Embed Size (px)
DESCRIPTION
picu
Citation preview
Ostomy Care(Managing the Premature
Neonate’s Stoma)
Prof. Maria Isabelita C. Rogado, RN, MAN8th Annual Convention, SPCCMP
January 18 – 20, 2012
Iloilo City
Objectives:1. Focus on managing the pre-term neonate’s stoma
2. Review briefly common diseases affecting the pre-term neonates that result in fecal diversion
3. Discuss ostomy management particularly skin barrier properties
4. Identify guidelines and practical strategies for managing premature ostomates.
Disclosure: NO grant or support has been received from any product company for this presentation!
INTRODUCTION
NICU personnel and pediatric surgeons have successfully improve the survival rates of premature neonates.
Surgical creation of fecal stomas allowing recovery of disease organs and surgical anastomosis distal to enterostomy
Usually temporary, creating a stage in the surgical management of congenital or acquired disease.
Caring for these low, very low or extremely low birth weight infants with their tiny stomas can be challenging and frustrating.
Challenges• Wide variety of stomas and stomal complications• More ostomy products that can be used• However: NOT available
LACK knowledge
• Stoma care is inappropriate for low gestational age infants
• Inconsistent care among caregivers• Ineffective care in containing effluent from stoma and
preventing stomal complications
Common Conditions Requiring Stomas in Premature Infants
• Necrotizing Entero-Colitis (NEC)• Anorectal Malformation• Hirschsprung Disease (HD)• Meconium Ileus• Intestinal Atresia
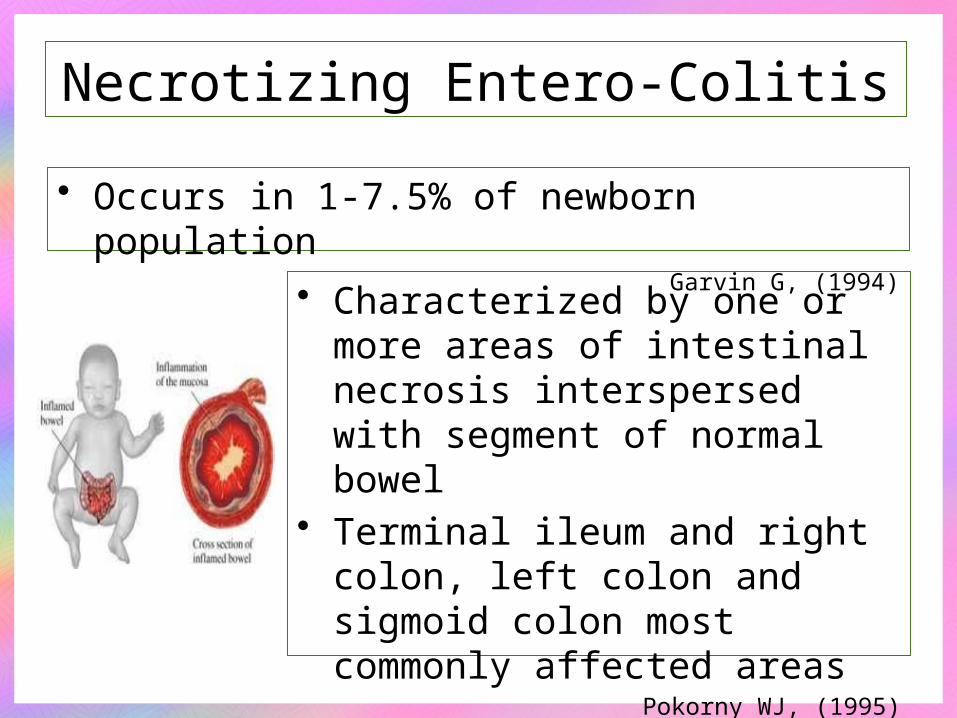
Necrotizing Entero-Colitis
• Occurs in 1-7.5% of newborn populationGarvin G, (1994)
• Characterized by one or more areas of intestinal necrosis interspersed with segment of normal bowel
• Terminal ileum and right colon, left colon and sigmoid colon most commonly affected areas
Pokorny WJ, (1995)
Necrotizing Entero-Colitis
Pathogenesis:• Availability of a substrate such as formula• Ischemic mucosal injury of the intestine
during perinatal asphyxia• Hypothermia or vasospasm during
umbilical artery catheterization• Bacterial colonization
Roberts P. (1990)
Necrotizing Entero-Colitis
Medical Management:• Bowel rest• NG decompression• IV alimentation• Transfusion• Antibiotics
Necrotizing Entero-Colitis
Surgical Interventions:• Indicated only if infants fail to respond to
medical management or• When gangrene develops or perforation of
the bowel occursSurgery is required in 25 – 50% of
newborn with NECCaty, M et al (2000)

Anorectal Malformations
• Occurs in 1 in 4000 birthsPeña, A. (1994)
• Encompass wide range of congenital abnormalitiesGI, urinary, and reproductive
systemsResults in abnormal
communications between rectum, GUT, or perineum
Guardino KO, (2000)
Anorectal Malformations
Requires immediate surgery:• If passage of urine or stool is obstructed• Feces is diverted via descending
colostomy (double barrel or loop) until infant is old enough to tolerate definitive surgical correction of the defect
• Complex anorectal malformation requires extensive surgical management
Peña, A.(1994)
Kiely EM; Peña, A. (1995)
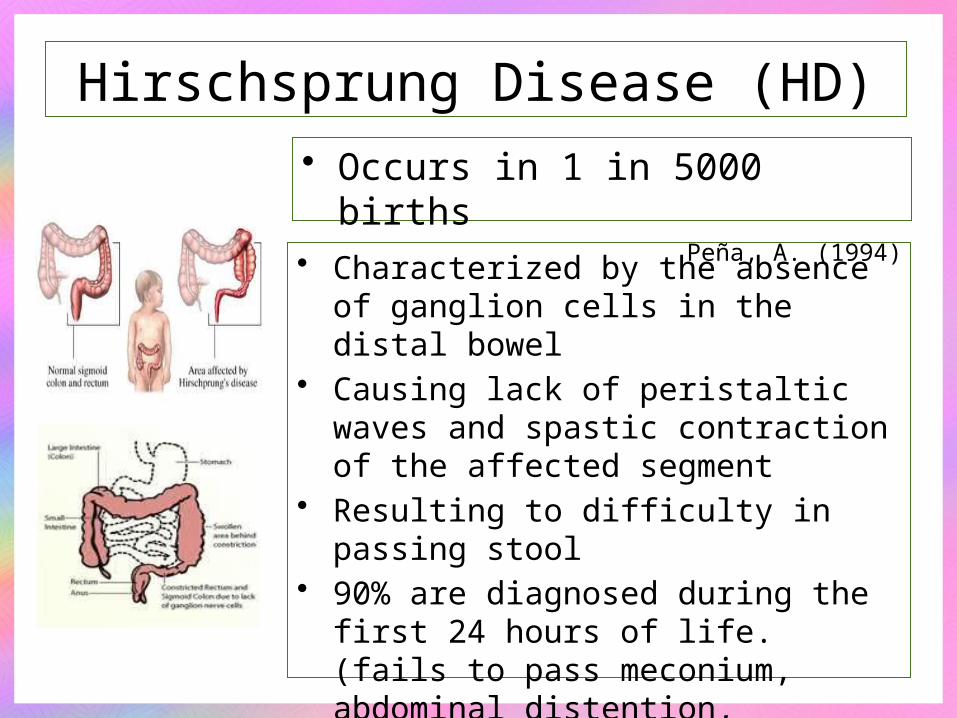
Hirschsprung Disease (HD)• Occurs in 1 in 5000 births
Peña, A. (1994)
• Characterized by the absence of ganglion cells in the distal bowel
• Causing lack of peristaltic waves and spastic contraction of the affected segment
• Resulting to difficulty in passing stool• 90% are diagnosed during the first 24
hours of life. (fails to pass meconium, abdominal distention, vomiting)
Puri, P. (1997)
Hirschsprung Disease (HD)
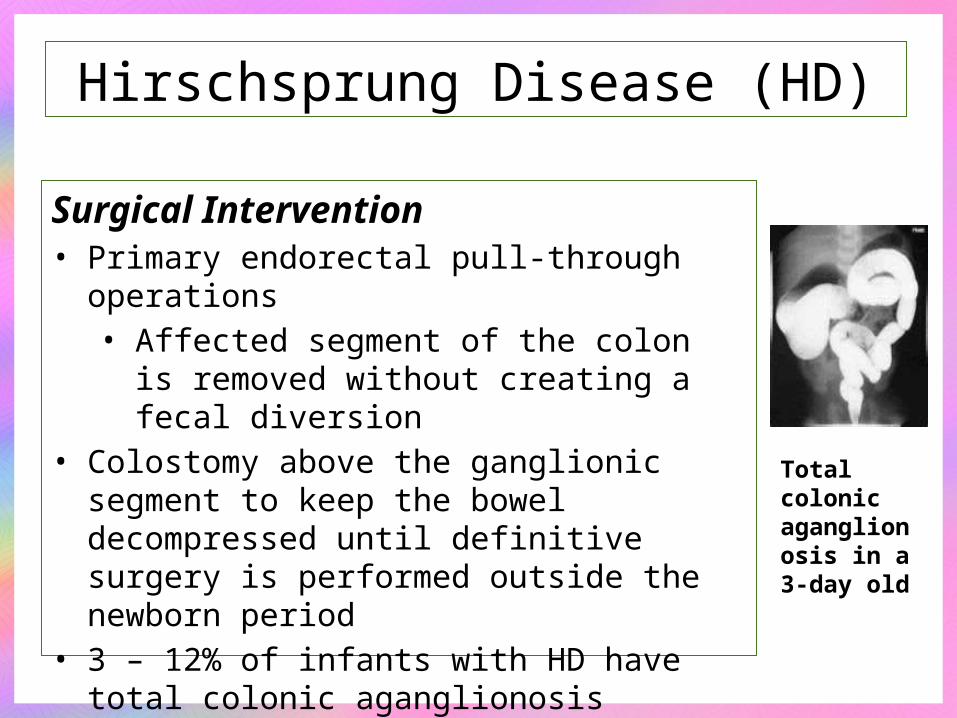
Surgical Intervention• Primary endorectal pull-through operations
• Affected segment of the colon is removed without creating a fecal diversion
• Colostomy above the ganglionic segment to keep the bowel decompressed until definitive surgery is performed outside the newborn period
• 3 – 12% of infants with HD have total colonic aganglionosis
Puri, P. (1997)
Total colonic aganglionosis in a 3-day old
Meconium Ileus• Results from abnormalities of the exocrine
mucous secretion• Contribute to the production of thick, sticky
meconium that obstruct the small intestinal lumen
• 95% of patients with meconium ileus will have cystic fibrosis
• Obstruction occurs in the distal 15 -30 cm terminal ileus
Haga, LI. (1999)
Meconium IleusManagement:• Resection of the dilated ileus and formation of
an ileostomy• Simple meconium ileus: instillation of N-
acetylcysteine into the bowel lumen through one or more enterostomies • soften inspissated stool, • manipulation of the bowel to move the
meconium into the colon where it can be easily expelled
Groff, DB. (2000)
Meconium IleusManagement:• Complicated meconium ileus
• Occurs when meconium contaminates peritoneum in utero / in the immediate perinatal period
• Bowel perforation + spillage of meconium results to • meconium ileus • Volvulus• Intestinal atresia or• Stenosis
• Surgical intervention is required Rescarla FJ, (1998)
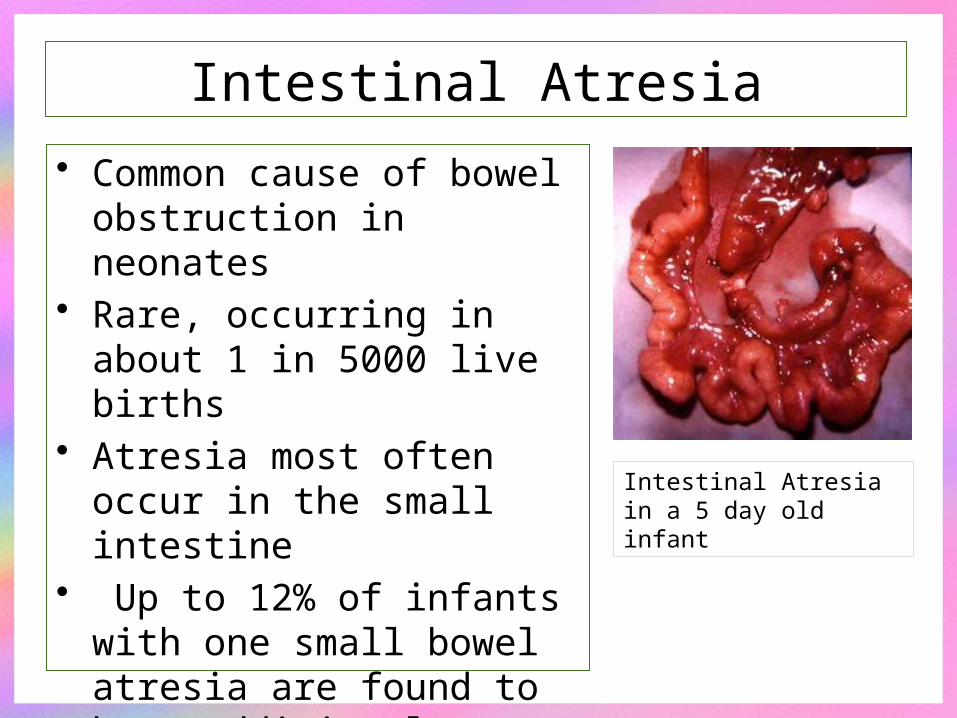
Intestinal Atresia
• Common cause of bowel obstruction in neonates
• Rare, occurring in about 1 in 5000 live births
• Atresia most often occur in the small intestine
• Up to 12% of infants with one small bowel atresia are found to have additional atresia
Newman K.. (1997)
Intestinal Atresia in a 5 day old infant
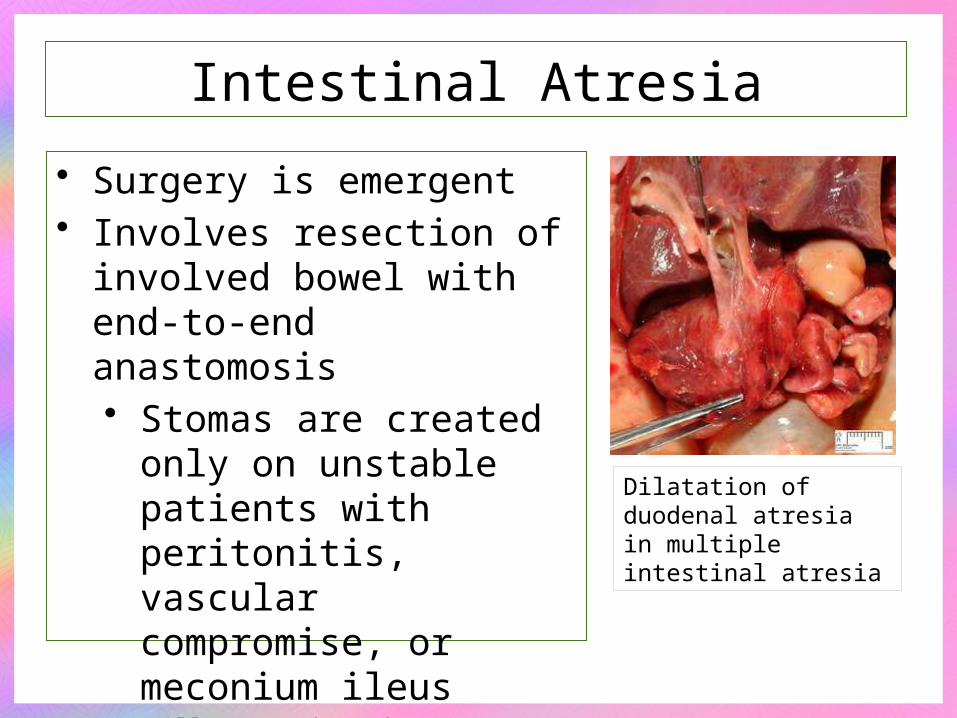
Intestinal Atresia
• Surgery is emergent• Involves resection of
involved bowel with end-to-end anastomosis• Stomas are created only
on unstable patients with peritonitis, vascular compromise, or meconium ileus
Millar , Rode and Cywes (2000)
Dilatation of duodenal atresia in multiple intestinal atresia

Preterm Infant Skin: Characteristics

Preterm Infant Skin: Characteristics
Physiologically and structurally immature requiring specialized care particularly
when the infant has enterostomy.
FUNCTION OF THE SKIN
• Acts an interface between the infants internal environment and outside world
• Regulates transepidermal water loss• Helps maintain electrolyte homeostasis• Function in thermoregulation and minimizes caloric expenditure
• Provides protection from environmental toxins, trauma, microorganism and UV radiation
• Perceives tactile sensation
ESSENTIALS IN PERFORMANCE OF SKIN FUNCTIONS
Competent Epidermal BarrierStrong Transepidermal AbsorptionAdequate Dermal-Epidermal JunctionAppropriate Ratio of Surface Area to Body
Weight Stable Acid MantleEfficient Nutritional Status
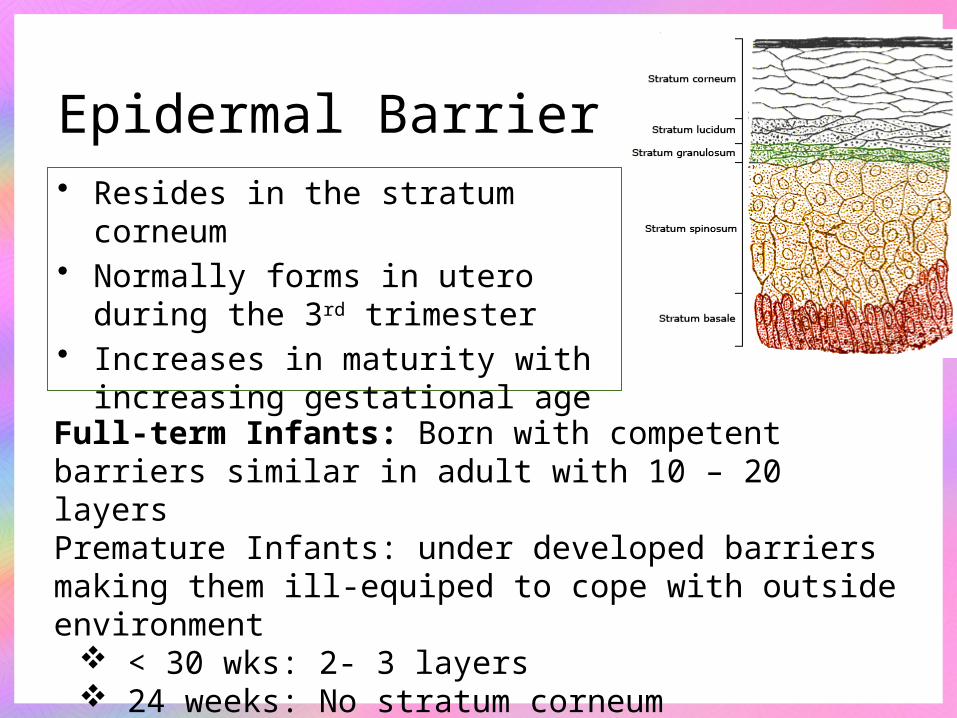
Epidermal Barrier• Resides in the stratum corneum• Normally forms in utero during the
3rd trimester• Increases in maturity with increasing
gestational age
Full-term Infants: Born with competent barriers similar in adult with 10 – 20 layersPremature Infants: under developed barriers making them ill-equiped to cope with outside environment
< 30 wks: 2- 3 layers 24 weeks: No stratum corneum
Lund C., (1999)
Incompetent Epidermal Barrier
Increase transepidermal absorption of topical agents
Increase susceptibility to chemical and mechanical injury
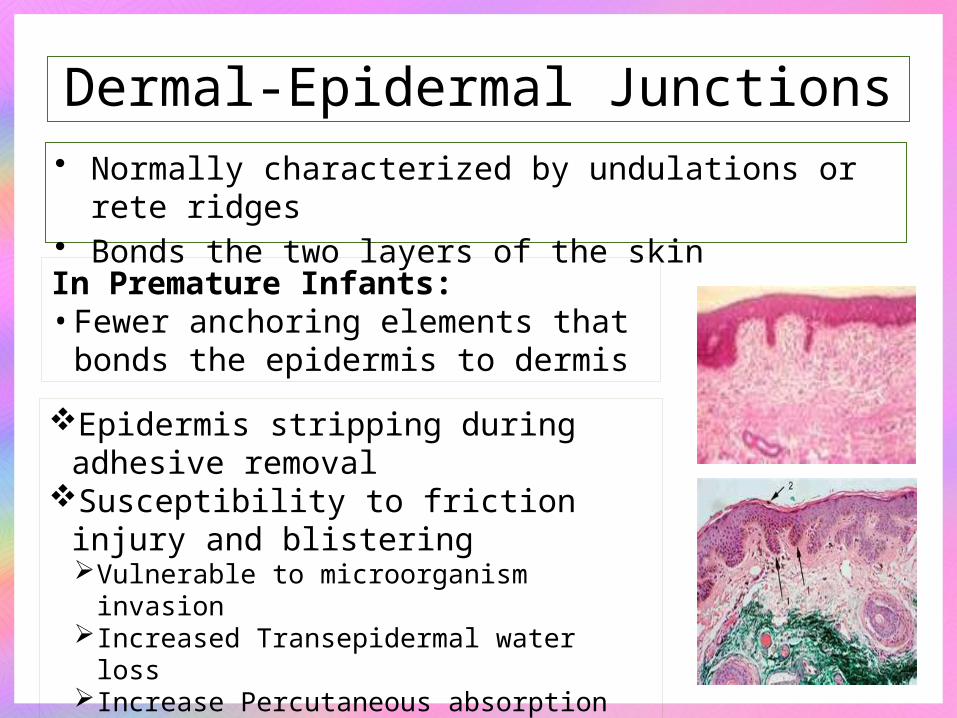
Dermal-Epidermal Junctions• Normally characterized by undulations or rete ridges• Bonds the two layers of the skin
In Premature Infants:• Fewer anchoring elements that bonds
the epidermis to dermis
Epidermis stripping during adhesive removal
Susceptibility to friction injury and blisteringVulnerable to microorganism invasionIncreased Transepidermal water lossIncrease Percutaneous absorption
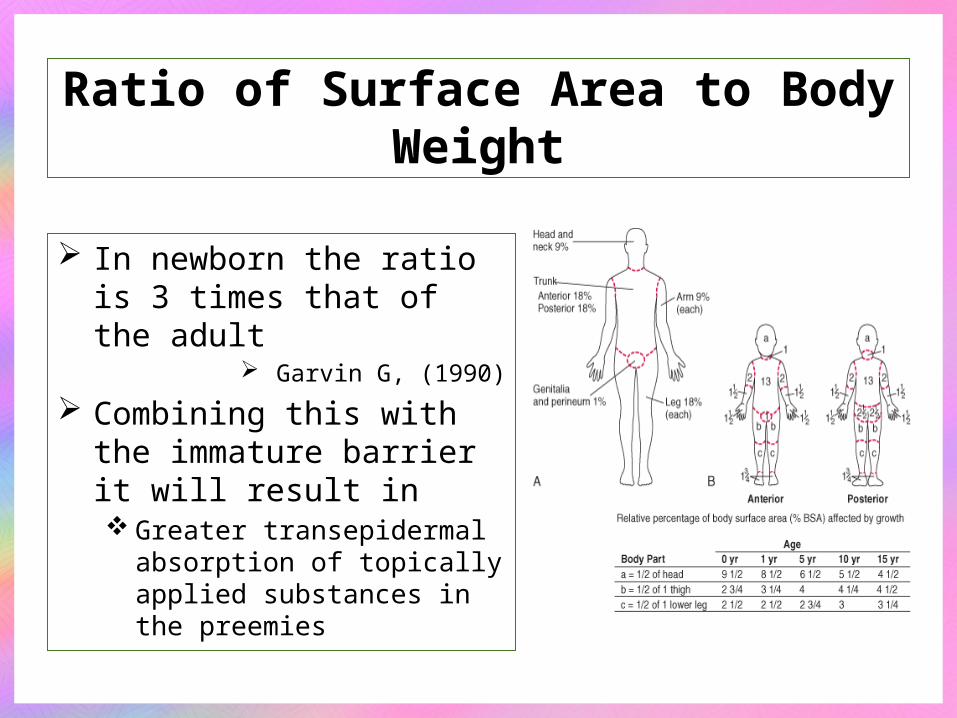
Ratio of Surface Area to Body Weight
In newborn the ratio is 3 times that of the adult
Garvin G, (1990)
Combining this with the immature barrier it will result in Greater transepidermal
absorption of topically applied substances in the preemies
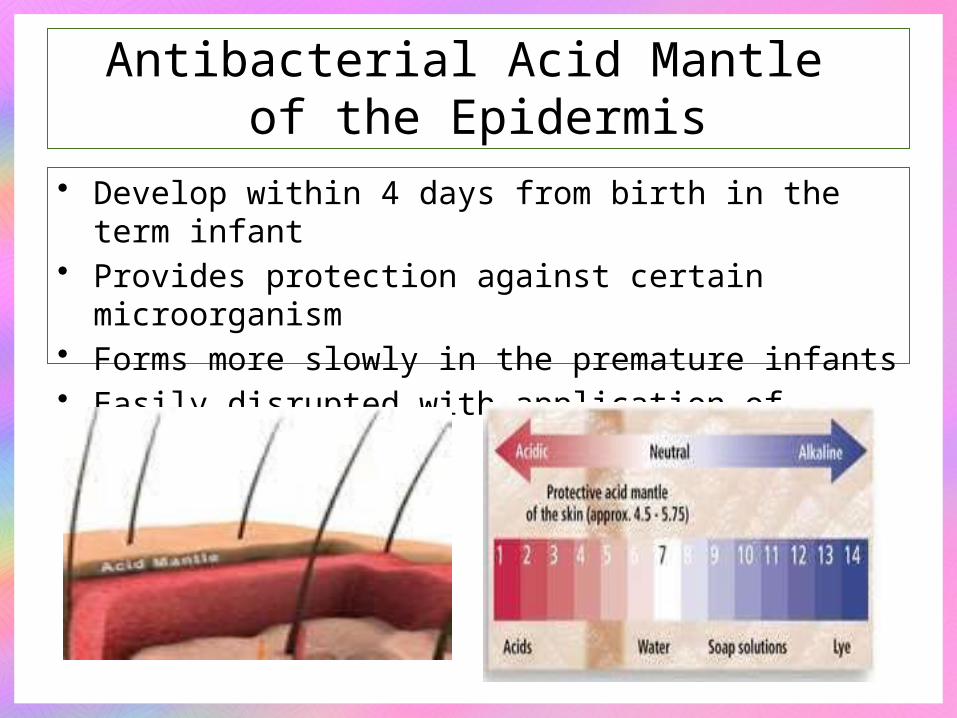
Antibacterial Acid Mantle of the Epidermis
• Develop within 4 days from birth in the term infant• Provides protection against certain microorganism• Forms more slowly in the premature infants• Easily disrupted with application of topical agents

Nutritional Status
• Preterm infants are at risks for the deficiencies in nutrients stored during the latter part of pregnancy
• Neonates with stomas are furthermore, at risk for mal-absorption
Garvin G (1990)
Due to shortened GI tractDecreased absorptive surface area
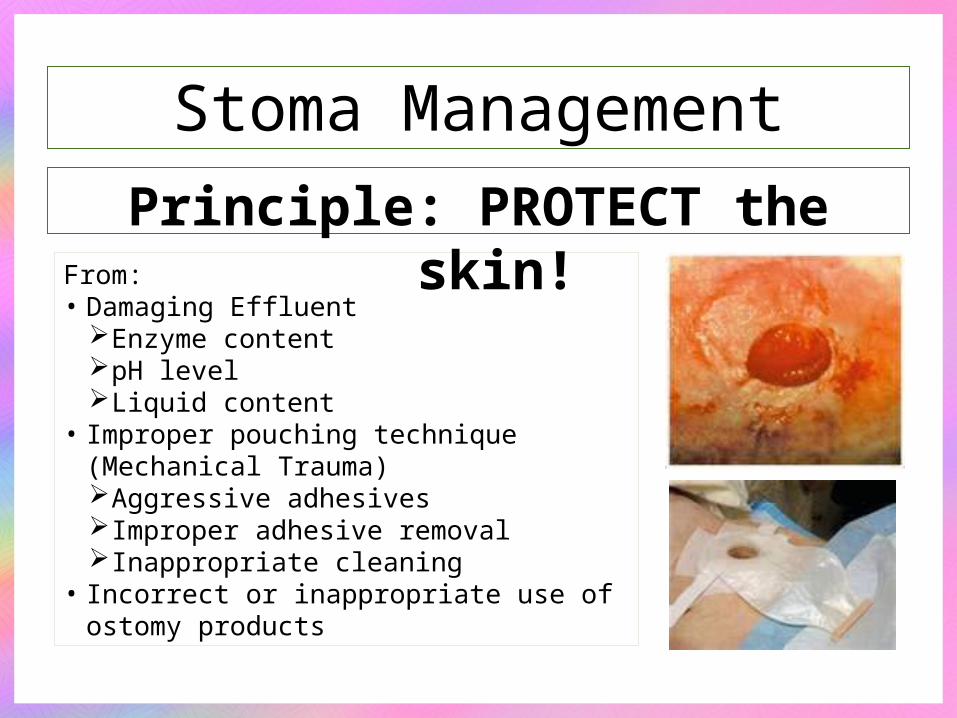
Stoma Management
Principle: PROTECT the skin!From:• Damaging Effluent
Enzyme contentpH levelLiquid content
• Improper pouching technique (Mechanical Trauma)Aggressive adhesivesImproper adhesive removalInappropriate cleaning
• Incorrect or inappropriate use of ostomy products

Many ostomy products and management techniques used effectively for an older child or adult ostomates may NOT be safely used in preterm infant.
Removal and Replacement of Ostomy Appliance
Loosen the barrier adhesive with soft cloth dampen with warm water.
Soap containing surfactant is helpful in decreasing friction required to remove adhesive barrier from skin with out trauma.
Nix DH, 2000
Removal and Replacement of Ostomy Appliance
Adhesive removers used in adults should not be used in infants.
It can cause toxic epidermal necroly due to exposure from petroleum distillates in infants of 26 weeks’ gestation after using it in removing electrodes
Ittman, PL, Bozynski ME, 2000
Contain alcohol causing topical and systemic effect like skin blisters, burn, necrosis, death due to elevated blood alcohol level.
Harpin V., 1982Schick JB, 1981
Removal and Replacement of Ostomy Appliance
Use of adhesive removers should be limited to situations in which adhesives are so bonded to the infants’ skin that they can not be removed without risking damage to the fragile epidermis
Removal and Replacement of Ostomy Appliance
Remember!Thoroughly wash and rinse the skin to
remove any chemical residuePectin remaining on the skin should not
interfere with pouch adherence and is not damaging to the skin… so do not remove it vigorously.
Rogers V., 2003
Removal and Replacement of Ostomy Appliance
Gently clean the peristomal skin with water between pouch applications.
Use of soup is discouraged: Residue left under the barrier could cause chemical dermatitis
If soap is used: pH neutralNo antibacterial No deodorant additivesRinsed well from skin
Rogers V., 2003

What should be avoided?• Alkaline Soap
Disrupts the acid mantle of preterm’s skin up to 7 days crippling an important barrier to infection
Kuller JM, 1993
• Moisturizing SoapShould be avoided ; interferes with pouch adherence
• Commercial WipesLanolin-based with alcohol; not suitable for cleansing
peristomal skin
Skin Sealants / Barriers Plasticizing agents applied to the skin to create barrier Protects from corrosive effects of stool Effectively used in incontinent population Contains alcohol as solvent Not used on the preterm infant Reduced adherence of appliance due to the plasticized
filmErwin-Toth P, Doughty DB, 1992

Currently, the only alcohol-free skin sealant on the market is CAVALON No Sting Film (3M)

Choosing an Appliance
Consider the following: Size of the infants abdomen Diameter and profile of the stoma Number and proximity of stoma Consistency and content of digestive enzymes (effluent) Volume of stool and gas effluent from stoma Presence of abdominal contours and scars Peristomal skin integrity Cost and product availability
Recommendation for Selection• Familiarity!• Determine which product is appropriate for a particular
patient or situation• For preterm infant choose pouch that is:
• Clear: to allow for inspection of stoma and effluent• Low-birth weight infant with single stoma: smaller
pouch that will not cover the whole abdomen• Larger infant or infant with more than one stoma:
use pouch with larger barrier

Recommendation for Selection• Landmarks on the infant’s abdomen may dictate which
shape will work best Daisy shaped Wafers: fit more easily on umbilicus or adjacent
mucous fistula Custom-trimmed barriers: fit well around abdominal landmarks Separate barrier and pouch: easier to trim Pouched attached to barrier: will have fewer pouching steps in
the process Barrier without starter hole: allows liberal placement that can be
shifted but difficult to cut Barrier with hole: take care to ensure opening is not larger than
stoma
Rogers V., 2003
Recommendation for Selection• The type of appliance and barrier will be influenced
by the placement of the stoma in the bowel no hydrocolloid skin barrier, or with a very thin barrier, although
allowing for conformability to abdominal contours, may not withstand caustic effluent from a proximal ileostomy or jejunostomy,
addition of a supplemental barrier under the pouch barrier may improve wear time
Several pectin-based moldable barriers and caulking strips are able to withstand exposure to corrosive effluent
Karaya is never used as a barrier on a premature infant because it releases acetic acid when it comes in contact with moisture and may burn the skin
Erwin-Toth P, Doughty DB, 1992

Recommendation for Selection
• Use of adhesive on preterm infant skin is discouraged to prevent epidermal stripping and removalMost preemie pouches do not have a tape adhesive
surrounding the pectin barrier. Generally, the pectin will bond with the skin and maintain
an adequate pouch seal. Pouch incorporating a gentle adhesive picture framed
around the wafer may prolong pouch life if the edges of the skin barrier loosen with continued exposure to extrinsic moisture
Erwin-Toth P, Doughty DB, 1992
Recommendation for Selection
• Flexibility is an important consideration when choosing a preterm infant pouch.Two-piece pouching systems, which incorporate firm,
snap-together rings or flanges, should not be used on premature infants.
Pouching systems in which the hydrocolloid barrier is available separate from the pouch but does not include a plastic flange are acceptable.
Erwin-Toth P, Doughty DB, 1992
When choosing an appropriate appliance, however, it is important to consider that NICU nurses may be unfamiliar with ostomy care, and it is important to design the simplest pouching system with the lowest likelihood of complications.
Wilson RE, 1994
Recommendation for Selection• A stoma will decrease in size over
6 to 8 weeks postoperatively and should be re-measured with each appliance change until the size is stabilized.The barrier should fit closely
around the stoma. Erwin-Toth P, Doughty DB, 1992
Lund C, 1984
Recommendation for Selection
• Uneven skin surfaces caused by incisions, skin creases, and other obstacles should be leveled before pouch application. Supplemental patches of moldable barrier or caulking
strips can be used to fill in gaps. Skin barrier pastes used to protect peristomal skin from
effluent and to create a level pouching surface should be avoided because of their alcohol and formaldehyde content (although in quantities small enough to avoid being listed in the ingredients)
A noncommercial, alcohol-free paste can be created by mixing skin barrier powder and glycerin.
Erwin-Toth P, Doughty DB, 1992

A flush or retracted stoma presents challenges in maintaining a pouch seal.
Recommendation for Selection
The addition of a moldable barrier or caulking strip beneath the pouch barrier adds gentle convexity and may improve wear time
An infant’s pouch needs to be able to accommodate a greater amount of gas than that of an adult because of air swallowing that occurs during sucking and crying
Boarini JH, 1989
Recommendation for Selection
Pouches filled with air can quickly compromise the pouch seal.
Some infant pouches come with a built-in charcoal filter, which allows the release of gas without a detectable odor.
Air-filled pouches, as with pouches containing stool, should be emptied frequently to prevent pressure from compromising the seal.
Peristomal skin can be damaged by: epidermal stripping from traumatic pouch removal tunneling of caustic effluent under the barrier sensitivity to ostomy products, or infections such as moniliasis.
Recommendation for Selection
Loss of the epidermis results in “weeping” of serous exudate can decrease adhesion
Treatment of the underlying cause and reevaluation of the pouching system is essential.
• Fungal infections, which can proliferate in the warm, moist environment beneath the barrier and erode the skin, can be treated with nystatin powder applied to the involved areaexcess being gently brushed away before
pouching. the powder can be mixed with water, painted over
the involved area, and allowed to dry before reapplying the pouch
Hagelgans NA, Janusz HB, 1994
Recommendation for Selection

• To ensure dryness of the peristomal skin before pouch application, a skin barrier powder can be applied to weepy areas prior to pouching to absorb moisture and protect the peristomal skin. Skin barrier powders are alcohol free and safe to use
on preterm infant skin. The contribution of inhaled powder to severe
respiratory symptoms and death in infants has been well documented.
Motomatso K, Adachi H, Uno K, 1979
Palraudeau PW, Wilson GR, Hall MA, Milne M, 1991
Recommendation for Selection
Prevent aspiration of aerosolized powder• Only the minimum amount of powder needed to seal the
denuded area of skin should be used, • Excess powder should be gently wiped away rather than
blown away. • The infant’s face should be shielded while applying the
powder. • The bottle opening can be enlarged, allowing powder to easily
be sprinkled without squeezing the bottle and creating a “puff” of powder.
• Alternatively, powder can be applied to a secondary surface, such as a gloved finger or gauze, and dabbed onto the skin
Prevent aspiration of aerosolized powder• If the use of antifungal or skin barrier powders limit
pouch adhesion, they can be “sealed” by patting the powder with a damp finger and allowing the area to dry.
• Any areas continuing to weep should be retreated with barrier powder in like manner until the exudate is contained.
Erwin-Toth P, Doughty DB, 1992
Pooling of liquid effluent• Pouch adhesion may be limited by liquid effluent pooling
around the stoma and degrading the barrier.• Measures should be taken to wick the liquid stool away
from the stoma.
Pouches can be angled to the side rather than toward the feet, allowing the liquid to drain away from the stoma while the infant is in a supine position.
A pouch with a drainage spout can be connected to continuous drainage if the effluent is high volume and liquid.
Gel crystals that absorb liquid several times their weight, can be used in preemie pouches.
Making barrier more adhesive
• After leveling the pouching surface, ensuring that the peristomal skin is completely dry, and applying the pouch, the barrier should be warmed.
• This can be accomplished by placing a hand over the barrier for 1 or 2 minutes after pouch application.
• Warming the barrier allows it to mold to the contours of the infant’s abdomen and increases adhesion of the barrier to the skin, improving wear time.
• Heating the barrier under a radiant warmer is discouraged because the amount of heat absorbed into the wafer is not controllable and an overheated barrier can easily burn fragile skin.
Pouch wear time• Pouch wear time for the preterm infant will not be
comparable with that for an older child or adult.• Factors such as liquid effluent, oily effluent from an
infant receiving enteral supplementation with medium chain triglyceride oil, a humidified environment, and a small pouching surface all decrease barrier adhesion.
• An initial goal for pouch adherence may be 24 hours. However, acceptable wear time may be 12 to 48 hours depending on the condition of the infant and the stoma, the volume of output, and other obstacles to pouch adhesion.
Care of denuded skin• Repeated efforts at repouching, a nonpouching
option for managing the stoma may be used for a short time.
• The peristomal skin must be protected from effluent by an occlusive barrier ointment such as petrolatum or zinc oxide.
• If the skin is denuded and oozing, a skin barrier powder can be applied to denuded areas, followed by liberal application of a protective ointment.
• Alternatively, the powder and ointment can be mixed together and applied to the excoriated skin.
Hagelgans NA, Janusz HB, 19

Key Points
• Although guided by principles that are the same for all patients with an enterostomy, managing the ostomy of a premature infant is not comparable with managing the ostomy of an adult, child or even a full-term infant and must take into consideration the unique characteristics of the preemie.
• Research-based evidence must guide the use of every substance used in caring for the premature infant with a stoma. Products and practices used safely in the adult population may pose a risk to the preemie.
• The simpler the pouching system that will maintain a good seal for 24 to 48 hours, the more reproducible it will be for the multiple caregivers involved in the care of the premature infant with an ostomy.

Thank you for not sleeping!
CCNAPI ConventionFebruary 24-25,2012
Diamond Hotel, Manila
Find us in Facebook!Critical care nurses





























