Embed Size (px)
Citation preview

Anaesthesia, 1982, Volume 37, pages 324327
C A S E R E P O R T
Open heart surgery in a patient with homozygous sickle cell disease
R . R I E T H M U L L E R , E. M . G R U N D Y A N D R . R A D L E Y - S M I T H
Summary
A child in heart failure nith homozygous sickle cell diseuse underwent corrective surgery on cardio- pulmonury bypass. The use of early intra-operative exchange transfusion produced a rapid fall in the level o j HbS. Postoperatively she developed falciparum malaria which responded to treatment. She was eventually discharged home to Nigeria 8 weeks after her operation.
Key words
Blood; haemoglobin, sickle cell anaemia. Surger,v; cardiovascular.
Case history
The patient was a negro currently residing in Nigeria. She had been slow to feed from birth and suffered with recurrent chest infections. At age 4 months a systolic murmur was present and her heart failure was controlled with digitalis and diuretics.
On admission she was 4 years 3 months old and weighed 12 kg. She was apyrexial but in heart failure with tachypnoea, marked rib recession and hepatomegaly. Anaemia and mild icterus were also noted, but no splenomegaly was detected. Angiography was compatible with double outlet right ventricle. The haematological investigations revealed a haemoglobin of 72 g/ litre with electrophoresis showing HbS 87% H b F 1076: Hh A, 3%; HbA not detectable. It was decided to exchange transfuse the child intra- operatively, because of the presence of heart failure.
She was premedicated with pethidine com- pound 1.2 ml (pethidine 30 mg, chlorpromazine 7.5 mg, promethazine 7.5 mg), and an hour later underwent an inhalation induction with halo- thane in oxygen. As soon as she was asleep an intravenous route was established, pancuronium 2.4 mg given and ventilation controlled on a 50:: oxygen, 50:/: nitrous oxide mixture. She was then intubated and monitoring lines were secured: these included an oesophageal temperature probe and an arterial and central venous line.
During the sternotomy blood loss was replaced volume for volume with fresh whole blood. The cardiopulmonary bypass pump (Bently BOS 5 ) was primed with 3 units of fresh heparinised blood. On commencement of cardiopulmonary bypass the first 800 ml of venous return from the caval cannulae was discarded and replaced with the extra volume in the pump prime. During a normothermic pump run of 58 minutes the double outlet right ventricle was repaired with
R. Riethmuller. FFARCS, Registrar. E.M. Grundy, MRCP, FFARCS, Senior Registrar. R. Radley-Smith, MRCP, MRACP. Consultant Paediatric Cardiologist. Harefield Hospital, Middlesex.
Correspondence should be sent to Dr E.M. Grundy, MRCP, FFARCS, Consultant Anaesthetist. Department of Anaesthetics, Hammersmith Hospital, Du Cane Road, London W12 ORS.
0003-2409/&2/030324 + 04 $02.00/0 @ 1982 The Association of Anaesthetists of Gt Britain and Ircland 324
Open heart surgery in a patient with homozygous sickle cell disease 325
a dacron graft, the heart having been perfused with cold cardioplegia solution. The girl was weaned from the pump without problems and was haemodynamically stable. Postoperatively she remained haemodynamically stable but required prolonged ventilation.
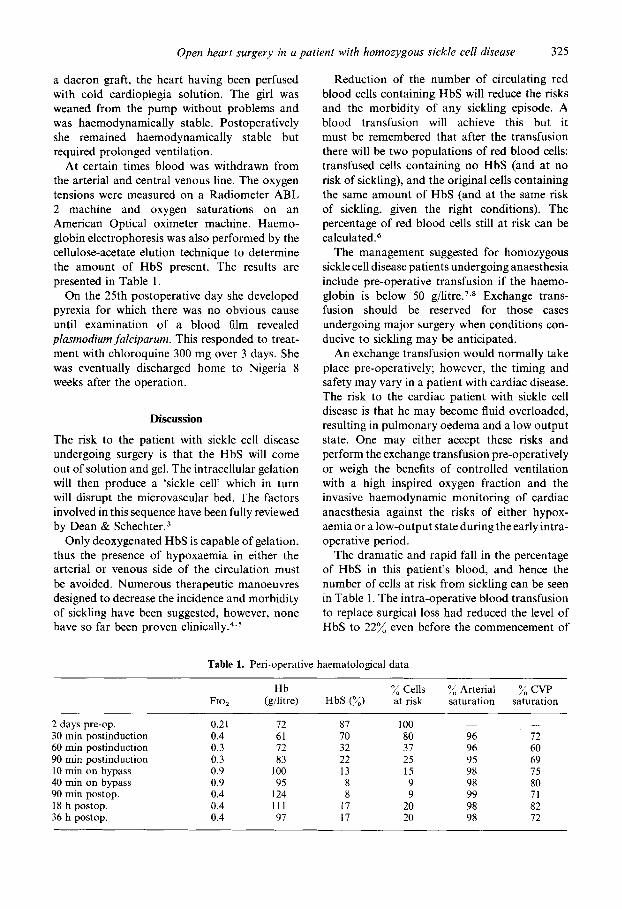
At certain times blood was withdrawn from the arterial and central venous line. The oxygen tensions were measured on a Radiometer ABL 2 machine and oxygen saturations on an American Optical oximeter machine. Haemo- globin electrophoresis was also performed by the cellulose-acetate elution technique to determine the amount of HbS present. The results are presented in Table 1.
On the 25th postoperative day she developed pyrexia for which there was no obvious cause until examination of a blood film revealed plasmodium falciparum. This responded to treat- ment with chloroquine 300 mg over 3 days. She was eventually discharged home to Nigeria 8 weeks after the operation.
Discussion
The risk to the patient with sickle cell disease undergoing surgery is that the HbS will come out of solution and gel. The intracellular gelation will then produce a ‘sickle cell’ which in turn will disrupt the microvascular bed. The factors involved in this sequence have been fully reviewed by Dean & S~hechter .~
Only deoxygenated HbS is capable of gelation, thus the presence of hypoxaemia in either the arterial or venous side of the circulation must be avoided. Numerous therapeutic manoeuvres designed to decrease the incidence and morbidity of sickling have been suggested, however, none have so far been proven ~ l in ica l ly .~ .~
Reduction of the number of circulating red blood cells containing HbS will reduce the risks and the morbidity of any sickling episode. A blood transfusion will achieve this but it must be remembered that after the transfusion there will be two populations of red blood cells: transfused cells containing no HbS (and at no risk of sickling), and the original cells containing the same amount of HbS (and at the same risk of sickling, given the right conditions). The percentage of red blood cells still at risk can be calculated.
The management suggested for homozygous sickle cell disease patients undergoing anaesthesia include pre-operative transfusion if the haemo- globin is below 50 g/litre.7.8 Exchange trans- fusion should be reserved for those cases undergoing major surgery when conditions con- ducive to sickling may be anticipated.
An exchange transfusion would normally take place pre-operatively; however, the timing and safety may vary in a patient with cardiac disease. The risk to the cardiac patient with sickle cell disease is that he may become fluid overloaded, resulting in pulmonary oedema and a low output state. One may either accept these risks and perform the exchange transfusion pre-operative1 y or weigh the benefits of controlled ventilation with a high inspired oxygen fraction and the invasive haemodynamic monitoring of cardiac anaesthesia against the risks of either hypox- aemia or a low-output state during the early intra- operative period.
The dramatic and rapid fall in the percentage of HbS in this patient’s blood, and hence the number of cells at risk from sickling can be seen in Table 1. The intra-operative blood transfusion to replace surgical loss had reduced the level of HbS to 22% even before the commencement of
Table 1. Peri-operative haematological data
Fio,
2 days pre-op. 30 min postinduction 60 min postinduction 90 min postinduction 10 rnin on bypass 40 min on bypass 90 min postop. 18 h postop. 36 h postop.
0.21 0.4 0.3 0.3 0.9 0.5, 0.4 0.4 0.4
Hh (gilitre)
72 61 72 83
100 95
124 111 97
HbS (%)
87 70 32 22 13 8 8
17 17
% Cells at risk
I00 80 37 25 15 9 9
20 20
”/, Arterial saturation
-
96 96 95 98 98 99 98 98
% C W saturation
- 72 60 69 75 80 71 82 12

326 R. Riethmuller, E M . Grundy and R. Radky-Smith
cardiopulmonary bypass. The additional partial exchange transfusion performed on establishing cardiopulmonary bypass further lowered the level of HbS to 13%.
Intra-operative management consists of avoidance of, and monitoring for. hypoxaemia and low-output states. A lower central venous oxygen tension (whilst not a true mixed venous sample) will suggest a low output state. Oxygen saturations are more relevant figures than oxygen tensions; however, it is well known that the haemoglobin-oxygen dissociation curve is shifted to the right for HbS, thus calculated saturations (which assume a normal dissociation curve) will be inaccurate and only measured saturations can be trusted.
Cardiopulmonary bypass in the heterozygote patient is not without risk. Leachman reports an aortic valve replacement in an undiagnosed case who died in crisis po~toperat ively,~ however, Samanthan reports a successful case of repair of atrial septa1 defect under deep hypothermia and circulatory arrest without exchange trans- fusion. ' O Pre-operative exchange transfusion has been utilised with a good result6 as has early intra-operative exchange transfusion on four reported cases.' L-13
Reported experience of cardiopulmonary bypass in the homozygote patient is limited to children. The five cases in the literature all underwent pre-operative exchange transfusion and had no problems from sickling.I4 With this case it was felt that a pre-operative exchange transfusion in a patient already in heart failure presented too great a risk. Instead the advantages of controlled ventilation and invasive haemo- dynamic monitoring, during the early intra- operative course, were thought to justify the risk of anaesthesia in a patient with heart failure without pre-operative exchange transfusion.
It is tempting to associate the postoperative appearance of clinical malaria with the low levels of HbS after the exchange transfusion. (It is known that the presence of HbS offers some protection against.fulcipurum malaria.) However. clinical malaria in the postoperative period following cardiopulmonary bypass has been reported in non-sickle patient,'*.l and detailcd enquiry from the family revealed a history of previous pyrexial illnesses very similar to this episode.
In the light of our experience in this case we feel that it would be justified to give malarial pro-
phylaxis to children %rho are homozygous for sickle cell disease prior to and after cardiac operations in which an extensive transfusion is given if they come from a country where malaria is endemic. ,This would diminish the risk of a recrudescence of malaria when the patient may be haemodynamically unstable.
In conclusion, we present a case of honio- zygous sickle cell disease who underwent cardio- pulmonary bypass. Early intra-operative ex- change transfusion was utilised because of the pre-operative presence of heart failure. The early and dramatic fall in the level of HbS suggest that this is a safe technique capable of greater utilisation. The appearance offakiparum malaria postoperatively was unexpected. It most proba- bly represented a recrudescence of a pre-operative infection and was unrelated to the presence of sickle cell disease
Acknowledgments
We would like to thank Mr M.H. Yacoub and D r R. Maclaurin for permission to report the details of this case and for their help and encouragement, and Mrs Shirley Richens for secretarial assistance.
References
I . ODURO KA, SEARLE JF. Anaesthesia in sicklc ccll states-a plea for simplicity. British Medical Journal 1972; iv: 59&8.
2. HOMI J. REYNOLDS J, SKINNER A, HANNA W. SERJEANT G. General anaesthesia in sicklc ccll disease. British Medical Journul 1979; k 1599-60 I .
3. DEAN J, SCHECHTER AN. Sickle cell anemia: molecular and cellular bases uf therapeulic approaches (first of three parts). New England Journal ojMedicine 1978: 299: 752-63.
4. DEAN J, SCHECHTER AN. Sickle cell anemia: molecular and cellular bases of therapeutic approaches (second of three parts). New Englmd Journal oJ' Medicine 1978; 299: 804- 1 I .
5. DEAN J. SCHECHTER AN. Sickle cell anemia: molecular and cellular bases of therapeutic approachcs (third of three parts). New England Journal of'lMedicine 1978; 299: 863-70.
6. HEINER M, TEASDALE SJ, DAVID T, SCOTT AA, CLYNN MFX. Aorto-coronary bypass in a paticnt with sickle cell trait. Canadian Anaesthefisis' Society Journal 1979; 26: 428-34.
7. HowF1.r.s TH, HUNTSMAN RG, BOYS JE, MAHMOOD A. Anaesthesia and sickle cell haemoglobin. British Journul of Anaesrhesia 1972; 44: 975-87.
8. SEARLE JF. Anaesthesia in sickle cell states: a review. Anaesthesiu 1973; 2 8 48-58.
9. LEACHMAX RD, MILLER WT, AKlAS IM. Sicklecell
Open heart surgery in u putient with homozygous sickle cell disease 327
trait complicated by sickle cell thrombi after open heart surgery. American Hearr Journal 1967; 7 4
10. SOMANATHAN S. Anaesthesia and hypothermia in sickle cell disease. Anuesrhesia 1976, 31: 113.
11. YACOUB MH, BARON J, ET-ETR A, KITTLE CF. Aortic homograft replacement of the mitral valve in sickle cell trait. Journal of’ Thoracic and Cardio- vascular Surgery 1970; 5 9 568-73.
12. DELEVAL MR, TASWELL HF, BOWIE EJW, DANIELSON GK. Open heart surgery in patients with inherited hemoglobinopathies, red cell dyscrasias, and coagulopathies. Archives ofsurgery
13. WENHAM PW, SCOTT GL, WISHEART JD. Red cell survival after aortic valve replacement with Bjork- Shiley prosthesis in presence of sickle cell trait. British Heart Journal 1978; 4 0 7034.
14. HARRIS LC, HAGGARD ME, TRAVIS LB. The coexistence of sickle cell disease and congenital heart disease: a report of three cases with repair
268-70.
1974; 109: 618-22.
under cardiopulmonary bypass in two. Puediarrics
15. PEARSON HA, SCHIEBLER GL, KROVETZ LJJ, BAKTLEY TD, DAVID JK. Sickle cell anemia associated with tetralogy of Fallot. New England Journal of Medicine 1965; 273 1079-83.
16. CKAENEN J, KILMAN J, HOSIER DM, WEINBERGER M. Mitral valve replacement in a child with sickle cell anemia. Journal of Thoracic and Cardiovascular Surgery 1972; 6 3 797-9.
17. SZENTPETERY S, ROBERTSON L, LQWER RR. Complete repair of tetralogy associated with sickle cell anemia and G-6-PD deficiency. Journal of Thoracic and Cardiovascular Surgery 1976; 72: 27& 279.
18. EYKYN SJ, BRAIMBKIDGE MV. Open heart surgery complicated by postoperative malaria. Lancet
19. MOK CK, CHEUNG KL, WAI KH, ONG GB. Malaria complicating open-heart surgery. Thorax
1964; 33: 562-70.
1977; 2 411-2.
1980; 35 89-91.