Embed Size (px)
Citation preview

1
Title of presentationTitle of presentation
Organ and Tissue Donation in Victoria
Presentation to the Legal and Social Issues Standing Committee 8-9-2011
Dr Helen Opdam
Victorian Medical Director of Organ and Tissue Donation
Intensive Care Specialist,Austin Hospital
2
Overview
Donation in Australia and Victoria – the scene in 2011 Factors limiting organ donation? Specific challenges in Victoria? Is it possible to increase organ donation and how? Victorian success to date – the reasons Next steps and future challenges

3
Organ donation in Australia and Victoria
– the scene in 2011

4
The SituationAustralia has had a relatively low donation rate by international standards
Australia is a world leader in successful transplantation outcomes
Our organ and tissue donation rates were static for many years

5
International Donor Statistics 2006
Donors PMP
Source: IRODaT (International Registry of Organ Donation and Transplantation)
33.8
26.9 26.423.2 21.7 20.7 20.1
16.3 15.3 15.1 14.1 13.0 11.4 10.5 9.87.2 6.0
18.8 17.7
Spain
USABelg
iumFran
ce Italy
Finland
Irelan
dCze
ch R
epHun
garyNor
wayGerm
any
Sweden
Canad
aPola
ndDen
mark UKAus
tralia
Greece NZ

6
30.425.6 23.4 21.7 19.6
15.9 15.1 13.8 13.7 13.3 13.0 12.69.7 9.4
13.914.8
PortugalUSA
Austria
Italy
Czech
Rep
German
y UKLatv
iaHungaryAustr
alia
Canad
aPolan
dNeth
erlan
dsSwitz
erlan
dIre
land NZ
International Donor Statistics 2010
Donors PMP
© ANZOD Registry
Source: IRODaT (International Registry of Organ Donation and Transplantation)

7
889668740736 860
991
204 202 198 259 247 309
16901757
1625 1650 15991716
0
500
1000
1500
2000
2500
3000
05 06 07 08 09 100
500
1000
1500
2000
2500
3000Deceased DonorsTransplantsWaiting List
2005 2006 2007 2008 2009 2010
Number of Deceased Donors Solid Organ Transplantsand Patients on the Waiting List 2005 - 2010
Australia
© ANZOD Registry
8
Before transplantation
After transplantation
9
Before transplantation
Australia has excellent transplantation outcomes!
5-year survival ratesLiver transplant - 85%
Heart transplant - 77%

10
Australia – Cumulative Donors

11
12
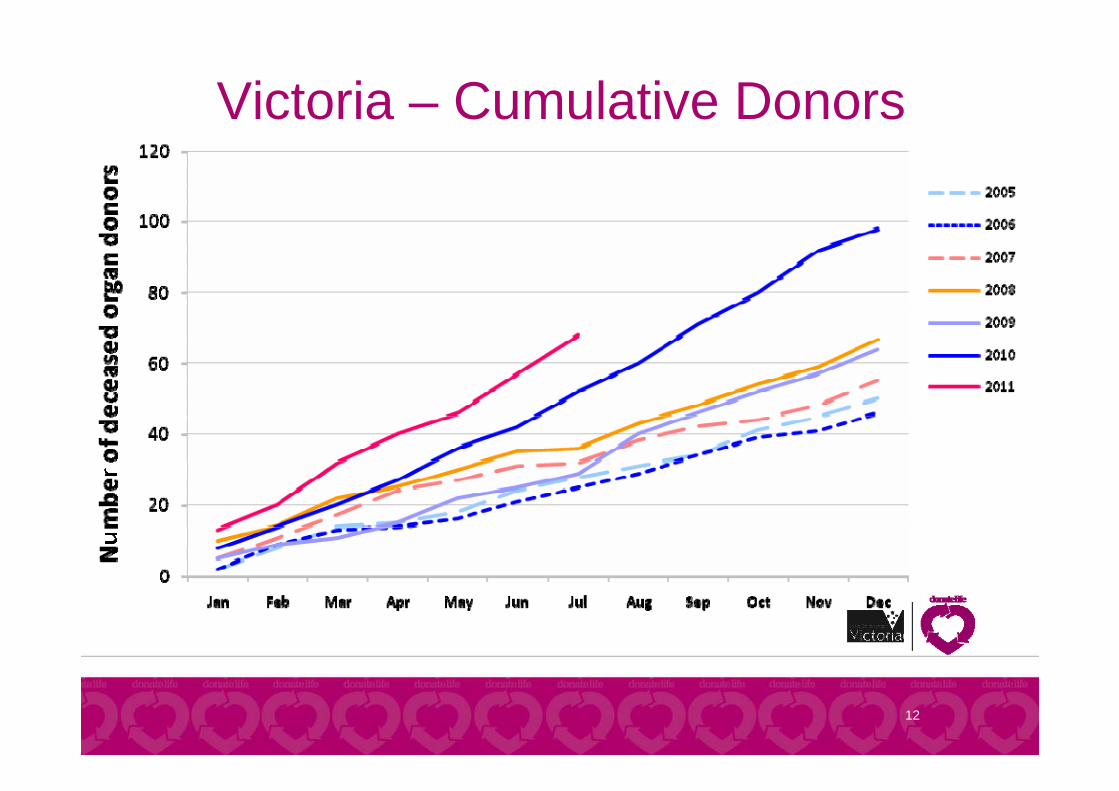
Victoria – Cumulative Donors
13
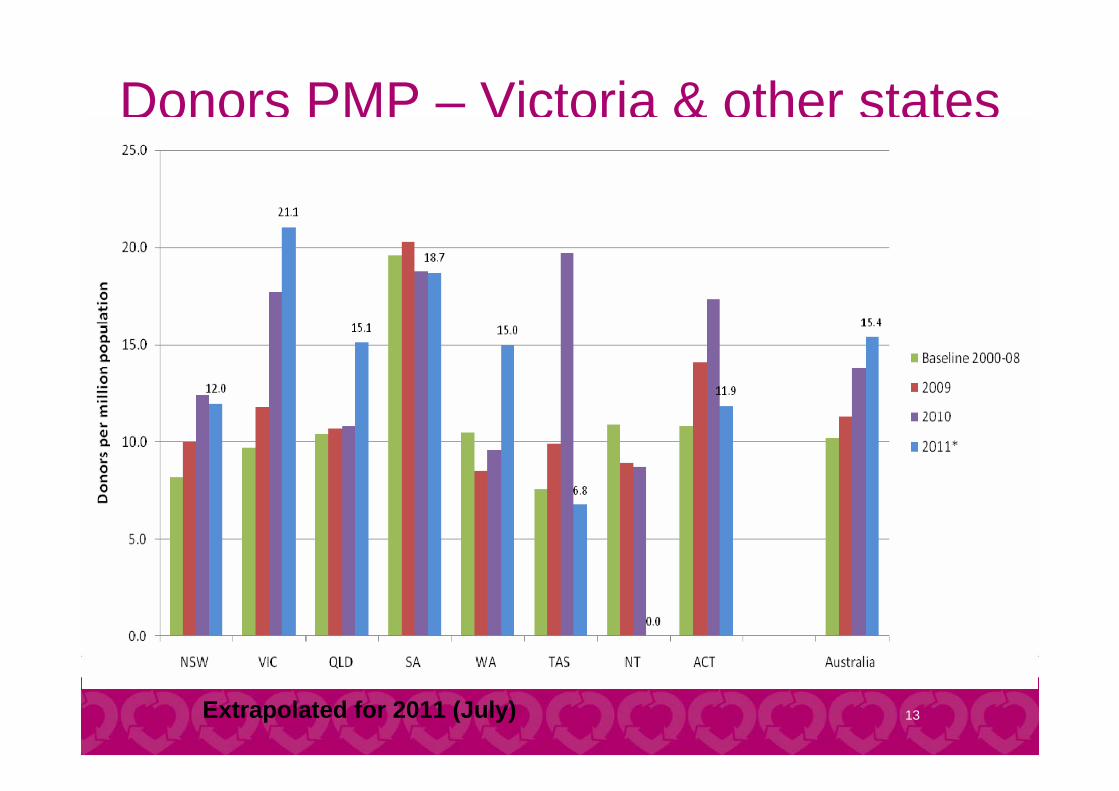
Donors PMP – Victoria & other states
Extrapolated for 2011 (July)

14
BD & DCD – Australia Cumulative Donors
Extrapolated for 2011 (July)

15
Factors limiting organ donation
16
The opportunity for organ donation occurs infrequently
A person has to die in specific circumstances for organ donation to be possible
Only 1 - 2% of people who die in hospital can donate organs
Who can be an organ donor?

17
No evidence of: Cancer Untreated major infection Other transmissible infectious diseases
(HIV etc.) Diseases making organs unsuitable
Intubated on a mechanical ventilator in theICU or the ED
Brain death or suitable for DCD
Who can be an organ donor?

18
... a person has died when there has occurred
a) Irreversible cessation of all function of the brain of the person, or
b) Irreversible cessation of circulation of blood in the body of the person
Definition of death:Human Tissue Act, 1982

19
1) Brain death (most common) loss of all brain function (death of the brain) due to
trauma, bleed, anoxia etc. diagnosed by clinical examination or scan showing no
blood flow to the brain
Pathways to donation
Normal flow No flow No flow

20
2) Donation after cardiac death (increasing)
death likely to occur soon (within 60 – 90 minutes) of withdrawal of treatment in the ICU
family can be with patient until just after death, patient then needs to be moved rapidly to operating theatre for donation surgery
fewer organs suitable for donation
Pathways to donation

21
The Situation for familiesUsually an unexpected and tragic event for a family
Families may have difficulty accepting the poor prognosis and inevitable death, the need to withdrawal treatment and/or the brain death diagnosis
Families may not know what their relative’s wishes were regarding organ donation
Donation may mean the end-of-life care process for a family may be extended by another 12 to 24 hours or more

22
Specific challenges in Victoria

23
Some Victorian challenges?
Resources / Low intensive care bed numbers
Cultural diversity
Population spread

24
Low intensive care bed numbers
CCR: Intensive Care Resources & Activity: Australia & New Zealand 2006/2007
State WA VIC NSW QLD SA
Ventilator beds/100000
4.65 5.8 6.07 6.58 8.39

25
Cultural diversity - Victoria
6.5%of Victorians are indigenous
24%were born overseas
44%have at least one parent born overseas
20%speak a language other than English at home
200 languages and dialects spoken
130religions and faiths2006 Census data
26
Victorian population ~5.4 million 3/4 in metropolitan Melbourne 1/10 in eight other urban areas
(Geelong, Ballarat, Bendigo, Shepparton, Melton, Warrnambool, Albury-Wodonga, Mildura)
The rest in towns of fewer than 20,000 or in rural areas
Population spread

27
2011 ANZOD data: www.anzdata.org.au/anzod

28
2011 ANZOD data: www.anzdata.org.au/anzod

29
Is it possible to increase organ donation and how?
30
Increasing the donation rate
Possible by: 1) Expanding the donor pool
2) Identifying all potential organ donors in hospitals and ensuring that the option of organ donation is raised with family
3) Higher consent rates

31
Increasing the donation rate
Possible by: 1) Expanding the donor pool
2) Identifying all potential organ donors in hospitals and ensuring that the option of organ donation is raised with family
3) Higher consent rates

32
1) Expanding the donor pool

33
1) Expanding the donor pool
Broadening medical suitability criteria (marginal and higher risk donors)
Donation after cardiac death (DCD)

34
Broadening suitability criteria Suitability criteria becoming more permissive
Also depends on recipient characteristics (e.g. transplant urgency)
Risk of transplantation versus ….risk of not receiving a transplant
Note: Hepatitis B or C, history of IV drug use or cured malignancy are NOT contraindications
Refer ALL potential donors to the Victorian Organ Donation Agency for assessment

35
Age limitsLungs 2 – 65yrs
Kidneys 1 – 75 (80)yrs
Liver 1 – 75 (80)yrs
Pancreas 10 – 50yrs
Heart 2 – 60yrs
Intestine < 55yrs

36
Age limitsLungs 2 – 65yrs
Kidneys 1 – 75 (80)yrs
Liver 1 – 75 (80)yrs
Pancreas 10 – 50yrs
Heart 2 – 60yrs
Intestine < 55yrs
75

37
BD & DCD – Australia Cumulative Donors
Extrapolated for 2011 (July)

38
DCD - Victoria & other States
July 2011

39
Victorian DCD Hospitals
July 2011

40
Increasing the donation rate
Possible by: 1) Expanding the donor pool
2) Identifying all potential organ donors in hospitals and ensuring that the option of organ donation is raised with family
3) Higher consent rates

41
2) Identification and request

42
2) Identification and request Identifying all potential organ donors in
hospitals
Ensuring that the option of organ donation is raised appropriately with family
43
Measure the potential for organ donation
Determine rates of consent, request
Identify missed donation opportunities – where and why they occur
Use this information locally and nationally Assess performance, identify barriers to donation,
implement change
Purposes of hospital death audit

44
Death audits* - Outcome Over 90000 deaths reviewed 1 in 5 potential organ donors – not identified and/or
organ donation not requested‒ Few missed donors with confirmed brain death‒ Modest number of patients in whom brain death may
have been present but not confirmed‒ Largest group were those with imminent brain death
who have treatment withdrawn
* Victorian death audit 2002-2008 &National Organ Donation Collaborative 2006-2009

45
69 yo with intracranial haemorrhage Past health history:
Irregular heart rhythm - on warfarin, high blood pressure
Tuesday 7pm: Headache, slurred speech. Ambulance – poorly conscious (GCS 4), intubated.
8.26pm: Emergency department – Right pupil enlarged and not constricting to light, sedation started
9pm: Both pupils now dilated and not constricting to light
CT brain: Multiple regions of haemorrhage with extension into ventricular system and marked cerebral oedema

46
……….. continued Neurosurgical review – surgery will not help, will die. Poor
prognosis conveyed to family 10.45pm: Family spoke to GP who explained in their language the
patient’s condition 11.30pm: Entire family present. Patient extubated, breathing
but irregular and poor effort 11.52pm: Patient has no respiration or palpable pulse. Priest
giving last rites.
(May have been a suitable kidney / liver donor)

47
Call ICU registrar or consultant for assessment regarding the potential for organ and tissue donation – (contact details)

48
Increasing the donation rate
Possible by: 1) Expanding the donor pool
2) Identifying all potential organ donors in hospitals and ensuring that the option of organ donation is raised with family
3) Higher consent rates

49
3) Increasing consent

50
3) Increasing consent Consent rate ~ 57% (Australian audits*)
Consent rate lower than that expected from public surveys
Consent rate lower if family discussion held by a junior rather than a senior doctor*
Consent rate higher if request made by someone knowledgeable about and supportive of organ donation
* Victorian death audit 2002-2008 &National Organ Donation Collaborative 2006-2009

51
Community and consent90% of Australians support organ and tissue donation
30% of Australians don't discuss their donation wishes with their family
Some families don’t give consent because they do not know the wishes of their loved one
Families rarely overrule a person's wishes if they know what they are

52
What can we do?
Public awareness and education
Ensuring that the organ donation discussion with families in hospitals is managed by informed and trained individuals

53

54
55

56
Victoria’s success to date – the reasons

57
Victoria’s success
National funding and implementation of the reform
Victoria’s prior participation in the National Organ Donation Collaborative (2006 – 2009, 7 hospitals)
Victorian audit of deaths to identify barriers to donation (pilot 1998/99, ongoing since 2002)
Strategy focused on the three areas where it is possible to increase donation (donor identification and request, consent, expanding the donor pool)
58
Victoria’s success
New hospital staff – fractionalised FTE
Other initiatives such as the Volunteer program

59
New hospital-based staff

60
Victorian Hospital-based staff
Medical Hospital Nursing
1.0 Alfred Hospital 1.5
1.0 Royal Melbourne Hospital 1.5
1.0 Austin Hospital 1.5
0.8 Monash Medical Centre 1.2
0.8 St Vincent's Hospital 0.8
0.5 Box Hill Hospital 0.5
0.5 Dandenong Hospital 0.5
0.5 Frankston Hospital 0.5
0.5 Geelong Hospital 0.5
0.3 Northern Hospital 0.8
0.5 Royal Children's Hospital 0.5
0.3 Western Hospital 0.8
Maroondah Hospital 0.5
Albury/Wodonga Health 0.5
Ballarat Hospital 0.5
Bendigo Hospital 0.5
Epworth Private Hospital 0.5
Latrobe Regional Hospital (Traralgon) 0.5
Mildura Base Hospital 0.5
Sale (Central Gippsland Health Service) 0.5
Shepparton (Goulburn Valley Health) 0.5
Wangaratta (Northeast Health) 0.5
7.7 Total FTE 15.6
David Pilcher (0.1)Alvin Teo (0.5)Steve Philpot (0.4)
Bill Silvester (0.4)Steve Warrillow (0.2)Daryl Jones (0.2)Sarah Rickman (0.2)
Johnny Millar (0.5)
Himangsu Gangopadhyay (0.2)Nick Kokotsis (Maroondah) (0.3)
Bernadette Hickey (0.4)Sandra Neate (0.4)
John Green (0.1)Graeme Duke (0.1)Andrew Casamento (0.1)
Gopal Taori (0.4)Felix Oberender( (0.2)David Ernest (0.2)
Forbes McGain (0.3)
Subhash Arora (0.3)Fabrice Pierre (0.2)
Mainak Majumdar (0.5)
David Green (0.5)
Shena Graham (0.6)Maureen Cushnie (0.5)Zillah Day-Smith (0.4)
Jodi Vuat (0.5)
Bridget O'Bree (0.5)
Kathryn Coumans (0.5)
Monica Dowling (0.8)
Nicola Stitt (0.6)Karli Brkljacic (0.6)
Lyn Ireland (0.5)
Julie Clark (0.5)Tracey Mackay (0.6)Vicki Rippon (0.4)
Elizabeth Skewes (0.4)Jacinta Schlitz (0.4)
Yasna Lara (0.5) Kylie Chambers (0.3)
Samantha Brean (0.5)
Ros Roberts (0.5)
Tracy McConnell-Henry (0.5)
Carolyn Hargreaves (0.5)
Catherine Chanter (0.3)Kristie Campbell (0.2)
Jane Morse (0.5)
Jaspreet Sidhu (0.5)
Sofia Sidiropoulos (0.5)Leanne McEvoy (0.5)Louise Bourke (0.5)
Damien Hurrell (0.5)
Joanna Forteath (0.5)
Shymala Sriram (0.2)Treena Quarin (0.2)Tom Rechnitzer (0.2)Rohit D’Costa (0.4)
Gwenda Dortmans (0.5)
Natalie Gaffy (0.25) Angela Walter (0.25)
61
Victorian Volunteer Program50 DonateLife Volunteers
Metro City – 10 East – 6 West – 4 North – 4 South – 7 Geelong – 7
Regional East (Gippsland) – 1 West (Ballarat, Bendigo, Gisborne,
Mildura, Warrnambool) – 5 North (Benalla, Mansfield, Tatong,
Wodonga) – 4 South (Moe) – 2
62
Victoria’s success Supportive relationships – DonateLife in Victoria (DLV),
Department of Health, Blood Service (host of DLV), Organ and Tissue Authority, Transplant units, Hospitals
Highly committed Agency staff that include: Operations and clinical managers
Organ donor coordinators (8.0 FTE)
Education coordinator, Communications advisor
Donor family support coordinator
Audit coordinator, Administrative staff
Medical consultants

63
Next steps and future challenges

64
Next steps and challenges
1) Implementation of DCD in further hospitals

65
Victorian DCD ImplementationHospital Activation dateAlfred Active (2006)Austin Active (2007)Royal Melbourne Active (2008)Western Active (2010)Geelong Active (2011)Northern Sep‐11Dandenong Nov‐11Epworth Private Nov‐11Frankston Nov‐11Monash Medical Centre Nov‐11Royal Children's Nov‐11St Vincent's Nov‐11Mercy for Women (neonates) 2012Box Hill 2013Maroondah 2013Royal Hobart (Tasmania) 2012

66
Next steps and challenges
1) Implementation of DCD in further hospitals
2) Ensuring that there is no loss of a donor due to inability to facilitate a donation (surgical retrieval services, access to ICU beds)
3) Managing the ongoing growth – staffing, resourcing
4) Supporting regional hospitals – barriers to transferring patients to Melbourne for donation

67
Where are we going?
Organ and tissue donation as a routine part of end-of-life care
Every potential donor is identified and every family is properly informed and supported to make a decision about donation
Families know each others wishes regarding donation

68
Questions?