Embed Size (px)
Citation preview

Optimisation For Surgery
Neil BibbyMacmillan Senior Specialist HPB Dietitian

Setting the scene
Malnutrition Sarcopenia Frailty Cachexia Defined as a physiologic imbalance in energy and nutrients resulting from inadequate or improper utilisation of food.
Prevalence of 39% weight loss >10% and 71% >5% in pancreatic cancer patients at diagnosis
Defined as progressive and generalizedloss of skeletal muscle mass and strength
Prevalence of 55.9%-63% reported in pancreatic cancer patients
Defined as a chronic, progressive, involuntary weight loss which ispoorly or only partially responsive to the common nutritional support
Prevalence of up to 80% in those with progressing pancreatic cancer
Defined as the age-related,multidimensional state of decreased physiologic reserves
Prevalence of 25% reported in pancreatic cancer patients


• Surgery induces a state of metabolic activation - hormonal, haematological, metabolic and immunological changes - Surgical stress response
• Increased cardiac output and oxygen consumption, mobilisation of energy reserves, repair tissues and synthesise proteins involved in the immune response
• Adequate pre-operative physiological reserve is required to meet the functional demands of the surgical stress response
• Surgical patients with low reserve, including malnourished, frail and sarcopenic have diminished capacity to respond to the added demands of a surgical insult

Prehabilitation

Prehabilitation• defined as “[A] process on the cancer continuum of care that
occurs between the time of cancer diagnosis and the beginning of acute treatment and includes physical and psychological assessments that establish a baseline functional level, identify impairments, and provide interventions that promote physical and psychological health to reduce the incidence and/or severity of future impairments”
Silver et al 2013

Silver 2014

Benefits of Prehabilitation
• Reduced post-operative complications - mortality and morbidity• Reduced length of stay and re-admissions• Improved functional levels and fitness • Improved nutritional status • Improved quality of life • Faster recovery / greater tolerance adjuvant treatment • Greater understanding / compliance with enhanced recovery principle• Sustained behaviour change- smoking / alcohol• Patient empowerment

Current Evidence

Evidence - Pancreatic cancer


Manchester experience

Nurse led pre-op clinic
Prehabilitation and enhanced
recovery at MRI
ERAS+
Surgical anaemia service
Cardiopulmonary exercise testing
Prehab and rehab in HPB
Pharmacist medication
optimisation
Surgery school
Carbohydrate loading

Project Overview
Prehabilitation and Enhanced Recovery - An integrated programme of exercise and improved general well-being, nutritional support and psychological screening for HPB cancer patients undergoing surgery
This programme spans the four phases of the patient pathway:• Prehabilitation;• Enhanced recovery after surgery;• Recovery and reablement; and • Living with and beyond cancer.
Aim to offer the right support, to the right patients, at the right time.Working together in partnership.

Baseline Preoperative Dietetic Assessment
Workup for Whipple/ Total Pancreatectomy/ IRE N= 180
Workup for Distal Pancreatectomy
N= 24Weight (Kg) 70.3 72.5
BMI (kg/m2) 24.9 25
Weight change (%) -6.5 -6
Weight loss >5% (%) 62 48
Weight loss >10% (%) 34 17
Handgrip (kg) 27 24.2
Handgrip <85% (%) 46 44
Short PG-SGA score 7 5
Full PG-SGA score 10 8
Gastro- intestinal symptom score 9 16.5

Biochemistry Blood results Freq. low or raised levels
Vitamins A (n= 40) 2/ 5%
Vitamin E (n= 42) 0 / 0%
Vitamin D (n= 53) 25-50nmol = 18 / 34%<25nmol = 15 / 28%
Selenium (n= 47) 20 / 43%
Zinc (n= 46) 13 / 28%
Copper (n= 46) 2/ 4%
Haemoglobin (n= 75) 35 / 47%
Ferritin (n= 71) 6 / 9%
Folate and B12 (n= 69, 70) 3 / 4% and 5 / 7%
Random glucose (n= 58) 6 / 10%
HbA1c (n= 60) 13 / 22%


Pancreatic Enzyme Replacement Questionnaire (red numbers - before Dietitian input)

Average score with Dietitian input = 74% Average score without Dietitian input = 55%

Physiotherapy Input• International physical activity questionnaire (IPAQ)• Submaximal Cardiac Exercise test – Chester step
test• Individualised exercise prescription / home exercise
programme• Hospital anxiety and depression score
Outcomes• IPAQ - Every patient reported a linear increase with
subjectively reported activity levels• All patients improved on their physical fitness tests
Struggled to obtain repeat physical fitness tests for all patients. Several patients showed improvement on repeat cardio-pulmonary exercise testing

Prehabilitation data (n= 87) - minimum 14 days inputMedian prehab duration - 35 days
Baseline Review
Weight (kg) 64.8 67.4
BMI (kg/m2) 23.1 23.3
Weight loss >5% (%) 67 2.3
Weight loss >10% (%) 36 0
Weight change (%) -7.1 +1.9
Handgrip <85% (%) n=54 43 30
Handgrip (kg) 26.6 29
Short PG-SGA score 7 0
Gastro-intestinal symptom score 13 8
Median values

Case Study70 year old female with newly diagnosed head of pancreas adenocarcinoma PMH - Multiple Sclerosis, type 2 Diabetes - on insulin
Initial assessment 4/7/17• Weight - 65.2kg BMI: 23.1kg/m2 • Weight loss 10.7% over 1 month• Handgrip - 14.9kg (60% of normal)
Patient generated subjective global assessment (PG-SGA © ©FD Ottery 2005, 2006, 2015 v3.22.15) • Reduced food intake, taste changes and diarrhoea. • Able to do little activity and spending most of the day in bed/chair last 1 month • Overall score 16

• Gastro-intestinal symptom scale Severe pale/ greasy/ oily stools. Occasional abdominal bloating, wind and tiredness
High blood sugars- 20mmols, Vitamin D 29.8nmol/l, Hb 130g/l
Dietetic Plan • High energy/ protein diet • Start pancreatic enzyme replacement therapy• Diabetes review • Physiotherapy review• Once a day multi-vitamin and vitamin D replacement

Dietetic review - 24/7/17 and 7/8/17
• Weight - 67.6kg (increase 3.2kg) • Handgrip - 17.5kg (increase 2.6kg)
Patient generated subjective global assessment • Appetite and food intake good. Taste changes settled. No further loose stools • Activity levels increased- walking/ stairs
Gastro-intestinal symptom score - 3• Occasional wind, pale stools and tiredness.
Pancreatic enzyme questionnaire showed good understanding of pancreatic enzymes but advised to increase current dose

Cardio Pulmonary Exercise Test 3/8/17
• Performed well and only marker for higher risk ? due to hyperventilation
• Fit to proceed to surgery

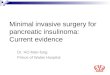
The Nutrition and Dietetic Patient Outcomes Questionnaire Adult Patient
01020304050607080
Helped you betterunderstand your
condition
Reassured you inmanaging condition
Helped you betterunderstand how to
manage your condition
Helped you feel lessanxious
Strongly agreeAgreeneither disagree or agreedisagreeStrongly disagree

“the intervention really did leave me feeling mentally, spiritually and physically fit in readiness of my surgery”
“feeling prepared and fit for an operation beforehand leaves you
feeling empowered”
Patient Interviews
“it was lovely being able to do something that would benefit me
post operatively”
“I found their advice and
support superb”
“feel the organisation should make this service available to more people”
“I was very weak and I was told I needed to get stronger for the operation, without their
help I wouldn’t be here today”
“Seeing the dietitian and physiotherapist reassured my mind as prior to my first visit I
was very very concerned”

Rehabilitation



1st Clinic Post-Op ReviewAll Patients N= 156
Weight (kg) 66.5
BMI (kg/m2) 23.2
Weight loss >5% (%) 72
Weight loss >10% (%) 28
Weight change (%) -9.1
Handgrip <85% (%) n=54 67
Handgrip (kg) 25.3
PG-SGA score 11
Gastro-intestinal symptom score 11

Whipple Adjusted Pathway
1st clinic post op (Year 1)
N = 38
1st clinic post-op (with call pre clinic appointment)
N= 16
Weight (Kg) 63.5 67
BMI (kg/m2) 21.6 23.2
Weight change (%) -8.4 -7.3
Weight loss >5% (%) 68 75
Weight loss >10% (%) 40 25
Handgrip <85% (%) 63 N= 30 87 N= 15
Short PG-SGA score 9 N= 36 9
Gastro- intestinal symptom score 11 N= 35 10 N= 13

Physiotherapy
• Patients reluctant to repeat formal exercise testing at this stage - when completed significantly below baseline
• Significantly reduced reported activity levels
• Evidence of muscle wasting
Greater evidence for supervised exercise sessions - feasibility likely greater in gyms more local to patients

1st clinic post opN= 63
Post chemo/ 6-12 months post op
Weight (Kg) 67.4 68.7
BMI (kg/m2) 23.3 23.7
Weight change (%) -9.1 +4
Handgrip (kg) 26.3 29
Handgrip <85% (%) 59 31
Short PG-SGA score 8 1
Gastro- intestinal symptom score 11 8
At 6-12 months patients gaining weight but is this actually muscle mass. Gastro-intestinal symptoms are often still present.

Ongoing gastrointestinal symptoms
• Ongoing diarrhoea and other GI symptoms can significantly impact on QOL
• If taking high dose PERT and PPI with no improvement other conditions should be investigated
• Bacterial overgrowth and bile salt malabsorption can occur

Challenges
• Clinical space to deliver the project as desired
• Robust referral and screening system
• Appropriate patients missed / not referred
• Requires patient engagement / travel distance / multiple appointments
• Limited time before surgery
• Adequate time on the day of surgery to repeat outcome measures

The future..• Proactive rather than reactive dietetic services
• Tertiary centres to train and support non-specialists
• Prehabilitation available to all patients
• Access to local centres for exercise support
• Greater use of technology
• Right treatment, for right patient, at the right time

Questions?