System (Nucle-tron, B.V., Veenendal, The Netherlands) or the three-di-mensional Brachyvision Planning System (Varian, PaloAlto, CA). Dose uniformity was achieved with individuallyoptimized seed selection for the LDR cases and varied dwellposition times for the HDR cases. The dose homogeneityindex (DHI) was calculated for each case as modified anddescribed in Radiation Therapy Oncology Group protocol95-17 and was defined as the prescription dose divided bythe mean central dose (1). A DHI of �0.85 was consideredideal, with a DHI of at least 0.75 considered acceptable.Skin doses were calculated and in all cases did not exceedthe prescription dose. Necessary catheter revision was oc-casionally needed to meet dosimetric goals. The prescribedminimal dose to the target in patients treated with LDRbrachytherapy was 45 Gy at a dose rate of 50 cGy/h. 192IrLDR sources were used. Patients treated with HDR brachy-therapy received a minimum of 34 Gy to the target. Thiswas delivered in 10 b.i.d. fractions of 3.4 Gy. An 192Ir HDRsource (nominal 10 Ci) was used for dose delivery. Afterdiscussion of the treatment delivery details, each patient wasoffered the opportunity to be treated with either HDR orLDR brachytherapy.
The radiobiologic equivalence between HDR and LDRbrachytherapy treatment has been discussed for many years,and the treatment schemes used in this study have beenaccepted as equivalent and reported elsewhere (1). Throughlinear-quadratic model calculations, the proper HDR frac-tionation scheme can be derived so that the expected radio-biologic effects are equivalent for both treatment ap-proaches used (28, 29). The biologic effective doses forLDR and HDR brachytherapy treatment are given by
BEDLDR � Rt�1 �2R
�(� / �)� �1 �1
�t�BEDHDR � Nd�1 �
d
� / ��where R � dose rate (Gy · h�1), t � LDR treatment time(h), N � number of HDR fractions (� 10), and d � HDRdose/fraction (Gy).
In this study, late effects were of importance. Therefore,assuming that the dose rate for 45 Gy LDR � 0.5 Gy · h�1
(treatment time 4 days � 90 h), �/� for late-reacting normaltissues � 2.5 Gy, and � for late-reacting normal tissues �0.46 h�1 (i.e., half time for repair � 1.5 h), the equationscan then be equated and solved for the HDR dose/fraction
683PBB after lumpectomy: HDR and LDR experience ● D. W. ARTHUR et al.

(d) suggesting that 34 Gy HDR delivered in 10 fractions of3.4 Gy and 45 Gy delivered at 50 cGy/h should yield thesame rate of fibrosis and fat necrosis.
Follow-up evaluationOnce treatment was completed, the catheters were re-
moved, and the patient was discharged home with skin careinstructions. Each patient was seen 2 weeks after treatmentcompletion and then at 3-month intervals. Mammogramswere obtained at 6 months after treatment and then yearly.In follow-up, special attention was given to the overallcosmetic outcome and cosmetic change due to brachyther-apy. Clinical examination was the basis for the cosmeticevaluation. The overall cosmetic outcome was scored ac-cording to the scale shown in Table 2. The score givenreflects the clinical examination performed by two physi-cians and the involved nurse at the time of last follow-up.Separate scoring systems for in-brachytherapy treatmentfield fibrosis and telangiectasia was used in an attempt toseparate cosmetic changes due to brachytherapy from post-operative changes. The scoring systems for these parametersare listed in Table 2. A cosmetic change after brachytherapywas designated if the patient was given an in-field fibrosisscore of 3 and/or a telangiectasia score of 2.
Statistical analysisIn this study, cosmetic outcome was dichotomized as a
cosmetic change postbrachytherapy score of 0 vs.1, telan-giectasia score of 0 vs. 1 or 2, and an in-brachytherapy fieldfibrosis score of 0 or 1 vs. 2 or 3 (Table 2). Univariatelogistic regression models (30) were constructed to evaluatewhich factors were significantly predictive of cosmetic out-come. The factors evaluated included tumor stage, primary
size, total excision volume, dose rate, number of catheters,planar separation, DHI, use of tamoxifen, use of adriamy-cin, age, estrogen receptor status, and number of days thecatheter was placed. Once specific characteristics were iden-tified to be an important predictor of cosmetic outcome, theodds ratios and associated 95% confidence intervals werecalculated from the fitted logistic regression model.
RESULTS
Between 1995 and 2000, 44 patients were treated withPBB only after lumpectomy. Most patients were found tohave infiltrating ductal cancer with a primary tumor size of�2 cm in greatest dimension (Table 1). The median tumorsize was 1.2 cm (range 0.3–3.7). Microscopically assessednegative surgical margins were documented in each case.Thirty-one patients were node negative and eight were nodepositive with �3 nodes involved with microscopic meta-static disease. Five had Stage NX as described above. Amedian of 14 catheters was used to cover the target; 31patients were treated with HDR brachytherapy, and 13 weretreated with LDR brachytherapy. The DHI was calculated ineach case to assess the quality of the implant, and all werejudged to be acceptable by this criterion. The DHI was�0.75 (median 0.78, range 0.70–0.92) in all cases, exceptone calculated to be 0.70.
The median follow-up for the entire group was 42 months(range 18–86). Because the dose rate used was determinedby patient preference, the median follow-up for patientstreated with LDR vs. HDR was similar (p � 0.60). Themedian follow-up for patients treated with LDR vs. HDRbrachytherapy was 42 months (range 30–55) and 45 months(range 11–86), respectively. On last follow-up, all patientsremain locally controlled without true recurrences, marginalmiss recurrences, or failures elsewhere as defined by Rechtet al. (31). All patients were alive at last follow-up; how-ever, 2 patients have developed distant metastasis. No re-gional nodal failures were documented. Reflecting bothsurgical and brachytherapy changes, the overall cosmeticoutcome was documented to be good/excellent in 35(79.6%) of the treated patients. Six patients (14%) werejudged to have cosmetic altering changes after brachyther-apy, represented by subcutaneous fibrosis and/or excessivetelangiectasia formation.
ToxicityAll patients tolerated catheter placement and completed
the planned brachytherapy treatment course. A minimallevel of discomfort from catheter presence was experiencedby most, with pain reportedly improving after the first 24 h.Mild pain medication was sporadically needed. Early in ourexperience, 1 patient developed cellulitis during treatmentfor which routine antibiotics were successfully used. Noincidences of significant acute skin toxicity during treatmentwere reported. Mild erythema and transient hyperpigmen-tation over the implant site was occasionally witnessed.However, recall reaction involving the treated skin was
Table 2. Breast outcome assessment
In-brachyherapy field fibrosis0—none1—mild parenchymal thickening, no visible changes2—prominent parenchymal fibrosis, no visible changes3—significant parenchymal fibrosis, visible changes, cosmesis
alteringTelangiectasia
0—none1—minimal, �2 cm2
2—significant, �2 cm2
Cosmetic change after brachytherapy0—No cosmetic change appreciated1—Cosmetic change (in-brachytherapy field fibrosis score of
3 and/or telangiectasia score of 2)Overall cosmesis
Excellent—Perfect symmetry, no visible distortionGood—Slight distortion of nipple, skin, any visible
telangiectasia, mild hyperpigmentation, absent nipple-areolar complex
Fair—Moderate distortion of nipple, breast asymmetry,moderate hyperpigmentation, prominent skin retractionor telangiectasia
Poor—Marked distortion of nipple, breast asymmetry, edema,fibrosis, severe hyperpigmentation
684 I. J. Radiation Oncology ● Biology ● Physics Volume 56, Number 3, 2003

noted to erupt in 43% of those patients who were subse-quently treated with adriamycin (6 of 14). The recall reac-tions documented in these patients followed the first cycleof adriamycin and were characterized by striking erythemaconfined to the skin overlying the brachytherapy target thatprogressed to patchy moist desquamation. The affected skinquickly healed with conservative skin care. Repeated recallreactions in these patients were varyingly seen with subse-quent cycles but with less intensity when documented.
Late toxicity due to brachytherapy consisted of telangi-ectasias and in-brachytherapy field fibrosis. When encoun-tered, they most often represented minimal change (Table3). Notable, cosmetic-altering changes were infrequentlyseen (6 of 44), but when seen were documented to bepresent within a short period, declaring their presencewithin a median time of 12 months after treatment comple-tion. Four patients were scored as developing cosmetic-altering fibrosis, one patient with dense telangiectasias, andone was scored with both cosmetic-altering fibrosis anddense telangiectasias.
Eight patients developed evidence of telangiectaticchange within the field of brachytherapy. Six of these pa-tients developed sparse skin changes limited to an area of
�1 cm2 and therefore were not considered a factor affectingthe overall cosmetic outcome. Only 2 patients developed afocused area of dense telangiectasias involving a portion ofthe skin overlying the brachytherapy field.
In-brachytherapy field cosmetic-altering fibrosis resultingclearly from the treatment delivered occurred in 4 patients.In these 4 cases, the area of fibrosis was prominent onpalpation and enough retraction was seen to affect breastsymmetry and cosmetic outcome. In 1 patient, an abscessdeveloped at the lumpectomy site 9 months after treatment.Treated with incision and drainage with a prolonged courseof antibiotics, the abscess healed with a fair cosmetic out-come as a result of breast asymmetry and was considered afair cosmetic outcome at last follow-up. Abscess leading toan unacceptable cosmetic result has been documented tooccur in series treating with lumpectomy and external beamradiation therapy (EBRT) (16). Because it is uncertain as towhether this was a direct result of brachytherapy, the cos-metic result was scored as a cosmetic change after brachy-therapy. Thirteen additional patients were found to havepalpable thickness of breast tissue within the treated area.However, this mild degree of fibrosis did not affect thecosmetic outcome. Ten patients described mild to moderatepain in the treated area of the breast at an interval of 4–7months after treatment completion. Nine were not consid-ered to have developed fat necrosis, because they failed todemonstrate associated clinical or mammographic changesconsistent with fat necrosis and the pain spontaneouslyresolved within several weeks. One patient had clinical andmammographic signs of fat necrosis when presenting withbreast pain. After the initiation of nonsteroidal anti-inflam-matory medication, the pain and parenchymal changes re-solved. The resulting cosmetic outcome, documented at her45-month follow-up evaluation, was scored as excellent.
CosmesisIn determining the critical parameters that may influence
the postbrachytherapy cosmetic outcome, several tumor andtreatment parameters were evaluated and have been previ-ously listed. From the univariate logistic regression models,we identified several parameters significantly predictive ofearly telangiectasias, cosmetic-altering fibrosis, and/or a
Table 3. Cosmetic outcome
Variable n %
Telangiectasia0 34 77.31 8 18.22 2 4.5
In-brachytherapy field fibrosis0 27 61.41 10 22.72 3 6.83 4 9.1
Cosmetic change after brachytherapy0 38 86.41 6 13.6
Overall cosmesisExcellent 18 40.9Good 17 38.6Fair 7 15.9Poor 2 4.6
Table 4. Univariate logistic regression results
Telangiectasia (0 vs. 1, 2)In-brachytherapy field fibrosis
(0, 1 vs. 2, 3)Change after brachytherapy
(0 vs. 1)
pOdds ratio(95% CI) p
Odds ratio(95% CI) p
Odds ratio(95% CI)
Dose, LDR 0.42 1.85 (0.4–8.1) 0.0006 25.7 (2.7–249.2) 0.003 18.75 (1.9–184.1)Adriamycin 0.004 9.00 (1.8–44.0) 0.001 21.75 (2.3–207.8) 0.005 16.11 (1.7–156.5)Recall reaction 0.0005 33.00 (3.2–344) 0.002 23.33 (3.0–184.3) 0.0006 36.00 (3.9–330.0)Age* 0.02 0.45 (0.2–0.9) 0.11 0.56 (0.3–1.2) 0.22 0.63 (0.3–1.3)
* Odds ratio calculated based on a change of 10 years.Abbreviations: CI � confidence interval; LDR � low dose rate.
685PBB after lumpectomy: HDR and LDR experience ● D. W. ARTHUR et al.

change in cosmesis after brachytherapy (Table 4). Thoseparameters not found significant are not listed in Table 4.Specifically, the odds of experiencing cosmetic-altering fi-brosis and a change in cosmesis after brachytherapy weresignificantly greater when LDR brachytherapy was usedcompared with HDR brachytherapy. Moreover, the odds ofexperiencing early telangiectasias, cosmetic-altering fibro-sis, and a change in cosmesis after brachytherapy weresignificantly greater when adriamycin was used and when arecall reaction was documented. Younger age was signifi-cantly predictive of early telangiectasias.
In those patients treated with HDR brachytherapy, 8 ofwhom also received adriamycin, 28 (90%) were scored witha good/excellent cosmetic outcome. The three (10%) judgedto have a fair cosmetic outcome were documented to have asignificant surgical defect before brachytherapy in two andan abscess formation in one. Among patients judged to havea fair to poor cosmetic outcome, there was a significantdifference with respect to the frequencies of patients dis-tributed among HDR vs. LDR brachytherapy and adriamy-cin chemotherapy (p � 0.048), suggesting that most ofthose who experienced suboptimal results were treated withboth LDR brachytherapy and adriamycin (Table 5). Toevaluate further the relationship between the dose rate usedand adriamycin chemotherapy, univariate logistic regres-sion models were constructed with the indicator variablescombined as LDR brachytherapy and adriamycin chemo-therapy, HDR brachytherapy and adriamycin, and LDRbrachytherapy without adriamycin. HDR brachytherapywithout adriamycin was used as the reference group. Thecombination of LDR brachytherapy and adriamycin provedto be highly predictive for the development of in-brachy-therapy field fibrosis (p � 0.01), with an odds ratio of 24.This combination of treatment modalities was also predic-tive for the development of a cosmetic change after brachy-therapy (p � 0.002), with an odds ratio of 110.
DISCUSSION
Promising results with PBB in selected patients withearly-stage breast cancer have caught the attention of bothpatients and physicians. As additional locations begin tooffer this as a treatment option, it will be important tocommunicate treatment outcomes so that toxicities can be
avoided and the learning curve for this treatment approachreduced. Individual subjectivity is a strong influence in anycosmetic scoring system and makes interinstitutional com-parisons difficult. This subjectivity is further complicatedby the inconsistent approach used between those who scorethe overall cosmetic outcome, as determined by both thesurgical and radiation change, and those who score cosmesison the basis of the radiation change only. Recognizing thesevariabilities, we selected end points that clearly reflected theresults of brachytherapy so that our treatment outcomewould be well-communicated and appropriate conclusionscould be drawn.
The use of PBB was first piloted at two institutions, andthe results with extended follow-up are now available. Vi-cini et al. (15) have updated their entire treatment experi-ence of 174 patients treated with brachytherapy only afterlumpectomy for Stage I-II breast cancer. The median fol-low-up for the entire group was 36 months; however, it wasnoted that 37% of patient had follow-up of �4 years and18% had follow-up of �5 years. Strict selection criteriawere used to avoid including patients with a risk of micro-scopic disease outside the immediate area of the lumpec-tomy cavity. One hundred twenty patients were treated withLDR brachytherapy (50 Gy at a dose rate of 52 cGy/h) and54 patients were treated with HDR brachytherapy (4 Gyb.i.d. to a total of 32 Gy or 3.4 Gy b.i.d. to a total of 34 Gy).A template was used throughout the treatment process toguide needle placement and to ensure consistent dose ho-mogeneity throughout treatment delivery. Implants weredesigned to irradiate the lumpectomy cavity plus a mini-mum of a 1–2-cm margin. One regional failure was re-ported; however, no true or marginal miss recurrences havebeen documented. The 5-year actuarial rate of locoregionalfailure was 1%, with a 5-year cause-specific survival rate of99%. A matched pair analysis was performed and no sta-tistically significant differences in treatment outcome weredetected between patients treated with EBRT and brachy-therapy only. Toxicity was reportedly low in those womentreated with brachytherapy only. Good to excellent cosmeticresults were seen in 90% of patients. Breast pain and asymp-tomatic fat necrosis were documented in only 3% and 4% ofpatients, respectively.
The experience initiated at the Oschner Clinic by Kuskeet al. (32) and updated by King et al. (16) reported on 50
Table 5. Patient distribution according to dose rate and adriamycin use
No adriamycin Adriamycin
HDR LDR p HDR LDR p
In brachytherapy field fibrosis 0.23 0.030,1 23 (100) 6 (86) 7 (87.5) 1 (17)2,3 0 (0) 1 (14) 1 (12.5) 5 (83)
Change after brachytherapy 0.77 0.0030 22 (95) 7 (100) 8 (100) 1 (17)1 1 (4) 0 (0) 0 (0) 5 (83)
Abbreviations: HDR � high dose rate; LDR � low dose rate.
686 I. J. Radiation Oncology ● Biology ● Physics Volume 56, Number 3, 2003

patients with 51 breast cancers. This group was composedof carefully selected patients with Tis, T1, and T2 lesionsresected with microscopically negative margins and 0–3lymph nodes positive without extracapsular extension. Themedian follow-up was 75 months. Twenty-five lesions weretreated with LDR brachytherapy (45 Gy within 4 days) and26 lesions with HDR brachytherapy (4 Gy b.i.d. to a totaldose of 32 Gy). The treatment target was defined as thelumpectomy cavity plus a 2-cm margin. The treatment out-come was compared with that of a contemporary group ofpatients who were eligible for brachytherapy only but weretreated with EBRT. At this follow-up interval, they reportedsimilar treatment outcomes between these two groups. Inthe patients treated with brachytherapy only, one in-breastfailure and three regional failures (8%) were reported. Thiscompares with a 5% breast recurrence rate in their cohort ofEBRT-treated patients. Grade 1 and 2 complications, rang-ing from self-limiting skin erythema and desquamation tomoderate changes resolving without surgical intervention,occurred in 80% of EBRT patients and only 22% of brachy-therapy-only patients. However, Grade 3 complications (se-vere and requiring surgical intervention) were documentedin 4 (8%) of the brachytherapy-only patients: one hema-toma, one infectious complication, and 2 cases of fat necro-sis. An earlier report stated that 10 additional patients weredocumented to have fat necrosis that resolved with conser-vative treatment (32). The Grade 3 complication rate theyreported with brachytherapy only compares directly withthe 5% Grade 3 complication rate experienced in theirpatients treated with EBRT.
Wazer et al. (33) reported on their recent experience of 30patients treated with HDR brachytherapy only after lumpec-tomy. Patients eligible included those with Stage T1, T2,N0, N1 (�3 nodes positive), M0 tumors of nonlobularhistologic subtype with negative surgical margins, no ex-tracapsular lymph node extension, and a negative postexci-sion mammogram. The median follow-up was 24 months.Patients were treated with 3.4 Gy b.i.d. on 5 consecutivedays to a total dose of 34 Gy to a target volume thatincluded the lumpectomy cavity plus a 2-cm margin. Clin-ically evident fat necrosis was reported, with a crude inci-dence of 27% (8 patients). A dosimetric analysis revealedthat the size of the implant as represented by the number ofdwell positions and the volume of breast tissue receivingfractional doses of 340, 510, and 680 cGy correlated sig-nificantly with the development of fat necrosis.
In our series of 44 patients treated with PBB only, 6patients experienced a suboptimal cosmetic change aftertreatment. These patients developed significant in-brachy-therapy field fibrosis and/or telangiectasias within a shortinterval after treatment completion (median 12 months).Our analyses suggest a correlation between cosmetic failureand the use of LDR brachytherapy in combination withadriamycin chemotherapy. In an attempt to explain thiscorrelation, potential contributions from the chemotherapyand RT aspects of treatment should be considered. Concur-rent and sequential delivery of adriamycin and RT is known
to result in increased interaction and toxicity (34). Devel-opment of a recall reaction when adriamycin was used afterbrachytherapy was not anticipated before initiation of thistreatment approach, but was experienced in 43% of patientswho received adriamycin. However, the use of adriamycinstrongly correlated with the risk of cosmetic failure whencombined with a LDR implant.
One possible explanation for the correlation betweenLDR PBB and adverse cosmetic results would be a differ-ence in the radiobiologic effective dose between the HDRand LDR dose scheme used. It is uncertain as to whether thesame dose–response rules that govern the cytotoxic effectsof radiation on tumor and normal tissue cells can be appliedto the development of late soft-tissue effects such as fibrosisand angiogenesis. We suspect that another contributing fac-tor is the key technical differences between free-hand HDRand LDR brachytherapy treatment delivery. The ability toprogram each dwell position in a HDR implant is a clearadvantage over LDR brachytherapy planning. Althoughlimited customization with varied 192Ir source strength anddifferential unloading is recognized, the homogeneity onecan achieve with a HDR planning system is superior. In thedelivery of the intended dose, HDR has additional advan-tages. In a HDR implant, the patient is easily repositioned asshe was for simulation for each fractional dose delivered,and the correct catheter position and intercatheter relation-ship can be guaranteed before each treatment. Therefore, theplanned dose homogeneity will equal the delivered dosehomogeneity. However, this cannot be assured with a free-hand LDR implant, because the intercatheter relationship isaltered with patient movement during the course of the 90-htreatment delivery. Patient movement can cause a collapseof the implant structure and potentially result in a significantincrease in the dose received to the targeted breast tissue.Because this effect cannot be documented during the treat-ment course, those patients in whom this might have hap-pened and the degree to which this occurred cannot beidentified. This likely variability suggests that the subopti-mal outcome experienced with LDR brachytherapy may bethe result of an undefinable degree of inhomogeneity.
CONCLUSION
Treatment with accelerated PBB in this experience re-sulted in a good to excellent overall cosmetic outcome in79.4% and controlled disease within the treated breast of100% with a median follow-up of 42 months. Treatmentwith HDR brachytherapy resulted in a 90% good/excellentoverall cosmetic outcome. The 10% scored as a fair cos-metic outcome were composed of 2 patients judged to havefair cosmesis after surgery and 1 after abscess formation.Overall cosmetic failures, as a result of the brachytherapytreatment, were reported in only 6 patients (14%). Thecorrelation of treatment parameters to treatment outcomefound a significant association between the risk of cosmeticfailure and the combined use of LDR brachytherapy andadriamycin. Other publications have not reported an adverse
687PBB after lumpectomy: HDR and LDR experience ● D. W. ARTHUR et al.

effect of adriamycin with the use of brachytherapy (15, 16,33). The results of this study suggest that the added negativeeffect of adriamycin is only realized when LDR brachyther-apy dose is used. This is possibly explained by the uncon-trolled dose delivery and limitations in source strengthoptimization, resulting in an undefinable dose inhomogene-ity that is further exacerbated with the use of adriamycin.Our HDR treatment experience indicates that with a prop-erly constructed implant and control over dose delivery,
good/excellent cosmetic results should be achieved evenwith the addition of adriamycin. On the basis of thesefindings, we no longer offer LDR brachytherapy and onlyoffer HDR brachytherapy for accelerated partial breast RTbecause of the additional control over catheter position andintercatheter relationship that it provides. If LDR brachy-therapy is to be used in this setting, it is recommended thata template be used to ensure the dose is delivered with itsintended homogeneity.
REFERENCES
1. Kuske RR, Bolton JS. A phase I/II trial to evaluate brachy-therapy as the sole method of radiation therapy for stage I andII breast carcinoma. Radiation Therapy Oncology Group Pub-lication No. 1055. Philadelphia: Radiation Therapy OncologyGroup, 1995.
2. Fischer B, Anderson S, Tan-Chiu E, et al. Fifteen-year prog-nostic discriminants for invasive breast carcinoma—NationalSurgical Adjuvant Breast and Bowel Project Protocol B-06.Cancer Suppl 2001;91:1679–1687.
3. Fischer B, Anderson S, Redmond CK, et al. Reanalysis andresults after 12 years of follow-up in a randomized clinicaltrial comparing total mastectomy with lumpectomy with orwithout irradiation in the treatment of breast cancer. N EnglJ Med 1995;333:1456–1461.
4. Schmidt-Ullrich RK, Wazer DE, DiPetrillo T, et al. Breastconservation therapy for early stage breast carcinoma withoutstanding 10-year locoregional control rates: A case foraggressive therapy to the tumor bearing quadrant. Int J RadiatOncol Biol Phys 1993;27:545–552.
5. National Institutes of Health. Consensus statement: Treatmentof early-stage breast cancer. NIH Consensus DevelopmentConference, June 18–21, 1990. Vol. 8, No. 6. Bethesda:National Institutes of Health, 1990: p. 1–9.
6. Veronesi U, Salvadori B, Luini A, et al. Breast conservation isa safe method in patients with small cancer of the breast:Long-term results of three randomised trials on 1,973 patients.Eur J Cancer 1995;31:1574–1579.
7. Athas WF, Adams-Cameron M, Hunt WC, et al. Travel dis-tance to radiation therapy and receipt of radiotherapy follow-ing breast-conserving surgery. J Natl Cancer Inst 2000;92:269–271.
8. Hevert-Croteau N, Brisson J, Latreille J, et al. Compliancewith consensus recommendation for the treatment of earlystage breast carcinoma in elderly women. Cancer 1999;85:1104–1113.
9. Du X, Freeman JL, Freeman DH, et al. Temporal and regionalvariation in the use of breast-conserving surgery and radio-therapy for older women with early-stage breast cancer from1983 to 1985. J Gerontol A Biol Sci Med Sci 1999;54:474–478.
10. Veronesi U, Luini A, Del Vecchio M, et al. Radiotherapy afterbreast-preserving surgery in women with localized cancer ofthe breast. N Engl J Med 1993;328:1587–1591.
11. Liljegren G, Holmberg L, Adami HO, et al., for the Uppsala-Oreboro Breast Cancer Study Group. Sector resection with orwithout post-operative radiotherapy for stage I breast cancer:Five-year results of a randomized trial. J Natl Cancer Inst1994;86:717–722.
12. Clark RM, Whelan T, Levine M, et al. for the Ontario ClinicalOncology Group. Randomized clinical trial of breast irradia-tion following lumpectomy and axillary dissection for node-negative breast cancer: An update. J Natl Cancer Inst 1996;88:1659–1664.
13. Fischer ER, Sass R, Fisher B, et al. Pathologic findings fromthe National Surgical Adjuvant Breast Project (protocol 6).Cancer 1986;57:1717–1724.
14. Ribiero GG, Dunn G, Swindell R, et al. Conservation of thebreast using two different radiotherapy techniques: Interimreport of a clinical trial. Clin Oncol 1993;5:278–283.
15. Vicini FA, Baglan KL, Kestin LL, et al. Accelerated treatmentof breast cancer. J Clin Oncol 2001;19:1993–2001.
16. King TA, Bolton JS, Kuske RR, et al. Long-term results ofwide-field brachytherapy as the sole method of radiation ther-apy after segmental mastectomy for Tis,1,2 breast cancer. Am JSurg 2000;180:299–304.
17. Cionini L, Pacini P, Marzano S, et al. Exclusive brachytherapyafter conservative surgery in cancer of the breast [Abstract].Lyon Chir 1993;9:128.
18. Berle L, Lowther D, DiPetrillo T, et al. A phase I/II Study ofHDR brachytherapy alone for T1/T2 breast cancer. Int JRadiat Oncol Biol Phys 2001;51(Suppl 1):5.
19. Kuske RR. Breast brachytherapy. Hematol Oncol Clin NorthAm 1999;13:543–558.
20. Vicini FA, Jaffray DA, Horowitz EM, et al. Implementation of3D-virtual brachytherapy in the management of breast cancer:A description of a new method of interstitial brachytherapy.Int J Radiat Oncol Biol Phys 1998;40:629–635.
21. Veronesi U, Orecchia R, Luini A, et al. A preliminary reportof intraoperative radiotherapy (IORT) in limited-stage breastcancers that are conservatively treated. Eur J Cancer 2001;37:2178–2183.
22. Vaidya JS, Baum M, Tobias JS, et al. Targeted intra-operativeradiotherapy (Targit): An innovative method of treatment forearly breast cancer. Ann Oncol 2001;12:1075–1080.
23. Edmundson GK, Vicini FA, Chen PY, et al. Dosimetric char-acteristics of the mammosite RTS: A new breast brachyther-apy applicator. Int J Radiat Oncol Biol Phys 2002;52:1132–1139.
24. Overgaard M, Hansen PS, Overgaard J, et al. The DanishBreast Cancer Cooperative Group 82b trial. N Engl J Med1997;337:949–955.
25. Ragaz J, Jackson SM, Le N, et al. Adjuvant radiotherapy andchemotherapy in node-positive premenopausal women withbreast cancer. N Engl J Med 1997;337:956–962.
26. Zwicker RD, Arthur DW, Kavanagh BD, et al. Optimizationof planar high-dose-rate implants. Int J Radiat Oncol BiolPhys 1999;44:1171–1177.
27. Zwicker RD, Schmidt-Ullrich R. Dose uniformity in a planarinterstitial implant system. Int J Radiat Oncol Biol Phys1994;31:149–155.
28. Orton CG, Brenner DJ, Dale RG, et al. Radiobiology. In: NagS, editor. High dose rate brachytherapy: A textbook. NewYork: Futura Publishing, 1994: p. 11–25.
29. Brenner DJ, Dale R, Orton CG, et al. Radiobiology of highdose-rate, low dose-rate, and pulsed dose-rate brachytherapy.
688 I. J. Radiation Oncology ● Biology ● Physics Volume 56, Number 3, 2003

In: Joslin CAF, Flynn A, Hall EJ, editors. Principles andpractice of brachytherapy using afterloading systems. NewYork: Oxford University Press, 2001: p. 189–204.
30. Kleinbaum DG. Logistic regression. New York: Springer-Verlag, 1994.
31. Recht A, Silver B, Schnitt S, et al. Breast relapse followingprimary radiation therapy for early breast cancer. I. classifi-cation, frequency and salvage. Int J Radiat Oncol Biol Phys1985;11:1271–1276.
32. Kuske RR, Bolton JS, McKinnon WMP, et al. 5-yr results of
a prospective phase II trial of wide-volume brachytherapy asthe sole method of breast irradiation in Tis, T1, T2, N0-1breast cancer [Abstract]. Int J Radiat Oncol Biol Phys 1998;42(Suppl 1):181.
33. Wazer DE, Lowther D, Boyle T, et al. Clinically evident fatnecrosis in women treated with high-dose-rate brachytherapyalone for early-stage breast cancer. Int J Radiat Oncol BiolPhys 2001;50:107–111.
34. Camidge R, Price A. Characterizing the phenomenon of radi-ation recall dermatitis. Radiother Oncol 2001;59:237–245.
689PBB after lumpectomy: HDR and LDR experience ● D. W. ARTHUR et al.





























