Embed Size (px)
Citation preview
Radiography (1995) 1, 3547
O R I G I N A L A R T I C L E S
T H L L E G E O F
RA ; I R A P H E R S
OSTEOPOROSIS W H A T IS IT, M E A S U R E D AND W H A T CAN
ABOUT IT? Clare F. Westmacott
H O W IS IT BE DONE
Centre for Bone and Body Composition Research, University of Leeds', Wellcome Wing, Gt George Street, Leeds LS1 3EX, U.K.
"Received 8 February 1995; accepted 31 March 1995)
Osteoporosis is a complex disease affecting one in four women and one in 12 men. Osteoporotic fractures of the wrist, spine and femur have a high cost in morbidity and mortality. There are several causes of osteoporosis, but the most important factor related to osteoporotic fracture in women is due to declining oestrogen levels after the menopause. There is a variety of treatments in use for the treatment of established osteoporosis but hormone replacement therapy is most commonly prescribed for the prevention of osteoporosis. Several techniques are available for the measurement of bone mineral density and are used to establish the patients' bone mineral status and monitor changes which may take place as a result of disease and/or therapy. Accurate prediction of fracture risk using these modalities will only be possible once prospective studies have been completed. Nonetheless prevention of fracture remains the primary target and Department of Health policy is to offer bone density measurements to all women considered to be at risk.
Key words: bone densitometry; treatment; fracture risk; prevention.
I N T R O D U C T I O N
'Thinning of the bones ' and its relationship with fractures in the elderly was first recognized in 1824 by Astley Cooper . As bone began to be studied radiologically, some classification was necessary, and in 1941 Fuller Albright defined osteoporosis as "a condit ion in which there is lack o f bone tissue, but that tissue which remains is normal"[1]. More recently, it has been defined as a reduct ion in bone density per unit volume, which is sufficient to compromise the skeleton so that fracture may occur with min imum t rauma [2]. Others define osteoporosis as a disease characterized by low bone mass and micro-architectural deterioration o f bone tissue, leading to enhanced bone fragility and a consequent increase in fracture risk [3]. However one may choose to categorize it, it is generally accepted today that osteoporosis is a complex disease which raises impor tan t issues. With an increasing and ageing popula t ion osteoporosis is a major social and health problem with a high cost both in morbidi ty and mortal i ty and financially. This is true for all Western populat ions [4].
It is estimated that one in four white British women aged 50 and over will have the condit ion [5]. In N o r t h America f rom the age o f 50 there is estimated to be a 40% risk in women and a 13% risk in men of sustaining a fracture o f the hip, spine or forearm.
1078 8174/95/010035+ 13 $08.00/0 © 1995 The College of Radiographers 35
36 Westmacot t
In Britain approximately 60 000 hip fractures, 50 000 wrist fractures and 40 000 clinically diagnosed vertebral fractures occur annually in post-menopausal women [6]. Patients with hip fracture account for over 20% of all orthopaedic beds. There is 20% increased mortality within 6 months of fracture and 50% of those who survive never regain full independence [7]. The average cost for hospitalization of a patient with a hip fracture is £3000 [8]. While osteoporotic vertebral fractures are not so costly financially (generally speaking they do not require surgery or hospitalization), it is estimated that 30% of women will have had a painful atraumatic fracture by the age of 65 [9]. Where several vertebral fractures occur in an individual the patient becomes stooped, causing crowding of the ribs with consequent impairment of lung function and unremitting pain. The average individual cost of clinically diagnosed vertebral fracture is £300, excluding physiotherapy, drug therapy and community care costs [8]. While wrist fractures are not as serious in their effects they are nevertheless painful and require visits to hospitals and general practitioners. The average cost of treatment is £170 per patient. The total annual cost for all osteoporotic fractures in this country was estimated in 1993 to be £640 million per annum [10].
BONE M A S S
Bone is a specialized tissue in which the collagen matrix becomes mineralized which has both a structural and metabolic function. All bones are made up of two types of tissue, cortical bone and trabecular bone tissue. Bone turnover or remodelling, as far as osteoporosis is concerned is controlled by cells on the surface of bone called osteoblasts and osteoclasts. Osteoblasts are the bone forming cells and are involved in bone mineralization. Osteoclasts are cells which resorb calcified bone by secreting acid in order to demineralize old bone. In the young healthy adult remodelling remains in equilibrium. Osteoporosis is the result of an imbalance in this process, when resorption exceeds formation [11]. Cortical bone forms the outer shell of bones with trabecular bone within. The cortex encloses the narrow struts (trabeculae), which brace the cortical exterior making the bones extremely strong without being too heavy. Although trabecular bone makes up 20% of the skeletal bone mass it provides 66% of the surface area of bone. Bone acts as a calcium reservoir storing greater than 95% of total body calcium [12]. Bones with a high proportion of trabecular structure and therefore a higher surface area of bone include the vertebral bodies, the epiphyses of the long bones, the calcaneum and the iliac crest [11]. Bone density in both cortical and trabecular bone declines with age. Trabecular bone can suffer micro-fractures which heal only slowly and as a result fracture risk increases [12]. In advanced osteoporosis, it is sometimes difficult on a radiograph to distinguish between bones and soft tissue.
The most important aspects when considering the risk of osteoporosis are the level of peak bone mass (usually around the age of 30), and the rate of bone loss [13]. Men have a higher peak bone mass and the reduction in their bone mass is consistent and gradual [14], but in women accelerated bone loss takes place around the menopause and far more women than men sustain osteoporotic fractures, in the 5 years after the menopause the loss is rapid due to declining oestrogen levels but then settles down to a gradual decline as in men [15]. On average women lose between one-third and one-half of their bone mass during their life-time [16].
Not only is peak bone mass of critical importance, the actual rate of bone loss may be of equal importance. One way of assessing the rate of loss is to use biochemical

Osteoporosis 37
markers of bone turnover. The rate of bone matrix formation or resorption can be measured in markers in the blood and in the urine. Markers of bone turnover can be used to assess the pathogenesis of osteoporosis [17]. They tend to be increased in post-menopausal osteoporosis. They may be used to predict bone loss and may also be used to monitor the effect of therapy. Alkaline phosphatase is one of the most commonly used markers of bone formation and is located primarily in the osteoblasts. Osteocalcin and procollagen peptide are proteins found in bone and are also markers of bone formation. Pyridinoline is one of the markers for bone resorption [18] which is cleared by the kidneys during collagen breakdown. Although current data suggests that markers of bone turnover may predict bone loss it is not yet clear whether this enables them to predict fracture.
RISK FACTORS
Although peak bone mass may initially be determined genetically there are many risk factors associated with the onset of osteoporosis. Some of them prevent the attainment of high bone mass. Others accelerate bone resorption and reduce bone formation, which can be caused by medical and surgical intervention, poor diet, certain diseases, inactivity and old age in both men and women. Hyperparathyroidism, renal disease, thyroid disease and diabetes are some of the conditions considered to be risk factors for osteoporosis, because they interfere with calcium metabolism [19]. With increasing survival after organ transplant osteoporosis is now regarded as a significant complica- tion following transplant surgery. Many of these patients have low bone mass before surgery, due to immobility and the metabolic effects of their condition. After transplan- tation, further bone loss occurs and after liver transplantation 65% of patients have been shown to suffer atraumatic vertebral fracture. This is probably due to treatment with steroids and cyclosporin and long-term studies show that the rate of bone loss reduces as the anti-rejection drugs dose is reduced [20]. Alcohol, which in addition to contributing to falls is also associated with malabsorption of calcium, with increased resorption and decreased bone mass as a result [21]. Chronic alcohol abuse is an important risk factor, particularly in men and in pre-menopausal women.
The precise role of calcium in the diet is not yet clear. Several studies have shown that a life long high calcium intake is associated with a higher bone mass and lower fracture incidence [22]. However there is no evidence yet that calcium by itself will afford protection against oestrogen-dependent bone loss [23].
Smoking may inhibit the growth of osteoblasts and is believed to interfere with the function of oestrogen. Certainly female smokers are thinner and have an earlier menopause [21]. Physical inactivity has been shown to reduce bone mass. indeed, studies on astronauts have shown that weightlessness in space had an adverse effect on bone mineral density (BMD) [24]. Prolonged bed rest has the same effect and localized osteoporosis can occur when a limb is immobilized for any length of time. Certain drug therapies can lead to secondary osteoporosis. In 1932 Cushing recognized osteoporosis in his patients, who had excess endogeneous glucocorticoid. Depending on dose and duration of treatment corticosteroid treatment leads to loss of bone mass as in cystic fibrosis and asthma. Hypogonadism in both males and females is associated with osteoporosis. For example in males with Klinefelter's syndrome treatment is with testosterone. In Turner's syndrome there is a reduction in both cortical and trabecula

38 W e s t m a c o t t
bone. The cause is thought to be more than simple oestrogen deficiency as it can also affect children [21].
Simple oestrogen deficiency can occur for a variety of reasons--for example anorexia nervosa causes amenorrhoea, which leads in turn to oestrogen deficiency, and ulti- mately to low bone mass. Similarly, excessive exercise has the same end point, starting with amenorrhoea [21], and bilateral oopherectomy has the same effect. However the largest group of sufferers is made up of post-menopausal women, whose declining oestrogen levels around the menopause are a major cause of bone loss and ultimately fracture.
When one looks at studies of the prevalence of osteoporotic fractures of the neck of femur for example, one can see wide variation between different racial groups. White women have a much higher incidence of osteoporotic-induced fractures than black, or other non-white groups. In an American study in 1984, white women were at twice the risk of sustaining an osteoporotic hip fracture compared with black women of the same age and another study in 1985 confirmed this finding, and also found that obese white women were less at risk than non-obese white women. This was true for both pre- and post-menopausal women [25].
M E A S U R E M E N T OF BONE
Histology of bone, from a bone biopsy taken from the iliac crest, is an accurate method of measuring bone mineral content (BMC) and the distribution of the trabeculae. It is however both costly and painful and so its use has been restricted largely to diagnosis in individual cases. Because it is a painful technique it was only when other less invasive methods became available that research into the cause of the disease and the ability to monitor its therapy became possible. As a result of these advances it was hoped that techniques would be developed that could predict those at risk of an osteoporotic fracture, particularly post-menopausal women. If a predictive method could be shown to be sufficiently accurate then patients at risk could be treated prophylactically without wasting resources on those not at risk.
Methods of measuring BMC have been evolving since radiographs were used in the 1920s. This was done by making morphometric measurements of the vertebrae, hands, and neck of femur to assess the degree of bone loss [26]. Singh grading was a technique developed to assess the changes in the distribution of the trabeculae in the proximal femur as a means of identifying the degree of osteoporosis in a patient. Radiographs of the hip were used to grade the degree of loss of the trabeculae and consequent loss of load bearing ability [27]. The first method of using a scanning densitometer was reported in S c i e n c e in 1939 [28]. In the early 1960s single photon absorptiometry of the forearm was first used to assess skeletal status [29]. The development of dual photon absorptiometry (DPA) [30] and subsequently dual energy X-ray absorptiometry (DXA) enabled the most important fracture sites to be measured directly. DPA and DXA scanners can measure the BMC in grammes or the area normalized BMC, the BMD, in grammes per square centimetre. The radiation dose is extremely small. DXA scan times are 10 and 6 min for the spine and femur respectively (Figs 1 and 2).
DXA uses, as its name suggests, two X-ray energies which are absorbed differentially by bone and tissue. However when one looks at the BMD distribution in populations with and without osteoporotic fractures there is considerable overlap [31]. Although BMD may be regarded as a measure of osteoporosis, it is clear that there are other

Osteoporosis 39
Figure 1. DXA scanner, for a lumbar spine scan the patient lies supine, legs supported as shown in order to maximize the spine to table contact. A rectilinear scan pattern is followed until the required number of vertebrae have been acquired. Photograph courtesy of AuRa Scientific.
factors to be considered when attempting to make a prediction of fracture risk. Nevertheless DXA is today the optimum method of monitoring treatment which it does with great precision. Many clinical trials into the effects of therapy on bone density use DXA to quantify change in BMD and often these are multi-centre studies.
As the changes in BMD may be quite small it is vital that reliable quality control and quality assurance are carried out in order to achieve maximum precision and accuracy. All manufacturers provide a 'phantom' with each instrument which should be used to assess daily any drift in instrument calibration. As each 'phantom' is unique it is recommended in multi-centre trials that a 'travelling phantom' is measured at all sites from time to time in order to correlate the pooled data [32]. A semi- anthropomorphic phantom has been developed under the auspices of the European Community in order to assess inter-centre and inter-machine variation. The European spine phantom (ESP) contains vertebral-shaped inserts with differing BMD values and it is currently in use in multi-centre studies as a means of optimizing precision and accuracy (Fig. 3).
A new generation of DXA scanners is now becoming available. Instead of single detector pencil-beam geometry the new systems use fan-beam geometry and multi- detector arrays. The focal spot size has been reduced as a result of which images of almost radiographic quality can be achieved. Also the use of fan-beam geometry reduces acquisition time to a matter of seconds. The new systems offer improvements in resolution, noise and contrast, however, at the cost of an increase in dose. A single lateral spine scan from the fifth thoracic vertebra (T5) to the fifth lumbar vertebra (L5) can be acquired in seconds and used both for morphometry and densitometry. Similarly high resolution scans of the femural neck can be acquired (Figs 4 and 5).
40 Westmacot t
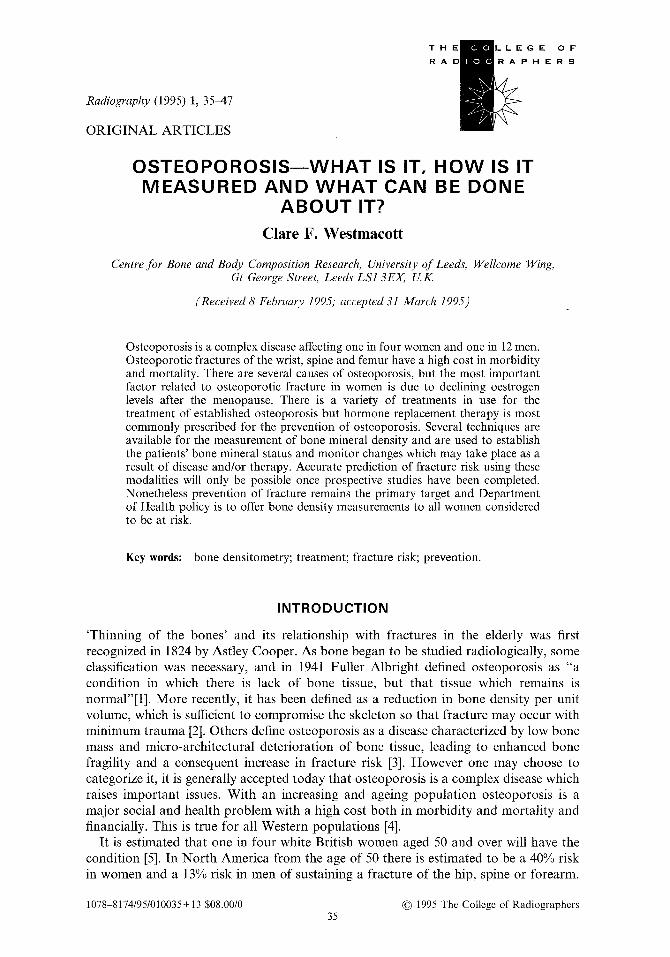
Figure 2. DXA hip scan. Three sites are measured; the neck of femur, Ward's triangle and the greater trochanter. In this case the neck of femur result is displayed in the graph on the right hand side of the photograph. The horizontal band demonstrates the normal range of values for the neck of femur, and the asterisk represents the position with regard to the normal range, of the values of this particular patient. Photograph courtesy of AuRa Scientific.
Quantitative computed tomography is another method in limited use for measuring BMD. Many of the advanced computer tomography scanners can be adapted for the quantitative measurement of vertebral bone mineral. The patient is scanned together with a reference phantom made up of varying concentrations of potassium hypophos- phate. A 'scout' view is used to locate the position of the vertebrae and a measurement is made from a slice from the centre of two to four lumbar vertebral bodies ensuring that the slice taken is parallel with the endplates of each vertebra. It is possible using this method to measure the trabecular structure alone by placing a region of interest over the anterior part of the vertebral body avoiding its cortical margin. However the equipment is more costly than DXA and the radiation dose higher, as a result most studies have been done using DXA.
The relationship between bone density and bone strength is complex, but DXA does not measure the strength of bone even though 60% of bone strength is attributed to density [25] and ultrasonic bone measurement is another more recent development
Osteoporosis 41
Figure 3. European spine phantom, this phantom contains vertebral shaped inserts with differing BMD values and is used in multi-centre studies to maximize precision and accuracy. Photograph courtesy of B. Lees.
which may go some way towards unravelling the complexity of this relationship. Currently this is the only method which is both non-invasive and free from ionizing radiation. All of the methods using ionizing radiation produce a measurement of the attenuation of the energy beam passing through bone and soft tissue, but they are not able to provide information regarding the biomechanical status of bone. Because the sound can be modified by the bone's structure and composition, ultrasound has the potential to provide information on both elasticity and structure in bone, a combination of which may improve the prediction of fracture risk.
The method of using ultrasound to measure bone uses two transducers, one transmitting and one receiving and is known as the transmission method. The sound wave passes through the bone to the receiver and the acoustic properties of the bone are obtained by comparing the received signal with a standard waveform. The bone is interrogated at several frequencies and the slope of the graph of sound attenuation vs
frequency, the broadband ultrasonic attenuation (BUA), provides a measure of bone architecture. In addition the speed of sound can be measured which is related to bone density. The calcaneum is usually measured as access is easy and it is high in trabecular content (Fig. 6). Precision of BUA measurements in most studies is of the order of 1.7%. Researchers are also looking at other sites, mainly the tibia. The use of ultrasound in the frequency range of 200-600 kHz has demonstrated considerable differences between normal and osteoporotic bone. Although the correlation with BMD as measured by DXA may not be high, studies using ultrasound with respect to fracture discrimination have had positive results [33]. Therefore ultrasound may have properties relevant to bone strength which are at least of equal importance to BMD when considering fracture risk (Table 1).

42 Westmacott
Figure 4. High resolution DXA spine scan, both densitometry and morphometry can be undertaken using the latest systems to become available. Photograph courtesy of Lunar Corporation.
T R E A T M E N T OF OSTEOPOROSIS
There are several therapies available for the treatment of established osteoporosis. Large doses o f calcium may reduce the rate of bone loss in women with established osteoporosis. This works by suppressing the secretion of parathyroid hormone, thereby decreasing bone resorption [34]. The estimated average requirement in this country per person per day is 600 mg [23]. Most experts stress the importance of calcium throughout life to help to keep the bone mass at its maximum level, but it will not put back bone that is lost [34].
Vitamin D is important in the regulation of calcium metabolism, and deficiency results in rickets in children and osteomalacia in adults. It is vital for the absorption of calcium [34]. Studies have produced conflicting evidence as to the benefit of vitamin D treatment on its own but there is evidence that vitamin D3 with calcium does increase bone mass i n the femur and reduces fracture rates: This is increasingly used in the treatment of elderly women [35].
Calcitonin is a peptide hormone which inhibits bone resorption by a direct action on the activity of osteoclasts. Calcitonin receptors are abundant on the surface of osteoclasts. Calcitonin levels are higher in men than in women and the difference increases with age. Nasally administered calcitonin is being used and has produced encouraging results although there are as yet no long term data on its ability to prevent fracture. Salmon calcitonin is used most frequently in these studies [36]. Studies show that certain anabolic steroids may reduce bone loss in patients with osteoporosis, probably by acting on androgen receptors in bone.
Sodium fluoride or monofluorophosphates have been widely used, especially in Europe for the treatment of established osteoporosis. It increases the number of

Osteoporosis 43
Figure 5. High resolution hip scan result. Photograph courtesy of Lunar Corporation.
osteoblasts, and thereby increases the rate of bone formation, particularly in the vertebral body. It is less effective in the neck of the femur [36]. Generally where fluoride is prescribed today, it is given in conjunction with vitamin D and calcium [34].
Bisphosphonates have been developed over the last 20 years for use in various diseases of calcium metabolism. They act to inhibit bone resorption by reducing the osteoclast activity and unlike other inhibitors of bone resorption, the pharmacological effects can last a long time after the end of treatment. Patients receive bisphosphonate followed by calcium on a cyclical basis. Significant increases in the BMC of the spine, and a reduction in the incidence of vertebral fractures have been demonstrated. The bone thus formed is histologically normal and there are generally no significant side effects [37].
These treatments are all in use for established osteoporosis but it is widely accepted that hormone replacement therapy (HRT) is currently the most effective treatment for preventing osteoporosis in post-menopausal women. During the reproductive years of a woman's life, 90% of oestrogens are synthesized in the ovary, and oestradiol is the main circulating oestrogen. Around the menopause as the ovaries become smaller the oestradiol levels fall. The first oestrogen was isolated and purified in 1923, from then the development and use of orally active synthetic and semi-synthetic oestrogens took place, and in the 1950s studies showed that long-term H R T reduced loss of height in post-menopausal women [38]. It has been shown that adequate levels of HRT will prevent bone loss for as long as the patient takes it. There may even be a limited increase in bone mass. However bone loss recurs as soon as therapy stops [39]. In the main these studies have been carried out on younger post-menopausal women. It is not possible yet to say with certainty, that a woman who takes H R T for 5 to 10 years from the age of 50, will not fracture 15 to 20 years after she has stopped taking HRT.

44 Westrnacott
Figure 6. Patient undergoing an ultrasound scan of the calcaneum. The calcaneum is placed in position between the transducers and speed of sound and broadbank ultrasonic attenuation are measured.
DISCUSSION
There is no doubt that osteoporosis is highly prevalent and incurs a high social and financial cost. As the population of elderly people increases the effects of osteoporosis will place an increasing burden on society. Although the therapies available for the treatment of established osteoporosis are becoming increasingly effective, as far as post-menopausal osteoporosis is concerned prevention remains the primary goal. Current published data suggests that low femoral neck BMD is the best predictor of hip fracture and that although the reduction in BMD with age does not totally correlate with fracture incidence, nevertheless preventative measures should be primarily aimed at those patients with the lowest hip BMD [40]. In February 1995 the Parliamentary Secretary at the Department of Health announced that national guidelines for the diagnosis and treatment of osteoporosis would be drawn up with greater emphasis being put on prevention. All health authorities and general practitioner fundholders would be encouraged to make provision for high-risk patients to have access to the assessment of their bone density status and be offered treatment accordingly. Methods of detection are becoming increasingly sophisticated as technology advances. Research continues into the genetic analysis of osteoporosis with a view to identifying a means of predicting bone density values and ultimately intervening in patients at high risk.
Osteoporosis 45
Nevertheless there is as yet no accurate means o f predicting fracture risk. Research into methods o f identifying and treating patients continues but until long-term studies have been carried out the full effect on fracture rates will not be known.
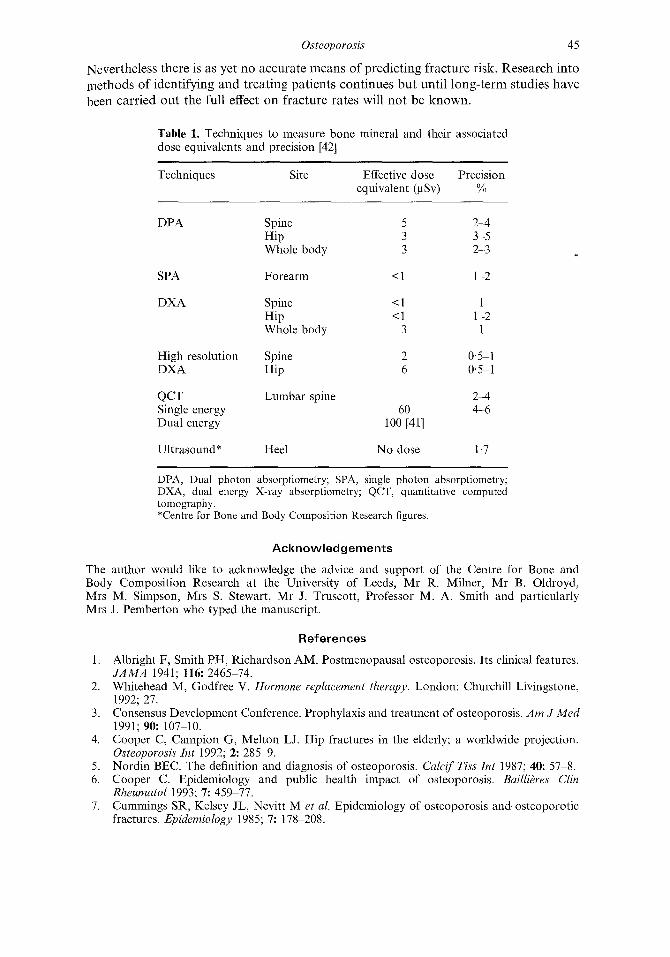
Table 1. Techniques to measure bone mineral and their associated dose equivalents and precision [42]
Techniques Site Effective dose Precision equivalent (gSv) %
DPA Spine 5 2-4 Hip 3 3-5 Whole body 3 2-3
SPA Forearm < 1 1-2
DXA Spine < 1 1 Hip < 1 1-2 Whole body 3 1
High resolution Spine 2 0"5 1 DXA Hip 6 0" 5-1
QCT Lumbar spine 2-4 Single energy 60 4-6 Dual energy 100 [41]
Ultrasound* Heel No dose 1,7
DPA, Dual photon absorptiometry; SPA, single photon absorptiometry; DXA, dual energy X-ray absorptiometry; QCT, quantitative computed tomography. *Centre for Bone and Body Composition Research figures.
Acknowledgements
The author would like to acknowledge the advice and support of the Centre for Bone and Body Composition Research at the University of Leeds, Mr R. Milner, Mr B. Oldroyd, Mrs M. Simpson, Mrs S. Stewart, Mr J. Truscott, Professor M. A. Smith and particularly Mrs J. Pemberton who typed the manuscript.
References
1. Albright F, Smith PH, Richardson AM. Postmenopausal osteoporosis. Its clinical features. JAMA 1941; 116: 2465-74.
2. Whitehead M, Godfree V. Hormone replacement therapy. London: Churchill Livingstone, 1992; 27.
3. Consensus Development Conference. Prophylaxis and treatment of osteoporosis. Am J Med 1991; 90:107 10.
4. Cooper C, Campion G, Melton LJ. Hip fractures in the elderly; a worldwide projection. Osteoporosis Int 1992; 2:285 9.
5. Nordin BEC. The definition and diagnosis of osteoporosis. Calcif Tiss Int 1987; 40: 57-8. 6. Cooper C. Epidemiology and public health impact of osteoporosis. BailliOres Clin
Rheumatol 1993; 7:459 77. 7. Cummings SR, Kelsey JL, Nevitt M e t al. Epidemiology of osteoporosis and osteoporotic
fractures. Epidemiology 1985; 7:178 208.

46
8.
9.
Westmacott
National Osteoporosis Society Scientific Advisory Committee. Priorities for prevention. Bath: National Osteoporosis Society, 1994: 5. Cooper C, Atkinson EJ, O'Fallon WM et al. The incidence of clinically diagnosed vertebral fractures: a population based study in Rochester, Minnesota 1985-1989. J Bone Miner Res 1992; 7:221 7.
10. National Osteoporosis Society Scientific Advisory Committee. Priorities' .for prevention. Bath: National Osteoporosis Society, 1994: 5.
11. Parfitt AM. Bone remodelling. In: Osteoporosis etiology, diagnosis and management, Riggs BL, Melton LJ, eds. New York: Raven Press, d988:45 93.
12. WoolfAD, Dixon AStJ. In: Osteoporosis: A clinicalguide. London: Martin Dunitz, 1988: 12. 13. Rodin A, Murby B, Smith MA, et al. Premenopausal bone loss in the lumbar spine and neck
of femur: a study of 225 Caucasian women. Bone 1990; 211: 1-5. 14. Riggs BL, Melton LJ. Medical progress: involutional osteoporosis. N Engl J Med 1986; 314:
1676-86. 15. Truscott JG, Oldroyd B, Simpson M et al. Variation in lumbar spine and femoral neck bone
mineral measured by dual energy X-ray absorption: a study of 329 normal women. Br J Radiol 1993; 66:514 21.
16. Melton LJ, Chao EYS, Lane J. Biomechanical aspects of fractures. In: Osteoporosis." etiology diagnosis and management Riggs BL, Melton L J, eds. New York: Raven Press, 1988:111 31.
17. Eastell R, Robins SP, Colwell A et al. Evaluation of bone turnover in type 1 osteoporosis using biochemical markers specific for both bone formation and bone resorption. Osteoporosis lnt 1993; 3:255 60.
18. Eastell R. Biochemical markers of bone remodelling in osteoporosis. In: Current research in osteoporosis and bone mineral measurement, III. London: BIR, 1994: 7.
19. Melton LJ, Riggs BL. Clinical spectrum. In: Osteoporosis." etiology, diagnosis' and manage- ment, Riggs BL, Melton LJ, eds. New York: Raven Press, 1988:155 79.
20. Francis RM, Anderson FH. Osteoporosis and organ transplantation. In: Current research in osteoporosis and bone mineral measurement, III. London: BIR, 1994: 106.
21. Lindsay R. Sex steroids in the pathogenesis and prevention of osteoporosis. In: Osteo- porosis: etiology, diagnosis and management, Riggs BL, Melton LJ, eds. New York: Raven Press, 1988: 333-59.
22. Matkovik V, Kestial K, Simonovik Ie t al. Bone status and fracture rates in two regions of Yugoslavia. Am J Clin Nut 1979; 32: 540-9.
23. Department of Health Report on Health and Social Subjects. Dietary reference values Jor food energy and nutrients for the United Kingdom. London: HMSO, 1991: 137.
24. Mack PB, Vogt EB. Roentgenographic bone density changes in astronauts during representative Apollo space flights. A JR 1971; 113: 621-3.
25. Smith MA, Drife JO. Hormone replacement therapy and breast cancer risk. In: Osteo- porosis: prevalence, prediction and prevention, Mann RD, ed. Carnforth: Parthenon, 1992: 117-27.
26. Bentley B. Modern radiological methods of bone dens i tomet r~a survey. Radiography 1967; 33: 155-62.
27. Singh M, Nagrutu AR, Maini PS. Changes in trabecular patterns of the upper end of the femur as an index of osteoporosis. J Bone Joint Surg 1970; 52A: 457 67.
28. Mack PB, Vogt FB. A method for estimating the degree of mineralisation of bones from tracings of roentgenograms. Science 1939; 89: 467.
29. Cameron JR, Sorenson J. Measurement of bone mineral in vivo; an improved method. Science 1963; 142: 2304.
30. Reed CW. Measurement of bone mineralisation from the relative transmission of 241 Am and 137 Cs radiation. Phys Med Biol 1966; I1: 174.
31. Law MR, Wald N J, Meade TW. Strategies for prevention of osteoporosis and hip fracture. BMJ 1991; 303: 453-9.
32. Miller CG. Bone density measurements in clinical trials: the challenge of ensuring optimal data. Br J Clin Res 1993; 4: 113--20.
33. Gluer CC, Genant HK. Quantitative ultrasound accomplishments and challenges. In: Proceedings" of Ultrasound Assessment of Bone. AEA, 1994: 3846.

Osteoporosis 47
34. Christiansen C, Riis BJ. Post menopausal osteoporosis. A handbook Jor the medical proJ~'ssion. Aalborg: Handelstrykkeriet, 1990: 66-75.
35. Chapuy MC, Arlot M, Duboeuf F et al. Vitamin D3 and calcium to prevent hip fractures in elderly women. N Engl Y Med 1992; 327: 163742.
36. Woolf AD, Dixon AStJ. Osteoporosis: A clinical guide. London: Martin Dunitz, 1988: 181-95.
37. Watts NB, Harris ST, Genant HK et al. Intermittent cyclical etidronate treatment of postmenopausal osteoporosis. N Engl J Med 1990; 323: 73-9.
38. Woolf AD, Dixon AStJ. Osteoporosis: a clinical guide. London: Martin Dunitz, 1988: 168-80.
39. Christiansen C, Christiansen MS, Transbel I. Bone mass in postmenopausal women after withdrawal of oestrogen/gestagen replacement therapy. Lancet 1981; i: 459-61.
40. Cummings SR, Black DM, Nevitt MC et al. Bone density at various sites for prediction of hip fractures. Lancet 1993; 341: 72-5.
41. Kalendar WA. Effective dose values in bone mineral measurements by photon absorpti~ ometry and computed tomography. Osteoporosis Int 1992; 2: 8~7.
42. Banks LM. Dual energy X-ray absorptiometry. In: Diagnostic radiology, 3rd edn. Grainger RG, Allison D J, eds. London: Churchill Livingstone, in press.





























