Embed Size (px)
Citation preview
OUTCOME AFTER TRANSSPHENOIDAL SURGERY FOR PITUITARY ADENOMA -
THE 2000-2010 HELSINKI UNIVERSITY HOSPITAL COHORT
Atte Karppinen
Departments of Neurosurgery and Endocrinology Helsinki University Hospital, Helsinki, Finland
and
University of Helsinki, Faculty of Medicine, Helsinki, Finland
ACADEMIC DISSERTATION
To be publicly discussed, with permission of
the Faculty of Medicine of the University of Helsinki, in Lecture Hall 1 of Töölö Hospital
on November 27th, 2015, at 12 noon.
Helsinki 2015
ISBN 978-951-51-1547-8 (pbk.) ISBN 978-951-51-1548-5 (PDF) Hansaprint Vantaa, Finland 2015
Supervisors Acting Professor Mika Niemelä Department of Neurosurgery Helsinki University Hospital Helsinki, Finland
Associate Professor Camilla Schalin-Jäntti Department of Endocrinology Helsinki University Hospital Helsinki, Finland
Reviewers Associate Professor Ville Vuorinen
Department of Neurosurgery Turku University Hospital Turku, Finland
Professor Pia Jaatinen University of Tampere Tampere, Finland
Opponent Associate Professor Paul A Gardner Department of Neurological Surgery University of Pittsburgh Pittsburgh, Pennsylvania, USA
Custos Acting Professor Mika Niemelä
Department of Neurosurgery Helsinki University Hospital Helsinki, Finland
To my darlings
Author’s contact information: Atte Karppinen Department of Neurosurgery Helsinki University Hospital Topeliuksenkatu 5 00260 Helsinki, Finland Mobile: + 358 50 427 2522 Fax: + 358 9 471 87560 Email: [email protected]
Abstract
Background and Objectives Pituitary adenomas are the most common tumors of the sella turcica. Incidental small pituitary adenomas are very common and seen in up to one-fifth of magnetic resonance imaging (MRI) studies. Treatment is based on clinical or biochemical indications. Many pituitary tumors can be left for follow-up, and some adenomas can be controlled with medication. Transsphenoidal surgery is indicated for specific functional and nonfunctional pituitary adenomas. Surgical techniques, hormonal medication, and radiotherapy are constantly evolving. Subsequently, improved tumor control and hormonal balance, contributing to a normal health-related quality of life (HRQoL) may be observed. Our objectives here were to describe the transitional phase from microscopic to endoscopic surgery for nonfunctional pituitary adenomas (NFPAs), and to outline the HRQoL and its determinants after treatment of different pituitary adenomas in a recent cohort from a single pituitary center. Materials and Methods We retrospectively collected the relevant data for a total of 320 patients who had undergone primary surgery for a newly diagnosed pituitary adenoma during 2000-2010 at Helsinki University Hospital. The first part of our study included 185 consecutive patients who had transsphenoidal surgery for NFPA. These patients were divided into two groups based on the surgical approach: microscopic (n=144) and endoscopic (n=41). Tumor size, location, and cavernous sinus invasion, prevalence of anterior hypopituitarism and diabetes insipidus, visual function, complication rates, and surgical time were compared between the groups. The second part of our study used a cross-sectional design and comprised all pituitary adenoma types. Each patient alive was sent a questionnaire (the 15D) assessing the HRQoL at the beginning of 2013, a mean of 7.4 years after the primary transsphenoidal surgery. One hundred functional pituitary adenoma (FPA) and 137 NFPA patients responded (response rate 78% and 74%, respectively). We then compared HRQoL (15D scores) between patients and a large sample of an age- and gender-standardized Finnish general population. Independent factors
influencing the overall HRQoL (mean 15D score) were estimated using multivariate analysis. Results
The effect of NFPA surgery on pituitary function in both surgical groups (microscopic and endoscopic) was neutral as evaluated at the 3-month follow-up; hypopituitarism had improved in 7% and 9% and had worsened in 13% and 9%, respectively. Of the patients, 51% in both groups received replacement therapy. Total tumor removal based on the 3-month follow-up MRI was achieved in 45% and 56% of patients, respectively (p=0.14). Visual fields had normalized or improved in 90% and 88% of patients, respectively (p=0.79). Postoperative cerebrospinal fluid leak appeared in 4% and 2% (p=0.74), and diabetes insipidus (transient or permanent) in 8% and 5% (p=0.54) of cases, respectively. Larger tumor size (p< 0.0005) and endoscopic technique (p=0.03) were independent predictors of increased mean surgical time.
At the time of survey (mean 7.4 years after transsphenoidal surgery), 44% and 62% of the FPA and NFPA patients, respectively, received replacement therapy. Hormonal remission rate of FPAs was 91%. Mean 15D scores were similar in FPA patients and their controls (0.917 vs. 0.922, p=0.568) and near-normal in NFPA patients compared with their controls (0.885 vs. 0.903, p=0.07).
On single dimensions, FPA patients were worse off regarding speech and sexual activity (both p<0.05), and NFPA patients had impaired dimensions of vision and sexual activity (both p<0.0005), more depression and distress (p=0.005 and 0.009, respectively), and less discomfort and symptoms (p=0.19).
Older age, thyroxine substitution and comorbidities were associated with impaired mean 15D score in both FPA and NFPA patients. Cushing’s disease independently predicted compromised mean 15D score. Re-operation and higher body mass index were independent predictors of impaired HRQoL and hydrocortisone and testosterone (males only) substitutions of improved HRQoL in NFPA patients. Radiotherapy had no effect on mean 15D score. Conclusions A good short-term surgical outcome can be achieved during the initial phase of transition from microscopic to endoscopic transsphenoidal surgery for NFPA
patients. Our first endoscopic single-center consecutive case series showed a trend towards improved tumor control but the operative time was longer than with the microscopic technique.
Current multimodal treatment protocols with optimized hormonal replacement therapies enable normal or at least near-normal overall HRQoL to be achieved in the majority of patients with all types of pituitary adenomas. However, patients with Cushing’s disease and NFPA may have clinically and statistically significant impairments of some single dimensions compared with the general population. Comorbidities are strong determinants of compromised overall HRQoL in patients treated for pituitary adenomas.
Tiivistelmä
Tausta ja tarkoitus Aivolisäkeadenooma on tavallisin sellassa eli kallonpohjan turkinsatulassa esiintyvä kasvain. Mahdollisen hormonaalisen aktiivisuuden (erityksen) perusteella aivolisäkeadenoomat jaetaan toimimattomiin ja toimiviin. Prolaktinooma on yleisin toimiva adenooma ja hoidetaan yleensä lääkityksellä. Kasvuhormonin liikaerityksestä johtuva akromegalia ja kortikotropiinin (ACTH) liikaerityksestä johtuva Cushingin tauti ovat seuraavaksi yleisimmät. Pieniä toimimattomia aivolisäkkeen kasvaimia todetaan sattumalöydöksinä jopa viidenneksessä pään magneetti kuvauksista (MK). Aivolisäkeadenoomat jaetaan koon perusteella mikro- (läpimitta <10 mm) ja makroadenoomiin (läpimitta ≥10 mm). Oireettoman aivolisäkeadenooman (esim. toimimaton mikroadenooma) hoidoksi riittää tavallisesti seuranta. Hoitoaiheet perustuvat kliinisiin ja biokemiallisiin löydöksiin. Tietyt aivolisäkeadenoomat poistetaan transsfenoidaalista reittiä tehtävällä leikkauksella. Osa biokemiallisesti aktiivisista kasvaimista hoidetaan lääkityksellä. Toimivat aivolisäkeadenoomat hoidetaan aina. Makroadenooma, joka painaa näköhermo(j)a heikentäen näkökykyä vaatii nopeata kirurgista hoitoa. Makroadenoomat voivat myös heikentää aivolisäkkeen normaalia toimintaa ja aiheuttaa hypopituitarismin. Kaikki aivolisäkehormoniakselit tutkitaan erikseen ja etenkin hypokortisolismin korvaushoidon aloitus on tärkeää. Kirurgiset tekniikat, lääkehoito ja sädehoito ovat jatkuvasti kehittyneet. Siksi aivolisäkeadenoomien hoidon tulosten ja sen myötä myös elämänlaadun voidaan olettaa parantuneen. Tämän tutkimuksen tarkoituksena oli kuvailla siirtymävaihetta mikroskooppisesta leikkaustekniikasta endoskooppiseen tekniikkaan toimimattomien aivolisäkeadenoomien hoidossa. Lisäksi selvitimme terveyteen liittyvää elämänlaatua ja siihen vaikuttavia tekijöitä eri tyyppisten aivolisäkeadenoomien leikkaushoidon jälkeen. Aineisto ja menetelmät Vuosina 2000-2010 Helsingin yliopistollisessa keskussairaalassa leikattiin 320 uutta aivolisäkeadenoomapotilasta, joiden sairauskertomustiedot kerättiin takautuvasti. Ensimmäisessä osatyössä tutkittiin 185 potilasta, jotka leikattiin toimimattoman aivolisäkeadenooman vuoksi transsfenoidaalista reittiä. Potilaat jaettiin kahteen ryhmään leikkaustekniikan perusteella:
mikroskooppinen (n=144) ja endoskooppinen (n=41). Kasvaimen kokoa, sijaintia ja invaasiota sinus cavernosukseen, aivolisäkkeen vajaatoimintaa, näkökykyä, leikkauskomplikaatioita sekä leikkauksen kestoa vertailtiin ryhmien välillä. Toisessa ja kolmannessa osatyössä selvitettiin läpileikkaustutkimuksella eri tyyppisten aivolisäkeadenoomapotilaiden terveyteen liittyvää elämänlaatua 15D mittarilla. Vuoden 2013 alussa, keskimäärin 7.4 vuotta transsfenoidaalisen leikkauksen jälkeen, kaikille elossa oleville potilaille lähetettiin elämänlaatua mittaavat kyselylomakkeet. Kyselyyn vastasi 100 hormonaalisesti toimivan ja 137 toimimattoman aivolisäkeadenooman vuoksi leikattua potilasta (vastanneiden osuudet 78% ja 74%). Näiden potilaiden elämänlaatua (15D arvoja: profiilipisteet ja kokonaisindeksi) verrattiin suureen kaltaistettuun suomalaiseen taustaväestöön. Itsenäisiä elämänlaatua (15D indeksi) selittäviä tekijöitä arvioitiin monimuuttuja-analyysilla. Tulokset Toimimattomien aivolisäkeadenoomien leikkaushoidon vaikutusta arvioitiin seurantakäynnin yhteydessä 3 kuukautta leikkauksen jälkeen. Aivolisäkkeen toiminnan muutokset olivat molemmissa ryhmissä (mikroskooppinen ja endoskooppinen) neutraaleja: hypopituitarismi oli korjaantunut 7%:lla ja 9%:lla ja pahentunut 13%:lla ja 9%:lla vastaavissa ryhmissä. Molempien ryhmien potilaista 51% tarvitsi korvaushoitoa. MK:n perusteella kasvain todettiin kokonaan poistetuksi 45%:lla ja 56%:lla (p=0.14). Näkökentät normalisoituivat tai paranivat 90%:lla ja 88%:lla (p=0.79). Leikkauksen jälkeistä likvorvuotoa todettiin 4%:lla ja 2%:lla (p=0.74) ja diabetes insipidus (ohimenevä tai pysyvä) 8%:lla ja 5%:lla (p=0.54). Kasvaimen suurempi koko (p<0.0005) ja endoskooppinen tekniikka (p=0.03) ennustivat pidempää leikkauksen kestoa. Kyselytutkimuksen ajankohtana (keskimäärin 7.4 vuotta leikkauksen jälkeen) 44% toimivan ja 62% toimimattoman aivolisäkeadenooman vuoksi leikatuista potilaista tarvitsi hormonikorvaushoitoa. Toimivista adenoomista 91% oli hormonaalisessa remissiossa. Keskimääräiset 15D indeksit olivat samankaltaiset toimivan adenooman vuoksi leikatuilla potilailla ja taustaväestöllä (0.917 ja 0.922, p=0.568), ja lähes normaalit toimimattomien adenoomien ryhmässä taustaväestöön nähden (0.885 ja 0.903, p=0.07).
Merkittävimmät heikentyneet elämänlaadun ulottuvuudet toimivien adenoomien ryhmässä olivat puhuminen ja seksuaalisuus (molemmissa p<0.05), ja toimimattomien adenoomien ryhmässä näkökyky ja seksuaalisuus (molemmissa p<0.0005) sekä masennus ja ahdistuneisuus (p=0.005 ja 0.009). Korkeampi ikä, tyroksiini korvaushoito ja oheissairaudet ennustivat heikompaa 15D indeksiä molemmissa ryhmissä (toimivat ja toimimattomat). Toimivien adenoomien ryhmässä Cushingin tauti ennusti huonompaa 15D indeksiä. Toimimattomien adenoomien ryhmässä uusintaleikkaus ja korkeampi painoindeksi (BMI) olivat 15D indeksiä heikentäviä, mutta hydrokortisoni- sekä (miesten) testosteroni korvaushoito 15D indeksiä parantavia ennustetekijöitä. Stereotaktisella sädehoidolla ei ollut vaikutusta 15D indeksiin kummassakaan ryhmässä. Johtopäätökset Toimimattomien aivolisäkekasvainten hyvät leikkaustulokset voitiin säilyttää mikroskooppisesta endoskooppiseen leikkaustekniikkaan tapahtuvan siirtymävaiheen aikana. Endoskooppisesti leikattujen potilaiden ryhmässä oli suuntaus vähäisempään jäännöskasvaimen määrään, mutta leikkausaika oli pidempi verrattuna mikroskooppisesti leikattuun ryhmään. Nykymenetelmin leikatuilla ja hoidetuilla aivolisäkeadenoomapotilailla todettiin lähes normaali elämänlaatu (15D indeksi). Cushingin tauti ja toimimattomat aivolisäkeadenoomat kuitenkin heikensivät joitakin yksittäisiä elämänlaadun ulottuvuuksia taustaväestöön verrattuna. Lisäksi oheissairauksien kertyminen oli merkittävä elämänlaatua (15D indeksi) heikentävä itsenäinen tekijä aivolisäkeadenoomapotilailla.
Contents
Abstract 6
Tiivistelmä 9
Abbreviations 16
List of original publications 18
A. Introduction 19
B. Review of the literature 20
1. Normal pituitary gland and its function 20
2. Pituitary adenomas 21
2.1. Pathobiology and development 21
2.2. Predisposing factors 21
2.3. Incidence and prevalence 22
2.4. Hormonally active pituitary adenomas 23
2.4.1. Prolactinomas 23
2.4.2. Growth hormone-producing adenomas 24
2.4.3. Adrenocorticotropic hormone-producing adenomas 25
2.4.4. Thyroid-stimulating hormone-producing adenomas 27
2.5. Hormonally inactive adenomas 28
3. General principles of evaluation 29
3.1. Pituitary function 30
3.3. Neuro-ophthalmology 30
3.4. Imaging 31
4. Surgical treatment of pituitary adenomas 33
4.1. History and evolution of transsphenoidal surgery 33
4.2. Transsphenoidal approaches 35
4.2.1. Microscopic technique 35
4.2.2. Endoscopic technique 37
4.3. Craniotomy 38
4.4. Intraoperative adjunctive methods 39
5. Radiotherapy 40
6. Outcome after transsphenoidal surgery 41
6.1. Tumor control 41
6.2. Pituitary function 42
6.3. Neuro-ophthalmological function 43
6.4. Complications 43
7. Health-related quality of life after treatment for pituitary adenomas 45
7.1. Measuring health-related quality of life 45
7.2. Health-related quality of life and functional pituitary adenoma 46
7.3. Health-related quality of life and nonfunctional pituitary adenoma 50
8. Multidisciplinary collaboration 52
C. Aims of the study 54
D. Patients and methods 55
1. Patients 55
2. Data collection 55
3. Surgery 56
3.1. Microscopic approach 56
3.2. Endoscopic approach 57
3.3. Postoperative care 57
4. Endocrine assessment and care 58
5. Radiology 58
6. Neuro-ophthalmology 59
7. Histopathology 59
8. Statistical methods 60
9. Ethical aspects 60
E. Results 61
1. Transsphenoidal surgery for nonfunctional pituitary adenomas – outcome after microscopic versus endoscopic resection 61
1.1. Patient and tumor characteristics 61
1.2. Pituitary function 62
1.3. Perioperative findings 64
1.4. Extent of resection 64
1.5. Visual outcome 65
1.6. Operative complications 65
1.7. Long-term tumor control and adjunctive treatment 66
2. Health-related quality of life (15D) after transsphenoidal surgery for pituitary adenomas 67
2.1. Characteristics of the study cohort 67
2.2. 15D and dimension scores compared with the control population 68
2.3. Independent predictors of 15D score 70
F. Discussion 72
1. Transition from microscopic to endoscopic transsphenoidal surgery 72
2. Health-related quality of life (15D) after transsphenoidal surgery for pituitary adenoma 75
3. Limitations of the study 81
G. Conclusions and future prospects 83
Acknowledgments 84
Appendices 86
Appendix 1 86
Appendix 2 90
Appendix 3 95
Appendix 4 96
References 97
16
Abbreviations
AcroQoL Acromegaly Quality of Life Questionnaire ACTH Adrenocorticotropic hormone ADH Antidiuretic hormone AIP Aryl hydrocarbon receptor-interacting protein ANOVA Analysis of variance BMI Body mass index CBTRUS Central Brain Tumor Registry of the United States CD Cushing’s disease CI Confidence interval CIS Checklist individual strength questionnaire CRH Corticotropin-releasing hormone CRT Craniotomy CS Cavernous sinus CSF Cerebrospinal fluid CT Computerized tomography Cushing QoL Cushing Quality of Life Questionnaire DI Diabetes insipidus EuroQoL (EQ-5D) European Quality of Life Scale FIPA Familial isolated pituitary adenoma FPA Functional pituitary adenoma FSH Follicle-stimulating hormone GH Growth hormone GHQ-12/28/30 General Health Questionnaire-12/28/30 GHRH Growth hormone-releasing hormone GWBS General Well-Being Schedule HADS Hospital Anxiety and Depression Scale HRQoL Health-related quality of life HUH Helsinki University Hospital HUSLAB Laboratory of Helsinki University Hospital IGF-1 Insulin-like growth factor 1 IPSS Inferior petrosal sinus sampling LH Luteinizing hormone
17
MEN Multiple endocrine neoplasia MIB-1 Monoclonal antibody MIB-1 MRI Magnetic resonance imaging NFPA Nonfunctional pituitary adenoma NHP Nottingham Health Profile NS Nonsignificant MDI Major Depression Inventory MFI Multi Fatigue Index OGTT Oral glucose tolerance test PA Pituitary adenoma (P)GWBS (Psychological) General Well-Being Schedule PRL Prolactin p53 Tumor suppressor p53 QALY Quality-adjusted life-years RT Radiotherapy SD Standard deviation SE Spin echo SF-20/36/SF-6D Short-Form health survey SIR Standardized incidence ratio SIADH Syndrome of inappropriate secretion of antidiuretic
hormone SSA Somatostatin analog STR Stereotactic radiotherapy TSH Thyroid-stimulating hormone TSS Transsphenoidal surgery Tuebingen CD-25 Tuebingen Cushing’s disease quality of life
inventory WHO World Health Organization WHODASII WHO Disability Assessment Schedule 15D 15D questionnaire
18
List of original publications
This thesis is based on the following original articles, which are referred to in the text by their Roman numerals:
I Karppinen A, Kivipelto L, Vehkavaara S, Ritvonen E, Tikkanen E, Kivisaari R, Hernesniemi J, Setälä K, Schalin-Jäntti C, Niemelä M. Transition from microscopic to endoscopic transsphenoidal surgery for nonfunctional pituitary adenomas. World Neurosurgery 2015 Jul;84(1):48-57.
II Ritvonen E1, Karppinen A1, Sintonen H, Vehkavaara S, Kivipelto L,
Roine RP, Niemelä M, Schalin-Jäntti C. Normal long-term health-related quality of life can be achieved in patients with functional pituitary adenomas having surgery as primary treatment. Clinical Endocrinology 2015 Mar;82(3):412-21.
III Karppinen A, Ritvonen E, Roine RP, Sintonen H, Vehkavaara S,
Kivipelto L, Grossmann A, Niemelä M, Schalin-Jäntti C. Health-related quality of life in patients treated for non-functioning pituitary adenomas during the years 2000-2010. Accepted to Clinical Endocrinology.
These original publications are reproduced with the permission of their copyright holders.
1The authors have contributed equally to this work.

19
A. Introduction
Pituitary adenomas (PAs) are common benign intracranial tumors. According to autopsy and magnetic resonance imaging (MRI) studies, their overall estimated prevalence is 17% (range 1.5%-39%) [1]. The biological and clinical manifestation of PAs is wide, from small, incidental, asymptomatic lesions to giant, invasive, hormone-producing tumors [2]. The objectives of treatment depend on the biochemical and anatomical characteristics of the tumor, but generally include preservation/restoration of pituitary function, decompression of neural structures and prevention of tumor recurrence. Treatment modalities have been constantly evolving, with introduction of new medications for biochemical control of tumors [3, 4], improved optimization of hormonal replacement therapies [5], novel surgical techniques for more efficient tumor removal [6, 7] and targeted methods to deliver radiotherapy [8].
The endoscopic transsphenoidal approach offers some technical advantages over the traditional microscopic approach, but the superiority of one technique over the other in terms of treatment outcome has not been established [9-11]. The trend, however, is strongly towards adopting the endoscopic technique in pituitary centers [12]. In Helsinki University Hospital (HUH) the microscope was replaced with the endoscope in 2008.
We conducted this study to elucidate the effects of operative technical evolution and multiple modern treatment modalities and to delineate the health-related quality of life (HRQoL) after transsphenoidal surgery for PAs in HUH between 2000 and 2010.

20
B. Review of the literature
1. Normal pituitary gland and its function
The pituitary gland is vital for the maintenance of the body’s homeostatic functions of metabolism, growth and reproduction. This pea-sized (averaging 13 x 9 x 6 mm) gland, weighing about 0.5 g, is located at the base of the brain in the sella turcica just above the sphenoid sinus. It can be seen as a protrusion from the bottom of the hypothalamus to which it is connected with a stalk also known as the infundibulum. The pituitary gland consists of anterior and posterior lobes containing the adenohypophysis and neurohypophysis, respectively. A third, intermediate part between the anterior and posterior lobes is not very distinct in humans [13].
The neurohypophysis is an extension of the hypothalamus, and is composed of neuronal processes. Antidiuretic hormone (ADH) is synthesized in the hypothalamus and stored in the neurohypophysis to be released for maintenance of the body’s water balance. Oxytocin, another neurohypophyseal hormone, plays an important role in sexual reproduction, especially during and after labor. Secretion of both neurohypophyseal hormones is under hypothalamic control. They are released to the blood circulation through pituitary vasculature [14].
The adenohypophysis is composed of hormone-secreting adenohypophyseal cells, which are of epithelial origin from the oral ectoderm. The adenohypophysis contains several cell types specific for different adenohypophyseal hormones and their production. Adrenocorticotropin (ACTH) stimulates glucocorticoid production of the adrenal cortex. Growth hormone (GH) regulates muscle and bone growth in adults. Prolactin (PRL) inhibits gonadal function and stimulates breast milk production. Thyroid-stimulating hormone (TSH), also known as thyrotropin, stimulates the thyroid gland to produce thyroid hormones. Gonadotropins (LH and FSH) regulate sex hormone production in gonads and germ-cell development. All (except PRL) of the adenohypophyseal hormones are under dual regulation: hypothalamic hormones and systemic. PRL and GH also have a direct feedback mechanism to the hypothalamus [13].
21
2. Pituitary adenomas
2.1. Pathobiology and development
Pituitary adenomas (PAs) are benign neoplasms consisting of adenohypophyseal cells. They show a wide range of biological behavior in terms of hormone secretion and tumor growth. PAs usually arise in the sella turcica and rarely elsewhere in the proximity of the sella [2]. A pseudocapsule composed of compressed adenohypophyseal tissue surrounds most PAs [15]. PAs are classified as micro- or macroadenomas based on their size (<10 mm or ≥10 mm, respectively). Depending on the cell line, they are further classified as hormonally active or inactive. Their growth rate is variable, but usually slow. The direction of growth is typically upwards into the suprasellar space towards the optic chiasm. Some PAs can invade downwards into the sphenoid sinus or laterally into the cavernous sinus [2, 16].
Most PAs are likely to arise from a genetic event (e.g. inactivation of tumor-suppressor gene), which alters cell proliferation or survival. This mutation allows the adenohypophyseal cell line to become more responsive to hormones or growth factors and ultimately leads to clonal expansion and development of PA [17, 18].
Some PAs have atypical features on immunohistochemical analysis: excessive p53 positivity, high proliferative index (MIB-1 over 3%), and increased mitotic activity. These tumors can be classified as atypical PAs, but their true clinical behavior has not yet been confirmed [19]. Very rarely, pituitary tumors metastasize to distant locations and are then classified as carcinomas [2].
2.2. Predisposing factors
Little is known about environmental factors promoting PA tumorigenesis, but some genetic factors have been found. Multiple endocrine neoplasia type 1 (MEN1) syndrome is a rare autosomal-dominant disorder caused by mutation in the MEN1 gene. This loss of tumor-suppressor gene is associated with a high incidence of PAs in affected patients. However, MEN1 mutations have
22
not been identified in patients with sporadic PA [20]. Other rare genetic syndromes predisposing to PAs are Carney complex and MEN4 [21]
Familial isolated pituitary adenoma (FIPA) is a clinical entity in which pituitary adenomas of all types occur in multiple members of a kindred in the absence of MEN1 [21]. A mutation in the aryl hydrocarbon receptor-interacting protein (AIP) gene is associated with some (15%) FIPA families [21, 22]. The AIP mutation predisposes patients to larger and treatment-resistant PAs (mostly somatropinomas) at an earlier age and may also be found in sporadic cases without FIPA family history [21-23].
2.3. Incidence and prevalence
Pituitary adenomas may be found incidentally on MRI and autopsy with a mean frequency of 22.5% and 14.4%, respectively [1]. Clinically significant PAs are less common, but recent data suggest increased incidences relative to earlier reports [24] [25].
PAs have constituted 14.7% of histologically verified central nervous system tumors in the US tumor registry (CBTRUS 2004-2007). The standardized incidence rate per 100000 (SIR) for PAs was 3.13 [26]. An Austrian registry-based study reported much lower SIR (1.63) for histologically verified PAs [27]. Incidence rates based on tumor specimen may underestimate the true incidence, as many PAs are diagnosed on a radiological and biochemical basis without histological confirmation.
In a Swedish population-based survey performed in 1958-1991, the age-standardized incidence of PA was only 0.6-1.1 cases per 100000 [28]. A more recent population-based retrospective study from Northern Finland included clinically relevant PA cases based on hormonal and radiological studies in 1992-2007. The authors identified 355 patients with freshly diagnosed PA and reported SIR of 3.98 [29]. Another recent study from Sweden, using the same design, reported a very similar SIR (3.9) for 2001-2011 [30]. The most common PA subtypes were prolactinoma and NFPA, combined constituting 86-88% of cases. The higher incidence numbers in cohorts collected after the 1990s can be explained by the more frequent use of high-resolution MRI as a diagnostic tool, resulting in larger numbers of incidental findings.
23
There is a clear rise in PA incidence in older males. This increase is most pronounced in NFPAs, while other subtypes occur at more stable rates over different age groups in males [29, 30]. In females, the PA incidence peaks in young adults (25-34 years), gradually decreasing thereafter. The upswing may be explained by diagnosis of prolactinomas when females reach the reproductive age.
A vast majority of patients harboring PAs are adults, with only 3-6% of cases being under 20 years of age [31]. According to the CBTRUS database, the SIR of pituitary tumors in the US before the age of 20 years is 0.49 cases per 100000.
Two population-based studies from Europe (Belgium and UK) explored the prevalence of clinically relevant PAs [32, 33], reporting a total prevalence of 94.0 and 77.6 per 100000, respectively. This roughly corresponds to one case per 1000 population. Both papers suggested that the most common PA subtype was prolactinoma, a clear majority of which were microadenomas (89%) in female patients (80%). Overall, women harbored PA twice as often as men (ratio 2:1) in both studies.
2.4. Hormonally active pituitary adenomas
2.4.1. Prolactinomas
Prolactinomas are the most common hormone-secreting tumors of the pituitary gland, representing up to 40% of all pituitary tumors. They present as microadenomas in 90% of cases and appear most frequently in females aged between 20 and 50 years; the sex ratio is 10:1 [34, 35]. Premenopausal women typically present with amenorrhea, infertility, and galactorrhea. Diagnosis is based on increased serum prolactin concentrations in the presence of an adenoma observed on MRI, after excluding other causes of raised prolactin levels. Some patients (typically males) may present with visual disturbance and hypopituitarism as a result of mass effect caused by macroprolactinoma.
For asymptomatic microadenomas, follow-up may be sufficient (typically postmenopausal women). The first-line treatment of symptomatic prolactinoma is dopamine agonist - cabergoline is preferred over
24
bromocriptine and quinagolide - which often reverses hyperprolactinemia relatively quickly and relieves eventual symptoms related to mass effect (headache, visual symptoms) often within a few days. After established normalization of prolactin concentrations and near complete tumor disappearance, the medication may be discontinued. Some patients will stay in remission [34, 36].
If dopamine agonist treatment is ineffective (10-20%) or the patient is non-compliant and/or suffers from side-effects (nausea, vomiting, dizziness), surgery maybe indicated. Over 70% of patients operated on for microprolactinoma reach hormonal remission [34, 36]. Macroprolactinomas often have an invasive growth pattern and are therefore more difficult to cure surgically, with remission rates under 40% [34, 36]. Recurrences after initial surgical remission are reported between 0 and 50% of prolactinoma cases, reflecting differences in neurosurgical expertise and patient selection between centers [36]. Radiotherapy has a minor role since medication and/or surgery very often have sufficient efficacy in treatment of prolactinomas.
2.4.2. Growth hormone-producing adenomas
Excessive production of GH leads to acromegaly, which markedly shortens life expectancy if left untreated or poorly controlled [37, 38]. Acromegaly typically presents as an insidious progressive disease with dysmorphic changes (broadened hands and feet, widened nose, and prominent cheekbones and jaw). Other manifestations are cardiovascular (arterial hypertension, cardiomyopathy, valve disease), metabolic (diabetes), sleep apnea, arthropathies, and increased risk for colon cancer [37]. In pediatric patients, excessive GH production leads to gigantism.
The diagnosis is based on typical clinical symptoms and biochemically confirmed increased GH concentration, which is not suppressed following an oral glucose load (oral glucose tolerance test, OGTT) [39]. An increase (relative to the age-adjusted normal range) in the serum concentration of IGF-I, the main GH-dependent growth factor, supports the diagnosis. Mixed GH- and PRL secreting adenomas are relatively common (25%), with clinical behavior similar to acromegaly [37].
25
Treatment of acromegaly aims to eliminate morbidity and reduce mortality to the expected age- and sex-adjusted rates. This is optimally achieved by using safe treatments to remove the mass effect of the tumor and to normalize the GH-IGF-1-axis function. Currently, the first-line treatment of GH-secreting adenoma is surgical removal, ideally with preservation or subsequent restoration of pituitary function [40, 41]. Approximately 80% of patients with microadenomas and less than 50% of patients with macroadenomas can be defined as controlled with transsphenoidal surgery [42, 43]. A small number of patients (less than 5%) develop tumor recurrence, although it is relatively rare compared with other functioning adenomas [44, 45]. If acromegaly is not controlled with surgery alone or surgery is not feasible or contraindicated, patients are offered medical treatments. Radiotherapy is recommended as a third treatment option in case both surgical and medical treatments fail to control the disease [40, 41].
Somatostatin receptor ligands (somatostatin analogs, SSAs, i.e. octreotide and lantreotide) are the primary medical treatment option for acromegaly, although cabergoline might be considered in mild cases [41]. If the response to SSA is not adequate, a switch to pegvisomant (GH-receptor antagonist) treatment or more often combination therapy with SSA and pegvisomant or cabergoline may be considered. Some authors have reported improved surgical remission rates with preoperative SSA treatment [46].
2.4.3. Adrenocorticotropic hormone-producing adenomas
Cushing’s syndrome refers to a condition induced by chronic exposure to excess glucocorticoid. In clinical practice, an iatrogenic source of glucocorticoid surplus (e.g. treatment of inflammatory diseases) is more common than endogenous hypercortisolemia. Cushing’s disease is caused by an ACTH-producing PA and represents 60-70% of endogenous Cushing’s syndromes [47]. Primary adrenocortical tumors and rare ectopic ACTH syndromes are other causes for endogenous hypercortisolemias. Patients affected by Cushing’s syndrome have high morbidity and mortality, and expeditious diagnostics and treatment are thus advisable [47].
Diagnosis of Cushing’s disease is based on serial stepwise investigations, which may be complex and puzzling [48, 49]. The majority of cases are
26
females presenting with microadenoma. The diagnostic work-up from a clinical standpoint comprises symptoms and signs suggestive of hypercortisolemia: cushingoid habitus (central obesity, thinned skin, purple striae, proximal muscle weakness, etc.), fatigue, arterial hypertension, glucose intolerance, menstrual irregularity, acne, and hirsutism. Biochemical diagnostics are preceded by exclusion of exogenous glucocorticoid use, and followed by screening and confirmation of excess glucocorticoid load using dexamethasone suppression test and measurement of 24 h urinary cortisol and late-night salivary cortisol. This is followed by determining whether cortisol production is ACTH-dependent or not (measurement of ACTH concentrations), and finally differentiating between an ectopic ACTH-producing tumor and a pituitary source (i.e. Cushing’s disease) using corticotropin-releasing hormone (CRH) stimulation test [48].
If hypercortisolemia is ACTH-dependent, but clinical, biochemical, and imaging results are discordant, bilateral inferior petrosal sinus sampling of ACTH (IPSS) is usually indicated. The ACTH concentration is then compared between the inferior petrosal sinus and peripheral samples (IPS:P). A central pituitary source for ACTH overproduction can be assumed if the IPS:P ratio is over 2:1 in cases where CRH is not used or if the ratio is over 3:1 after administration of CRH [48]. IPSS has a high (98-99%) positive predictive value, but unfortunately a lower (22-29%) negative predictive value [48, 50, 51].
High-quality pituitary MRI with appropriate imaging sequences is mandatory for detecting small adenomas and to give the neurosurgeon an exact intraoperative roadmap for finding the target [52]. MRI may remain equivocal despite repeated and focused scanning.
The best treatment for Cushing’s disease is transsphenoidal surgery, which is highly effective in expert hands [53]. Surgery should be considered also in cases of ACTH-dependent Cushing’s disease and noncentralized or technically unsuccessful IPSS without evidence of ectopic tumor [51]. Remission rates vary between 65% and 98%, and disease relapse is reported in up to 35% of cases at long-term follow up after transsphenoidal surgery [54].
A special challenge for the pituitary surgeon is an MRI-negative adenoma, which requires careful exploration of the whole pituitary gland in order to find the tiny microadenoma. If the adenoma is not found despite all efforts, the surgeon has to decide whether to proceed with subtotal hypophysectomy or to

27
withdraw and re-evaluate treatment options postoperatively with the whole pituitary team [55, 56].
Unfortunately, drugs available for Cushing’s disease have poor efficacy, and therefore, long-term medical treatment is seldom indicated [53]. Ketoconazole, metyrapone, and mitotane have been used to inhibit the adrenal synthesis of steroids [47]. A pituitary-targeted medication, pasireotide, has been developed, but its high cost and side-effects (e.g. hyperglycemia) limit its use [57]. Generally, drugs may be used as an adjunct in cases where surgery has been unsuccessful or contraindicated and while waiting for response to radiotherapy [53]. Alternatively, bilateral adrenalectomy may be considered when rapid resolution of severe hypercortisolemia is preferred in Cushing’s disease [58].
2.4.4. Thyroid-stimulating hormone-producing adenomas
Thyroid-stimulating hormone-secreting PA is a very rare cause of hyperthyroidism and constitute only 2% of all pituitary tumors [59]. About one-third of TSH-secreting adenomas are plurihormonal, secreting also GH, PRL, or rarely gonadotropins [2]. They usually present as macroadenomas with mass effect on the surrounding structures. Symptoms of hyperthyroidism may be mild and obscured by visual disturbances, hypopituitarism, or secretion of other hormones (plurihormonal adenomas). Goiter is very common, almost a rule, and many patients are misdiagnosed as having primary hyperthyroidism.
Evidence of increased thyroid hormone concentrations in association with measurable TSH concentrations is biochemically characteristic of central hyperthyroidism. Dynamic testing (thyroid hormone suppression test), which is rarely required, differentiates TSH-secreting PAs from the syndromes of thyroid hormone resistance [59, 60].
The treatment of choice for TSH-secreting adenomas is transsphenoidal surgery [60]. These adenomas are often macroadenomas with a hard consistency and invasive growth to parasellar structures, and consequently, hormonal remission is achieved in only in 44-58% of cases with surgery alone [61, 62]. Medical treatment of TSH adenomas is based on administration of

28
long-lasting somatostatin analogues, which are effective in up to 95% of patients [63].
2.5. Hormonally inactive adenomas
Nonfunctional PAs refers to a clinical entity in which symptoms and signs of hormonal hypersecretion are absent in the presence of a pituitary tumor. Subclasses of NFPAs are null cell adenoma and oncocytoma, which have negative hormonal immunostaining [64]. Occasionally, NFPAs present as silent adenomas, which express hormones in immunohistochemistry, but do not secrete them [2].
NFPA is the most common indication for pituitary surgery, constituting about 50% of operated PAs [65]. Mean age at diagnosis is between 50 and 55 years, with slight male preponderance (57%). NFPA typically presents with visual disturbance and/or hypopituitarism related to mass effect of the tumor. Half of the patients have visual deficits on formal neuro-ophthalmological examination and almost 80% have dysfunction of at least one hormonal axis on endocrinological assessment [64]. Since NFPA may go unnoticed for years (even a lifetime) before reaching a symptomatic size, up to 26% of cases are nowadays discovered incidentally on MRI [66]. Occasionally (5-10% of cases), hemorrhagic infarction of the adenoma (apoplexy) may cause a sudden increase in size and pressure of the tumor and subsequently lead to acute severe headache, visual disturbance, and hypopituitarism [64, 67]. However, any PA subtype may present with apoplexy.
Many NFPAs cause mild to moderate hyperprolactinemia by compressing the stalk and inhibiting effects of dopamine on lactotroph cells of adenohypophysis (stalk effect). In clinical practice, NFPAs can usually be distinguished from prolactinomas, which typically produce much higher levels of prolactin with respect to smaller tumor size.
For asymptomatic and small NFPAs, follow-up is usually sufficient. Transsphenoidal surgery is the primary treatment for NFPAs. The most important objective for surgery is reversal of visual deterioration. At the time of surgery, all tumors are macroadenomas, some even giant, making it a challenge for the pituitary surgeon to achieve total excision of the lesion. Reported rates of gross total resection have ranged from 28% to 83% [64].

29
However, tumor control seems to be improving since recent papers have reported complete resections ranging from 56% to 96% [68]. Despite some tumor residuals, the great majority (80%) of patients experience improvements in their visual disturbance, with full normalization in up to 40% [64]. Most studies report postoperative improvements in hypopituitarism. Recurrences after gross total resection are seen on average in 17% (range 0-32%) of cases, and residual tumors progress on average in 43% (range 13-73%) of cases depending on the length of postoperative follow-up (mean range 4-10 years) [64]. NFPAs require extended follow-up of possible hypopituitarism and hormonal substitution, and MRI surveillance should be considered on an individual basis, guided by the possible residue and its estimated growth [69, 70].
Since medical treatment (e.g. dopamine agonists) is inadequate for controlling NFPAs, tumor residuals are, when needed, either re-operated or referred for stereotactic radiotherapy [64]. Treatment decisions are made individually, favoring watchful waiting in cases where the tumor residual is small, asymptomatic, or shows no progression and is situated far away from the optic chiasm [71]. Commonly, radiotherapy stops the tumor growth, but risks the residual function of the pituitary. Modern stereotactic methods of delivering radiotherapy have reduced but not eliminated the harmful effects of ionized radiation [72].
3. General principles of evaluation
Clinical and biochemical assessment of pituitary hormonal function is the cornerstone of evaluating a possible PA. Assessment of visual function by ophthalmological studies and outlining sellar anatomy with radiological studies complete the evaluation. Since diagnostic and treatment guidelines are different for each PA subgroup, an endocrinologist should carefully oversee the stepwise investigations.
30
3.1. Pituitary function
Excess hormonal production and subsequent symptoms and signs are specific for each functional adenoma as already described. The first-line biochemical tests of hormonal overproduction are selected accordingly and often repeated or supplemented to reach diagnosis. Even if the patient presents with neurological symptoms of mass effect with no obvious signs of hormonal overproduction, the possibility of a FPA, especially a prolactinoma, should not be overlooked.
Hypopituitarism is defined as a partial or complete defect in anterior (or posterior) pituitary hormone secretion. It can be secondary to compression of the pituitary gland by the adenoma itself or may develop as a consequence of surgery and/or radiotherapy. In addition, hyperprolactinemia may lead to hypogonadism. The most commonly hypofunctional anterior pituitary axes are adrenal, gonadal, and thyroid. Depending on the degree and number of deficient hormones, the presenting symptoms of hypopituitarism can vary widely, from subtle hypothyroidism to severe hypocortisolism, which may result in shock. ADH deficiency leads to the syndrome of diabetes insipidus (DI), inability to concentrate the urine, leading to polyuria, dehydration, and extreme thirst and polydipsia, as well as hypernatremia. Symptoms and signs secondary to hypopituitarism are reviewed by means of clinical examination and careful history. Each anterior hormonal axis is tested in patients undergoing diagnostic evaluation for PA [5]. Screening is done by measuring basal concentrations of serum cortisol, T4, and in males, testosterone, and in females of reproductive age, also by assessing the menstrual cycle. Mild forms of hypopituitarism may require stimulation testing for proper assessment (e.g. ACTH stimulation for detection of hypocortisolism). Generally, all deficient hormones are replaced.
3.3. Neuro-ophthalmology
Visual disturbances are noted when the PA grows superiorly beyond the sella and compresses optic nerves anteriorly, the optic chiasm centrally, or optic tracts posteriorly. The classic presentation is a slowly progressive bitemporal hemianopia caused by pressure on nasal fibers of the chiasm. Bilateral
31
deterioration of central visual acuity is a relatively insensitive indicator of mass effect and correlates poorly with visual deficit. However, reduced color vision is usually one of the first signs of compressive optic neuropathy [73].
Neuro-ophthalmological assessment is requested in case of visual symptoms or macroadenoma compressing the optic nerve(s) or chiasm. Evaluation includes testing of visual fields and acuity, and auxiliary testing may be helpful in detecting subtle deficits [74].
An abrupt hemorrhage or infarction or both within the pituitary adenoma causes pituitary apoplexy, which usually presents with sudden onset of severe headache and visual disturbance. Besides visual loss, ophthalmologic symptoms often include diplopia due to lateral compression of cranial nerves in the cavernous sinus. Unstable or progressive visual deterioration is an indication for urgent transsphenoidal decompression and tumor removal [67].
3.4. Imaging
Imaging documents the existence of the pituitary lesion, shows its exact location within the gland, and evaluates its size. Imaging does not, however, distinguish one type of adenoma from another. It provides anatomical information about surrounding structures and their involvement. MRI offers soft tissue differentiation, whereas computerized tomography (CT) scanning yields information on the bony structures of paranasal sinuses and the skull base around the sella [75].
The most common MRI technique is a T1-weighted spin echo (SE) sequence obtained in coronal and sagittal planes before and after injection of intravenous contrast media [75]. The post-contrast sequences are the most valuable part of the examination, usually depicting the adenoma as a hypoenhancing lesion surrounded an enhancing normal gland. A very useful sign, supporting the pituitary origin of the tumor, is the demonstration of a connection with the pituitary gland within the sella.
Additional T2-weighted images are usually obtained in coronal and sagittal planes to better outline cystic or calcified areas of the tumor. For neurosurgeons, MRI is invaluable for planning pituitary transsphenoidal surgery. Preoperatively, tumor extensions to supra- and parasellar structures must be carefully reviewed. Position and possible deviation of the pituitary
32
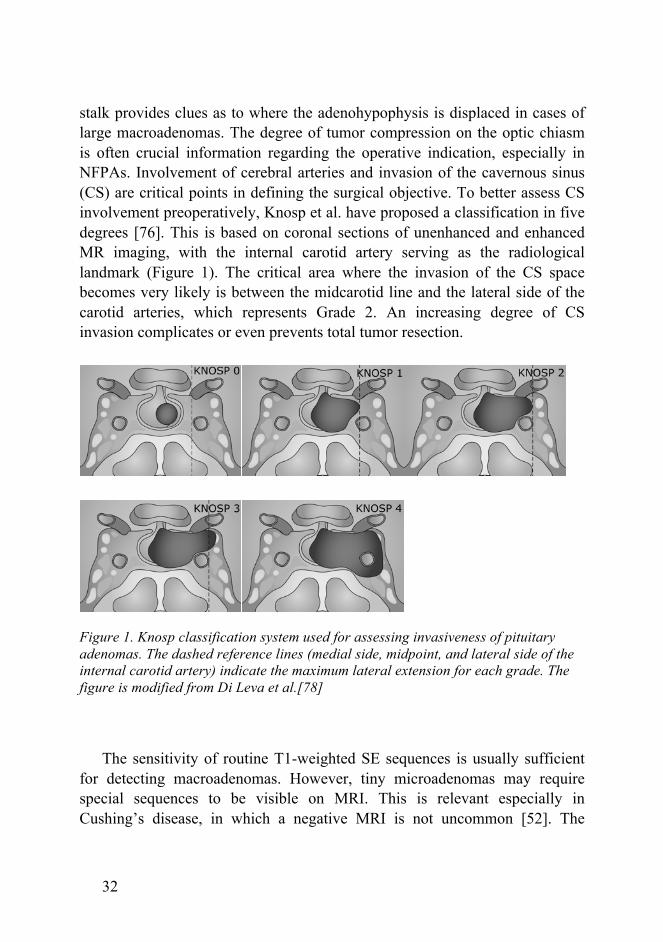
stalk provides clues as to where the adenohypophysis is displaced in cases of large macroadenomas. The degree of tumor compression on the optic chiasm is often crucial information regarding the operative indication, especially in NFPAs. Involvement of cerebral arteries and invasion of the cavernous sinus (CS) are critical points in defining the surgical objective. To better assess CS involvement preoperatively, Knosp et al. have proposed a classification in five degrees [76]. This is based on coronal sections of unenhanced and enhanced MR imaging, with the internal carotid artery serving as the radiological landmark (Figure 1). The critical area where the invasion of the CS space becomes very likely is between the midcarotid line and the lateral side of the carotid arteries, which represents Grade 2. An increasing degree of CS invasion complicates or even prevents total tumor resection.
Figure 1. Knosp classification system used for assessing invasiveness of pituitary adenomas. The dashed reference lines (medial side, midpoint, and lateral side of the internal carotid artery) indicate the maximum lateral extension for each grade. The figure is modified from Di Leva et al.[78]
The sensitivity of routine T1-weighted SE sequences is usually sufficient
for detecting macroadenomas. However, tiny microadenomas may require special sequences to be visible on MRI. This is relevant especially in Cushing’s disease, in which a negative MRI is not uncommon [52]. The
33
contrast between the hypoenhancing microadenoma and the hyperenhancing surrounding pituitary gland can be improved by using either a spoiled gradient recall acquisition technique or dynamic fast SE sequences with 1.5 mm slice thickness [75]. Three Tesla MRI may offer further improved resolution as compared with 1.5 Tesla scanners [77]. Regardless of the chosen method, imaging should start immediately after the contrast media injection because a delay will diminish the deferential enhancement of the adenoma from the normal pituitary.
4. Surgical treatment of pituitary adenomas
4.1. History and evolution of transsphenoidal surgery
The first published attempt to reach a pituitary tumor was made in year 1893 [79]. A temporal approach was used for a 35-year-old woman presenting with signs and symptoms consistent with intracranial hypertension and acromegaly. Intraoperative swelling of the brain prevented tumor resection, but decompressive craniectomy relieved symptoms, and the patient survived for two months. Autopsy revealed a pituitary mass the size of “a tangerine orange” with extensive parasellar invasion. Subsequently, Sir Victor Horsley operated on ten pituitary tumors during 1904-1906 using subfrontal and temporal approaches, with a 20% mortality rate [80]. At the same time (1905), German neurosurgeon Feodor Krause used a frontal transcranial approach to reach the sella turcica. His procedure provided the basis for later modifications introduced by Dandy, Frazier, and Cushing.
High mortality rates of early transcranial approaches led surgeons to seek alternative and safer routes to the sella turcica. In 1907, a successful removal of the pituitary through a lateral rhinotomy was reported [81]. During the next three years the transsphenoidal approach was further improved by introducing endonasal transseptal and sublabial techniques (Hirsch and Halstead, respectively) [80]. Harvey Cushing quickly adapted the transsphenoidal technique by using a sublabial incision, and introduced submucosal dissection and resection of the nasal septum, and endotracheal (instead of local) anesthesia. Cushing subsequently used the transsphenoidal approach for over
34
200 patients between the years 1910 and 1929. By the end of the 1930s, he nearly abandoned the transsphenoidal technique and continued using the transfrontal approach, which he had learned to perform outstandingly [82]. The neurosurgical community followed Cushing’s example, and the transsphenoidal technique was virtually forgotten for the next 35 years.
Norman Dott had visited Cushing during 1923-1924 and adopted the transsphenoidal technique, which he kept using contrary to the neurosurgical the mainstream after his return to Edinburgh. A young French neurosurgeon, Gerard Guiot, adopted the procedure from Dott while at the Edinburgh Royal Infirmary in 1956. Back in Paris, Guiot refined the transsphenoidal approach by using fluoroscopy to navigate his instruments during the nasal and sellar phases of the operation [83]. He applied the transsphenoidal technique in more than 1000 PAs and pioneered its use for craniopharyngiomas, clival chordomas, and parasellar lesions as well.
Jules Hardy of Montreal, Canada, worked as a fellow to Guiot in Paris to learn his transsphenoidal approach. By 1968, Hardy had refined the technique further and had introduced the operating microscope and the concept of using it for selective adenoma removal while preserving pituitary function [84]. The microsurgical approach revolutionized the transsphenoidal technique, which was gradually adopted as the first-line choice for PA removal worldwide. Besides improved illumination with the microscope, the increasing availability of antibiotics and the introduction of corticosteroid replacement led to decreased postoperative morbidity and mortality. Three decades earlier, Cushing had been missing these three factors, and this most likely caused him to revert to the transcranial approach. Since Hardy launched the new era of transsphenoidal microsurgery, it has undergone several refinements. It is the preferred operative technique for PA removal today [85, 86], and it currently has two main variations: microscopic and endoscopic.
The first evolutionary steps of the endoscopic technique were described by Guiot already in 1963 [87]. However, it took another 30 years of technical development before the endoscopic equipment offered high-quality visualization of the operative field, which allowed accurate microsurgical dissection [88, 89]. Extended approaches have been described, and the introduction of a fully endoscopic endonasal technique has further expanded the indications and limits of transsphenoidal surgery [90, 91]. Currently, most

35
centers use the endoscopic technique, and the continuous need for better results will push the techniques and skills to new levels in the future [12, 92].
Transnasal pituitary surgery was first introduced in Finland by otorhinolaryngologist Bertel Grahne. He was followed by neurosurgeon Simo Valtonen, who used the sublabial transsphenoidal approach, which he had learned from Graham Teasdale while visiting the Glasgow Institute of Neurological Sciences during 1976-1977. After returning to Helsinki, Dr. Valtonen gradually took over transsphenoidal pituitary surgery and gained further experience by visiting Dr. Gerard Guiot in Hôpital Foch, Paris. After a few years as the sole pituitary surgeon in Helsinki, Dr. Valtonen was joined by his neurosurgical colleague Antti Poranen who introduced the transseptal technique during the early 1980’s. The microscopic transsphenoidal technique was the method of choice until June 2008, when it was replaced by the endoscopic approach.
4.2. Transsphenoidal approaches
4.2.1. Microscopic technique
The microscopic technique is well described by several authors [90, 93, 94]. Using the keywords “microscopic transsphenoidal surgery” retrieves approximately 200 illustrative operative videos from YouTube (September 2015). The microscopic technique has three variations for access to the sphenoid sinus: sublabial [94], transseptal (submucosal endonasal) [93], and direct endonasal [90] techniques. Sublabial access through gingival incision offers the widest route and view to the sphenoid sinus and sellar floor. By contrast, direct endonasal modification is the least invasive as minimal dissection of the anterior nasal structures is required. The transseptal technique involves an anterior septal incision for access and a subsequent submucosal septal dissection. To keep the surgical pathway open, an automatic retractor of appropriate size is routinely introduced, if necessary, under fluoroscopic control. The sphenoid articulation of the vomer is removed, and a relatively wide anterior sphenoidectomy is performed with a rongeur or high-speed drill. Anatomical landmarks of the sphenoid roof (septae, carotid and optic
36
protuberances, opto-carotid recess, sellar floor, etc.) can then be identified. Once the nasal phase of the approach has been completed, all modifications of microscopic techniques continue in an identical manner for PA removal. The sellar floor is next opened, exposing the dura mater and the borders of the venous sinuses laterally and infero-superiorly. When in doubt, the position of the carotid artery can be confirmed with micro-Doppler before incision of the dura [90]. Ideally, the pituitary gland, its capsule (pial surface), and the tumor should be left intact at this phase. In case of a microadenoma, the tumor is carefully localized, if necessary reviewing the preoperative images once more, before incising the capsule of the pituitary gland. PAs are surrounded by a pseudocapsule, which serves as an excellent cleavage plane for dissection around the adenoma tissue to be excised [15]. The tumor with its capsule is removed using suction, ring curettes, and pituitary rongeurs of appropriate sizes and angles. In case of a large macroadenoma, an internal decompression is usually necessary before a cleavage plane can be developed around the adenoma. At this time, the tumor removal and dissection is started infero-laterally and working posteriorly, leaving the antero-superior part untouched as long as possible. After no more tumor is seen, an (assisting) endoscope can be utilized to look for tumor remnants around the corners [95].
Once the removal is completed, cerebrospinal fluid (CSF) leakage is looked for and if necessary confirmed with the Valsalva maneuver. There are various protocols for closing the sellar floor. Generally, the more voluminous the CSF leakage is detected, the more meticulous the patching and reconstruction of the sellar floor [96]. In case of no leakage, the dural access site can be covered with a sponge or equivalent to offer some scaffolding for vascularized (pseudo)dural regrowth. If the CSF leakage is generous, an autologous fascia-fat graft (harvested from the thigh or abdomen) and a piece of titanium mesh, porous plastic, or bony septum (vomer) are placed in a multilayer and watertight manner to cover the sellar floor defect. Usually, the reconstruction is covered with glue to seal and offer some support for the patching material. Additionally, a spinal drain may be used for a few days to eliminate any excess intracranial pressure at the repair site.

37
4.2.2. Endoscopic technique
The endoscopic technique has been well described by a number of groups [6, 91, 97, 98]. Using the keywords “endoscopic transsphenoidal surgery” retrieves approximately 800 illustrative operative videos from YouTube (September 2015). Compared with the microscopic technique, the advantages of endoscopy include minimal access with less dissection of the nasal structures, a panoramic view of the operative field, an improved lateral view with angled optics, and more versatility for accessing different and extensive lesions around the anterior cranial base. For these reasons, the endoscopic technique has largely replaced the microscopic technique [99].
Endoscopic endonasal access uses one or both nostrils as a natural corridor to reach the sphenoid sinus. Surgery usually commences via the right nostril by introducing a rigid 4 mm, 0° endoscope with an irrigation sheath. The middle turbinate is lateralized and the sphenoid ostium localized. In cases with a narrow nostril or a large tumor, or if the surgeon prefers, a left-sided route may also be created to work binarially. A nasoseptal flap is raised as necessary for later reconstruction of the sellar floor [100, 101]. In a typical PA surgery, with no need for nasoseptal flap, the mucosa around the sphenoid ostium is coagulated and the bone is removed with a rongeur to create a sufficiently wide sphenoidectomy to insert the endoscope and instruments into the sphenoid cavity. The endoscope may be then fixed with an adjustable holder mildly stretching the nostril upwards to allow space for the instruments working below. Alternatively, the assistant can hold the optics, allowing constant fine adjustments as necessary, to keep the surgical focus in the middle of the screen. From this point, the procedure continues in the same fashion as in the microscopic technique until no more tumor is seen. To complete the tumor removal, 30° and 45° optics are introduced, as necessary, to visualize a possible tumor residual. Reconstruction of the sellar floor follows the same principles as in the microscopic technique.
The main disadvantage of the endoscopic technique is a lack of stereoscopic vision, which can be compensated by moving the optics to and fro as necessary, using instruments with depth markings (e.g. mark 10 mm from the tip) and repetitive training of hand-eye coordination [102]. The first versions of 3D endoscopic instrumentation are already available, and
38
undoubtedly, it will eventually replace the current 2D endoscopic equipment [7, 103].
4.3. Craniotomy
Tumor extensions into the retrochiasmatic area, posterior fossa, or temporal or frontal lobe have traditionally been regarded as contraindications for the transsphenoidal approach. This rule does not necessarily apply to the endoscopic endonasal approach, which has improved transsphenoidal access. Its extended modifications enable access into most parasellar areas, and sufficient tumor control can be achieved in many giant PAs [104], decreasing the need for open craniotomy. However, complete removal of an invasive, laterally stretching large adenoma is a complex task for any pituitary surgeon or approach.
A large dumbbell-shaped adenoma with firm consistency and suprasellar adherence to neurovascular structures is often difficult to remove with a transsphenoidal approach. Dissection of critical structures may place the patient at considerable risk. Under these circumstances, a staged transsphenoidal approach may be advisable. The first session includes a safe resection of the lower portion of the tumor. The adherent suprasellar part of the tumor usually descends into the sella during the following months, offering itself for easier removal through redo transsphenoidal surgery instead of a transcranial approach [105].
Specific features favoring to elect the transcranial open craniotomy over the transsphenoidal route are exceptional supra- or retrosellar or lateral extensions of the tumor, hard tumor consistency, brain edema and invasion, and encasement of cerebral arteries or visual apparatus [106]. Especially multilobular shape and extension past the lateral wall of the cavernous sinus are beyond the scope of transnasal surgery [104].
There are several modifications of anterior/anterolateral transcranial approaches to the sellar area such as pterional frontotemporal or subfrontal craniotomies [107]. A more complex extradural approach for pituitary tumors is described by Dolenc [108]. The size and the direction in which the adenoma extends/invades will dictate the appropriate cranial approach in individual cases. However, a transcranial operation places the adjacent frontal lobe(s),
39
cranial nerves, vascular structures, and neuroendocrine pathways (hypothalamus, pituitary stalk) at risk. Since larger tumors are more likely to be treated with the transcranial approach, an unbiased comparison of results and complications with the transnasal approach is difficult. Reports comparing the approaches are conflicting regarding visual outcome, but the transnasal technique seems to offer superior results in terms of recovery of pituitary function and less frequent new hormonal dysfunction [109].
The choice between the transsphenoidal and transcranial approach is usually made case-by-case, taking into account the characteristics of the tumor and the patient, and the expertise of the surgical team. The techniques should be seen as complementary, rather than oppositional. They can even be applied simultaneously during the same surgical session [110].
4.4. Intraoperative adjunctive methods
Neuronavigation. Initially, with the advent of the microscopic transsphenoidal technique, fluoroscopy was introduced by Guiot and Hardy to guide the operative approach to the sella [111]. By the end of the 1990s, image guidance for neurosurgery (neuronavigation) was available for intracranial operations, including transsphenoidal surgery [112]. The main advantage of neuronavigation over traditional fluoroscopy is multiplanarity (enabling especially midline orientation). Neuronavigation has most likely increased safety during the transsphenoidal approach, particularly in cases with aberrant nasal and skull base anatomy, where the pituitary surgeon may get lost and in worst case scenario end up damaging e.g. the carotid artery. Large variation exists in how and when neuronavigation is used in different pituitary centers [12].
Intraoperative MRI. The concept of intraoperative MRI was introduced at the end of the 1990s [113]. Intraoperative MRI enables detection of possible residual tumor when no more tumor is visible in the operative field through the microscope or endoscope. This gives the surgeon an immediate second chance to complete the resection. Intraoperative MRI is shown to be a feasible adjunct in transsphenoidal surgery, and reports suggest improved rates of complete resection and higher extent of tumor removal even in combination with the
40
endoscopic technique [114, 115]. However, tiny tumor remnants may be hidden in the sellar circumference and can be below the detection level of MRI [116]. Another drawback is the major investments (millions of euros) required for establishing this sophisticated form of intraoperative visualization [117].
5. Radiotherapy
Radiotherapy can be delivered as conventional external beam radiation therapy in fractions (conventional radiotherapy) or as stereotactic radiotherapy (STR), which can be delivered as a single shot or fractionated treatment. STR is delivered using stereotactic methods for high precision. The most common STR systems are cobalt-based (e.g. Gammaknife) and linear accelerator-based (e.g. Novalis and Cyberknife) [8]. STR is best suited for spherical PAs with a diameter of less than 3 cm. Historical series of less focused conventional radiotherapy show significant long-term side-effects, such as hypopituitarism and temporal lobe atrophy, in patients treated for PA [118]. Modern planning and targeting techniques have increased the safety and accuracy of external beam radiotherapy. It is currently indicated in larger PAs, which are not suitable for STR [8].
The literature does not support the routine use of radiotherapy as a primary treatment for PAs. However, very old or medically ill patients deemed unsuitable candidates for surgery may be considered for STR as an initial treatment [119]. STR is typically utilized in NFPA patients with substantial residual tumor or recurrence after transsphenoidal operation. It seems to be very efficient for this indication, with tumor control rates ranging from 83% to 100% [8].
STR may be employed for selected patients with FPAs who have not achieved endocrine remission after surgery. In Cushing’s disease, the reported response to STR has been quite variable, with a mean of 51% (range 0-100%) of patients achieving remission. The mean time from treatment to remission has been 12 months [120]. Similarly, unsuccessful transsphenoidal surgery for acromegaly may be an indication for STR, unless long-term medical therapy is chosen. Some treatment-resistant GH-producing adenomas may require multimodality management, including STR. The reported rate of hormonal remission after STR for acromegaly is on average 45% (range 0-82%), with a
41
mean time to remission of 24 months [8]. Prolactinomas are primarily and efficiently managed with medical treatment. Drug-resistant cases are rare and possibly represent a biologically different subgroup of prolactinomas. Post STR remission rates are lower than in other FPAs, with a median of 35% (range 0-100%) [8].
Single-session STR margin doses have been on average 16 Gy and 22-24 Gy for NFPA and FPA, respectively. New or worsening hypopituitarism after STR has been reported in 9% and 15-24% of NFPA and FPA patients, respectively [8]. Higher margin dose probably explains the difference in hypopituitarism between NFPA and FPA. Using fractionated STR for various PAs with at an average dose of 45 Gy (range 45-54 Gy) in 25 fractions, hypopituitarism was noted in 40% of cases, but the effect of preceding surgery was included [121]
6. Outcome after transsphenoidal surgery
6.1. Tumor control
Success of surgery for functional adenoma is primarily determined by hormonal remission, and radiological extent of resection is a secondary measure of tumor control. All patients harboring FPA should be evaluated for hormonal cure after surgery using consensus guidelines and criteria [39, 48]. Reported rates of remission are primarily dependent on FPA subtype [122]. Sensitive hormonal assays may detect secretory tumor residuals even if postoperative high-quality MRI is negative [75].
The main objective of NFPA surgery is to decompress the optic nerve(s) and chiasm. This goal may be achieved even if some tumor is left behind, unlike in FPA, when residual tumor inevitably causes surgical failure as hormonal hypersecretion continues. Tumor control of NFPA is presented as the success rate of gross total resection or extent of resection. Quality of resection has gradually improved over time, and currently complete removal of NFPA is accomplished in more than 50% (up to 95%) of cases [64, 68]. The two strongest independent risk factors for incomplete resection are larger tumor size and higher grade of lateral tumor invasion [68, 123, 124].

42
Several studies have made comparisons between endoscopic and microscopic outcomes in terms of tumor control, but have found no significant differences [11, 122, 125, 126]. To date, no randomized controlled comparisons exist, but one controlled single-center study reported improved tumor control with the endoscopic approach relative to the microscopic approach [9]. Most authors conclude that the quality of resection is highly dependent on the surgical experience, with better outcome correlating with a higher number of operated cases [127, 128].
6.2. Pituitary function
Recovery and/or loss of hormonal function are well-known consequences of transsphenoidal surgery for PA. Postoperatively, improved function of the anterior pituitary has been reported in 33-50% of patients [129-132]. New or worsening anterior pituitary insufficiency has ranged from 1% to 33%. Permanent DI has been reported in 0.4-8.8% of cases, but it generally occurs in under 3% of cases [131, 133-137]. Transient forms of DI are much more common and have been noted in up to 50% of patients in some reports [136].
Larger tumor size, transcranial technique, and limited surgical experience have been factors leading to deteriorating pituitary function [131, 133, 138]. As can be expected, these factors correlate inversely with the probability of improving pituitary function [131, 138, 139]. In addition, endoscopic technique, younger age, absence of systemic hypertension, absence of tumor invasion, and hyperprolactinemia secondary to stalk compression have been suggested to improve chances for recovery of pituitary function [9, 131, 138]. Adenoma subtype may have an impact on postoperative hormonal recovery since adrenal insufficiency was reversed more often in acromegalic patients than in NFPA patients, independent of tumor size or invasion [140].
Successful surgery for Cushing’s disease leads to transient secondary adrenal insufficiency in a majority of patients. In most cases, adrenal responsiveness is restored to normal over a period of several months to one year [141-144]. Poorer recovery of function and higher rates of hypopituitarism are related to partial hypophysectomy, which is sometimes required for hormonal remission in Cushing’s disease [145].

43
The overall variability in reported rates of altered pituitary function reflects several factors, including different surgical strategies with respect to normal gland manipulation and preservation, transsphenoidal surgical experience, tumor size, and hormonal testing protocols and the criteria for improved or deteriorated function.
6.3. Neuro-ophthalmological function
Successful transsphenoidal surgery for PA will usually improve deficient visual function or even restore it to normal. There is a strong correlation between improvement of visual acuity and visual field recovery, but outcomes are not parallel in every case. Postoperative improvement of visual fields is reported in 77-95% of cases, and no improvement or deterioration in 8-19% of cases [146-148]. Reported rates of improved visual acuity are clearly more variable, ranging from 45% to 81% [148, 149].
Although visual function can recover several years after surgery, most of it returns within the first 6 months [147]. Longer history and larger degree of visual impairment are linked with worse recovery. Thus, prompt diagnosis and early, even prophylactic, surgery is recommended in patients with PA [147]. Permanent visual deterioration caused by surgical manipulation is very rare, usually reported in less than 1% of cases [10, 123].
6.4. Complications
Contemporary techniques of transsphenoidal surgery are considered relatively safe, and operative mortality is less than 0.5% according to a meta-analysis [10]. The potential complications of transsphenoidal pituitary surgery are varied. They are related to nasal dissection, opening of the sellar floor, manipulation of the pituitary gland and/or stalk, and intracranial vascular and neural injury. Lack of uniform grading or classification systems complicates comparison and interpretation of the literature.
Except for hormonal impairments (hypopituitarism), the most commonly quoted complication is nasal CSF leakage ranging from 1% to 9% (pooled rate 7%) [7, 10, 86, 133, 150]. The main risk factor for postoperative CSF
44
rhinorrhea is intraoperative disruption of the arachnoid membranes. Other suggested risk factors are larger tumor size, age (both younger and advanced), body mass index, repeat operation, and previous radiotherapy [151-154].
A serious consequence of CSF leakage is postoperative meningitis, which is reported in between 0-2% of cases [10, 133]. Syndrome of inappropriate secretion of antidiuretic hormone (SIADH) may complicate pituitary surgery in up to 35% of cases, and typically presents approximately one week postoperatively [155, 156].
The most feared morbidity related to transsphenoidal surgery is caused by injury to the vasculature or the cranial nerves. Loss of midline orientation and consequent carotid artery injury or inappropriate handling of para/suprasellar vessels are the two most common reasons for vascular complications, occurring in about 1% of surgeries [10]. Cranial nerve injury is related to attempts to remove lateral tumor remnants from the cavernous sinus. Permanent cranial nerve damage is rare, occurring in only 0.5% of cases [10, 133].
Minor sinonasal complaints, such as nasal congestion, crusting, and altered smell/taste, are common (up to 60%), but are often self-limiting [42]. Major epistaxis or sinusitis requiring treatment is rare, generally reported in 0.6-2% and 0.4-2% of cases, respectively [90, 102, 137, 157]. A small meta-analysis found rhinological complications in up to 13% of patients after microscopic surgery compared with 1.2% after endoscopic surgery [126]. By contrast, in a retrospective analysis of acromegalic patients having undergone microscopic or endoscopic transsphenoidal surgery [158] the self-reported incidence of alterations in taste or smell was 26% versus 5% (P=0.008), and in sinusitis 26% versus 3% (P=0.002). The authors concluded that sinonasal complications could be regarded as a natural consequence of operative manipulation and dissection associated with both techniques. Increasing awareness of this complication and consequently more active inquiry and recording may also explain the higher incidence. In addition, acromegalic patients often report preoperative sinonasal complaints as one feature of their morbid condition [42].
Many authors have found surgical experience in terms of a higher number of performed operations to be a significant factor in a lower rate of complications [102, 127, 133, 154]. However, the superiority of one
45
transsphenoidal technique over the other with respect to rate of complications has been much more difficult to demonstrate [10, 159, 160].
7. Health-related quality of life after treatment for pituitary adenomas
7.1. Measuring health-related quality of life
The WHO definition of health is based on physical, mental, and social well-being. Health-related quality of life (HRQoL) can be defined as the functional effect of an illness and its consequent therapy on a patient, as perceived by the patient. This is further modified by the patient’s individual goals, expectations, standards, concerns, and cultural context. No gold standard exists for measurement of HRQoL. Commonly, a self-administered questionnaire-based method (instrument) is used. The HRQoL instrument may describe one’s health in different dimensions (profile) or as a single index (total score). It can either be generic, disease-specific, or domain (e.g. fatigue, anxiety) -specific.
Generic questionnaires can be used to measure HRQoL regardless of the disease or medical condition, and different patient groups can be compared with each other. Additionally, generic instruments are utilized for assessing quality-adjusted life-years (QALYs). Examples of common generic questionnaires are the Short-Form health survey (SF-20/36/SF-6D), the Nottingham Health Profile (NHP), the European Quality of Life Scale (EQ-5D), the 15D, the General Well-Being Schedule (GWBS), the WHO Disability Assessment Schedule (WHODASII), and the General Health Questionnaire (GHQ)-12/28/30 [161, 162].
The Finnish 15D questionnaire is a generic HRQoL instrument that combines the advantages of a profile and a preference-based, single index measure [163]. It is a comprehensive (15-dimensional) questionnaire that can be completed within 5-10 minutes. The 15D instrument has been applied in drug evaluations, surgical outcome studies, assessment of rehabilitation results, and many other medical treatments and conditions including PA. There are currently (as of September 2015) 370 peer-reviewed publications
46
using the 15D instrument (http://www.15d-instrument.net/service.cntum?pageId=110293).
Disease-specific questionnaires have been developed to increase the sensitivity for detection of impairments and changes associated with a disorder. Such instruments for specific pituitary purposes are available for Cushing’s disease [164], acromegaly [165, 166], and hypopituitarism [167, 168].
Numerous domain-specific questionnaires are available for measuring the effect of particular symptoms or functions on a patient’s HRQoL regardless of etiology. Examples of domain specific questionnaires used for PA patients are the Hospital Anxiety Depression Scale (HADS), the Multidimensional Fatigue Inventory (MFI-20), and the Major Depression Inventory (MDI) [162].
Unfortunately, there has been little consistency in measuring the HRQoL in PA patients. At least 49 different questionnaires have been applied to assess the HRQoL, and only a minority of cross-sectional reports have used an age and gender-adjusted control population [162].
7.2. Health-related quality of life and functional pituitary adenoma
Prolactinoma. Relatively few studies on HRQoL after treatment of prolactinoma have been published [162]. The largest study, including 128 prolactinoma patients, suggested a trend towards impaired HRQoL total score (SF-36) after treatment (27% surgery) relative to a control population, but no statistical significance was detected [169]. Moreover, no independent factors for compromised HRQoL scores were found either.
Another study on female patients (n=55) treated exclusively with dopamine agonists for microprolactinoma (67% in remission) suggested increased anxiety and depression score in HADS, increased fatigue on most of the subscales of the MFI-20, and worse scores on social functioning in both SF-36 and HADS [170]. Outcomes were compared with an age-matched control population (e.g. friend, neighbor) provided by each patient. The authors found no correlation between HRQoL scores and age, prolactin level, present use of dopamine agonist, or hypogonadism.
A Brazilian study showed poorer HRQoL score in prolactinoma patients treated with dopamine agonists (n=50) than in a healthy control population
47
(hospital staff). Patients in biochemical remission (50%) showed statistically better HRQoL scores than patients with hyperprolactinemia (50%) [171].
A Finnish study reported multiple HRQoL (15D) impairments in surgically treated prolactinoma patients compared with age- and sex-adjusted controls. The authors did not find any correlation between postoperative hyperprolactinemia and 15D score, but their cohort consisted of only 17 patients [172].
In conclusion, especially mental health and psychological function measures have been impaired in prolactinoma patients. Larger studies including gender- and age-adjusted control populations are needed.
Acromegaly. Many cross-sectional studies have shown severe impairments of HRQoL in patients treated for acromegaly [173-176]. A disease-specific questionnaire (AcroQoL) has indicated compromised HRQoL on all subscales: appearance, physical performance, psychological well-being, and personal relations [165, 174, 176].
The largest study on HRQoL of acromegalic patients (n=231) used the generic 15D instrument [175]. The main finding was reduced total HRQoL score in patients treated for acromegaly compared with the age- and gender-standardized control population. The strongest independent negative factors for HRQoL were advanced age, higher BMI, and radiotherapy. Interestingly, the 15D score was related to nadir GH in oral glucose tolerance testing in an inverted U-shape: lower or higher GH-values were associated with worse HRQoL score relative to values between 0.3 and 1.0 µg/L.
Slowly progressive disease with often delayed diagnosis may cause irreversible changes in appearance and internal tissues, which has been reflected in impaired HRQoL in acromegalic patients even after successful treatment and biochemical remission [174]. However, several studies have shown that control of GH/IGF-1 excess by surgery or medical treatment has improved the HRQoL score [165, 175-177]. Remission after surgery alone is related to a better HRQoL outcome than surgery followed by SSA treatment [178].
The need for postoperative SSA medication has been shown to be correlated with worse HRQoL score despite similar IGF-1 levels [172, 179]. A small (n=20) placebo-controlled, double-blinded crossover study suggested that addition of pegvisomant treatment for biochemically controlled (IGF-1
48
normal for age) patients receiving SSA improved their QoL [166]. Thus, normalized IGF-1 values did not necessarily guarantee optimal HRQoL. However, this result has not been repeated in any other study.
In summary, HRQoL may be impaired in acromegaly despite disease control, and independent factors associated with better outcome need further investigations [162]. Table 1 presents the results of selected studies (based on size and publication year) of HRQoL after treatment of acromegaly. Cushing’s syndrome/disease. A review of 22 studies, including a total of 1713 patients harboring Cushing’s syndrome, suggests a clearly negative impact on HRQoL as compared with healthy controls or reference values [162]. Cushing’s syndrome has been reported to impair HRQoL on many dimensions: physical functioning, bodily pain, mental and general health, and anxiety [169, 180]. Authors mostly agree that there are no differences in HRQoL between patients with Cushing’s syndrome of adrenal or pituitary origin [181-183].
Several studies show poorer HRQoL independently of treatment modality and biochemical remission, possibly explained by chronic hypercortisolemia preceding treatment [183-186]. However, patients show improvements after treatment, and a better HRQoL score has correlated with biochemical remission, especially in the disease-specific questionnaires [3, 180, 182, 187].
Presence of depression had a lowering effect on HRQoL in two large studies using disease-specific questionnaires [3, 181]. Other factors negatively influencing HRQoL in Cushing’s disease have been older age, female gender, hypopituitarism, and shorter duration of remission, but the literature is inconsistent [162, 164, 182, 184].
Disease remission after successful treatment with subsequent gradual improvement in HRQoL has been the most consistent finding in studies using either generic or disease-specific questionnaires for Cushing’s disease [164]. Table 1 presents the results of selected studies (based on size and publication year) of HRQoL after treatment of Cushing’s disease.
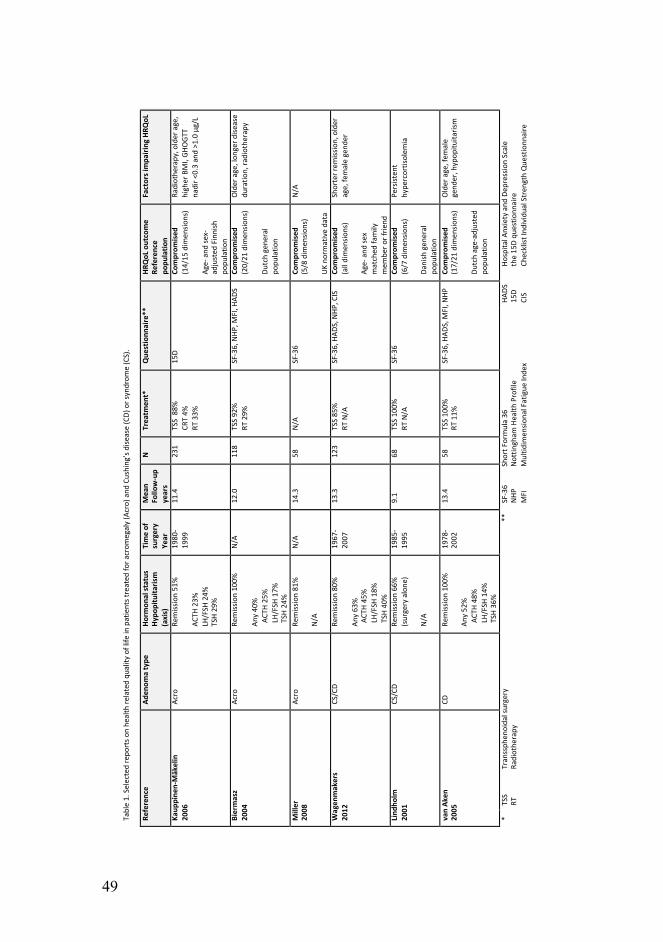
49
!Table&1.&Selected&repo
rts&o
n&he
alth&re
lated&qu
ality
&of&life
&in&patients&treated
&for&a
crom
egaly&(Acro)&and
&Cushing’s&dise
ase&(CD)&or&syndrom
e&(CS).&
Reference'
Aden
oma'type
'Ho
rmon
al'status'
Hypo
pituita
rism'
(axis)'
Time'of'
surgery'
Year'
Mean'
Follo
w>up'
years'
N'
Treatm
ent*'
Que
stionn
aire**'
HRQoL'outcome'
Reference'
popu
latio
n'
Factors'impa
iring'HRQ
oL'
Kaup
pine
n>Mäkelin'
2006
'Acro&
Remission&51%&
& ACTH
&23%
&LH
/FSH
&24%
&TSH&29%&
1980M
1999&
11.4&
231&
TSS&&88%
&CR
T&4%
&RT
&33%
&
15D&
Comprom
ised
'(14/15
&dim
ensio
ns)&
& AgeM&and
&sexM
adjusted
&Finnish&
popu
latio
n&
Radiothe
rapy,&older&age,&
higher&BMI,&GH
OGT
T&nadir&<
0.3&and&>1.0&μg/L&
Biermasz'
2004
'Acro&
Remission&100%
&& An
y&40%&
&&ACT
H&25%&
&&LH/FSH&17%&
&&TSH
&24%
&
N/A&
12.0&
118&
TSS&92%&
RT&29%
&SFM36,&NHP
,&MFI,&H
ADS&
Comprom
ised
&(20/21
&dim
ensio
ns)&
& Dutch&gene
ral&
popu
latio
n&
Older&age,&lon
ger&d
isease&
duratio
n,&ra
diothe
rapy&
Miller'
2008
'Acro&
Remission&81%&
& N/A&
N/A&
14.3&
58&
N/A&&
SFM36&
Comprom
ised
'(5/8&dim
ensio
ns)&
& UK&no
rmative&data&
N/A&
Wagen
makers'
2012
'CS/CD&
Remission&80%&
& Any&63%&
&&ACT
H&45%&
&&LH/FSH&18%&
&&TSH
&40%
&
1967M
2007&
13.3&
123&
TSS&85%&
RT&N/A&
SFM36,&HAD
S,&NHP
,&CIS&
Comprom
ised
&(all&dimen
sions)&
& AgeM&and
&sex&
matched
&family&
mem
ber&o
r&frie
nd&
Shorter&rem
ission,&older&
age,&fe
male&gend
er&
Lind
holm
'2001
'CS/CD&
Remission&66%&
(surgery&alone
)&& N/A&
1985M
1995&
9.1&
68&
TSS&100%
&RT
&N/A&
SFM36&
Comprom
ised
&(6/7&dim
ensio
ns)&
& Danish&gen
eral&
popu
latio
n&
Persisten
t&hype
rcortisolem
ia&
van'Ak
en'
2005
'CD
&Re
mission&100%
&& An
y&52%&
&&ACT
H&48%&
&&LH/FSH&14%&
&&TSH
&36%
&
1978M
2002&
13.4&
58&
TSS&100%
&RT
&11%
&SFM36,&HAD
S,&M
FI,&N
HP&
Comprom
ised
&(17/21
&dim
ensio
ns)&
& Dutch&ageMadjusted
&po
pulatio
n&
Older&age,&fem
ale&
gend
er,&hypop
ituita
rism&
*&TSS&
Transsph
enoidal&surgery&
RT&
Radiothe
rapy&
**&
SFM36&
Short&F
ormula&36&
NHP
&Nottin
gham
&Health
&Profile&&
MFI&
Multid
imen
sional&Fatigue
&Inde
x&
HADS
&Ho
spita
l&Anxiety&and
&Dep
ression&Scale&
15D&
the&15D&qu
estio
nnaire&
CIS&
Checklist&Individu
al&Stren
gth&Que
stionn
aire&
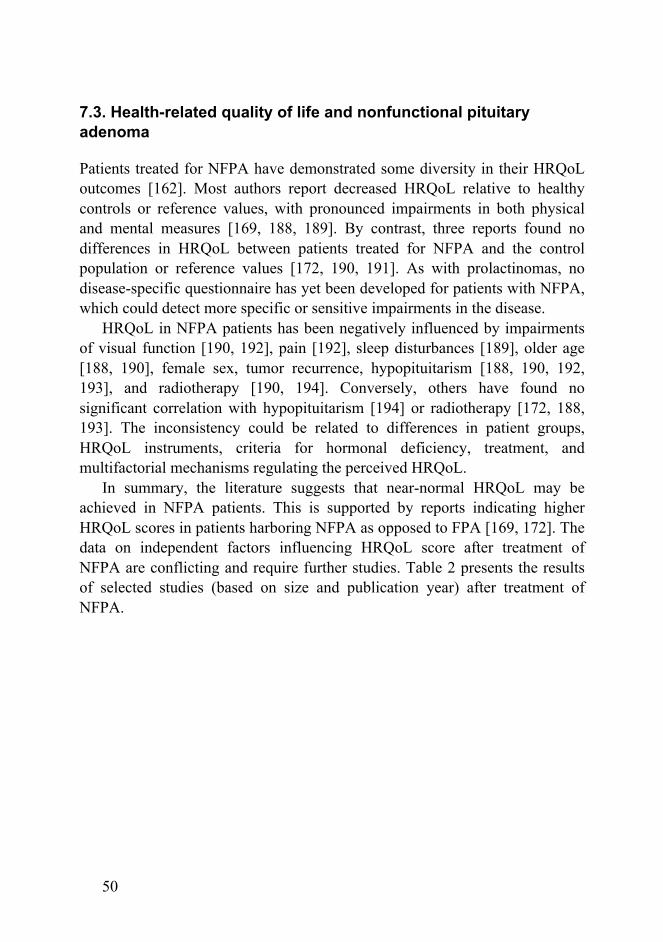
50
7.3. Health-related quality of life and nonfunctional pituitary adenoma
Patients treated for NFPA have demonstrated some diversity in their HRQoL outcomes [162]. Most authors report decreased HRQoL relative to healthy controls or reference values, with pronounced impairments in both physical and mental measures [169, 188, 189]. By contrast, three reports found no differences in HRQoL between patients treated for NFPA and the control population or reference values [172, 190, 191]. As with prolactinomas, no disease-specific questionnaire has yet been developed for patients with NFPA, which could detect more specific or sensitive impairments in the disease.
HRQoL in NFPA patients has been negatively influenced by impairments of visual function [190, 192], pain [192], sleep disturbances [189], older age [188, 190], female sex, tumor recurrence, hypopituitarism [188, 190, 192, 193], and radiotherapy [190, 194]. Conversely, others have found no significant correlation with hypopituitarism [194] or radiotherapy [172, 188, 193]. The inconsistency could be related to differences in patient groups, HRQoL instruments, criteria for hormonal deficiency, treatment, and multifactorial mechanisms regulating the perceived HRQoL.
In summary, the literature suggests that near-normal HRQoL may be achieved in NFPA patients. This is supported by reports indicating higher HRQoL scores in patients harboring NFPA as opposed to FPA [169, 172]. The data on independent factors influencing HRQoL score after treatment of NFPA are conflicting and require further studies. Table 2 presents the results of selected studies (based on size and publication year) after treatment of NFPA.
51
! Table&2.&Selected&repo
rts&o
n&he
alth&re
lated&qu
ality
&of&life
&in&patients&treated
&for&n
onfunctio
nal&pitu
itary&ade
noma&
Reference'
Hypo
pituita
rism'
(axis)'
Time'of'
surgery'
Year'
Mean'
Follo
w<
up'
years'
N'
Treatm
ent*'
Que
stionn
aire**'
HRQoL'outcome'
' Reference'po
pulatio
n'
Factors'impa
iring'HRQ
oL'
Capa
tina'
2012
'AC
TH&44%
&LH
/FSH
&51%
&TSH&46%&
N/A&
6.0&
193&
TSS&100%
&RT
&41.7%
&SFJ36,&NHP
,&EuroQ
oL&
Not'com
prom
ised
'Ag
eJrelated&UK&po
pulatio
n&Tumor&re
curren
ce,&fem
ale&gend
er,&older&age,&visu
al&
field&defects,&non
Jtreated
&hypogon
adism
&
Raap
pana
'2012
'An
y&60%&
1992
J2004&
&6.3&&
53&
TSS&92%&
CRT&8%
&RT
&11%
&
15D&
Not'com
prom
ised
&Ag
eJ&and
&sexJadjusted
&Finnish&pop
ulation'
Non
e&de
tected
&
Biermasz'
2011
'An
y&88%&
N/A&
8.0&
17&
TSS&100%
&SFJ36,&M
FIJ20,&HAD
S&Co
mprom
ised
'(9/16&dimen
sions)&
Locally&re
cruited&matched
&pop
ulation&
N/A&
van'de
r'Klau
uw'
2008
'
ACTH
&63%
&LH
/FSH
&80%
&TSH&62%&
N/A&
&10&&
99&
TSS&100%
&RT
&37%
&SFJ36,&NHP
,&MFIJ20,&
HADS
&Co
mprom
ised
'(all&dimen
sions)&
Comparable&ageJ&and
&sex&distrib
ution&
from
&dire
ct&so
cial&enviro
nmen
t&
Hypo
pituita
rism,&older&age,&fem
ale&gend
er&
Nielsen
'2007
'An
y&73%&
1985
J1996&
13.1&
192&
TSS&87%&
CRT&13%&
RT&&30%
&
SFJ36,&M
DIJ10&
Not'com
prom
ised
&Ag
eJ&and
&sexJspecific&Da
nish&pop
ulation&
Craniotomy&
Dekkers'
2006
'An
y&93%&
1985
J2004&
&9.9&&
99&
TSS&100%
&&RT
&37%
&SFJ36,&NHP
,&MFIJ20,&
HADS
&Co
mprom
ised
&(10/20
&dim
ensio
ns)&
Dutch&and&West&E
urop
ean&ageJadjusted
&po
pulatio
n'
Older&age,&hypop
ituita
rism,&fem
ale&gend
er&
*TSS&
&Transsph
enoidal&surgery&
CRT&
&Craniotomy&
RT&
&Ra
diothe
rapy&
' '
**SFJ36&
&Short&F
ormula&36
&NHP
&&
Nottin
gham
&Health
&Profile&&
EuroQoL&&&&&&&&&&&&&&&&&Europ
ean&Quality&of&Life
&Scale&
MFI&
&Multid
imen
sional&Fatigue
&Inde
x&HA
DS&
&Ho
spita
l&Anxiety&and
&Dep
ression&Scale&
15D&
&the&15D&qu
estio
nnaire&
MDIJ10&
&Major&Dep
ression&Inventory&
&
52
8. Multidisciplinary collaboration
Pituitary adenomas constitute a complex and diverse spectrum of disorders, which may involve multiple organs or body functions either directly or indirectly. State-of-the-art care for patients with pituitary adenomas is preferably offered in a multidisciplinary collaborative organization. Stepwise diagnostics, treatment and follow-up are best coordinated by an endocrinologist.
Transsphenoidal pituitary surgery differs anatomically from mainstream transcranial neurosurgery. The transnasal route requires special skills and knowledge. A close cooperation between the pituitary surgeon and an otorhinolaryngologist familiar with endoscopic sinus surgery is particularly useful when operating on patients with pre-existing sinus disease, septal perforations, or septal deviations [102]. According to a recent international survey, pituitary surgery is conducted most commonly by a neurosurgeon or a team of neurosurgeons together with an otorhinolaryngologist, and in a few units is performed by the otorhinolaryngologist alone [12].
Pituitary surgery has anesthesiological features requiring special attention. Perioperative pituitary insufficiency and replacement therapy, where necessary, must to be considered. A difficult intubation must be anticipated in cases of acromegaly and sometimes in Cushing’s disease. Intraoperative blood pressure control contributes to adequate hemostasis and a bloodless surgical field. To push suprasellar tumor remnants down into the operative view, the anesthetist may use controlled hypercapnia and/or the Valsalva maneuver. Postoperative water balance needs careful monitoring for an often unpredictable course [195].
Pathological analysis of pituitary tumors has become complex, with the advent of novel categories defined by WHO [2]. Although most adenomas may be easily classified, others may require the expertise of a dedicated neuropathologist. Molecular signatures of pituitary adenomas using genomics and proteomics are being increasingly used to identify invasive and atypical tumors and to guide treatment [196].
Experienced pituitary practitioners in neurosurgery and endocrinology, together with teams from neuro-ophthalmology, neuropathology, neuro-oncology, diagnostic and interventional neuroradiology, and otorhinolaryngological surgery, can constitute a center of excellence [128]. A

53
coordinated multidisciplinary approach and regionalized treatment centers are supported by data showing better outcomes in experienced hands with a sufficient number of cases treated [197].
54
C. Aims of the study
1. To describe the transitional phase from microscopic to endoscopic transsphenoidal surgery for nonfunctional pituitary adenoma and to clarify its effects on outcome at HUH during 2000-2010.
2. To investigate health-related quality of life in patients operated on for a functional pituitary adenoma.
3. To evaluate health-related quality of life in patients operated on for a nonfunctional pituitary adenoma.
55
D. Patients and methods
1. Patients
Over an 11-year period (from 2000 to 2010), 330 newly diagnosed pituitary adenoma patients were operated on at Helsinki University Hospital.
Patients harboring a pituitary carcinoma (n=2), patients with a history of previous pituitary surgery (n=34), or patients undergoing a craniotomy (n=2) were excluded from the study.
Publication I (Transition from microscopic to endoscopic transsphenoidal surgery for nonfunctional pituitary adenomas.): This study included 185 patients operated on for a NFPA. Patients were divided into two groups: the Microscopic group (n=144) was operated on during the first 101 months and the Endoscopic group (n=41) during the last 31 months of the study period.
Publication II (Normal long-term health-related quality of life can be achieved in patients with functional pituitary adenomas having surgery as primary treatment): This study included patients operated on for a FPA. A survey was sent to 128 patients, 100 of whom responded. Consequently, the actual study population comprised 47 patients with acromegaly, 21 patients with Cushing’s disease, 26 patients with prolactinoma, two patients with TSH-adenomas, and four patients harboring gonadotropinomas.
Publication III (Health-related quality of life in patients treated for non-functioning pituitary adenomas during the years 2000-2010): This study included patients operated on for a NFPA. A survey was sent to 161 patients, 137 of whom returned the questionnaires.
2. Data collection
Publications I, II, and III: Data were collected retrospectively from medical reports and imaging studies. Informed written consent to gather follow-up data from other hospitals was obtained from all patients. Data collection ensued between January 2012 and June 2013.
56
Publications II and III: A 15D questionnaire assessing health-related quality of life (Appendices 1 and 2) and a supplementary survey assessing educational background, marital status, current medication, and major comorbidities (type 1 and type 2 diabetes, essential hypertension, coronary artery disease, and depression) (Appendices 3 and 4) were sent to all patients alive at the beginning of 2013. One reminder was sent to nonrespondents two months later.
3. Surgery
All operations were performed by experienced neurosurgeons. An assistant surgeon was engaged infrequently. The transsphenoidal technique was modified in June 2008, and the microscope was switched to the endoscope, which was thereafter used solely. Fluoroscopy was used in all microscopic approaches. Neuronavigation was rarely used during the study period. The protocol and the instruments applied for tumor removal were alike in both approaches. An ultrasonic aspirator was not utilized. Intra- or postoperative lumbar drainage was rarely used.
3.1. Microscopic approach
The microscopic transseptal technique was applied. The mucosal incision was made at the anterior nasal septum, and the subsequent submucosal dissection continued up to the sphenoid ostia. A nasal speculum was used to maintain access between the septal mucosa. Anterior sphenoidectomy was done with rongeurs and/or a high-speed drill. The septae of the sphenoid sinus were removed, as necessary, and the sellar floor at the midline was identified. The sellar floor was removed and the dura incised to uncover the tumor/pituitary gland. A selection of suction, ring curettes, and pituitary rongeurs of appropriate sizes and angles was applied to excise the adenoma. Once the removal was completed, CSF leakage was carefully inspected. If leakage had occurred, an autologous fascia-fat graft was harvested from the thigh and placed in the sellar floor to seal the defect.
57
3.2. Endoscopic approach
The endoscopic endonasal technique was used. The endoscope was introduced through nostril(s) and middle turbinate(s) lateralized as necessary to create a free passage for the instruments. The mucosa around the sphenoid ostium was coagulated and access into the sphenoid sinus created as in the microscopic approach. The endoscope was fixed with an adjustable holder, mildly stretching the nostril upwards to allow room for the instruments introduced below. When in doubt, the position of the carotid artery was established with a micro-Doppler before dural incision. From this point, the procedure continued in the same fashion as in the microscopic approach until no more tumor was seen. To complete the tumor removal, 30° and 45° optics were used, if necessary, to visualize any tumor remnant “around the corners” of the sellar opening. Steering of the angled endoscope was done freehand, usually with a curved-tip suction tube in the other hand. Alternatively, the angled endoscope was fixed in position to operate with both hands (two instruments). Reconstruction of the sellar floor was performed as in the microscopic approach.
3.3. Postoperative care
Immediate postoperative care and follow-up took place at the Neurosurgical Unit. Occasional CSF rhinorrhea (or its suspicion) was primarily managed with a lumbar drain, and only persistent leakage was sealed with repeat surgery. On the 2nd postoperative day, the Endocrine Unit took over the care for a further 2-3 days. Patients were observed and evaluated for continuation or discontinuation of perioperative hydrocortisone substitution, managed for possible water and electrolyte disturbances (diabetes insipidus), and usually discharged on the 5th or 6th postoperative day.

58
4. Endocrine assessment and care
Pituitary function was assessed using in-house assays and clinical evaluation. Laboratory measurements were performed at the laboratory of Helsinki University Hospital (HUSLAB), and standard accredited assays were used. For study purposes, specific pituitary axes were classified as dysfunctional if they were substituted. All patients were re-evaluated during the first postoperative week, and the function of adrenal axis and posterior pituitary lobe was substituted as necessary. Three months after the surgery, patients came to the Endocrine Unit for more thorough evaluation (hypo- and hyperpituitarism) of relevant pituitary axes. The GHRH-arginine test (in addition to GH- and IGF-1 measurements) was a prerequisite for reimbursement of GH replacement therapy. All clinically significant deficiencies were substituted, unless contraindicated. Assessment of hormonal remission and optimization of treatment for acromegaly and Cushing’s disease were accomplished according to available international consensus criteria and/or scientific evidence [41, 48, 53, 198, 199]. For study purposes, hormonal remission was assessed according to the most recent criteria [39, 53]. During later follow-up patients were seen at the Endocrine Unit for hormonal assessment on a regular basis, usually once a year.
5. Radiology
The routine scanning protocol consisted of sagittal and coronal T1-weighted thin sliced sequences, with and without contrast media, using a 1.5 Tesla MRI. In case there was a contraindication for MRI, the imaging was done with computerized tomography. The tumor dimensions were measured (A: height, B: width, C: length), and the volume was estimated (ABC/2) independently by a radiologist (Kivisaari) and a neurosurgeon (Karppinen). Knosp classification was used for judging the lateral extension [76]. The Knosp grades 0 and 1 suggest a noninvasive tumor and grades 2 to 4 increasing invasion of the cavernous sinus. In case of discrepant (Kivisaari vs. Karppinen) measurements or Knosp classification, the larger value or higher grade was used for study purposes.
59
Postoperative MRI was repeated at 3 and 12 months, and thereafter at 1- to 3-year intervals, based on biochemical and clinical data/analyses. The quality of resection (total or subtotal) was based on assessment using the 3-month postoperative scan. The grading was done in favor of an existing residual, if postoperative artifacts prevented precise evaluation. Tumor remnant was measured in three dimensions, and the volume and residual percentage estimated. A recurrent tumor was defined as a new tumor growth in cases with initial total excision (no tumor detected at 3-month postoperative scan). A postoperative residual tumor was graded according to the Response Evaluation Criteria in Solid Tumors (RECIST) guidelines as progressive (at least 20% increase), stable, or shrunken (at least 30% decrease) during later follow-up [200].
6. Neuro-ophthalmology
An experienced neuro-ophthalmologist assessed visual acuity and visual fields preoperatively in cases where impaired vision was confirmed by the patient when asked about it and/or the pituitary tumor was in contact with the optic nerve(s) or chiasm, as assessed by MRI. All patients presenting with impaired visual fields and/or impaired visual acuity were re-examined postoperatively. Preoperative visual acuity/visual fields were classified as either normal or impaired. For study purposes, a single variable was formulated indicating either normal visual function or impaired function (any function, any degree). Furthermore, the postoperative outcome was categorized as “normal”, “normalized”, “improved”, “unchanged”, or “further impaired”. The postoperative assessment took place 3-12 months after surgery.
7. Histopathology
All tumor samples were verified according to WHO classification [2] as benign pituitary adenomas by an experienced neuropathologist. However,

60
immunohistochemistry (pituitary hormones, p53 and MIB-1) was not routinely performed during the first half of the study period.
8. Statistical methods
Results are given as mean, range, and standard deviation for continuous variables and as frequency for categorical variables. Data were analyzed using SPSS 22 (SPSS Inc., Chicago, IL, USA) software. The Tobit model was estimated with Limdep 7 (Econometric Software Inc., Plainview, NY, USA). Publication I: Pairwise comparisons of categorical variables were made using Fischer’s exact and x2 tests. The distributions of continuous variables were visually checked, and a subsequent log-transformation was used for operation time. The multivariate analysis was performed using linear and logistic regression analysis. Means among three or more groups were compared using one-way analysis of variance test (ANOVA). A p-value of <0.05 was regarded as significant. Publications II and III: The statistical significances of the differences in the means of continuous variables between different groups were calculated using independent samples t-test. Pearson correlation coefficient was used in calculating correlations between continuous variables. A Tobit model was utilized to estimate the influence of different factors on HRQoL (15D score as dependent variable). A p-value of <0.05 was regarded as significant.
9. Ethical aspects
The study protocol was approved by the institutional review board and the local committee of ethics (registration no. 68/2012). Each patient gave signed informed consent for participation in the study.
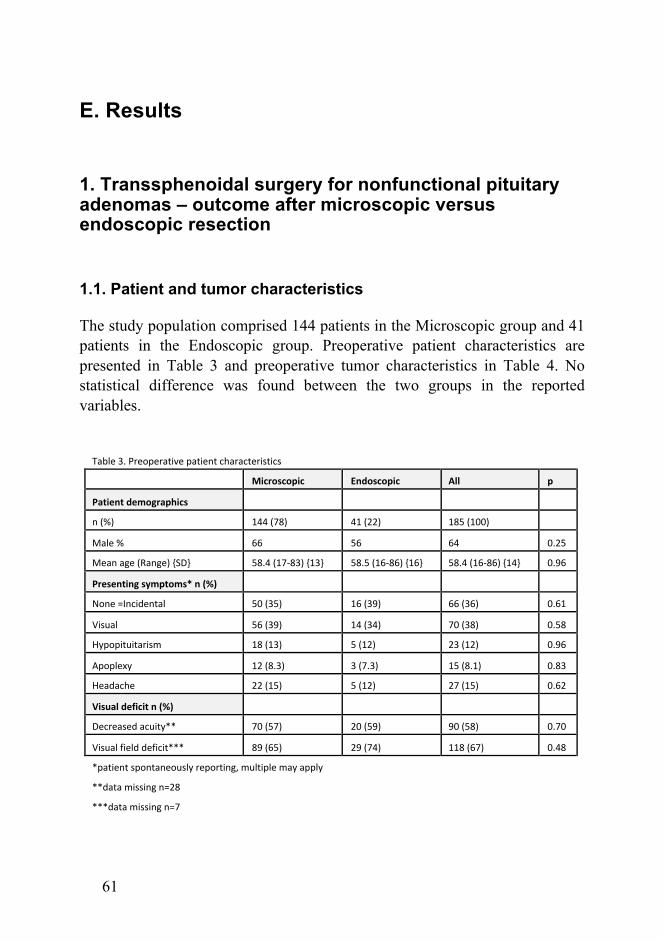
61
E. Results
1. Transsphenoidal surgery for nonfunctional pituitary adenomas – outcome after microscopic versus endoscopic resection
1.1. Patient and tumor characteristics
The study population comprised 144 patients in the Microscopic group and 41 patients in the Endoscopic group. Preoperative patient characteristics are presented in Table 3 and preoperative tumor characteristics in Table 4. No statistical difference was found between the two groups in the reported variables.
Table&3.&Preoperative&patient&characteristics& &
&& Microscopic( Endoscopic( All( p(
Patient(demographics( & & & &
n&(%)& 144&(78)& 41&(22)& 185&(100)& &
Male&%& 66& 56& 64& 0.25&
Mean&age&(Range)&{SD}& 58.4&(17F83)&{13}& 58.5&(16F86)&{16}& 58.4&(16F86)&{14}& 0.96&
Presenting(symptoms*(n((%)( & & & &
None&=Incidental& 50&(35)& 16&(39)& 66&(36)& 0.61&
Visual& 56&(39)& 14&(34)& 70&(38)& 0.58&
Hypopituitarism& 18&(13)& 5&(12)& 23&(12)& 0.96&
Apoplexy& 12&(8.3)& 3&(7.3)& 15&(8.1)& 0.83&
Headache& 22&(15)& 5&(12)& 27&(15)& 0.62&
Visual(deficit(n((%)( & & & &
Decreased&acuity**& 70&(57)& 20&(59)& 90&(58)& 0.70&
Visual&field&deficit***& 89&(65)& 29&(74)& 118&(67)& 0.48&
*patient&spontaneously&reporting,&multiple&may&apply& &
**data&missing&n=28& &
***data&missing&n=7& &
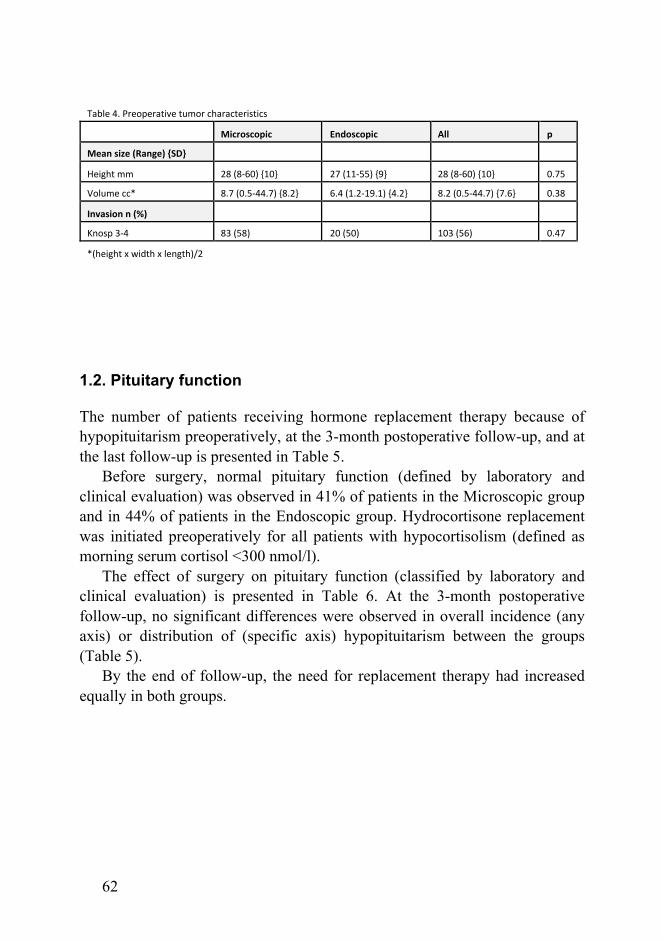
62
1.2. Pituitary function
The number of patients receiving hormone replacement therapy because of hypopituitarism preoperatively, at the 3-month postoperative follow-up, and at the last follow-up is presented in Table 5.
Before surgery, normal pituitary function (defined by laboratory and clinical evaluation) was observed in 41% of patients in the Microscopic group and in 44% of patients in the Endoscopic group. Hydrocortisone replacement was initiated preoperatively for all patients with hypocortisolism (defined as morning serum cortisol <300 nmol/l).
The effect of surgery on pituitary function (classified by laboratory and clinical evaluation) is presented in Table 6. At the 3-month postoperative follow-up, no significant differences were observed in overall incidence (any axis) or distribution of (specific axis) hypopituitarism between the groups (Table 5).
By the end of follow-up, the need for replacement therapy had increased equally in both groups.
Table&4.&Preoperative&tumor&characteristics& &
&& Microscopic( Endoscopic( All( p(
Mean(size((Range)({SD}( & & & &
Height&mm& 28&(8:60)&{10}& 27&(11:55)&{9}& 28&(8:60)&{10}& 0.75&
Volume&cc*&& 8.7&(0.5:44.7)&{8.2}& 6.4&(1.2:19.1)&{4.2}& 8.2&(0.5:44.7)&{7.6}& 0.38&
Invasion(n((%)( & & & &
Knosp&3:4& 83&(58)& 20&(50)& 103&(56)& 0.47&
*(height&x&width&x&length)/2& &
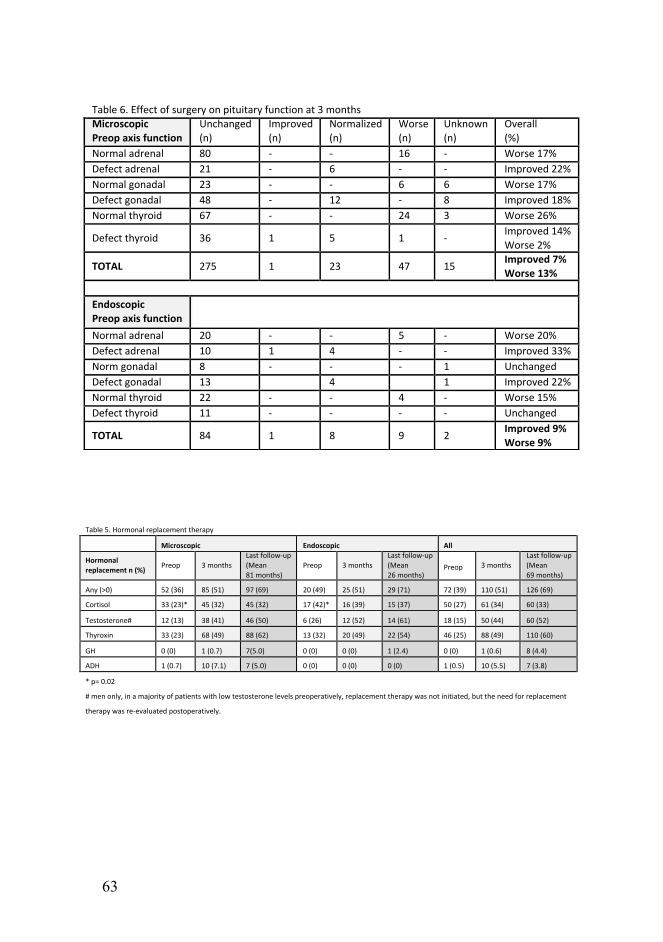
63
Table&6.&Effect&of&surgery&on&pituitary&function&at&3&months&
Microscopic(Preop(axis(function(
Unchanged&
(n)&
Improved&
(n)&
Normalized&
(n)&
Worse&
(n)&
Unknown&
(n)&
Overall&
(%)&
Normal&adrenal& 80& H& H& 16& H& Worse&17%&
Defect&adrenal& 21& H& 6& H& H& Improved&22%&
Normal&gonadal& 23& H& H& 6& 6& Worse&17%&
Defect&gonadal& 48& H& 12& H& 8& Improved&18%&
Normal&thyroid& 67& H& H& 24& 3& Worse&26%&
Defect&thyroid& 36& 1& 5& 1& H&Improved&14%&
Worse&2%&
TOTAL( 275& 1& 23& 47& 15&Improved(7%(Worse(13%&
&
Endoscopic(Preop(axis(function( &
Normal&adrenal& 20& H& H& 5& H& Worse&20%&
Defect&adrenal& 10& 1& 4& H& H& Improved&33%&
Norm&gonadal& 8& H& H& H& 1& Unchanged&
Defect&gonadal& 13& & 4& & 1& Improved&22%&
Normal&thyroid& 22& H& H& 4& H& Worse&15%&
Defect&thyroid& 11& H& H& H& H& Unchanged&
TOTAL( 84& 1& 8& 9& 2&Improved(9%(Worse(9%&
Table&5.&Hormonal&replacement&therapy&
&& Microscopic( Endoscopic( All(
Hormonal(replacement(n((%)( Preop& 3&months&
Last&follow9up&
(Mean&
81&months)&
Preop& 3&months&
Last&follow9up&
(Mean&
26&months)&Preop& 3&months&
Last&follow9up&
(Mean&
69&months)&
Any&(>0)& 52&(36)& 85&(51)& 97&(69)& 20&(49)& 25&(51)& 29&(71)& 72&(39)& 110&(51)& 126&(69)&
Cortisol& 33&(23)*& 45&(32)& 45&(32)& 17&(42)*& 16&(39)& 15&(37)& 50&(27)& 61&(34)& 60&(33)&
Testosterone#& 12&(13)& 38&(41)& 46&(50)& 6&(26)& 12&(52)& 14&(61)& 18&(15)& 50&(44)& 60&(52)&
Thyroxin& 33&(23)& 68&(49)& 88&(62)& 13&(32)& 20&(49)& 22&(54)& 46&(25)& 88&(49)& 110&(60)&
GH& 0&(0)& 1&(0.7)& 7(5.0)& 0&(0)& 0&(0)& 1&(2.4)& 0&(0)& 1&(0.6)& 8&(4.4)&
ADH& 1&(0.7)& 10&(7.1)& 7&(5.0)& 0&(0)& 0&(0)& 0&(0)& 1&(0.5)& 10&(5.5)& 7&(3.8)&
*&p=&0.02&
#&men&only,&in&a&majority&of&patients&with&low&testosterone&levels&preoperatively,&replacement&therapy&was¬&initiated,&but&the&need&for&replacement&
therapy&was&re9evaluated&postoperatively.&
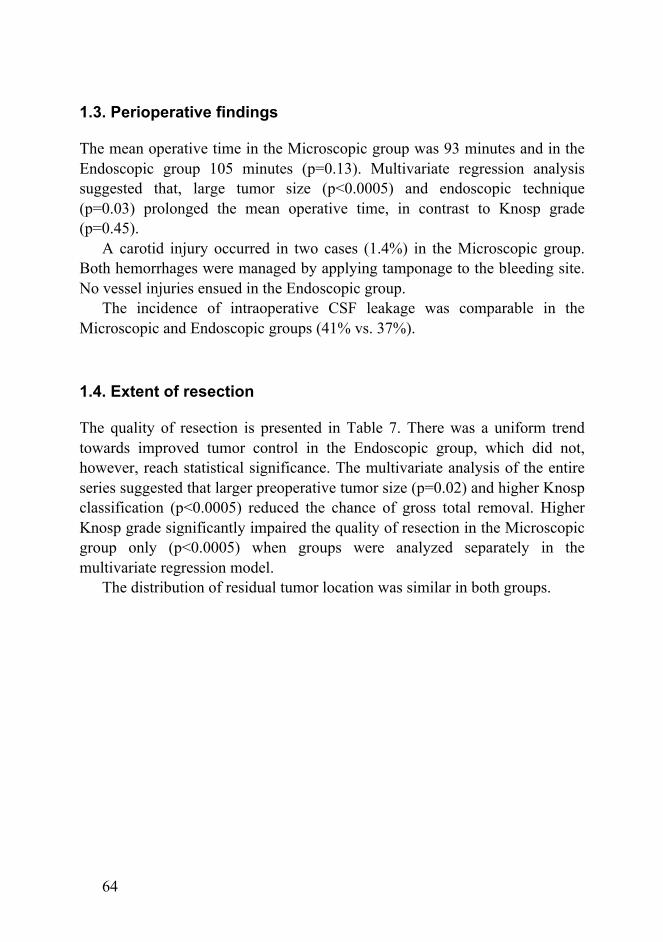
64
1.3. Perioperative findings
The mean operative time in the Microscopic group was 93 minutes and in the Endoscopic group 105 minutes (p=0.13). Multivariate regression analysis suggested that, large tumor size (p<0.0005) and endoscopic technique (p=0.03) prolonged the mean operative time, in contrast to Knosp grade (p=0.45).
A carotid injury occurred in two cases (1.4%) in the Microscopic group. Both hemorrhages were managed by applying tamponage to the bleeding site. No vessel injuries ensued in the Endoscopic group.
The incidence of intraoperative CSF leakage was comparable in the Microscopic and Endoscopic groups (41% vs. 37%).
1.4. Extent of resection
The quality of resection is presented in Table 7. There was a uniform trend towards improved tumor control in the Endoscopic group, which did not, however, reach statistical significance. The multivariate analysis of the entire series suggested that larger preoperative tumor size (p=0.02) and higher Knosp classification (p<0.0005) reduced the chance of gross total removal. Higher Knosp grade significantly impaired the quality of resection in the Microscopic group only (p<0.0005) when groups were analyzed separately in the multivariate regression model.
The distribution of residual tumor location was similar in both groups.
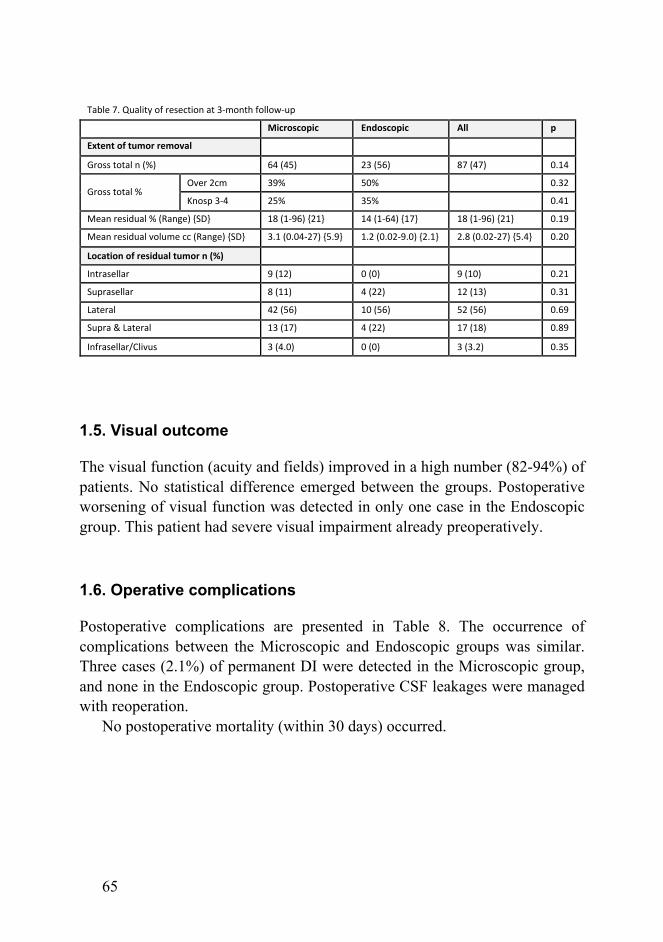
65
1.5. Visual outcome
The visual function (acuity and fields) improved in a high number (82-94%) of patients. No statistical difference emerged between the groups. Postoperative worsening of visual function was detected in only one case in the Endoscopic group. This patient had severe visual impairment already preoperatively.
1.6. Operative complications
Postoperative complications are presented in Table 8. The occurrence of complications between the Microscopic and Endoscopic groups was similar. Three cases (2.1%) of permanent DI were detected in the Microscopic group, and none in the Endoscopic group. Postoperative CSF leakages were managed with reoperation.
No postoperative mortality (within 30 days) occurred.
Table&7.&Quality&of&resection&at&35month&follow5up& &
&& Microscopic( Endoscopic( All( p(
Extent(of(tumor(removal( & & & &
Gross&total&n&(%)& 64&(45)& 23&(56)& 87&(47)& 0.14&
Gross&total&%&Over&2cm& 39%& 50%& & 0.32&
Knosp&354& 25%& 35%& & 0.41&
Mean&residual&%&(Range)&{SD}& 18&(1596)&{21}& 14&(1564)&{17}& 18&(1596)&{21}& 0.19&
Mean&residual&volume&cc&(Range)&{SD}& 3.1&(0.04527)&{5.9}& 1.2&(0.0259.0)&{2.1}& 2.8&(0.02527)&{5.4}& 0.20&
Location(of(residual(tumor(n((%)( & & & &
Intrasellar& 9&(12)& 0&(0)& 9&(10)& 0.21&
Suprasellar& 8&(11)& 4&(22)& 12&(13)& 0.31&
Lateral& 42&(56)& 10&(56)& 52&(56)& 0.69&
Supra&&&Lateral& 13&(17)& 4&(22)& 17&(18)& 0.89&
Infrasellar/Clivus& 3&(4.0)& 0&(0)& 3&(3.2)& 0.35&
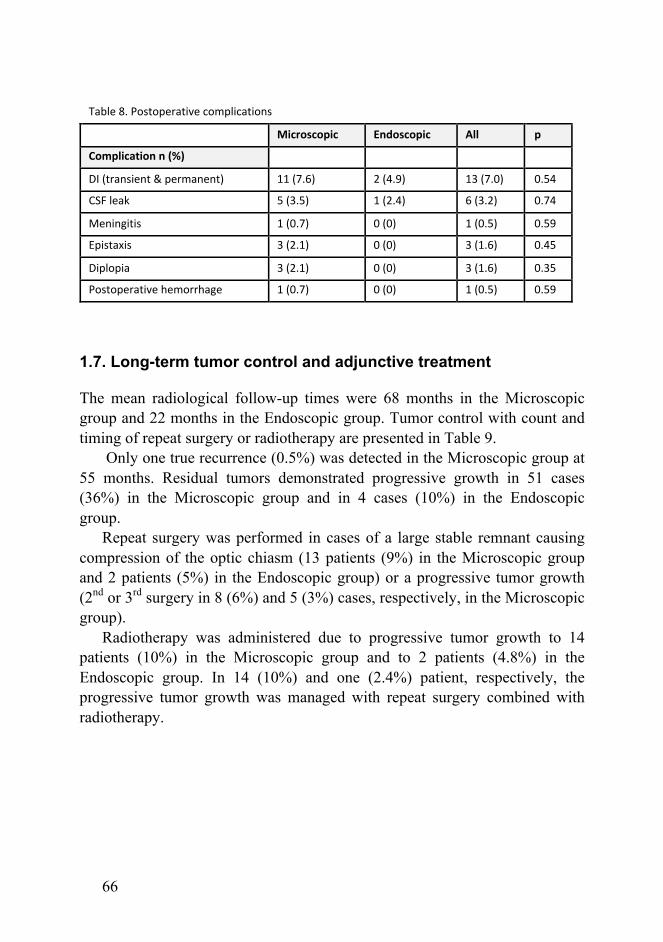
66
1.7. Long-term tumor control and adjunctive treatment
The mean radiological follow-up times were 68 months in the Microscopic group and 22 months in the Endoscopic group. Tumor control with count and timing of repeat surgery or radiotherapy are presented in Table 9.
Only one true recurrence (0.5%) was detected in the Microscopic group at 55 months. Residual tumors demonstrated progressive growth in 51 cases (36%) in the Microscopic group and in 4 cases (10%) in the Endoscopic group.
Repeat surgery was performed in cases of a large stable remnant causing compression of the optic chiasm (13 patients (9%) in the Microscopic group and 2 patients (5%) in the Endoscopic group) or a progressive tumor growth (2nd or 3rd surgery in 8 (6%) and 5 (3%) cases, respectively, in the Microscopic group).
Radiotherapy was administered due to progressive tumor growth to 14 patients (10%) in the Microscopic group and to 2 patients (4.8%) in the Endoscopic group. In 14 (10%) and one (2.4%) patient, respectively, the progressive tumor growth was managed with repeat surgery combined with radiotherapy.
Table&8.&Postoperative&complications! &
&& Microscopic! Endoscopic! All! p!
Complication!n!(%)! & & & &
DI&(transient&&&permanent)& 11&(7.6)& 2&(4.9)& 13&(7.0)& 0.54&
CSF&leak& 5&(3.5)& 1&(2.4)& 6&(3.2)& 0.74&
Meningitis& 1&(0.7)& 0&(0)& 1&(0.5)& 0.59&
Epistaxis& 3&(2.1)& 0&(0)& 3&(1.6)& 0.45&
Diplopia& 3&(2.1)& 0&(0)& 3&(1.6)& 0.35&
Postoperative&hemorrhage& 1&(0.7)& 0&(0)& 1&(0.5)& 0.59&
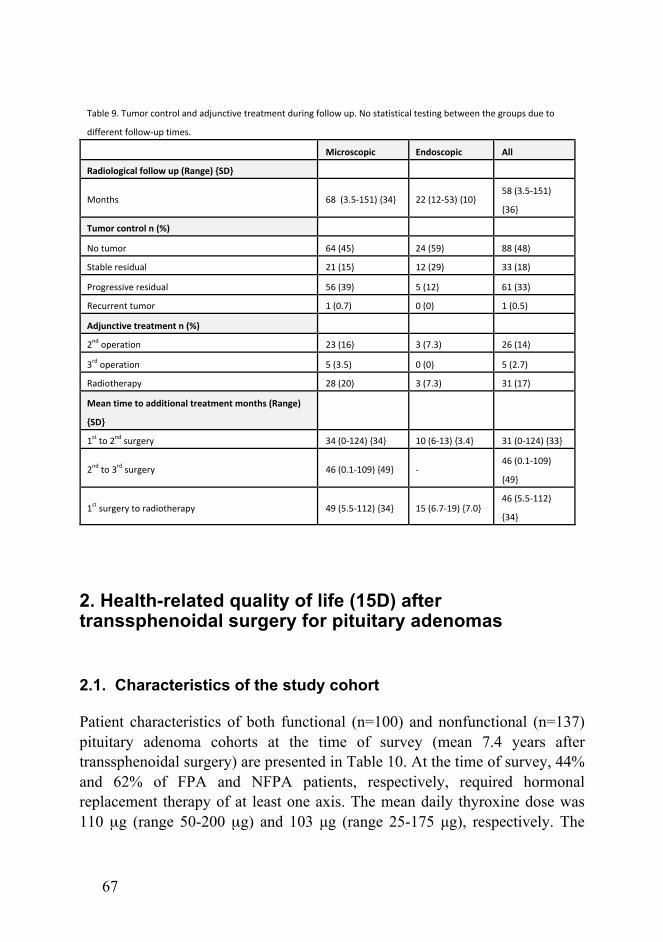
67
2. Health-related quality of life (15D) after transsphenoidal surgery for pituitary adenomas
2.1. Characteristics of the study cohort
Patient characteristics of both functional (n=100) and nonfunctional (n=137) pituitary adenoma cohorts at the time of survey (mean 7.4 years after transsphenoidal surgery) are presented in Table 10. At the time of survey, 44% and 62% of FPA and NFPA patients, respectively, required hormonal replacement therapy of at least one axis. The mean daily thyroxine dose was 110 µg (range 50-200 µg) and 103 µg (range 25-175 µg), respectively. The
Table&9.&Tumor&control&and&adjunctive&treatment&during&follow&up.&No&statistical&testing&between&the&groups&due&to&
different&follow;up×.!
& Microscopic! Endoscopic! All!
Radiological!follow!up!(Range)!{SD}! & & &
Months! 68&&(3.5;151)&{34}& 22&(12;53)&{10}&58&(3.5;151)&
{36}&
Tumor!control!n!(%)! & & &
No&tumor& 64&(45)& 24&(59)& 88&(48)&
Stable&residual& 21&(15)& 12&(29)& 33&(18)&
Progressive&residual& 56&(39)& 5&(12)& 61&(33)&
Recurrent&tumor& 1&(0.7)& 0&(0)& 1&(0.5)&
Adjunctive!treatment!n!(%)! & & &
2nd&operation& 23&(16)& 3&(7.3)& 26&(14)&
3rd&operation& 5&(3.5)& 0&(0)& 5&(2.7)&
Radiotherapy& 28&(20)& 3&(7.3)& 31&(17)&
Mean!time!to!additional!treatment!months!(Range)!
{SD}!& & &
1st&to&2nd&surgery& 34&(0;124)&{34}& 10&(6;13)&{3.4}& 31&(0;124)&{33}&
2nd&to&3rd&surgery& 46&(0.1;109)&{49}& ;&46&(0.1;109)&
{49}&
1st&surgery&to&radiotherapy& 49&(5.5;112)&{34}& 15&(6.7;19)&{7.0}&46&(5.5;112)&
{34}&
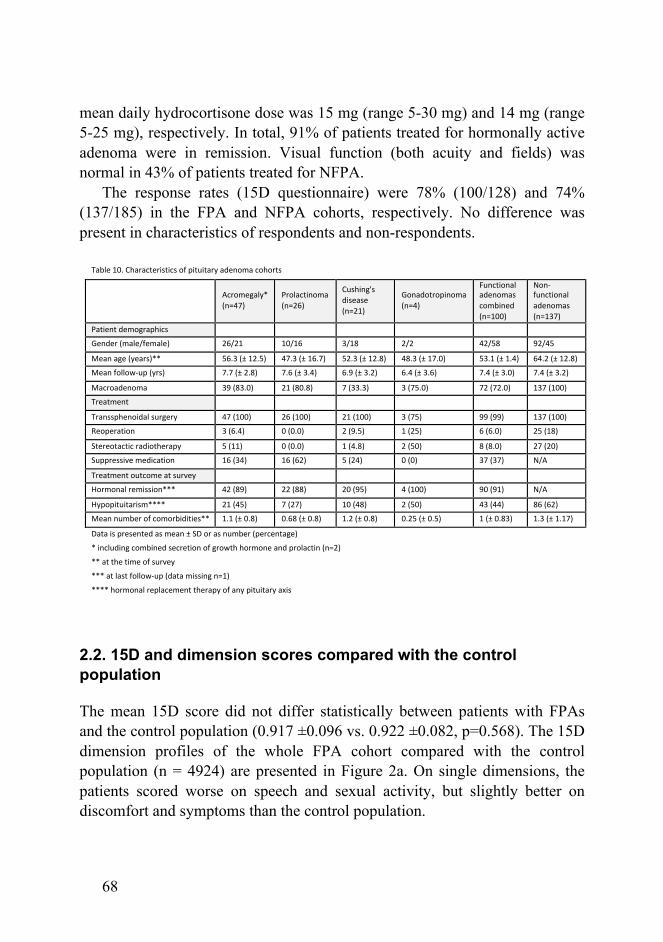
68
mean daily hydrocortisone dose was 15 mg (range 5-30 mg) and 14 mg (range 5-25 mg), respectively. In total, 91% of patients treated for hormonally active adenoma were in remission. Visual function (both acuity and fields) was normal in 43% of patients treated for NFPA.
The response rates (15D questionnaire) were 78% (100/128) and 74% (137/185) in the FPA and NFPA cohorts, respectively. No difference was present in characteristics of respondents and non-respondents.
2.2. 15D and dimension scores compared with the control population
The mean 15D score did not differ statistically between patients with FPAs and the control population (0.917 ±0.096 vs. 0.922 ±0.082, p=0.568). The 15D dimension profiles of the whole FPA cohort compared with the control population (n = 4924) are presented in Figure 2a. On single dimensions, the patients scored worse on speech and sexual activity, but slightly better on discomfort and symptoms than the control population.
Table&10.&Characteristics&of&pituitary&adenoma&cohorts&
&
&
Acromegaly*&&&&&&&&&&&&&&&
(n=47)&
Prolactinoma&&&&&&&&&&&&&&&&&&
(n=26)&
Cushing's&
disease&&&&&&&&&&&&&&&&&&&&&&&&
(n=21)&
Gonadotropinoma&&&&&&&&&&&&&&&&&&
(n=4)&
Functional&
adenomas&
combined&&&&&&&&&&&&&&&&&&
(n=100)&
NonH
functional&
adenomas&
(n=137)&
Patient&demographics& && && && && && &&
Gender&(male/female)& 26/21& 10/16& 3/18& 2/2& 42/58& 92/45&
Mean&age&(years)**& 56.3&(±&12.5)& 47.3&(±&16.7)& 52.3&(±&12.8)& 48.3&(±&17.0)& 53.1&(±&1.4)& 64.2&(±&12.8)&
Mean&followHup&(yrs)& 7.7&(±&2.8)& 7.6&(±&3.4)& 6.9&(±&3.2)& 6.4&(±&3.6)& 7.4&(±&3.0)& 7.4&(±&3.2)&
Macroadenoma& 39&(83.0)& 21&(80.8)& 7&(33.3)& 3&(75.0)& 72&(72.0)& 137&(100)&
Treatment&& && && && && && &&
Transsphenoidal&surgery& 47&(100)& 26&(100)& 21&(100)& 3&(75)& 99&(99)& 137&(100)&
Reoperation& 3&(6.4)& 0&(0.0)& 2&(9.5)& 1&(25)& 6&(6.0)& 25&(18)&
Stereotactic&radiotherapy& 5&(11)& 0&(0.0)& 1&(4.8)& 2&(50)& 8&(8.0)& 27&(20)&
Suppressive&medication& 16&(34)& 16&(62)& 5&(24)& 0&(0)& 37&(37)& N/A&
Treatment&outcome&at&survey& && && && && && &&
Hormonal&remission***& 42&(89)& 22&(88)& 20&(95)& 4&(100)& 90&(91)& N/A&
Hypopituitarism****& 21&(45)& 7&(27)& 10&(48)& 2&(50)& 43&(44)& 86&(62)&
Mean&number&of&comorbidities**& 1.1&(±&0.8)& 0.68&(±&0.8)& 1.2&(±&0.8)& 0.25&(±&0.5)& 1&(±&0.83)& 1.3&(±&1.17)&
Data&is&presented&as&mean&±&SD&or&as&number&(percentage)&
*&including&combined&secretion&of&growth&hormone&and&prolactin&(n=2)& &
**&at&the&time&of&survey& &
***&at&last&followHup&(data&missing&n=1)&
****&hormonal&replacement&therapy&of&any&pituitary&axis&
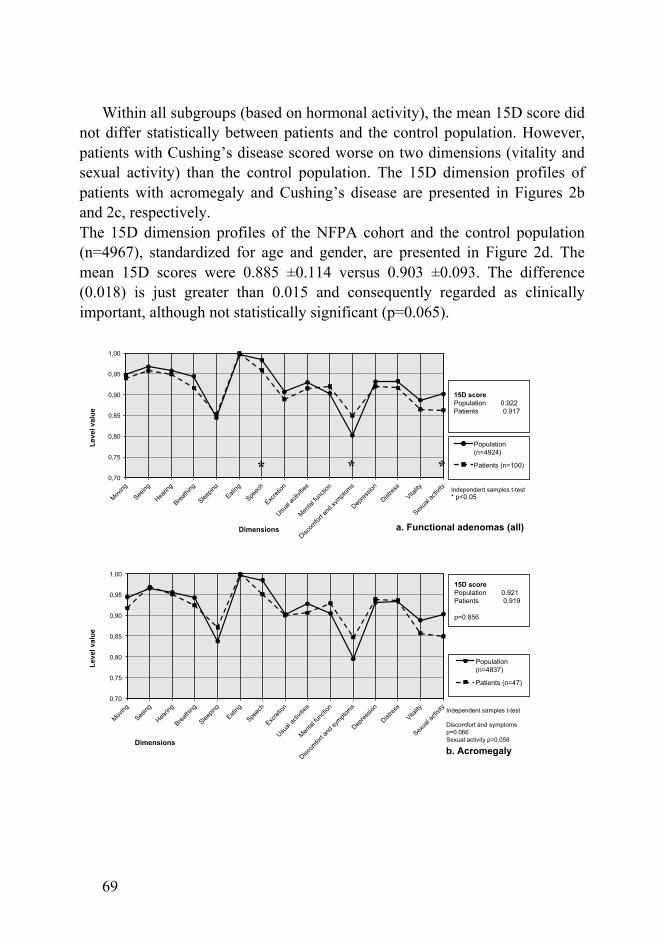
69
Within all subgroups (based on hormonal activity), the mean 15D score did not differ statistically between patients and the control population. However, patients with Cushing’s disease scored worse on two dimensions (vitality and sexual activity) than the control population. The 15D dimension profiles of patients with acromegaly and Cushing’s disease are presented in Figures 2b and 2c, respectively. The 15D dimension profiles of the NFPA cohort and the control population (n=4967), standardized for age and gender, are presented in Figure 2d. The mean 15D scores were 0.885 ±0.114 versus 0.903 ±0.093. The difference (0.018) is just greater than 0.015 and consequently regarded as clinically important, although not statistically significant (p=0.065).
0,70
0,75
0,80
0,85
0,90
0,95
1,00
Moving
Seeing
Hearin
g
Breathi
ng
Sleepin
g
Eating
Speec
h
Excret
ion
Usual
activ
ities
Mental
func
tion
Discom
fort a
nd sy
mptoms
Depres
sion
Distres
s
Vitality
Sexua
l acti
vity
Leve
l val
ue
Dimensions
Population (n=4924)
Patients (n=100)
15D score Population 0.922 Patients 0.917
a. Functional adenomas (all)
Independent samples t-test * p<0.05
* * *
0,70
0,75
0,80
0,85
0,90
0,95
1,00
Moving
Seeing
Hearin
g
Breathi
ng
Sleepin
g
Eating
Speec
h
Excret
ion
Usual
activ
ities
Mental
func
tion
Discom
fort a
nd sy
mptoms
Depres
sion
Distres
s
Vitality
Sexua
l acti
vity
Leve
l val
ue
Dimensions
Population (n=4837)
Patients (n=47)
15D score Population 0.921 Patients 0.919 p=0.856
b. Acromegaly
Independent samples t-test Discomfort and symptoms p=0.066 Sexual activity p=0.058
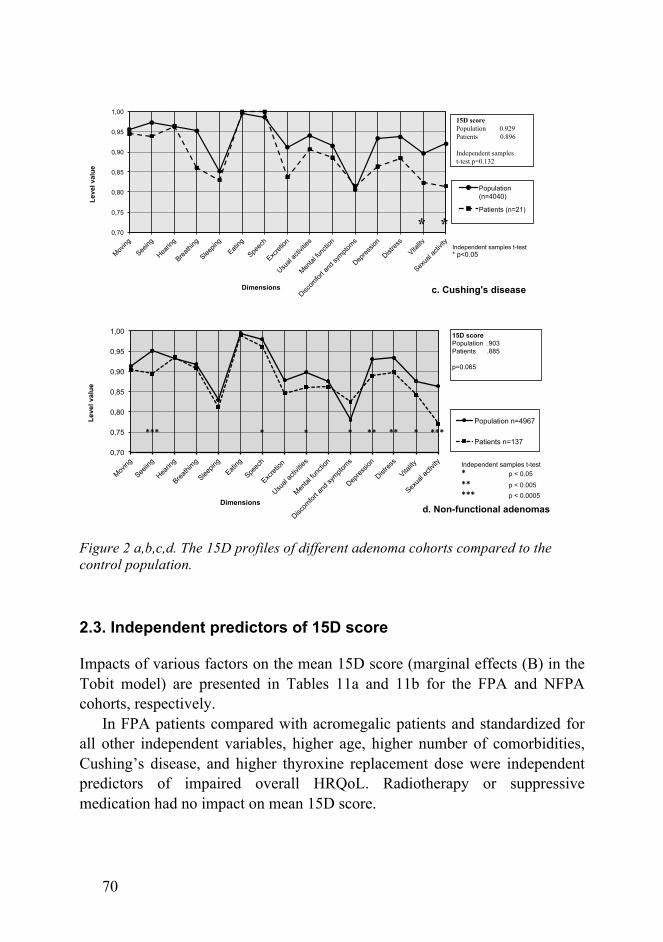
70
Figure 2 a,b,c,d. The 15D profiles of different adenoma cohorts compared to the control population.
2.3. Independent predictors of 15D score
Impacts of various factors on the mean 15D score (marginal effects (B) in the Tobit model) are presented in Tables 11a and 11b for the FPA and NFPA cohorts, respectively.
In FPA patients compared with acromegalic patients and standardized for all other independent variables, higher age, higher number of comorbidities, Cushing’s disease, and higher thyroxine replacement dose were independent predictors of impaired overall HRQoL. Radiotherapy or suppressive medication had no impact on mean 15D score.
0,70
0,75
0,80
0,85
0,90
0,95
1,00
Moving
Seeing
Hearin
g
Breathi
ng
Sleepin
g
Eating
Speec
h
Excret
ion
Usual
activ
ities
Mental
func
tion
Discom
fort a
nd sy
mptoms
Depres
sion
Distres
s
Vitality
Sexua
l acti
vity
Leve
l val
ue
Dimensions
Population (n=4040)
Patients (n=21)
15D score Population 0.929 Patients 0.896 Independent samples t-test p=0.132
c. Cushing's disease
* *Independent samples t-test * p<0.05
0,70
0,75
0,80
0,85
0,90
0,95
1,00
Moving
Seeiin
g
Hearin
g
Breathi
mg
Sleepin
g
Eating
Speec
h
Excret
ion
Usual
activ
ities
Mental
func
tion
Discom
fort a
nd sy
mptoms
Depres
sion
Distres
s
Vitality
Sexua
l acti
vity
Leve
l val
ue
Dimensions d. Non-functional adenomas
Population n=4967
Patients n=137
15D score Population .903 Patients .885 p=0.065
***"*" **" *"**"*"*"
Independent samples t-test * "p < 0.05"** "p < 0.005"*** "p < 0.0005"
***"

71
In NFPA patients, age, BMI, comorbidities, reoperation, and thyroxine substitution were all independent predictors of impaired mean 15D score. Hydrocortisone and testosterone substitution (males only) were positive predictors of mean 15D score. NFPA patients with and without hydrocortisone substitution demonstrated no differences in single 15D dimension scores. Males receiving testosterone replacement therapy scored higher on numerous single dimensions, including moving, breathing, excretion, mental function, and usual activities, than those not receiving testosterone replacement therapy.
Table&11&a."&The&independent&impact&(the&Tobit&model)&of&various&factors&on&the&15D&score&of&patients&with&FPAs.&
&& B& p@value&
Age&(years)& #0.0023" 0.0008"
Gender&(1=male,&0=female)& @0.0008& 0.9637&
Number&of&comorbidities& #0.0303" 0.0091"
Tumor&size&(1=macro,&0=micro)& @0.0415& 0.0514&
Follow@up&time&(years)& 0.0029& 0.2988&
Prolactinoma&(1=yes,&0=no)& @0.0042& 0.8438&
Cushing's&disease&(1=yes,&0=no)& #0.0488" 0.0341"
Hormonal&remission*&(1=yes,&0=no)& 0.0275& 0.3472&
Radiotherapy&(1=yes,&0=no)& 0.0114& 0.7002&
Suppressive&medication**&(1=yes,&0=no)& 0.0018& 0.9262&
Cortisone&replacement&(1=yes,&0=no)& @0.0002& 0.9942&
Growth&hormone&replacement&(1=yes,&0=no)& @0.0377& 0.4248&
Testosterone&replacement&(1=yes,&0=no)& 0.0404& 0.1884&
Thyroxine&dose&(µg/day)& #0.0005" 0.0024"
bold&indicates&statistical&significance&
*&at&last&follow@up&
**&at&the&time&of&the&survey&
Table&11&b.&Tobit,model&of&independent&factors&influencing&the&15D&score&of&patients&with&NFPAs.&! B& p,value&
Age! "0.0015! 0.0228!
Gender&(1=male,&0=female)& ,0.0381& 0.0562&
BMI& "0.0046! 0.0197!
Living&alone&(1=yes,&0=no)& ,0.0351& 0.0512&
Academic&education&(1=yes,&0=no)& 0.0128! 0.5102!
Diabetes&(1=yes,&0=no)& 0.0617! 0.0245!
Coronary&disease&(1=yes,&0=no)& ,0.0271! 0.2316!
Depression&(1=yes,&0=no)& "0.0852! 0.0004!
Cortisone&substitution&(1=yes,&0=no)& 0.0359! 0.0481!
Testosterone&substitution&(1=yes,&0=no)& 0.0880& <0.0005&
Thyroxine&substitution&(1=yes,&0=no)& "0.0583! 0.0018!
Operative&technique&(1=endoscopic,&0=microscopic)& 0.0164& 0.3593&
Reoperation&(1=yes,&0=no)& "0.0467& 0.0213&
Radiotherapy&(1=yes,&0=no)& 0.0200! 0.3604!
Normal&visual&function&(1=yes,&0=no)& 0.0098& 0.5507&
bold&indicates&statistical&significance&
72
F. Discussion
1. Transition from microscopic to endoscopic transsphenoidal surgery
The first part of this study describes our single-center experience of the technical modification in transsphenoidal surgery for NFPAs in which we compared the outcomes before and after the transition in the operative technique. The endoscopic endonasal skull base operations can be divided into five levels (I-V) according to the degree of technical difficulty and the demand of surgical skills [98]. Pituitary operations correspond to level II and represent the first and perhaps the longest step in the progressive gain of experience needed to advance to the next level. Despite our limited foregoing endoscopic experience, the initial results of the endoscopic technique were comparable to those achieved with the microscopic technique. Moreover, there was a trend towards a higher rate of gross total resection in the Endoscopic group. The preceding 30-year institutional experience in transsphenoidal surgery at Helsinki University Hospital probably provided a strong basis for upgrading the technique, allowing quick adaptation to differences in surgical access and depth perception.
Introducing a novel operative technique puts a surgeon at the bottom of a new learning curve [98, 201]. In this study, the multivariate analysis suggested that the tumor size (p<0.0005) was the strongest factor for longer mean operative time, and that the endoscopic technique was another independent factor (p=0.03) associated with a longer mean operative time. In earlier publications, endoscopic technique was associated with shorter operation times. However, preoperative tumor size or type was not included in their analyses [11, 137, 202, 203].
The midline structures, below the level of the diaphragm, are well visualized with both microscopic and endoscopic techniques. However, suprasellar and lateral cavernous sinus compartments are usually “in a blind spot” of the microscopic view, while the endoscope provides an outstanding panoramic view, a view that can be further improved with angled optics.
73
According to this study, the gross total tumor removal was negatively influenced by larger preoperative tumor size and higher Knosp grade, but not by the surgical technique. The invasive nature of the pituitary adenoma seems to be the strongest factor impairing the surgical result in terms of total removal [9, 123]. Gross total removal was achieved more frequently in the Endoscopic group than in the Microscopic group (56% vs. 45%), in agreement with pre-existing data (complete resection rates 36-83%) [68, 138, 204, 205]. This trend was observed also in the mean extent of resection (86% vs. 82%). In addition, we found that higher Knosp grade did not impair the quality of resection in the Endoscopic group. Overall, our results suggest a tendency towards improved quality of tumor removal in the Endoscopic group.
Although the early reports of the endoscopic technique revealed a high incidence of CSF leakage (up to 10%), this complication rate decreased after introduction of correct methods for repair of the sellar floor [9, 90, 98, 125]. More recently, microscopic and endoscopic approaches have generally ranked equally regarding postoperative CSF leakage [10, 11, 125, 137]. In our series, we found no difference in postoperative CSF leakage between the two groups (3.5% vs. 2.4%), indicating that low rates of CSF leakage can be maintained even in early series of the endoscopic technique.
There were two carotid artery injuries in the present series. Both occurred in the Microscopic group (1.4%). The frequent use of micro-Doppler for localizing the carotid arteries exclusively in the Endoscopic group may explain the difference. In a recent meta-analysis by Ammirati et al. [10] that compared short-term complications between the techniques, the only significant difference was a 3-fold risk of vascular complications with the endoscopic technique (1.6% vs. 0.5%). The authors suggested that this could be due to a more extensive sphenoid exposure of the carotid optic recess or to the lack of three-dimensional depth perception during suprasellar dissection. Our series does not support this conclusion since our vascular complications were the result of midline disorientation due to aberrant anatomy.
We found that the need for hormonal substitution was equally distributed between the groups over time. The effect of surgery on overall pituitary function (assessed 3 months postoperatively) was slightly adverse in the Microscopic group (7% improved, 13% worse) and neutral in the Endoscopic group (9% improved, 9% worse). The proportion of hypopituitary patients (any one hormonal axis affected) increased after surgery from 59% to 65%
74
within the Microscopic group and from 56% to 61% within the Endoscopic group. The existing data on the effect of transsphenoidal surgery on pituitary function are not uniform. Some report a neutral effect similar to our series [9, 132], but others [123, 138] describe overall improvement between 33% and 72% and worsening between 1.5% and 7.5% of the separate pituitary axes. The discrepancies can be explained by the application of diverse endocrine tests (or no tests at all), by various criteria for the diagnosis of hypopituitarism, or by different surgical skills/technique. Transient postoperative DI, requiring at least one dose of desmopressin, was detected in 7.6% and 4.9% of microscopic and endoscopic cases, respectively. This corresponds well to the figures reported earlier for both techniques [10, 123, 125].
At the end of follow-up (mean 68 months for microscopic cases and 22 months for endoscopic cases), the need for replacement therapy had further increased in both groups. At this later stage, hypopituitarism is the result of the combined treatments (radiotherapy, repeat surgeries). Especially radiotherapy is known to have a harmful effect on pituitary function over time [72, 129].
In this study, the ophthalmological outcome was very good in both groups; 90% of previously impaired visual fields and acuity either normalized or improved. Our finding is in line with earlier reports [9, 86, 123, 125] and supports the conclusion that the optic chiasm can be successfully decompressed with either of the transsphenoidal techniques.
A recent retrospective and uncontrolled study of untreated NFPAs (n=66) indicated tumor progression in 58% of patients during a mean follow-up period of 4.3 years [206]. The overall median annual growth rate was 0.8 mm/year (range 0.1-7.7 mm/year). Surgical series of treated NFPAs report progression of residual tumor in 8-70% (mean 43%) of cases during a 5-year postoperative follow-up [64]. We found tumor progression in 33% of our NFPA cohort (both groups combined) during a mean follow-up of 4.8 years. Due to different follow-up times between the Microscopic and Endoscopic groups (mean 5.7 vs. 1.8 years), no statistical comparisons were performed regarding medium- to long-term tumor control or pituitary function. Taken together, this data suggests that some NFPAs (naïve or residual), especially in elderly patients without tumor compression of the optic chiasm, may be managed conservatively with monitoring of pituitary function and serial neuro-ophthalmological and MRI studies. On the other hand, many NFPAs
75
tend to progress, which favors aggressive management with either gross total surgical removal or supplemented with STR.
Outcomes after microscopic and endoscopic transsphenoidal pituitary surgery have been described in numerous publications. Yet, to date, there is no proof of the superiority of one technique over the other, with good results achieved with both techniques [71, 97, 123, 125, 138, 204, 207, 208]. However, several factors distinguish the microscopic from the endoscopic technique, and many of them are difficult (or impossible) to measure using scientific or statistical methods. From the surgeon’s (and the patient’s) point of view, the endoscopic technique can be preferred for numerous reasons. The anterior nasal structures may be better preserved. Since the approach is guided by anatomic structures, the need for fluoroscopy or neuronavigation is infrequent. The visual field and quality is superior to the microscopic view, enabling the technique to be utilized on more extensive tumors of the sellar region. Introducing instruments via both nostrils allows more precise microsurgical dissection as there is a wider and more comfortable range of movements than with a single tubular microscopic access through the nasal speculum. Furthermore, the assistants, students, and the entire surgical team can see and follow the surgical procedure through the same high-quality endoscopic videostream.
2. Health-related quality of life (15D) after transsphenoidal surgery for pituitary adenoma
The second part of our study compared the HRQoL of patients operated on for a pituitary adenoma with that of the general population. In addition, we estimated the independent factors affecting the overall HRQoL in our patients. Most existing data suggests that HRQoL is impaired after treatment of both FPA [170, 174, 175, 183, 184, 209] and NFPA [188, 189, 210, 211]. In this study we showed that the current treatment options allow normal or near-normal HRQoL to be achieved in patients with FPAs and NFPAs after transsphenoidal surgery as a primary treatment.
The 15D. We chose to measure the HRQoL with the 15D questionnaire, which is a generic instrument [212], unlike the AcroQoL and other disease-specific questionnaires [165, 187]. The major advantage of the 15D is that it
76
allows us to compare our results with those of large, age- and gender-adjusted samples of the Finnish general population, recently compiled from the Finnish Health 2011 Survey [213]. In addition, the use of the 15D enabled indirect comparisons with the previous studies demonstrating impaired HRQoL in Finnish patients with acromegaly [214] and different pituitary adenoma subgroups [172].
Overall HRQoL. Our observation that the overall HRQoL of FPA patients after several years (mean 7.4 years) is similar to that of the general population is probably the result of two main factors: high remission rates (overall 91%) and optimal/physiological replacement therapy for hypopituitarism. Despite using strict remission criteria [39], high remission rates were anticipated in the acromegalic group (89%), and even higher rates in patients treated for Cushing’s disease (95%). However, patients with hormonally active disease (n=10) had HRQoL scores similar to patients in remission. This may seem conflicting, but this small subgroup of patients with active disease was significantly younger than those in remission, and younger age was a strong positive predictor of HRQoL in the multivariate analysis.
In concordance with FPA patients, the overall HRQoL of our NFPA patients could be regarded as near-normal compared with that of the general population. The difference in total 15D scores exceeded 0.015, which is considered the smallest clinically relevant difference [215], although the difference was not statistically significant (p=0.065). Our findings are in line with another recent series, suggesting that it is possible to achieve near-normal HRQoL in surgically treated NFPA patients under regular follow-up and care in specialized pituitary centers [190].
Comorbidities. Our data clearly indicate that age and comorbidities are independent predictors of impaired overall HRQoL in PA patients. Over two-thirds of our FPA and NFPA patients had at least one comorbidity and one-third had two or more. The negative impact of various comorbidities on the overall HRQoL has been previously demonstrated [216]. Especially depression has a strong adverse effect on overall HRQoL and on mental components of functioning [217]. Similarly, several studies have demonstrated that the overall HRQoL in PA patients deteriorates with age [169, 188, 190, 191].
An association between BMI and impaired 15D score was apparent in multivariate (p=0.020) analysis in our NFPA patients. The mean BMI of this
77
cohort was 26.9, which is close to the national average [218]. The correlation between impaired HRQoL and obesity is likewise well acknowledged [219, 220].
Hypopituitarism and replacement therapy. Some [169, 188, 221], but not all [190, 194], previous studies have found hypopituitarism to be associated with impaired HRQoL. Hypopituitarism required (any) treatment in 62% of our NFPA patients, compared with the greater proportions of 73%, 87% and 93% in previously published Danish [191], British [194], and Dutch [188] studies, respectively. The need for (any) replacement therapy was lower in our FPA patients than in our NFPA patients (44% vs. 62%), corresponding well to the literature reporting marked variation (range 27-52%) in (any) hypopituitarism in FPA patients [169, 174, 183, 184, 214]. This variation and the different treatment protocols and definitions for hypopituitarism likely explain the somewhat conflicting effects of hypopituitarism on overall HRQoL.
In our patients (both FPA and NFPA), the overall HRQoL was independently impaired by thyroxine replacement. This may reflect clinicians aiming to alleviate nonspecific symptoms, such as discomfort and fatigue, with thyroxine when free T4 concentrations are in the low normal range. The follow-up protocol of the present cohort included yearly evaluation of hormonal replacement therapy and dose adjustments when needed. We also detected a positive and independent impact of hydrocortisone replacement therapy on overall HRQoL in NFPA patients. Concurrently, the mean 15D scores were equivalent in NFPA patients receiving (30%) and not receiving (70%) hydrocortisone. The mean hydrocortisone replacement dosing used was rather low, 14 mg (range 5-25 mg). This positive association probably reflects optimal dosing in this study, as both excessively low and excessively high hydrocortisone replacement dosages may impair well-being. A similar correlation of overall HRQoL with hydrocortisone replacement was not detected in FPA patients. This may be due to the smaller number of FPA patients receiving replacement therapy, as compared with NFPA patients, or the effect of optimal dosing of hydrocortisone (mean 15 mg, range 5–30 mg) in FPA patients.
Males (NFPA) receiving testosterone replacement (40%) had significantly higher mean 15D score relative to NFPA patients not receiving testosterone replacement. This significant effect was seen in the following single
78
dimensions: moving, breathing, excretion, mental function, and usual activities (all p < 0.05). However, we did not detect a similar effect in male FPA patients, possibly due to the smaller proportion (29% vs. 40%) of patients receiving testosterone replacement therapy and their younger age (mean 56 vs. 65 years) compared with their NFPA counterparts. Parallel to our results, Capatina et al. reported that males (NFPA cohort) with non-replaced hypogonadism scored significantly worse on several dimensions of daily living than males getting substitution for hypogonadism [190]. Others have not studied this aspect in NFPA patients in detail [188, 191].
Sexual activity. Our finding that sexual activity is impaired in PA patients compared with controls is interesting; limited data regarding this function after treatment of PA exist. Most authors [162, 169, 188, 191] have used the SF-36 questionnaire, which does not assess sexual activity. Capatina et al. [190] used the NHP (along with the SF-36) questionnaire, which did include valuation of sex life (NHP second part). However, they did not find significant impairment in their NFPA study cohort (38% of male and 20% of female patients reporting sexual problems), but their control group was historical [222]. Previously, impairment of sexual function has been reported in only three studies: in acromegalic patients [214, 223] and in a small number of patients treated for prolactinoma [172]. The 15D profiles of our FPA subgroups, however, suggested impaired sexual activity in patients with Cushing’s disease (p=0.047), but not with acromegaly (p=0.058) or prolactinoma. In a sub-analysis of our patients, impaired sexual activity seemed to be related to male gender and number of comorbidities in both FPA and NFPA patients. In addition, we observed a significant association between hydrocortisone replacement therapy and impaired sexual activity in FPA patients, but somewhat discordantly, not in NFPA patients. It remains unclear whether this reflects a true correlation or is related to the effect mediated by Cushing’s disease in which up to 35% of patients were receiving hydrocortisone replacement at the time of survey.
Adenomas subtypes. Several studies have shown the deleterious effect of Cushing’s disease on HRQoL and mental condition, even after biochemical cure [180, 183, 184]. Likewise, our data suggest an independent negative effect of Cushing’s disease on overall HRQoL. Yet, the mean 15D score of patients with Cushing’s disease was equivalent to that of healthy controls, indicating that near-normal overall HRQoL can be achieved even in Cushing’s
79
disease. Since this subgroup was small, the results of our study must be interpreted with caution. The long-term hormonal remission in most Cushing’s patients best explains the exceptionally good overall HRQoL in this series.
In 2008, a Dutch report on a large number (n=403) of diverse adenomas, using the SF-36, suggested all subscales of HRQoL to be most impaired in acromegaly, followed by Cushing’s disease, compared with prolactinoma patients and NFPA patients [169]. Importantly, however, these authors did not distinguish the effect of comorbidities on HRQoL from the impact of the disease itself. Furthermore, their control population (n = 440) was much smaller (than in our study), and the absolute HRQoL scores could only be compared at the whole study group (all adenomas combined) level.
The largest study published on HRQoL in acromegalic patients using the 15D reported significantly impaired HRQoL compared with a large age- and gender-adjusted control population. This study cohort included 231 patients diagnosed between 1980 and 1999, of whom 92% underwent surgery as primary treatment, but only 51% were in remission and 33% had been given adjuvant radiotherapy, which was administered as conventional two-field radiotherapy in the majority of cases. The present contemporary series of acromegalic patients had all been operated on transsphenoidally, 89% were in remission, and 11% had been given modern fractionated stereotactic radiotherapy, but none conventional radiotherapy.
Two longitudinal studies demonstrated positive effects of improved hormonal control in acromegaly on overall HRQoL using the AcroQoL questionnaire during a 6-month follow-up [165, 224]. Conversely, another longitudinal study (4-year follow-up) using both the SF-36 and the AcroQoL reported progressive impairment of HRQoL in biochemically cured acromegalic patients, with previous radiotherapy being the predominant independent impairing factor [225]. These authors did not, however, compare the results with those of age- and gender-matched controls, nor did they consider the possible negative effect of other comorbidities on HRQoL in acromegaly. Likewise, the effect of SSA treatment on HRQoL remains unsettled, with opposing effects reported [179, 226]. Since only a small number (n=11) of our acromegalic patients were on SSA treatment at the time of survey, our study did not allow for definite conclusions regarding the effect of SSA treatment on HRQoL.
80
Previous reports on HRQoL of prolactinoma patients, the majority of whom were treated with dopamine agonists alone, are conflicting [169, 171]. Our data, albeit based on a small number of patients (n=26), indicate that HRQoL is not impaired in prolactinoma patients treated with transsphenoidal surgery a mean of 7.6 years earlier, 62% of whom had received adjuvant therapy, with a remission rate of 88%.
A Finnish study assessing HRQoL (and using 15D questionnaire) in patients with diverse pituitary adenomas suggested impaired HRQoL in patients with Cushing’s disease, prolactinoma, or acromegaly on SSA treatment, but not in NFPA patients [172]. This author’s conclusions are limited by the small number of patients in subgroups (45 FPA and 53 NFPA patients), the older series (surgery performed in 1992-2004), and the outdated remission criteria for the 22 acromegalic patients. In addition, 12% of their patients (n =12) had undergone craniotomy, compared with the almost exclusively transsphenoidally operated patients (only one craniotomy) in the present FPA cohort. Visual function. Decompression of the optic nerve(s) and chiasm is a major indication for surgery in patients with NFPA. Available data regarding the effect of visual function on HRQoL after pituitary surgery are limited and in part conflicting. Cross-sectional studies of NFPA patients have either suggested a negative effect of post-operative residual visual deficit (vs. no deficit) on HRQoL score (interests and hobbies subscale of the NHP),[190] or observed no effect of residual visual deficit on any HRQoL scores (SF-36, NHP, MFI). Our NFPA cohort had a significantly impaired single dimension of sight relative to controls, although the Tobit model did not suggest an independent impact of visual function on overall HRQoL. Similarly, in a study comparing cataract patients with controls, no differences emerged in the mean 15D score, but the single dimension of seeing was significantly impaired in the patient group [227].
Re-operation. We found an independent negative effect of re-operation on overall HRQoL. Some of our NFPA patients (18%) had to undergo re-operation, which required a transcranial approach in 28% of cases instead of the transsphenoidal route used in 72%. Due to invasive growth, the tumor remnant could be totally excised in only two cases (8%). In addition, 14 (56%) of the re-operated NFPA patients were given adjuvant stereotactic radiotherapy as a consequence of tumor remnant progression. This group of re-
81
operated NFPA patients was thus characterized by persistent disease, and some of them underwent craniotomy followed by radiotherapy. This strenuous treatment protocol and most patients being left with residual tumors presumably explain why re-operation impaired their overall HRQoL. Others have similarly reported impaired HRQoL after craniotomy or re-operation [190, 191]. In our FPA patients, re-operation was rare (n=6), and its effect on HRQoL was not investigated.
Surgical technique. The mean 15D score in our NFPA patients was not altered by the transsphenoidal technique (microscopic vs. endoscopic). This was expected since we (first part of this study) and others [10] have demonstrated that short-term outcome is similar with both techniques, and the survey took place a mean of 7.4 years after the surgery.
Radiotherapy. Stereotactic radiotherapy was administered to 8% of our FPA patients and 20% of NFPA patients. The Tobit model did not suggest any impairing effect on HRQoL in either group. Modern methods of delivering ionized radiation for tumor control may be safer than conventional two-field radiotherapy, and a recent large study with 42% of a NFPA cohort having undergone radiotherapy suggested, in line with our results, no effect on HRQoL [190].
3. Limitations of the study
The first part of our study is limited by the retrospective design, the absence of contemporary controls, and the disproportion of number of patients and mean follow-up times between the groups. Especially the relatively small number of endoscopic cases reduces the power of the study to detect differences between the groups. Although no difference between the surgeons emerged in operative time or extent of resection, we cannot exclude the impact of surgeon-specific differences. Due to a continuous learning curve in all surgical procedures, the primary surgeons might have built up surgical knowledge and skills in pituitary surgery during the 11-year course of the study. This could have prejudiced the results in favor of the Endoscopic group.
The main limitation of the second part of our study is the relatively small number of patients in the FPA subgroups. No recruitment bias occurred, however, as our cohort represents a consecutive surgical series in a single
82
institution covering a population of nearly 2 million people. Moreover, during an 11-year period no patients were lost to follow-up, and the response rate was as high as 78% in the FPA cohort. Due to the cross-sectional study design, we cannot comment on a possible change in HRQoL score during the course of pituitary disease and its treatment.

83
G. Conclusions and future prospects
With this study, we show a smooth transition from microscopic to endoscopic transsphenoidal surgery for pituitary adenomas, as we could maintain the previous level of outcome, with a trend towards improved quality of resection. Our initial endoscopic results serve as an encouraging example for those pituitary centers and surgeons considering an introduction of the endoscopic technique.
Findings in this study also suggest that current multimodal treatment protocols with optimized hormonal replacement therapies allow normal or near-normal overall HRQoL in patients with all types of pituitary adenomas. Older age and cumulative comorbidities are often the major determinants of HRQoL in patients treated for pituitary adenomas. The quest for an optimal surgical approach and technique for removing pituitary adenomas continues. Improved methods and applications of intraoperative viewing with ultra-high definition and 3D endoscopic videostreaming will help subspecialized pituitary surgeons in their attempts to remove tumors. A randomized study would be the gold standard for proving the superiority of a novel method. However, the endoscopic technique is already such an established method that we are unlikely to see its randomization against the microscopic approach. Instead, prospective data collection (electronic databases) will increase, and the outcomes in terms of hormonal function, tumor control, and HRQoL will be constantly monitored to evaluate treatment (cost)effectiveness. Novel targeted medication, especially for hormonally active adenomas, is being developed, and it remains to be seen how long surgical treatment will hold the status of principal treatment method for acromegaly or Cushing’s disease.
84
Acknowledgments
This work was carried out at the Departments of Neurosurgery and Endocrinology, Helsinki University Hospital, during 2011-2015. I thank the many people who have helped me and supported me during these arduous years.
I am especially grateful to:
Dr. Paul A Gardner for kindly agreeing to be my opponent at the defense.
Dr. Ville Vuorinen and Dr. Pia Jaatinen for pre-examining and critically revising this thesis, and Carol Ann Pelli for editing the language of the manuscript. The insightful observations, comments, and corrections considerably improved the final product.
Dr. Mika Niemelä and Dr. Camilla Schalin-Jäntti for excellent guidance
and supervision of this thesis. I was privileged to have you as my mentors. Dr. Juha Hernesniemi for giving me the idea for this project and the initial
push to start the work. I still can’t understand how you accomplished this. Dr. Leena Kivipelto for being my teacher both in the operating room and at
the writing desk. Thank you for introducing me to the world of pituitary surgery.
My co-authors and the numerous collaborators who made this project
possible. Dr. Elina Ritvonen for her generous help in putting together many missing pieces of puzzle. Dr. Satu Vehkavaara for her endocrinological expertise and help during the backbreaking phase of data collection. Dr. Riku Kivisaari for his genial help with the radiological assessment of thousands of scans. Dr. Risto Roine and Dr. Harri Sintonen for their vast knowledge of scientific methods. Emmi Tikkanen for her kind assistance with the statistical analysis. Dr. Kirsi Setälä for her expert interpretation of visual outcomes. Dr. Ashley Grossman for his superb and fast revision of the publication III. Colleagues Anita Gynther, Vesa Ilvesmäki, Päivi Kekäläinen, Otto Knutar, Pasi Salmela, Juha Saltevo, Lorenzo Sandini, and Marjo Tamminen for their
85
help with data collection. Jessica Peltonen and Terttu Säisä for their irreplaceable help with patient records. Dr. Simo Valtonen for shedding light on the early days of transsphenoidal surgery in Helsinki.
Dr. Minna Oinas, Dr. Päivi Koroknay-Pal, and Dr. Anna Piippo for their
understanding and flexibility in covering my absences from the pediatric service.
My friend and colleague Joona Varis for dropping me a line in May 1997
about a summer vacancy at the Department of Neurosurgery. There was no turning back after this point.
My family for unconditional love and understanding during this work. My
father, a true surgeon, and my mother, a true angel, for your influence on my career choice. My sons, Eetu and Roope, and my wife, Tiina, I am fortunate to be able to share my life with you.
This work has been financially supported by the Helsinki University
Hospital Research Fund, Novartis Finland Oyj, Helsingin Lääkäriyhdistys ry, and the Maire Taponen Foundation.
Helsinki, November 2015 Atte Karppinen
86
Appendices
Appendix 1
QUALITY OF LIFE QUESTIONNAIRE (15D©)/Harri Sintonen Please read all of the alternative responses to each question before marking with an x the alternative best describing your present health status. Answer all 15 questions in this manner, providing only one response for each question. QUESTION 1. MOBILITY 1() I am able to walk normally (without difficulty) indoors, outdoors, and on stairs. 2() I am able to walk without difficulty indoors, but outdoors and/or on stairs I have slight difficulties. 3() I am able to walk without help indoors (with or without an appliance), but outdoors and/or on stairs only with considerable difficulty or with help from others. 4() I am able to walk indoors only with help from others. 5() I am completely bedridden and unable to move about. QUESTION 2. VISION 1() I see normally, i.e. I can read newspapers and TV text without difficulty (with or without glasses). 2() I can read papers and/or TV text with slight difficulty (with or without glasses). 3() I can read papers and/or TV text with considerable difficulty (with or without glasses). 4() I cannot read papers or TV text with glasses or without, but I can see enough to walk about without guidance. 5() I cannot see enough to walk about without a guide, i.e. I am almost or completely blind. QUESTION 3. HEARING 1() I can hear normally, i.e. normal speech (with or without a hearing aid). 2() I hear normal speech with a little difficulty. 3() I hear normal speech with considerable difficulty; in conversation I need voices to be louder than normal.
87
4() I hear even loud voices poorly; I am almost deaf. 5() I am completely deaf. QUESTION 4. BREATHING 1() I am able to breathe normally, i.e. with no shortness of breath or other breathing difficulty. 2() I have shortness of breath during heavy work or sports, or when walking briskly on flat ground or slightly uphill. 3() I have shortness of breath when walking on flat ground at the same speed as others my age. 4() I get shortness of breath even after light activity, e.g. washing or dressing myself. 5() I have breathing difficulties almost all the time, even when resting. QUESTION 5. SLEEPING 1() I am able to sleep normally, i.e. I have no problems with sleeping. 2() I have slight problems with sleeping, e.g. difficulty in falling asleep, or sometimes waking at night. 3() I have moderate problems with sleeping, e.g. disturbed sleep, or the feeling that I have not slept enough. 4() I have great problems with sleeping, e.g. having to use sleeping pills often or routinely, or usually waking at night and/or too early in the morning. 5() I suffer from severe sleeplessness, e.g. sleep is almost impossible even with use of sleeping pills, or I stay awake most of the night. QUESTION 6. EATING 1() I am able to eat normally, i.e. with no help from others. 2() I am able to eat by myself with minor difficulty (e.g. slowly, clumsily, shakily, or with special appliances). 3() I need some help from another person with eating. 4() I am unable to eat by myself at all so I must be fed by another person. 5() I am unable to eat at all, so I am fed either by tube or intravenously. QUESTION 7. SPEECH 1() I am able to speak normally, i.e. clearly, audibly, and fluently. 2() I have slight speech difficulties, e.g. occasional fumbling for words, mumbling, or changes of pitch.
88
3() I can make myself understood, but my speech is disjointed, faltering, stuttering, or stammering. 4() Most people have great difficulty understanding my speech. 5() I can only make myself understood by gestures. QUESTION 8. EXCRETION 1() My bladder and bowel work normally and without problems. 2() I have slight problems with my bladder and/or bowel function, e.g. difficulties with urination, or loose or hard stools. 3() I have marked problems with bladder and/or bowel function, e.g. occasional 'accidents', or severe constipation or diarrhea. 4() I have serious problems with my bladder and/or bowel function, e.g. routine 'accidents', or need catheterization or enemas. 5() I have no control over my bladder and/or bowel function. QUESTION 9. USUAL ACTIVITIES 1() I am able to perform my usual activities (e.g. employment, studying, housework, free-time activities) without difficulty. 2() I am able to perform my usual activities slightly less effectively or with minor difficulty. 3() I am able to perform my usual activities much less effectively, with considerable difficulty, or incompletely. 4() I can only manage a small proportion of my previous usual activities. 5() I am unable to manage any of my previous usual activities. QUESTION 10. MENTAL FUNCTION 1() I am able to think clearly and logically, and my memory functions well. 2() I have slight difficulties in thinking clearly and logically, or my memory sometimes fails me. 3() I have marked difficulties in thinking clearly and logically, or my memory is somewhat impaired. 4() I have great difficulties in thinking clearly and logically, or my memory is seriously impaired. 5() I am permanently confused and disoriented in place and time. QUESTION 11. DISCOMFORT AND SYMPTOMS
89
1() I have no physical discomfort or symptoms, e.g. pain, ache, nausea, itching, etc. 2() I have mild physical discomfort or symptoms, e.g. pain, ache, nausea, itching, etc. 3() I have moderate physical discomfort or symptoms, e.g. pain, ache, nausea, itching, etc. 4() I have severe physical discomfort or symptoms, e.g. pain, ache, nausea, itching, etc. 5() I have unbearable physical discomfort or symptoms, e.g. pain, ache, nausea, itching, etc. QUESTION 12. DEPRESSION 1() I do not feel at all sad, melancholic, or depressed. 2() I feel slightly sad, melancholic, or depressed. 3() I feel moderately sad, melancholic, or depressed. 4() I feel very sad, melancholic, or depressed. 5() I feel extremely sad, melancholic, or depressed. QUESTION 13. DISTRESS 1() I do not feel at all anxious, stressed, or nervous. 2() I feel slightly anxious, stressed, or nervous. 3() I feel moderately anxious, stressed, or nervous. 4() I feel very anxious, stressed, or nervous. 5() I feel extremely anxious, stressed, or nervous. QUESTION 14. VITALITY 1() I feel healthy and energetic. 2() I feel slightly weary, tired, or feeble. 3() I feel moderately weary, tired, or feeble. 4() I feel very weary, tired, or feeble, almost exhausted. 5() I feel extremely weary, tired, or feeble, totally exhausted. QUESTION 15. SEXUAL ACTIVITY 1() My state of health has no adverse effect on my sexual activity. 2() My state of health has a slight effect on my sexual activity. 3() My state of health has a considerable effect on my sexual activity. 4() My state of health makes sexual activity almost impossible. 5() My state of health makes sexual activity impossible.
90
Appendix 2
TERVEYTEEN LIITTYVÄN ELÄMÄNLAADUN KYSELYLOMAKE (15D©)/Harri Sintonen (in Finnish) Ohje: Lukekaa ensin läpi huolellisesti kunkin kysymyksen kaikki vastausvaihtoehdot. Merkitkää sitten rasti (x) sen vaihtoehdon kohdalle, joka parhaiten kuvaa nykyistä terveydentilaanne. Menetelkää näin kaikkien kysymysten 1-15 kohdalla. Kustakin kysymyksestä rastitetaan siis yksi vaihtoehto. KYSYMYS 1. LIIKUNTAKYKY 1 ( ) Pystyn kävelemään normaalisti (vaikeuksitta) sisällä, ulkona ja portaissa. 2 ( ) Pystyn kävelemään vaikeuksitta sisällä, mutta ulkona ja/tai portaissa on pieniä vaikeuksia. 3 ( ) Pystyn kävelemään ilman apua sisällä (apuvälinein tai ilman), mutta ulkona ja/tai portaissa melkoisin vaikeuksin tai toisen avustamana. 4 ( ) Pystyn kävelemään sisälläkin vain toisen avustamana. 5 ( ) Olen täysin liikuntakyvytön ja vuoteenoma. KYSYMYS 2. NÄKÖ 1 ( ) Näen normaalisti eli näen lukea lehteä ja TV:n tekstejä vaikeuksitta (silmälaseilla tai ilman). 2 ( ) Näen lukea lehteä ja/tai TV:n tekstejä pienin vaikeuksin (silmälaseilla tai ilman). 3 ( ) Näen lukea lehteä ja/tai TV:n tekstejä huomattavin vaikeuksin (silmälaseilla tai ilman). 4 ( ) En näe lukea lehteä enkä TV:n tekstejä ilman silmälaseja tai niiden kanssa, mutta näen kulkea ilman opasta. 5 ( ) En näe kulkea oppaatta eli olen lähes tai täysin sokea. KYSYMYS 3. KUULO 1 ( ) Kuulen normaalisti eli kuulen hyvin normaalia puheääntä (kuulokojeella tai ilman). 2 ( ) Kuulen normaalia puheääntä pienin vaikeuksin. 3 ( ) Minun on melko vaikea kuulla normaalia puheääntä, keskustelussa on käytettävä normaalia kovempaa puheääntä. 4 ( ) Kuulen kovaakin puheääntä heikosti; olen melkein kuuro. 5 ( ) Olen täysin kuuro.
91
KYSYMYS 4. HENGITYS 1 ( ) Pystyn hengittämään normaalisti eli minulla ei ole hengenahdistusta eikä muita hengitysvaikeuksia. 2 ( ) Minulla on hengenahdistusta raskaassa työssä tai urheillessa, reippaassa kävelyssä tasamaalla tai lievässä ylämäessä. 3 ( ) Minulla on hengenahdistusta, kun kävelen tasamaalla samaa vauhtia kuin muut ikäiseni. 4 ( ) Minulla on hengenahdistusta pienenkin rasituksen jälkeen, esim. peseytyessä tai pukeutuessa. 5 ( ) Minulla on hengenahdistusta lähes koko ajan, myös levossa. KYSYMYS 5. NUKKUMINEN 1 ( ) Nukun normaalisti eli minulla ei ole mitään ongelmia unen suhteen. 2 ( ) Minulla on lieviä uniongelmia, esim. nukahtamisvaikeuksia tai satunnaista yöheräilyä. 3 ( ) Minulla on melkoisia uniongelmia, esim. nukun levottomasti tai uni ei tunnu riittävältä. 4 ( ) Minulla on suuria uniongelmia, esim. joudun käyttämään usein tai säännöllisesti unilääkettä, herään säännöllisesti yöllä ja/tai aamuisin liian varhain. 5 ( ) Kärsin vaikeasta unettomuudesta, esim. unilääkkeiden runsaasta käytöstä huolimatta nukkuminen on lähes mahdotonta, valvon suurimman osan yöstä. KYSYMYS 6. SYÖMINEN 1 ( ) Pystyn syömään normaalisti eli itse ilman mitään vaikeuksia. 2 ( ) Pystyn syömään itse pienin vaikeuksin (esim. hitaasti, kömpelösti, vavisten tai erityisapuneuvoin). 3 ( ) Tarvitsen hieman toisen apua syömisessä. 4 ( ) En pysty syömään itse lainkaan, vaan minua pitää syöttää. 5 ( ) En pysty syömään itse lainkaan, vaan minulle pitää antaa ravintoa letkun avulla tai suonensisäisesti. KYSYMYS 7. PUHUMINEN 1 ( ) Pystyn puhumaan normaalisti eli selvästi, kuuluvasti ja sujuvasti. 2 ( ) Puhuminen tuottaa minulle pieniä vaikeuksia, esim. sanoja on etsittävä tai ääni ei ole riittävän kuuluva tai se vaihtaa korkeutta.
92
3 ( ) Pystyn puhumaan ymmärrettävästi, mutta katkonaisesti, ääni vavisten, sammaltaen tai änkyttäen. 4 ( ) Muilla on vaikeuksia ymmärtää puhettani. 5 ( ) Pystyn ilmaisemaan itseäni vain elein. KYSYMYS 8. ERITYSTOIMINTA 1 ( ) Virtsarakkoni ja suolistoni toimivat normaalisti ja ongelmitta. 2 ( ) Virtsarakkoni ja/tai suolistoni toiminnassa on lieviä ongelmia, esim. minulla on virtsaamisvaikeuksia tai kova tai löysä vatsa. 3 ( ) Virtsarakkoni ja/tai suolistoni toiminnassa on melkoisia ongelmia, esim. minulla on satunnaisia virtsanpidätysvaikeuksia tai vaikea ummetus tai ripuli. 4 ( ) Virtsarakkoni ja/tai suolistoni toiminnassa on suuria ongelmia, esim. minulla on säännöllisesti "vahinkoja" tai peräruiskeiden tai katetroinnin tarvetta. 5 ( ) En hallitse lainkaan virtsaamista ja/tai ulostamista. KYSYMYS 9. TAVANOMAISET TOIMINNOT 1 ( ) Pystyn suoriutumaan normaalisti tavanomaisista toiminnoista (esim. ansiotyö, opiskelu, kotityö, vapaa-ajan toiminnot). 2 ( ) Pystyn suoriutumaan tavanomaisista toiminnoista hieman alentuneella teholla tai pienin vaikeuksin. 3 ( ) Pystyn suoriutumaan tavanomaisista toiminnoista huomattavasti alentuneella teholla tai huomattavin vaikeuksin tai vain osaksi. 4 ( ) Pystyn suoriutumaan tavanomaisista toiminnoista vain pieneltä osin. 5 ( ) En pysty suoriutumaan lainkaan tavanomaisista toiminnoista. KYSYMYS 10. HENKINEN TOIMINTA 1 ( ) Pystyn ajattelemaan selkeästi ja johdonmukaisesti ja muistini toimii täysin moitteettomasti. 2 ( ) Minulla on lieviä vaikeuksia ajatella selkeästi ja johdonmukaisesti, tai muistini ei toimi täysin moitteettomasti. 3 ( ) Minulla on melkoisia vaikeuksia ajatella selkeästi ja johdonmukaisesti, tai minulla on jonkin verran muistinmenetystä. 4 ( ) Minulla on suuria vaikeuksia ajatella selkeästi ja johdonmukaisesti, tai minulla on huomattavaa muistinmenetystä. 5 ( ) Olen koko ajan sekaisin ja vailla ajan tai paikan tajua.
93
KYSYMYS 11. VAIVAT JA OIREET 1 ( ) Minulla ei ole mitään vaivoja tai oireita, esim. kipua, särkyä, pahoinvointia, kutinaa jne. 2 ( ) Minulla on lieviä vaivoja tai oireita, esim. lievää kipua, särkyä, pahoinvointia, kutinaa jne. 3 ( ) Minulla on melkoisia vaivoja tai oireita, esim. melkoista kipua, särkyä, pahoinvointia, kutinaa jne. 4 ( ) Minulla on voimakkaita vaivoja tai oireita, esim. voimakasta kipua, särkyä, pahoinvointia, kutinaa jne. 5 ( ) Minulla on sietämättömiä vaivoja ja oireita, esim. sietämätöntä kipua, särkyä, pahoinvointia, kutinaa jne. KYSYMYS 12. MASENTUNEISUUS 1 ( ) En tunne itseäni lainkaan surulliseksi, alakuloiseksi tai masentuneeksi. 2 ( ) Tunnen itseni hieman surulliseksi, alakuloiseksi tai masentuneeksi. 3 ( ) Tunnen itseni melko surulliseksi, alakuloiseksi tai masentuneeksi. 4 ( ) Tunnen itseni erittäin surulliseksi, alakuloiseksi tai masentuneeksi. 5 ( ) Tunnen itseni äärimmäisen surulliseksi, alakuloiseksi tai masentuneeksi. KYSYMYS 13. AHDISTUNEISUUS 1 ( ) En tunne itseäni lainkaan ahdistuneeksi, jännittyneeksi tai hermostuneeksi. 2 ( ) Tunnen itseni hieman ahdistuneeksi, jännittyneeksi tai hermostuneeksi. 3 ( ) Tunnen itseni melko ahdistuneeksi, jännittyneeksi tai hermostuneeksi. 4 ( ) Tunnen itseni erittäin ahdistuneeksi, jännittyneeksi tai hermostuneeksi. 5 ( ) Tunnen itseni äärimmäisen ahdistuneeksi, jännittyneeksi tai hermostuneeksi. KYSYMYS 14. ENERGISYYS 1 ( ) Tunnen itseni terveeksi ja elinvoimaiseksi. 2 ( ) Tunnen itseni hieman uupuneeksi, väsyneeksi tai voimattomaksi. 3 ( ) Tunnen itseni melko uupuneeksi, väsyneeksi tai voimattomaksi. 4 ( ) Tunnen itseni erittäin uupuneeksi, väsyneeksi tai voimattomaksi, lähes "loppuun palaneeksi". 5 ( ) Tunnen itseni äärimmäisen uupuneeksi, väsyneeksi tai voimattomaksi, täysin "loppuun palaneeksi". KYSYMYS 15. SUKUPUOLIELÄMÄ
94
1 ( ) Terveydentilani ei vaikeuta mitenkään sukupuolielämääni. 2 ( ) Terveydentilani vaikeuttaa hieman sukupuolielämääni. 3 ( ) Terveydentilani vaikeuttaa huomattavasti sukupuolielämääni. 4 ( ) Terveydentilani tekee sukupuolielämäni lähes mahdottomaksi. 5 ( ) Terveydentilani tekee sukupuolielämäni mahdottomaksi
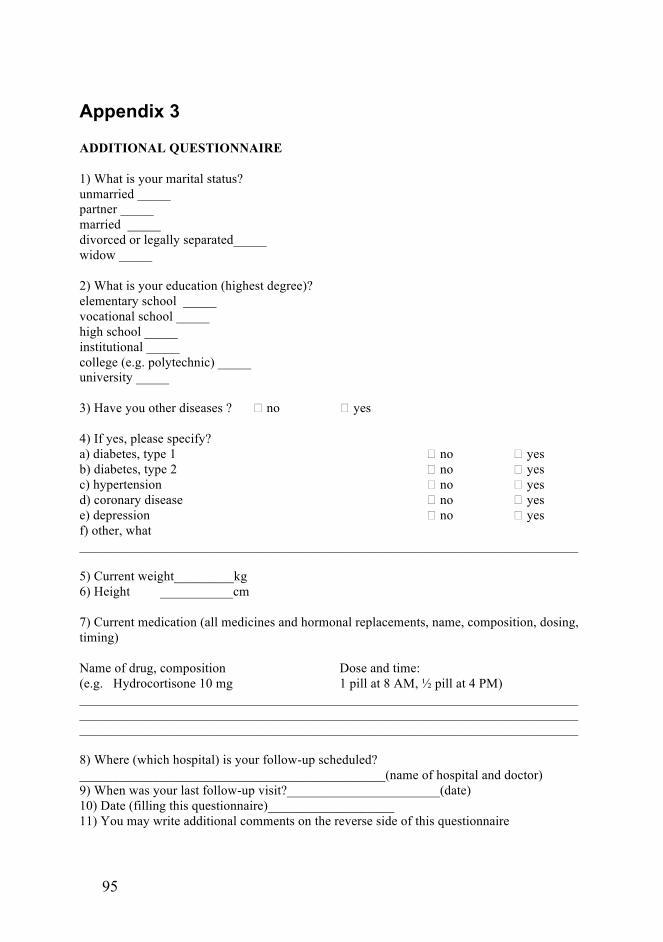
95
Appendix 3
ADDITIONAL QUESTIONNAIRE 1) What is your marital status? unmarried _____ partner _____ married _____ divorced or legally separated_____ widow _____ 2) What is your education (highest degree)? elementary school _____ vocational school _____ high school _____ institutional _____ college (e.g. polytechnic) _____ university _____ 3) Have you other diseases ? � no � yes 4) If yes, please specify? a) diabetes, type 1 � no � yes b) diabetes, type 2 � no � yes c) hypertension � no � yes d) coronary disease � no � yes e) depression � no � yes f) other, what ___________________________________________________________________________ 5) Current weight_________kg 6) Height ___________cm 7) Current medication (all medicines and hormonal replacements, name, composition, dosing, timing) Name of drug, composition Dose and time: (e.g. Hydrocortisone 10 mg 1 pill at 8 AM, ½ pill at 4 PM) _________________________________________________________________________________________________________________________________________________________________________________________________________________________________ 8) Where (which hospital) is your follow-up scheduled? ______________________________________________(name of hospital and doctor) 9) When was your last follow-up visit?_______________________(date) 10) Date (filling this questionnaire)___________________ 11) You may write additional comments on the reverse side of this questionnaire
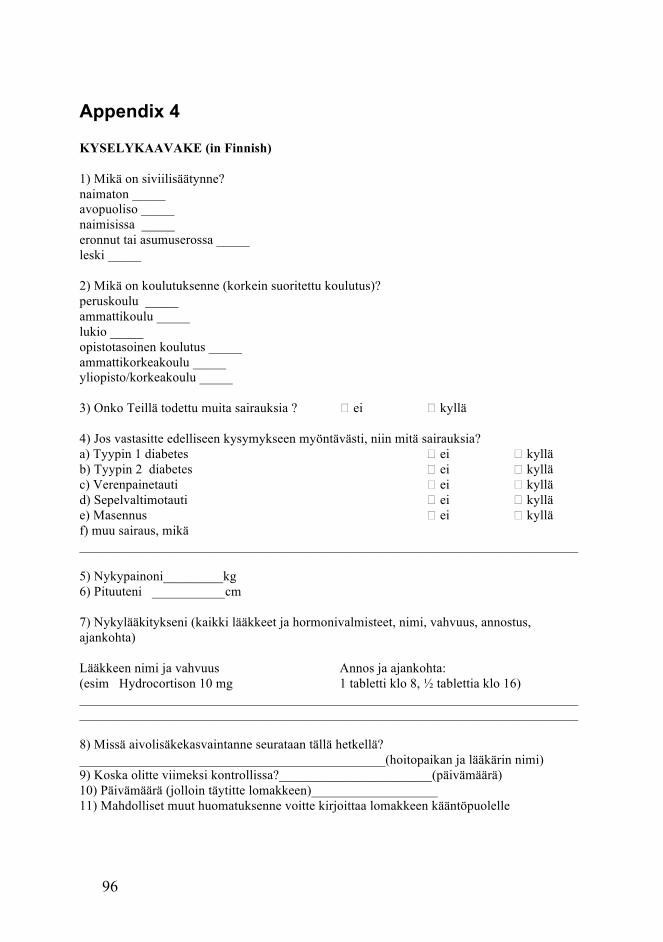
96
Appendix 4
KYSELYKAAVAKE (in Finnish) 1) Mikä on siviilisäätynne? naimaton _____ avopuoliso _____ naimisissa _____ eronnut tai asumuserossa _____ leski _____ 2) Mikä on koulutuksenne (korkein suoritettu koulutus)? peruskoulu _____ ammattikoulu _____ lukio _____ opistotasoinen koulutus _____ ammattikorkeakoulu _____ yliopisto/korkeakoulu _____ 3) Onko Teillä todettu muita sairauksia ? � ei � kyllä 4) Jos vastasitte edelliseen kysymykseen myöntävästi, niin mitä sairauksia? a) Tyypin 1 diabetes � ei � kyllä b) Tyypin 2 diabetes � ei � kyllä c) Verenpainetauti � ei � kyllä d) Sepelvaltimotauti � ei � kyllä e) Masennus � ei � kyllä f) muu sairaus, mikä ___________________________________________________________________________ 5) Nykypainoni_________kg 6) Pituuteni ___________cm 7) Nykylääkitykseni (kaikki lääkkeet ja hormonivalmisteet, nimi, vahvuus, annostus, ajankohta) Lääkkeen nimi ja vahvuus Annos ja ajankohta: (esim Hydrocortison 10 mg 1 tabletti klo 8, ½ tablettia klo 16) ______________________________________________________________________________________________________________________________________________________ 8) Missä aivolisäkekasvaintanne seurataan tällä hetkellä? ______________________________________________(hoitopaikan ja lääkärin nimi) 9) Koska olitte viimeksi kontrollissa?_______________________(päivämäärä) 10) Päivämäärä (jolloin täytitte lomakkeen)___________________ 11) Mahdolliset muut huomatuksenne voitte kirjoittaa lomakkeen kääntöpuolelle
97
References
1. Ezzat, S., S.L. Asa, W.T. Couldwell, C.E. Barr, W.E. Dodge, M.L.
Vance, and I.E. McCutcheon, The Prevalence of Pituitary Adenomas. Cancer, 2004. 101(3): p. 613-619.
2. Lloyd RJ, K.K., Young WF Jr, Farrell WE, Asa SL, Trouillas J, et al, Tumors of the Pituitary Gland, in Pathology and Genetics of Tumors of Endocrine Organs, L.R. DeLellis R, Heitz P, et al, Editor. 2004, International Agency for Research and Cancer: Lyon. p. 9–48.
3. Colao, A., S. Petersenn, J. Newell-Price, J.W. Findling, F. Gu, M. Maldonado, U. Schoenherr, D. Mills, L.R. Salgado, and B.M. Biller, A 12-Month Phase 3 Study of Pasireotide in Cushing's Disease. N Engl J Med, 2012. 366(10): p. 914-24.
4. van der Lely, A.J., R.K. Hutson, P.J. Trainer, G.M. Besser, A.L. Barkan, L. Katznelson, A. Klibanski, V. Herman-Bonert, S. Melmed, M.L. Vance, P.U. Freda, P.M. Stewart, K.E. Friend, D.R. Clemmons, G. Johannsson, S. Stavrou, D.M. Cook, L.S. Phillips, C.J. Strasburger, S. Hackett, K.A. Zib, R.J. Davis, J.A. Scarlett, and M.O. Thorner, Long-Term Treatment of Acromegaly with Pegvisomant, a Growth Hormone Receptor Antagonist. Lancet, 2001. 358(9295): p. 1754-9.
5. Ascoli, P. and F. Cavagnini, Hypopituitarism. Pituitary, 2006. 9(4): p. 335-342.
6. Cappabianca, P., L.M. Cavallo, D. Solari, V. Stagno, F. Esposito, and M. de Angelis, Endoscopic Endonasal Surgery for Pituitary Adenomas. World Neurosurgery, 2014. 82(6, Supplement): p. S3-S11.
7. Kari, E., N.M. Oyesiku, V. Dadashev, and S.K. Wise, Comparison of Traditional 2-Dimensional Endoscopic Pituitary Surgery with New 3-Dimensional Endoscopic Technology: Intraoperative and Early Postoperative Factors. Int Forum Allergy Rhinol, 2012. 2(1): p. 2-8.
8. Ding, D., R.M. Starke, and J.P. Sheehan, Treatment Paradigms for Pituitary Adenomas: Defining the Roles of Radiosurgery and Radiation Therapy. J Neurooncol, 2014. 117(3): p. 445-57.
9. Messerer, M., J.C. De Battista, G. Raverot, S. Kassis, J. Dubourg, V. Lapras, J. Trouillas, G. Perrin, and E. Jouanneau, Evidence of Improved Surgical Outcome Following Endoscopy for Nonfunctioning Pituitary Adenoma Removal. Neurosurgical Focus, 2011. 30(4): p. E11.
10. Ammirati, M., L. Wei, and I. Ciric, Short-Term Outcome of Endoscopic Versus Microscopic Pituitary Adenoma Surgery: A Systematic Review and Meta-Analysis. Journal of Neurology, Neurosurgery & Psychiatry, 2013. 84(8): p. 843-849.
98
11. Rotenberg, B., S. Tam, W.H.A. Ryu, and N. Duggal, Microscopic Versus Endoscopic Pituitary Surgery: A Systematic Review. The Laryngoscope, 2010. 120(7): p. 1292-1297.
12. de Divitiis, E., E.R. Laws, U. Giani, S.L. Iuliano, O. de Divitiis, and M.L. Apuzzo, The Current Status of Endoscopy in Transsphenoidal Surgery: An International Survey. World Neurosurg, 2014.
13. Sane, T., Aivolisäkkeen Etulohko, in Endokrinologia, M.S. Välimäki, Timo; Dunkel Leo, Editor. 2009, Duodecim: Helsinki.
14. Sane, T., Aivolisäkkeen Takalohko Ja Vesiaineenvaihdunta, in Endokrinologia, M.S. Välimäki, Timo; Dunkel Leo, Editor. 2009, Duodecim: Helsinki.
15. Edward H. Oldfield and Alexander O. Vortmeyer, Development of a Histological Pseudocapsule and Its Use as a Surgical Capsule in the Excision of Pituitary Tumors. Journal of Neurosurgery, 2006. 104(1): p. 7-19.
16. Krisht, A.F.H.M., Pathology of Sellar and Parasellar Tumours, in Pituitary Disorders: Comprehensive Management, A.F.T. Krisht, Georg T, Editor. 1999, Lippincott Williams & Wilkins: Baltimore. p. 99-113.
17. Asa, S.L. and S. Ezzat, The Cytogenesis and Pathogenesis of Pituitary Adenomas. Endocrine Reviews, 1998. 19(6): p. 798-827.
18. Alexander, J.M., Molecular Pathogenesis of Human Pituitary Tumors, in Pituitary Disorders: Comprehensive Management, A.F.T. Krisht, Georg T, Editor. 1999, Lippincott Williams & Wilkins: Baltimore. p. 61-77.
19. Zada, G., W.W. Woodmansee, S. Ramkissoon, J. Amadio, V. Nose, and E.R. Laws, Atypical Pituitary Adenomas: Incidence, Clinical Characteristics, and Implications. Journal of neurosurgery, 2011. 114(2): p. 336-344.
20. Asa, S.L. and S. Ezzat, The Pathogenesis of Pituitary Tumours. Nat Rev Cancer, 2002. 2(11): p. 836-849.
21. Daly, A.F., M.A. Tichomirowa, and A. Beckers, The Epidemiology and Genetics of Pituitary Adenomas. Best Practice & Research Clinical Endocrinology & Metabolism, 2009. 23(5): p. 543-554.
22. Vierimaa, O., M. Georgitsi, R. Lehtonen, P. Vahteristo, A. Kokko, A. Raitila, K. Tuppurainen, T.M.L. Ebeling, P.I. Salmela, R. Paschke, S. Gündogdu, E. De Menis, M.J. Mäkinen, V. Launonen, A. Karhu, and L.A. Aaltonen, Pituitary Adenoma Predisposition Caused by Germline Mutations in the Aip Gene. Science, 2006. 312(5777): p. 1228-1230.
23. Daly, A.F., M.A. Tichomirowa, P. Petrossians, E. Heliövaara, M.-L. Jaffrain-Rea, A. Barlier, L.A. Naves, T. Ebeling, A. Karhu, A. Raappana, L. Cazabat, E.D. Menis, C.F. Montañana, G. Raverot, R.J. Weil, T. Sane, D. Maiter, S. Neggers, M. Yaneva, A. Tabarin, E. Verrua, E. Eloranta, A. Murat, O. Vierimaa, P.I. Salmela, P. Emy, R.A. Toledo, M.I. Sabaté, C. Villa, M. Popelier, R. Salvatori, J. Jennings,
99
Á.F. Longás, J.I.L. Aizpún, M. Georgitsi, R. Paschke, C. Ronchi, M. Valimaki, C. Saloranta, W.D. Herder, R. Cozzi, M. Guitelman, F. Magri, M.S. Lagonigro, G. Halaby, V. Corman, M.-T. Hagelstein, J.-F. Vanbellinghen, G.B. Barra, A.-P. Gimenez-Roqueplo, F.J. Cameron, F. Borson-Chazot, I. Holdaway, S.P.A. Toledo, G.K. Stalla, A. Spada, S. Zacharieva, J. Bertherat, T. Brue, V. Bours, P. Chanson, L.A. Aaltonen, and A. Beckers, Clinical Characteristics and Therapeutic Responses in Patients with Germ-Line Aip Mutations and Pituitary Adenomas: An International Collaborative Study. The Journal of Clinical Endocrinology & Metabolism, 2010. 95(11): p. E373-E383.
24. Daly, A.F., M.A. Tichomirowa, and A. Beckers, The Epidemiology and Genetics of Pituitary Adenomas. Pituitary Tumours, 2009. 23(5): p. 543-554.
25. Haley Gittleman, Quinn T. Ostrom, Paul D. Farah, A. Ondracek, Yanwen Chen, Yingli Wolinsky, Carol Kruchko, Justin Singer, Varun R. Kshettry, Edward R. Laws, Andrew E. Sloan, Warren R. Selman, and Jill S. Barnholtz-Sloan, Descriptive Epidemiology of Pituitary Tumors in the United States, 2004–2009. Journal of Neurosurgery, 2014. 121(3): p. 527-535.
26. Ostrom, Q.T., H. Gittleman, P. Farah, A. Ondracek, Y. Chen, Y. Wolinsky, N.E. Stroup, C. Kruchko, and J.S. Barnholtz-Sloan, Cbtrus Statistical Report: Primary Brain and Central Nervous System Tumors Diagnosed in the United States in 2006-2010. Neuro-Oncology, 2013. 15(Suppl 2): p. ii1-ii56.
27. Wöhrer, A., T. Waldhör, H. Heinzl, M. Hackl, J. Feichtinger, U. Gruber-Mösenbacher, A. Kiefer, H. Maier, R. Motz, A. Reiner-Concin, B. Richling, C. Idriceanu, M. Scarpatetti, R. Sedivy, H.-C. Bankl, W. Stiglbauer, M. Preusser, K. Rössler, and J. Hainfellner, The Austrian Brain Tumour Registry: A Cooperative Way to Establish a Population-Based Brain Tumour Registry. Journal of Neuro-Oncology, 2009. 95(3): p. 401-411.
28. Nilsson, B., E. Gustavsson-Kadaka, B.-Å. Bengtsson, and B. Jonsson, Pituitary Adenomas in Sweden between 1958 and 1991: Incidence, Survival, and Mortality. The Journal of Clinical Endocrinology & Metabolism, 2000. 85(4): p. 1420-1425.
29. Raappana, A., J. Koivukangas, T. Ebeling, and T. Pirila, Incidence of Pituitary Adenomas in Northern Finland in 1992-2007. Journal of Clinical Endocrinology & Metabolism, 2010. 95(9): p. 4268-4275.
30. Tjörnstrand, A., K. Gunnarsson, M. Evert, E. Holmberg, O. Ragnarsson, T. Rosén, and H. Filipsson Nyström, The Incidence Rate of Pituitary Adenomas in Western Sweden for the Period 2001–2011. European Journal of Endocrinology, 2014. 171(4): p. 519-526.
31. Webb, C. and R.A. Prayson, Pediatric Pituitary Adenomas. Archives of Pathology & Laboratory Medicine, 2008. 132(1): p. 77-80.
100
32. Daly, A.F., M. Rixhon, C. Adam, A. Dempegioti, M.A. Tichomirowa, and A. Beckers, High Prevalence of Pituitary Adenomas: A Cross-Sectional Study in the Province of Liège, Belgium. The Journal of Clinical Endocrinology & Metabolism, 2006. 91(12): p. 4769-4775.
33. Fernandez, A., N. Karavitaki, and J.A.H. Wass, Prevalence of Pituitary Adenomas: A Community-Based, Cross-Sectional Study in Banbury (Oxfordshire, Uk). Clinical Endocrinology, 2010. 72(3): p. 377-382.
34. Colao, A., The Prolactinoma. Pituitary Tumours, 2009. 23(5): p. 575-596.
35. Schlechte, J.A., Clinical Practice. Prolactinoma. N Engl J Med, 2003. 349(21): p. 2035-41.
36. Gillam, M.P., M.E. Molitch, G. Lombardi, and A. Colao, Advances in the Treatment of Prolactinomas. Endocrine Reviews, 2006. 27(5): p. 485-534.
37. Chanson, P., S. Salenave, P. Kamenicky, L. Cazabat, and J. Young, Acromegaly. Pituitary Tumours, 2009. 23(5): p. 555-574.
38. Kauppinen-Mäkelin, R., T. Sane, A. Reunanen, M.J. Välimäki, L. Niskanen, H. Markkanen, E. Löyttyniemi, T. Ebeling, P. Jaatinen, H. Laine, P. Nuutila, P. Salmela, J. Salmi, U.-H. Stenman, J. Viikari, and E. Voutilainen, A Nationwide Survey of Mortality in Acromegaly. The Journal of Clinical Endocrinology & Metabolism, 2005. 90(7): p. 4081-4086.
39. Giustina, A., P. Chanson, M.D. Bronstein, A. Klibanski, S. Lamberts, F.F. Casanueva, P. Trainer, E. Ghigo, K. Ho, and S. Melmed, A Consensus on Criteria for Cure of Acromegaly. J Clin Endocrinol Metab, 2010. 95(7): p. 3141-8.
40. Katznelson, L., E.R.L. Jr, S. Melmed, M.E. Molitch, M.H. Murad, A. Utz, and J.A.H. Wass, Acromegaly: An Endocrine Society Clinical Practice Guideline. The Journal of Clinical Endocrinology & Metabolism, 2014. 99(11): p. 3933-3951.
41. Giustina, A., P. Chanson, D. Kleinberg, M.D. Bronstein, D.R. Clemmons, A. Klibanski, A.J. van der Lely, C.J. Strasburger, S.W. Lamberts, K.K. Ho, F.F. Casanueva, and S. Melmed, Expert Consensus Document: A Consensus on the Medical Treatment of Acromegaly. Nat Rev Endocrinol, 2014. 10(4): p. 243-8.
42. Jane, J.A., Jr., R.M. Starke, M.A. Elzoghby, D.L. Reames, S.C. Payne, M.O. Thorner, J.C. Marshall, E.R. Laws, Jr., and M.L. Vance, Endoscopic Transsphenoidal Surgery for Acromegaly: Remission Using Modern Criteria, Complications, and Predictors of Outcome. Journal of Clinical Endocrinology & Metabolism, 2011. 96(9): p. 2732-2740.
43. Abu Dabrh, A.M., K. Mohammed, N. Asi, W.H. Farah, Z. Wang, M.H. Farah, L.J. Prokop, L. Katznelson, and M.H. Murad, Surgical Interventions and Medical Treatments in Treatment-Naive Patients
101
with Acromegaly: Systematic Review and Meta-Analysis. J Clin Endocrinol Metab, 2014. 99(11): p. 4003-14.
44. Nomikos, P., M. Buchfelder, and R. Fahlbusch, The Outcome of Surgery in 668 Patients with Acromegaly Using Current Criteria of Biochemical ‘Cure’. European Journal of Endocrinology, 2005. 152(3): p. 379-387.
45. Kreutzer, J., M.L. Vance, M.B. Lopes, and E.R. Laws, Jr., Surgical Management of Gh-Secreting Pituitary Adenomas: An Outcome Study Using Modern Remission Criteria. J Clin Endocrinol Metab, 2001. 86(9): p. 4072-7.
46. Nunes, V.S., J.M.S. Correa, M.E.S. Puga, E.M.K. Silva, and C.L. Boguszewski, Preoperative Somatostatin Analogues Versus Direct Transsphenoidal Surgery for Newly-Diagnosed Acromegaly Patients: A Systematic Review and Meta-Analysis Using the Grade System. Pituitary, 2015. 18(4): p. 500-8.
47. Bertagna, X., L. Guignat, L. Groussin, and J. Bertherat, Cushing's Disease. Pituitary Tumours, 2009. 23(5): p. 607-623.
48. Arnaldi, G., A. Angeli, A.B. Atkinson, X. Bertagna, F. Cavagnini, G.P. Chrousos, G.A. Fava, J.W. Findling, R.C. Gaillard, A.B. Grossman, B. Kola, A. Lacroix, T. Mancini, F. Mantero, J. Newell-Price, L.K. Nieman, N. Sonino, M.L. Vance, A. Giustina, and M. Boscaro, Diagnosis and Complications of Cushing's Syndrome: A Consensus Statement. Journal of Clinical Endocrinology & Metabolism, 2003. 88(12): p. 5593-5602.
49. Nieman, L.K., B.M. Biller, J.W. Findling, J. Newell-Price, M.O. Savage, P.M. Stewart, and V.M. Montori, The Diagnosis of Cushing's Syndrome: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab, 2008. 93(5): p. 1526-40.
50. Swearingen, B., L. Katznelson, K. Miller, S. Grinspoon, A. Waltman, D.J. Dorer, A. Klibanski, and B.M.K. Biller, Diagnostic Errors after Inferior Petrosal Sinus Sampling. The Journal of Clinical Endocrinology & Metabolism, 2004. 89(8): p. 3752-3763.
51. Sheth, S.A., M.K. Mian, J. Neal, N.A. Tritos, L. Nachtigall, A. Klibanski, B.M. Biller, and B. Swearingen, Transsphenoidal Surgery for Cushing Disease after Nondiagnostic Inferior Petrosal Sinus Sampling. Neurosurgery, 2012. 71(1): p. 14-22.
52. Patronas, N., N. Bulakbasi, C.A. Stratakis, A. Lafferty, E.H. Oldfield, J. Doppman, and L.K. Nieman, Spoiled Gradient Recalled Acquisition in the Steady State Technique Is Superior to Conventional Postcontrast Spin Echo Technique for Magnetic Resonance Imaging Detection of Adrenocorticotropin-Secreting Pituitary Tumors. J Clin Endocrinol Metab, 2003. 88(4): p. 1565-9.
53. Biller, B.M., A.B. Grossman, P.M. Stewart, S. Melmed, X. Bertagna, J. Bertherat, M. Buchfelder, A. Colao, A.R. Hermus, L.J. Hofland, A. Klibanski, A. Lacroix, J.R. Lindsay, J. Newell-Price, L.K. Nieman, S.
102
Petersenn, N. Sonino, G.K. Stalla, B. Swearingen, M.L. Vance, J.A. Wass, and M. Boscaro, Treatment of Adrenocorticotropin-Dependent Cushing's Syndrome: A Consensus Statement. J Clin Endocrinol Metab, 2008. 93(7): p. 2454-62.
54. Dallapiazza, R., E. Oldfield, and J. Jane, Jr., Surgical Management of Cushing’s Disease. Pituitary, 2015. 18(2): p. 211-6.
55. Jagannathan, J., J.P. Sheehan, and J.A. Jane, Jr., Evaluation and Management of Cushing Syndrome in Cases of Negative Sellar Magnetic Resonance Imaging. Neurosurg Focus, 2007. 23(3): p. E3.
56. Pouratian, N., D.M. Prevedello, J. Jagannathan, M.B. Lopes, M.L. Vance, and E.R. Laws, Jr., Outcomes and Management of Patients with Cushing's Disease without Pathological Confirmation of Tumor Resection after Transsphenoidal Surgery. J Clin Endocrinol Metab, 2007. 92(9): p. 3383-8.
57. Petersenn, S. and M. Fleseriu, Pituitary-Directed Medical Therapy in Cushing's Disease. Pituitary, 2015. 18(2): p. 238-44.
58. Katznelson, L., Bilateral Adrenalectomy for Cushing's Disease. Pituitary, 2015. 18(2): p. 269-73.
59. Beck-Peccoz, P., L. Persani, D. Mannavola, and I. Campi, Tsh-Secreting Adenomas. Best Practice & Research Clinical Endocrinology & Metabolism, 2009. 23(5): p. 597-606.
60. Beck-Peccoz, P., A. Lania, A. Beckers, K. Chatterjee, and J.L. Wemeau, 2013 European Thyroid Association Guidelines for the Diagnosis and Treatment of Thyrotropin-Secreting Pituitary Tumors. Eur Thyroid J, 2013. 2(2): p. 76-82.
61. Michelle J. Clarke, Dana Erickson, M. Regina Castro, and John L. D. Atkinson, Thyroid-Stimulating Hormone Pituitary Adenomas. Journal of Neurosurgery, 2008. 109(1): p. 17-22.
62. Socin, H.V., P. Chanson, B. Delemer, A. Tabarin, V. Rohmer, J. Mockel, A. Stevenaert, and A. Beckers, The Changing Spectrum of Tsh-Secreting Pituitary Adenomas: Diagnosis and Management in 43 Patients. Eur J Endocrinol, 2003. 148(4): p. 433-42.
63. Beck-Peccoz, P., L. Persani, D. Mannavola, and I. Campi, Tsh-Secreting Adenomas. Pituitary Tumours, 2009. 23(5): p. 597-606.
64. Greenman, Y. and N. Stern, Non-Functioning Pituitary Adenomas. Best Pract Res Clin Endocrinol Metab, 2009. 23(5): p. 625-38.
65. Saeger, W., D.K. Ludecke, M. Buchfelder, R. Fahlbusch, H.J. Quabbe, and S. Petersenn, Pathohistological Classification of Pituitary Tumors: 10 Years of Experience with the German Pituitary Tumor Registry. European Journal of Endocrinology, 2007. 156(2): p. 203-216.
66. Losa, M., C.A. Donofrio, R. Barzaghi, and P. Mortini, Presentation and Surgical Results of Incidentally Discovered Nonfunctioning Pituitary Adenomas: Evidence for a Better Outcome Independently of Other Patients' Characteristics. Eur J Endocrinol, 2013. 169(6): p. 735-42.
103
67. Murad-Kejbou, S. and E. Eggenberger, Pituitary Apoplexy: Evaluation, Management, and Prognosis. Current opinion in ophthalmology, 2009. 20(6): p. 456-461.
68. Dallapiazza, R.F.M.D.P., Y.M.D. Grober, R.M.M.D.M. Starke, E.R.J.M.D. Laws, and J.A.J.M.D. Jane, Long-Term Results of Endonasal Endoscopic Transsphenoidal Resection of Nonfunctioning Pituitary Macroadenomas. Neurosurgery, 2015. 76(1): p. 42-53.
69. Coulter, I.C., N. Mukerji, N. Bradey, V. Connolly, and P.J. Kane, Radiologic Follow-up of Non-Functioning Pituitary Adenomas: Rationale and Cost Effectiveness. Journal of neuro-oncology, 2009. 93(1): p. 157-163.
70. Honegger, J., S. Zimmermann, T. Psaras, M. Petrick, M. Mittelbronn, U. Ernemann, M. Reincke, and K. Dietz, Growth Modelling of Non-Functioning Pituitary Adenomas in Patients Referred for Surgery. Eur J Endocrinol, 2008. 158(3): p. 287-94.
71. Park, P., W.F. Chandler, A.L. Barkan, J.J. Orrego, J.A. Cowan, K.A. Griffith, and C. Tsien, The Role of Radiation Therapy after Surgical Resection of Nonfunctional Pituitary Macroadenomas. Neurosurgery, 2004. 55(1): p. 100-106.
72. Gopalan, R., D. Schlesinger, M.L. Vance, E. Laws, and J. Sheehan, Long-Term Outcomes after Gamma Knife Radiosurgery for Patients with a Nonfunctioning Pituitary Adenoma. Neurosurgery, 2011. 69(2): p. 284-93.
73. Prasad, S.M.D., N.J.M.D. Volpe, and L.J.M.D.M. Balcer, Approach to Optic Neuropathies: Clinical Update. Neurologist, 2010. 16(1): p. 23-34.
74. Jayaraman, M., S. Ambika, R.A. Gandhi, S.R. Bassi, P. Ravi, and P. Sen, Multifocal Visual Evoked Potential Recordings in Compressive Optic Neuropathy Secondary to Pituitary Adenoma. Doc Ophthalmol, 2010. 121(3): p. 197-204.
75. Patronas, N. and C.-Y. Liu, State of Art Imaging of the Pituitary Tumors. Journal of Neuro-Oncology, 2014. 117(3): p. 395-405.
76. Knosp, E., E. Steiner, K. Kitz, and C. Matula, Pituitary Adenomas with Invasion of the Cavernous Sinus Space: A Magnetic Resonance Imaging Classification Compared with Surgical Findings. Neurosurgery, 1993. 33(4): p. 610-618.
77. Wolfsberger, S., A. Ba-Ssalamah, K. Pinker, V. Mlynarik, T. Czech, E. Knosp, and S. Trattnig, Application of Three-Tesla Magnetic Resonance Imaging for Diagnosis and Surgery of Sellar Lesions. J Neurosurg, 2004. 100(2): p. 278-86.
78. Di Ieva, A., F. Rotondo, L.V. Syro, M.D. Cusimano, and K. Kovacs, Aggressive Pituitary Adenomas[Mdash]Diagnosis and Emerging Treatments. Nat Rev Endocrinol, 2014. 10(7): p. 423-435.
79. Caton, R., Notes of a Case of Acromegaly Treated by Operation. Br Med J, 1893. 2(1722): p. 1421-3.
104
80. James K. Liu, Kaushik Das, Martin H. Weiss, J. Edward R. Laws, and William T. Couldwell, The History and Evolution of Transsphenoidal Surgery. Journal of Neurosurgery, 2001. 95(6): p. 1083-1096.
81. Schmidt, R.F., O.J. Choudhry, R. Takkellapati, J.A. Eloy, W.T. Couldwell, and J.K. Liu, Hermann Schloffer and the Origin of Transsphenoidal Pituitary Surgery. Neurosurg Focus, 2012. 33(2): p. E5.
82. Harold Rosegay, Cushing's Legacy to Transsphenoidal Surgery. Journal of Neurosurgery, 1981. 54(4): p. 448-454.
83. Hardy, J. and S.M. Wigser, Trans-Sphenoidal Surgery of Pituitary Fossa Tumors with Televised Radiofluoroscopic Control. Journal of neurosurgery, 1965. 23(6): p. 612-619.
84. Hardy, J., Transsphenoidal Hypophysectomy. Journal of neurosurgery, 1971. 34(4): p. 582-594.
85. Cawley, M.T.G., Transsphenoidal Surgery: Operative Techniques, in Pituitary Disorders: Comprehensive Management, A.F.T. Krisht, Georg T, Editor. 1999, Lippincott Williams & Wilkins: Baltimore. p. 349-359.
86. Jane Jr, J.A. and E.R. Laws Jr, The Surgical Management of Pituitary Adenomas in a Series of 3,093 Patients. Journal of the American College of Surgeons, 2001. 193(6): p. 650-659.
87. Guiot J, R.J., Fourestier M, Fournier A, Comoy C Vulmiere J, Groux R, Intracranial Endoscopic Explorations. Presse Med, 1963. 18(71): p. 1225-1228.
88. Jho, H.D. and R.L. Carrau, Endoscopy Assisted Transsphenoidal Surgery for Pituitary Adenoma. Acta Neurochirurgica, 1996. 138(12): p. 1416-1425.
89. Cappabianca, P., A. Alfieri, A. Colao, D. Ferone, G. Lombardi, and E. de Divitiis, Endoscopic Endonasal Transsphenoidal Approach: An Additional Reason in Support of Surgery in the Management of Pituitary Lesions. Skull base surgery, 1999. 9(2): p. 109-117.
90. Fatemi, N., J.R. Dusick, M.A. de Paiva Neto, and D.F. Kelly, The Endonasal Microscopic Approach for Pituitary Adenomas and Other Parasellar Tumors: A 10-Year Experience. Neurosurgery, 2008. 63(4) (Operative Neurosurgery Supplement 2): p. 244-256.
91. Schwartz, T.H.M.D., J.F.M.D. Fraser, S.M.D. Brown, A.M.D. Tabaee, A.M.D. Kacker, and V.K.M.D. Anand, Endoscopic Cranial Base Surgery: Classification of Operative Approaches. Neurosurgery, 2008. 62(5): p. 991-1005.
92. Zada, G. and P. Cappabianca, Raising the Bar in Transsphenoidal Pituitary Surgery. World Neurosurg, 2010. 74(4-5): p. 452-4.
93. Jane, J.A.J.M.D., K.M.D.P.D. Thapar, G.J.M.D. Kaptain, N.M.D. Maartens, and E.R.J.M.D. Laws, Pituitary Surgery: Transsphenoidal Approach. Neurosurgery, 2002. 51(2): p. 435-444.
105
94. P. Benjamin Kerr and Edward H. Oldfield, Sublabial–Endonasal Approach to the Sella Turcica. Journal of Neurosurgery, 2008. 109(1): p. 153-155.
95. Nancy McLaughlin, Amy A. Eisenberg, Pejman Cohan, Charlene B. Chaloner, and Daniel F. Kelly, Value of Endoscopy for Maximizing Tumor Removal in Endonasal Transsphenoidal Pituitary Adenoma Surgery. Journal of Neurosurgery, 2013. 118(3): p. 613-620.
96. Esposito, F., J.R. Dusick, N. Fatemi, and D.F. Kelly, Graded Repair of Cranial Base Defects and Cerebrospinal Fluid Leaks in Transsphenoidal Surgery. Neurosurgery, 2007. 60(4 Suppl 2): p. 295-303; discussion 303-4.
97. Frank, G., E. Pasquini, G. Farneti, D. Mazzatenta, V. Sciarretta, V. Grasso, and M. Faustini Fustini, The Endoscopic Versus the Traditional Approach in Pituitary Surgery. Neuroendocrinology, 2006. 83(3-4): p. 240-248.
98. Kassam, A.B., D.M. Prevedello, R.L. Carrau, C.H. Snyderman, A. Thomas, P. Gardner, A. Zanation, B. Duz, S.T. Stefko, K. Byers, and M.B. Horowitz, Endoscopic Endonasal Skull Base Surgery: Analysis of Complications in the Authors' Initial 800 Patients. Journal of neurosurgery, 2011. 114(6): p. 1544-1568.
99. de Divitiis, E., E.R. Laws, U. Giani, S.L. Iuliano, O. de Divitiis, and M.L. Apuzzo, The Current Status of Endoscopy in Transsphenoidal Surgery: An International Survey. World Neurosurg, 2015. 83(4): p. 447-54.
100. Liu, J.K., R.F. Schmidt, O.J. Choudhry, P.A. Shukla, and J.A. Eloy, Surgical Nuances for Nasoseptal Flap Reconstruction of Cranial Base Defects with High-Flow Cerebrospinal Fluid Leaks after Endoscopic Skull Base Surgery. Neurosurg Focus, 2012. 32(6): p. E7.
101. Hadad, G., L. Bassagasteguy, R.L. Carrau, J.C. Mataza, A. Kassam, C.H. Snyderman, and A. Mintz, A Novel Reconstructive Technique after Endoscopic Expanded Endonasal Approaches: Vascular Pedicle Nasoseptal Flap. Laryngoscope, 2006. 116(10): p. 1882-6.
102. Berker, M., D.B. Hazer, T. Yucel, A. Gurlek, A. Cila, M. Aldur, and M. Onerci, Complications of Endoscopic Surgery of the Pituitary Adenomas: Analysis of 570 Patients and Review of the Literature. Pituitary, 2012. 15(3): p. 288-300.
103. Tabaee, A.M.D., V.K.M.D. Anand, J.F.M.D. Fraser, S.M.M.D.M.B.A. Brown, A.M.D. Singh, and T.H.M.D. Schwartz, Three-Dimensional Endoscopic Pituitary Surgery. Neurosurgery, 2009. 64(5) Operative Neurosurgery Supplement(2): p. ons288-ons295.
104. Koutourousiou, M., P.A. Gardner, J. Fernandez-Miranda, A. Paluzzi, E.W. Wang, and C.H. Snyderman, Endoscopic Endonasal Surgery for Giant Pituitary Adenomas: Advantages and Limitations. Journal of neurosurgery, 2013. 118(3): p. 621-631.
106
105. Saito, K., A. Kuwayama, N. Yamamoto, and K. Sugita, The Transsphenoidal Removal of Nonfunctioning Pituitary Adenomas with Suprasellar Extensions: The Open Sella Method and Intentionally Staged Operation. Neurosurgery, 1995. 36(4): p. 668-75; discussion 675-6.
106. Zada, G., R. Du, and E.R. Laws, Jr., Defining the "Edge of the Envelope": Patient Selection in Treating Complex Sellar-Based Neoplasms Via Transsphenoidal Versus Open Craniotomy. J Neurosurg, 2011. 114(2): p. 286-300.
107. Buchfelder, M. and S. Schlaffer, Surgical Treatment of Pituitary Tumours. Pituitary Tumours, 2009. 23(5): p. 677-692.
108. Dolenc, V.V., Transcranial Epidural Approach to Pituitary Tumors Extending Beyond the Sella. Neurosurgery, 1997. 41(3): p. 542-50; discussion 551-2.
109. Buchfelder, M. and J. Kreutzer, Transcranial Surgery for Pituitary Adenomas. Pituitary, 2008. 11(4): p. 375-384.
110. Nishioka, H., T. Hara, M. Usui, N. Fukuhara, and S. Yamada, Simultaneous Combined Supra-Infrasellar Approach for Giant/Large Multilobulated Pituitary Adenomas. World Neurosurgery, 2012. 77(3–4): p. 533-539.
111. Hardy, J. and S.M. Wigser, Trans-Sphenoidal Surgery of Pituitary Fossa Tumors with Televised Radiofluoroscopic Control*. Journal of Neurosurgery, 1965. 23(6): p. 612-619.
112. Gumprecht, H.K.M.D., D.C.M.D. Widenka, and C.B.M.D. Lumenta, Brainlab Vectorvision Neuronavigation System: Technology and Clinical Experiences in 131 Cases. Neurosurgery, 1999. 44(1): p. 97-104.
113. Bohinski, R.J., R.E. Warnick, M.F. GaskillShipley, M. Zuccarello, H.R. van Loveren, D.W. Kormos, and J.M. Tew, Jr., Intraoperative Magnetic Resonance Imaging to Determine the Extent of Resection of Pituitary Macroadenomas During Transsphenoidal Microsurgery. Neurosurgery, 2001. 49(5): p. 1133-1144.
114. Nimsky, C., B.V. Keller, O. Ganslandt, and R. Fahlbusch, Intraoperative High-Field Magnetic Resonance Imaging in Transsphenoidal Surgery of Hormonally Inactivepituitary Macroadenomas. Neurosurgery, 2006. 59(1): p. 105-114.
115. Schwartz, T.H., P.E. Stieg, and V.K. Anand, Endoscopic Transsphenoidal Pituitary Surgery with Intraoperative Magnetic Resonance Imaging. Neurosurgery, 2006. 58(1 Suppl): p. ONS44-51; discussion ONS44-51.
116. Fahlbusch, R., B. Keller, O. Ganslandt, J. Kreutzer, and C. Nimsky, Transsphenoidal Surgery in Acromegaly Investigated by Intraoperative High-Field Magnetic Resonance Imaging. Eur J Endocrinol, 2005. 153(2): p. 239-48.

107
117. Makary, M., E.A. Chiocca, N. Erminy, M. Antor, S.D. Bergese, M. Abdel-Rasoul, S. Fernandez, and R. Dzwonczyk, Clinical and Economic Outcomes of Low-Field Intraoperative Mri-Guided Tumor Resection Neurosurgery. Journal of Magnetic Resonance Imaging, 2011. 34(5): p. 1022-1030.
118. al-Mefty, O., J.E. Kersh, A. Routh, and R.R. Smith, The Long-Term Side Effects of Radiation Therapy for Benign Brain Tumors in Adults. J Neurosurg, 1990. 73(4): p. 502-12.
119. Lee, C.C., H. Kano, H.C. Yang, Z. Xu, C.P. Yen, W.Y. Chung, D.H. Pan, L.D. Lunsford, and J.P. Sheehan, Initial Gamma Knife Radiosurgery for Nonfunctioning Pituitary Adenomas. J Neurosurg, 2014. 120(3): p. 647-54.
120. Jason P. Sheehan, Zhiyuan Xu, David J. Salvetti, Paul J. Schmitt, and Mary Lee Vance, Results of Gamma Knife Surgery for Cushing's Disease. Journal of Neurosurgery, 2013. 119(6): p. 1486-1492.
121. Schalin-Jäntti, C., L. Valanne, M. Tenhunen, K. Setälä, A. Paetau, T. Sane, and M. Kouri, Outcome of Fractionated Stereotactic Radiotherapy in Patients with Pituitary Adenomas Resistant to Conventional Treatments: A 5·25-Year Follow-up Study. Clinical endocrinology, 2010. 73(1): p. 72-77.
122. Dorward, N., Endocrine Outcomes in Endoscopic Pituitary Surgery: A Literature Review. Acta Neurochirurgica, 2010. 152(8): p. 1275-1279.
123. Losa, M., P. Mortini, R. Barzaghi, P. Ribotto, M.R. Terreni, S.B. Marzoli, S. Pieralli, and M. Giovanelli, Early Results of Surgery in Patients with Nonfunctioning Pituitary Adenoma and Analysis of the Risk of Tumor Recurrence. Journal of neurosurgery, 2008. 108(3): p. 525-532.
124. Chang, E.F., G. Zada, S. Kim, K.R. Lamborn, A. Quinones-Hinojosa, J.B. Tyrrell, C.B. Wilson, and S. Kunwar, Long-Term Recurrence and Mortality after Surgery and Adjuvant Radiotherapy for Nonfunctional Pituitary Adenomas. Journal of neurosurgery, 2008. 108(4): p. 736-745.
125. Dehdashti, A.R., A. Ganna, K. Karabatsou, and F. Gentili, Pure Endoscopic Endonasal Approach for Pituitary Adenomas: Early Surgical Results in 200 Patients and Comparison with Previous Microsurgical Series. Neurosurgery, 2008. 62(5): p. 1006-1017.
126. Goudakos, J.K., K.D. Markou, and C. Georgalas, Endoscopic Versus Microscopic Trans-Sphenoidal Pituitary Surgery: A Systematic Review and Meta-Analysis. Clin Otolaryngol, 2011. 36(3): p. 212-20.
127. Shahlaie, K., N. McLaughlin, A.B. Kassam, and D.F. Kelly, The Role of Outcomes Data for Assessing the Expertise of a Pituitary Surgeon. Curr Opin Endocrinol Diabetes Obes, 2010. 17(4): p. 369-76.
128. McLaughlin, N., E.R. Laws, N.M. Oyesiku, L. Katznelson, and D.F. Kelly, Pituitary Centers of Excellence. Neurosurgery, 2012. 71(5): p. 916-926.
108
129. Colao, A., G. Cerbone, P. Cappabianca, D. Ferone, A. Alfieri, F. Di Salle, A. Faggiano, B. Merola, E. de Divitiis, and G. Lombardi, Effect of Surgery and Radiotherapy on Visual and Endocrine Function in Nonfunctioning Pituitary Adenomas. J Endocrinol Invest, 1998. 21(5): p. 284-90.
130. Webb, S.M., M. Rigla, A. Wägner, B. Oliver, and F. Bartumeus, Recovery of Hypopituitarism after Neurosurgical Treatment of Pituitary Adenomas. The Journal of Clinical Endocrinology & Metabolism, 1999. 84(10): p. 3696-3700.
131. Fatemi, N., J.R. Dusick, C. Mattozo, D.L. McArthur, P. Cohan, J. Boscardin, C. Wang, R.S. Swerdloff, and D.F. Kelly, Pituitary Hormonal Loss and Recovery after Transsphenoidal Adenoma Removal. Neurosurgery, 2008. 63(4): p. 709-719.
132. Nelson, A.T., H.S. Tucker, and D.P. Becker, Residual Anterior Pituitary Function Following Transsphenoidal Resection of Pituitary Macroadenomas. Journal of neurosurgery, 1984. 61(3): p. 577-580.
133. Ciric, I., A. Ragin, C. Baumgartner, and D. Pierce, Complications of Transsphenoidal Surgery: Results of a National Survey, Review of the Literature, and Personal Experience. Neurosurgery, 1997. 40(2): p. 225-236.
134. Edward C. Nemergut, Zhiyi Zuo, John A. Jane Jr., and Edward R. Laws Jr., Predictors of Diabetes Insipidus after Transsphenoidal Surgery: A Review of 881 Patients. Journal of Neurosurgery, 2005. 103(3): p. 448-454.
135. Rudolf A. Kristof, Maria Rother, Georg Neuloh, and Dietrich Klingmüller, Incidence, Clinical Manifestations, and Course of Water and Electrolyte Metabolism Disturbances Following Transsphenoidal Pituitary Adenoma Surgery: A Prospective Observational Study. Journal of Neurosurgery, 2009. 111(3): p. 555-562.
136. Schreckinger, M., N. Szerlip, and S. Mittal, Diabetes Insipidus Following Resection of Pituitary Tumors. Clin Neurol Neurosurg, 2013. 115(2): p. 121-6.
137. Tabaee, A., V.K. Anand, Y. Barrón, D.H. Hiltzik, S.M. Brown, A. Kacker, M. Mazumdar, and T.H. Schwartz, Endoscopic Pituitary Surgery: A Systematic Review and Meta-Analysis. Journal of neurosurgery, 2009. 111(3): p. 545-554.
138. Nomikos, P., C. Ladar, R. Fahlbusch, and M. Buchfelder, Impact of Primary Surgery on Pituitary Function in Patients with Non-Functioning Pituitary Adenomas -- a Study on 721 Patients. Acta Neurochirurgica, 2004. 146(1): p. 27-35.
139. Nemergut, E.C., Z. Zuo, J.A. Jane, and E.R. Laws, Predictors of Diabetes Insipidus after Transsphenoidal Surgery: A Review of 881 Patients. Journal of Neurosurgery, 2005. 103(3): p. 448-454.
140. Yedinak, C., N. Hameed, M. Gassner, J. Brzana, S. McCartney, and M. Fleseriu, Recovery Rate of Adrenal Function after Surgery in Patients
109
with Acromegaly Is Higher Than in Those with Non-Functioning Pituitary Tumors: A Large Single Center Study. Pituitary, 2015.
141. Lodish, M., S.V. Dunn, N. Sinaii, M.F. Keil, and C.A. Stratakis, Recovery of the Hypothalamic-Pituitary-Adrenal Axis in Children and Adolescents after Surgical Cure of Cushing's Disease. The Journal of Clinical Endocrinology & Metabolism, 2012. 97(5): p. 1483-1491.
142. Berr, C.M., G. Di Dalmazi, A. Osswald, K. Ritzel, M. Bidlingmaier, L.L. Geyer, M. Treitl, K. Hallfeldt, W. Rachinger, N. Reisch, R. Blaser, J. Schopohl, F. Beuschlein, and M. Reincke, Time to Recovery of Adrenal Function after Curative Surgery for Cushing's Syndrome Depends on Etiology. J Clin Endocrinol Metab, 2014: p. jc20143632.
143. Aranda, G., J. Ensenat, M. Mora, M. Puig-Domingo, M.J. Martinez de Osaba, G. Casals, E. Verger, M.T. Ribalta, F.A. Hanzu, and I. Halperin, Long-Term Remission and Recurrence Rate in a Cohort of Cushing's Disease: The Need for Long-Term Follow-Up. Pituitary, 2015. 18(1): p. 142-9.
144. Bochicchio, D., M. Losa, and M. Buchfelder, Factors Influencing the Immediate and Late Outcome of Cushing's Disease Treated by Transsphenoidal Surgery: A Retrospective Study by the European Cushing's Disease Survey Group. J Clin Endocrinol Metab, 1995. 80(11): p. 3114-20.
145. Kelly, D.F., Transsphenoidal Surgery for Cushing's Disease: A Review of Success Rates, Remission Predictors, Management of Failed Surgery, and Nelson's Syndrome. Neurosurg Focus, 2007. 23(3): p. E5.
146. Peter, M. and N.D. Tribolet, Visual Outcome after Transsphenoidal Surgery for Pituitary Adenomas. British Journal of Neurosurgery, 1995. 9(2): p. 151-158.
147. Gnanalingham, K.K., S. Bhattacharjee, R. Pennington, J. Ng, and N. Mendoza, The Time Course of Visual Field Recovery Following Transphenoidal Surgery for Pituitary Adenomas: Predictive Factors for a Good Outcome. J Neurol Neurosurg Psychiatry, 2005. 76(3): p. 415-9.
148. Powell, M., Recovery of Vision Following Transsphenoidal Surgery for Pituitary Adenomas. British Journal of Neurosurgery, 1995. 9(3): p. 367.
149. Kristof, R.A., D. Kirchhofer, D. Handzel, G. Neuloh, J. Schramm, C.A. Mueller, and N. Eter, Pre-Existing Chiasma Syndromes Do Not Entirely Remit Following Transsphenoidal Surgery for Pituitary Adenomas. Acta Neurochir (Wien), 2011. 153(1): p. 26-32.
150. Dallapiazza, R.F. and J.A. Jane Jr, Outcomes of Endoscopic Transsphenoidal Pituitary Surgery. Endocrinology and Metabolism Clinics of North America, 2015. 44(1): p. 105-115.
151. Nishioka, H., J. Haraoka, and Y. Ikeda, Risk Factors of Cerebrospinal Fluid Rhinorrhea Following Transsphenoidal Surgery. Acta Neurochirurgica, 2005. 147(11): p. 1163-1166.
110
152. Black, P.M., N.T. Zervas, and G.L. Candia, Incidence and Management of Complications of Transsphenoidal Operation for Pituitary Adenomas. Neurosurgery, 1987. 20(6): p. 920-4.
153. Dlouhy, B.J., K. Madhavan, J.D. Clinger, A. Reddy, J.D. Dawson, E.K. O'Brien, E. Chang, S.M. Graham, and J.D.W. Greenlee, Elevated Body Mass Index and Risk of Postoperative Csf Leak Following Transsphenoidal Surgery. Journal of neurosurgery, 2012. 116(6): p. 1311-1317.
154. Halvorsen, H., J. Ramm-Pettersen, R. Josefsen, P. Ronning, S. Reinlie, T. Meling, J. Berg-Johnsen, J. Bollerslev, and E. Helseth, Surgical Complications after Transsphenoidal Microscopic and Endoscopic Surgery for Pituitary Adenoma: A Consecutive Series of 506 Procedures. Acta Neurochir (Wien), 2014. 156(3): p. 441-9.
155. Sane, T., K. Rantakari, A. Poranen, R. Tähtelä, M. Välimäki, and R. Pelkonen, Hyponatremia after Transsphenoidal Surgery for Pituitary Tumors. The Journal of Clinical Endocrinology & Metabolism, 1994. 79(5): p. 1395-1398.
156. Olson, B.R., D. Rubino, J. Gumowski, and E.H. Oldfield, Isolated Hyponatremia after Transsphenoidal Pituitary Surgery. The Journal of Clinical Endocrinology & Metabolism, 1995. 80(1): p. 85-91.
157. Gondim, J., J. Almeida, L. Albuquerque, M. Schops, E. Gomes, T. Ferraz, W. Sobreira, and M. Kretzmann, Endoscopic Endonasal Approach for Pituitary Adenoma: Surgical Complications in 301 Patients. Pituitary, 2011. 14(2): p. 174-183.
158. Starke, R.M., D.M. Raper, S.C. Payne, M.L. Vance, E.H. Oldfield, and J.A. Jane, Jr., Endoscopic Vs Microsurgical Transsphenoidal Surgery for Acromegaly: Outcomes in a Concurrent Series of Patients Using Modern Criteria for Remission. J Clin Endocrinol Metab, 2013. 98(8): p. 3190-8.
159. Strychowsky, J., S. Nayan, K. Reddy, F. Farrokhyar, and D. Sommer, Purely Endoscopic Transsphenoidal Surgery Versus Traditional Microsurgery for Resection of Pituitary Adenomas: Systematic Review. J Otolaryngol Head Neck Surg, 2011. 40(2): p. 175-85.
160. Goudakos, J.K., K.D. Markou, and C. Georgalas, Endoscopic Versus Microscopic Trans-Sphenoidal Pituitary Surgery: A Systematic Review and Meta-Analysis. Clinical Otolaryngology, 2011. 36(3): p. 212-220.
161. Cieza, A. and G. Stucki, Content Comparison of Health-Related Quality of Life (Hrqol) Instruments Based on the International Classification of Functioning, Disability and Health (Icf). Quality of Life Research, 2005. 14(5): p. 1225-1237.
162. Andela, C., M. Scharloo, A. Pereira, A. Kaptein, and N. Biermasz, Quality of Life (Qol) Impairments in Patients with a Pituitary Adenoma: A Systematic Review of Qol Studies. Pituitary, 2015. 18(5): p. 752-76.
111
163. Sintonen, H., The 15d Instrument of Health-Related Quality of Life: Properties and Applications. Annals of Medicine, 2001. 33(5): p. 328-336.
164. Badia, X., E. Valassi, M. Roset, and S.M. Webb, Disease-Specific Quality of Life Evaluation and Its Determinants in Cushing’s Syndrome: What Have We Learnt? Pituitary, 2014. 17(2): p. 187-195.
165. Webb, S.M., X. Badia, and N.L.S.f.t.S.A.S. Group, Validity and Clinical Applicability of the Acromegaly Quality of Life Questionnaire, Acroqol: A 6-Month Prospective Study. European Journal of Endocrinology, 2006. 155(2): p. 269-277.
166. Neggers, S.J., M.O. van Aken, W.W. de Herder, R.A. Feelders, J.A. Janssen, X. Badia, S.M. Webb, and A.J. van der Lely, Quality of Life in Acromegalic Patients During Long-Term Somatostatin Analog Treatment with and without Pegvisomant. J Clin Endocrinol Metab, 2008. 93(10): p. 3853-9.
167. Rosilio, M., W.F. Blum, D.J. Edwards, E.P. Shavrikova, D. Valle, S.W.J. Lamberts, E.M. Erfurth, S.M. Webb, R.J. Ross, K. Chihara, G. Henrich, P. Herschbach, and A.F. Attanasio, Long-Term Improvement of Quality of Life During Growth Hormone (Gh) Replacement Therapy in Adults with Gh Deficiency, as Measured by Questions on Life Satisfaction-Hypopituitarism (Qls-H). The Journal of Clinical Endocrinology & Metabolism, 2004. 89(4): p. 1684-1693.
168. McKenna, S.P., L.C. Doward, J. Alonso, T. Kohlmann, M. Niero, L. Prieto, and L. Wiren, The Qol-Aghda: An Instrument for the Assessment of Quality of Life in Adults with Growth Hormone Deficiency. Qual Life Res, 1999. 8(4): p. 373-83.
169. van der Klaauw, A.A., M. Kars, N.R. Biermasz, F. Roelfsema, O.M. Dekkers, E.P. Corssmit, M.O. van Aken, B. Havekes, A.M. Pereira, H. Pijl, J.W. Smit, and J.A. Romijn, Disease-Specific Impairments in Quality of Life During Long-Term Follow-up of Patients with Different Pituitary Adenomas. Clinical endocrinology, 2008. 69(5): p. 775-784.
170. Kars, M., A.A. van der Klaauw, C.S. Onstein, A.M. Pereira, and J.A. Romijn, Quality of Life Is Decreased in Female Patients Treated for Microprolactinoma. European Journal of Endocrinology, 2007. 157(2): p. 133-139.
171. Cesar de Oliveira Naliato, E., Quality of Life in Women with Microprolactinoma Treated with Dopamine Agonists. Pituitary, 2008. 11(3): p. 247-54.
172. Raappana, A., T. Pirila, T. Ebeling, P. Salmela, H. Sintonen, and J. Koivukangas, Long-Term Health-Related Quality of Life of Surgically Treated Pituitary Adenoma Patients: A Descriptive Study. Isrn Endocrinology Print, 2012. 2012: p. 675310.
173. Leon-Carrion, J., J.F. Martin-Rodriguez, A. Madrazo-Atutxa, A. Soto-Moreno, E. Venegas-Moreno, E. Torres-Vela, P. Benito-López, M.Á. Gálvez, F.J. Tinahones, and A. Leal-Cerro, Evidence of Cognitive and

112
Neurophysiological Impairment in Patients with Untreated Naive Acromegaly. The Journal of Clinical Endocrinology & Metabolism, 2010. 95(9): p. 4367-4379.
174. Biermasz, N.R., S.W.v. Thiel, A.M. Pereira, H.C. Hoftijzer, A.M.v. Hemert, J.W.A. Smit, J.A. Romijn, and F. Roelfsema, Decreased Quality of Life in Patients with Acromegaly Despite Long-Term Cure of Growth Hormone Excess. The Journal of Clinical Endocrinology & Metabolism, 2004. 89(11): p. 5369-5376.
175. Kauppinen-Mäkelin, R., T. Sane, H. Sintonen, H. Markkanen, M.J. Välimäki, E. Löyttyniemi, L. Niskanen, A. Reunanen, and U.-H. Stenman, and the Finnish Acromegaly Study Group, Quality of Life in Treated Patients with Acromegaly. The Journal of Clinical Endocrinology & Metabolism, 2006. 91(10): p. 3891-3896.
176. Trepp, R., Assessment of Quality of Life in Patients with Uncontrolled Vs. Controlled Acromegaly Using the Acromegaly Quality of Life Questionnaire (Acroqol). Clinical endocrinology, 2005. 63(1): p. 103-110.
177. Matta, M.P., Impaired Quality of Life of Patients with Acromegaly: Control of Gh/Igf-I Excess Improves Psychological Subscale Appearance. European journal of endocrinology, 2008. 158(3): p. 305-310.
178. Rubeck, K.Z., M. Madsen, C.M. Andreasen, S. Fisker, J. Frystyk, and J.O.L. Jørgensen, Conventional and Novel Biomarkers of Treatment Outcome in Patients with Acromegaly: Discordant Results after Somatostatin Analog Treatment Compared with Surgery. European Journal of Endocrinology, 2010. 163(5): p. 717-726.
179. Postma, M.R., R.T. Netea-Maier, G. van den Berg, J. Homan, W.J. Sluiter, M.A. Wagenmakers, A.C. van den Bergh, B.H. Wolffenbuttel, A.R. Hermus, and A.P. van Beek, Quality of Life Is Impaired in Association with the Need for Prolonged Postoperative Therapy by Somatostatin Analogs in Patients with Acromegaly. European Journal of Endocrinology, 2012. 166(4): p. 585-592.
180. Lindsay, J.R., T. Nansel, S. Baid, J. Gumowski, and L.K. Nieman, Long-Term Impaired Quality of Life in Cushing’s Syndrome Despite Initial Improvement after Surgical Remission. The Journal of Clinical Endocrinology & Metabolism, 2006. 91(2): p. 447-453.
181. Valassi, E., A. Santos, M. Yaneva, M. Tóth, C.J. Strasburger, P. Chanson, J.A.H. Wass, O. Chabre, M. Pfeifer, R.A. Feelders, S. Tsagarakis, P.J. Trainer, H. Franz, K. Zopf, S. Zacharieva, S.W.J. Lamberts, A. Tabarin, and S.M. Webb, The European Registry on Cushing's Syndrome: 2-Year Experience. Baseline Demographic and Clinical Characteristics. European Journal of Endocrinology, 2011. 165(3): p. 383-392.
182. Santos, A., E. Resmini, M.A. Martinez-Momblan, I. Crespo, E. Valassi, M. Roset, X. Badia, and S.M. Webb, Psychometric

113
Performance of the Cushingqol Questionnaire in Conditions of Real Clinical Practice. Eur J Endocrinol, 2012. 167(3): p. 337-42.
183. Wagenmakers, M.A.E.M., R.T. Netea-Maier, J.B. Prins, T. Dekkers, M. den Heijer, and A.R.M.M. Hermus, Impaired Quality of Life in Patients in Long-Term Remission of Cushing's Syndrome of Both Adrenal and Pituitary Origin: A Remaining Effect of Long-Standing Hypercortisolism? European Journal of Endocrinology, 2012. 167(5): p. 687-695.
184. Aken, M.O.v., A.M. Pereira, N.R. Biermasz, S.W.v. Thiel, H.C. Hoftijzer, J.W.A. Smit, F. Roelfsema, S.W.J. Lamberts, and J.A. Romijn, Quality of Life in Patients after Long-Term Biochemical Cure of Cushing’s Disease. The Journal of Clinical Endocrinology & Metabolism, 2005. 90(6): p. 3279-3286.
185. Lindholm, J., S. Juul, J.O.L. Jorgensen, J. Astrup, P. Bjerre, U. Feldt-Rasmussen, C. Hagen, J. Jorgensen, M. Kosteljanetz, L.O. Kristensen, P. Laurberg, K. Schmidt, and J. Weeke, Incidence and Late Prognosis of Cushing's Syndrome: A Population-Based Study*. Journal of Clinical Endocrinology & Metabolism, 2001. 86(1): p. 117-123.
186. Pikkarainen, L., T. Sane, and A. Reunanen, The Survival and Well-Being of Patients Treated for Cushing's Syndrome. Journal of internal medicine, 1999. 245(5): p. 463-468.
187. Webb, S.M., X. Badia, M.J. Barahona, A. Colao, C.J. Strasburger, A. Tabarin, M.O. van Aken, R. Pivonello, G. Stalla, S.W.J. Lamberts, and J.E. Glusman, Evaluation of Health-Related Quality of Life in Patients with Cushing's Syndrome with a New Questionnaire. European Journal of Endocrinology, 2008. 158(5): p. 623-630.
188. Dekkers, O.M., A.A. van der Klaauw, A.M. Pereira, N.R. Biermasz, P.J. Honkoop, F. Roelfsema, J.W. Smit, and J.A. Romijn, Quality of Life Is Decreased after Treatment for Nonfunctioning Pituitary Macroadenoma. Journal of Clinical Endocrinology & Metabolism, 2006. 91(9): p. 3364-3369.
189. Biermasz, N.R., S.D. Joustra, E. Donga, A.M. Pereira, N.v. Duinen, M.v. Dijk, A.A.v.d. Klaauw, E.P.M. Corssmit, G.J. Lammers, K.W.v. Kralingen, J.G.v. Dijk, and J.A. Romijn, Patients Previously Treated for Nonfunctioning Pituitary Macroadenomas Have Disturbed Sleep Characteristics, Circadian Movement Rhythm, and Subjective Sleep Quality. The Journal of Clinical Endocrinology & Metabolism, 2011. 96(5): p. 1524-1532.
190. Capatina, C., C. Christodoulides, A. Fernandez, S. Cudlip, A.B. Grossman, J.A.H. Wass, and N. Karavitaki, Current Treatment Protocols Can Offer a Normal or near-Normal Quality of Life in the Majority of Patients with Non-Functioning Pituitary Adenomas. Clinical endocrinology, 2013. 78(1): p. 86-93.
191. Nielsen, E.H., J. Lindholm, P. Laurberg, P. Bjerre, J.S. Christiansen, C. Hagen, S. Juul, J. Jorgensen, A. Kruse, and K. Stochholm,
114
Nonfunctioning Pituitary Adenoma: Incidence, Causes of Death and Quality of Life in Relation to Pituitary Function. Pituitary, 2007. 10(1): p. 67-73.
192. Tanemura, E., T. Nagatani, Y. Aimi, Y. Kishida, K. Takeuchi, and T. Wakabayashi, Quality of Life in Nonfunctioning Pituitary Macroadenoma Patients before and after Surgical Treatment. Acta Neurochirurgica, 2012. 154(10): p. 1895-1902.
193. van Beek, A.P., A.C. van den Bergh, L.M. van den Berg, G. van den Berg, J.C. Keers, J.A. Langendijk, and B.H. Wolffenbuttel, Radiotherapy Is Not Associated with Reduced Quality of Life and Cognitive Function in Patients Treated for Nonfunctioning Pituitary Adenoma. Int J Radiat Oncol Biol Phys, 2007. 68(4): p. 986-91.
194. Page, R.C.L., M.S. Hammersley, C.W. Burke, and J.A.H. Wass, An Account of the Quality of Life of Patients after Treatment for Non-Functioning Pituitary Tumours. Clinical Endocrinology, 1997. 46(4): p. 401-406.
195. Dunn, L.K. and E.C. Nemergut, Anesthesia for Transsphenoidal Pituitary Surgery. Curr Opin Anaesthesiol, 2013. 26(5): p. 549-54.
196. Kontogeorgos, G., Predictive Markers of Pituitary Adenoma Behavior. Neuroendocrinology, 2006. 83(3-4): p. 179-188.
197. Shahlaie, K., N. McLaughlin, A.B. Kassam, and D.F. Kelly, The Role of Outcomes Data for Assessing the Expertise of a Pituitary Surgeon. Current Opinion in Endocrinology, Diabetes & Obesity, 2010. 17(4): p. 369-376.
198. Giustina, A., A. Barkan, F.F. Casanueva, F. Cavagnini, L. Frohman, K. Ho, J. Veldhuis, J. Wass, K. Von Werder, and S. Melmed, Criteria for Cure of Acromegaly: A Consensus Statement. J Clin Endocrinol Metab, 2000. 85(2): p. 526-9.
199. Meier, C.A. and B.M. Biller, Clinical and Biochemical Evaluation of Cushing's Syndrome. Endocrinol Metab Clin North Am, 1997. 26(4): p. 741-62.
200. Eisenhauer, E.A., P. Therasse, J. Bogaerts, L.H. Schwartz, D. Sargent, R. Ford, J. Dancey, S. Arbuck, S. Gwyther, M. Mooney, L. Rubinstein, L. Shankar, L. Dodd, R. Kaplan, D. Lacombe, and J. Verweij, New Response Evaluation Criteria in Solid Tumours: Revised Recist Guideline (Version 1.1). Eur J Cancer, 2009. 45(2): p. 228-47.
201. Leach, P., A.H. AbouZeid, T. Kearney, J. Davis, P.J. Trainer, and K.K. Gnanalingham, Endoscopic Transsphenoidal Pituitary Surgery: Evidence of an Operative Learning Curve. Neurosurgery, 2010. 67(5): p. 1205-1212.
202. Casler, J.D., A.M. Doolittle, and E.A. Mair, Endoscopic Surgery of the Anterior Skull Base. The Laryngoscope, 2005. 115(1): p. 16-24.
203. Higgins, T.S., C. Courtemanche, D. Karakla, B. Strasnick, R.V. Singh, J.L. Koen, and J.K. Han, Analysis of Transnasal Endoscopic Versus
115
Transseptal Microscopic Approach for Excision of Pituitary Tumors. American Journal of Rhinology, 2008. 22(6): p. 649-652.
204. Zhang, X., Z. Fei, J. Zhang, L. Fu, Z. Zhang, W. Liu, and Y. Chen, Management of Nonfunctioning Pituitary Adenomas with Suprasellar Extensions by Transsphenoidal Microsurgery. Surgical neurology, 1999. 52(4): p. 380-385.
205. Honegger, J., U. Ernemann, T. Psaras, and B. Will, Objective Criteria for Successful Transsphenoidal Removal of Suprasellar Nonfunctioning Pituitary Adenomas. A Prospective Study. Acta Neurochirurgica, 2007. 149(1): p. 21-29.
206. Sam, A.H., S. Shah, K. Saleh, J. Joshi, F. Roncaroli, S. Robinson, J. Cox, N.M. Martin, N. Mendoza, K. Meeran, A. Mehta, and W.S. Dhillo, Clinical Outcomes in Patients with Nonfunctioning Pituitary Adenomas Managed Conservatively. Clin Endocrinol (Oxf), 2015.
207. Cappabianca, P., L.M. Cavallo, F. Esposito, V. Valente, and E. de Divitiis, Sellar Repair in Endoscopic Endonasal Transsphenoidal Surgery: Results of 170 Cases. Neurosurgery, 2002. 51(6): p. 1365-1372.
208. Kabil, M.S., J.B. Eby, and H.K. Shahinian, Fully Endoscopic Endonasal Vs. Transseptal Transsphenoidal Pituitary Surgery. Minimally Invasive Neurosurgery, 2005. 48(6): p. 348-354.
209. Tiemensma, J., A.A. Kaptein, A.M. Pereira, J.W. Smit, J.A. Romijn, and N.R. Biermasz, Affected Illness Perceptions and the Association with Impaired Quality of Life in Patients with Long-Term Remission of Acromegaly. J Clin Endocrinol Metab, 2011. 96(11): p. 3550-8.
210. Brummelman, P., M.F. Elderson, R.P.F. Dullaart, A.C.M. van den Bergh, C.A. Timmer, G. van den Berg, J. Koerts, O. Tucha, B.H.R. Wolffenbuttel, and A.P. van Beek, Cognitive Functioning in Patients Treated for Nonfunctioning Pituitary Macroadenoma and the Effects of Pituitary Radiotherapy. Clinical Endocrinology, 2011. 74(4): p. 481-487.
211. Van Beek, A.P., Radiotherapy Is Not Associated with Reduced Quality of Life and Cognitive Function in Patients Treated for Nonfunctioning Pituitary Adenoma. International journal of radiation oncology biology physics, 2007. 68(4): p. 986-991.
212. Hawthorne, G., J. Richardson, and N.A. Day, A Comparison of the Assessment of Quality of Life (Aqol) with Four Other Generic Utility Instruments. Ann Med, 2001. 33(5): p. 358-70.
213. Koskinen, S., A. Lundqvist, and N. Ristiluoma, Health, Functional Capacity and Welfare in Finland in 2011, 2012, National Institute for Health and Welfare (THL): Helsinki.
214. Kauppinen-Makelin, R., T. Sane, H. Sintonen, H. Markkanen, M.J. Valimaki, E. Loyttyniemi, L. Niskanen, A. Reunanen, U.H. Stenman, and G. the Finnish Acromegaly Study, Quality of Life in Treated
116
Patients with Acromegaly. Journal of Clinical Endocrinology & Metabolism, 2006. 91(10): p. 3891-3896.
215. Alanne, S., R. Roine, P. Räsänen, T. Vainiola, and H. Sintonen, Estimating the Minimum Important Change in the 15d Scores. Quality of Life Research, 2015. 24(3): p. 599-606.
216. Alonso, J., M. Ferrer, B. Gandek, J.E. Ware, Jr., N.K. Aaronson, P. Mosconi, N.K. Rasmussen, M. Bullinger, S. Fukuhara, S. Kaasa, and A. Leplege, Health-Related Quality of Life Associated with Chronic Conditions in Eight Countries: Results from the International Quality of Life Assessment (Iqola) Project. Qual Life Res, 2004. 13(2): p. 283-98.
217. Alonso, J., M.C. Angermeyer, S. Bernert, R. Bruffaerts, T.S. Brugha, H. Bryson, G. de Girolamo, R. Graaf, K. Demyttenaere, I. Gasquet, J.M. Haro, S.J. Katz, R.C. Kessler, V. Kovess, J.P. Lepine, J. Ormel, G. Polidori, L.J. Russo, G. Vilagut, J. Almansa, S. Arbabzadeh-Bouchez, J. Autonell, M. Bernal, M.A. Buist-Bouwman, M. Codony, A. Domingo-Salvany, M. Ferrer, S.S. Joo, M. Martinez-Alonso, H. Matschinger, F. Mazzi, Z. Morgan, P. Morosini, C. Palacin, B. Romera, N. Taub, and W.A. Vollebergh, Disability and Quality of Life Impact of Mental Disorders in Europe: Results from the European Study of the Epidemiology of Mental Disorders (Esemed) Project. Acta Psychiatr Scand Suppl, 2004(420): p. 38-46.
218. Song, X., J. Pitkaniemi, W. Gao, R.J. Heine, K. Pyorala, S. Soderberg, C.D.A. Stehouwer, B. Zethelius, J. Tuomilehto, T. Laatikainen, A.G. Tabak, and Q. Qiao, Relationship between Body Mass Index and Mortality among Europeans. Eur J Clin Nutr, 2012. 66(2): p. 156-165.
219. Kolotkin, R.L., K. Meter, and G.R. Williams, Quality of Life and Obesity. Obes Rev, 2001. 2(4): p. 219-29.
220. Taylor, V.H., M. Forhan, S.N. Vigod, R.S. McIntyre, and K.M. Morrison, The Impact of Obesity on Quality of Life. Best Practice & Research Clinical Endocrinology & Metabolism, 2013. 27(2): p. 139-146.
221. Santos, A., Quality of Life in Patients with Pituitary Tumors. Current opinion in endocrinology diabetes and obesity, 2009. 16(4): p. 299-303.
222. Hunt, S.M., J. McEwen, and S.P. McKenna, Perceived Health: Age and Sex Comparisons in a Community. J Epidemiol Community Health, 1984. 38(2): p. 156-60.
223. Celik, O., E. Hatipoglu, S. Akhan, uuml, E. leyman, S. Uludag, and P. Kadioglu, Acromegaly Is Associated with Higher Frequency of Female Sexual Dysfunction: Experience of a Single Center. Endocrine Journal, 2013. 60(6): p. 753-761.
224. Paisley, A.N., S.V. Rowles, M.E. Roberts, S.M. Webb, X. Badia, L. Prieto, S.M. Shalet, and P.J. Trainer, Treatment of Acromegaly
117
Improves Quality of Life, Measured by Acroqol. Clin Endocrinol (Oxf), 2007. 67(3): p. 358-62.
225. van der Klaauw, A.A., N.R. Biermasz, H.C. Hoftijzer, A.M. Pereira, and J.A. Romijn, Previous Radiotherapy Negatively Influences Quality of Life During 4 Years of Follow-up in Patients Cured from Acromegaly. Clinical endocrinology, 2008. 69(1): p. 123-128.
226. Mangupli, R., P. Camperos, and S.M. Webb, Biochemical and Quality of Life Responses to Octreotide-Lar in Acromegaly. Pituitary, 2014. 17(6): p. 495-9.
227. Rasanen, P., K. Krootila, H. Sintonen, T. Leivo, A.M. Koivisto, O.P. Ryynanen, M. Blom, and R.P. Roine, Cost-Utility of Routine Cataract Surgery. Health Qual Life Outcomes, 2006. 4: p. 74.