Embed Size (px)
DESCRIPTION
N.A. The following is not an indication for surgical correction of orbital Fx 1. A. Double vision 2. B. Enophthalmos 3. C. Greater than 50% floor involvement 4. D. Exophthalmos 5. E. None of the above
Citation preview
Orbital Trauma
David M. Yousem, M.D., M.B.A.Johns Hopkins Medical Institution
0% 0% 0% 0% 0%
1 2 3 4 5
N.A. What constrains a retinal detachment?
1. A. Ciliary body2. B. Hyaloid vessels3. C. Ora Serrata4. D. Zonular ligaments5. E. Orbital septum
0% 0% 0% 0% 0%
1 2 3 4 5
N.A. The following is not an indication for surgical correction of
orbital Fx
1. A. Double vision2. B. Enophthalmos3. C. Greater than 50%
floor involvement4. D. Exophthalmos5. E. None of the above
• Describe injuries to globe (bulbar)• List indications for acute globe
intervention• Describe retrobulbar injuries including
fractures (intraconal/conal/extraconal)• Discuss controversies re: fracture
intervention
Orbital Trauma Goals and Objectives

Orbital Trauma : Background
• Trauma to eye = 3% of ED visits• 4.5% of all orbital pathology is from
trauma• 40% of monocular blindness in US is
from trauma• Some findings require acute
treatment
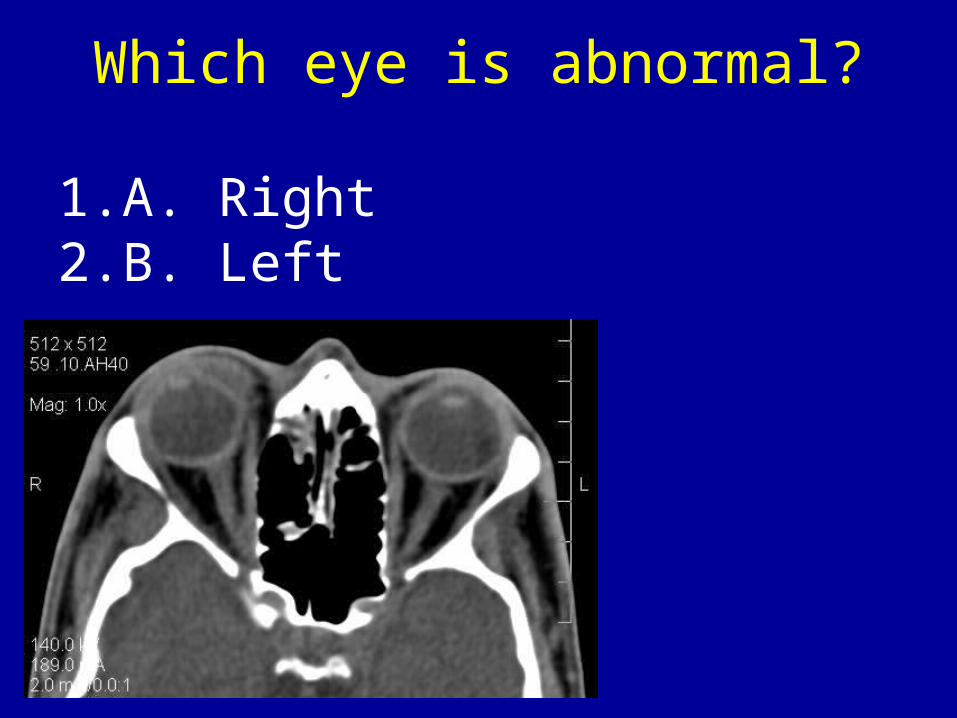
Which eye is abnormal?
1. A. Right2. B. Left

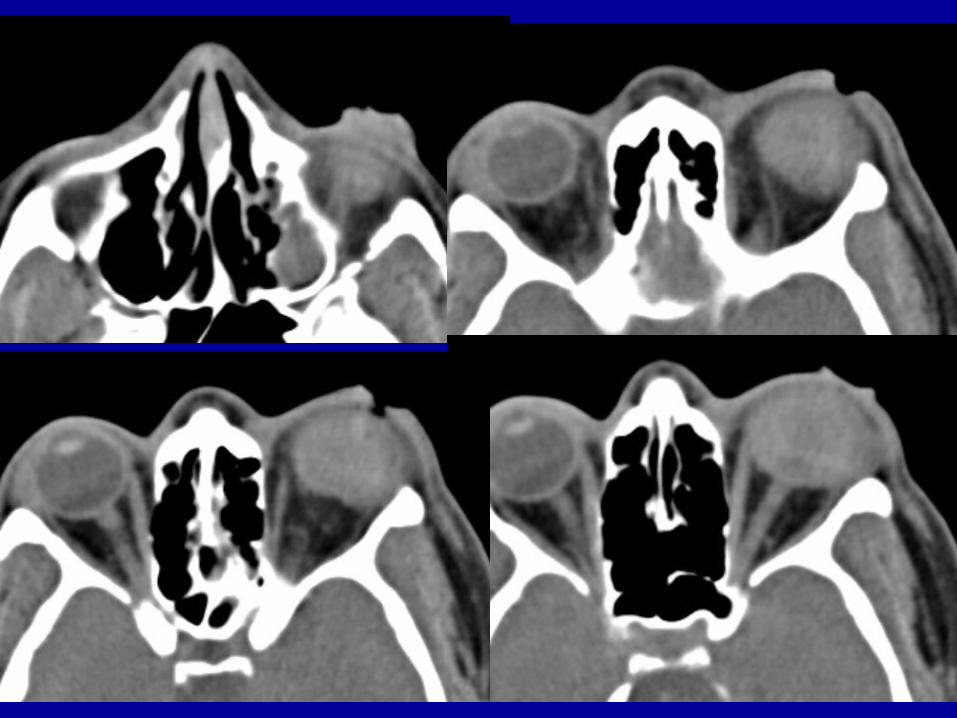
Ocular Blood Locations:
• Anterior chamber: anterior hyphema• Posterior chamber: posterior
hyphema• Vitreous: vitreous hemorrhage• Choroidal detachment• Retinal detachment
Anterior Chamber Trauma
• Rupture– Pain, decreased vision, hyphema– Flourescein slitlamp cobalt blue dilution
• Open injury• Hyphema
– Delayed/acute glaucoma : laser iridotomy• Traumatic cataract• Lens Displacement / dislocation
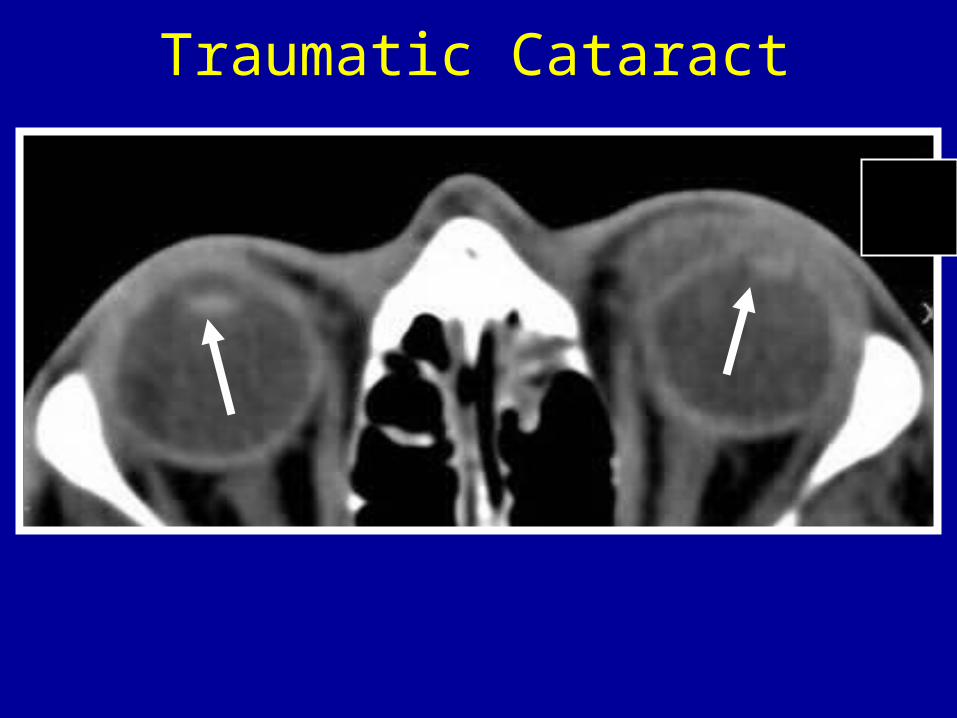
Traumatic Cataract
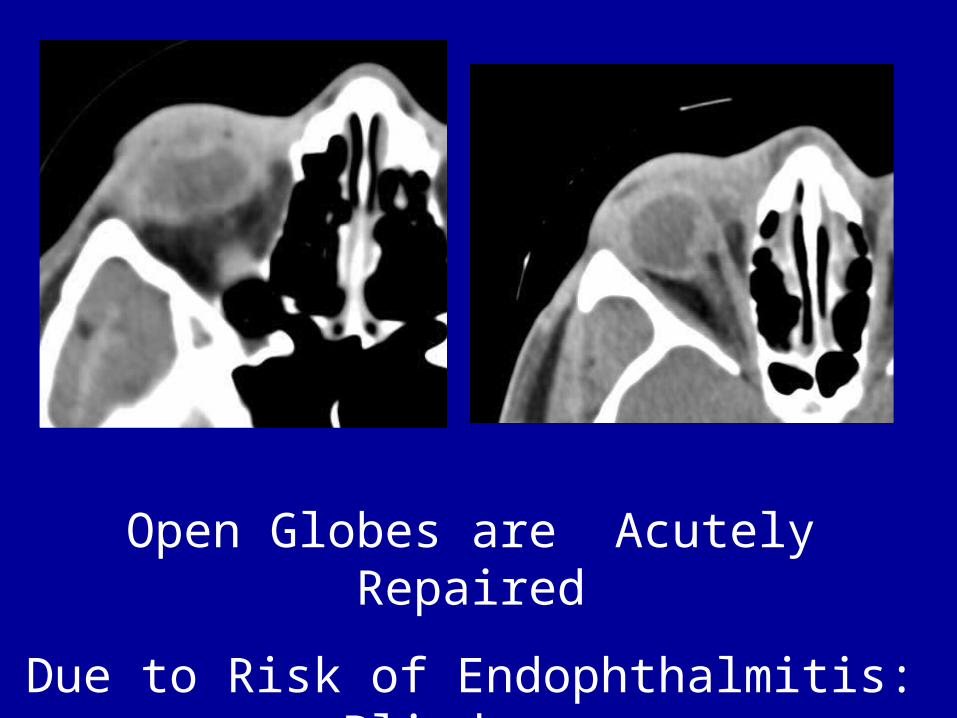
Open Globes are Acutely Repaired
Due to Risk of Endophthalmitis: Blindness
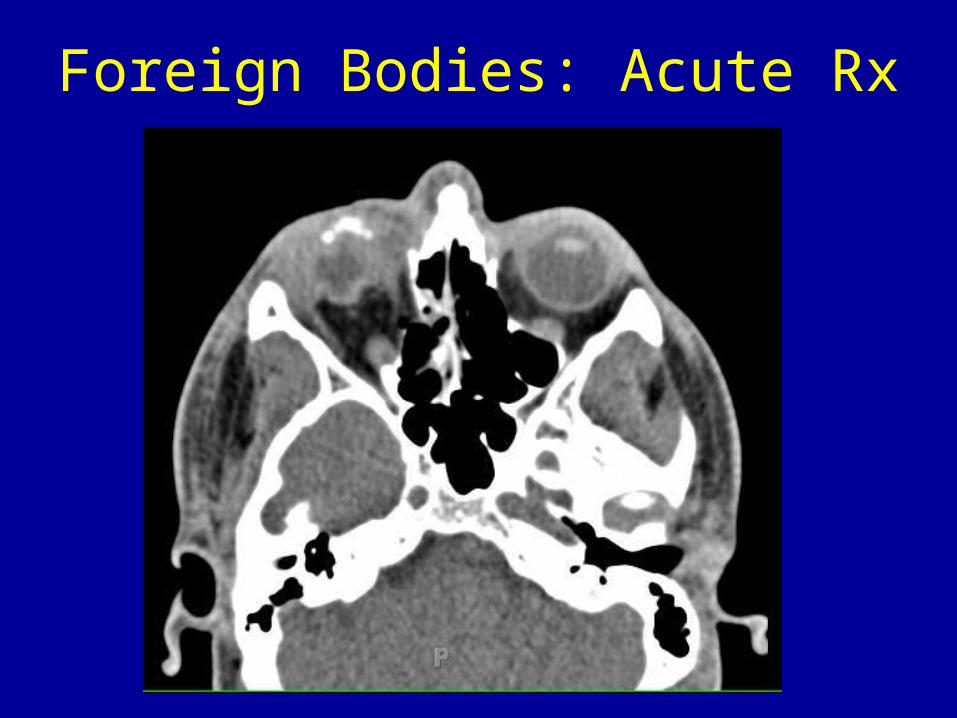
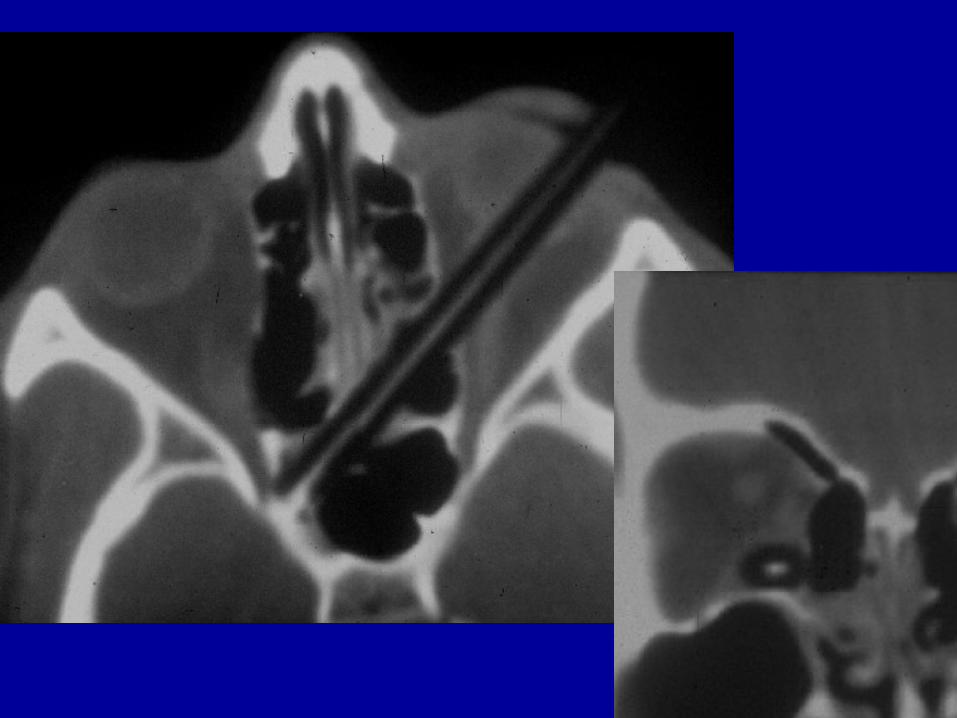
Foreign Bodies: Acute Rx
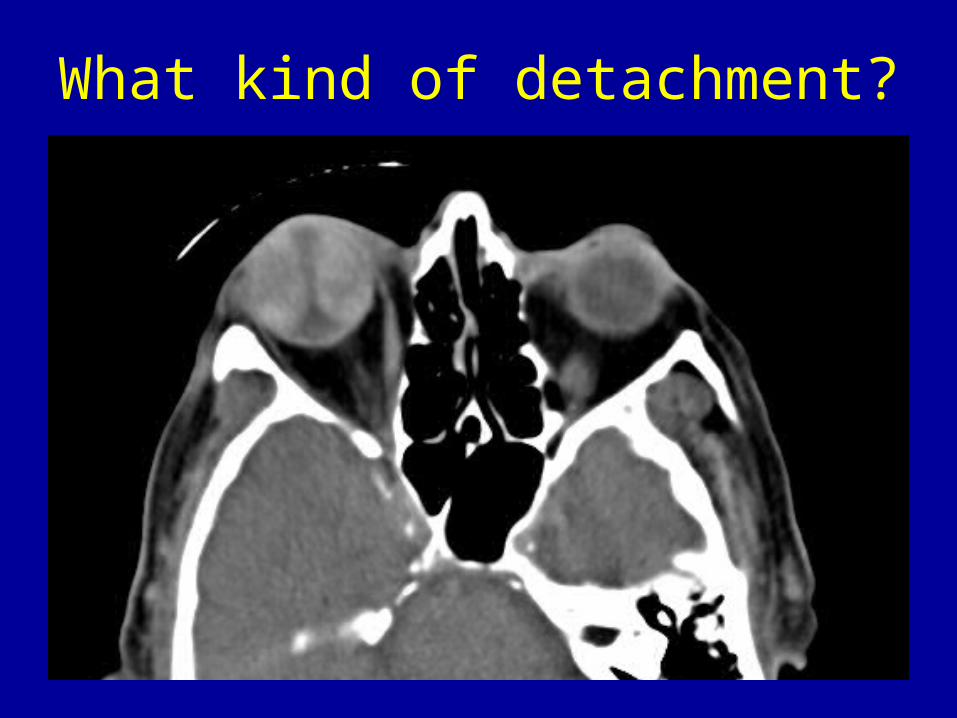
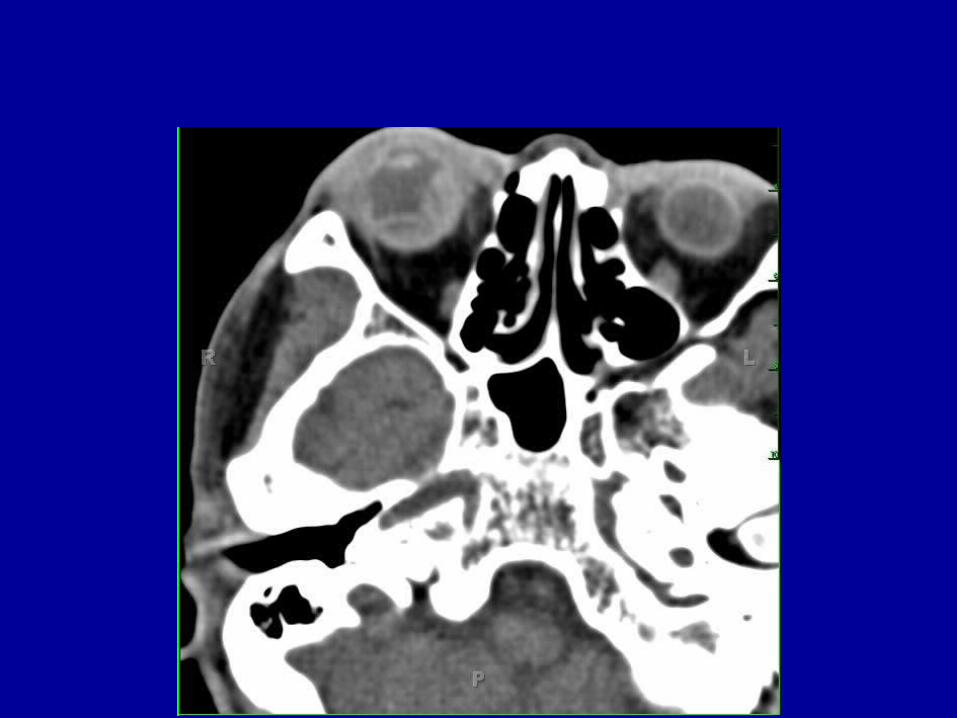
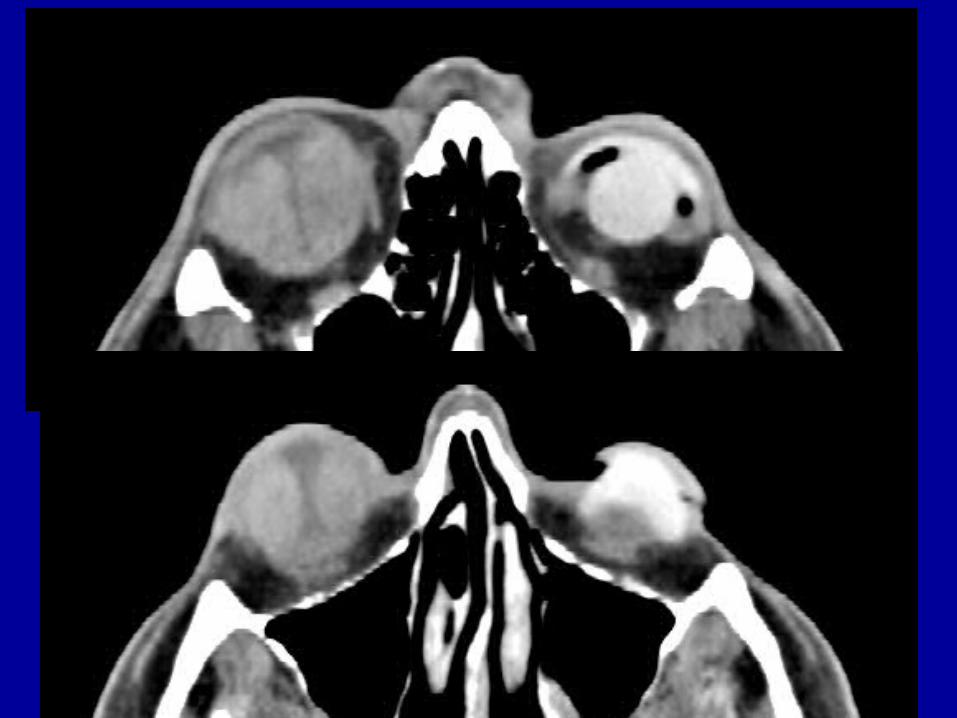
What kind of detachment?
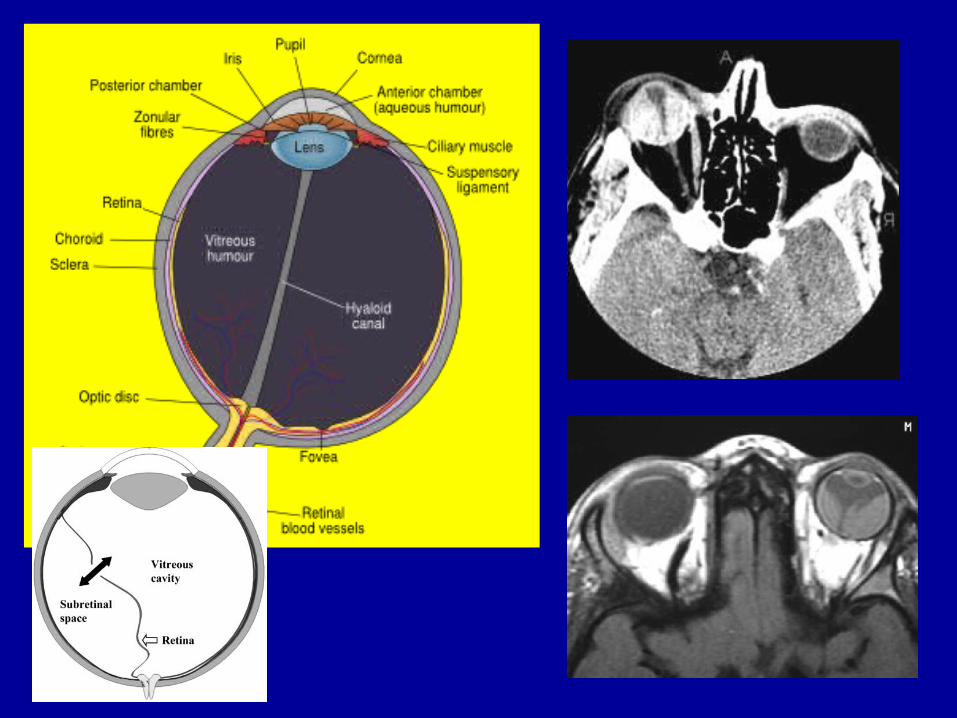
Ocular Membranes
• Retinal detachment– NAT!
• Choroidal detachment• Subhyaloid detachment• Puncture
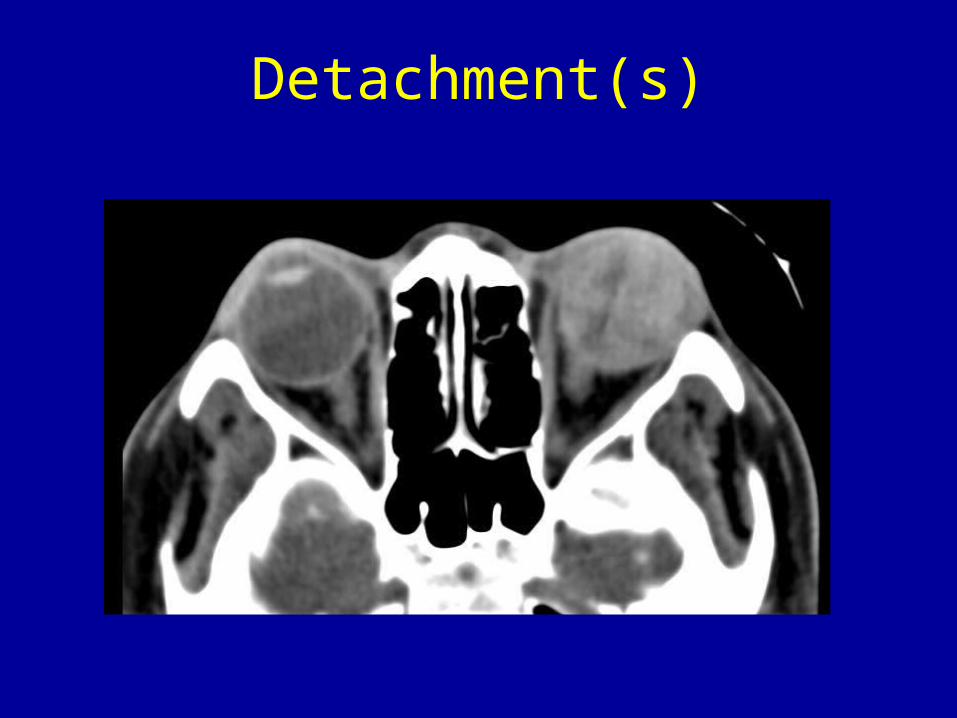
Detachment(s)


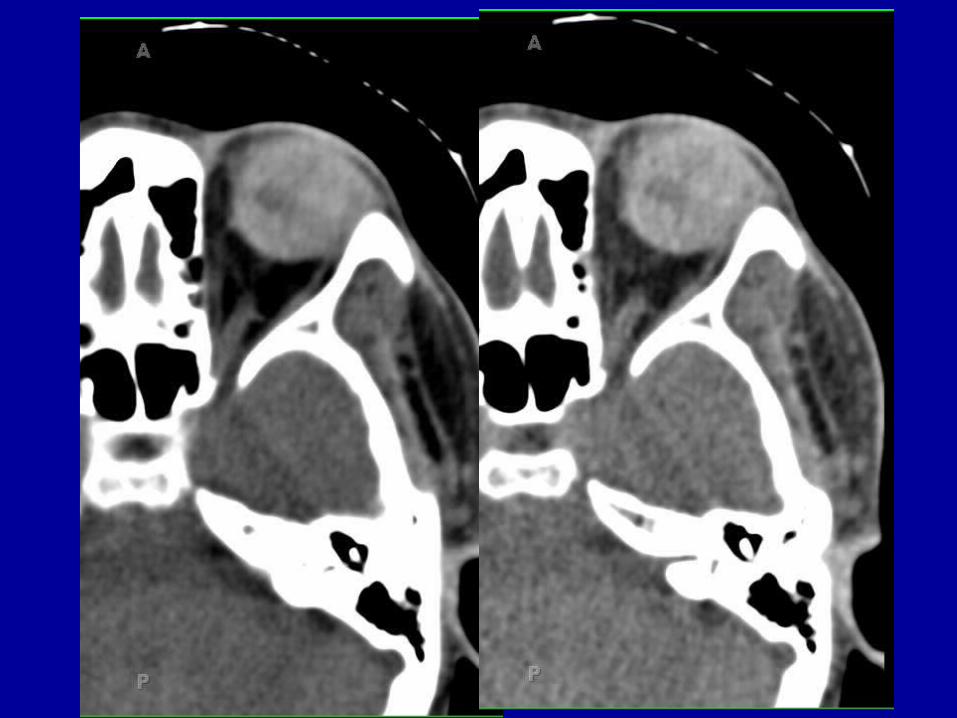
Vitreous Chamber
• Classic rupture• Ocular hypotony• Hemorrhage• Puncture• Late effect: Phthisis Bulbi
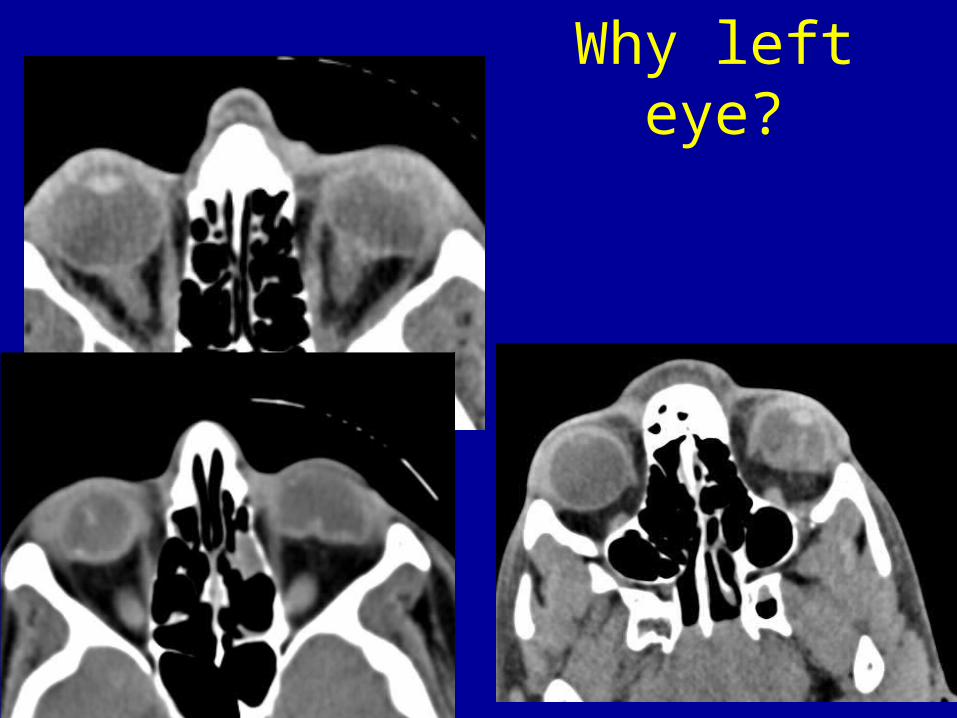
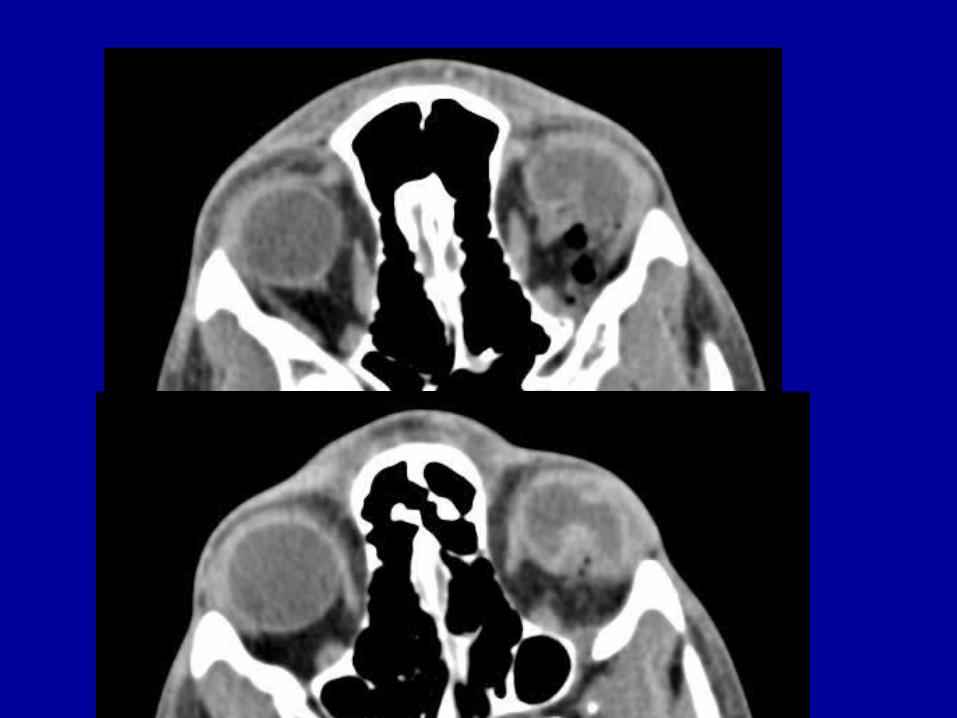
Why left eye?
Early Ocular Intervention• Open globe• Foreign bodies• Corneal abrasions• Hyphema• Globe lacerations• Detachments
– Scleral buckling / vitrectomy• Suck vitreous, treat retina, reinflate
oil/gas/saline
Surgery for Hyphema
• Uncontrolled elevated IOP• Corneal blood staining (opacification)• Large hyphemas of long duration • Sickle cell• Active bleeding
• Paracentesis, AC washout, hyphectomy, trabeculectomy
Complications
• Phthisis bulbi• Endophthalmitis in 10% of open globes
– Staph, Strep, Bacillus (rural, FB)– Antibiotics mandatory; ? Pars plana
vitrectomy– Vision loss in days
• Glaucoma: Drops then laser iridotomy– Potential for optic nerve ischemia
• Staphyloma
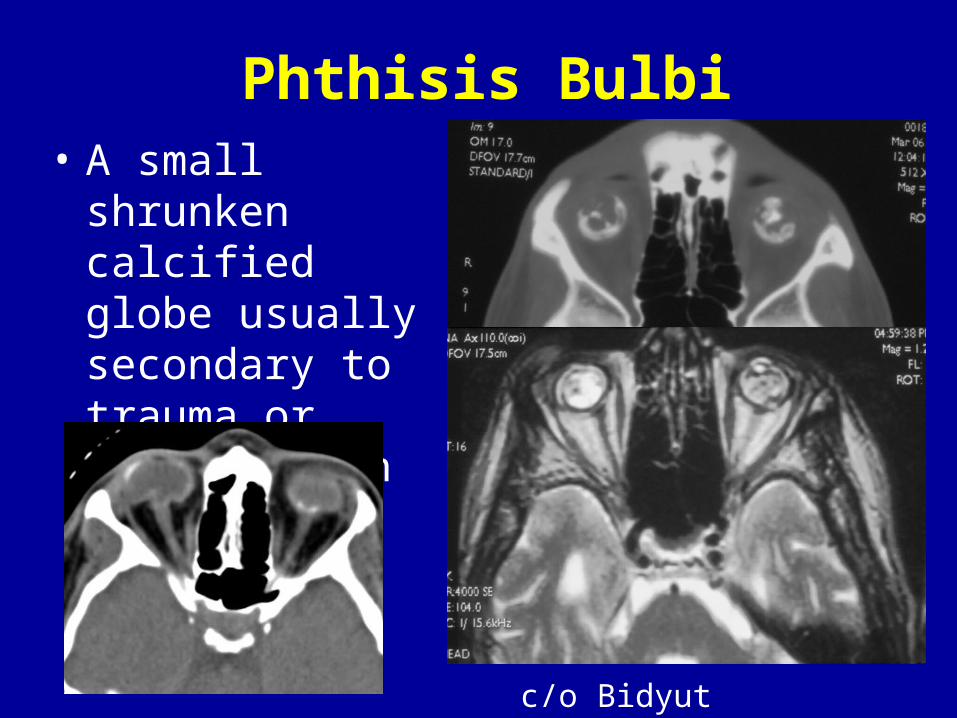
Phthisis Bulbi• A small shrunken
calcified globe usually secondary to trauma or inflammation
c/o Bidyut Pramanik
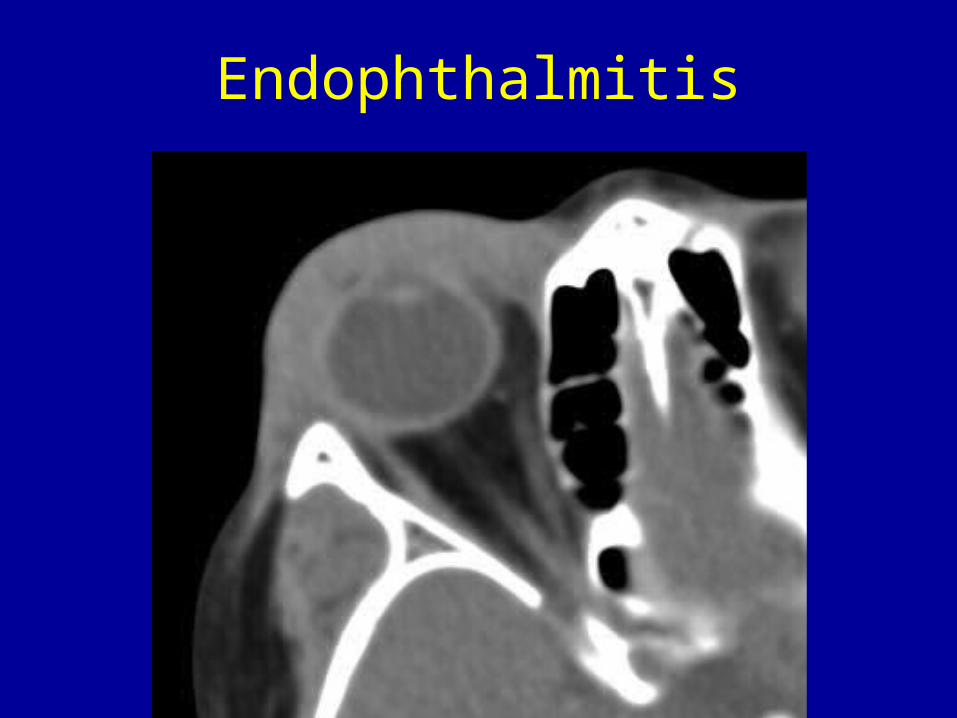
Endophthalmitis
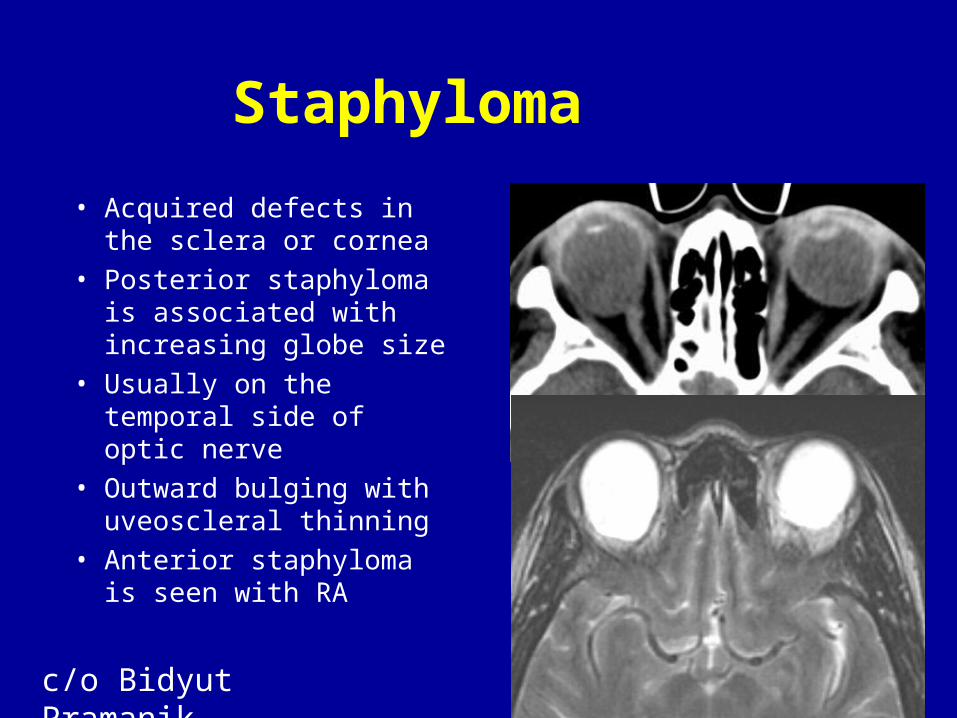
Staphyloma• Acquired defects in the
sclera or cornea• Posterior staphyloma is
associated with increasing globe size
• Usually on the temporal side of optic nerve
• Outward bulging with uveoscleral thinning
• Anterior staphyloma is seen with RA
c/o Bidyut Pramanik
Enucleation
• Blind painful eye• Endophthalmitis (esp open globe)• Phthisis bulbi• Severe traumatic rupture• Unsightly eye• Glaucoma
Non-ocular Orbital Trauma
• Intraconal / Conal– Retrobulbar hematoma– Optic nerve sheath hematoma– Injury to nerve– Injury to vessels– Traumatic muscle edema/hematoma– Muscular avulsion (Medial rectus)– Vascular
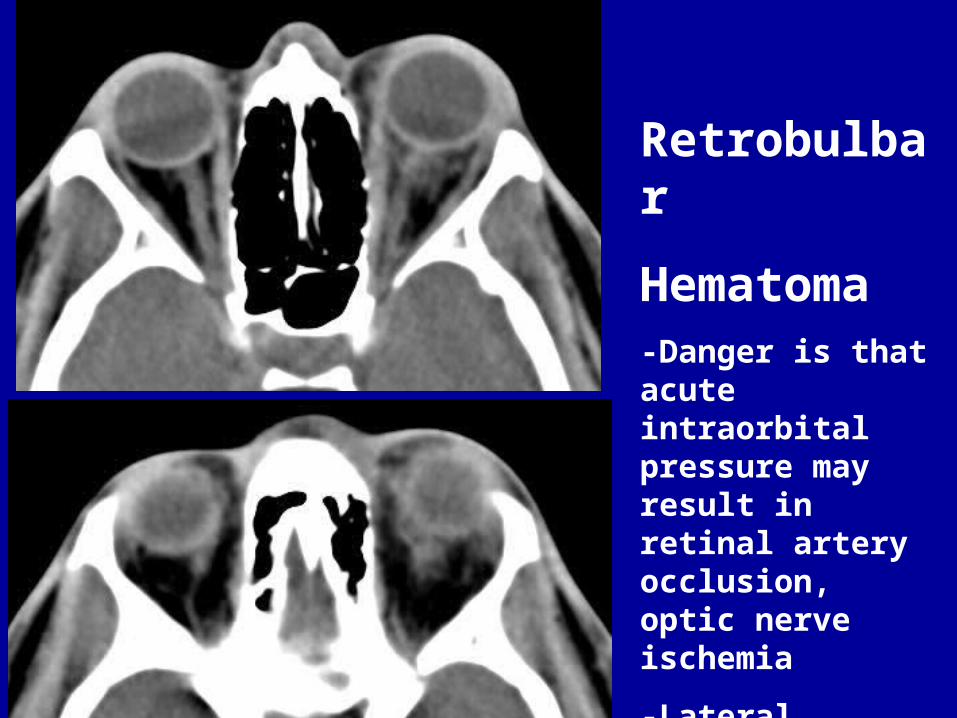
Retrobulbar
Hematoma-Danger is that acute intraorbital pressure may result in retinal artery occlusion, optic nerve ischemia
-Lateral canthotomy decompression

sheath
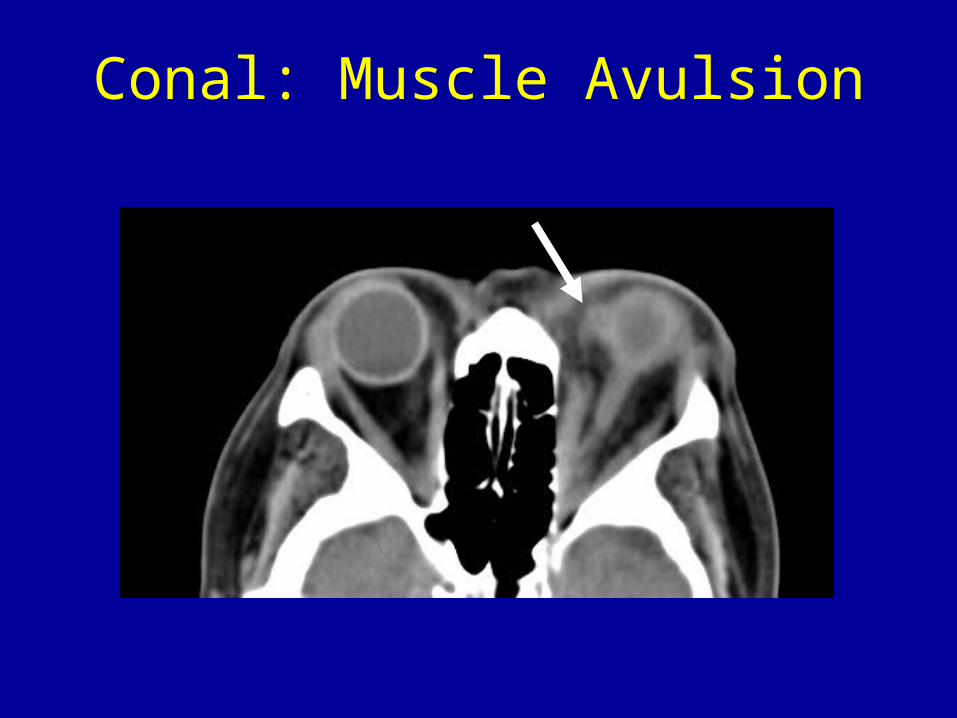
Conal: Muscle Avulsion
Orbital Trauma Vascular
• Carotid-cavernous fistula• Pseudoaneurysm• Varicosities
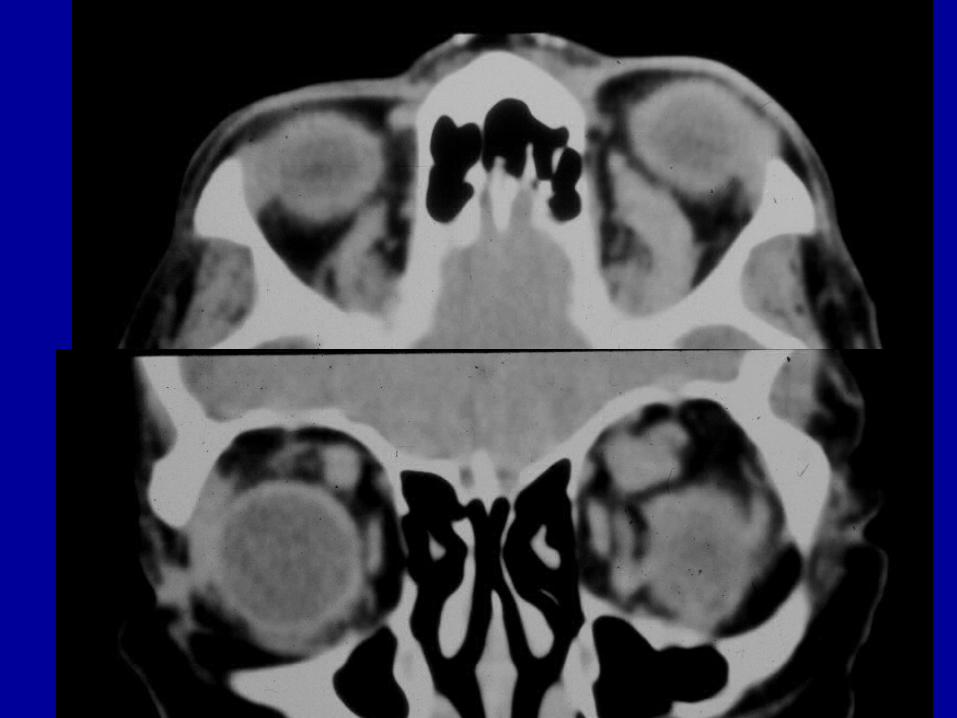
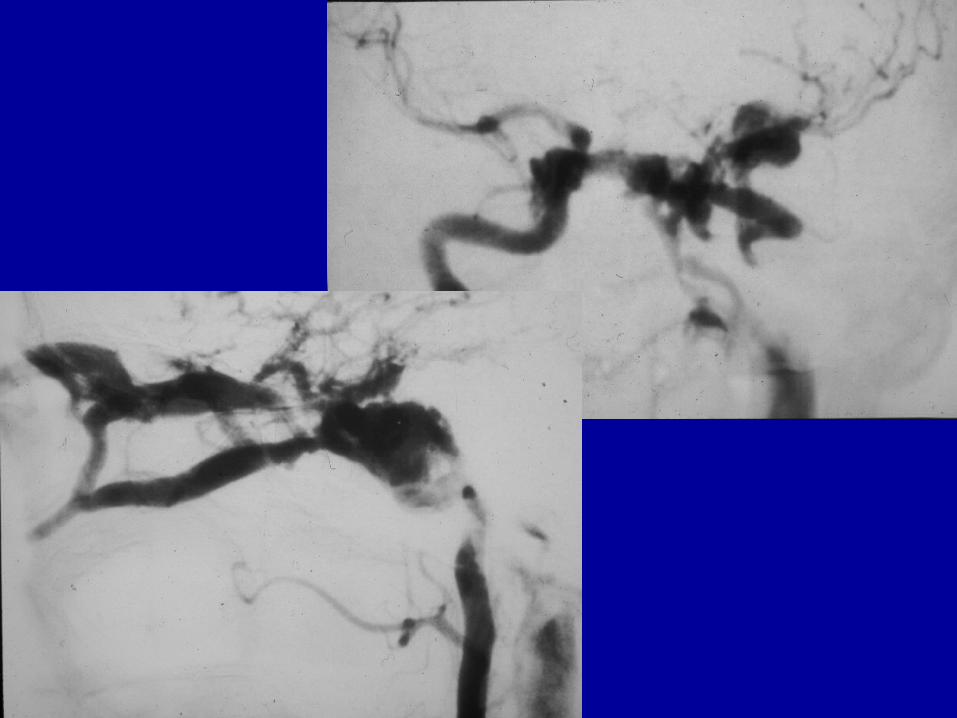
Carotid Cavernous Fistula
• May result in EOM enlargement due to venous engorgement
• All EOMs involved• Superior Ophthalmic Vein is dilated• Usually unilateral

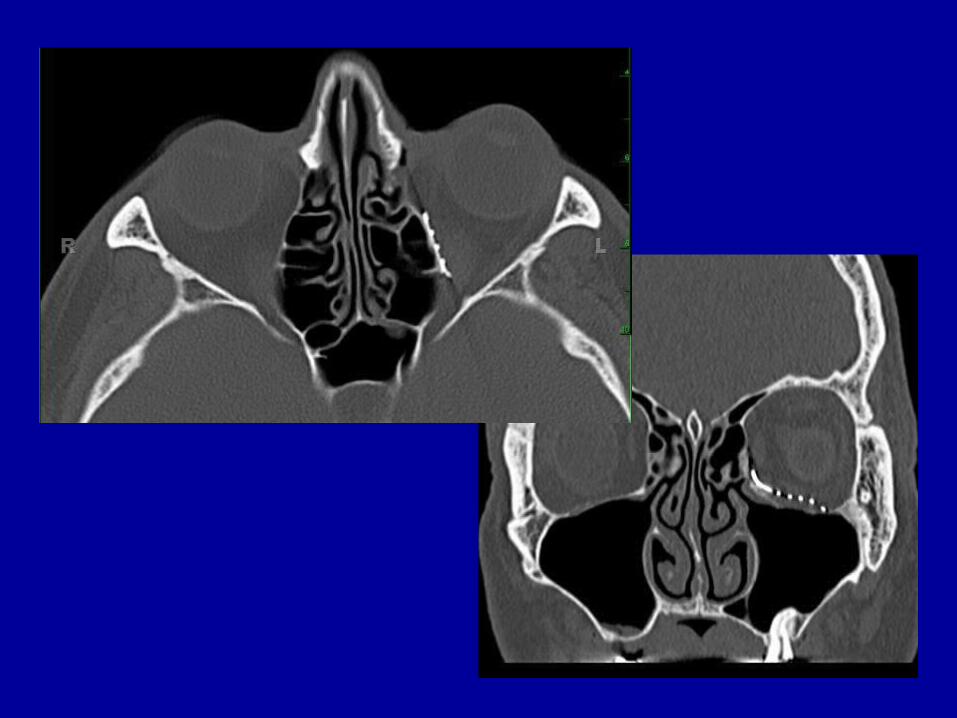
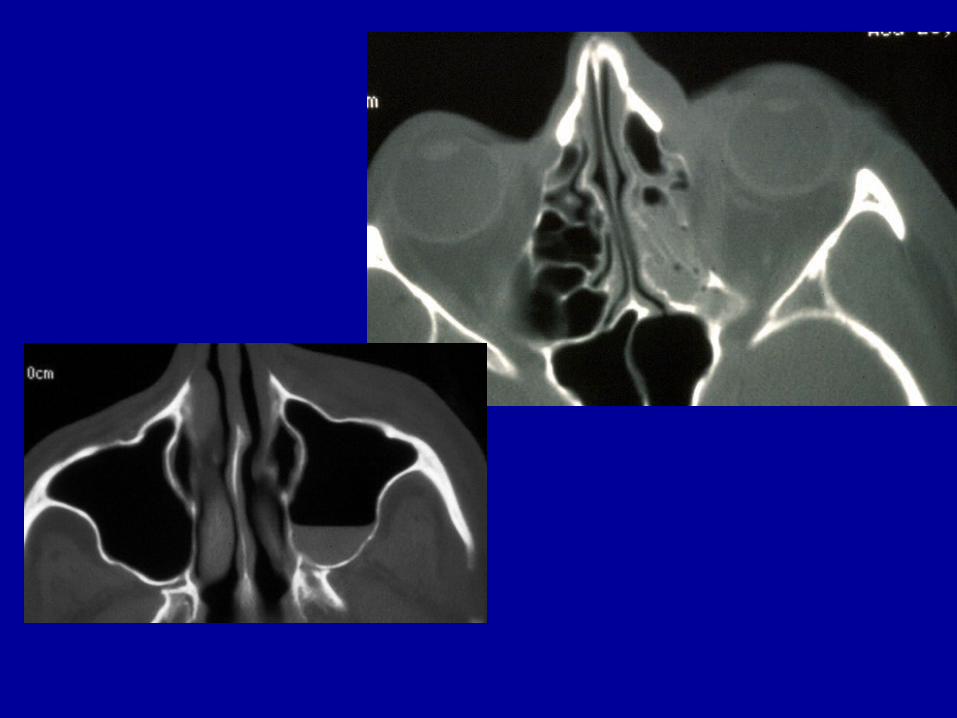
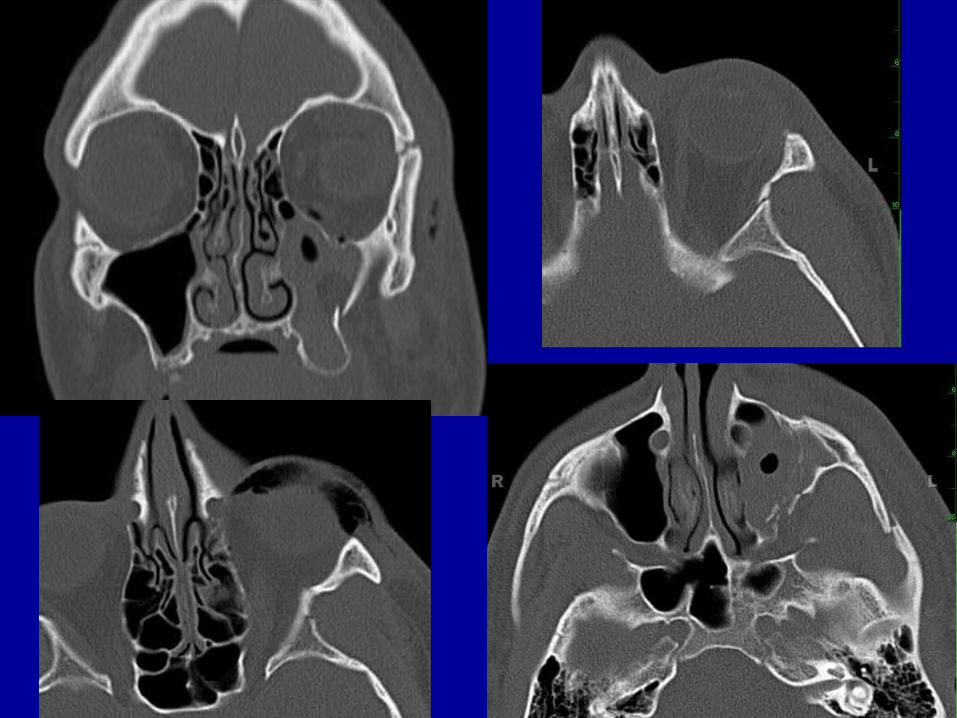
Extraconal: Orbital Fractures
• Orbital rim• Orbital floor• Medial orbital wall: lamina papyracea• Lateral orbital wall• Superior wall
– Globe injuries occur in 10-25% of patients with orbital fractures

Indications for Surgery for Orbital Fractures
• Enophthalmos > 2 mm (> 50% of floor)• Hypoglobus (downward displaced globe)• Diplopia
– Edema, heme, n. palsy, direct trauma• Increase in orbital volume > 1 cc
– Correlates with enophthalmos• Limited mobility (entrapment of EOM)• Compressive optic neuropathy
Kontio R, Lindquist C. OMFC 2009: 21: 209-220

Indications for Surgery for Orbital Fractures
• Fracture of > 50% of floor• Orbital tissue entrapment• Diplopia• Non-resolving oculocardiac reflex, also
known as Aschner reflex, – Decrease in pulse rate associated with
traction applied to extraocular muscles and/or compression of the eyeball
Chen CT et al. Cur Opinion Otol HNS 2010: 18: 311-6
Controversies in Surgery• When to repair orbital fractures
– Rarely considered emergent– ? Adhesions when delayed– ? Benefit of decreased swelling– Some say 14-21 days
• Unless optic neuropathy– Oculocardiac reflex: vagus– Children get operated earlier d/t increased
entrapment– Early surgery for penetration
Kontio R, Lindquist C. OMFC 2009: 21: 209-220
Controversies in Surgery
• What to repair with– Must be rigid to contain orbital contents– Restore form and volume– Contourable
• Autogenous grafts (iliac bone)– ? Too rigid, difficult to place
• Alloplasts (non/resorbable)– Many varieties
• Titanium mesh, MedporKontio R, Lindquist C. OMFC 2009: 21: 209-220
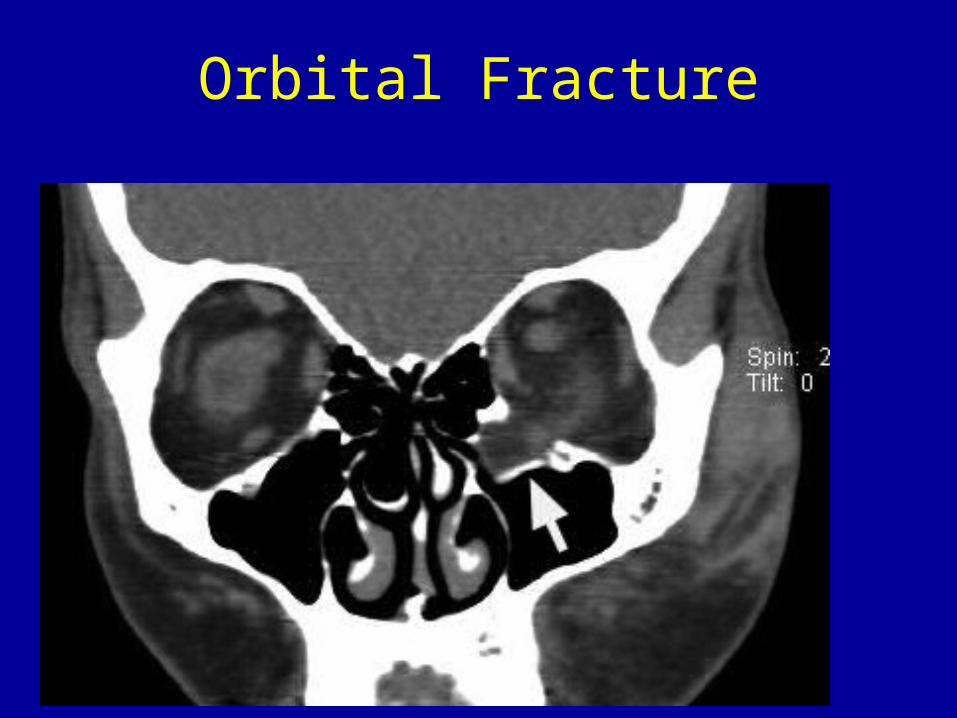
Orbital Fracture

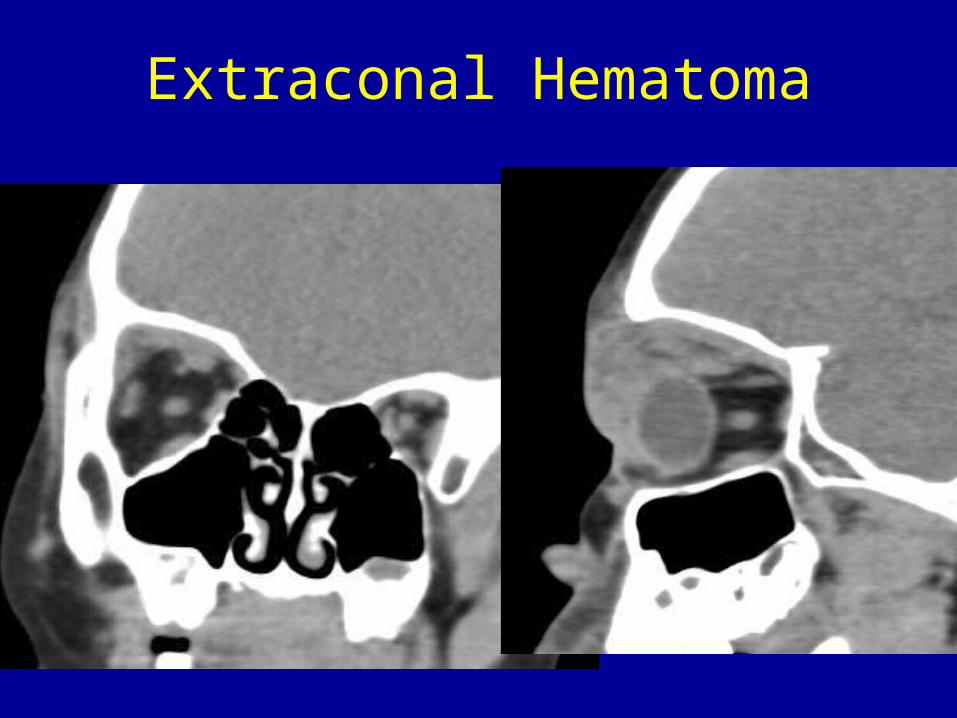
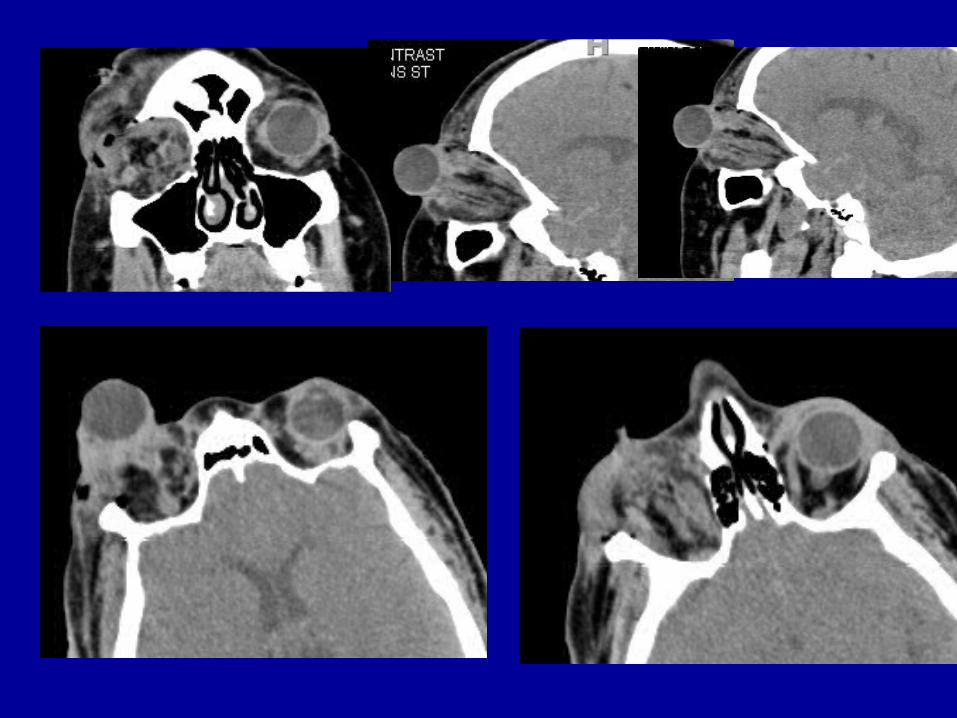
Extraconal Hematoma
Conclusions
• A common indication in ED practice• Ocular, non-ocular findings often
equally important• Some fractures should be treated
acutely• Long term sequelae