Embed Size (px)
Citation preview

1Donald M, et al. BMJ Open 2018;8:e019814. doi:10.1136/bmjopen-2017-019814
Open Access
Self-management interventions for adults with chronic kidney disease: a scoping review
Maoliosa Donald,1,2,3 Bhavneet Kaur Kahlon,3 Heather Beanlands,4 Sharon Straus,5,6 Paul Ronksley,2,3 Gwen Herrington,7 Allison Tong,8 Allan Grill,9 Blair Waldvogel,7 Chantel A Large,7 Claire L Large,7 Lori Harwood,10 Marta Novak,11,12 Matthew T James,1,2,3 Meghan Elliott,6 Nicolas Fernandez,7 Scott Brimble,13 Susan Samuel,14 Brenda R Hemmelgarn1,2,3
To cite: Donald M, Kahlon BK, Beanlands H, et al. Self-management interventions for adults with chronic kidney disease: a scoping review. BMJ Open 2018;8:e019814. doi:10.1136/bmjopen-2017-019814
► Prepublication history and additional material for this paper are available online. To view these files, please visit the journal online (http:// dx. doi. org/ 10. 1136/ bmjopen- 2017- 019814).
Received 5 October 2017Revised 22 January 2018Accepted 24 January 2018
For numbered affiliations see end of article.
Correspondence toDr Brenda R Hemmelgarn; B rend a.He mmel garn @ alber tahealthser vices. ca
Research
AbstrACtObjective To systematically identify and describe self-management interventions for adult patients with chronic kidney disease (CKD).setting Community-based.Participants Adults with CKD stages 1–5 (not requiring kidney replacement therapy).Interventions Self-management strategies for adults with CKD.Primary and secondary outcome measures Using a scoping review, electronic databases and grey literature were searched in October 2016 to identify self-management interventions for adults with CKD stages 1–5 (not requiring kidney replacement therapy). Randomised controlled trials (RCTs), non-RCTs, qualitative and mixed method studies were included and study selection and data extraction were independently performed by two reviewers. Outcomes included behaviours, cognitions, physiological measures, symptoms, health status and healthcare.results Fifty studies (19 RCTs, 7 quasi-experimental, 5 observational, 13 pre-post intervention, 1 mixed method and 5 qualitative) reporting 45 interventions were included. The most common intervention topic was diet/nutrition and interventions were regularly delivered face to face. Interventions were administered by a variety of providers, with nursing professionals the most common health professional group. Cognitions (ie, changes in general CKD knowledge, perceived self-management and motivation) were the most frequently reported outcome domain that showed improvement. Less than 1% of the interventions were co-developed with patients and 20% were based on a theory or framework.Conclusions There was a wide range of self-management interventions with considerable variability in outcomes for adults with CKD. Major gaps in the literature include lack of patient engagement in the design of the interventions, with the majority of interventions not applying a behavioural change theory to inform their development. This work highlights the need to involve patients to co-developed and evaluate a self-management intervention based on sound theories and clinical evidence.
IntrOduCtIOn Chronic kidney disease (CKD) is associated with adverse health outcomes, poor quality of life and high healthcare costs.1 Patients with CKD often experience a number of comorbidities including diabetes, cardiovas-cular disease and depression.2 They must balance the medical management of their kidney disease and other chronic conditions with demands of their daily lives, including managing the emotional and psychosocial consequences of living with chronic disease. In a recent CKD research priority setting
strengths and limitations of this study
► A strength of our study is that it is the first scoping review to apply the principles of patient-oriented research, where patient partners were engaged in determining the research question, advising us on search terms and reviewing the results to ensure we captured and reported the data meaningfully.
► Our scoping review is comprehensive in nature, with inclusion of all study designs and consideration of self-management features that have not been in-vestigated previously.
► Due to the heterogeneous nature of the literature, it was challenging to synthesise the data. To address this challenge the two reviewers used two stan-dardised tools to independently extract data and independently coded the outcomes into categories using the revised Self- and Family Management Framework.
► A limitation of our scoping review is that we were unable to assess the self-management outcomes in terms of sustained changes in behaviour, physiolog-ical and health status.
► We were unable to draw conclusions regarding the most effective self-management intervention for adult patients with chronic kidney disease, keeping in mind that our aim was to review the breadth of the current literature and present the gaps that exist.
on January 13, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2017-019814 on 22 March 2018. D
ownloaded from

2 Donald M, et al. BMJ Open 2018;8:e019814. doi:10.1136/bmjopen-2017-019814
Open Access
study, individuals with non-dialysis CKD, their caregivers, clinicians and policy-makers identified the need to develop optimal strategies to enable patients to manage their CKD and related comorbidities to slow or prevent the progression to end-stage kidney disease (ESKD).3 International data in research priority setting for kidney disease also highlights self-management as a top priority to prevent progression.4
Self-management interventions aim to facilitate an individual’s ability to make lifestyle changes and manage symptoms, treatment and the physical and psychosocial consequences inherent in living with CKD and associ-ated comorbidities.5 Self-management of CKD involves focusing on illness needs (developing knowledge, skills and confidence to manage medical aspects), activating resources (identifying and accessing resources and supports) and living with the condition (learning to cope with the condition and its impact on their lives as well as the emotional consequences of the illness).6 Self-man-agement requires patient engagement; however, the degree to which patients are able or willing to participate in self-management can vary, and individual and health system factors may serve as facilitators or barriers to self-management processes.7
Despite the high prevalence of CKD and its impact on patient outcomes, there is limited evidence on the effec-tiveness of self-management interventions. Prior system-atic reviews8–11 and three integrative reviews12–14 found that self-management interventions were variable in their effectiveness for managing and preventing progression of CKD. While these reviews add to the knowledge base, they have restricted inclusion criteria (eg, study type, patient population) and unclear reporting strategies (ie, describing complex self-management interventions in detail and providing structured accounts of the interven-tions and outcomes). In particular, features of self-man-agement interventions such as person centeredness, applicability to comorbidities associated with CKD, physi-ological and non-physiological outcomes and application of any behavioural change theories are often lacking. Self-management interventions need to be tailored to suit diverse patient needs and preferences as well as the local healthcare context.7 Therefore, investigating the ‘who’, ‘what’ and the ‘how’ of self-management interven-tions is crucial. We used recognised literature synthesis and reporting guidelines, along with engagement of our patient partners in determining the research question and search terms as well as reviewing the results to ensure we captured and reported the data meaningfully.
To our knowledge, there is no literature synthesis that systematically and comprehensively summarises the breadth of evidence found in primary quantitative, quali-tative and mixed methods research regarding self-manage-ment interventions for adult patients with CKD. We used a scoping review methodology to understand the range and types of interventions including both educational and support interventions for CKD to inform the future design of a self-management intervention. Specifically,
we conducted a scoping review to identify and describe self-management interventions for adult patients with CKD (stages 1–5; non-dialysis, non-transplant).
MAterIAls And MethOdsWe used a scoping review methodology to enable us to incorporate a broad range of studies and to summarise the knowledge from a variety of sources and types of evidence.15 Our aim was to identify gaps in literature related to CKD self-management interventions and inform future research. A unique and important aspect was the involvement of ‘patient partners’. Through a national initiative, Canadians Seeking Solutions and Innovations to Overcome CKD (Can-SOLVE CKD), patients work side by side with researchers, clinicians and decision makers to address patient-oriented research priorities.16 Our research team includes Can-SOLVE CKD patient partners with CKD and caregivers.16 Using the Joanna Briggs Institute framework for scoping reviews, we undertook the following steps: (1) identified the research question, (2) identified relevant studies, (3) completed study selection, (4) charted, collated, summarised and reported the results (5) and consulted with our patient partners.15 17 These steps were iterative to ensure compre-hensive inclusion of the literature and continued mean-ingful engagement with our patient partners. This work involves identifying, reviewing and categorising data from primary articles and does not involve human participants and is exempt from ethics approval.
research aimOur scoping review aimed to determine the available self-management interventions for adults aged 18 years and over and diagnosed with CKD stages 1–5 (not requiring dialysis or transplant).
search and selection of studiesWe worked with an information specialist (DL) to identify key words that represented the population (CKD) and the intervention (self-management). We searched a broad range of information sources including the following online databases: MEDLINE (OVID), EMBASE, PsycINFO, Cochrane Central Register of Controlled Trials, CINAHL Plus and Cochrane Database of Systematic Reviews for published studies, with no limits on date (inception to October 2016), language, age or study design. We also searched Web of Science from 2006 to October 2016 to capture recently published meeting abstracts and summa-ries. Using the Canadian Agency for Drugs and Tech-nology (CADTH) Grey Matters approach,18 we searched Google Canada, Health Technology Assessment (HTA) agencies (Canada, Australia, Ireland, UK and USA) and Clinical Trials databases (Biomed Central—ISRCTN Registry, US National Institutes of Health, ClinicalTrials. gov) during October 2016 with no language restrictions (online supplementary table 1). Our search strategy for grey literature was guided by the specific database (ie,
on January 13, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2017-019814 on 22 March 2018. D
ownloaded from

3Donald M, et al. BMJ Open 2018;8:e019814. doi:10.1136/bmjopen-2017-019814
Open Access
Google search operators, website search filters) and was completed within a single session for each search strategy to ensure consistency due to the dynamic nature of the internet (online supplementary table 2). Two reviewers (BK and MD) also reviewed the reference lists of included studies, along with those identified in past systematic and integrative reviews of our research topic. We contacted authors of relevant protocols and conference abstracts to ascertain if their work and findings were published.
A study was included if the population involved adults with CKD (stages 1–5, non-dialysis, non-transplant). Self-management interventions included strategies, tools or resources in any delivery format (print, electronic, face to face and so on) that facilitated an individual’s ability to make lifestyle changes or to manage symptoms, treatment or the physical and psychosocial consequences inherent in living with CKD and other associated comorbidities. Interventions targeted only at selection of treatment for ESKD (ie, dialysis, kidney transplant) were excluded. Other self-management interventions or standard care were considered as a comparison. We included primary studies that used quantitative, qualitative or mixed methods. Systematic and integrative reviews were identi-fied for the purpose of reviewing their included studies for potential relevant studies. We excluded case series, case studies, case reports, clinical practice guidelines, theses and opinion-driven reports (editorials, non-system-atic or literature/narrative reviews).
Three reviewers (BK, MD and BH) performed an initial screen of titles and abstracts using a citation screening tool. To determine inter-rater reliability, a calibration exer-cise was performed by the three reviewers. Pilot testing a random sample of 50 citations achieved good agreement (kappa=0.79) at which point the three reviewers screened the remaining titles and abstracts. Two reviewers (BK and MD) followed a similar procedure for identifying relevant full text studies, with good agreement between the two reviewers (kappa=0.78). Disagreements were resolved by discussion and obtaining consensus between the three reviewers.
Charting, collating and summarising the dataWe developed a data extraction form based on the Template for Intervention Description and Replication (TIDieR) checklist.19 This checklist provides a template to structure accounts of an intervention (eg, goal of intervention, materials used, who delivered the inter-vention and how, where, when and how much and how well the intervention was delivered). We also used the Effective Practice and Organisation of Care (EPOC) data collection form20 to ensure we were comprehensive in extracting relevant study characteristics as outlined by Cochrane EPOC group. Study characteristics (eg, study design, country of origin, publication year), popu-lation characteristics (eg, CKD stage, comorbidities) and self-management intervention characteristics (eg, topics, format, target audience, providers, location, dose, duration and so on) were documented. For the study
outcomes, the two reviewers (BK and MD) independently coded each outcome into categories identified by Grey et al (eg, behaviours, cognitions, physiological measures, symptoms, health status, healthcare and other).6 We pilot tested the form on a random sample of 10 eligible studies and once consensus between the two reviewers was reached, we independently abstracted data from the remaining eligible studies. Data were categorised and reported descriptively (ie, counts and frequencies). For qualitative studies, we identified the methodology and key concepts presented by the authors.
Consultation with patient partnersPatient partners were engaged throughout this work, specifically to provide input on the research ques-tion, search strategies (eg, grey literature sources) and reviewing the final results. The results were presented and discussed at the national Can-SOLVE CKD meeting.
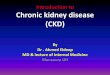
resultssearch resultsFrom 12 583 unique citations (figure 1), we included 50 full text studies.21–70
description of studiesA summary of the 50 studies included in this review is provided in table 1.
The most common study designs were randomised controlled trials (RCTs) (38%). Non-RCTs consisted of quasi-experimental (14%), observational (10%), pre-post intervention (26%), qualitative (10%) and mixed methods (2%). The studies were conducted in 14 coun-tries, including the USA (20%), UK (14%) and Australia (12%). Most studies were published in the last 5 years (64%).
Patient population characteristicsThe target population in most studies was CKD (72%) and 15 studies mentioned CKD plus one or more asso-ciated comorbidities. The average ages of participants reported across studies were 50.2 to 74.3 years.
description of self-management interventionsTable 2 summarises the characteristics of the self-man-agement interventions. Five studies reported the same self-management intervention;21–25 therefore, 45 inter-ventions were summarised. The most common inter-vention topic was diet/nutrition (64%) and the least common topics were symptom management and lifestyle (13% and 11%, respectively). The most frequent modes of delivering the intervention were face to face (80%), multiple (ie, more than one mode) (71%) and print (64%). Electronic was the least common delivery mode (16%). Interventions were administered by a variety of providers. The most common category of providers was ‘other’ (56%), which was made up of various types of health professionals and lay people. However, the most common identifiable group of providers were nursing
on January 13, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2017-019814 on 22 March 2018. D
ownloaded from

4 Donald M, et al. BMJ Open 2018;8:e019814. doi:10.1136/bmjopen-2017-019814
Open Access
professionals (49%). Patient volunteer/mentor was the least common (9%). The outpatient setting was the most common location for providing the self-management intervention (51%), and the inpatient setting was the least popular (2%). Many studies did not report the inter-vention language (53%), but 12 languages were repre-sented and seven studies reported that they provided the intervention in multiple languages.
In terms of intervention development, only 20% of studies mentioned the use of evidence such as theories or frameworks. These included the transtheoretical model of behaviour change, social cognitive theory and chronic care model.26–30 Less than 1% of the studies involved patients in the design of the intervention, where patients were interviewed regarding intervention content.26 31–33
description of quantitative study outcomes and resultsCharacteristics of the quantitative study outcomes are presented in table 3. Twenty-three (46%) studies measured physiological outcomes (ie, laboratory tests, body composition and so on). The least common outcomes reported by studies were health status and healthcare (each 10%) and symptoms (ie, fatigue) (4%). Table 4 summarises the details of the quantitative studies. We categorised the overall study results descriptively as improved, unchanged or worse. Many studies had more than one outcome measure (eg, one measure improved, another had no change) and they were reported as mixed results. Based on this method of categorization, 89 outcomes were reported, of which 61% improved, 20% had no change, 1% worsened and 13% had mixed results. Four of the results were reported as not applicable as the outcomes were not relevant. Of the 54 outcome categories
that improved, 15 were cognition, 9 were physiological measures, 8 were behaviours, 8 were individual outcomes, 5 were health status, 4 were healthcare, 4 were interven-tion specific and 1 was symptom management.
description of qualitative study outcomes and resultsTable 5 summaries the findings from six qualitative studies that explored patient perspectives, one of these being a mixed methods study. All studies used semistruc-tured interviews and one also used a questionnaire. The aims of all these studies were to examine patient perspec-tives’ regarding the self-management interventions they were involved in. Due to the variety of interventions (eg, intervention topics, delivery mode and providers of the intervention), it was difficult to summarise findings into meaningful categories. Overall, patients highlighted that interventions needed to be individualised and tailored to their specific situations and preferences (eg, awareness of having CKD, stage of CKD, knowledge of the disease, access to resources and so on).
dIsCussIOnTo our knowledge, this is the first scoping review involving patients as research partners to identify and summarise self-management interventions for adults with CKD. The scoping review methodology enabled us to systematically summarise a broad range of self-management interven-tions and describe their features. We identified 50 studies that investigated self-management interventions for adults with CKD, with considerable variation in interven-tions, outcomes assessed and results obtained (ie, some improved and/or some worsened and/or some did not
Figure 1 Prisma flow diagram.
on January 13, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2017-019814 on 22 March 2018. D
ownloaded from

5Donald M, et al. BMJ Open 2018;8:e019814. doi:10.1136/bmjopen-2017-019814
Open Access
change). We found that self-management interventions for CKD is an emerging area with most studies published within the last 5 years which may be related to the growing recognition of the importance of incorporating patients and their families in managing their disease to improve outcomes.7
Our findings are similar to prior reviews reporting that the design of self-management interventions for CKD has not been theoretically driven and they have been predomi-nately designed by healthcare professionals without input from patients.13 14 Person-centred care is changing how healthcare professionals deliver care to patients, but more importantly how patients and their families are actively involved in self-managing their chronic conditions.71 Engaging patients by having them co-design self-manage-ment interventions will ensure that patient preferences based on their values, culture and psychosocial needs will be addressed in the self-management intervention.12–14 Through our current national partnership with patients, researchers and clinicians, we have the opportunity to
Table 1 Characteristics of the studies included in scoping review
CharacteristicStudies (n=50)
Study design
Randomised controlled trial 19
Pre-post test 13
Quasi-experimental (controlled/non-random) 7
Observational 5
Qualitative 5
Mixed methods 1
Origin of study
USA 10
UK 7
Australia 6
Canada 5
Taiwan 5
Netherlands 3
Spain 3
Italy 2
Japan 2
New Zealand 2
Sweden 2
Brazil 1
Denmark 1
Korea 1
Year of publication
2012–2016 32
2007–2011 11
Prior 7
Table 2 Overall characteristics of self-management interventions
VariableIntervention count (n=45)
Intervention topics
Diet/nutrition 29
General CKD knowledge 18
Other (ie, advanced care planning, meditation)
18
Medication 17
Modalities 13
Physical activity 13
Comorbidities 11
Symptom management 6
Lifestyle 5
Mode of delivery
Face to face (ie, group, one-on-one) 36
Multiple modes 32
Print 29
Distance (ie, telephone, email) 13
Digital (ie, DVD, PowerPoint, audio recording)
8
Electronic (ie, website, mobile application)
7
Type of providers
Other* 25
Nurse/nurse practitioner 22
Dietitian 14
Multiple providers 13
Social worker 6
Physician/primary care physician 6
Nephrologist/nephrology fellows 5
Patient volunteer/mentor 4
Pharmacist 1
Location of intervention
Outpatient 23
Not specified 12
Community (non-clinic)† 10
Patient home 10
Multiple locations 7
Inpatient 1
Intervention languages
Not Specified 24
English 10
Multiple languages 7
Mandarin 4
Spanish 3
Taiwanese 3
Continued
on January 13, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2017-019814 on 22 March 2018. D
ownloaded from

6 Donald M, et al. BMJ Open 2018;8:e019814. doi:10.1136/bmjopen-2017-019814
Open Access
obtain patient perspectives, along with incorporating a behaviour change theory to inform the future design of a self-management intervention for CKD.
Only 28% of studies that we identified included patients with CKD plus other comorbidities, despite the common presence of comorbidities in this patient population. Less than one-quarter of included studies provided infor-mation on how to manage comorbid conditions such as tracking lab results and symptom management. This highlights the need to consider ‘whole person care’,
where the self-management intervention needs to encom-pass the physical, mental and emotional needs of the patient72 73 that are important to them as well as meeting the individuals desires by collaboration between relevant providers.71
Forty-five different self-management interventions were identified, with one or more topics presented in a variety of formats and by a variety of providers. Symptom management and lifestyle topics were not included in many of the interventions. Based on prior work,3 non-di-alysis patients with CKD have indicated that these were important topics for them in managing their CKD with an aim to slow the progression of CKD and will be important to consider in the development of future interventions. Face to face was the most common delivery format while electronic (internet or mobile application) was least common, with many studies reporting multiple formats (ie, face to face and printed materials). With the expan-sion of electronic platforms for supporting patients and providers in the uptake of evidence-based care, there is the potential to use an electronic format to support patients in self-managing their CKD and other comorbidities.74 It is worth noting that there was variability in duration and frequency of face to face encounters, from a single session to multiple sessions over weeks to months. While varied options for in-person delivery is good if it meets the needs of the patients and their families, it may not be feasible on a larger scale due to the resources required. Only five studies looked at self-management healthcare cost-effectiveness, healthcare utilisation and access, each measuring different end-points with mixed results. Future self-management interventions should include the essen-tial principles to self-management (eg, accessing rele-vant health information, adhering to multiple treatment
VariableIntervention count (n=45)
Dutch 2
Cantonese 1
French 1
Greek 1
Italian 1
Japanese 1
Swedish 1
Vietnamese 1
Intervention development
Use of framework or theory 9
Codesigned with patients 4
*Other providers: Trained research assistant, lay health worker, Bengali worker, Educators (health, cook, diabetic), online tool, physician assistant, exercise physiologist, technician, psychologist, employment expert, instructor, interpreter, physiotherapist, patient, principal investigator.†Community: gym, grocery store, "study room". CKD, chronic kidney disease.
Table 2 Continued
Table 3 Summary of quantitative study outcomes*
Common outcomes DescriptionNumber of studies
Number of studies in which outcome improved
Physiological measures
Changes in laboratory tests, blood pressure, body composition, functional/performance tests and cardiovascular risk
23 9
Cognitions Changes in general CKD knowledge, self-efficacy, self-management, motivation, perceived stress, anxiety and fear
21 15
Behaviours Adherence to diet, medication, physical activity, sleep, blood pressure control
13 8
Individual outcomes QOL, well-being and general satisfaction 11 8
Intervention specific Reporting of general concepts regarding feasibility of intervention, enjoyment and interest in intervention
9 4
Healthcare Measurements of cost effectiveness, healthcare utilisation and access
5 4
Health status Measurements of morbidity and mortality (ie, time to dialysis, survival, all-cause mortality)
5 5
Symptoms Changes in overall symptoms (ie, pain, fatigue) 2 1
*Based on primary and distal outcomes from Grey et al.6
CKD, chronic kidney disease; QOL, quality of life.
on January 13, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2017-019814 on 22 March 2018. D
ownloaded from

7Donald M, et al. BMJ Open 2018;8:e019814. doi:10.1136/bmjopen-2017-019814
Open Access
Tab
le 4
S
umm
ary
of q
uant
itativ
e st
udie
sS
tud
y an
d
year
(Ref
eren
ce)
Des
ign
Targ
et p
op
ulat
ion
Stu
dy
size
Ag
e (y
ears
)In
terv
enti
on
top
ic(s
)P
rovi
der
(s)
Del
iver
y fo
rmat
Des
crip
tio
n o
f in
terv
enti
on
Stu
dy
out
com
esS
tud
y re
sult
s
RC
T
Bin
ik e
t al
(1
993)
34R
CT
Pre
-RR
T C
KD
(c
reat
inin
e>35
0 μm
ol/L
an
d r
isin
g ra
pid
ly)
204
(E=
87,
C=
92, n
ot p
art
of e
duc
atio
n=25
)A
ge: 5
0.2
►
Gen
eral
CK
D k
now
led
ge
►D
iet/
nutr
ition
►
Mod
aliti
es
Trai
ned
res
earc
h as
sist
ant
►
Prin
t
►Fa
ce t
o fa
ce
►P
ower
Poi
nt s
lides
‘Enh
ance
d e
duc
atio
n’:
►
22-p
age
boo
klet
►
Ind
ivid
ual s
lide
pre
sent
atio
n (7
5 m
in)
Dur
atio
n—on
e se
ssio
nC
omp
arat
or: s
tand
ard
car
e
Hea
lth s
tatu
s:
►D
urat
ion
bet
wee
n se
ssio
n an
d
dia
lysi
s in
itiat
ion—
pat
ient
in
E g
roup
sur
vive
d 4
.6 m
onth
s lo
nger
w/o
req
uirin
g R
RT
Gill
is e
t al
(1
995)
35R
CT
CK
D 3
–584
0(u
ncle
ar)
Age
: NR
►
Die
t/nu
triti
onD
ietic
ian
►
Prin
t
►Fa
ce t
o fa
ce‘M
odifi
catio
n of
die
t in
ren
al d
isea
se’:
►
‘Kee
pin
g Tr
ack’
boo
klet
►
Mon
thly
mee
ting
with
die
ticia
n
►P
rote
in W
ise
Cou
nter
(lis
ts p
rote
in c
onte
nt
of fo
ods)
►
‘Sho
pp
ing
Wis
e’: a
gui
de
to c
onve
nien
ce
and
fast
food
s
►V
isite
d r
esta
uran
ts a
nd s
hop
sD
urat
ion—
26 m
onth
sC
omp
arat
or: s
tand
ard
pro
tein
die
t
Cog
nitio
ns:
►
Pat
ient
rel
ianc
e on
die
ticia
n’s
feed
bac
k, s
upp
ort
and
m
odel
ling
stra
tegi
es—
dec
reas
ed o
ver
time
in
E g
roup
Ind
ivid
ual o
utco
mes
:
►To
p r
ated
inte
rven
tions
by
pat
ient
s—co
unse
lling
, sel
f-m
onito
ring,
pro
tein
cou
nter
Dev
ins
et a
l (2
003)
36
RC
TC
KD
(cre
atin
ine<
300
μmol
/L a
nd d
eem
ed t
one
ed R
RT
in
6–18
mon
ths)
297
(E=
149,
C=
148)
Age
: 58.
6
►
Gen
eral
CK
D k
now
led
ge
►D
iet/
nutr
ition
►
Med
icat
ion
►
Mod
aliti
es
►Li
fest
yles
Soc
ial w
orke
r
►P
rint
►
Face
to
face
►
Tele
pho
ne
‘Psy
choe
duc
atio
n’:
►
60-p
age
boo
klet
►
90 m
in in
tera
ctiv
e ed
ucat
iona
l int
erve
ntio
n p
erso
nalis
ed fo
r ea
ch p
atie
nt
►S
upp
ortiv
e (1
0 m
in m
ax) p
hone
cal
ls Q
3 w
eeks
Dur
atio
n—18
mon
ths
or in
itiat
ion
of R
RT
Com
par
ator
: sta
ndar
d c
are
Hea
lth s
tatu
s:
►Ti
me
to d
ialy
sis—
E g
roup
ha
d 3
mon
th d
elay
in d
ialy
sis
com
par
ed w
ith C
gro
up
Dev
ins
et a
l (2
005)
37
RC
TC
KD
with
pro
gres
sive
red
uctio
n in
kid
ney
func
tion
335
(E=
172,
C=
163)
Age
: 47.
4–53
.9
►
Gen
eral
CK
D K
now
led
ge
►D
iet/
nutr
ition
►
Mod
aliti
es
Hea
lth e
duc
ator
►
Prin
t
►Fa
ce t
o fa
ce
►P
ower
Poi
nt s
lides
‘Psy
choe
duc
atio
n se
ssio
n’:
►
22-p
age
boo
klet
►
Ind
ivid
ual s
lide
pre
sent
atio
n (6
0–75
min
long
)D
urat
ion—
one
visi
tC
omp
arat
or: s
tand
ard
car
e
Hea
lth s
tatu
s:
►S
urvi
val p
red
ialy
sis
and
aft
er
dia
lysi
s in
itiat
ion—
sign
ifica
ntly
lo
nger
in t
he E
gro
up
(2.2
5 ye
ars
and
8 m
onth
s,
resp
ectiv
ely)
Cam
pb
ell e
t al
(2
008)
38
RC
TC
KD
4–5
47 (E=
24,
C=
23)
Age
: 68.
5–72
.6
►
Die
t/nu
triti
on
►O
ther
(ie,
sel
f-m
anag
emen
t p
rinci
ple
s)
Die
ticia
n
►Fa
ce t
o fa
ce
►Te
lep
hone
‘Ind
ivid
ual n
utrit
iona
l cou
nsel
ling’
:
►In
itial
ind
ivid
ual c
onsu
ltatio
n w
ith d
ietic
ian
►
Then
pho
ne fo
llow
-up
Q2
wee
ks x
1 m
onth
th
en Q
1 m
onth
Dur
atio
n: 1
2 w
eeks
Com
par
ator
: sta
ndar
d c
are
Ind
ivid
ual o
utco
mes
:
►Q
OL—
man
y co
mp
onen
ts
of K
DQ
OLS
F V.
1.3
imp
rove
d: C
KD
sym
pto
ms,
co
gniti
ve fu
nctio
n, v
italit
y
Phy
siol
ogic
al m
easu
res:
►
Nut
ritio
nal a
sses
smen
t P
G-S
GA
—in
E g
roup
tho
se
who
wer
e m
alno
uris
hed
at
bas
elin
e im
pro
ved
, in
C g
roup
m
alno
uris
hed
from
12.
5%–2
5%
Byr
ne e
t al
(2
011)
26
RC
TC
KD
1–4
+H
TN81 (E
=40
,C
=41
)A
ge: 6
2.8–
65.4
►
Com
orb
iditi
es (i
e, H
TN
man
agem
ent)
Nur
se
►P
rint
►
Face
to
face
►
Tele
pho
ne
‘Str
uctu
red
ed
ucat
ion
sess
ion’
:
►Le
aflet
on
HTN
man
agem
ent
►
CH
EE
RS
pat
ient
ed
ucat
ion
inte
rven
tion
and
st
and
ard
car
e
►2.
5-ho
ur g
roup
ses
sion
►
Pho
ne s
upp
ort
from
nur
seD
urat
ion:
one
ses
sion
Com
par
ator
: sta
ndar
d c
are
Inte
rven
tion
spec
ific:
►
Feas
ibili
ty (r
ecru
itmen
t,
rete
ntio
n, p
atie
nt s
atis
fact
ion,
p
atie
nt a
cces
s of
ad
diti
onal
su
pp
ort)—
find
ings
sug
gest
d
eliv
erin
g/ev
alua
ting
an
effe
ctiv
e st
ruct
ured
gro
up
educ
atio
nal i
nter
vent
ion
to
pro
mot
e b
ette
r B
P c
ontr
ol
wou
ld b
e ch
alle
ngin
g
Con
tinue
d
on January 13, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2017-019814 on 22 March 2018. D
ownloaded from

8 Donald M, et al. BMJ Open 2018;8:e019814. doi:10.1136/bmjopen-2017-019814
Open Access
Stu
dy
and
ye
ar(R
efer
ence
)D
esig
nTa
rget
po
pul
atio
nS
tud
y si
zeA
ge
(yea
rs)
Inte
rven
tio
n to
pic
(s)
Pro
vid
er(s
)D
eliv
ery
form
atD
escr
ipti
on
of
inte
rven
tio
nS
tud
y o
utco
mes
Stu
dy
resu
lts
Che
n et
al
(201
1)39
RC
TC
KD
3–5
54 (E=
27,
C=
27)
Age
: 68.
2
►
Gen
eral
CK
D k
now
led
ge
►D
iet/
nutr
ition
►
Med
icat
ion
►
Life
styl
e
►M
odal
ity in
form
atio
n fo
r st
age
IV
Nur
se, d
ietic
ian,
ne
phr
olog
ist,
p
eers
, vol
unte
ers
►
Prin
t
►Fa
ce t
o fa
ce
►Te
lep
hone
‘Sel
f-m
anag
emen
t S
upp
ort’
:
►In
div
idua
l mon
thly
hea
lth e
duc
atio
n
►W
eekl
y te
lep
hone
bas
ed s
upp
ort
►
Aid
of s
upp
ort
grou
p t
wic
e m
onth
ly (5
–10
pat
ient
s)D
urat
ion:
12
mon
ths
Com
par
ator
: sta
ndar
d c
are
Phy
siol
ogic
al m
easu
res:
►
eGFR
cha
nge—
high
er in
E
grou
p
►eG
FR r
educ
tion
of >
50%
less
in
E g
roup
►
ES
RD
req
uirin
g R
RT
and
all-
caus
e m
orta
lity—
no s
igni
fican
t d
iffer
ence
bet
wee
n gr
oup
s
Hea
lth s
tatu
s:
►#
of h
osp
italis
atio
ns in
1 y
ear
of fo
llow
-up
—le
ss in
E g
roup
Fles
her
et a
l (2
011)
40R
CT
CK
D 3
–4+
HTN
40 (E=
23,
C=
17)
Age
: 63.
4
►
Die
t/nu
triti
on
►P
hysi
cal a
ctiv
ityN
urse
, exe
rcis
e p
hysi
olog
ist,
d
ietic
ian,
coo
k ed
ucat
or
►
Prin
t
►Fa
ce t
o fa
ce‘C
ooki
ng a
nd e
xerc
ise
clas
s’:
►
Sta
ndar
d c
are
and
:
►G
roup
CK
D n
utrit
ion
clas
s (w
ith d
ietic
ian
and
co
ok e
duc
ator
: 2 h
our
sess
ions
ove
r 4
wee
ks)
plu
s on
e sh
opp
ing
tour
led
by
a d
ietic
ian
►
CK
D c
ookb
ook
►
12-w
eek
exer
cise
pro
gram
me
(3 ×
1 h
our
sess
ions
/wee
k) le
d b
y a
cert
ified
exe
rcis
e p
hysi
olog
ist
and
nur
seD
urat
ion:
12
wee
ksC
omp
arat
or: s
tand
ard
car
e
Phy
siol
ogic
al m
easu
res:
►
Imp
rove
men
t in
4/5
of t
he
follo
win
g: u
rinar
y p
rote
in, t
otal
ch
oles
tero
l, eG
FR d
eclin
e,
BP,
urin
ary
sod
ium
—w
as
cons
ider
ed a
suc
cess
—61
% in
E
gro
up v
s 12
% in
C g
roup
Beh
avio
urs:
►
SM
sco
re—
som
e ch
ange
s in
som
e co
mp
onen
ts in
bot
h gr
oup
s
Job
oshi
et
al
(201
2)41
RC
TC
KD
31 (E=
19,
C=
12)
Age
: 69.
8
►
Oth
erN
urse
►
Face
to
face
►
Tele
pho
ne
►E
mai
l
‘EA
SE
(enc
oura
ge a
uton
omou
s se
lf-en
richm
ent)
pro
gram
me’
:
►N
urse
s lis
ten
to w
hat
pat
ient
s ha
ve d
ifficu
lties
an
d d
iscu
ss h
ow t
hey
will
try
to
imp
rove
►
Face
to
face
inte
rvie
w m
onth
ly
►Te
lep
hone
or
emai
l con
tact
eve
ry 2
wee
ksD
urat
ion:
12
wee
ksC
omp
arat
or: s
tand
ard
car
e
Cog
nitio
ns:
►
Sel
f-ef
ficac
y
Beh
avio
urs:
►
Med
icat
ion
adhe
renc
e
► A
dhe
renc
e to
BP
and
wei
ght
mea
sure
men
ts
►
Lim
iting
sal
t in
take
►
Alc
ohol
con
sum
ptio
n
► S
mok
ing
Phy
siol
ogic
al m
easu
res:
►
BP
Will
iam
s et
al
(201
2)42
RC
TC
KD
2–4
(dia
bet
icki
dne
y d
isea
se)+
DM
+H
TN
75 (E=
39,
C=
41)
Age
: 67
►
Med
icat
ion
►
Com
orb
iditi
esN
urse
►
Prin
t
►Fa
ce t
o fa
ce
►Te
lep
hone
►
DV
D
‘Mul
tifac
toria
l int
erve
ntio
n’:
►
Ind
ivid
ual m
edic
atio
n re
view
(dra
w c
hart
)
►D
aily
sel
f-m
onito
ring
of B
P ×
3 m
onth
s
►20
min
DV
D
►Q
2 w
eek
mot
ivat
iona
l int
ervi
ewin
g fo
llow
-up
via
pho
ne ×
12
wee
ks t
o su
pp
ort
BP
m
anag
emen
t an
d o
ptim
ise
med
icat
ion
SM
Dur
atio
n: 1
2 w
eeks
Com
par
ator
: sta
ndar
d c
are
Phy
siol
ogic
al m
easu
res:
►
BP
—no
diff
eren
ce b
etw
een
grou
ps
Beh
avio
urs:
►
Med
icat
ion
adhe
renc
e—no
d
iffer
ence
bet
wee
n gr
oup
s
Tab
le 4
C
ontin
ued
Con
tinue
d
on January 13, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2017-019814 on 22 March 2018. D
ownloaded from

9Donald M, et al. BMJ Open 2018;8:e019814. doi:10.1136/bmjopen-2017-019814
Open Access
Stu
dy
and
ye
ar(R
efer
ence
)D
esig
nTa
rget
po
pul
atio
nS
tud
y si
zeA
ge
(yea
rs)
Inte
rven
tio
n to
pic
(s)
Pro
vid
er(s
)D
eliv
ery
form
atD
escr
ipti
on
of
inte
rven
tio
nS
tud
y o
utco
mes
Stu
dy
resu
lts
Will
iam
s et
al
(201
2)43
RC
TC
KD
2–4
+D
M+
card
iova
scul
ar d
isea
se78 (E
=40
,C
=38
)A
ge: 7
4.31
►
Med
icat
ion
►
Com
orb
iditi
es
►O
ther
(ie,
sel
f-ef
ficac
y)
Nur
se, i
nter
pre
ter
►
Prin
t
►Fa
ce t
o fa
ce
►Te
lep
hone
►
Pow
erP
oint
slid
es
‘Sel
f-ef
ficac
y M
edic
atio
n In
terv
entio
n (S
EM
)’:
►In
div
idua
l med
icat
ion
revi
ew—
char
t in
Eng
lish
but
inte
rpre
ter
wro
te o
n m
edic
atio
n b
oxes
in
pat
ient
s la
ngua
ge o
r us
ed s
ymb
ols
►
Ind
ivid
ual s
lide
pre
sent
atio
n (2
0 m
in) v
ia
inte
rpre
ter
(Gre
ek, I
talia
n, V
ietn
ames
e)
►Q
2 w
eek
mot
ivat
iona
l int
ervi
ewin
g fo
llow
-up
vi
a p
hone
× 1
2 w
eeks
Dur
atio
n: 1
2 w
eeks
Com
par
ator
: sta
ndar
d c
are
Inte
rven
tion
spec
ific:
►
Att
ritio
n ra
te t
o as
sess
fe
asib
ility
of s
tud
y—hi
gh
attr
ition
Cog
nitio
ns:
►
Med
icat
ion
self-
effic
acy—
no
diff
eren
ce b
etw
een
grou
ps
Hea
lthca
re:
►
Hea
lth c
are
utili
zatio
n—no
d
iffer
ence
bet
wee
n gr
oup
s
Phy
siol
ogic
al m
easu
res:
►
Rou
tine
clin
ical
lab
sur
roga
te
mea
sure
s—no
diff
eren
ce
Beh
avio
urs:
►
Med
icat
ion
adhe
renc
e—no
d
iffer
ence
Ind
ivid
ual o
utco
mes
:
►G
ener
al w
ell-
bei
ng—
no
diff
eren
ce
de
Brit
o-A
shur
st e
t al
(2
013)
44
RC
TC
KD
3–5
+H
TN
(BP
>13
0/80
)+
Ben
gali
pop
ulat
ion
56 (E=
28,
C=
28)
Age
: 55.
7–60
.7
►
Die
t/nu
triti
onD
ietic
ian
and
B
enga
li w
orke
r
►Fa
ce t
o fa
ce
►Te
lep
hone
‘Die
t ad
vice
’:
►P
ract
ical
coo
king
and
ed
ucat
ion
sess
ions
in
the
com
mun
ity fa
cilit
ated
by
a B
enga
li w
orke
r
►Fo
llow
ed b
y Q
2 w
eek
pho
ne c
alls
to
rein
forc
e ad
vice
and
set
new
tar
gets
Dur
atio
n: 6
mon
ths
Com
par
ator
: sta
ndar
d c
are
Phy
siol
ogic
al m
easu
res:
►
BP
—d
ecre
ased
by
8 m
m H
g in
E g
roup
►
24 h
ours
urin
ary
salt
excr
etio
n—d
ecre
ase
in E
gr
oup
►
eGFR
—no
diff
eren
ce b
etw
een
grou
ps
Pae
s-B
arre
to
et a
l (20
13)45
RC
TC
KD
3–5
89 (E=
43,
C=
46)
Age
: 63.
4
►
Die
t/nu
triti
onD
ietic
ian
►
Prin
t
►Fa
ce t
o fa
ce
►Te
lep
hone
‘Nut
ritio
n ed
ucat
ion
pro
gram
me’
:
►S
tand
ard
die
tary
cou
nsel
ling
AN
D
►E
duc
atio
n fo
lder
with
rec
ipes
to
rep
lace
sal
t w
ith s
odiu
m fr
ee s
easo
ning
ble
nds
►
Ind
ivid
ual 1
5–20
min
cla
ss
►H
and
s on
ses
sion
ab
out
pro
tein
ric
h fo
od
►H
and
s on
ses
sion
usi
ng t
est
tub
es w
ith t
he
amou
nt o
f sal
t in
diff
eren
t fo
ods
►
4 m
onth
ly fo
llow
-up
vis
its
►Te
lep
hone
cal
l to
add
ress
any
dou
bts
with
d
ieta
ry p
lan
Dur
atio
n: 4
–7 m
onth
sC
omp
arat
or: s
tand
ard
car
e
Beh
avio
urs:
►
Red
uctio
n in
pro
tein
inta
ke—
dec
reas
ed
►A
dhe
renc
e to
low
pro
tein
d
iet—
effe
ctiv
e
Phy
siol
ogic
al m
easu
res:
►
Bod
y co
mp
ositi
on: w
aist
ci
rcum
fere
nce,
bod
y fa
t,
BM
I, m
id-a
rm m
uscl
e ci
rcum
fere
nce—
no c
hang
e
► S
erum
alb
umin
—no
cha
nge
Bla
kem
an e
t al
(2
014)
46
RC
TC
KD
343
6(E
=21
5,C
=22
1)A
ge: 7
2.1
►
Gen
eral
CK
D k
now
led
ge
►C
omor
bid
ities
►
Oth
er (i
e, c
omm
unity
re
sour
ces
Lay
heal
th w
orke
r
►P
rint
►
Web
site
►
Tele
pho
ne
‘Info
rmat
ion
and
tel
epho
ne-g
uid
ed a
cces
s to
co
mm
unity
ser
vice
s’:
►
Kid
ney
Info
rmat
ion
Gui
deb
ook
►
Pat
ient
-Led
Ass
essm
ent
for
Net
wor
k S
upp
ort
‘PLA
NS
’ boo
klet
and
inte
ract
ive
web
site
—ta
ilore
d a
cces
s to
com
mun
ity r
esou
rces
►
Tele
pho
ne g
uid
ed h
elp
from
a la
y he
alth
w
orke
rD
urat
ion:
6 m
onth
sC
omp
arat
or: s
tand
ard
car
e
Cog
nitio
ns:
►
Pos
itive
and
act
ive
enga
gem
ent
in li
fe (h
eiQ
)—no
d
iffer
ence
bet
wee
n gr
oup
s
Phy
siol
ogic
al m
easu
res:
►
BP
con
trol
—b
ette
r B
P
mai
nten
ance
in E
gro
up
Ind
ivid
ual o
utco
mes
:
►H
ealth
rel
ated
QO
L (E
uroQ
oL
EQ
-5D
ind
ex)—
high
er in
E
grou
p
Tab
le 4
C
ontin
ued
Con
tinue
d
on January 13, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2017-019814 on 22 March 2018. D
ownloaded from

10 Donald M, et al. BMJ Open 2018;8:e019814. doi:10.1136/bmjopen-2017-019814
Open Access
Stu
dy
and
ye
ar(R
efer
ence
)D
esig
nTa
rget
po
pul
atio
nS
tud
y si
zeA
ge
(yea
rs)
Inte
rven
tio
n to
pic
(s)
Pro
vid
er(s
)D
eliv
ery
form
atD
escr
ipti
on
of
inte
rven
tio
nS
tud
y o
utco
mes
Stu
dy
resu
lts
McM
anus
et
al
(201
4)47
RC
TH
TN (B
P>
130/
80)
+C
KD
3 or
DM
or
CH
D55
5(E
=27
7,C
=27
8)A
ge: 6
9.3–
69.6
►
Med
icat
ion
►
Com
orb
iditi
esG
ener
al
pra
ctiti
oner
, p
atie
nt
►
Prin
t
►Fa
ce t
o fa
ce‘S
elf-
mon
itorin
g of
BP
and
sel
f-tit
ratio
n of
m
edic
atio
ns’:
►
Sel
f-m
onito
ring
of B
P
►S
elf-
titra
tion
of m
edic
atio
ns fo
llow
ing
a 3-
step
p
lan
des
igne
d b
y ge
nera
l pra
ctiti
oner
and
p
atie
ntD
urat
ion:
12
mon
ths
Com
par
ator
: sta
ndar
d c
are
Phy
siol
ogic
al m
easu
res:
►
SB
P a
t 12
mon
ths—
no
diff
eren
ce
Hea
lthca
re:
►
Pre
scrip
tion
of
antih
yper
tens
ive
med
icat
ions
in
crea
sed
in b
oth
grou
ps
but
gr
eate
r si
gnifi
canc
e in
E g
roup
Sym
pto
m m
gmt.
:
►A
dve
rse
effe
cts—
no
sign
ifica
nt d
iffer
ence
bet
wee
n gr
oup
s
►
Ind
ivid
ual o
utco
mes
:
►Q
OL—
no s
igni
fican
t d
iffer
ence
b
etw
een
grou
ps
Par
k et
al
(201
4)48
RC
TC
KD
3+H
TN+
Afr
ican
-Am
eric
an15 A
ge: 5
8.7
►
Oth
er (i
e, m
edita
tion)
Prin
cip
le
inve
stig
ator
, p
atie
nt
►
Face
to
face
►
Aud
io r
ecor
din
g‘M
ind
fuln
ess
med
itatio
n (M
M)’
►
14 m
in o
f pre
reco
rded
gui
ded
MM
usi
ng M
P3
pla
yer
and
hea
dp
hone
sD
urat
ion:
one
ses
sion
Com
par
ator
: BP
ed
ucat
ion
Phy
siol
ogic
al m
easu
res:
►
BP
—d
ecre
ase
in S
BP
/D
BP
/ HR
/ M
AP
►
Mus
cle
sym
pat
hetic
ner
ve
activ
ity—
dec
reas
ed
How
den
et
al
(201
5)49
RC
TC
KD
3–4
and
>
1 un
cont
rolle
dca
rdio
vasc
ular
ris
k fa
ctor
72 (E=
36,
C=
36)
Age
60.
2–62
.0
►
Phy
sica
l act
ivity
Nur
se p
ract
ition
er,
soci
al w
orke
r, ex
erci
se
phy
siol
ogis
t,
die
ticia
n,
psy
chol
ogis
t,
dia
bet
es e
duc
ator
►
Prin
t
►Fa
ce t
o fa
ce‘E
xerc
ise
trai
ning
and
life
styl
e in
terv
entio
n’:
►
Sta
ndar
d c
are
AN
D
►D
etai
led
med
ical
/sur
gica
l his
tory
tak
en b
y nu
rse
pra
ctiti
oner
►
Ed
ucat
ion
abou
t ex
erci
sing
saf
ely:
m
aint
aini
ng h
ydra
tion,
sig
ns/s
ymp
tom
s of
ab
norm
al r
esp
onse
to
exer
cise
►
If d
iab
etic
—ed
ucat
ion
on h
ypog
lyca
emia
►
Exe
rcis
e p
resc
riptio
n in
div
idua
lised
on
pat
ient
’s c
omor
bid
con
diti
ons
►
Goa
l=15
0 m
in/w
eek
of m
oder
ate
inte
nsity
ex
erci
se p
lus
resi
stan
ce t
rain
ing
►
8 w
eeks
sup
ervi
sed
, the
n 10
mon
th h
ome
bas
ed
►P
atie
nts
got:
exe
rcis
e b
all,
resi
stan
ce t
rain
ing
boo
klet
►
Pat
ient
s co
ntac
ted
reg
ular
ly t
o m
onito
r ad
here
nce
to t
rain
ing
Dur
atio
n: 1
2 m
onth
sC
omp
arat
or: s
tand
ard
car
e
Phy
siol
ogic
al m
easu
res:
►
ME
TS—
imp
rove
d
►6
min
wal
k d
ista
nce—
imp
rove
d
►B
MI—
imp
rove
d
Leeh
ey e
t al
(2
016)
50
RC
TC
KD
2–
4+D
M2+
BM
I>30
+p
ersi
sten
t p
rote
inur
ia
36 (Exe
rcis
e+d
iet
= 1
8,D
iet=
18)
Age
: 66
►
Die
t/nu
triti
on
►P
hysi
cal a
ctiv
ityP
erso
nal t
rain
er
►Fa
ce t
o fa
ce
►Te
lep
hone
‘Str
uctu
red
exe
rcis
e p
rogr
amm
e’:
►
Die
tary
cou
nsel
ling=
bas
elin
e nu
triti
onal
co
unse
lling
with
nin
e fo
llow
-up
pho
ne c
alls
(b
oth
grou
ps)
AN
D
►S
uper
vise
d e
xerc
ise
pro
gram
me
3× w
eek
(60
min
car
dio
plu
s 25
–30
min
res
ista
nce
trai
ning
)
►Fo
llow
ed b
y ho
me
exer
cise
pha
se: 3
×/w
eek
×
60 m
in w
ith w
eekl
y fo
llow
-up
pho
ne c
alls
and
p
atie
nt e
ncou
rage
d t
o m
eet
trai
ner
Q1
mon
thD
urat
ion:
12
mon
ths
Com
par
ator
: die
t co
unse
lling
onl
y
Phy
siol
ogic
al m
easu
res:
►
Urin
e p
rote
in t
o cr
eatin
ine
ratio
—no
cha
nge
at 5
2 w
eeks
►
Sym
pto
m li
mite
d a
nd
cons
tant
wor
k ra
te t
read
mill
tim
e—si
gnifi
cant
incr
ease
in
die
t+ex
erci
se g
roup
at
12 b
ut
not
52 w
eeks
►
Urin
e al
bum
in t
o cr
eatin
ine
ratio
—no
cha
nge
►
eGFR
—no
cha
nge
►
Infla
mm
atio
n—no
cha
nge
►
End
othe
lial f
unct
ion—
no
chan
ge
►B
ody
com
pos
ition
—no
cha
nge
Tab
le 4
C
ontin
ued
Con
tinue
d
on January 13, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2017-019814 on 22 March 2018. D
ownloaded from

11Donald M, et al. BMJ Open 2018;8:e019814. doi:10.1136/bmjopen-2017-019814
Open Access
Stu
dy
and
ye
ar(R
efer
ence
)D
esig
nTa
rget
po
pul
atio
nS
tud
y si
zeA
ge
(yea
rs)
Inte
rven
tio
n to
pic
(s)
Pro
vid
er(s
)D
eliv
ery
form
atD
escr
ipti
on
of
inte
rven
tio
nS
tud
y o
utco
mes
Stu
dy
resu
lts
Mon
toya
et
al
(201
6)30
RC
TC
KD
430 (E
=16
,C
=14
)A
ge: 6
7.9–
68.3
►
Gen
eral
CK
D k
now
led
ge
►D
iet/
nutr
ition
►
Med
icat
ion
►
Mod
aliti
es
►O
ther
(ie,
put
ting
affa
irs in
or
der
)
Nep
hrol
ogis
t,
nurs
e p
ract
ition
er,
die
ticia
n, s
ocia
l w
orke
r
►
Prin
t
►Fa
ce t
o fa
ce
►P
ower
Poi
nt s
lides
‘Nur
se p
ract
ition
er fa
cilit
ated
CK
D g
roup
vis
it’:
►
Bin
der
with
sec
tion
on in
div
idua
l lab
s, a
noth
er
sect
ion
for
top
ics
of g
roup
s vi
sits
►
Six
1.5
–2-h
our
long
mon
thly
gro
up v
isits
of 8
p
atie
nts
(~1/
2 ha
d fa
mily
mem
ber
s w
ith t
hem
)
►Th
ree
visi
ts d
one
in c
onju
nctio
n w
ith
nep
hrol
ogis
t’s e
xam
inat
ions
(firs
t ha
lf=ap
t,
seco
nd h
alf=
educ
atio
n)
►th
ree
visi
ts=
educ
atio
n on
ly
►In
tera
ctiv
e d
iscu
ssio
n at
eac
h vi
sit
►
Slid
e p
rese
ntat
ion
(30–
45 m
in)
Dur
atio
n: 9
mon
ths
Com
par
ator
: sta
ndar
d c
are
Cog
nitio
ns:
►
CK
D k
now
led
ge—
imp
rove
d in
b
oth
grou
ps
►
Sel
f-ef
ficac
y/d
isea
se S
M—
upw
ard
tre
nd in
E g
roup
Ind
ivid
ual o
utco
mes
:
►S
atis
fact
ion—
high
Non
-RC
T
Rob
inso
n et
al
(198
8)51
Ob
sC
KD
25 Age
: NR
►
Gen
eral
CK
D k
now
led
ge
►D
iet/
nutr
ition
►
Med
icat
ion
►
Oth
er (i
e, s
elf-
care
act
iviti
es
►M
odal
ities
NR
►
Face
to
face
‘Ren
al B
ingo
’:
►B
ingo
gam
e fo
rmat
/gro
up g
amin
g te
chni
que
►
Pro
visi
on o
f ref
resh
men
ts &
priz
es fo
r m
otiv
atio
n
►R
efre
shm
ents
mad
e w
ith d
ietic
ian
cons
ulta
tion,
rei
nfor
ced
die
tary
reg
imen
Dur
atio
n: o
ne s
essi
onC
omp
arat
or: n
one
Cog
nitio
ns:
►
Info
rmat
ion
was
gai
ned
or
rein
forc
ed—
des
irab
le o
utco
me
►
Met
a v
arie
ty o
f lea
rnin
g ne
eds—
des
irab
le o
utco
me
Inte
rven
tion
spec
ific:
►
Par
ticip
atio
n w
as e
njoy
ed—
des
irab
le o
utco
me
►
Inte
rest
exp
ress
ed fo
r re
pea
ting
the
exer
cise
—d
esira
ble
out
com
e
Kla
ng e
t al
(1
998)
52
QE
CK
D 4
–556 (E
=28
,C
=28
)A
ge: 5
4–58
►
Gen
eral
CK
D k
now
led
ge
►D
iet/
nutr
ition
►
Phy
sica
l act
ivity
►
Mod
aliti
es
►O
ther
(ie,
psy
chos
ocia
l—im
pac
t of
CK
D o
n ec
onom
y,
fam
ily a
nd s
ocia
l life
)
Nur
se, p
hysi
cian
, so
cial
wor
ker,
die
ticia
n,
phy
siot
hera
pis
t
►
Face
to
face
‘Pre
-dia
lysi
s p
atie
nt e
duc
atio
n’:
►
Four
2-h
our
sess
ions
of g
roup
tea
chin
g w
ith a
cl
assr
oom
ap
pro
ach
►
Ind
ivid
ual s
upp
ort
follo
w-u
p b
y ne
phr
olog
y te
am m
emb
erD
urat
ion:
four
ses
sion
sC
omp
arat
or: s
tand
ard
car
e
Ind
ivid
ual o
utco
mes
:
►Fu
nctio
nal a
nd e
mot
iona
l wel
l-b
eing
—b
ette
r in
E g
roup
*
Cup
isiti
et
al
(200
2)53
PP
CK
D 3
b-5
20 Age
: NR
►
Die
t/nu
triti
onN
R
►P
rint
‘Veg
etar
ian
die
t’:
►
Alte
rnat
e b
etw
een
anim
al b
ased
con
vent
iona
l lo
w p
rote
in d
iet
and
a v
eget
able
-bas
ed lo
w-
pro
tein
die
t
►B
ookl
ets
exp
lain
ing
gene
ral g
uid
elin
es a
nd
feat
ures
of t
he d
iet
Dur
atio
n: o
ne s
essi
onC
omp
arat
or: c
onve
ntio
nal p
rote
in d
iet
Ind
ivid
ual o
utco
mes
:
►O
pin
ions
on
die
t—90
%
enjo
yed
Phy
siol
ogic
al m
easu
res:
►
Cre
atin
ine—
no c
hang
e
►A
lbum
in—
no c
hang
e
►To
tal p
rote
in—
no c
hang
e
► L
ipid
s—d
ecre
ased
► E
lect
roly
tes—
no c
hang
e
►H
aem
atoc
rit—
no c
hang
e
► U
rinar
y p
rote
in e
xcre
tion—
d
ecre
ased
►U
rinar
y ur
ea e
xcre
tion—
dec
reas
ed
►
Bod
y w
eigh
t—no
cha
nge
Tab
le 4
C
ontin
ued
Con
tinue
d
on January 13, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2017-019814 on 22 March 2018. D
ownloaded from

12 Donald M, et al. BMJ Open 2018;8:e019814. doi:10.1136/bmjopen-2017-019814
Open Access
Stu
dy
and
ye
ar(R
efer
ence
)D
esig
nTa
rget
po
pul
atio
nS
tud
y si
zeA
ge
(yea
rs)
Inte
rven
tio
n to
pic
(s)
Pro
vid
er(s
)D
eliv
ery
form
atD
escr
ipti
on
of
inte
rven
tio
nS
tud
y o
utco
mes
Stu
dy
resu
lts
Gut
iérr
ez
Vila
pla
na e
t al
(2
007)
57
PP
CK
D24 A
ge: 6
4.5
►
Gen
eral
CK
D k
now
led
ge
►D
iet/
nutr
ition
►
Mod
aliti
es
►O
ther
Nur
se, p
atie
nt
volu
ntee
rs
►P
rint
►
Face
to
face
►
Pow
erP
oint
slid
es
‘Ed
ucat
ion
Inte
rven
tion’
►
Eig
ht 2
-hou
r cl
asse
s
►D
idac
tic a
nd d
iscu
ssio
nD
urat
ion:
6 m
onth
sC
omp
arat
or: n
one
Cog
nitio
ns:
►
Imp
rove
men
t in
kno
wle
dge
of
CK
D
Beh
avio
urs:
►
Mod
ified
life
styl
e, d
iet
Inte
rven
tion
spec
ific:
►
Red
uctio
n of
str
ess,
fear
►Im
pro
vem
ent
in t
hera
peu
tic
rela
tions
hip
s w
ith h
ealth
care
p
rovi
der
s, c
omp
anio
ns a
nd
mul
ti- d
isci
plin
ary
team
.
Pag
els
et a
l (2
008)
55
Ob
sC
KD
58 Age
: 65
►
Gen
eral
CK
D k
now
led
geN
urse
►
Prin
t
►A
dia
ry t
o p
rom
ote
dis
ease
rel
ated
kn
owle
dge
, inv
olve
men
t an
d s
elf-
care
ab
ility
an
d t
o p
rom
ote
coop
erat
ion
bet
wee
n p
atie
nt
and
nur
seD
urat
ion:
12
mon
ths
Com
par
ator
: non
e
Cog
nitio
ns:
►
Par
ticip
atio
n, s
elf-
care
and
d
isea
se r
elat
ed k
now
led
ge
Inte
rven
tion
spec
ific:
►
Use
of d
iary
►
Sui
tab
ility
for
teac
hing
p
urp
oses
Yen
et a
l (2
008)
56P
PC
KD
366 A
ge: 6
7.4
►
Gen
eral
CK
D k
now
led
ge
►D
iet/
nutr
ition
►
Phy
sica
l act
ivity
►
Med
icat
ion
Nep
hrol
ogis
t,
nurs
e, d
ietic
ian,
so
cial
wor
ker
►
Prin
t
►Fa
ce t
o fa
ce
►Te
lep
hone
‘Ed
ucat
iona
l int
erve
ntio
n’:
►
Han
dou
ts
►O
ne 1
50 m
in w
orks
hop
►
Ind
ivid
ual c
onsu
lts Q
6 m
onth
with
nur
se
►P
hone
num
ber
pro
vid
ed t
o p
artic
ipan
ts fo
r q
uest
ions
►
Des
sert
s re
com
men
ded
by
die
ticia
n gi
ven
at
wor
ksho
p fo
r ed
ucat
iona
l pur
pos
es, l
unch
b
oxes
des
igne
d b
y d
ietic
ian
give
n ou
t at
the
en
d o
f the
wor
ksho
pD
urat
ion:
12
mon
ths
Com
par
ator
: non
e
Cog
nitio
ns:
►
QO
L (W
HO
QO
L-B
RE
F Ta
iwan
ve
rsio
n)—
glob
al in
crea
se
►K
now
led
ge o
f ren
al fu
nctio
n p
rote
ctio
n (c
heck
list
mad
e b
y in
vest
igat
ors)
—no
cha
nge
Phy
siol
ogic
al m
easu
res:
►
Cre
atin
ine—
no c
hang
e
► B
UN
—no
cha
nge
►
GFR
—no
cha
nge
►
Bod
y w
eigh
t—no
cha
nge
►
Mus
cle
wei
ght—
no c
hang
e
►%
Bod
y fa
t—no
cha
nge
►
Wai
st-t
o-hi
p r
atio
— s
igni
fican
t d
ecre
ase
in E
gro
up
►
BM
I—si
gnifi
cant
dec
reas
e in
E
gro
up
►
BP
—no
cha
nge
Gut
iérr
ez-
Vila
pla
na e
t al
(2
009)
54
PP
CK
D 4
–541 A
ge: 6
0.56
►
Gen
eral
CK
D k
now
led
ge
►D
iet/
nutr
ition
►
Phy
sica
l act
ivity
►
Mod
aliti
es
►O
ther
(ie,
psy
chos
ocia
l—im
pac
t of
CK
D fa
mily
, fin
ance
s, s
ocia
l life
)
Nur
se, p
hysi
cian
, te
chni
cian
, thr
ee
exp
ert
pat
ient
s
►
Prin
t
►Fa
ce t
o fa
ce‘T
each
ing
grou
p’:
►
Six
2-h
our
mon
thly
gro
up e
duc
atio
n se
ssio
ns
►B
ookl
et fo
r fu
ture
ref
eren
ceD
urat
ion:
6 m
onth
sC
omp
arat
or: n
one
Cog
nitio
ns:
►
Anx
iety
—d
ecre
ased
►
Fear
—m
ore
cont
rol o
f fea
r re
spon
se
►S
tres
s—d
ecre
ased
Wu
et a
l (2
009)
58
QE
CK
D 3
–557
3(E
=28
7,C
ohor
t=28
6)A
ge: 6
3.4
►
Gen
eral
CK
D k
now
led
ge
►D
iet/
nutr
ition
►
Med
icat
ion
►
Life
styl
e
Nur
se, s
ocia
l w
orke
r, d
ietic
ian,
H
D/P
D p
atie
nt
volu
ntee
rs,
phy
sici
ans
►
Face
to
face
‘Mul
tidis
cip
linar
y p
red
ialy
sis
educ
atio
n (M
PE
)’:
►In
div
idua
l lec
ture
s, c
onte
nt-b
ased
on
CK
D
stag
e
►D
ieta
ry c
ouns
ellin
g b
iann
ually
Dur
atio
n: 1
2 m
onth
sC
omp
arat
or: s
tand
ard
car
e
Hea
lth s
tatu
s:
►E
SR
D w
arra
ntin
g R
RT—
13.9
%
in E
gro
up v
s 43
% in
C g
roup
►
All
caus
e m
orta
lity—
1.7%
in E
gr
oup
vs
10.1
% in
C g
roup
Hea
lthca
re:
►
Hos
pita
lisat
ion—
2.8%
E g
roup
ve
rsus
16.
4% in
C g
roup
Tab
le 4
C
ontin
ued
Con
tinue
d
on January 13, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2017-019814 on 22 March 2018. D
ownloaded from

13Donald M, et al. BMJ Open 2018;8:e019814. doi:10.1136/bmjopen-2017-019814
Open Access
Stu
dy
and
ye
ar(R
efer
ence
)D
esig
nTa
rget
po
pul
atio
nS
tud
y si
zeA
ge
(yea
rs)
Inte
rven
tio
n to
pic
(s)
Pro
vid
er(s
)D
eliv
ery
form
atD
escr
ipti
on
of
inte
rven
tio
nS
tud
y o
utco
mes
Stu
dy
resu
lts
Wie
rdsm
a et
al
(201
1)59
QE
CK
D54 (E
=28
,C
=26
)A
ge: 5
5–59
►
Med
icat
ion
Nur
se p
ract
ition
er
►Fa
ce t
o fa
ce
►P
rint
‘Mot
ivat
iona
l int
ervi
ewin
g’:
►
Cou
nsel
ling
by
nurs
e p
ract
ition
er (i
n ad
diti
on
to c
are
by
nep
hrol
ogis
t) us
ing
mot
ivat
iona
l in
terv
iew
ing
►
Usi
ng t
he ‘L
ong-
Term
Med
icat
ion
Beh
avio
ur
Sel
f-E
ffica
cy S
cale
(LTM
BS
ES
)’—ar
eas
with
sc
ore<
5 w
ere
iden
tified
and
the
n up
to
five
area
s (p
icke
d b
y p
atie
nt) w
ere
dis
cuss
ed a
nd
solu
tions
and
goa
ls w
ere
set
Dur
atio
n: 6
mon
ths
Com
par
ator
: sta
ndar
d c
are
Cog
nitio
ns:
►
LTM
BS
ES
—d
iffer
ence
in m
ean
self-
effic
acy
scor
e at
pos
t-te
st
Agu
ilera
Flo
rez
et a
l (20
12)60
Ob
sC
KD
19 Age
: 58
►
Gen
eral
CK
D k
now
led
ge
►D
iet/
nutr
ition
►
Med
icat
ion
►
Sym
pto
m m
anag
emen
t
►P
hysi
cal a
ctiv
ity
►M
odal
ities
►
Oth
er
Nur
se,
phy
siot
hera
pis
t,
die
ticia
n,
pha
rmac
ist,
p
sych
olog
ist,
co
ord
inat
ors,
ne
phr
olog
ist,
p
atie
nt m
ento
rs
►
Face
to
face
‘Esc
uela
ER
CA’
:
►7
1.5
hour
mul
tidis
cip
linar
y gr
oup
ed
ucat
ion
sess
ions
hel
d b
iwee
kly
►
Up
to
10 p
atie
nts
per
gro
up w
ith fa
mily
m
emb
ers
►
Did
actic
plu
s d
iscu
ssio
n fo
rmat
Dur
atio
n: n
ot r
epor
ted
Com
par
ator
: non
e
Cog
nitio
ns:
►
Kno
wle
dge
►
Anx
iety
—in
crea
sed
Ind
ivid
ual o
utco
mes
:
►S
atis
fact
ion
in g
roup
the
rap
y
Cho
i et
al
(201
2)61
QE
CK
D 1
–561 (E
=31
,C
=30
)A
ge: 5
3.93
–58.
33
►
Gen
eral
CK
D k
now
led
ge
►D
iet/
nutr
ition
►
Mod
aliti
es
►O
ther
(ie,
und
erst
and
ing
and
co
mp
lianc
e w
ith S
M)
Phy
sici
an, n
urse
, d
ietic
ian
►
Face
to
face
►
Pow
erP
oint
slid
es‘F
ace-
to-f
ace
SM
pro
gram
me’
:
►90
min
lect
ure
with
slid
es (3
–5 p
eop
le/g
roup
)
►20
min
ind
ivid
ual c
onsu
lt
►1
wee
k la
ter
ind
ivid
ual r
einf
orce
men
t ed
ucat
ion
and
con
sulta
tion
Dur
atio
n: t
wo
sess
ions
Com
par
ator
: gen
eral
mai
nten
ance
Cog
nitio
ns:
►
Kno
wle
dge
of C
KD
sca
le—
incr
ease
>in
E g
roup
Beh
avio
urs:
►
Sel
f-ca
re p
ract
ice
scal
e fo
r p
atie
nts
with
CK
D—
no
diff
eren
ce b
etw
een
E g
roup
an
d C
gro
up b
ut d
id in
crea
se
over
tim
e fo
r b
oth
grou
ps
Phy
siol
ogic
al m
easu
res:
►
BU
N/C
reat
inin
e—no
cha
nge
►
Na/
K—
no c
hang
e
► C
a/P
O4—
no c
hang
e
► H
aem
oglo
bin
—no
cha
nge
►
GFR
—no
cha
nge
Kao
et
al
(201
2)27
QE
CK
D 1
–494 (E
=45
,C
=49
)A
ge: 7
3.17
►
Gen
eral
CK
D k
now
led
ge
►P
hysi
cal a
ctiv
ityIn
stru
ctor
►
Prin
t
►Fa
ce t
o fa
ce
►Te
lep
hone
‘Exe
rcis
e ed
ucat
ion
inte
rven
tion’
:
►M
anua
l
►1.
5-ho
ur e
xerc
ise/
heal
th e
duc
atio
n co
urse
►
Dra
fted
exe
rcis
e co
ntra
ct a
nd e
xerc
ise
pro
gram
mes
►
Follo
w-u
p p
hone
cal
ls
►1x
/mon
th fo
r p
atie
nts
in m
aint
enan
ce p
hase
►
2×/m
onth
for
pat
ient
s in
act
ion/
pre
p s
tage
s
►4×
/mon
th fo
r p
atie
nts
at p
reco
ntem
pla
tion/
cont
emp
latio
n st
ages
►
Goa
l: w
orko
ut 3
–5×
/wee
k ×
30
min
for
3 m
onth
sD
urat
ion:
4 m
onth
sC
omp
arat
or: s
tand
ard
car
e
Beh
avio
urs:
►
Exe
rcis
e b
ehav
iour
—im
pro
ved
in
E g
roup
Cog
nitio
ns:
►
Dep
ress
ion—
scor
e d
ecre
ased
(ie
, im
pro
ved
) in
E g
roup
Sym
pto
m m
anag
emen
t:
►Fa
tigue
—sc
ore
dec
reas
ed in
E
gro
up
Tab
le 4
C
ontin
ued
Con
tinue
d
on January 13, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2017-019814 on 22 March 2018. D
ownloaded from

14 Donald M, et al. BMJ Open 2018;8:e019814. doi:10.1136/bmjopen-2017-019814
Open Access
Stu
dy
and
ye
ar(R
efer
ence
)D
esig
nTa
rget
po
pul
atio
nS
tud
y si
zeA
ge
(yea
rs)
Inte
rven
tio
n to
pic
(s)
Pro
vid
er(s
)D
eliv
ery
form
atD
escr
ipti
on
of
inte
rven
tio
nS
tud
y o
utco
mes
Stu
dy
resu
lts
Dia
man
tidis
et
al (
2013
)62P
PC
KD
3–5
108
Age
: 64
►
Die
t/nu
triti
on
►M
edic
atio
nO
nlin
e to
ol
►W
ebsi
te‘D
isea
se-s
pec
ific
safe
ty in
form
atio
n’:
►
Saf
e ki
dne
y ca
re w
ebsi
te—
pat
ient
/fam
ily
mem
ber
and
pro
vid
er p
orta
ls
►E
duc
atio
n m
odul
es d
isp
laye
d in
circ
ular
d
istr
ibut
ion
to a
void
prio
ritis
atio
n of
top
ics
Dur
atio
n: n
ot a
pp
licab
leC
omp
arat
or: n
one
Inte
rven
tion
spec
ific:
►
Firs
t en
try
into
web
site
-<
30%
of p
artic
ipan
ts e
nter
ed
with
in 3
65 d
ays
(tota
l fol
low
-up
p
erio
d)
►
Ave
rage
dw
ell t
ime
on t
he
web
site
—7
min
►
Mod
ules
wer
e ra
nked
by
freq
uenc
y of
sel
ectio
n—Th
e th
ree
mos
t fr
eque
ntly
vis
ited
p
ages
wer
e ‘R
enal
func
tion
calc
ulat
or’,
‘Pill
s to
avo
id’ a
nd
‘Foo
ds
to a
void
’
Kaz
awa
et
al
(201
3)31
PP
CK
D 3
–4 (d
iab
etic
ne
phr
opat
hy)
30 Age
: 67
►
Die
t/nu
triti
on
►M
edic
atio
ns
►P
hysi
cal a
ctiv
ity
►C
omor
bid
ities
►
Oth
er (i
e, s
tres
s m
anag
emen
t, id
entif
y su
pp
orte
rs (f
amily
) & h
ow
they
can
con
trib
ute,
goa
l se
ttin
g)
Nur
se
►P
rint
►
Face
to
face
►
Tele
pho
ne
►E
mai
l
‘SM
ski
lls p
rogr
amm
e’:
►
Text
boo
k
►D
aily
jour
nal
►
Four
1 h
our
face
-to-
face
ses
sion
s Q
2 w
eeks
at
out
pat
ient
clin
ic o
r in
hom
e
►Tw
o 30
min
pho
ne o
r em
ail s
essi
ons
Q1
mon
th
►Th
en Q
1 m
onth
pho
ne c
alls
Dur
atio
n: 6
mon
ths
Com
par
ator
: non
e
Ind
ivid
ual o
utco
mes
:
►Q
OL—
self-
effic
acy
and
SM
b
ehav
iour
s im
pro
ved
Phy
siol
ogic
al m
easu
res:
►
Ren
al fu
nctio
n—no
cha
nge
►
Hae
mog
lob
in A
1c—
dec
reas
ed
pos
tinte
rven
tion
Lin
et
al
(201
3)63
PP
CK
D 1
-3a
37 Age
67.
42
►O
ther
(ie,
sel
f-re
gula
tion/
self
man
agem
ent
top
ics)
Nur
se
►P
rint
►
Face
to
face
►
Vid
eo
‘SM
pro
gram
me’
:
►S
elf-
mon
itorin
g w
orkb
ook
►
5 w
eek
SM
pro
gram
me
►
Wee
kly
90 m
in fa
ce-
to-f
ace
grou
p s
essi
ons
(6–8
pat
ient
s)
►C
KD
SM
vid
eo a
bou
t se
lf-re
gula
tion
Dur
atio
n: 5
wee
ksC
omp
arat
or: n
one
Cog
nitio
ns:
►
CK
D s
elf-
effic
acy—
incr
ease
d
Beh
avio
urs:
►
CK
D S
M—
no
chan
ge
Phy
siol
ogic
al m
easu
res:
►
Cre
atin
ine—
mar
gina
lly
sign
ifica
nt d
ecre
ase
►
GFR
—re
mai
ned
sta
ble
Mur
ali
et a
l (2
013)
28P
PC
KD
412 A
ge: 6
8
►D
iet/
nutr
ition
Onl
ine
tool
►
Web
site
‘Die
tary
ass
essm
ent
and
eva
luat
ion
tool
’:
►S
elf-
adm
inis
tere
d
►O
bta
ins
24 h
ours
food
his
tory
►
Then
eva
luat
es d
iet
bas
ed o
n K
DO
QI G
L
►Th
en s
hare
gen
eral
tip
s fo
r su
cces
s
►A
rep
ort
is g
ener
ated
for
the
nep
hrol
ogis
t to
gu
ide
dis
cuss
ion
with
pat
ient
sD
urat
ion:
sin
gle
exp
osur
eC
omp
arat
or: n
one
Cog
nitio
ns:
►
Cha
nge
in p
atie
nts’
sel
f-ef
ficac
y to
ad
here
to
KD
OQ
I G
L af
ter
sing
le e
xpos
ure
to t
he
tool
—th
ree
wor
sene
d, t
hree
im
pro
ved
, six
no
chan
ge
Inte
rven
tion
spec
ific:
►
Tool
acc
epta
bili
ty –
wel
l ac
cep
ted
►C
ongr
uenc
e of
pat
ient
an
d p
rovi
der
att
itud
es—
inco
ngru
ence
in 4
/10
case
s w
here
pro
vid
er s
tate
s us
ed
rep
ort
but
pat
ient
doe
sn’t
verif
y
Nau
ta e
t al
(2
013)
32P
PC
KD
22 Age
: 55.
2–59
.8
►D
iet/
nutr
ition
►
Phy
sica
l act
ivity
►
Life
styl
e
Onl
ine
tool
►
Prin
t
►W
ebsi
te‘L
ifest
yle
man
agem
ent
tool
’:
►33
-pag
e q
uick
sta
rt g
uid
e p
rovi
ded
►
Pat
ient
s ha
d a
cces
s to
site
for
4 m
onth
s—p
atie
nt c
hoic
e to
freq
uenc
y of
vis
its t
o w
ebsi
te
►D
urat
ion:
4 m
onth
s
►C
omp
arat
or: n
one
Cog
nitio
ns:
►
Sel
f-ef
ficac
y—lim
ited
ef
fect
iven
ess
Beh
avio
urs:
►
SM
—lim
ited
eff
ectiv
enes
s
Tab
le 4
C
ontin
ued
Con
tinue
d
on January 13, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2017-019814 on 22 March 2018. D
ownloaded from

15Donald M, et al. BMJ Open 2018;8:e019814. doi:10.1136/bmjopen-2017-019814
Open Access
Stu
dy
and
ye
ar(R
efer
ence
)D
esig
nTa
rget
po
pul
atio
nS
tud
y si
zeA
ge
(yea
rs)
Inte
rven
tio
n to
pic
(s)
Pro
vid
er(s
)D
eliv
ery
form
atD
escr
ipti
on
of
inte
rven
tio
nS
tud
y o
utco
mes
Stu
dy
resu
lts
Thom
as a
nd
Bry
ar (2
013)
33M
MD
iab
etic
nep
hrop
athy
(D
M+
mic
roal
bum
inur
ia)
176
(E=
116,
C=
60)
Age
: NR
►
Gen
eral
CK
D k
now
led
ge
►C
omor
bid
ities
►
Life
styl
e
NR
►
Prin
t
►D
VD
‘SM
pac
kage
’:
►W
ritte
n m
ater
ials
►
20 m
in D
VD
►
Sel
f-m
onito
ring
dia
ry
►Fr
idge
mag
net
with
key
mes
sage
s
►B
P m
onito
r if
need
edD
urat
ion:
one
ses
sion
Com
par
ator
: sta
ndar
d c
are
Phy
siol
ogic
al m
easu
res:
►
BP
—no
sta
tistic
ally
sig
d
iffer
ence
►
Hae
mog
lob
in A
1c—
no c
hang
e
►B
MI—
no c
hang
e
Wal
ker
et
al
(201
3)64
PP
CK
D w
ith h
igh
risk
of
Pro
gres
sion
+D
M2+
HTN
+
alb
umin
uria
52 Age
: 57.
5
►D
iet/
nutr
ition
►
Med
icat
ion
►
Sym
pto
m m
anag
emen
t
►P
hysi
cal a
ctiv
ity
►O
ther
(ie,
com
plia
nce)
Nur
se, n
urse
p
ract
ition
er
►P
rint
►
Face
to
face
‘Nur
se p
ract
ition
er in
terv
entio
n in
prim
ary
care
se
ttin
g’:
►
SM
boo
klet
►
Initi
al a
sses
smen
t of
life
styl
e b
ehav
iour
s, S
M
pra
ctic
e, h
ealth
/med
icat
ion
know
led
ge
►In
div
idua
l ed
ucat
ion
►
Ind
ivid
ualis
ed p
atie
nt m
anag
emen
t p
lan
give
n at
end
of 1
2 w
eeks
►
Q2
wee
k 30
min
long
ass
essm
ents
and
rev
iew
×
12
wee
ksD
urat
ion:
12
wee
ksC
omp
arat
or: n
one
Beh
avio
urs:
►
SM
(Par
tner
s in
Hea
lth (P
IH)
inst
rum
ent)—
had
cha
nge
in
cert
ain
dom
ains
Wrig
ht N
unes
et
al
(201
3)65
QE
CK
D 1
–555
6(E
=15
5,
Coh
ort=
401)
Age
: 57
►
Gen
eral
CK
D k
now
led
ge
►D
iet/
nutr
ition
►
Med
icat
ion
►
Phy
sica
l act
ivity
►
Life
styl
e
►C
omor
bid
ities
►
Oth
er (i
e, c
omp
lianc
e)
Nep
hrol
ogy
fello
ws
►
Prin
t
►Fa
ce t
o fa
ce‘P
hysi
cian
-del
iver
ed e
duc
atio
n to
o’
►1-
pag
e in
terv
entio
n w
orks
heet
del
iver
ed
dur
ing
clin
ic v
isits
—ta
ke 1
–2 m
in t
o ad
min
iste
rD
urat
ion:
one
ses
sion
Com
par
ator
: ‘hi
stor
ical
gro
up’—
who
dev
elop
ed
shee
t
Cog
nitio
ns:
►
Kid
ney
spec
ific
know
led
ge—
asso
ciat
ed w
ith in
crea
se in
kn
owle
dge
Inte
rven
tion
spec
ific:
►
Feas
ibili
ty o
f int
erve
ntio
n—p
hysi
cian
s fo
und
it u
sefu
l an
d e
ffici
ent
but
had
con
cern
re
gard
ing
som
e of
the
tal
king
p
oint
s
Wal
ker
et
al
(201
4)24
PP
CK
D w
ith h
igh
risk
of
Pro
gres
sion
+D
M2+
HTN
+
alb
umin
uria
52 Age
: 57.
5
►S
ee W
alke
r et
al64
Nur
se, n
urse
p
ract
ition
er
►S
ee W
alke
r et
al64
►
See
Wal
ker
et a
l64P
hysi
olog
ical
mea
sure
s:
►A
lbum
inur
ia—
imp
rove
d
►G
FR—
no c
hang
e
►5
year
ab
solu
te c
ard
iova
scul
ar
risk—
imp
rove
d
►B
P—
imp
rove
d
►To
tal c
hole
ster
ol—
imp
rove
d
►H
aem
oglo
bin
A1c
—im
pro
ved
Cog
nitio
ns:
►
Kno
wle
dge
of m
edic
atio
ns/
cond
ition
s im
pro
ved
Beh
avio
urs:
►
Med
icat
ion
adhe
renc
e,
adhe
renc
e to
hea
lthy
lifes
tyle
im
pro
ved
Enw
orom
et
al (
2015
)66Q
EC
KD
1–4
49 (E=
25,
C=
24)
Age
: 73
►
Gen
eral
CK
D k
now
led
ge
►S
ymp
tom
s m
anag
emen
t
►M
odal
ities
►
Com
orb
iditi
es
►O
ther
(ie,
ad
vanc
ed c
are
pla
nnin
g)
Nur
se p
ract
ition
er,
phy
sici
an
assi
stan
ts, c
linic
al
nurs
e sp
ecia
list
►
Face
to
face
‘Kid
ney
Dis
ease
Ed
ucat
ion
(KD
E)’
►
six
educ
atio
n cl
asse
s on
one
on
one
or g
roup
b
asis
Dur
atio
n: u
ncle
arC
omp
arat
or: n
o K
DE
Phy
siol
ogic
al m
easu
res:
►
GFR
dec
line—
slow
er in
E
grou
p
►H
aem
oglo
bin
—E
gro
up
mai
ntai
ned
mor
e st
able
leve
l co
mp
ared
with
non
-KD
E g
roup
w
ho lo
st 1
g/L
from
bas
elin
e
Cog
nitio
ns:
►
Kid
ney
dis
ease
kno
wle
dge
(K
iKS
sur
vey)
—no
cha
nge
Tab
le 4
C
ontin
ued
Con
tinue
d
on January 13, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2017-019814 on 22 March 2018. D
ownloaded from

16 Donald M, et al. BMJ Open 2018;8:e019814. doi:10.1136/bmjopen-2017-019814
Open Access
Stu
dy
and
ye
ar(R
efer
ence
)D
esig
nTa
rget
po
pul
atio
nS
tud
y si
zeA
ge
(yea
rs)
Inte
rven
tio
n to
pic
(s)
Pro
vid
er(s
)D
eliv
ery
form
atD
escr
ipti
on
of
inte
rven
tio
nS
tud
y o
utco
mes
Stu
dy
resu
lts
Vann
et
al
(201
5)29
PP
CK
D 3
b-4
9 Age
: mea
n N
R
►G
ener
al C
KD
kno
wle
dge
►
Die
t/nu
triti
on
►S
ymp
tom
man
agem
ent
►
Mod
aliti
es
►C
omor
bid
ities
►
Oth
er (i
e, s
elf-
care
m
anag
emen
t st
rate
gies
and
b
ehav
iour
s)
Nur
se p
ract
ition
er
►P
rint
►
Web
site
►
Face
to
face
►
Whi
te b
oard
‘CK
D E
duc
atio
n P
rogr
amm
e’
►C
KD
ed
ucat
ion
sess
ions
►
Ass
essm
ent
of r
ead
ines
s to
cha
nge
►
CK
D t
oolk
it in
div
idua
lised
for
each
par
ticip
ant
►
Col
lab
orat
ive
goal
set
ting
bet
wee
n nu
rse
pra
ctiti
oner
and
pat
ient
►
Info
rmat
ion
boo
klet
with
web
site
s lis
ted
►
Pat
ient
s m
et w
ith n
urse
pra
ctiti
oner
for
60 m
inD
urat
ion:
ove
r si
x vi
sits
Com
par
ator
: non
e
Cog
nitio
ns:
►
CK
D-r
elat
ed k
now
led
ge—
imp
rove
d
Beh
avio
urs:
►
Sel
f rep
orte
d b
ehav
iour
ch
ange
—im
pro
ved
Cup
isiti
et
al
(201
6)67
Ob
sC
KD
3b
-582
3(E
=30
5,C
=51
8)A
ge: 6
9–74
►
Die
t/nu
triti
onD
ietic
ian
►
Face
to
face
‘Nut
ritio
nal T
reat
men
t’
►R
enal
die
ticia
n as
sess
ed d
ieta
ry h
abits
us
ing
3-d
ay d
ieta
ry r
ecal
l & p
erfo
rmed
an
inte
rven
tion
tailo
red
to
the
need
s/cl
inic
al
feat
ures
of t
he p
atie
nt
►P
rogr
esse
d fr
om ‘n
orm
al’ d
iet
→ lo
w p
rote
in
die
t →
ver
y lo
w p
rote
in d
iet
dep
end
ing
on
need
sD
urat
ion:
at
leas
t 6
mon
ths
Com
par
ator
: sta
ndar
d c
are
Phy
siol
ogic
al m
easu
res:
►
Pho
spha
turia
—lo
wer
in E
gr
oup
Hea
lthca
re:
►
Furo
sem
ide
use—
low
er in
E
grou
p
►
Cal
cium
free
pho
spha
te b
ind
us
e—lo
wer
in E
gro
up
►
ES
A u
se—
low
er in
E g
roup
►
Act
ive
vita
min
D p
rep
arat
ion
use—
low
er in
E g
roup
Ind
ivid
ual o
utco
mes
:
►D
ieta
ry s
atis
fact
ion
que
stio
nnai
re—
maj
ority
of E
gr
oup
pat
ient
s w
ere
satis
fied
w
ith t
heir
die
Ong
et
al
(201
6)68
PP
CK
D 4
–545 A
ge: 5
9.4
►
Med
icat
ions
►
Sym
pto
m m
anag
emen
t
►C
omor
bid
ities
►
Oth
er (i
e, t
rack
ing
lab
re
sults
)
Mob
ile a
pp
licat
ion
►
Sm
art
pho
ne
app
licat
ion
‘Sm
artp
hone
bas
ed S
M s
yste
m’
►
Ap
plic
atio
n ge
nera
ted
per
sona
lised
pat
ient
m
essa
ges
bas
ed o
n p
reb
uilt
algo
rithm
sD
urat
ion:
6 m
onth
sC
omp
arat
or: n
one
Phy
siol
ogic
al m
easu
res:
►
BP
—ch
ange
in h
ome
BP
re
adin
gs
Inte
rven
tion
spec
ific:
►
Med
icat
ions
— 1
27 m
edic
atio
n d
iscr
epan
cies
iden
tified
Pen
aloz
a-R
amos
et
al
(201
6)25
Ob
sH
TN
(BP
>13
0/80
)+C
KD
sta
ge
thre
e or
CVA
/TIA
or
DM
or
MI o
r an
gina
or
CA
BG
NR
Age
: NA
►
See
McM
anus
et
al47
Gen
eral
p
ract
ition
er,
pat
ient
►
See
McM
anus
et
al47
►
See
McM
anus
et
al47
Hea
lthca
re:
►
Cos
t ef
fect
ive—
yes
Not
ap
plic
able
.
Out
com
e im
pro
ved
pos
t in
terv
entio
n.
Out
com
e w
orse
ned
pos
t in
terv
entio
n.
Out
com
e un
chan
ged
pos
t in
terv
entio
n.
Out
com
e ha
d m
ixed
res
ults
(som
e im
pro
ved
and
/or
som
e w
orse
ned
and
/or
som
e d
id n
ot c
hang
e).
BM
I, b
ody
mas
s in
dex
; BP,
blo
od p
ress
ure;
C, c
ontr
ol; C
ALD
, cul
tura
lly a
nd li
ngui
stic
ally
div
erse
; CH
D, c
oron
ary
hear
t d
isea
se; C
HE
ER
S, C
ontr
ollin
g H
yper
tens
ion:
Ed
ucat
ion
and
Em
pow
erm
ent
Ren
al S
tud
y; C
KD
, chr
onic
kid
ney
dis
ease
; CVA
, ce
reb
rova
scul
ar a
ccid
ent;
DB
P, d
iast
olic
blo
od p
ress
ure;
DM
, dia
bet
es m
ellit
us; E
, exp
erim
enta
l; eG
FR, e
stim
ated
glo
mer
ular
filtr
atio
n ra
te; E
SA
, ert
hrop
oies
is s
timul
atin
g ag
ents
; ES
RD
, ear
ly s
tage
ren
al d
isea
se; H
TN, h
yper
tens
ion;
MM
, mix
ed m
etho
ds;
N
R, n
ot r
epor
ted
; Ob
s, o
bse
rvat
iona
l; P
P, p
re-p
ost
inte
rven
tion;
QE
, qua
si-e
xper
imen
tal;
QO
L, q
ualit
y of
life
; RC
T, r
and
omis
ed c
ontr
olle
d t
rial;
RR
T, r
enal
rep
lace
men
t th
erap
y; S
BP,
sys
tolic
blo
od p
ress
ure;
SM
, sel
f-m
anag
emen
t; T
IA, t
rans
ient
isch
aem
ic
atta
ck.
Tab
le 4
C
ontin
ued
on January 13, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2017-019814 on 22 March 2018. D
ownloaded from

17Donald M, et al. BMJ Open 2018;8:e019814. doi:10.1136/bmjopen-2017-019814
Open Access
Tab
le 5
S
umm
ary
of q
ualit
ativ
e st
udie
s
Stu
dy
(Ref
eren
ce)
Targ
et p
op
ulat
ion
Num
ber
of
par
tici
pan
tsA
im/I
nter
vent
ion
Met
hod
sS
umm
ary
of
find
ing
s
Blic
kem
et
al21
CK
D s
tage
320
‘To
exp
lore
the
exp
erie
nce
of
pat
ient
-led
ass
essm
ent
for
netw
ork
sup
por
t (P
LAN
S) f
rom
the
p
ersp
ectiv
es o
f par
ticip
ants
and
te
lep
hone
sup
por
t w
orke
rs.’
(p. 1
)In
terv
entio
n: s
ee t
able
4
Bla
kem
an e
t al
46
Inte
rvie
ws
and
focu
s gr
oup
s: n
o an
alyt
ic
met
hod
olog
y d
iscu
ssed
►
Mix
ed r
ecep
tion
from
par
ticip
ants
►
Form
ulat
ion
of ‘h
ealth
’ in
ever
yday
life
(ie,
p
artic
ipan
ts u
naw
are
of h
avin
g C
KD
or
its
sign
ifica
nce—
conf
used
ab
out
rele
vanc
e of
P
LAN
S)
►
Traj
ecto
ries
and
tip
pin
g p
oint
s (ie
, eng
agem
ent
in
PLA
NS
dep
end
ed o
n p
artic
ipan
ts’ s
tage
of l
ife—
eith
er c
ould
influ
ence
try
ing
new
thi
ngs
or d
isru
pt
rout
ines
)
►Tr
ust
in n
etw
orks
(ie,
unw
illin
gnes
s to
see
k su
pp
ort,
intr
usiv
e, o
ther
s sa
w im
pro
ved
aw
aren
ess/
acce
ss t
o lo
cal r
esou
rces
; tai
lore
d
sup
por
t)
Hei
den
et
al 69
CK
D p
red
ialy
sis,
d
ialy
sis,
tra
nsp
lant
5To
iden
tify
par
ticip
ant’s
per
spec
tive
rega
rdin
g a
‘web
ap
plic
atio
n p
roto
typ
e to
hel
p m
ake
dec
isio
ns
rega
rdin
g d
iet
rest
rictio
ns a
nd
pho
spha
te b
ind
er d
osag
e.’ (
p. 5
44)
Inte
rven
tion:
Web
site
too
l for
p
atie
nts
that
incl
uded
thr
ee
com
pon
ents
—d
iet/
fluid
ed
ucat
ion;
d
iet
regi
stry
and
pho
spha
te b
ind
er
dec
isio
n su
pp
ort
tool
.
Inte
rvie
ws:
no
anal
ytic
m
etho
dol
ogy
dis
cuss
ed
►B
enefi
ts:
–E
duc
atio
n to
ol in
crea
sed
insi
ght
and
un
der
stan
din
g –A
ssis
ted
in t
rack
ing
and
cho
osin
g b
est
food
al
tern
ativ
e –D
ecis
ion
sup
por
t fo
r b
ind
er d
osag
e
►Li
mita
tions
: –Ta
rget
ed u
sers
fam
iliar
with
usi
ng c
omp
uter
s –U
sers
had
diff
eren
t in
form
atio
n ne
eds
–O
ne-w
ay c
omm
unic
atio
n –N
eed
sel
f-ca
re r
esou
rces
in p
lace
to
carr
y ou
t re
com
men
dat
ions
Jans
en e
t al
70C
KD
sta
ges
4–5
7Fe
asib
ility
of ‘
a p
sych
osoc
ial
inte
rven
tion
to a
ssis
t E
SR
D p
atie
nts
and
the
ir p
artn
ers
in in
tegr
atin
g re
nal d
isea
se a
nd t
reat
men
t in
to
dai
ly a
ctiv
ities
, prim
ary
wor
k an
d
ther
eby
incr
easi
ng a
uton
omy.
’ (p
. 280
)In
terv
entio
n: g
roup
tea
chin
g an
d h
and
boo
k re
gard
ing
cop
ing
stra
tegi
es a
nd g
oals
bas
ed o
n se
lf-re
gula
tion,
soc
ial l
earn
ing
and
sel
f-d
eter
min
atio
n th
eorie
s.
Inte
rvie
ws:
no
anal
ytic
m
etho
dol
ogy
dis
cuss
ed
►B
enefi
ts:
–G
roup
incl
uded
pre
dia
lysi
s an
d d
ialy
sis
pat
ient
s –Le
ader
s ad
dre
ssed
ind
ivid
ual n
eed
s, s
ituat
ions
an
d q
uest
ions
►
Lim
itatio
ns:
–P
atie
nt p
refe
renc
es fo
r in
form
atio
n d
iffer
ed b
y st
ages
of C
KD
–P
atie
nt s
ched
ules
nee
d t
o b
e co
nsid
ered
whe
n in
terv
entio
n of
fere
d –C
onsi
der
offe
ring
inte
rven
tion
shor
tly a
fter
d
iagn
osis
of C
KD
Con
tinue
d
on January 13, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2017-019814 on 22 March 2018. D
ownloaded from

18 Donald M, et al. BMJ Open 2018;8:e019814. doi:10.1136/bmjopen-2017-019814
Open Access
Stu
dy
(Ref
eren
ce)
Targ
et p
op
ulat
ion
Num
ber
of
par
tici
pan
tsA
im/I
nter
vent
ion
Met
hod
sS
umm
ary
of
find
ing
s
Thom
as e
t al
33Ty
pe
1 or
2
DM
with
m
icro
alb
umin
uria
5 (3
face
-to
-fac
e in
terv
iew
s)
To e
valu
ate
‘whe
ther
pat
ient
s un
der
stoo
d t
he c
onte
nt o
f the
pac
k an
d w
heth
er t
hey
coul
d m
ake
any
reco
mm
end
atio
ns.’
(p. 2
75)
Inte
rven
tion:
see
tab
le 4
Th
omas
et
al30
Que
stio
nnai
re a
nd
inte
rvie
w: n
o an
alyt
ic
met
hod
olog
y d
iscu
ssed
►
Mix
ed r
esp
onse
s
►D
VD
—co
nten
t d
istr
essi
ng a
nd t
ook
effo
rt t
o us
e
►W
ritte
n m
ater
ial u
sefu
l, b
ut n
eed
to
elab
orat
e on
se
rious
ness
of d
isea
se
►P
acka
ge h
elp
ed c
hang
e b
ehav
iour
—st
op
smok
ing,
mon
itorin
g D
M
Will
iam
s et
al22
CK
D s
tage
s 2–
4 w
ith d
iab
etes
and
ca
rdio
vasc
ular
d
isea
se
26‘E
xam
ine
the
per
cep
tions
of a
gro
up
of C
ALD
par
ticip
ants
with
com
orb
id
dia
bet
es, c
hron
ic k
idne
y d
isea
se
and
car
dio
vasc
ular
dis
ease
… u
sing
an
inte
rven
tion
to in
fluen
ce t
heir
med
icat
ion
self-
effic
acy.
’ (p
. 127
1)In
terv
entio
n: s
ee t
able
4
Will
iam
s et
al43
Inte
rvie
ws:
Ritc
hie
and
Sp
ence
r th
emat
ic
app
roac
h
►
Att
itud
es t
owar
ds
taki
ng m
edic
atio
ns (i
e,
app
reci
ate
imp
orta
nce
of t
akin
g; m
edic
atio
n b
urd
en; c
once
rn w
ith t
he n
umb
er o
f med
icat
ions
, ef
fect
iven
ess
and
sid
e ef
fect
s of
med
icat
ions
►
Hav
ing
to t
ake
med
icat
ions
(ie,
beh
avio
urs
and
fa
mily
sup
por
t to
ass
ist
taki
ng m
edic
atio
ns;
forg
ettin
g an
d n
on-a
dhe
rent
; mot
ivat
ion
to t
ake
to
pre
vent
bec
omin
g w
orse
)
►Im
ped
imen
ts t
o ch
roni
c ill
ness
med
icat
ion
self-
effic
acy
(ie, l
ack
of k
now
led
ge r
egar
din
g m
edic
atio
n; s
tron
g fa
ith in
phy
sici
an’s
ad
vice
; m
ultip
le m
edic
atio
ns t
oo o
verw
helm
ing;
cos
t)
Will
iam
s et
al23
CK
D s
tage
s 2–
4,
with
coe
xist
ing
dia
bet
es a
nd
hyp
erte
nsio
n
39In
div
idua
l per
cep
tions
of a
‘t
elep
hone
cal
l usi
ng a
mot
ivat
iona
l in
terv
iew
ing
app
roac
h to
im
pro
ve m
edic
atio
n ad
here
nce
in p
artic
ipan
ts w
ith c
oexi
stin
g d
iab
etes
, CK
D a
nd h
yper
tens
ion.
’ (p
. 472
)In
terv
entio
n: s
ee t
able
4
Will
iam
s et
al42
Inte
rvie
ws:
Ritc
hie
and
Sp
ence
r th
emat
ic
app
roac
h
►
Imp
orta
nce
of h
ealth
(ie,
det
erm
ined
the
deg
ree
of h
ealth
beh
avio
ur; a
ltere
d m
edic
atio
ns o
r us
e of
co
mp
lem
enta
ry m
edic
ine
to c
ontr
ol h
ealth
)
►P
erce
ived
ser
ious
ness
of d
isea
se (i
e, t
hink
ing
abou
t m
orta
lity;
com
orb
iditi
es c
omp
licat
e ca
re;
acut
e ill
ness
with
chr
onic
con
diti
ons)
►
Per
ceiv
ed t
hrea
t of
dis
ease
(ie,
wan
t to
lear
n ab
out
dis
ease
con
trol
ear
lier;
sym
pto
m
man
agem
ent;
look
ing
for
reas
ons
to e
xpla
in w
hy
ill)
CK
D, c
hron
ic k
idne
y d
isea
se; D
M, d
iab
etes
mel
litus
.
Tab
le 5
C
ontin
ued
on January 13, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2017-019814 on 22 March 2018. D
ownloaded from

19Donald M, et al. BMJ Open 2018;8:e019814. doi:10.1136/bmjopen-2017-019814
Open Access
protocols, changing health behaviours, shared decision making with healthcare providers),7 75 along with evalua-tion of the cost-effectiveness and resource utilisation.
The majority of studies did not identify a single primary outcome but rather multiple outcomes. We found that physiological outcomes (ie, blood pressure) were the most commonly reported and symptoms were the least mentioned. These findings demonstrate the lack of patient-driven outcomes that may be important to them, for example, a patient’s individual health goals across a variety of dimensions (ie, symptoms, mobility, social and role function in the family or community) that could possibly maximise their quality of life. Work by Tong et al (2015) highlights this concept, where patients with CKD are more interested in treatment choices that influence non-traditional clinical outcomes such as impact on family and lifestyle.72 A holistic approach should be considered where mental and psychosocial outcomes are investigated, rather than just physiolog-ical endpoints.
Our findings from the qualitative studies looking at patient perspectives are inconclusive because of the limited number of studies and the heterogeneity of the interventions. Havas et al12 similarly reported a lack of research related to patient perspectives on self-man-agement in CKD.12 There is also a lack of qualitative studies overall, which could provide valuable information regarding attitudes and challenges of self-management interventions from the perspective of both providers and patients.
Strengths of our study include the comprehensive nature of our search, inclusion of all study designs and consideration of self-management features that have not been investigated previously. We also engaged patient partners in determining the research question, advising us on search terms, grey literature sources and reviewing the results to ensure we captured and reported the data meaningfully. One of the main limitations was the chal-lenge in synthesising the data given its heterogeneous nature. To address this challenge, the two reviewers used two standardised tools TIDieR19 and the EPOC tool20 to independently extract data and independently coded the outcomes into categories using the revised Self-and Family Management Framework .6 Also, we were unable to assess the self-management outcomes in terms of sustained changes in behaviour, physiological and health status. A final limitation was our inability to draw conclusions regarding the most effective self-man-agement intervention for adult patients with CKD, keeping in mind that our aim was to review the breadth of the current literature and present the gaps that exist.
Overall, we found considerable variation in self-man-agement interventions for adults with CKD with respect to their content and delivery as well as the outcomes assessed and results obtained. Major gaps in the literature include the lack of patient engagement in the design of the self-management intervention, along with the lack of a behavioural change theory to
inform their design. Our future research will incorpo-rate intervention frameworks to codevelop and eval-uate a self-management intervention based on a sound behavioural theory involving our national patient part-ners, specialists, primary care providers and decision makers.
Author affiliations1Department of Medicine, University of Calgary, Calgary, Canada2Interdisciplinary Chronic Disease Collaboration, Calgary, Canada3Department of Community Health Sciences, University of Calgary, Calgary, Canada4Daphne Cockwell School of Nursing, Ryerson University, Toronto, Canada5Institute of Health Policy, Management and Evaluation, University of Toronto, Toronto, Canada6Li Ka Shing Knowledge Institute, St. Michael’s Hospital, Toronto, Canada7Can-SOLVE CKD Network, Patient Partner, Pouce Coupe, Canada8Sydney School of Public Health, The University of Sydney, Sydney, New South Wales9Department of Family and Community Medicine, University of Toronto, Toronto, Canada10Lawson Health Research Institute, London, UK11Centre for Mental Health, University Health Network, Toronto, Canada12Department of Psychiatry, University of Toronto, Toronto, Canada13Department of Medicine, McMaster University, Ontario, Canada14Department of Pediatrics, University of Calgary, Calgary, Canada
Acknowledgements Diane Lorenzetti for providing support and direction regarding search strategies. We would also like to thank Sarah Gil in assisting us with acquiring full text studies.
Contributors All authors contributed to the research idea and study design. MD and BKK acquired the data. MD, BKK and BRH completed data analysis and interpretation. All authors contributed important intellectual content during manuscript drafting and revisions. They also read and approved the final manuscript. BRH and PR provided mentorship.
Funding MD is a recipient of the 2016 Alberta SPOR Graduate Studentships in Patent- Oriented Research. Alberta SPOR Graduate Studentships in Patient-Oriented Research are jointly funded by Alberta Innovates and the Canadian Institute of Health Research. BRH is supported by the Roy and Vi Baay Chair in Kidney Research, Canadian Institutes of Health Research’s Strategy for Patient-Oriented Research (SPOR).
disclaimer The funding organisations had no role in the design and conduct of the study; data collection, analysis and interpretation or preparation, review or approval of the manuscript.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
data sharing statement The following data will be available, study protocol and analysis plan, to anyone who wishes to access them and will be available immediately following publication from the corresponding author.
Open Access This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http:// creativecommons. org/ licenses/ by- nc/ 4. 0/
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
reFerenCes 1. Arora P, Vasa P, Brenner D, et al. Prevalence estimates of chronic
kidney disease in Canada: results of a nationally representative survey. CMAJ 2013;185:e417–23.
on January 13, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2017-019814 on 22 March 2018. D
ownloaded from

20 Donald M, et al. BMJ Open 2018;8:e019814. doi:10.1136/bmjopen-2017-019814
Open Access
2. Tonelli M, Wiebe N, Guthrie B, et al. Comorbidity as a driver of adverse outcomes in people with chronic kidney disease. Kidney Int 2015;88:859–66.
3. Hemmelgarn BR, Pannu N, Ahmed SB, et al. Determining the research priorities for patients with chronic kidney disease not on dialysis. Nephrology, dialysis. Transplantation 2017;32:847–54.
4. Tong A, Chando S, Crowe S, et al. Research priority setting in kidney disease: a systematic review. American Journal of Kidney Diseases 2015;65:674–83.
5. Richard AA, Shea K. Delineation of self-care and associated concepts. J Nurs Scholarsh 2011;43:no–64.
6. Grey M, Schulman-Green D, Knafl K, et al. A revised Self- and Family Management Framework. Nurs Outlook 2015;63:162–70.
7. Novak M, Costantini L, Schneider S, et al. Approaches to self-management in chronic illness. Semin Dial 2013;26:188–94.
8. Lopez-Vargas PA, Tong A, Howell M, et al. Educational interventions for patients with CKD: a systematic review. Am J Kidney Dis 2016;68:353–70.
9. Mason J, Khunti K, Stone M, et al. Educational interventions in kidney disease care: A systematic review of randomized trials. Am J Kidney Dis 2008;51:933–51.
10. Lee MC, Wu SV, Hsieh NC, et al. Self-management programs on eGFR, depression, and quality of life among patients with chronic kidney disease: a meta-analysis. Asian Nurs Res 2016;10:255–62.
11. Lin MY, Liu MF, Hsu LF, et al. Effects of self-management on chronic kidney disease: a meta-analysis. Int J Nurs Stud 2017;74:128–37.
12. Havas K, Bonner A, Douglas C. Self-management support for people with chronic kidney disease: Patient perspectives. J Ren Care 2016;42:7–14.
13. Bonner A, Havas K, Douglas C. Self-management programmes in stages 1-4 chronic kidney disease: A literature review. J Ren Care 2014;40:194–204.
14. Welch JL, Johnson M, Zimmerman L, et al. Self-management interventions in stages 1 to 4 chronic kidney disease: an integrative review. West J Nurs Res 2015;37:652–78.
15. Levac D, Colquhoun H, O'Brien KK. Scoping studies: advancing the methodology. Implement Sci 2010;5:69.
16. Levin A. Canadians Seeking Solutions and Innovations to Overcome Chronic Kidney Disease (Can-SOLVE CKD). CIHR Grant 2015.
17. Peters MD, Godfrey CM, Khalil H, et al. Guidance for conducting systematic scoping reviews. Int J Evid Based Healthc 2015;13:141–6.
18. Canadian Agency for Drugs and Technologies in Health (CADTH). Grey Matters: A practical search tool for evidence-based medicine. https://www. cadth. ca/ resources/ finding- evidence/ grey- matters (accessed Sep 2015).
19. Template for intervention description and replication (TIDieR) checklist. http://www. equator- network. org/ wp- content/ uploads/2014/03/TIDieR-Checklist-PDF(accessed Sept 2016).
20. Effective Practice and Organisation of Care (EPOC) data collection. http:// epoc. cochrane. org/ epoc- specific- resources- review- authors (accessed Oct 2016).
21. Blickem C, Kennedy A, Jariwala P, et al. Aligning everyday life priorities with people's self-management support networks: an exploration of the work and implementation of a needs-led telephone support system. BMC Health Serv Res 2014;14:262.
22. Williams A, Manias E, Cross W, et al. Motivational interviewing to explore culturally and linguistically diverse people's comorbidity medication self-efficacy. J Clin Nurs 2015;24:1269–79.
23. Williams A, Manias E. Exploring motivation and confidence in taking prescribed medicines in coexisting diseases: a qualitative study. J Clin Nurs 2014;23:471–81.
24. Walker RC, Marshall MR, Polaschek NR. A prospective clinical trial of specialist renal nursing in the primary care setting to prevent progression of chronic kidney: a quality improvement report. BMC Fam Pract 2014;15:155.
25. Penaloza-Ramos MC, Jowett S, Mant J, et al. Cost-effectiveness of self-management of blood pressure in hypertensive patients over 70 years with suboptimal control and established cardiovascular disease or additional cardiovascular risk diseases (TASMIN-SR). Eur J Prev Cardiol 2016;23:902–12.
26. Byrne J, Khunti K, Stone M, et al. Feasibility of a structured group education session to improve self-management of blood pressure in people with chronic kidney disease: an open randomised pilot trial. BMJ Open 2011;1:e000381.
27. Kao Yu‐Hsiu, Huang Yi‐Ching, Chen Pei‐Ying, Kao Y, Huang Y, Chen P, et al. The effects of exercise education intervention on the exercise behaviour, depression, and fatigue status of chronic kidney disease patients. Health Educ 2012;112:472–84.
28. Murali S, Arab L, Vargas R, et al. Internet-based tools to assess diet and provide feedback in chronic kidney disease stage IV: a pilot study. J Ren Nutr 2013;23:e33–e42.
29. Vann JC, Hawley J, Wegner S, et al. Nursing intervention aimed at improving self-management for persons with chronic kidney disease in North Carolina Medicaid: A pilot project. Nephrol Nurs J 2015;42:239–55.
30. Montoya V, Sole ML, Norris AE. Improving the care of patients with chronic kidney disease using group visits: a pilot study to reflect an emphasis on the patients rather than the disease. Nephrol Nurs J 2016;43:207–22.
31. Kazawa K, Moriyama M. Effects of a self-management skills-acquisition program on pre-dialysis patients with diabetic nephropathy. Nephrol Nurs J 2013;40:141–8.
32. Nauta J, van der Boog J, Slegten J, 2013. Web-based lifestyle management for chronic kidney disease. eTELEMED 2013, The Fifth International Conference on eHealth, Telemedicine, and Social Medicine, Nice, France 141–6
33. Thomas N, Bryar R. An evaluation of a self-management package for people with diabetes at risk of chronic kidney disease. Prim Health Care Res Dev 2013;14:270–80.
34. Binik YM, Devins GM, Barre PE, et al. Live and learn: patient education delays the need to initiate renal replacement therapy in end-stage renal disease. J Nerv Ment Dis 1993;181:371–6.
35. Gillis BP, Caggiula AW, Chiavacci AT, et al. Nutrition intervention program of the Modification of Diet in Renal Disease Study: a self-management approach. J Am Diet Assoc 1995;95:1288–94.
36. Devins GM, Mendelssohn DC, Barré PE, Binik YM, et al. Predialysis psychoeducational intervention and coping styles influence time to dialysis in chronic kidney disease. Am J Kidney Dis 2003;42:693–703.
37. Devins GM, Mendelssohn DC, Barré PE, et al. Predialysis psychoeducational intervention extends survival in CKD: a 20-year follow-up. Am J Kidney Dis 2005;46:1088–98.
38. Campbell KL, Ash S, Bauer JD. The impact of nutrition intervention on quality of life in pre-dialysis chronic kidney disease patients. Clin Nutr 2008;27:537–44.
39. Chen SH, Tsai YF, Sun CY, et al. The impact of self-management support on the progression of chronic kidney disease-a prospective randomized controlled trial. Nephrology, Dialysis. Transplantation 2011;26:3560–6.
40. Flesher M, Woo P, Chiu A, et al. Self-management and biomedical outcomes of a cooking, and exercise program for patients with chronic kidney disease. J Ren Nutr 2011;21:188–95.
41. Joboshi H, Oka M, Takahashi S, et al. Effects of the EASE program in chronic kidney disease education: A randomized controlled trial to evaluate self-management. J Jpn Acad Nurs Sci 2012;32:21–9.
42. Williams A, Manias E, Walker R, et al. A multifactorial intervention to improve blood pressure control in co-existing diabetes and kidney disease: a feasibility randomized controlled trial. J Adv Nurs 2012;68:2515–25.
43. Williams AM, Liew D, Gock H, et al. Working with CALD groups: testing the feasibility of an intervention to improve medication self- management in people with kidney disease, diabetes, and cardiovascular disease. Renal Society of Australasia Journal 2012;8:62–9.
44. de Brito-Ashurst I, Perry L, Sanders TA, et al. The role of salt intake and salt sensitivity in the management of hypertension in South Asian people with chronic kidney disease: a randomised controlled trial. Heart 2013;99:1256–60.
45. Paes-Barreto JG, Silva MI, Qureshi AR, et al. Can renal nutrition education improve adherence to a low-protein diet in patients with stages 3 to 5 chronic kidney disease? J Ren Nutr 2013;23:164–71.
46. Blakeman T, Blickem C, Kennedy A, et al. Effect of information and telephone-guided access to community support for people with chronic kidney disease: randomised controlled trial. PLoS One 2014;9:e109135.
47. McManus RJ, Mant J, Haque MS, et al. Effect of self-monitoring and medication self-titration on systolic blood pressure in hypertensive patients at high risk of cardiovascular disease: the TASMIN-SR randomized clinical trial. JAMA 2014;312:799.
48. Park J, Lyles RH, Bauer-Wu S. Mindfulness meditation lowers muscle sympathetic nerve activity and blood pressure in African-American males with chronic kidney disease. Am J Physiol Regul Integr Comp Physiol 2014;307:R93–R101.
49. Howden EJ, Coombes JS, Strand H, Douglas B, et al. Exercise training in CKD: efficacy, adherence, and safety. Am J Kidney Dis 2015;65:583–91.
50. Leehey DJ, Collins E, Kramer HJ, et al. Structured exercise in obese diabetic patients with chronic kidney disease: A randomized controlled Trial. Am J Nephrol 2016;44:54–62.
51. Robinson JA, Robinson KJ, Lewis DJ. Games: a motivational educational strategy. Anna J 1988;15:277–9.
on January 13, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2017-019814 on 22 March 2018. D
ownloaded from

21Donald M, et al. BMJ Open 2018;8:e019814. doi:10.1136/bmjopen-2017-019814
Open Access
52. Klang B, Björvell H, Berglund J, et al. Predialysis patient education: effects on functioning and well-being in uraemic patients. J Adv Nurs 1998;28:36–44.
53. Cupisti A, Morelli E, Meola M, et al. Vegetarian diet alternated with conventional low-protein diet for patients with chronic renal failure. J Ren Nutr 2002;12:32–7.
54. Gutiérrez Vilaplana JM, Zampieron A, Craver L, et al. Evaluation of psychological outcomes following the intervention 'teaching group': study on predialysis patients. J Ren Care 2009;35:159–64.
55. Pagels A, Wang M, Magnusson A, et al. Using patient diary in chronic illness care: Evaluation of a tool promoting self-care. Vard I Norden 2008;28:49–52.
56. Yen M, Huang JJ, Teng HL. Education for patients with chronic kidney disease in Taiwan: a prospective repeated measures study. J Clin Nurs 2008;17:2927–34.
57. Gutiérrez Vilaplana Josep Mª, Samsó Piñol E, Cosi Ponsa J, et al. Evaluación de la intervención enseñanza: grupo en la consulta de enfermedad renal crónica avanzada. Revista de la Sociedad Española de Enfermería Nefrológica 2007;10:280–5.
58. Wu IW, Wang SY, Hsu KH, et al. Multidisciplinary predialysis education decreases the incidence of dialysis and reduces mortality--a controlled cohort study based on the NKF/DOQI guidelines. Nephrol Dial Transplant 2009;24:3426–33.
59. Wierdsma J, van Zuilen A, van der Bijl J. Self-efficacy and long-term medication use in patients with chronic kidney disease. J Ren Care 2011;37:158–66.
60. Aguilera Florez AI, Velasco MP, Romero LG, et al. A little-used strategy in caring for patients with chronic kidney disease: Multidisciplinary education of patients and their relatives. Enferm Nefrol 2012;15:14–21.
61. Choi ES, Lee J. Effects of a face-to-face self-management program on knowledge, self-care practice and kidney function in patients with chronic kidney disease before the renal replacement therapy. J Korean Acad Nurs 2012;42:1070–8.
62. Diamantidis CJ, Fink W, Yang S, et al. Directed use of the internet for health information by patients with chronic kidney disease: prospective cohort study. J Med Internet Res 2013;15:e251.
63. Lin CC, Tsai FM, Lin HS, et al. Effects of a self-management program on patients with early-stage chronic kidney disease: a pilot study. Appl Nurs Res 2013;26:151–6.
64. Walker R, Marshall MR, Polaschek NR. Improving self-management in chronic kidney disease: a pilot study. Renal Society of Australasia Journal 2013;9:116–25.
65. Wright Nunes J, Greene JH, Wallston K, et al. Pilot study of a physician-delivered education tool to increase patient knowledge about CKD. Am J Kidney Dis 2013;62:23–32.
66. Enworom CD, Tabi M. Evaluation of kidney disease education on clinical outcomes and knowledge of self-management behaviors of patients with chronic kidney disease. Nephrol Nurs J 2015;42:363–72.
67. Cupisti A, D'Alessandro C, Di Iorio B, et al. Nutritional support in the tertiary care of patients affected by chronic renal insufficiency: report of a step-wise, personalized, pragmatic approach. BMC Nephrol 2016;17:124.
68. Ong SW, Jassal SV, Miller JA, et al. Integrating a Smartphone-Based Self-Management System into usual care of advanced CKD. Clin J Am Soc Nephrol 2016;11:1054–62.
69. Heiden S, Buus AA, Jensen MH, et al. A diet management information and communication system to help chronic kidney patients cope with diet restrictions. Stud Health Technol Inform 2013;192:543–7.
70. Jansen DL, Heijmans M, Rijken M, et al. The development of and first experiences with a behavioural self-regulation intervention for end-stage renal disease patients and their partners. J Health Psychol 2011;16:274–83.
71. Brummel‐Smith K, Butler D, Frieder M, et al. The American Geriatrics Society Expert Panel on Person-Centered, C. (2016). Person‐centered care: a definition and essential elements. J Am Geriatr Soc 2016;64:15–18.
72. Tong A, Sainsbury P, Chadban S, et al. Patients' experiences and perspectives of living with CKD. Am J Kidney Dis 2009;53:689–700.
73. Hutchinson TA, Hutchinson N, Arnaert A. Whole person care: encompassing the two faces of medicine. CMAJ 2009;180:845–6.
74. Trisolini M, Roussel A, Zerhusen E, et al. Activating chronic kidney disease patients and family members through the Internet to promote integration of care. Int J Integr Care 2004;4:e17.
75. Ong SW, Jassal SV, Porter E, et al. Using an electronic self-management tool to support patients with chronic kidney disease (CKD): a CKD clinic self-care model. Semin Dial 2013;26:195–202.
on January 13, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2017-019814 on 22 March 2018. D
ownloaded from