Embed Size (px)
Citation preview

Ovarian Cancer Overview for Health Care Providers
• Created by the GOC CoP Nursing group: – Heidi Thomas, Joanne Power, Janet
Giroux, Nancy Drummond, Lynne Jolicoeur, Joanne Brodeur and Elisha Andrews
– Reviewed and edited by Dr. L. Elit

The slides presented are meant to be used as an orientation package for health care providers new to gynecologic oncology; to review the management and treatment of ovarian cancer with a focus on epithelial subtypes Variation across the country can occur in accordance within provincial guidelines. Remember that not all patients are the same and that some deviation CAN and often does occur.
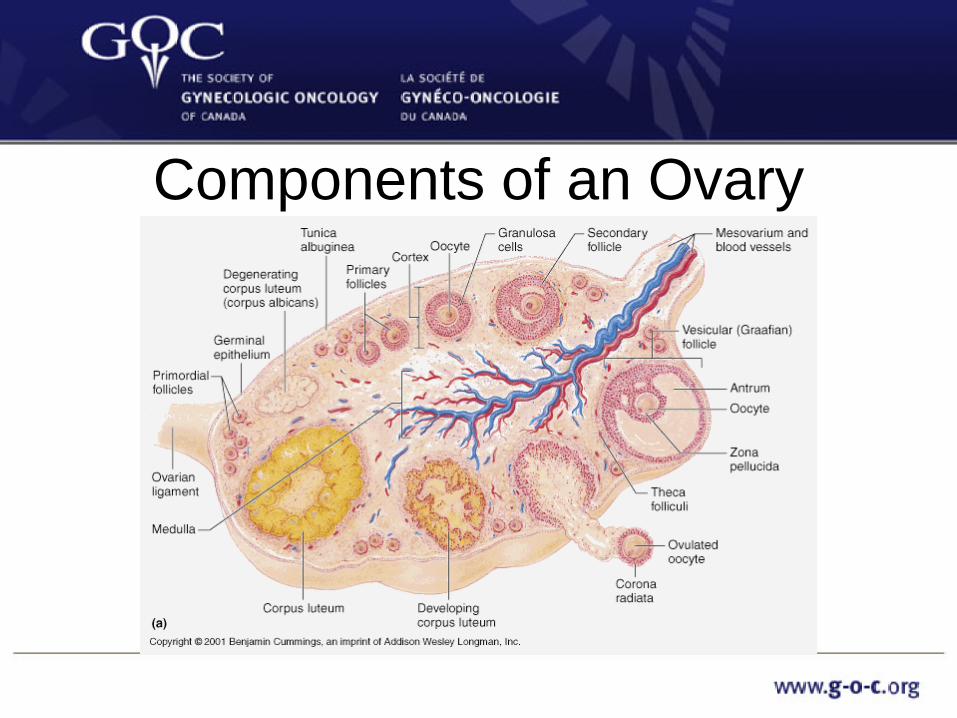
Components of an Ovary

Incidence of Ovarian cancer • Incidence
– In 2013 it is estimated 2,600 women will be diagnosed and 1,750 women will die from ovarian cancer in Canada
– Median age of diagnosis is 56.3 years – 2.9% of all cancers diagnosed in women are ovarian
• Mortality – Ovarian cancer is the most lethal of all gynecologic cancers – It is the 5th leading cause of cancer deaths overall – 5 year survival rate is 45.5%
• Lifetime Risk – 1.5% or 1 in 68 women
Canadian Cancer Society’s Advisory Committee on Cancer Statistics. Canadian Cancer Statistics 2013.

Stage and Survival Stage 5 Year Survival
Rate
I 89%
II 66%
III 34%
IV 18%
Surveillance, Epidemiology, and End Results Program (SEER). National Cancer Institute, 2014.
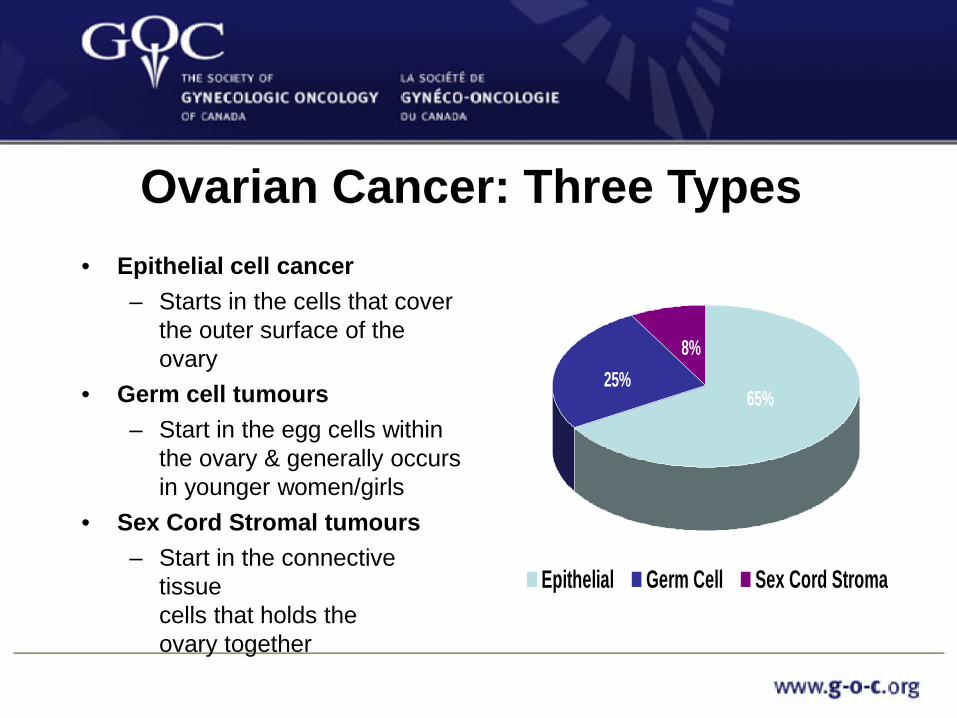
Ovarian Cancer: Three Types • Epithelial cell cancer
– Starts in the cells that cover the outer surface of the ovary
• Germ cell tumours – Start in the egg cells within
the ovary & generally occurs in younger women/girls
• Sex Cord Stromal tumours – Start in the connective
tissue cells that holds the ovary together
8%25%
65%
Epithelial Germ Cell Sex Cord Stroma

Epithelial Subtypes
• Serous • Endometrioid • Undifferentiated • Borderline • Clear Cell • Mucinous
Epithelial Ovarian Cancer

Pathophysiology • Paradigm Shift in past 7 – 8 years • Ovarian Cancer begins in the fallopian tubes and falls
on to the ovarian epithelial surface
Epithelial Ovarian Cancer
Fallopian tube
Fallopian tube

Ovarian Cancer Risk Factors Increase Decrease
Age Oral Contraceptive Use Positive Family history of
Ovarian or Breast Ca Pregnancy and Breastfeeding
Infertility/low parity (not bearing children) Salpingectomy
Personal cancer history of Breast, Colon or Uterine
Ca
Hysterectomy/Removal of Both Ovaries + tubes
Epithelial Ovarian Cancer

Oral Contraceptives Duration of Use Decrease in Risk ALL YOUNG WOMEN Never 0 3 months – 4 years 30-40% 5 – 9 years 60% 10 years and greater 80% BRCA Carriers 50-60%
Epithelial Ovarian Cancer

Pregnancy and Breastfeeding No of term pregnancies Decrease in Risk 0 0 1 40% 2 47% 3 52% 4 64% 5 67% > 6 71% BRCA 1 or 2, or both 12%/birth
Epithelial Ovarian Cancer

Familial Oncology Genetics • 10% overall risk • Patients at high-risk
– +/- Genetic Testing – BRCA 1 or 2 mutation – Hereditary Non Polyposis
Colon Cancer – Familial Ovarian/Breast
Cancer – Ethnicity – Personal history of Serous/
Endometrioid Ovarian Cancer
• Counseling – Breast Cancer risk – Screening Programs for
breast cancer – Prophylactic oophorectomy,
hysterectomy & mastectomy – Genetic counseling and
testing
Epithelial Ovarian Cancer
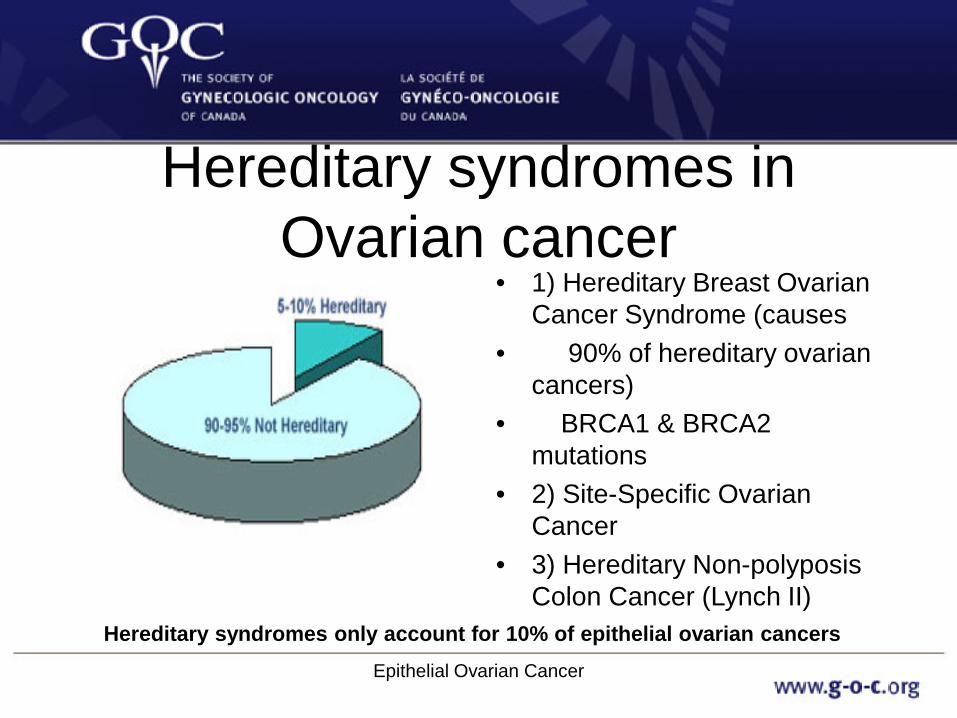
Hereditary syndromes in Ovarian cancer
• 1) Hereditary Breast Ovarian Cancer Syndrome (causes
• 90% of hereditary ovarian cancers)
• BRCA1 & BRCA2 mutations
• 2) Site-Specific Ovarian Cancer
• 3) Hereditary Non-polyposis Colon Cancer (Lynch II)
Hereditary syndromes only account for 10% of epithelial ovarian cancers Epithelial Ovarian Cancer
BRCA mutations and ethnicity • 4 founder mutations among
Ashkenazi Jews – Prevalence 1 in 40
• Other groups with BRCA1/2
mutation families: – French-Canadian – Mennonite – Icelandic – Scandinavian
Epithelial Ovarian Cancer

BRCA 1 Hereditary Breast and Ovarian Cancer
Breast cancer 85%
Average Risk of Ovarian Cancer Up to Age 50 BRCA1 20% General Pop 1.7%
Second primary breast cancer 40%-60%
Average Risk of Ovarian Cancer up to Age 80 BRCA1 50% General Pop 1.4%

BRCA2 Hereditary Breast and Ovarian Cancer
breast cancer (30%-85%)
ovarian cancer (10%-20%)
male breast cancer (6.7%)
Average Risk of Ovarian Cancer Up to Age 50 BRCA2 3% General Pop 1.7%
Average Risk of Ovarian Cancer up to Age 80 BRCA2 20% General Pop 1.4%
Red Flags • BRCA 1 and 2
mutations • Breast cancer prior to age of
50 • Ovarian cancer at any age • Multiple primary cancers • Ashkenazi Jewish ancestry • Relatives of a BRCA
mutation carrier
• HNPCC (Lynch II) • Onset of colorectal cancer
before age 50 • Onset of endometrial cancer
before age 50 • Two or more HNPCC
cancers in an individual or family
Signs and symptoms • Bloating, increased
abdominal girth • Pelvic or abdominal
pain • Dyspepsia, indigestion,
early satiety • Urinary symptoms
(urgency or frequency) • Muscle wasting of
extremities/face
• Fatigue • Gas, change in bowel
habits • Rectal/bladder pressure • Unusual vaginal
bleeding • Weight loss or weight
gain • SOB on exertion or at
rest *June 2007 ACS, SOGC (US), GCF, IGCS Epithelial Ovarian Cancer
Symptoms: exfoliation and implantation of cancer cells on surfaces of peritoneal cavity
• Ovarian cancer cells shed
from original site in the ovary and land anywhere on lining of pelvic abdominal peritoneum, causing:
• Ascites • Bowel Obstruction • Pleural Effusion
Most problems relate to the abdominal area where the disease tends to stay Epithelial Ovarian Cancer
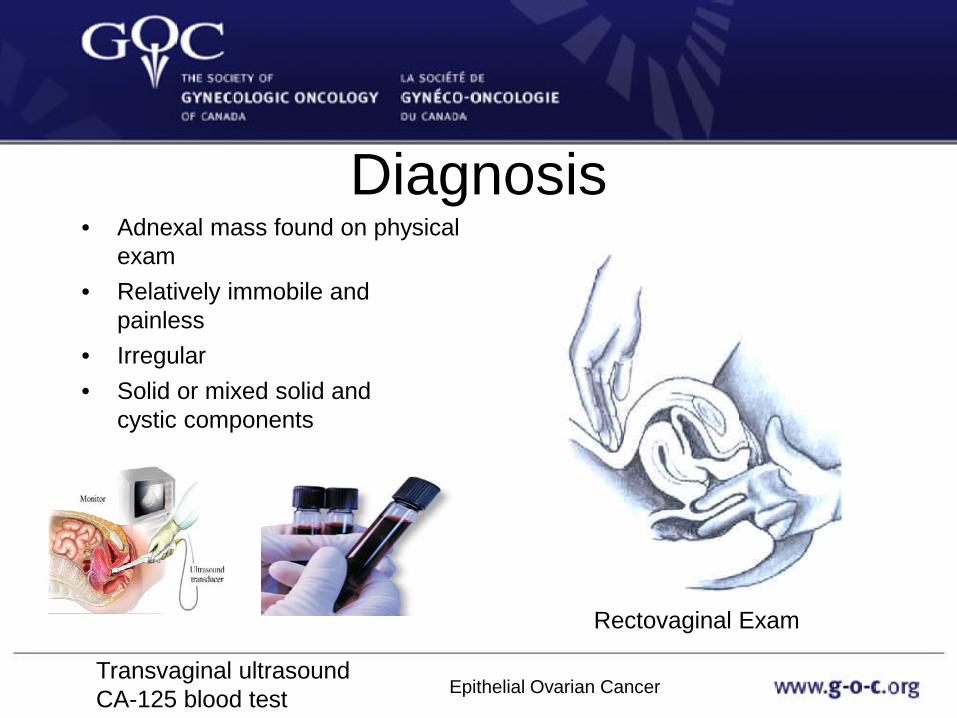
Diagnosis • Adnexal mass found on physical
exam • Relatively immobile and
painless • Irregular • Solid or mixed solid and
cystic components
Rectovaginal Exam
Transvaginal ultrasound CA-125 blood test Epithelial Ovarian Cancer

Diagnosis – Imaging studies (ultrasound, CT, MRI) – Blood tests (CA-125) – Biopsy of omental cake or other solid lesions – Analysis of peritoneal fluid (ascites) or pleural fluid
Ultrasound image CT image Epithelial Ovarian Cancer
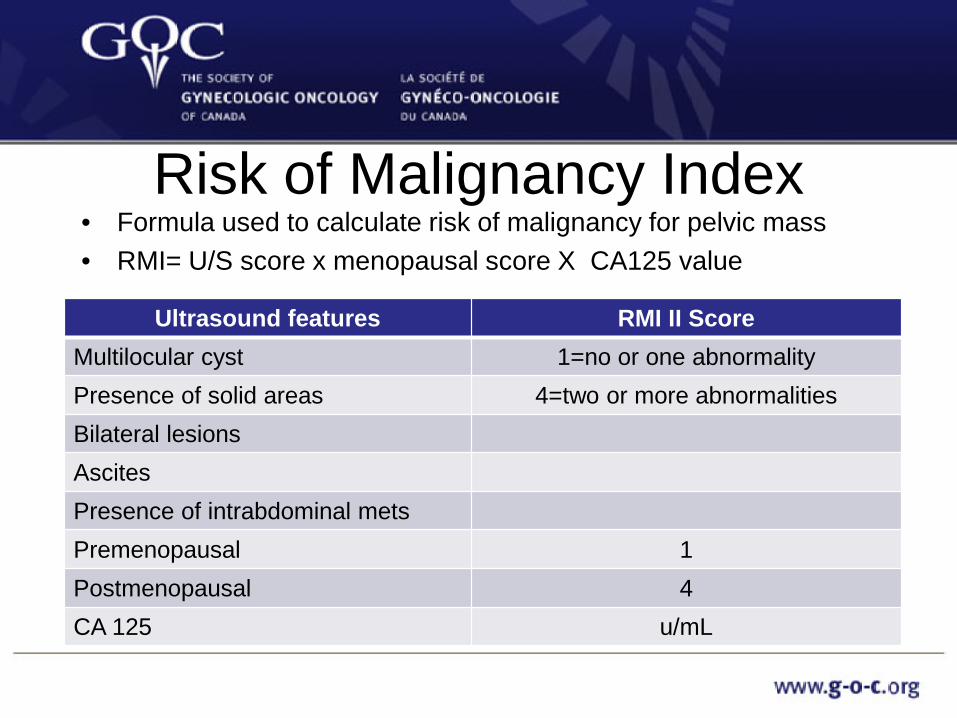
Risk of Malignancy Index • Formula used to calculate risk of malignancy for pelvic mass • RMI= U/S score x menopausal score X CA125 value
Ultrasound features RMI II Score Multilocular cyst 1=no or one abnormality Presence of solid areas 4=two or more abnormalities Bilateral lesions Ascites Presence of intrabdominal mets Premenopausal 1 Postmenopausal 4 CA 125 u/mL
CA-125 • A mucin-like glycoprotein that increases in response to disturbances of
the peritoneal surface • Known as a tumor associated antigen • In patients <50 years of age an elevated CA-125 is associated with a
malignant mass <25% of the time • In patients >50 years of age this association increase to 80% of the
time • Is not a screening or diagnostic test • Nonspecific tumour marker with variations in interpretation depending
on the patient’s medical history & age • Level does not correlate with burden of disease • False positive & negative results
Epithelial Ovarian Cancer
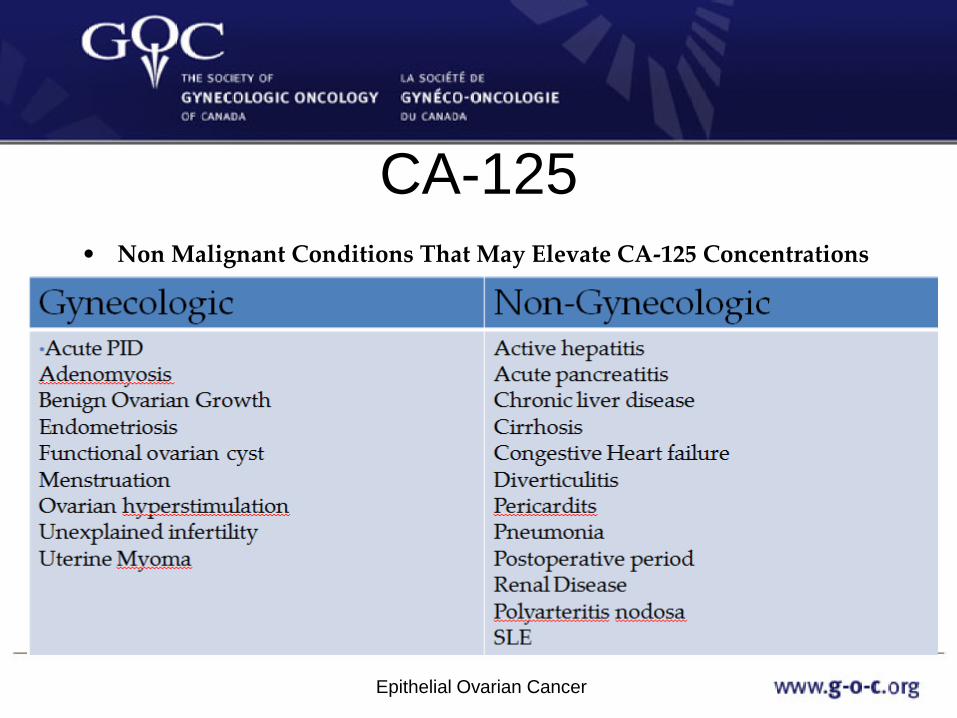
CA-125 • Non Malignant Conditions That May Elevate CA-125 Concentrations
Epithelial Ovarian Cancer

Spread of Ovarian Cancer
Epithelial Ovarian Cancer

Medical Management Includes
• Awareness of multisystem dysfunction – Peritoneal Ascites – Pleural Effusions – Bowel Obstructions – Malnutrition – Side Effects from
Chemotherapy – Blood Clots (VTEs or CAT) – Pain Management – Psychosocial Care
Epithelial Ovarian Cancer

Treatment of Ovarian Cancer • Surgery • Chemotherapy
– Neo-adjuvant – Adjuvant
• Clinical trials • Palliative care
Intravenous chemotherapy
Intraperitoneal chemotherapy
Epithelial Ovarian Cancer

Goals of Care • Communication & Education
– Patient’s goals & expectations – Incorporate combination of interventions – Improve QoL
• Alleviation of symptoms – Managing GI side effects/complications presents unique
challenges – Support active & functional life
– Obtain benefits of therapy – Optimize interventions & monitoring
Epithelial Ovarian Cancer

Role of Neoadjuvant Chemotherapy vs. Primary Debulking
• Majority of patients present with advanced disease (Stage 3C/4) • Goal of surgery is complete resection of all macroscopic disease • Surgery has been standard of care as primary treatment of ovarian
cancer however advanced disease presents challenges as patients considerably sicker
• Primary cytoreductive/debulking surgery is associated with higher complications including: – Post op infections – Venous complications – Fistulae – Hemorrhage – Postop mortality/morbidity Vergote, Gynecologic Oncology, 2010, 119(1), 1-2

Role of Neoadjuvant Chemotherapy vs. Primary Debulking
• Neoadjuvant chemotherapy (3 cycles) followed by interval debulking surgery found not to be inferior to primary debulking
• Only patients with Stage 3C or 4 should be considered for neoadjuvant chemo
• Postop complications and mortality rates were decreased after neoadjuvant chemo vs primary debulking
• Overall survival and progression free survival similar between two groups
Vergote, Gynecologic Oncology, 2010, 119(1), 1-2

Procedures Required For Surgical Staging of Ovarian Cancer
• Surgery is the main diagnostic tool Ovarian Cancer
Epithelial Ovarian Cancer

Surgical Management • Based on the spread pattern of ovarian cancer • Operation: Total abdominal hysterectomy, bilateral salpingo-
oophorectomy with staging, pelvic lymph node dissection, omentectomy and debulking
• Two goals of surgery: – Diagnose – Stage – Remove all gross disease
• Disease completely resected ↑ survival outcomes • Incomplete resection, goal is to ↓ tumour burden (Poorer
prognostic factor)
Epithelial Ovarian Cancer

Definition of Terms • Omentectomy: The surgical removal of a sheet of fat
that is located under the fascia, attached to the bottom edge of the stomach and liver.
• Staging: The process of obtaining specimens intra-operatively to determine the spread of ovarian cancer which determines the stage of ovarian cancer the patient has.
• Debulking: The removal of all visible tumor that can be safely removed without damaging major organs.
Epithelial Ovarian Cancer
The Importance of Specialty Care
• % Comprehensive Staging
• 35% General Surgeon • 52% OB/Gyn • 97% Gyn/Onc
• Studies have shown Gynecologic Oncologists have higher rates of complete and “optimal resection” of ovarian cancer at initial surgery and are more likely to perform comprehensive surgical staging as well as provide care that results in 25% improved survival for women as compared to Ob/Gyn and General Surgeons
• Source: Junor et al, Brit J
Ob/Gyn, 11/99 • McGowen et al Ob/Gyn 1985
Epithelial Ovarian Cancer
Epithelial Ovarian Cancer

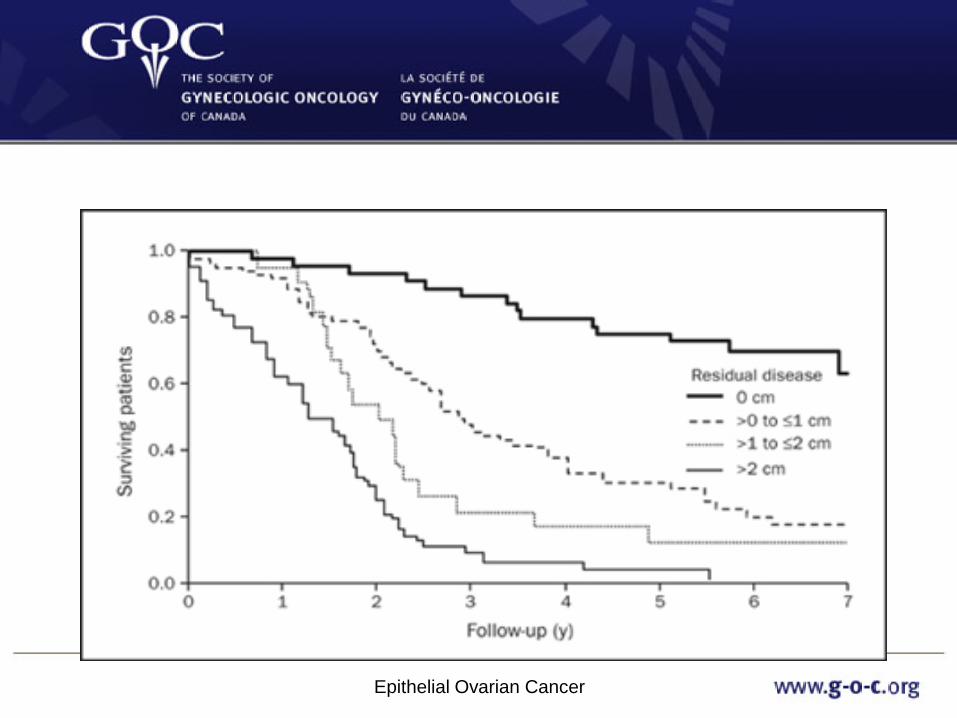
Advanced Disease • Patients with advanced disease can
achieve complete remission – >80% of those who completely respond to chemotherapy
eventually relapse
• 5 year survival is related to volume of residual disease – 40-75% if microscopic (no residual disease) – 30-40% if macroscopic (<1-2cm residual disease) – 5% if suboptimally debulked (>1-2cm)
Bhoola & Hoskins, 2006
FIGO Staging • https://www.sgo.org/wp-
content/uploads/2012/09/FIGO-Ovarian-Cancer-Staging_1.10.14.pdf
Updated FIGO staging Jan 1, 2014

Postoperative care pain management options
PCA Epidural
Grass, 2005

PCA (Patient controlled analgesia) • Infusion pump with opioids available • When patient experiences pain, they can push a
button and PCA will administer controlled amount of opioids intravenously
• Has advantages/disadvantages • Prescriber orders type and dose of opioid, allotting
timing for injection availability and lock out period to prevent over dose or adverse effects (respiratory depression)
• Each institution has it’s own training specific to PCA use

Epidural Pain Management • Analgesia:
– Agents diffuse across meninges & CSF & into neural tissue of cord to act on analgesic receptors of the dorsal horn; systemically by the epidural vasculature & across the dura to penetrate the cord
• Local Anesthetics: – Agent diffuse from epidural space to nerve roots, blocking impulse
conduction – Lower concentrations usually block transmission of pain &
temperature along sensory fibers without blocking the transmission of touch, pressure or motor impulses
• Frequently a combination of opioid and local anesthetic is used, reducing the total amount of each agent required to relieve pain
• Side effects: pruritis, increased susceptibility to UTI, prolonged hospitalization

Chemotherapy • Intravenous chemotherapy with Carboplatin &
Paclitaxel is the standard of practice for epithelial ovarian cancer
• Chemotherapy is given – Cure – Control disease – Palliate symptoms
Epithelial Ovarian Cancer
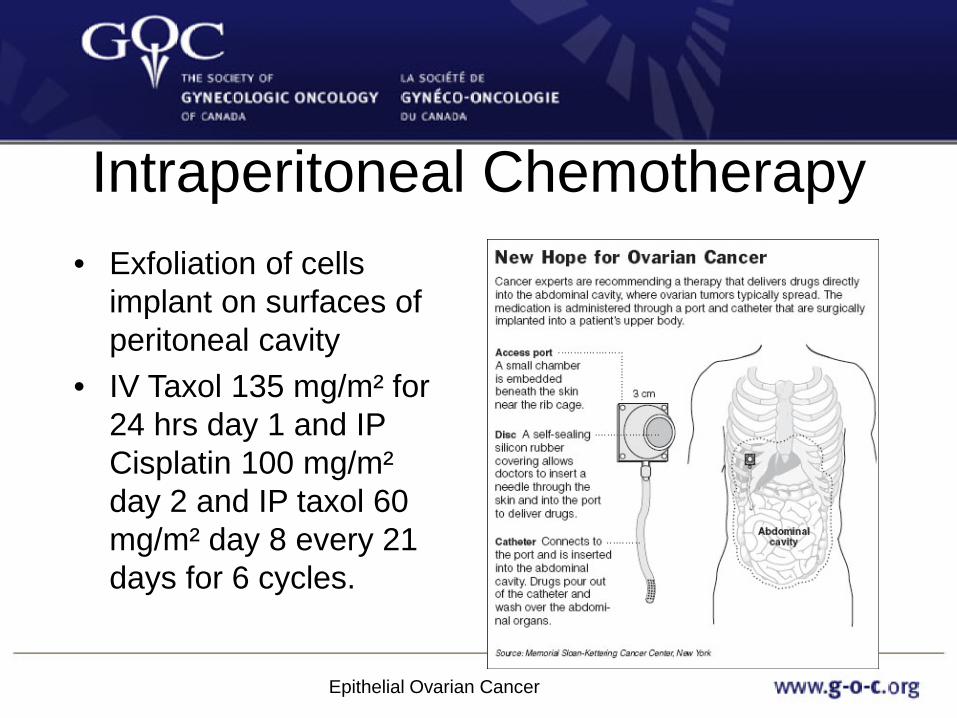
Intraperitoneal Chemotherapy • Exfoliation of cells
implant on surfaces of peritoneal cavity
• IV Taxol 135 mg/m² for 24 hrs day 1 and IP Cisplatin 100 mg/m² day 2 and IP taxol 60 mg/m² day 8 every 21 days for 6 cycles.
Epithelial Ovarian Cancer

Intraperitoneal Chemotherapy
• National Cancer Institute & Gynecologist Oncologist of Canada – IP chemotherapy for patients with newly diagnosed stage III,
optimally debulked ovarian cancer • Armstrong et al. (2006) GOG 172 Clinical Trial
– IP chemotherapy improves progression-free survival (PFS) & overall survival
Ovarian cancer experts: Deborah Armstrong, M.D. & Robert Bristow, M.D.
Epithelial Ovarian Cancer

Improvements in staging, cytoreductive surgery and adjuvent therapies have improved 5 year survival
Epithelial Ovarian Cancer

Paclitaxel • Often given in combination with Carboplatin • Has potential for hypersensitivity reactions, pts need to be premedicated with
steroids • Indicated for patients with ovarian cancers, cervical cancers and endometrial
cancers. • Potential side effects:
– Alopecia -Neutrophil nadir—Day 10-12 – Mucositis -Platelet nadir—Day 8-9 – Myelosuppresion -Cardiovascular—hypotension, bradycardia, – Myalgia, arthralgia hypertension – Peripheral neuropathy -Injection site reactions—erythema, tenderness, – Visual disturbances skin discoloration, swelling—extravasation – Ototoxicity hazard irritant – Diarrhea -Elderly patients have more myelosuppression, – Nausea, vomiting neuropathy and cardiovascular toxicities
Carboplatin • Usually infused over 60 minutes. • Often given in combination with Taxol.
– Taxol should be given before Carboplatin to increase efficiency and limit myelopsuppression.
• Indicated for patients with ovarian cancers, cervical cancers and endometrial cancers.
Side effects: -↓Na, ↓Mg, ↓Ca, ↓K -Vomiting -↑ Creatinine -↑liver function
– Myleosupression (Neutropenia/thrombrocytopenia) – Neuropathies – Ototoxicity – Potential allergic reaction (typically in 2nd line)
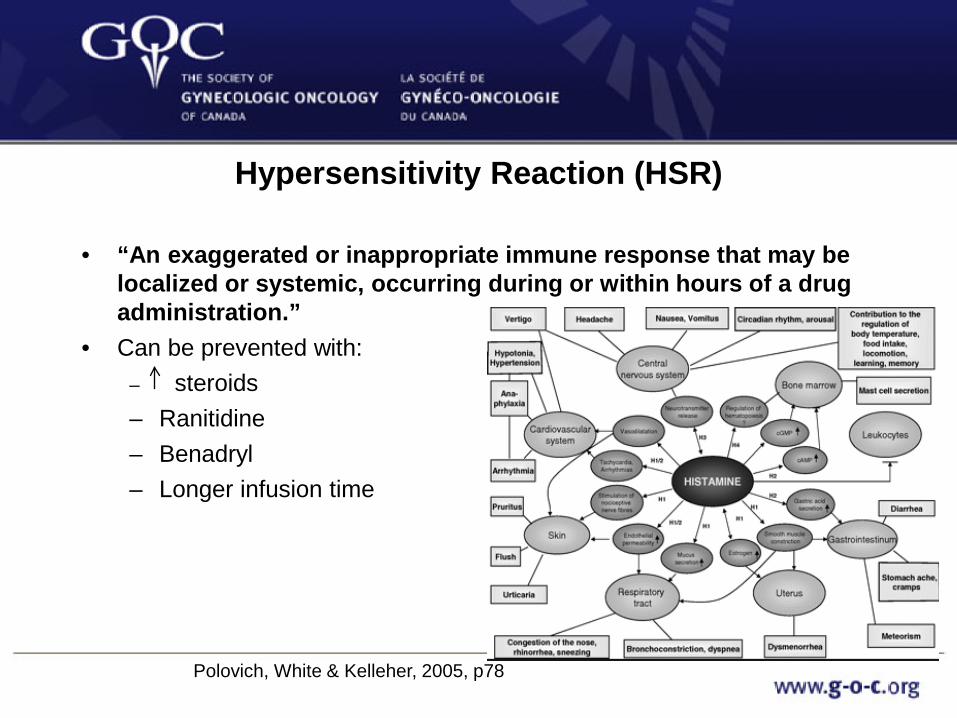
Hypersensitivity Reaction (HSR)
• “An exaggerated or inappropriate immune response that may be localized or systemic, occurring during or within hours of a drug administration.”
• Can be prevented with: – steroids – Ranitidine – Benadryl – Longer infusion time
Polovich, White & Kelleher, 2005, p78
Cisplatin • Pre-treatment hydration VERY important
before Cisplatin. • Compatible with NS (normal saline) Side effects: - Significant nausea and vomiting
– Myelosuppression – Nephrotoxicity – ↓Mg – Neurotoxicity and autotoxicity

Peglated Lipsomal Doxorubicin
• Anthracycline • Molecules of the drug are enclosed (encapsulated) in a fatty coating
known as liposome – The liposome allows the doxorubicin to remain in the body for
longer so that a greater amount of chemotherapy is delivered to the cancer cells, while having fewer side effects on healthy tissue
• Cumulative dose • Sore mouth and ulcers • Skin changes
– Soreness and redness of the palms of hands & soles of feet (PPE—Palmar plantar erythema)
• Cardiomyopathy – Echo or MUGA scan

Topotecan • Used as second line chemotherapy option in platinum sensitive disease • Common side effects:
– Neutropenia, thrombocytopenia, anemia, myelosuppression – Neutrophil nadir—Day 12-15 – Platelet nadir—Day 15 – Neutropenic colitis (typhilits)-life threatening condition, caused by
transmural inflammation of the cecum, ascending colon and ileum—consider if pts present with fever, neutropenia and abdominal pain
– Nausea/vomiting – Diarrhea, constipation – Rash – Alopecia
Gemcitabine • Salvage Therapy for patients with disease recurrence • Side effects:
– Myleosuppressive—leukopenia, anemia, thrombocytopenia – Leg swelling – Pulmonary side effects (pulmonary edema, interstital
pneumonitis, pulmonary fibrosis) – Increased number of visits and infusions (Day 1,8,15 q21
days)
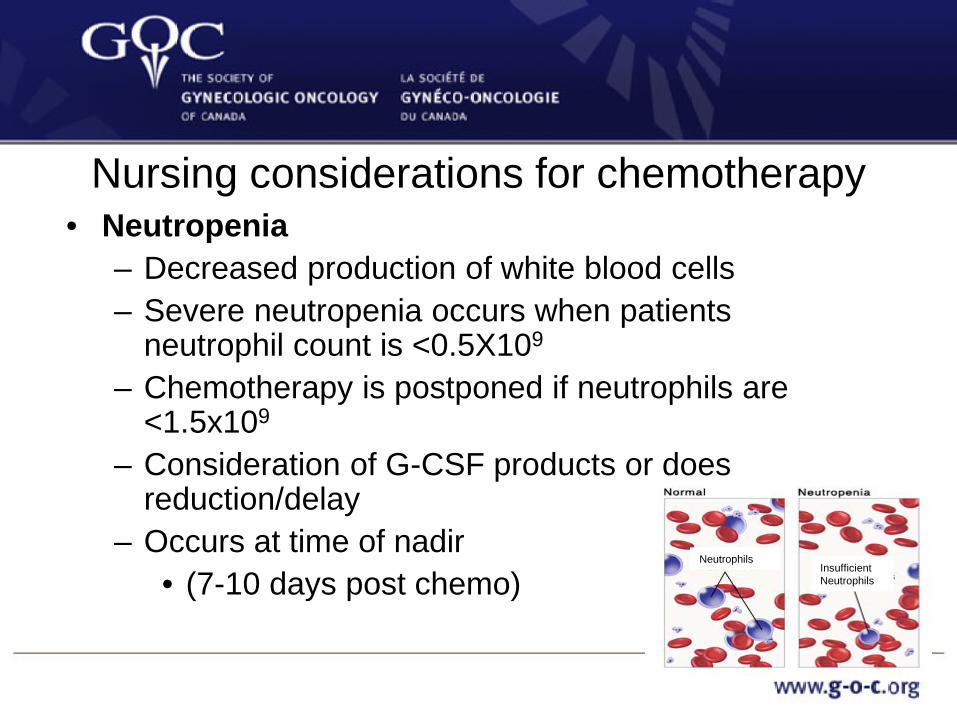
Nursing considerations for chemotherapy • Neutropenia
– Decreased production of white blood cells – Severe neutropenia occurs when patients
neutrophil count is <0.5X109
– Chemotherapy is postponed if neutrophils are <1.5x109
– Consideration of G-CSF products or does reduction/delay
– Occurs at time of nadir • (7-10 days post chemo)
Insufficient Neutrophils
Neutrophils
Nursing considerations for chemo administration
• Neutrophils must be > 1.5 x109 to proceed with chemo
• Neutrophil count < 1.0- 1.4 x109 --Individualized consideration by physician/centre policy about administration
• Neutrophil count < 1.0 x109 , chemo delayed

Nursing considerations for chemotherapy
• Anemia – Low red blood cell count – Normal Hgb 120-160 g/dL – Chemotherapy can still be given if patient anemic and
patient is asymptomatic – Blood transfusion if symptomatic
• SOB • Extreme fatigue • Heart palpitations/vertigo
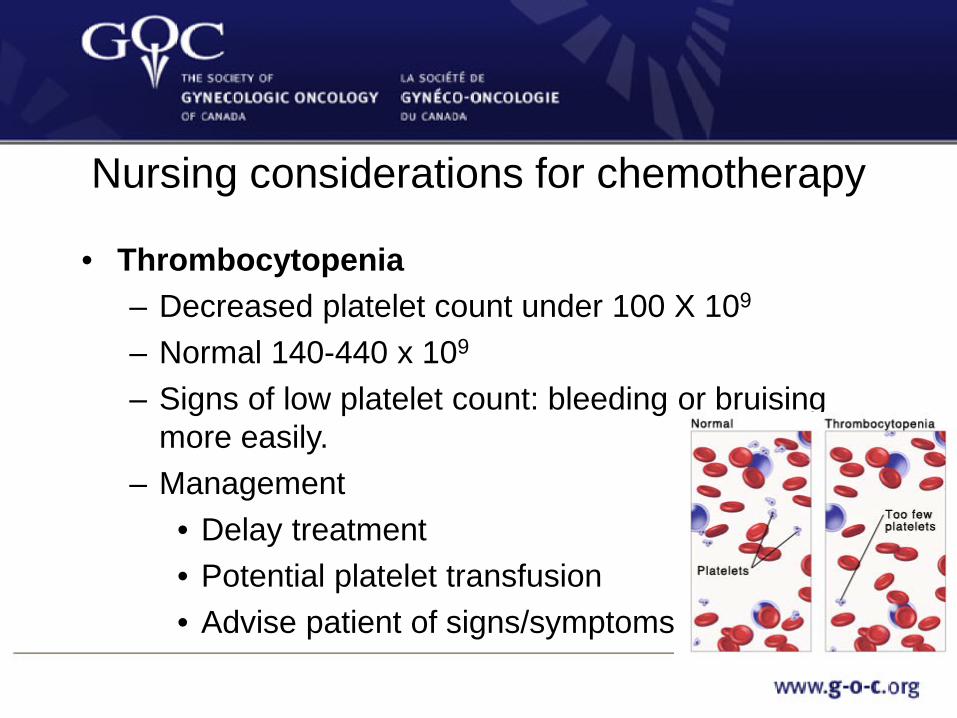
Nursing considerations for chemotherapy
• Thrombocytopenia – Decreased platelet count under 100 X 109
– Normal 140-440 x 109
– Signs of low platelet count: bleeding or bruising more easily.
– Management • Delay treatment • Potential platelet transfusion • Advise patient of signs/symptoms

Nausea & Vomiting
https://www.cancercare.on.ca/CCO_DrugFormulary/Pages/FileContent.aspx?fileId=97473

Taste Changes & Nutritional Alterations
• Chemotherapy drugs most commonly associated with taste changes include – Carboplatin – Cisplatin – Paclitaxel
• Loss of appetite • Mouth care • Mucosal inflammation • Eating takes effort • Consider switching to plastic
cutlery (Metal Taste) • Cachexia
– A state of malnutrition & protein (muscle) wasting
https://www.cancercare.on.ca/CCO_DrugFormulary/Pages/FileContent.aspx?fileId=154808

Mucositis (stomatitis) • Mouth sores--Causes swelling, pain, leads to
malnutrition and dehydration. • Patient could obtain a prescription for magic
mouthwash
https://www.cancercare.on.ca/CCO_DrugFormulary/Pages/FileContent.aspx?fileId=154819

Peripheral Neuropathy • Any injury, inflammation, or degeneration of the peripheral nerves
(Almadrones, Armstrong, Gilbert & Schwartz, 2002) • Many contributing factors • Taxanes & Platinum analogs
– PN enhanced by other factors, including cumulative dose, rapid infusion times, high single dose, & prior or concurrent use of other neurotoxic drugs or agents
– Incidence estimated at 3-7% single agent & up to 38% with multiple agents
• Quality of Life Issues – Painful (burning, sharp, stabbing, electric), numbness, tingling,
weakness, sensory loss, perception of wearing a sock or glove, muscle weakness & loss of dexterity/coordination
– Strategies to alleviate symptoms & prevent injury

Constipation • Insufficient or irregular evacuation of the bowels • Symptoms: – Anorexia, nausea/vomiting, coliky abdominal pain,
bloating, tenesmus • Encourage patient to: – add fiber to their diet, drink plenty of water, increase
physical activity • Review use and indication of laxatives (stool
softeners, stimulants etc). https://www.cancercare.on.ca/CCO_DrugFormulary/Page
s/FileContent.aspx?fileId=154797

Diarrhea • Excessive and loose bowel movements • Can lead to: – Dehydration – Electrolyte imbalances – Skin breakdown • Management – Drink plenty of water and add electrolyte sports drinks – Eat small frequent meals (BRAT diet) – Avoid foods that are high in fat/fiber – Stop laxatives!

Fatigue • Overwhelming & sustained exhaustion & capacity for physical
and/or mental work • Most common complaint related to:
-cancer itself -dehydration -cancer treatment -environmental -anemia -depression -chronic pain -insufficient sleep or rest -stress -inadequate nutritional
intake
https://www.cancercare.on.ca/cms/one.aspx?portalId=1377&pageId=156541

Anxiety/depression
• Anxiety—a feeling of fear or nervousness • Depression—a serious medical condition where a
person feels sad/hopeless • ESAS and Distress Thermometer given to patients at
each visit. • Refer appropriately to services such as Psychosocial
Oncology
https://www.cancercare.on.ca/cms/one.aspx?portalId=1377&pageId=156540
Hair loss (alopecia) • Complete loss of hair on body including head, eyelashes,
eyebrows, arms, legs, nose etc. • Duration for the length of the treatment. It is not permanent. • Regrowth is usually 2-4 months after chemotherapy • May regrow back slightly different in color and texture. • Look Good Feel better Program and CanSupport
Fertility • Loss of the ability to have children • May be related to the chemotherapy, surgical
procedure, age and general health status. • Important to discuss this with patient as early as
possible and offer appropriate support • Emphasize birth control measures for young women
with functioning ovaries • Consider referral to fertility specialist - http://fertilefuture.ca/
Recurrence • 75% of patients recur (not curable at this point)
• Platinum refractory (progresses on treatment) • Platinum resistant (recurs less than 6 months after completing
prior chemotherapy treatment) • Platinum sensitive ( recurs more than 6 months after completing
prior chemotherapy treatment) • Encourage clinical trials • 2nd line therapies (not curative) Caelyx, gemcitabine, etoposide,
topotecan, taxanes, vinorelbine • Median survial time is 2 years for women with bulky disease to
more than 5 years for those with small volume disease. Fewer than 50% of women survive 5 years after the diagnosis
Epithelial Ovarian Cancer

Carcinomatosis
Epithelial Ovarian Cancer

Specific Issues • Decision to start treatment made on a case
by case basis because no survival advantage to starting chemotherapy when patient is asymptomatic
• Can be viewed more as a chronic illness • May go through repeated cycles of
aggressive chemotherapy with little respite • Symptom management and good palliative
care

Common Symptoms Experienced by Women with Recurrent Ovarian Cancer
• Abdominal Changes (Bowels & Ascites) – Cramping – Bloating – Swelling – Pressure/Heaviness/Tightness – Distended hard abdomen – Constipation – Diarrhea – Indigestion – Nausea
•Bankhead, Kehoe, Austoker, 2005; Fitch, Gray & Franssen, 2000; Fox & Lyon, 2007; Lockwood-Rayermann, 2007

Ascites
• Tumor implants block or impede normal peritoneal lymph flow
• Peritoneal surfaces produce an increased amount of fluid
• Symptoms of early satiety, anorexia, indigestion, decreased bowel motility, constipation and decreased bladder capacity. Abdominal skin becomes taut and shiny

Assessing for Ascites

Treatment for Ascites 2) Non-invasive • Diet:
– Frequent, small meals high protein, low sodium.
– Decrease total fluid volume • Rest (on left side, feet elevated)
– Alleviate pressure on internal organs,
– Improve vascular return from lower extremities
– Facilitate lymphatic flow – Improve diuresis
1) Paracentesis

Pleural Effusion • Flow of pleural fluid form the parietal pleura to
the visceral pleura is impaired. • Carcinomatous involvement of the parietal
and/or visceral pleura, these membranes suffer an inflammatory response and injury with resulting increased output and accumulation of fluid in the pleural space.
• Symptoms shortness of breath, hypoxia, pleuritic chest pain and cough
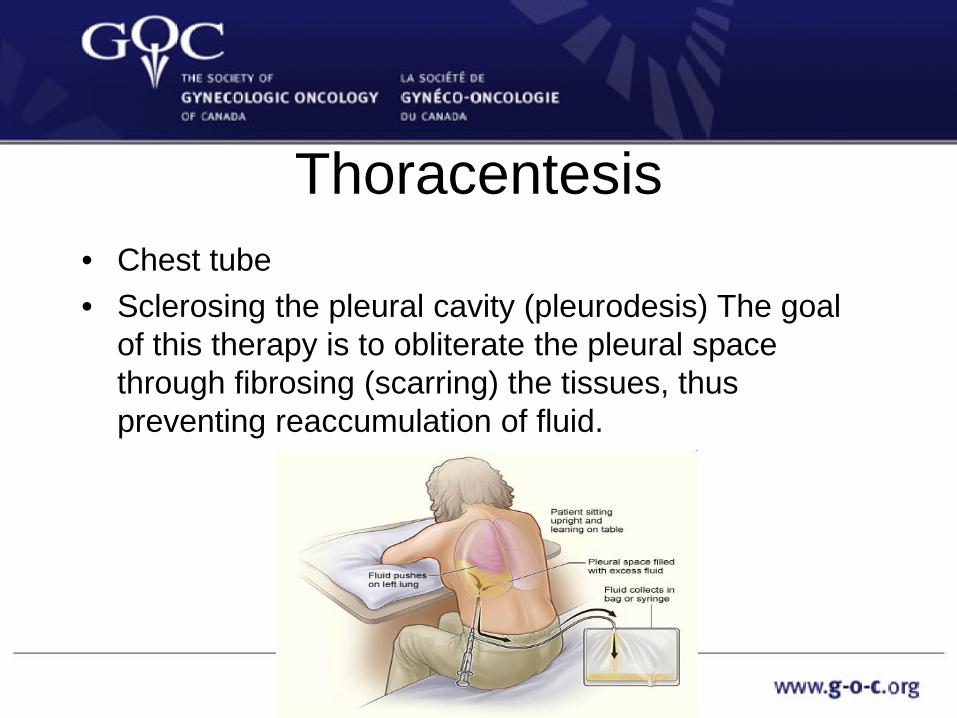
Thoracentesis • Chest tube • Sclerosing the pleural cavity (pleurodesis) The goal
of this therapy is to obliterate the pleural space through fibrosing (scarring) the tissues, thus preventing reaccumulation of fluid.
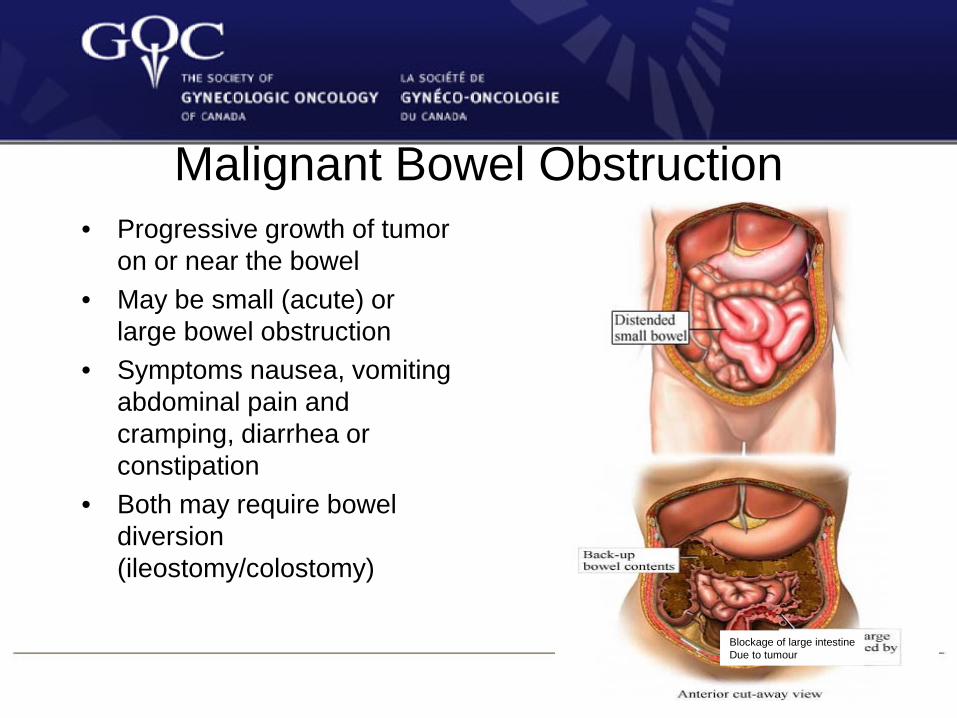
Malignant Bowel Obstruction • Progressive growth of tumor
on or near the bowel • May be small (acute) or
large bowel obstruction • Symptoms nausea, vomiting
abdominal pain and cramping, diarrhea or constipation
• Both may require bowel diversion (ileostomy/colostomy)
Blockage of large intestine Due to tumour

• Overall incidence of MBO with advanced cancer is 3%
• The incidence of MBO in ovarian cancer patients is between 5 to 42%
• Incidence of MBO in GI cancer patients is 4 to 24%
• Other cancers such as breast, lung, or melanoma also have the ability to spread to the abdomen and cause MBO. Incidence for each cancer is not explicitly described in the literature.
MBO - Incidence
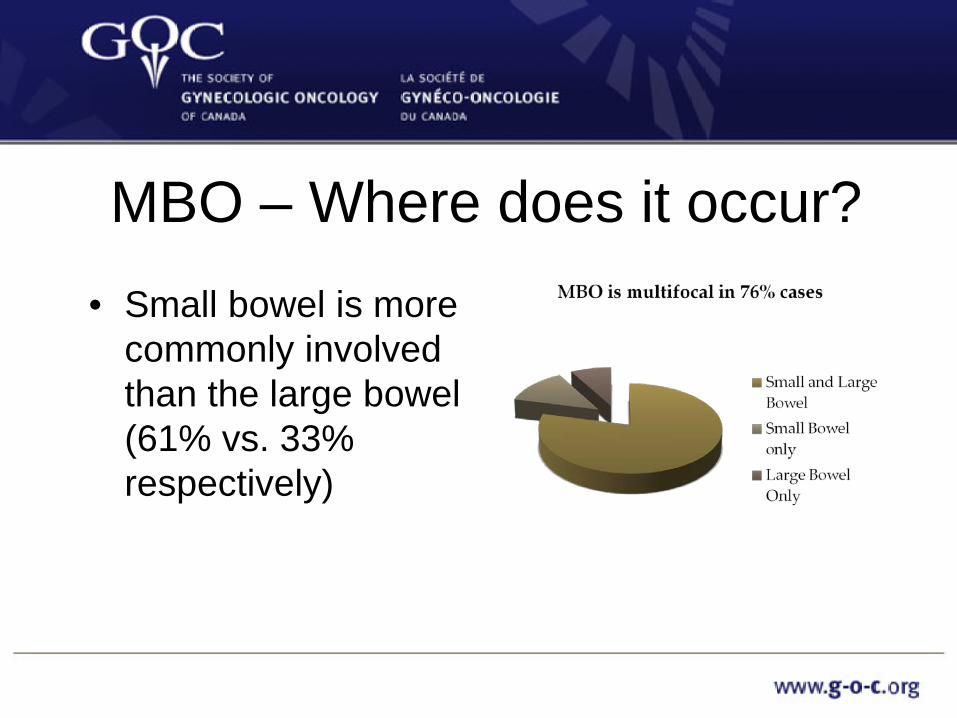
MBO – Where does it occur? • Small bowel is more
commonly involved than the large bowel (61% vs. 33% respectively)

Why is MBO important for Nurses to discuss?
• Physical Symptoms: – Pain (60% of pts.) – Nausea (60 – 70% pts.) – Vomiting – Cramping/borborgami – Change in BM (none or
thin/diarrhea) • Complex management
– Anticipate interventions
• The bigger picture: – MBO can be a terminal
condition – In the setting of
carcinomatosis median survival is < 3months

Pathophysiology of MBO
CONTINUOUS PAIN Exacerbated by tumor
mass
Contributing factors: •Bowel edema •Fecal impaction •Constipating drugs •Hypokalemia
NAUSEA & VOMITING Ripamonti 2007

Signs and Symptoms of MBO
Most common symptoms experienced by patients with MBO:
• Intestinal colic 72-76%
• Abdominal pain 92% • Vomiting 68-100%

Consequences of Bowel obstruction
• Metabolic disorders/malnutrition • Renal failure • Electrolyte instability • Strangulation/perforation of the bowel • Compromised mucosal blood flow with
potential for translocation of endotoxins across the bowel wall
Management: ACUTE • NPO • Hydration (IV fluids or SC) • NG tube
TPN – only considered in patients who would have a clinical or life-extending benefit - it is not
recommended for terminally ill patients

• Goal: relieve symptoms of nausea, vomiting, pain and dehydration – Try to reverse bowel
obstruction
Important to differentiate between partial and complete obstruction as prokinetic agents are inappropriate in complete bowel obstruction
Parenteral routes must be
used as absorption orally is variable and not predictable

Symptom control: Pain in MBO Analgesics should not
be avoided for fear of aggravating the obstruction
Choice of medication and dosage are titrated based on effect
If colicky pain persists despite the use of an opioid, Buscopan may be a useful adjuvant
1. Non-opioid +/- Adjuvant
Analgesics: WHO GUIDELINES

Surgical management • Surgery is considered
for unifocal bowel obstruction and each patient should be evaluated to see if they are a surgical candidate
• Purpose: palliate symptoms of obstruction by: – stoma formation, – bypassing the obstruction – resecting a portion of
bowel – placement of colorectal
stent • Post-op morbidity 5 – 90% • Post-op mortality
Surgical management • Surgical complications include:
• Entero-cutaneous or entero-vaginal fistula
• Anastomosis leaks • Short bowel syndrome • DVT/PE • GI Bleed • Sepsis
• Suitability for surgery should be assessed to justify any surgical intervention – this includes assessing the general condition of the patient, evidence of mechanical obstruction, reasonable expectation of survival and quality of life. (Alberta Cancer Board, 2001, p. 46).
Guidelines to direct which patients with MBO are surgical candidates are not clear
Parameters suggesting surgery is inadvisable include: ascites ≥ 3 L, a palpable abdominal mass, pre-operative weight loss >9 kg, carcinomatosis, previous RT
Rate of inoperable cases in patients with MBO is 6.2% to 50%

Percutaneous Endoscopic Gastrostomy (PEG) Tube
• An alternative to NGT in patients whose symptoms are refractory to pharmacologic measures
• Achieves intestinal decompression
• Complications from PEG tubes include tube obstruction requiring replacement, digestion of surrounding skin, abscess formation, pain when the tube is inadvertently tugged

Nursing Considerations for patients with MBO
Nursing care for the Whole person
• Inability to eat • Alteration in activity • Deterioration of mental abilities • Social isolation • Waiting • Lack of direction • Personal reflection
Every patient indicated that nursing staff could be
a major source of support- providing an
opportunity to reflect on their situation and
meaning of the illness.

Radiation Therapy • The use of high-energy x-rays to destroy cancer cells • May be used to relieve side effects of progressive cancer in select
cases (isolated pelvic/vaginal vault recurrence) • Side effects of treatment
– Fatigue – Mild skin reactions – Nausea – Diarrhea – Cystitis – Vaginal stenosis – Skin integrity

Clinical Trials • Provide novel treatments that show promise
in treatment of ovarian cancer • Available clinical trials should always be
presented as an option to eligible patients

Nursing Management • Therapeutic Communication
– Attentive Listening • Understanding of disease process—from diagnosis to palliation • Be sensitive to patient changes • Encourage your patient and/or family to express their feelings • Promote a therapeutic environment • Assist in adapting to new body changes • Collaborate with other professionals • Care for the “Caregiver”
References Alberts,D.S. & Delforge, A (2006). Maximizing the delivery of intraperitoneal therapy while minimizing drug
toxicity and maintaining quality of life. Seminars in Oncology, 33 (Supp 12), S8-S17.
Alhayki, M., Hopkins, L., & Le, T. (2006). Intraperitoneal chemotherapy for epithelial ovarian cancer. Obstetrics and Gynecological Survey, 61, 8, 529-534.
Almadrones, L (2007). Evidence-based research for intraperitoneal chemotherapy in epithelial ovarian cancer. Clinical Journal of Oncology nursing, 11, 2, 211-216.
Almadrones, L., Flaherty, A.M., & Hydzik, C. (2005). Your guige to intraperitoneal therapy Memorial Sloan-Kettering Cancer Centre, New York.
Almadrnes-Cassidy, L. (ed) (2010). Site specific cancer series: Gynecolgoic cancers. Pittsburg, ONS Publishing.
Armstrong, D.K., Bundy, G., Wenzel, L., Huang, H.Q., Baergan, R., Lele, S., Gynecologic Oncology Group. (2006). Intraperitoneal Cisplatin and Paclitaxel in ovarian cancer. New England Journal of Medicine, 354, 34-43.
Arcangelo, V.P. & Peterson, A.M. (2006) Pharmacotherapeutics for Advanced Practice (2nd ed.). New York: Lippincott, Williams & Wilkins.
Barakat, R. R., Bevers, M.W., Gershenson, D.M. & Hoskins, W.J. (eds) (2000). Handbook of Gynecologic Oncology. MD Anderson Cancer Center & Memorial Sloan-Kettering Cancer Center. London, Martin Dunitz Publishers, Ltd.
Berek, J.S. & Hacker, N.F. (2000). Practical Gynecologic Oncology, 3rd ed. Philadelphia, Lippincott,Williams & Wilkins.
References Bhoola, S. & Hoskins, W.J. (2006). Diagnosis and Management of Epithelial Ovarian Cancer. Obstetrics &
Gynecology, 107, 1399-1410.
Bajway, Z.H. & Smith, H.S. (2011). Overview of the treatment of chronic pain. Retrieved October 15, 2011 from http://www.uptodate.com.myaccess.library.utoronto.ca/contents/overview-of-the-treatment-of-chronic-pain?source=search_result&search=chronic+pain&selectedTitle=1~150.
Bankhead, C.R., Kehoe, S.T. & Austoker, J. (2005). BJOG: an International Journal of Obstetrics and Gynaecology, 112, 857-865. DOI: 10.1111/j.1471-0528.2005.00572.x
Baumann, T.J., Strickland, J.M. & Herndon, C.M. (2011) Pain Management. In J.T. Dipiro, R.L. Talbert, G.C. Yee, G.R. Matzke, B.G. Wells, & M. Posey (Eds.), Pharmacotherapy: A pathophysiologic approach 8th edition (pp. 989-1003). China: McGraw-Hill Companies Inc.
Cannistra, SA. (2006). Intraperitoneal chemotherapy comes of age. The New England Journal of Medicine, 354, 1, 77-79.
Clermont, S. (2007). Intraperitoneal (IP) chemotherapy administration self-learning package, 2nd revision. The Ottawa Hospital, Ottawa.
Daz, J. J et al. (2008). Guidelines for management of small bowel obstruction. Journal of Trauma 64(6) 1651 – 1664.
Decker, G.M., Lee, C.O. (2010). Handbook of integrative oncology nursing: Evidence-based practice. Pittsburg: Oncology nursing society.

References Dedrick, R.L., Myers, C.E., Bungay, P.M., & DeVita, V.T., Jr. (1978). Pharmacokinetic rationale for peritoneal
drug administration in the treatment of ovarian cancer. Cancer Treatment Reports, 62, 1, 1-11.
Donovan, H.S., Hartenbach, E.M. & Method, M.W. (2005). Patient-provider communication and perceived control for women experiencing multiple symptoms assoicated with ovarian cancer. Gynecologic Oncologic, 99, 2, 404-411.
Elit, L., Oliver, TK., Covens, A., Kwon, J. Fung, MF., Hirte, HW., & Oza, AM. (2007). Intraperitoneal chemotherapy in the first-line treatment of women with stage III epithelial ovarian cancer: a systematic review with metaanalyses. Cancer, 109, 4, 692-702.
Elit, L., Oliver, TK., Covens, A., Kwon, J. Fung, MF., Hirte, HW., & Oza, AM. And the Gynecology Cancer Disease Site Group. (2006). The role of intraperitoneal chemotherapy in the first-line treatment of women with stage III epithelial ovarian cancer: a clinical practice guideline. Cancer Care Ontario, July 5, 2006.
Fitch, M., Gray, R.E. & Franssen, E. (2000). Women’s perspectives regarding the impact of ovarian cancer: Implications for nurses. Cancer nursing, 23, 5, 359-366.
Fraser Health (November 2006). Hospice Palliative Care Program Symptom Guidelines:Malignant bowel obstruction. From website: http://www.fraserhealth.ca/media/13FHSymptomGuidelinesMalignantBowelObstruction.pdf visited June 5, 2011.
Fujiwara, K., Armstrong, D., Morgan, M., & Markman, M. (2007). Principles and practice of intraperitoneal chemotherapy for ovarian cancer. International journal of gynecological cancer, 17, 1, 1-20.

References
Fung-Kee-Fung, M., Provencher, D., Rosen, B., Hoskins, P., Rambout, L., Oliver, T., W. Gotlief, Covens, A. et. al. (2007). Intraperitoneal chemotherapy for patients with advanced ovarian cancer: A review of the evidence and standards for the delivery of care. Gynecology Oncology, 105, 3, 747-756.
Gillis, T.A. (2003). Rehabilitation Medicine Interventions. In E. Bruera & Potenay (Eds.), Cancer pain: Assessment and management (pp. 238-326). Cambridge: Cambridge University Press.
Gilron, I., Bailey, J. M., Tu, D., Holden, R. R., Weaver, D. F., & Houlden, R. I. (2005). Morphine, gabapentin or their combination for neuropathic pain. New England Journal of Medicine, 352: 1324-1334.
Gilron, I., Watson, C.P.N., Cahill, C.M., & Moulin, D.E. (2006). Neuropathic pain: A practical guide for the clinician. Canadian Medical Association Journal, 175(3), 265-275.
Gordon, D.B., Dahl, J.L., Miaskowski, C., McCarberg, B., Todd, K.H., Paice, JA., et al. (2005). American Pain Society recommendations for improving the quality of acute and cancer pain management. Archives of Internal Medicine, 165, 1574-1580.
Grossman, P., Niemann, L., Schmidt, S., & Walach, H. (2004). Mindfulness-based stress reduction and health benefits: A meta-analysis. Journal of Psychosomatic Research, 57(1), 35-43.

References Graham, I. & Logan, J. (2004). Innovations in knowledge transfer and continuity of care. Canadian Journal of
Nursing Research, 36, 2, 89-103.
Grass, J.A. (2005). Patient-Controlled Analgesia. Anesthesia & Analgesia, 101, S44-S61.
Gwilliam, B. & Bailey, C. (October 2001). The nature of terminal malignant bowel obstruction and its impact on patients with advanced cancer. International Journal of Palliative Nursing 4(2) 474 – 476, 478 – 481.
Hamilton, CA. & Berek, JS. (2006). Intraperitoneal chemotherapy for ovarian cancer. Current opinion in oncology, 18, 507-515.
Hart, J. (2008). Complementary therapies for chronic pain management. Alternative & Complementary Therapies, April, 64-68.
Houldin, A.D. (2007). A qualitative study of caregivers’ experiences with newly diagnosed advanced colorectal cancer. Oncology nursing forum, 34, 2, 323
Kemp, C. (1999). Terminal illness: A guide to nursing care (2nd ed.). Philadelphia: Lippincott.
Kim, H.S., Fish, D.E., & Choi, H. (2011). Pain medicine: Pocketpedia. Philadelphia: Wolters Kluwer/Lippincott Williams & Wilkins.
Kucukmetin, A., Naik,R., Galaal, B.A. & Dickinson, H. (2010). Palliative surgery versus medical management for bowel obstruction in ovarian cancer,(Review). The Cochrane Library 7. From website: www.thecochranelibrary.com, visited April 10, 2011.

References Lee, M. (2007). Intraperitoneal chemotherapy: Trials & Triumphs. Grand Rounds PowerPoint Presentation,
September 27, 2007.
Lockwood-Rayermann, S. (2007). Lymphedema in gynecologic cancer survivors. Cancer nursing, 30, 4, E11-E18.
Loeser, J., Melzack, R. (1999). Pain: an overview. The Lancet, 353, (9146), 1607-1609.
Lynch, B. & Sarazine, J. (April 2006). A guide to understanding malignant bowel obstruction. International Journal of Palliative Nursing. 12(4)164 – 166.
Makhija, S. (2001). Complications associated with intraperitoneal chemotherapy catheters. Gynecologic Oncology, 81, 71-81.
Markman, M.. (2003). Intraperitoneal antineoplastic drug delivery: Rationale and results. Lancet, 4, 277-283.
Markman, M., & Walker, J. L.,(2006), Intraperitoneal chemotherapy for ovarian cancer: A review with a focus on practical aspects of treatment. Journal of Clinical Oncology, 24, 6, 988-994.
Martin, VR. (2006). Shining a light on ovarian cancer, the hidden tumor. Nursing made incredibly easy, November/December, 28-37.
Martin, VR. (2007). Ovarian cancer: An overview of treatment options. Clinical journal of oncology nursing, 11, 2, 201-207.
Mattson Porth, C. (2002). Pathophysiology Concepts of Altered Health States (6th ed). Philadelphia, PA: Lippincott.

References McCaffery, M. & Pasero, C. (1999). Practical non-drug approaches to pain. In M. McCaffery & C. Pasero. Pain:
Clinical manual, 2nd Ed. (406-421). Mosby, Inc. St. Lewis, Missouri. Ontario Cancer Symptom Management Collaborative. (2010). Cancer Care Ontario’s Symptom Management Guides-to-Practice: Pain. Cancer Care Ontario, August Retrieved on November 10, 2011 from https://www.cancercare.on.ca.
Moulin, D.E., Clark, A.J., Gilron, I., Ware, M.A., Watson, C.P.N., Sessle, B.J., et al. (2007). Pharmacological management of chronic neuropathic pain – consensus statement and guidelines from Canadian Pain Society. Pain Research and Management, 12(1), 13-21.
Munir, M.A., Enany, N., & Zhang, J. M. (2007). Nonopioid analgesics. Medical Clinics of North America, 91(1), 97-111.
National Cancer Institute. (2006). NCI announcement on intraperitoneal cancer therapy for ovarian cancer. Retrieved October 5, 2007, from http://www.cancer.gov/clinicaltrials/results/ovarian-meta-analysis1206
NCCAM. (2011) Herbs at a glance. Retrieved October 14, 2011 from http://nccam.nih.gov/health/herbsataglance.htm
Otto, S.E. (2001). Oncology Nursing, 4th Ed. St. Louis, Mosby.
Pasero,C. Management of breakthrough pain in the cancer patient. US Oncological Disease. 2006
Pereira, J. & Bruera, E. (2001). Alberta Hospice Palliative Care Resource Manual (2nd ed). From website: www.palliative.org visited June 5, 2011.
Platt, V. (November 2001). Malignant bowel obstruction: So much more than symptomcontrol. International Journal of Palliative Nursing 7(11) 547 – 554.

References Potter, K. & Held-Warmkessel, J. (2008). Intraperitoneal chemotherapy for women with ovarian cancer. Clinical
journal of oncology nursing, 12, 2, 265-271.
Pratt, RR. (2004). Art, dance, and music therapy. Physical Medicine and Rehabilitation Clinics of North America, 15, 827-841.
Rang, H. P., Dale, M. M., Ritter, J. M. & Flowers, R. J. (2007). Pharmacology (6th ed). Philadelphia, PA: Churchill Livingstone Elsevier.
Ripamonti, C. I. (2007). Palliative medical management of malignant bowel obstruction. American Society of Clinical Oncology. From website: http://www.asco.org/ascov2/Home/Education%20&%20Training/Educational%2 0Book/PDF%20Files/2007/07patient07.pdf visited May 20, 2011.
Schumacher, K.L., Stewart, B.J., Archbold, P.G., Caparro, M., Mutale, F. & Agrawal, S. (2008). Effects of caregiving demand, mutuality, and preparedness on family caregiving outcomes during cancer treatment. Oncology nursing forum, 35, 1, 49-56.
Selby, D., Wright, F., Stilos, K., Daines, P., Moravan, V., Gill, A. Chakraborty, A. (2010). Room for improvement? A quality-of-life assessment in patients with malignant bowel obstruction. Palliative Medicine 24(1) 38 – 45.
References Sherman, C. (2010). Managing adult cancer pain: The latest NCCN guidelines. Oncology Nurse Advisor.
Retrieved on October 14, 2012 from: http://www.oncologynurseadvisor.com/managing-adult-cancer-pain-the-latest-nccn-guidelines/article/171563/
Singhal, P. & Lele, S. (2006). Intraperitoneal chemotherapy for ovarian cancer: Where are we now? Journal of the national comprehensive cancer network, 4, 9, 941-946.
Sobo, E.J., Eng, B. & Kassity-Krich, N. (2006). Canine visitation (pet) therapy. Journal of holistic nursing, 24 (1), 51-57.
The Society of Gynecologic Oncologists of Canada. (2006). Intraperitoneal chemotherapy for ovarian cancer: A complex strategy but what an exciting avenue! Retrieved October 5, 2007 from http://gog.org/ipchemoed/GOCPositionStmt.PDF
Turner, J., Cummin, T., Bennet, A., Swift, G. & Green, J. (December 2008). Stents and stentability: treatment for malignant bowel obstruction. British Journal of Hospital Medicine. 69(12) 676 – 680.
Vergote, I., Amant, F., & Leunen, K., (2010). Neoadjuvant Chemotherapy in Advanced Ovarian Cancer: What kind of evidence Is needed to convince US gynaecological oncologists? Gynecologic Oncology, 119 (1): 1-2.
Vergote, I., & Trope, C.G., et al, (2010). Neoadjuvant Chemotherapy or Primary Surgery in Stage IIIC or IV Ovarian Cancer, New England Journal of Medicine, 363:10, 943-953.

References
Vermorken, JB. (2006). Intraperitoneal chemotherapy in advanced ovarian cancer: recognition at last. Annals of oncology, 17 (Supplement 10), 241-246.
Walker, JL., Armstrong, DK., Huang, HQ., Fowler, J., Webster, K., Burger, RA., & Clarke-Person, D. (2006). Intraperitoneal catheter outcomes in a phase III trial of intravenous versus intraperitoneal chemotherapy in optimal stage III ovarian and primary peritoneal cancer: A Gynecologic Oncology Group study. Gynecologic Oncology, 100, 27-32.
Ware, M.A. (2011). Complementary and alternative medicines. In M.E. Lynch, K.D. Craig & P.W.H. Peng (Eds.), Clinical pain management: A practical guide (pp. 215-223). Malaysia: Wiley Blackwell.
World Health Organization. (2011). WHO’s pain ladder. Retrieved October 15, 2011 from http://www.who.int/cancer/palliative/painladder/en/
Yarbro, C. H., Frogge, M. H., Goodman, M. (2005). Cancer nursing principles and practice (6th ed). Mississauga, ON: Jones and Barlett.

















![Molecular Mechanisms of PARP Inhibitors in BRCA-related ... · cancer and up to a 54% for ovarian cancer), and other cancer types as pancreatic and prostate [12-15]. About 10-15%](https://img.dokumen.tips/doc/110x75/5f024f757e708231d403a2ca/molecular-mechanisms-of-parp-inhibitors-in-brca-related-cancer-and-up-to-a-54.jpg)












