Embed Size (px)
Citation preview

Journal of The Association of Physicians of India ■ Vol. 64 ■ February 2016 81
Ondansetron-Induced Life Threatening HypokalemiaSK Mathew1, K Krishnan Kutty2, I Ramya3, C Padmakumar2, Prince Pius2
AbstractOndansetron is widely used in general practice for nausea and vomiting due to any cause. We report a rare side effect, life-threatening hypokalaemia following intravenous Ondansetron injection. It may be judicious to restrict the use of Odansetron to patients with severe vomiting due to chemotherapy or in post-operative state. Life-threatening hypokalemia can occur without any warning and may be difficult to manage in a primary set up.
1Retired Professor, 2Assistant Professor of Medicine, Kanyakumari Medical College and Government Hospital, Tamil nadu; 3Associate Professor of Medicine, CMC Hospital, VelloreReceived; 09.05.2013; Revised; 22.07.2013; Accepted: 23.07.2013
Introduction
Since their introduction in 1990’s the 5HT3 antagonists (Ondansetron,
G r a n i s e t r o n , D o l a s e t r o n a n d Palansetron) have become the most widely used drugs for chemotherapy and radiotherapy-induced emesis. 1 Hypokalaemia is a rare adverse effect of IV Ondansetron use well described in pediatric population when used for chemotherapy-induced emesis.2
Case Report
45 year old male was brought to the casualty of Kaniyakumari Medical co l lege and Government General Hospital with history of sudden onset weakness of both lower limbs of two hours duration. Six hours earlier he had visited a local hospital for fever of two days duration associated with nausea. He reported that he was given two injections at this hospital, one in the right cubital fossa and another in the gluteal region. He felt better and went home. After about 4 hours when he was walking to the river to wash, his knees buckled and he fell down. He could not get up by himself. The patient was helped by his friends and transported to the local hospital and referred to us for evaluation of sudden onset lower limbs weakness.
Patient was neither a known diabetic nor hypertensive and did not have any major illness in the past. He was a teetotaler and had never used illicit drugs or herbal preparations.
On arrival at our hospital the patient was conscious and well oriented. His vital signs were stable, his cardiac, respiratory and abdominal examination was unremarkable. On examination
of central nervous system, higher functions and cranial nerves were normal and there were no features of focal neurological involvement. But he had hypotonia of both his upper and lower limbs, the power and reflexes at various joints were 3/5 at the elbow and shoulder, wrist 4/5, hip and knee 1/5 and ankle 4/5.
The supinator, biceps and triceps deep tendon reflexes were normal. Knee jerk was absent, ankle was just present and plantar was bilateral flexor.
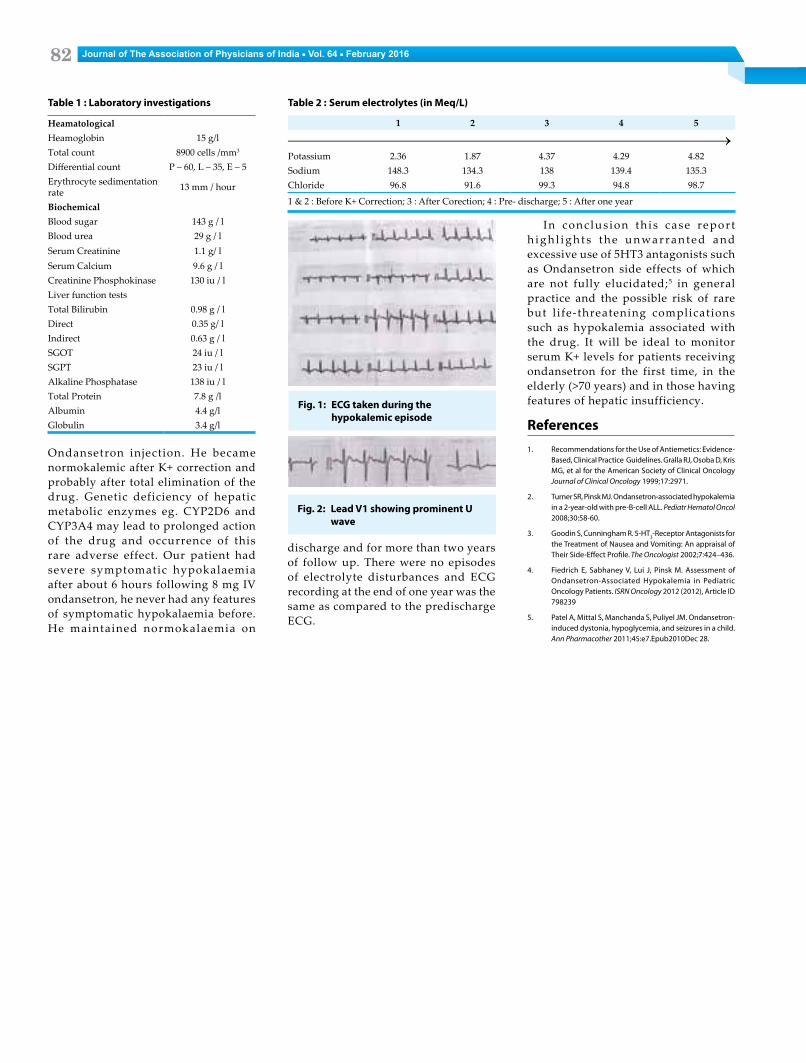
I n ve s t i g a t i o n s d o n e ( Ta b l e 1 ) revealed very low potassium level and U waves in electrocardiogram (ECG) (Figure 1). The patient was admitted to the intensive care unit and immediately started on potassium replacement at 10 meq/hr. The patient showed rapid clinical improvement, ECG changes also rapidly reverted and the serum potassium values became normal (Table 2). He regained normal power of all the muscles over 12 hours.
Urine 24 h K+ was not done due to lack of this facility in our hospital, moreover serum potassium levels became normal within 12 h of admission. Liver function, thyroid hormone profile, routine blood parameters and cardiac ECHO, Doppler and USG abdomen were within normal limits.
As the patient had no previous similar episodes of weakness and the patient had taken two injections just before the onset weakness, drug-induced hypokalemia and was suspected. The local practitioner disclosed that he had
given 8 mg intravenous Ondansetron and intramuscular paracetamol.
Discussion
5HT3 receptor antagonis ts are considered the “gold standard” in chemotherapy-induced nausea and vomiting (CINV).2
A c c o r d i n g t o t h e p r e s c r i b i n g information from the US FDA, IV O n d a n s e t r o n i n j e c t i o n h a s o n l y two indications namely CINV and post-operative nausea and vomiting (PONV). In general practice IV and oral Ondansetron are used excessively for nausea and vomiting due to any cause.
R e p o r t e d s i d e e f f e c t s o f Ondansetron include anaphylaxis, extrapyramidal effects, grand mal seizures, rarely angina pectoris, ECG changes, hypotension,tachycardia , bronchospasm, vascular events and constipation can develop in about 11% of the patients, transient hepatic enzyme abnormalities are seen in 5% and skin rash in 1%. Rarely hypokalaemia also has been reported.3
Hypokalemia caused by Ondansetron is due to its effect on the renal tubule, the effect on the renal tubule is not a class effect and it is unique to ondansetron. Ondansetron downregulates the Na+-K+-2Cl-(NKCC2) cotransporter, which results in increased sodium delivery to the distal nephron. This results in increased excretion of potassium via the renal outer medullary potassium channe (ROMK) receptor to facilitate electroneutral Na absorption. The second mechanism is upregulation of Na K ATPase particularly in the distal nephron which causes salt wasting.4
As chemotherapy, radiotherapy, and post-operative states are associated with prolonged vomiting and electrolyte disturbances hypokalemia cannot be directly attributed to Ondansetron. But in our patient there was not a single episode of vomiting so the hypokalemia can be attributed to the intravenous
Journal of The Association of Physicians of India ■ Vol. 64 ■ February 201682
Ondansetron injection. He became normokalemic after K+ correction and probably after total elimination of the drug. Genetic deficiency of hepatic metabolic enzymes eg. CYP2D6 and CYP3A4 may lead to prolonged action of the drug and occurrence of this rare adverse effect. Our patient had severe symptomatic hypokalaemia after about 6 hours following 8 mg IV ondansetron, he never had any features of symptomatic hypokalaemia before. He maintained normokalaemia on
Table 1 : Laboratory investigations
HeamatologicalHeamoglobin 15 g/lTotal count 8900 cells /mm3
Differential count P – 60, L – 35, E – 5Erythrocyte sedimentation rate 13 mm / hour
Biochemical Blood sugar 143 g / lBlood urea 29 g / lSerum Creatinine 1.1 g/ lSerum Calcium 9.6 g / lCreatinine Phosphokinase 130 iu / lLiver function testsTotal Bilirubin 0.98 g / lDirect 0.35 g/ lIndirect 0.63 g / lSGOT 24 iu / lSGPT 23 iu / lAlkaline Phosphatase 138 iu / lTotal Protein 7.8 g /lAlbumin 4.4 g/lGlobulin 3.4 g/l
discharge and for more than two years of follow up. There were no episodes of electrolyte disturbances and ECG recording at the end of one year was the same as compared to the predischarge ECG.
Fig. 2: Lead V1 showing prominent U wave
Fig. 1: ECG taken during the hypokalemic episode
Table 2 : Serum electrolytes (in Meq/L)
1 2 3 4 5
Potassium 2.36 1.87 4.37 4.29 4.82Sodium 148.3 134.3 138 139.4 135.3Chloride 96.8 91.6 99.3 94.8 98.7
1 & 2 : Before K+ Correction; 3 : After Corection; 4 : Pre- discharge; 5 : After one year
In conc lus ion th is case repor t h i g h l i g h t s t h e u n wa r r a n t e d a n d excessive use of 5HT3 antagonists such as Ondansetron side effects of which are not fully elucidated;5 in general practice and the possible risk of rare but l ife-threatening complications such as hypokalemia associated with the drug. It will be ideal to monitor serum K+ levels for patients receiving ondansetron for the first time, in the elderly (>70 years) and in those having features of hepatic insufficiency.
References 1. Recommendations for the Use of Antiemetics: Evidence-
Based, Clinical Practice Guidelines. Gralla RJ, Osoba D, Kris MG, et al for the American Society of Clinical Oncology Journal of Clinical Oncology 1999;17:2971.
2. Turner SR, Pinsk MJ. Ondansetron-associated hypokalemia in a 2-year-old with pre-B-cell ALL. Pediatr Hematol Oncol 2008;30:58-60.
3. Goodin S, Cunningham R. 5-HT3-Receptor Antagonists for the Treatment of Nausea and Vomiting: An appraisal of Their Side-Effect Profile. The Oncologist 2002;7:424–436.
4. Fiedrich E, Sabhaney V, Lui J, Pinsk M. Assessment of Ondansetron-Associated Hypokalemia in Pediatric Oncology Patients. ISRN Oncology 2012 (2012), Article ID 798239
5. Patel A, Mittal S, Manchanda S, Puliyel JM. Ondansetron-induced dystonia, hypoglycemia, and seizures in a child. Ann Pharmacother 2011;45:e7.Epub2010Dec 28.





























