Upload
vczeszyn
View
224
Download
0
Embed Size (px)
Citation preview
8/3/2019 Oncology Pipelines
1/92
www.exanebnpparibas-equities.com
Please refer to important disclosuresat the end of this report.
Bionest Partners Exane BNP ParibasFrdric Desdouits Sbastien Berthon
Stphane Parnis Vincent MeunierAlain Gilbert Valrie Moulle
Claude Allary Franois Schmitt
[email protected] [email protected]
Drug development is increasingly risky
We estimate that the chances of success for cancer products starting clinical trials are 3%, three
times less than in other therapeutic areas (average 10%), and are steadily declining. We calculate
that, statistically, 83 new molecules are due for approval by 2012 whereas only 200 have been
approved to date.
Rising barriers to market access
Oncology is wrongly perceived as a collection of niches accessible to small players; large
companies have a growing advantage. The development of cancer drugs is increasingly complex
and market access ever more difficult. Standards of care are evolving fast and there is a clear first-
mover advantage forcing the development of compounds in several indications at once. This blitz
approach demands ever more expertise, breadth and financing power.
Hope still drives the oncology segment
Due to the high medical need and despite a low success rate and mounting competition, almost
every mid-size or big pharma company has a clinical programme in cancer. Over the last ten years,
the number of molecules tested in cancer has multiplied by 2.4x and 70% of the molecules in phaseII or III are developed by small companies.
Success does not always breed success among European players
Roche will retain its leadership in the next 5-6 years, but challenged by GlaxoSmithKline, the
potential Merck/Schering and, to a lesser extent, Novartis. AstraZeneca and Sanofi-Aventis face a
high generic risk, the latter being in a better situation with a larger and more diverse pipeline.
Newcomers such as Serono, Novo Nordisk, UCB and Merck KGaA stand-alone, will have to gain
critical mass through acquisitions given their limited financing power and the rising cost of
development in oncology.
Oncology Pipelines: Searching is not Finding
Sector review - March 2006
!"#$%&"$ ''()(( ''()((
8/3/2019 Oncology Pipelines
2/92
2 Pharmaceuticals
Contents
Executive summary ______________________________________ 3
Oncology - the gold rush is not over ________________________ 8
Unmet medical need remains high________________________________________ 8
Very active research and development ____________________________________ 9
Knowledge is everywhere: low entry barriers in research _____________________ 12
High prices target unmet medical need _________________________________ 14
Areas left to explore __________________________________________________ 16
Success rates: three times lower than pharma average, and getting worse _______ 19
Developing cancer drugs is all about managing complexity ___ 22
Product positioning with or against competitors ? ___________________________ 22
One bullet for several targets?__________________________________________ 25
Oral drug approaches vs biologicals: who will win? __________________________ 27
Centralised vs decentralised marketing organizations ________________________ 29
No place for slow players ________________________________ 32
A strong first-mover advantage _________________________________________ 32
Price pressure will soon weigh on cancer _________________________________ 39
European oncology players ______________________________ 43
Companies ____________________________________________ 49
Exane BNP Paribas
Sbastien Berthon Valrie Moulle+33 1 44 95 68 61 +33 1 44 95 53 81
[email protected] [email protected]
Vincent Meunier Franois Schmitt
+33 1 42 99 24 42 +33 1 44 95 41 [email protected] [email protected]
Bionest Partners
Frdric Desdouits Claude Allary
+33 1 58 05 14 05 +33 1 58 05 14 [email protected] [email protected]
Stphane Parnis Alain Gilbert
+33 1 58 05 14 21 +33 1 58 05 14 [email protected] [email protected]
8/3/2019 Oncology Pipelines
3/92
3 Pharmaceuticals
Executive summary
Cancer is a growing area of interest in the pharmaceutical industry, in which late-stage
products have doubled in the last ten years. But, according to our calculations, theprobability of success for a phase II product in oncology is close to only 6% and is
declining. Our detailed analysis of more than 800 products currently in pipelines shows
therapeutic areas where innovation will probably rise in the coming years and where
competition will become even stronger. But our understanding is that the barriers to
entry are rising very quickly in favour of large players with strong investment capacities.
At the same time, we find that market conditions are becoming more difficult with a
strong first-mover advantage and mounting price pressure.
Statistics tell us that around 83 products should reach the market by 2012. As there are
around 200 products approved today, either the market will change completely or
success rates will decline sharply.
Looking at European pharmaceutical companies, Roche/Genentech appears to be a
clear future leader. GlaxoSmithKline appears as a potential challenger, together with
Novartis and potentially the merged Merck-Schering group. Sanofi-Aventis and
AstraZeneca are facing generic risks in the foreseeable future, the former having a
broader pipeline to protect its franchise. Newcomers such as Serono, Novo Nordisk, UCB
and Merck KGaA stand-alone, will have to gain critical mass through acquisitions given their
limited financing power and the rising cost of development in oncology.
Cancer: A very active sector in clinical development
Oncology represents about 10% of the current pharmaceutical market but nearly 30%
of the drugs in clinical development and is the primary focus of 20% of the publicly
listed European Biotech companies. The number of drugs in clinical development has
increased 2.4 times in ten years and almost every single mid- to large-sized company
now has an ongoing oncology programme in clinical development.
Several factors have contributed to this onco-boom. On the demand side, although the
average survival after diagnosis has improved dramatically, cancer remains the
second-highest cause of death in developed countries and a strong research effort is
still needed to improve the survival of patients in many cancers. On the feasibility side,
the main factor is certainly the technological advances with the omics revolution and
the understanding of the biology of several cancers, as well as the development of
preclinical models.
The development of the biotechnologies has enabled small companies to identify drug
candidates and develop them up to early clinical stages (phases I/II). We estimate that70% of cancer products tested in humans today are from small Biotech companies.
The reality favours these small companies even more if we include those that have
been acquired by big pharma companies. The numbers are particularly striking for
recombinant proteins (89%) and biological peptides/proteins (84%).
In this report, we review more than 800 molecules in phases II and III and analyse their
characteristics, their expected indications and their owners. We have grouped the
different cancers according to their incidence, the probability of five-year survival and
the intensity of clinical research. As an example, we show the relative number of
products in development in the different pathologies in the following graph.
8/3/2019 Oncology Pipelines
4/92
4 Pharmaceuticals
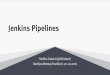
Chart 1: Relation between number of drugs in phase II or III, incidence and 5-yearsurvival
Source: Bionest Partners, Exane BNP Paribas
The factors underpinning the above matrix are analysed in detail in this report. For
instance, below, we have used it to represent the number of molecules that could be on
the market by 2012 in each pathology divided by the number of registered drugs in the
same pathology.
This metric gives us a picture of the intensity of the competition coming from the
pipelines to replace existing drugs. Interestingly, two zones are being investigated more
than others: the Improvable niches and the Challenging niches. Those are the areaswhere the medical need is still high or relatively high and where there are few marketed
drugs. Surprisingly, the lung area does not show up as a very intense zone.
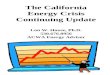
Chart 2: Relation between number of projected new drugs and marketed drugs
Breast
Leukemias
Lymphoma and multiple myeloma
Ovarian
Tracheal bronchus lung
Colorectal
Testicular
Prostate
Renal
Pancreas
Bladder
Head & Neck
Corpus uterus
Skin and Melanoma
Liver
Stomach
Cervix uteri
Brain
Oesophagus
0
50
100
1 10 100 1000
Incidence (Log scale)
5ysurviva
l
THE BIG CHALLENGE
BIG AND CROWDED
COVERED NICHE
CHALLENGING NICHE
Satisfying
treatment
High
unmet
need
Low population High population
CROWDED WITH UNMET NEED
IMPROVABLE NICHES
1 new projected drug
for 2 existing drugs
Source: Bionest Partners, Exane BNP Paribas
LateStagePipeline
Breast
Leukemias
Ovarian
Tracheal bronchus lung
Testicular
Prostate
Pancreas
Corpus uterus
Skin and Melanoma
Liver
Stomach
Cervix uteri
Lymphoma and multiple myeloma
Colorectal
Brain
Renal
Bladder
Head & Neck
Oesophagus
0
50
100
1 10 100 1000
Incidence (log scale)
5ysurvival
THE BIG CHALLENGE
BIG AND CROWDED
COVERED NICHE
CHALLENGING NICHE
Satisfying
treatment
High
unmet
need
Low population High population
CROWDED WITH UNMET NEED
IMPROVABLE NICHES
15 projects
8/3/2019 Oncology Pipelines
5/92
5 Pharmaceuticals
Success rates: three times lower than pharma average, and getting
worse
We have calculated attrition rates in oncology by following the compounds entering
phase 1, 2 or 3 each year since 1996. As shown below, oncology drug candidates have
much lower average success rates than other therapeutic areas in late stagedevelopment (phases 2 and 3).
A cancer product entering phase II has about a 6% chance of making it to market
(industry average: 16%) and around 3% when it is entering phase I (industry average:
10%).
We have calculated, based on our estimated attrition rate, the number of molecules
that could reach the market by 2012 (molecules that are already in phase II). We
estimate that around 83 new molecules should be launched while there are only
around 200 approved today.
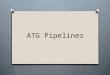
But this calculation might turn out to be overly optimistic as we believe success rates
are declining in oncology. Between 1996 and 2000, the cumulative success rates from
first-in-man to registration decreased by 23%, from 4.1% to 3.2%. This increasing
failure rate is due to a sharp decline in phase II productivity and, to a lesser extent, to
phase III productivity.
Chart 3: Change of success rate in oncology by phase of development between1996 and 2000
45.1%
38.3%41.7%
57.1%
4.1%
52.2%
21.0%
34.8%
83.3%
3.2%
0%
20%
40%
60%
80%
100%
Phase I Phase II Phase III Pre-registration Phase I to launch
Successrate
1996 2000
+46%
+16%
-45% -17%
-23%
Source: Bionest Partners, Exane BNP Paribas
Developing cancer drugs is about managing complexity
Oncology is one of the main science-driven specialties in medicine, with highly
technical products and complex patient management. This makes research in this area
particularly complex and unpredictable. To make matters worse, many teams are
competing not only on similar targets but also on different approaches to the same
targets (for instance, chemicals and biologicals on certain membrane receptors) and on
different approaches to the same disease (for instance, there are 92 molecules in
phase II and III in breast cancer).
8/3/2019 Oncology Pipelines
6/92
6 Pharmaceuticals
To balance the risk of development and because the understanding of the biology has
increased significantly, companies are now trying to test their compounds in several
indications in parallel. But this strategy makes development highly complex as standard
therapies are evolving very quickly and are sometimes becoming fragmented, i.e. there
can be several equivalent treatment options for the same patient. The products are now
often developed with competitors products and can sometimes strengthen competitors
positions.
This makes it difficult to define a marketing strategy as how the clinical trials are
designed includes a portion of the risk in the choice of the reference treatment and
requires a close and sustained presence in hospitals and with key opinion leaders. At
the same time, clinicians profiles are also changing, evolving into a more prominent
role for organ specialists versus traditional oncologists. As a consequence, cancer
marketing and sales forces will have to adapt to physicians with a less academic profile
and deliver a more GP-oriented marketing promotion.
Tougher market conditions
There is clearly a strong first-mover advantage in cancer, as illustrated by the taxane,
aromatase inhibitors and LHRH agonists markets, where the first entrant maintained a
50-70% market share against its competitors. This requires that products be clearly
differentiated within the scope of approved indications, in terms of organs and
therapeutic lines, and also that these indications be obtained as fast as possible.
Given the increasing competition in cancer research, being first to market requires very
fast development. As a result, companies have adapted their approach with what we
call the blitz strategy, which consists of testing new drugs in parallel in a large number
of indications and sometimes in several settings. A good example presented in this
report is Avastins clinical development. The emergence of this strategy contrasts with
the more traditional step-by-step Domino strategy, presented in this report with the
Rituxan example.
The very high unmet medical needs of the cancer market have thus far allowed
companies to obtain high prices for their drugs, but this will not last forever. Two factors
will contribute to the growing pressure on the prices of cancer drugs in particular: 1) the
very fast growth of spending for cancer treatments as part of total healthcare spending
and 2) increased competition amongst a higher number of players. Some price
pressure is already at work through an increasing use of generics, as is the case in
other therapeutic areas.
European cancer players: who will win?
We have analysed how European cancer players (AstraZeneca, GSK, Merck KGaA,
Novartis, Roche, Sanofi-Aventis and Schering AG) are positioning themselves to tackle
the opportunities and challenges of the cancer market over the next five years and howtheir positions will evolve.
We have identified four success factors: in-licensing attractiveness, size of the pipeline
vs size of the current cancer franchise, diversity of therapeutic approaches and
exposure to generic risk.
Table 1: Winners/losers by success factor
Success factor Strong position Weak position
In-licensing attractiveness Roche, Sanofi-Aventis, AstraZeneca, Novartis Serono, Novo Nordisk, UCBPipeline depth vs current franchise Roche, GSK, Merck/Schering AstraZenecaDiversity of therapeutic approaches Roche, GSK, Sanofi-Aventis AstraZeneca, Serono, Novo Nordisk, UCBExposure to generic risk Roche, Merck/Schering, Serono, Novo Nordisk, UCB Sanofi-Aventis, AstraZeneca
Source: Company, Bionest Partners, Exane BNP Paribas
8/3/2019 Oncology Pipelines
7/92
7 Pharmaceuticals
The superstar is Roche/Genentech, which is in a strong position in all four success
factors. GlaxoSmithKline and Merck/Schering (if the combination is successful) are
the rising stars. Novartis should maintain its recently developed cancer franchise.
AstraZeneca is in the toughest situation, with high generic risk and a concentrated
pipeline. Maintaining its leadership in cancer will require higher-than-average success
rates and possibly acquisitions. Sanofi-Aventis also faces a challenge given its
generic risk exposure, but enjoys a deeper and more diversified pipeline than
AstraZeneca.
For the newcomers, Serono, Novo Nordisk and UCB, it will take time and major
investments to build a cancer franchise. Given their limited financing power and the
rising costs of development, gaining scale through acquisitions will likely be necessary
to be successful in this segment.
Chart 4: Cancer franchise in 2005 vs potential new drug launches by 2011
GSKMRK
NOVN
ROG
SAVE
SCH
AZN
NOVOUCB SEO
MRK-SCH Newco
0
2
4
6
8
10
0.0 0.5 1.0 1.5 2.0 2.5 3.0 3.5
Number of projected new drugs
2005cancersales(USDbn)
Rising stars
Declining players
Super star
Emerging players
Established players
Source: Bionest Partners, Exane BNP Paribas
8/3/2019 Oncology Pipelines
8/92
8 Pharmaceuticals
Oncology - the gold rush is not over
Unmet medical need remains high
The oncology market, which accounted for nearly 10% of the global pharmaceutical
market in 2005, is expected to keep on growing faster than the rest of the industry with
average annual turnover growth of around 10% in the coming years. This growth will be
driven by the development of new blood cell factors, targeted therapies and novel
chemotherapeutics. According to the National Cancer Institutes estimates, cancer
treatment cost around USD70bn in the USA in 2004 and has grown 75% over the last ten
years.
Chart 5: Evolution of worldwide market for oncology
0
20
40
60
80
2004 2009e
Oncologydrugsales(USDbn)
CAGR: +10%
Source: Bionest Partners, Exane BNP Paribas
Despite the stabilisation of incidence rates and the steady increase of survival rates for
some tumours (i.e. prostate, breast, colorectal), cancer remains one of largest cause of
deaths in industrial nations. Cancer is the second cause of mortality in the USA, with
approximately 570,000 deaths and 1.4m new cases diagnosed in 2005. However, the
survival and incidence rates vary strongly according to the site of the cancer, as shown
in the following chart.
Prostate, breast, lung and colorectal cancers are still the most common forms. In 2005,
they accounted for more than half of all new cancers. It was projected that there would
have been 1,372,910 new cancer cases in 2005, 17% of which would have been
prostate cancer; 15% female breast cancer, 13% lung cancer and 11% cancer of the
colon. Although therapies for prostate and breast cancer have helped increase
five-year survival rates, it is not the case for pulmonary and pancreatic cancers.
8/3/2019 Oncology Pipelines
9/92
9 Pharmaceuticals
Chart 6: Five-year survival and incidence rates of cancers
Breast
Prostate
Renal
Bladder
Testicular
Lung
Leukaemia
Lymphoma and
multiple myeloma
Pancreas
StomachLiver and biliary
Colorectal
Uterine
Cervical
Ovarian
Head & neck
Brain
Melanoma
Oesophagus
0
10
20
30
40
50
60
70
80
90
100
1 10 100 1,000
Incidence (per 100,000)
5ysurvival
Breast
Prostate
Renal
Bladder
Testicular
Lung
Leukaemia
Lymphoma and
multiple myeloma
Pancreas
StomachLiver and biliary
Colorectal
Uterine
Cervical
Ovarian
Head & neck
Brain
Melanoma
Oesophagus
0
10
20
30
40
50
60
70
80
90
100
1 10 100 1,000
Incidence (per 100,000)
5ysurvival
Source: American Cancer Society, National Cancer Institute
Very active research and development
Between 1995 and 2005, the number of oncology products under development
(corresponding to phase I, II or III clinical trials) increased by 138% from 299 to 713.
This increase was approximately 1.5x higher than the overall pharmaceutical pipeline
growth, which rose by 88% from 1,268 drug candidates to 2,375 during the same
period. The oncology pipeline particularly increased in phase II and phase III.
Chart 7: Oncology and pharmaceutical pipeline growth between 1995 and 2005
Pharmaceutical pipeline* Oncology pipeline
0
200
400
600
800
1,000
Ph I Ph II Ph III
Numberofdrugs
1995 2005
+172%
+247%
+111%
0
100
200
300
400
Ph I Ph II Ph III
Numberofdrugs
1995 2005
+239%
+229%
+160%
* Oncology products are excluded from the pharmaceutical pipeline
Source: Pharmaprojects
8/3/2019 Oncology Pipelines
10/92
10 Pharmaceuticals
Oncology: roughly a quarter of the scientific interest
Several of the factors that we have analysed highlight the great interest in oncology
and the importance of research in this therapeutic area (scientific publications,
preclinical alliances, intensity of research in biotech companies, etc.).
Firstly, at the research level, oncology is the main focus of interest. Between 2000 and
2005, oncology was the subject of almost 40% of scientific publications and was
awarded almost twice as much print space than cardiovascular disease, the second
most investigated therapeutic area.
Chart 8: Scientific publications by therapeutic area for the 2000-2005 period
Cardiovascular
diseases
23%
Infectious diseases
16%
Neurodegenerative
diseases
14%
Metabolic diseases
8%
Oncology
39%
Publication distribution over the period 2000-2005 was obtained using the Pubmed database and its Meshsearch engine. This system allows a wide research with occurrences based on concepts
Source: Pubmed
Oncology is believed to represent 25%-33% of all the alliances and preclinical
transactions in the sector. Of the 152 firms currently listed EU biotech companies
analysed, 20% have a clear focus on oncology (33 firms) and account for roughly 25%
of the market capitalisation.
Oncology research benefited strongly from omics
In our view, the oncology pipeline boom in the mid-1990s is a direct result of scientific
and technological improvements that occurred in the early-1990s. We have identified
several factors that have driven oncology pipeline growth:
development of "omics" technologies in the 1990s, resulting in the identification of
many novel potential therapeutic targets. Genomic and proteomic development were
made possible by molecular biology improvements and have strongly contributed to the
identification/development of new therapeutic mechanisms (i.e. apoptosis,
anti-angiogenesis, pathway inhibition, etc.);
improvements to chemical synthesis, molecule library and formulation have
motivated high throughput screening of molecules and lead identifications;
advances in preclinical and toxicity studies have enabled more molecules to be
turned into medicines;
progress in the characterisation and production of biological molecules has
accelerated the emergence of very promising molecule types, such as monoclonal
antibodies and recombinant proteins.
8/3/2019 Oncology Pipelines
11/92
11 Pharmaceuticals
Chart 9: New cancer drug compounds and uses approved per year (1949- 2005)
New cancer drug compounds approved per year New cancer drug uses approved per year
0
2
4
6
8
10
12
14
16
18
20
1949
1957
1965
1973
1981
1989
1997
2005
0
2
4
6
8
10
12
14
16
18
20
1949
1957
1965
1973
1981
1989
1997
2005
Source: FDA, Bionest Partners, Exane BNP Paribas
This wave of innovations led to the late-1990's clinical evaluation of many novel agents
that targeted growth factor receptors and signal transduction pathways: the targeted
therapies. At this time, there was massive therapeutic potential. It was assumed that
these agents would be so specific that their effects would be limited to cancer cells and
spare normal cells. It was also assumed that these drugs would be so effective that
they would largely supplant non-specific cytotoxic agents.
Over a decade later, broad-acting therapies remain. They account for 35% of total drugcandidates under phase II or III whereas targeted therapies represent 39%.
Chart 10: Breakdown of current phase II and phase III drugs by therapeutic class
Phase II products Phase III products
Antimitotic/Cell-
cycle modulator
36
12%
Other anticancer
agent
15
5%
Hormonal
modulator
17
6%
Pathway inhibitor/
Apoptose
activator
42
14%
Antimetabolite
36
12%
Alkylating
7
2%
Angiogenesis
inhibitor
20
7% Therapeutic
vaccine
29
10%
Other cytotoxic
agent
18
6%
Immunomodula-
tor
46
17%
Radio/chemosen-
sitizer
11
4%
Prophylactic
vaccine
1
0%
Radio/chemopro-
tective
14
5%
Antimitotic/Cell-
cycle modulator
8
13%
Other anticancer
agent
3
5%
Hormonal
modulator
4
6%
Pathway
inhibitor/
Apoptose
activator10
15%
Antimetabolite
3
5%
Alkylating
3
5%
Angiogenesis
inhibitor
3
5%
Therapeutic
vaccine
8
12%
Other cytotoxic
agent
7
11%
Immunomo-dulator
4
6%
Radio/chemosen-
sitizer
6
10%
Prophylactic
vaccine
1
2%
Radio/chemopro-
tective
3
5%
Light-grey: broad-acting; dark-grey: targeted therapies
Source: Bionest Partners, Exane BNP Paribas
It appears that there is still strong interest in broad-acting therapies as opposed to
targeted ones.
8/3/2019 Oncology Pipelines
12/92
12 Pharmaceuticals
Knowledge is everywhere: low entry barriers inresearch
Targeted therapies are changing the landscape of cancer treatment and are likely to be
used for the majority of cancer patients within five to ten years, according to the
specialists we interviewed. One direct outcome of the development of targeted
therapies is the paradigm change occurring in oncology: cancer is transforming from a
uniform collection of organ-based diseases into subsets of biologically differentiated
patients. This change is fuelled by the greater understanding of the molecular
mechanisms of cancerogenesis that leads to a development of large variety of
therapeutic approaches.
In this context, many therapeutic strategies are pursued to cure a same cancer type,
spreading knowledge between many players and thereby increasing competition.
The following chart shows that biotechs are fuelling oncology innovation more than
ever. Over 70% of drugs currently under development in phase II or III clinical trials
come directly from biotech labs. In reality even more come from small companies assome of them have been acquired by big players and therefore their research effort is
accounted as if it had been discovered in a big pharma laboratory.
The early development of some molecule types could be tagged "biotech specific". For
example, 89% of recombinant proteins or 84% biological peptides/proteins currently
under phase II/III clinical trials have been discovered by a biotech company,
highlighting the specific positioning of biotech for biological development.
Chart 11: Contribution of biotech companies to innovation in oncology
Originator of current phase II/III drugsBreakdown of phase II/III drugs by molecule type andoriginator
Chemical71%
Synthetic
peptide
5%
Monoclonal
antibody
12%
Gene therapy
1%
Biological
peptide/
protein
1%
Other
2%Recombi-
nant protein
8%
80
6
1
14
9
1
2
159
15
8
36
35
14
9
16
17
0% 20% 40% 60% 80% 100%
Chemical
Synthetic peptide
Biological peptide/protein
Monoclonal antibody
Recombinant protein
Cellular therapy
sIRNA
Gene therapy
Other
Pharma Biotech
Of the 360 drugs under phase II or III development we analysed, 268 (75%) come from biotech labs whereas 88 (
8/3/2019 Oncology Pipelines
13/92
13 Pharmaceuticals
All major pharma players are betting on oncology
We have analysed the late-stage pipelines (phase II and phase III portfolios) of major
pharmaceutical players. The facts are striking; all major players have drugs under
development for oncology.
The following chart illustrates that chemicals still represent the majority of drug
candidates. However, some companies are absent from the chemical arena: mainly
biotech-like companies such as Biogen Idec, UCB or Novo Nordisk, but surprisingly
one large company is also missing, Merck & Co.
On the other hand, some other companies have a "purely" chemical approach like
AstraZeneca or Wyeth.
Chart 12: Development programmes of the major oncology players by nature of product
0 5 10 15 20 25 30 35 40 45 50
Abbott
AEterna Zentaris
Amgen
AstraZeneca
Baxter International
Bayer
Biogen Idec
Bristol-Myers Squibb
Eli Lilly
Genzyme
GlaxoSmithKline
Johnson & Johnson
MedImmune
Merck & Co
Merck KGaA
Novartis
Novo nordisk
Pfizer
Pierre Fabre
Roche/Genentech
Sanofi-Aventis
Schering AG
Schering-Plough
Serono
UCB
Wyeth
Chemical Peptide/protein Cellular therapy Gene therapy Monoclonal ant ibody Others
Source: Bionest Partners, Exane BNP Paribas
8/3/2019 Oncology Pipelines
14/92
14 Pharmaceuticals
High prices target unmet medical need
We believe that the prices of cancer drugs follow the same overall rules as for other
therapeutic areas. Efficacy and medical need are the two main criteria driving prices.
Based on the assumption that it is mainly drugs targeting unmet medical diseases that
are subject to accelerated approvals, we assessed the links between accelerated
approval gain and the price of the drug. In order to do so, we examined a study
conducted by the NCI and Bethesda NIH demonstrating that the average wholesale
price (AWP) obtained by the 22 cancer drugs approved by the FDA between December
1992 and June 2003 amounted to USD17,488 per cycle of treatment1.
Table 2: Price of 22 oncology products approved by the FDA between 1993 and 2004
Product Molecule Molecule type Therapeutic class Company Date of FDAapproval
Months Acceleratedapproval
AWP / cycle(USD)
Bexxar Tositumomab* Monoclonal antibody Pathway inhibitor /Apoptose activator
GlaxoSmithKline 7 Jun. 03 64 Yes 32,400
Velcade Bortezomib* Chemical Pathway inhibitor /Apoptose activator
Millenium 13 May 03 89 Yes 3,378
Iressa Gefitinib Chemical Pathway inhibitor /Apoptose activator
AstraZeneca 5 May 03 105 Yes 1,747
Eloxatin Oxaliplatin Chemical Alkylating Sanofi Aventis 9 Aug. 02 116 Yes 6,424
Zevalin Ibritumomab Monoclonal antibody Pathway inhibitor /Apoptose activator
Schering AG 19 Feb. 02 46 Yes 30,662
Glivec Imatinib Chemical Pathway inhibitor /Apoptose activator
Novartis 18 Apr. 01 59 Yes 2,290
Campath Alemtuzumab* Monoclonal antibody Pathway inhibitor /Apoptose activator
Genzyme /Schering AG
5 Jul. 01 90 Yes 199,332
Trisenox Arsenic trioxide Chemical Pathway inhibitor /Apoptose activator
Cephalon 25 Sep. 00 13 No 19,743
Mylotarg Gemtuzumab Monoc lonal antibody Pathway inhibitor /
Apoptose activator
Wyeth 17 May 00 160 Yes 15,723
Temodar Temozolomide Chemical Alkylating Schering Plough 11 Aug. 99 105 Yes 11,029
Valstar Valrubicin Biologicalpeptide/protein
Antibiotic Anthra 25 Sep. 98 219 No 13,296
Herceptin Trastuzumab* Monoclonal antibody Antimitotic/Cell-cyclemodulator
Roche/Genentech 25 Sep. 98 28 No 3,672
Xeloda Capecitabine Chemical Antimetabolite Roche/Genentech 30 Apr. 98 113 Yes 1,470
Mabthera /Rituxan
Rituximab* Monoclonal antibody Pathway inhibitor /Apoptose activator
Roche/Genentech 26 Nov. 97 66 No 15,048
Intron A Interferon a2b recombinant protein Immunomodulator Schering Plough 6 Nov. 97 103 No 3,570
Camptosar Irinotecan Chemical Antimitotic/Cell-cyclemodulator
Pfizer 14 Jun. 96 106 Yes 5,100
Hycamtin Topotecan* Chemical Antimitotic/Cell-cyclemodulator
GlaxoSmithKline 28 May 96 90 No 3,000
Gemzar Gemcitabine Chemical Antimetabolite Lilly 15 May 96 107 No 3,591Taxotere Docetaxel* Chemical Antimetabolite Sanofi Aventis 14 May 96 106 Yes 3,580
Vesanoid Tretinoin* Chemical Other anticanceragent
Roche 22 Nov. 95 39 No 6,925
Leustatin Cladribine* Chemical Antimetabolite Johnson &Johnson
26 Feb. 93 71 No 2,268
Taxol Paclitaxel Chemical Antimitotic/Cell-cyclemodulator
BMS 29 Dec. 92 165 No 1,945
* Products with the shortest approvable time; AWP (Average Wholesale Price) per unit and per cycle (man 1.7m tall, weight of 75kg, body surfacearea of 2m) ; Prices taken from the US Red Book, except for Paclitaxel and Cladribine for which reference prices come from the US Blue Book(prices of the generics)
NB. The authors excluded growth factors (pegfilgrastim, darbopoietin) and hormonal modulators (anastrozole) from the scope of their analysis,although they were approved during the period
Source: Journal of Clinical Oncology, December 2005, American Cancer Society, Bionest Partners, Exane BNP Paribas estimates
1Nevertheless, there are significant disparities between products. For example, the price obtained for Xeloda (Roche) was USD1,470 per cycle vs a
massive USD199,332 per cycle for Campath (Schering AG / Genzyme)
8/3/2019 Oncology Pipelines
15/92
15 Pharmaceuticals
The authors proved a link between the price obtained and the time required by the FDA to
give its green light. Among the approved drugs, the 11 fastest approvals during the period
(59 months on average) obtained an AWP of USD28,975 per cycle, and USD6,791 per
cycle when eliminating the two radio-labelled monoclonal antibodies Bexxar and Zevalin
(for which the very high prices integrate some logistics costs and are therefore hardly
comparable). This level of price was significantly higher than for the 11 slowest drugs
(127 months on average, with an average price of USD6,000 per cycle).
Several observations reinforce this view:
the price is not directly l inked to the incidence of the cancer: a rare cancer does not
automatically deserve a high price. However, the relation between price and incidence
appears clearer for biologics (indicated by a circle in the chart below) than for
chemicals;
product prices are more or less in a defined range for each indication;
there is no clear link between the range, the date of approval, the chemical/biologic
origin or the therapeutic class of the products.
Chart 13: Price and cancer incidence relation for chemicals and biologics
Iressa
Eloxatin
Trisenox
Temodar
Valstar
Camptosar
Hycamtin
Vesanoid
Taxol
Mylotarg
Erbitux
Mabthera/Rituxan
SutentNexavar
Herceptin
Velcade
Glivec
Xeloda
Gemzar
LeustatinAlimta
Tarceva
Avastin
Taxotere
0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
16,000
18,000
20,000
0 20 40 60 80 100 120 140
Incidence of approved indication
Average
Who
lesa
lePrice
(USD)
Colorectal
Lung cancer
Breast
We compared the prices of 25 cancer drugs approved from 1992 to 2005 vs the incidence of their cancerindication. In addition to the list of drugs used by NCI and NIH researchers, we included six drugs that wereapproved more recently: Erbitux (cetuximab, Merck KGaA), AWP per cycle USD7,800; Alimta (pemetrexed,Lilly), AWP per cycle USD1,912; Avastin (bevacizumab, Roche / Genentech), AWP per cycle USD4,523;Tarceva (erlotinib, Roche / Genentech, AWP per cycle USD1,772; Sutent (sunitinib, Pfizer) , AWP USD4,725 permonth; Nexavar, AWP USD4,333 per month
Source: American Cancer Society, US red book, Bionest Partners, Exane BNP Paribas estimates.
but pricing is under scrutiny
Cancer drugs are expected to be under pressure in the future. This is a general trend
affecting the whole of the pharmaceutical industry, since healthcare cost containment
policies have been conducted in most industrialised countries. Two factors will
contribute to the growing pressure on prices: 1) the very fast growth of cancer
treatment spending as part of the total healthcare spending; and 2) increased
competition amongst a greater number of players.
Price pressure is already at work through an increasing use of generics, like in other
therapeutic areas. On the one hand this would leave room for branded drugs, allowing
expensive biologics and pathway inhibitors to resist. But on the other hand, the
increase in patient access to these new therapies will not permit healthcare systems
public or private to sustain such levels a long time.
8/3/2019 Oncology Pipelines
16/92
16 Pharmaceuticals
Areas left to explore
We tried to assess the link between the number of products, the frequency of cancer
and the medical need. We therefore compared the number of drugs by therapeutic area
with the incidence and five-year survival rates (see following charts). Our approachconsidered both marketed drugs and molecules in late-stage clinical evaluation (under
phase II or phase III).
We identified six main segments of the cancer market, illustrated on matrix.
1) Big and crowded market segments: breast, prostate
This first market segment is the most important in terms of approved drugs, and offers
high margins pharma companies: incidence and survival rates are sufficiently high to
permit long-term use for an important number of patients.
Breast and prostate cancers have comparable incidence and five-year survival rates,
but there are slightly more drugs available for the former. One reason could be thathormone therapy, surgery (orchiectomy) and cryotherapy provide good stabilisation
prospects for the male patients.
On the pipeline side, the high number of drugs under development for breast cancer
suggests that the prospects for oncology players to develop efficient molecules
showing reduced side-effects are still attractive. The situation is obviously different for
prostate cancer since only one large pharmaceutical player has a molecule for this
indication in phase III (Roche: Avastin).
2) Crowded segment, but with unmet need: leukaemia, lymphoma, ovarian, colorectal
This segment comprises cancers with treatments already available but which still pose
a challenge as five-year survival rates remain low. Leukaemia and lymphoma, with the
highest number of approved drugs, and ovarian cancer belong to this segment. The
latter is the second-most crowded gynaecological cancer, after breast cancer.
Although the incidence rates for colorectal cancer are relatively high, we have included
it in this segment as five-year survival rates are still low. On the pipeline matrix, we can
see that these indications still stimulate players, and could fuel competition on these
markets in coming years.
3) Covered niche market segments: testicular, melanoma
This segment comprises testicular and melanoma cancers associated with high
survival rates and a relatively high number of available drugs. However, some
differences need to be highlighted between these two pathologies.
As testicular cancer patients appear to benefit from efficient therapies, it is not
surprising to see so few products under clinical evaluation.
The situation is different in melanomas. Although excision is the treatment of choice,
about 18% of melanomas are metastatic and remain difficult to cure because of
regional and distant metastases, in which survival rates are 60% and 14% respectively.
The outlook for patients with metastatic melanoma continues to be poor since chemo-
or immune therapies are associated with response rates of 10%-15% and median
survival of about one year.
8/3/2019 Oncology Pipelines
17/92
17 Pharmaceuticals
4) Improvable niche market segments: five cancer types
In this segment, we can identify a series of cancers with a surprisingly low number of
products, despite incidence / survival profiles comparable to more crowded therapeutic
areas: head & neck, renal, cervix uteri, bladder and corpus uterus. It is interesting to
note that competition in renal cancer has increased since the very recent approval ofPfizers Sutent and Bayer Sorafenib.
This indication is an entry-point in the battle-field before an extension to the "big and
crowded" area where Avastin is currently dominating development (see case study for
more details).
The limited number of drugs for cervix uteri and corpus uterus cancers is partially due
to the large occurrence of surgery procedures in this domain. As such, it is not
surprising to see that very few molecules under development for uterine cancer and
cervix uteri.
As a result we believe that bladder cancer is a sweet spot for newcomers in the cancer
arena as surgery procedures seem to be less frequent than for cancers of the uterus
and cervix. The low number of drugs under development for this indication reinforces
our impression.
5) Challenging niche market segments: five cancer types
This segment groups a series of cancers with relatively low incidence and five-year
survival rates and a limited number of approvals: pancreas, liver, stomach, oesophagus
and, to a lesser extent, brain cancer. We believe this is clearly the consequence of a
choice based on pharmaco-economic considerations. These niche cancers could
theoretically interest newcomers or small players, as the medical need is huge. The
main challenge remains the poor survival rates, making it difficult to prove a therapeutic
efficacy.
However, we believe that pancreas cancer could become a highly competitive segmentin a near future. Many large players have molecules targeting this indication and the
number of products under clinical evaluation is increasing.
6) The big challenge: lung cancer
Tracheal bronchus lung cancer is one of the most frequent indications, with one of the
lowest five-year survival rates, explaining the high number of products approved. It is
worth noting that lung cancer frequency is sharply increasing notably due to smoking
habits and is one of the pathologies with the poorest prognosis. As a result, high
competition and poor improvement from existing drugs make this therapeutic area one
of the most difficult to address, but also one of the most potentially profitable. Because
the disease has usually spread by the time it is discovered, radiation therapy and
chemotherapy are often used, sometimes in combination with surgery.
8/3/2019 Oncology Pipelines
18/92
18 Pharmaceuticals
Chart 14: Relation between number of drugs approved, incidence and 5-yearsurvival
Source: Bionest Partners, Exane BNP Paribas
Chart 15: Relation between number of drugs in phase II or III, incidence and5-year survival
Source: Bionest Partners, Exane BNP Paribas
To address the future evolution of the different therapeutic classes, we have assumed
that the attrition rates (see next section) were the same in all of the segments and
calculated the average number of molecules that could reach the market in each
segment. We have then divided this by the number of marketed molecules in each
segment. This metric gives us an indication of the intensity of the competition that the
existing drugs face from the pipelines.
Interestingly, two zones are more investigated than others: the "improvable niches" and
the "challenging niche". Those are the areas where the medical need is still high or
relatively high and where there are little players. Surprisingly, the lung area does not
show up as a very intense zone.
Market Leukemias
Lymphoma and multiple myeloma
Breast
Prostate
Ovarian
Colorectal
Skin and Melanoma
Liver
Corpus uterus
Stomach
Bladder
Pancreas
Cervix uteri
Oesophagus
Testicular
Brain
Renal
Head & Neck
0
50
100
1 10 100 1000
Incidence (log scale)
5ysurvival
THE BIG CHALLENGE
BIG AND CROWDED
COVERED NICHE
CHALLENGING NICHE
Satisfying
treatment
High
unmet
need
Low population High population
CROWDED WITH UNMET NEED
IMPROVABLE NICHES
1 approval
LateStagePipeline
Breast
Leukemias
Ovarian
Tracheal bronchus lung
Testicular
Prostate
Pancreas
Corpus uterus
Skin and Melanoma
Liver
Stomach
Cervix uteri
Lymphoma and multiple myeloma
Colorectal
Brain
Renal
Bladder
Head & Neck
Oesophagus
0
50
100
1 10 100 1000
Incidence (log scale)
5ysurvival
THE BIG CHALLENGE
BIG AND CROWDED
COVERED NICHE
CHALLENGING NICHE
Satisfying
treatment
High
unmet
need
Low population High population
CROWDED WITH UNMET NEED
IMPROVABLE NICHES
15 projects
8/3/2019 Oncology Pipelines
19/92
19 Pharmaceuticals
Chart 16: Relation between number of projected new drugs and marketed drugs
Breast
Leukemias
Lymphoma and multiple myeloma
Ovarian
Tracheal bronchus lung
Colorectal
Testicular
Prostate
Renal
Pancreas
Bladder
Head & Neck
Corpus uterus
Skin and Melanoma
Liver
Stomach
Cervix uteri
Brain
Oesophagus
0
50
100
1 10 100 1000
Incidence (Log scale)
5ysurvival
THE BIG CHALLENGE
BIG AND CROWDED
COVERED NICHE
CHALLENGING NICHE
Satisfying
treatment
High
unmet
need
Low population High population
CROWDED WITH UNMET NEED
IMPROVABLE NICHES
1 new projected drug
for 2 existing drugs
Source: Bionest Partners, Exane BNP Paribas
Success rates: three times lower than pharma average,and getting worse
Several examples of promising drugs that have encountered regulatory setbacks
indicate the challenges that oncology drug candidates must face. Our analysis shows
that success rates in the development of cancer drugs are three times lower than for
the rest of the industry, and getting worse.
We have calculated attrition rates in oncology. As shown below, the average success
rates of oncology drug candidates are much lower than other therapeutic areas in
late-stage development; phase II and III.
A cancer product entering phase II has about a 6% chance of getting to the market (industry
average: 16%) and around 3% when it is entering phase I (industry average: 10%).
Chart 17: Success rate by phase of development and by therapeutic area
52%
21%
35%
83%
60%
29%
40%
70%
60%
39%
56%
74%
0%
20%
40%
60%
80%
100%
Phase I Phase II Phase III Registration
Successra
te
Oncology (Exane BNPP & Bionest Partners)Oncology (Nature Reviews)Pharma sector (Nature Reviews)
Source: Nature reviews (success rates were determined by the analysis of the success and failure of top ten bigpharma portfolios during 1991-2000), Bionest Partners (based on Pharmaprojects database with productsentered in phase II, II and III in 2000), Exane BNP Paribas
8/3/2019 Oncology Pipelines
20/92
20 Pharmaceuticals
Several factors may explain the low success rates of oncology drug candidates.
On the research side, there are more and more novel approaches to anti-cancer drug
development. For example, more than 40% of cancer drugs under development are
directed against novel mechanisms, and almost 70% of the drug targets that are being
investigated in discovery are innovative. The price to pay for innovation is the risk
attached to it;
There is also a relative lack of adequate preclinical models and translatable preclinical
biomarkers in oncology, which, in some other therapeutic areas, are relied on for early
target validation. In addition, there is often a lack of robust biomarkers that can be used
to obtain proof of concept and gauge whether meaningful therapeutic targeting is
occurring in early-stage clinical evaluations. This is particularly true for drug candidates
targeting innovative mechanisms;
More broadly, oncology is one of the disease areas where the phase II results are of a
different nature than the one necessary for registration. In phase II, products usually
prove their toxicity toward the tumour and the end point is usually the size of thetumour. The fine-tuning is to find an active toxic dose which not too toxic for the rest of
the body. In phase III, the drug is challenged on its global biological impact and the end
point becomes disease free survival or survival, a much more complex outcome.
An illustration of the higher bar and the increase in the length of clinical trials is in
advanced colecteral cancer, in which improvements coming from new therapies are
making the work harder for new players.
Chart 18: Goals in the treatment of Advanced colorectal cancer
Source: Sanofi-Aventis
Many new molecules are expected to be launched
As we have mentioned, a cancer product entering phase II has about a 6% chance of
getting to the market and around 3% of entering phase I.
We have calculated, based on our estimated attrition rate, the number of molecules
that could reach the market by 2012 (molecules that are already in phase II). We
estimate that around 83 new molecules will be launched while there are "only" around
200 approved today.
But, this makes sense only if the attrition rates measured today remain stable with time.
8/3/2019 Oncology Pipelines
21/92
21 Pharmaceuticals
Table 3: Estimates of the total number of new molecules reaching the market
Tumour site Number ofphase II
programmes
Number ofphase III
programmes
Total numberof late stageprogrammes
No. of moleculesreaching the market
by 2012
Numberof currently
approved drugs
Breast 79 13 92 8.6 42
Leukaemia 50 9 59 5.6 42Lymphoma and multiple myeloma 57 15 72 7.8 22Ovarian 46 7 53 4.8 12Tracheal bronchus lung 114 15 129 11.3 18Colorectal 62 7 69 5.8 12Testicular 1 0 1 0.1 10Brain 36 4 40 3.3 6Prostate 86 9 95 7.8 12Renal 40 5 45 3.9 6Pancreas 48 9 57 5.5 3Bladder 12 3 15 1.6 3Head & Neck 24 4 28 2.6 3Corpus uterus 5 5 0.3 2Skin and Melanoma 61 8 69 6.0 9Liver 23 5 28 2.8 2Stomach 12 2 14 1.3 3Oesophagus 8 4 8 1.6 1Cervix uteri 13 3 16 1.7 1
Total 777 122 895 83 209
Source: Pharmaprojects, Bionest Partners, Exane BNP Paribas
Success rates are declining in oncology
We have measured success rates in oncology by following each and every new
molecule entering phase I, II or III since 1996. We have analysed the development of
773 drug candidates. On average, compounds spent around three years in phase II
and two in phase III, therefore our analysis stopped with products entered in respective
phases in 2000 (the numbers obtained with the 2001 cohort are similar to 2000).
To illustrate our methodology: the success rate for phase I products in 1996 was
determined by following all of the drugs that entered in phase I in 1996 over a number
of years.
Chart 19: Change of success rate in oncology by phase of development between1996 and 2000
45.1%
38.3%41.7%
57.1%
4.1%
52.2%
21.0%
34.8%
83.3%
3.2%
0%
20%
40%
60%
80%
100%
Phase I Phase II Phase III Pre-registration Phase I to launch
Successrate
1996 2000
+46%
+16%
-45% -17%
-23%
Source: Bionest Partners, Exane BNP Paribas
This approach enables us to clearly demonstrate that hurdles have become higher in
oncology development. Between 1996 and 2000, cumulated success rates from
first-in-man to registration have decreased by 23% from 4.1% to 3.2%. This increasing
rate of failure is due to a sharp decline in phase II productivity and to a lesser extent to
phase III productivity.
However, products that are able to reach the registration stage have a better chance of
success.
8/3/2019 Oncology Pipelines
22/92
22 Pharmaceuticals
Developing cancer drugs is all aboutmanaging complexity
Oncology is one of the main science-driven specialties in medicine, with high technicalproducts and complex patient management. This makes research in this area
particularly complex and unpredictable. To make things worst, many teams are
competing not only on similar approaches but also on different approaches on the
same targets (for instance chemicals and biologicals on certain membrane receptors)
and on different approaches on the same disease.
To balance the development risk and because the understanding of the biology has
strongly progressed, companies are now trying to test their compounds in several
indications in parallel. But this strategy renders the development highly complex as
standard therapies are evolving very fast and are sometimes getting fragmented, i.e.
there can be several equivalent treatment options for the same patient. The products
are now often developed with competitors products and can sometimes reinforce
competitors position.
This makes marketing strategies difficult as the design of clinical trials contains an
element of risk in the choice of reference treatment and necessitates a close and
sustained presence in hospitals and among key opinion leaders. At the same time the
clinician profile is also changing, evolving to a more prominent role of organ specialists
versus traditional oncologists. As a consequence, cancer marketing and sales forces
will have to adapt to a less academical physician profile and deliver a more GP
oriented marketing promotion.
Table 4: Sources of complexity
Research Development
R&D
More competition on similar targets
More approaches to same targets
Clinical trials run in several indications in parallel
Increasing number of backbone therapies
MarketingMore competition on to access to Key Opinion Leaders
Emergence of organ specialists more GP oriented
Source: Bionest Partners, Exane BNP Paribas
Product positioning with or against competitors ?
For obvious reasons, treatment guidelines are lagging behind discovery and local
habits die hard. Consequently, there are usually several reference treatments in each
pathology and there is not always a consensus on the backbone of the treatment, i.e.
the set of drugs used as a standard in a particular cancer. When developing a new
drug to treat cancer, companies are essentially left with two options: either to develop
the compound on top of existing standards, the add-on strategy, or to replace one or
several of the components of a treatment, the switch strategy.
In fact, we are currently assisting at an increase in the number of drugs combinations
within an indication, offering practitioners a very high number of possible treatments.
This is mainly the consequence of the add-on strategy, which consists in testing a new
drug in addition to the backbone in an indication. This phenomenon not only
increases complexity for doctors, it also changes the way pharmaceuticals companies
must address the development of new drugs.
8/3/2019 Oncology Pipelines
23/92
23 Pharmaceuticals
This is because of:
the increase in the number of trials due to the rising number of utilized combinations
of existing drugs;
time constraints, as best practices evolve and companies have to run clinical trials
as fast as possible to reach the market with a setting that is still meaningful topractitioners.
Another approach to product development is to show superiority to existing treatments,
creating a replacement rather than an add-on. This is the switch strategy.
Clearly, the objective is to move the drug rapidly to the backbone and thus into the
guidelines. Then, new compounds will be tested more often on top of the drug rather
than against it.
The switch strategy is the fastest route to becoming a foundation stone
The switch strategy is supposedly used to replace a conventional treatment with a new,
more efficient one. That way, the new drug enters directly in the backbone of thetreatment by replacing a constitutive element of it. For instance, Sanofi-Aventiss
strategy for Eloxatine in colorectal cancer was to go head-to-head against Pfizers
Camptosar, the gold standard at the time. With better clinical outcomes, Eloxatine
succeeded in moving rapidly from second to first line and in taking over a leading share
of the market.
Another example is Glivec, from Novartis, which was approved in chronic myelogenous
leukaemia in 2001. Prior to the arrival of Novartiss tyrosine kinase inhibitor, the main
treatment options for this rare hematological cancer were interferon (mild- to high
efficacy but important side effects), Hydrea (poor efficacy and low side effects), and
medullar graft (capable of definitive cure, but associated with a very high mortality).
With high efficacy and relatively low safety concerns, Glivec succeeded in this nichemarket and is now the gold-standard.
Unfortunately, not all the drugs have the ability to show superiority and, most of the
time, switch strategies are used to replace one of the components of the treatment
setting with a similar product that improve solely safety or convenience.
For instance, three companies are currently playing this strategy to replace a very old
injectable cancer product, 5-FU. The new drugs are more convenient products, oral
versions, and have a better side-effect profile. These drugs are Merck KGaAs UFT,
Taiho S-1 and Roches Xeloda (capecitabine).
Roches reach in the oncology market and rich pipeline has led to the company being
the most aggressive of the three aforementioned companies. Roche includes
systematically in its clinical trials an arm containing Xeloda to replace 5-FU, when this
compound is part of the core-treatment. For example, the rapid development of Avastin
benefits Xeloda as there is often a Xeloda instead of 5-FU arm in the clinical
programmes for Avastin. This is a way of imposing the usage of Xeloda together with
Avastin and replace 5-FU.
8/3/2019 Oncology Pipelines
24/92
24 Pharmaceuticals
The add-on strategy is more complex and involves numerous backbones
Cancer drugs are mostly prescribed in settings combining several compounds. In the
most frequent situations, the backbone of the treatment is composed of two or three
chemotherapy agents. Historically, these compounds belong to therapeutic classes
such as alkylating agents or antimitotic agents or antimetabolites. On top of thisbackbone, we have observed the progressive appearance of molecules with more
targeted mechanisms of action: a new generation of chemotherapeutic agents
(antimitotic agents such as taxanes or topoisomerases) and more recently the so-called
targeted disease drugs. This last class covers the pathway inhibitors,
immunomodulators and/or monoclonal antibodies.
The chart below illustrates the evolution of backbones over time in colorectal, breast
cancers and non-Hodgkins lymphomas.
Chart 20: Illustration of backbones and add-on cancer therapies (non-exhaustive)
Colorectal cancer
Avastin Erbitux
Add-ons Oxaliplatin Irinotecan Avastin Avastin
Avastin Avastin Erbitux Erbitux Erbitux Erbitux
Irinotecan Oxaliplatin Oxaliplatin Irinotecan Oxaliplatin Irinotecan Oxaliplatin Irinotecan
5FU 5FU 5FU 5FU 5FU 5FU 5FU 5FU 5FU 5FU 5FU
Backbone LV LV LV LV LV LV LV LV LV LV LV LV
1952 1962 1992 1996 2004 2004
5FULV FOLFOX FOLFIRI FUTURE BACKBONES?
LV = Leucovorin, generics
5FU: Fluorouracile = Adrucil, generics
Irinotecan = Campto
Oxaliplatin = Eloxatin
Breast cancer
Add-ons Doxo 5FU Paclitaxel Docetaxel
Paclitaxel Docetaxel
Doxo Doxo Doxo Doxo
Backbone Cyclo Doxo Cyclo Cyclo Doxo Cyclo Doxo Cyclo Cyclo Cyclo
1959 1974 1994 1996 2002
C A AC FAC AP AC AT TAC NEW BACKBONES
Cyclophosphamide = Cytoxan, generics
Doxorubicine = Adriamycin, generics
Paclitaxel = Taxol, generics
Docetaxel = Taxotere
Non Hodgkin Lymphoma
Add-ons
R: Rituximab
P: Prednisone P: Prednisone P: Prednisone
O: Vincristine O: Vincristine O: Vincristine
H: Doxo H: Doxo H: Doxo
Backbone Cyclo C: Cyclo C: Cyclo C: Cyclo
1959 1979* 2002
C CHOP R-CHOP NEWBACKBONE
C: Cyclophosphamide = Cytoxan, generics
H: Doxorubicin/hydroxydoxorubin, Adriamycin, generics
O: Vincristine = Oncovin, generics
P: Prednisone, generics
R: Rituximab = Rituxan/Mabthera
*: Miller TP, Jones SE, Chemotherapy of localised histiocytic lymphoma, Lancet. 1979 Feb 17;1(8112):358-60
R: Rituximab
Source: Bionest Partners, Exane BNP Paribas
The consequence of the widespread use of the add-on strategy is the multiplication of
backbones, as illustrated above. New players now have to multiply clinical trials in
order to be associated with the existing backbones. For most companies, the impliedcosts of clinical trials are becoming unsustainable and it is becoming necessary to
make choices.
8/3/2019 Oncology Pipelines
25/92
25 Pharmaceuticals
For example, Avastin (Roche, Genentech) and Erbitux (Merck KGaA, BMS, Imclone)
are each currently under test in 30 clinical trials (see table below).
Table 5: Clinical trials with Avastin and Erbitux in colorectal cancer
Avastin ErbituxStill recruiting trials 38 29
No more recruiting trials 21 12
Source: Clinicaltrials.gov
The strategic decision of a backbone can be critical for the future of the product.
Avastin and Erbitux in colorectal were first developed with Pfizers irinotecan (in 2000-
2003), which has been swiftly replaced by Sanofi-Aventiss oxaliplatin (after 2003). Had
Erbitux chosen oxaliplatin first, it would probably have had an edge over Avastin.
There are collateral benefits to becoming part of a backbone: not only does the drug
become a standard, its use is also automatically boosted by other drugs in trials
seeking to prove added efficacy. The best illustration is Avastin (see case study) which
is on its way to becoming a backbone drug in several cancers. An increasing number of
trials with other cancer compounds now involve this anti-angiogenesis drug. As
Roches compound is becoming increasingly important, the company could now be in
the situation to get a direct return from competitors by participating in clinical trials: it
would certainly make sense for Sanofi-Aventis to try Taxotere + Avastin in some
settings to secure the use of Taxotere instead of Taxol; the PACCE clinical trial is
another illustration as this phase III trial combines Amgens panitumumab with Avastin
in first line metastatic colorectal cancer.
One bullet for several targets?
Not only is it becoming more complex to access an indication but companies are alsotrying to impose their drugs in several indications in parallel. This is due to the added
complexity of backbones and to the need to be faster to the market in several cancers
(the blitz strategy, see below).
In our universe of pharmaceuticals companies (see graph below), we have noticed that
there is an average of one to five programmes per molecule in phase II or III. Our work
suggests that there is no clear correlation between the average number of indications
tested and the nature of the molecule, the size of the group or the indications sought.
Very few companies develop their molecules in a single indication but there seems to
be a trend among smaller companies to explore a smaller number of indications per
molecule. In our universe, only UCB, Novo Nordisk, Serono, Genzyme and Biogen
Idec, all relatively small companies, remain very focused. While we have not found a
clear correlation, it seems that investment capacity is a limiting step in the current
development strategies. For instance, it is striking to see that with about the same
number of molecules AEterna Zentaris is running half the number of programmes
compared to AstraZeneca or J&J.
Most of the companies are running two or three studies in parallel per molecule.
Although we do not have the corresponding data for ten years ago, based on our
interviews, we strongly believe that the increase in development costs over the last
years has a lot to do with this pan-indication strategy.
The benefits from the strategy are highlighted by the recent failure of Wyeths mTOR
inhibitor, temsirolimus, in phase III for metastatic breast cancer and the parallelannouncement that two other phase III programmes were being maintained, in renal
cancer and certain forms of lymphoma.
8/3/2019 Oncology Pipelines
26/92
26 Pharmaceuticals
Chart 21: No correlation between the size of the portfolio and the number of programme per molecule
UCBNovo nordisk
Novartis
Merck & Co
Genzyme Biogen Idec
AEterna Zentaris
Average
Wyeth
Serono
Schering-Plough
Schering AG
Sanofi-Aventis
Roche/Genentech
Pierre Fabre
Pfizer
Merck KGaAMedImmune
Johnson & Johnson
GlaxoSmithKline
Eli Lilly
Bristol-Myers SquibbBayer
Baxter
AstraZeneca
Amgen
Abbott
1.0
2.0
3.0
4.0
5.0
6.0
0 2 4 6 8 10 12 14 16 18 20Total number of molecules in phase 2 or 3
Averagenumberofprograms
permoleculeinphase2or3
Source: Bionest Partners, Exane BNP Paribas
Among the larger companies, it seems that some prefer to spread the risk over several
indications (AstraZeneca, J&J and BMS) while others focus their resources (Pfizer,
Sanofi-Aventis). The vast majority of companies are running more than two studies per
molecule (the average is 2.8 in this sample and 2.3 in our global database) and the
comments made during the interviews convince us that most of the companies are
willing to spend more money in phase II to get some signal in different indications
rather than betting on a single bullet.
Chart 22: Number of programmes per product in phase II and III
0.8 1.2 1.6 2.0 2.4 2.8 3.2 3.6 4.0 4.4 4.8 5.2 5.6
Abbott
AEterna Zentaris
Amgen
AstraZeneca
Baxter
Bayer
Biogen Idec
Bristol-Myers Squibb
Eli Lilly
Genzyme
GlaxoSmithKline
Johnson & Johnson
MedImmune
Merck & Co
Merck KGaA
Novartis
Novo nordisk
Pfizer
Pierre Fabre
Roche/Genentech
Sanofi-Aventis
Schering AG
Schering-Plough
Serono
UCB
Wyeth
NB: Black indicates companies with fewer than two studies per molecule on average; white indicates above average.
Source: Bionest Partners, Exane BNP Paribas
8/3/2019 Oncology Pipelines
27/92
27 Pharmaceuticals
Lowering the costs. But at what cost?
To keep the cost of clinical development down, companies are tempted to run trials in
eastern Europe ort Asia. However, this is not always possible or appropriate. First, the
standard of care is usually not the same as in western countries and it is difficult torecruit patient when the clinicians are not familiar with the tested arm and the control
arm. Second, for a study to be accepted it must be supported by globally recognizedkey opinion leaders. With rare exceptions, these live in the largest pharma markets.
Oral drug approaches vs biologicals: who will win?
When a company starts work on a project with a tropism toward oncology, it is
sometimes difficult to identify the right pathology. In the past we have seen that most
companies targeted several indications at once in order to increase their chances of
success and so leapfrog competitors.
In addition to this risk of not finding the right indication, or of not identifying it fast
enough, each programme is in competition with:
similar development approaches at other companies (me-toos);
different approaches on the same biological target (monoclonal antibodies,
chemicals, vaccines, etc.);
different approaches on the same pathology (different biological targets).
A good example is the VEGF approach (vascular epithelial growth factor). Among the
eight products listed in the table below, three are biological and five are chemicals.
However, all eight target the same mechanism: blockage of the VEGF pathway either
by blocking the receptor (Avastin and CDP-791) or its functioning (chemicals) or its
ligand (AVE005). Clinically it seems that these molecules have different features and
are finally ending in different indications. For instance, Avastin has been launched in
colorectal cancer but Nexavar and Sutent in renal cancer. PTK 787 did not show greatresults in colorectal and is not being investigated in renal.
Table 6: VEGF approaches
Laboratory Nature of molecule Most advance stage ofdevelopment
Avastin Genentech/Roche Monoclonal antibody CommercializedNexavar Bayer Chemical CommercializedSutent Pfizer Chemical Commercialized
PTK 787 Schering/Novartis Chemical Phase IIIZactima AstraZeneca Chemical Phase IIIAG-013736 Pfizer Chemical Phase IIAVE005 / VEGF-Trap SAVE/Regeneron Biological inhibitor Phase IICDP-791 UCB/ImClone Antibody fragment Phase II
Source: Bionest Partners, Exane BNP Paribas
Pipelines are still very chemical
To illustrate the situation, we have sorted our 465-drug database of products in phase II
or 3 in oncology (based on Pharmaprojects and other sources) by type and therapeutic
class. In our database, products are referred to according to their most advanced
phase, i.e. a product in phase III and in phase II in other indications is referred as in
phase III. As a result, products on the market or in registration but which are also being
developed for other indications are not included in the following analyses.
8/3/2019 Oncology Pipelines
28/92
28 Pharmaceuticals
Focusing on molecules with phase II or III as most advanced stage, chemicals still
represent the majority of drug candidates in development. With 191 small molecules,
they account for 52% of new phase II/III drugs.
Surprisingly, monoclonal antibodies and recombinant proteins account for only 23% of
new phase II/III therapies under development whereas cellular, gene and SiRNA-based
therapies represent 11%.
Concerning complexity, almost every biological product is challenged by a chemical
approach usually on the same molecular target or on its direct cascade of action. This
means that laboratories developing biologicals have to add to the risk of development
and production, the risk of being leapfrogged by a targeted chemical approach.
Chart 23: New phase II/III drug candidates by molecule type
Phase II products Phase III products
Biological
peptide/protein
7
2%
Chemical
149
51%
Other
19
7%
SiRNA
8
3%
Synthetic peptide
20
7%
Monoclonal
antibody
34
12%
Recombinant
protein
27
9%
Gene therapy
15
5%
Cellular therapy
12
4%
Cellular therapy
2
3%
Gene therapy2
3%
Recombinant
protein
12
17%
Monoclonal
antibody
8
12%
Synthetic peptide
1
1%
Chemical
42
61%
Biological
peptide/protein
2
3%
Source: Bionest Partners, Exane BNP Paribas
Interestingly, on average there are more clinical programmes with chemicals (3.3 per
molecule) than biologicals (around 2). This could be due to the mechanism of action of
some biologicals with limited possible indications as they are usually targeting specific
extracellular biomarkers. One spectacular exception though is Avastin (see case study
below).
Most actors have some presence in either or both peptides/proteins or monoclonal
antibodies; the main exceptions are Wyeth and AstraZeneca. Roche/Genentech has
the most balanced portfolio with an impressive proportion of biologicals in its pipeline.
GSK also has a greater presence in this biological field than is perceived by the
market.
Some companies are not present in the chemical arena. These are mainly biotech-like
companies such as Biogen Idec, UCB or Novo Nordisk but the list also surprisingly
counts one large company, Merck & Co.
Some other companies have a purely chemical approach, for example AstraZeneca
or Wyeth. More surprisingly, Medimmune and Genzyme also have only chemicals in
there oncology pipeline.
8/3/2019 Oncology Pipelines
29/92
29 Pharmaceuticals
Chart 24: Molecules in development by nature of products
0 2 4 6 8 10 12 14 16 18 20
Abbott
AEterna Zentaris
Amgen
AstraZeneca
Baxter International
Bayer
Biogen Idec
Bristol-Myers Squibb
Eli Lilly
Genzyme
GlaxoSmithKline
Johnson & Johnson
MedImmune
Merck & Co
Merck KGaA
Novartis
Novo nordisk
Pfizer
Pierre Fabre
Roche/Genentech
Sanofi-Aventis
Schering AG
Schering-Plough
Serono
UCB
Wyeth
Chemical Peptide/protein Cel lular therapy Gene therapy Monoclonal ant ibody Others
Source: Bionest Partners, Exane BNP Paribas
Centralised vs decentralised marketing organizations
Even the marketing organization needs to be adjusted to the project. Schematically,
there are two principal types of marketing organization within Pharma companies in
oncology: centralised and decentralised. We have identified a steady shift from the
decentralised (regional) to the centralised pattern. This will continue as:
the number of clinical trials is sharply increasing with a multiplication of indications
(see above);
larger patient samples are required to obtain statistically significant data;
managing clinical trials is becoming more and more complex.
As a result, companies will have to take an increasingly systematic approach, for which
the centralised organization is better suited.
The centralised marketing organization
The centralised marketing organization consists in a top-down decision taking process,
where a corporate-level team defines the rules for all the country subsidiaries. This
approach necessitates a clearly empowered corporate team that drives the relationship
with the KOL and precisely set the framework for clinical trials: clinical trials are
designed at the corporate-level, with few modifications at the local level.
8/3/2019 Oncology Pipelines
30/92
30 Pharmaceuticals
Bristol-Myers Squibb developed this approach, with a catalogue of clinical trials
communicated by the corporate to the subsidiaries that had to execute. Another
example of this approach was the design of Herceptin phase III clinical trial in breast
cancer: Roche / Genentech designed only one trial applied worldwide with no
possibility for physicians to modify the design. This approach is well adapted to a blitz
strategy (see paragraph below) where products are tested in parallel in a high number
of indications (organs) and lines (first and second lines, adjuvant setting).
The decentralised marketing organization
The decentralised marketing organization consists in a locally-driven decision taking
process. Aventis used this approach for the development of Taxotere. This approach
helped Aventis to compete against BMS Taxol and contribute to differentiate in local
markets the two products.
However, this highly decentralised approach does not always allow good control over
the design of trials. For instance, in the ovary indication, this led to mixed results that
were insufficient to battle against well-established Taxol. In addition, Aventis was late in
designing combination trials with innovative targeted therapies due to a lack of global
vision (e.g. combination with Avastin in breast cancer and colorectal cancer, with
Herceptin in breast cancer or even with Iressa in lung cancer).
Table 7: Centralised vs decentralised organization in oncology
Organization Advantages Inconvenient
Centralised
Homogeneity of trials (limits double counting and gaps)
Fast recruitment with large population size
Better identification of strategic opportunities (e.g.Association with new molecules)
Well adapted to a mosaic strategy
Risk of poor adhesion at the local level if it is only execution
Risk of poor relationship with KOL due to low localinvolvement and poor listening to KOL needs
Decentralised
Adhesion of the local level
Close relationship with investigators and KOL
Identification of local opportunities (e.g. Local partnerships,new regimens)
Heterogeneity of trials
Double counting and gaps
Source: Bionest Partners, Exane BNP Paribas estimates
Prescribers are evolving too
The situation is complicated by the evolution in the profile of prescribers. In Europe, for
some time now, patients are treated by oncologists but also organ specialists. In the
USA, the movement is starting and could change the face or marketing as companies
might have to adopt their marketing strategy per therapeutic segment.
This has been confirmed by interviews with industry managers. These have have
highlighted a difference between the habits of pure oncologists and organ-specialized
physicians. Put simply, in most countries pure oncologists take care of a series of
cancers that are not under the coverage of organ-specialized physicians, for example,
breast cancer, leukaemias and lymphomas, or colorectal cancer. In contrast,
pathologies such as lung, prostate, bladder or renal cancers are more often under the
charge of organ-specialized physicians (pneumologists, urologists).
Things are even more complicated as there are differences in each cancer in each
region. For example, in Germany breast cancer seems to be taken in care by
gynecologists rather than by oncologists; the opposite is true in the USA.
8/3/2019 Oncology Pipelines
31/92
31 Pharmaceuticals
This difference not only has an impact on the organisation of the marketing and sales
forces, it also has an impact on sales. Whereas pure oncologists are used to
integrating new drugs into their practice rapidly, it seems that penetration is slower
among organ-specialized physicians, which necessitates greater marketing efforts.
Consequently, cancer marketing and sales forces would have to adapt to physicians
with a less academically oriented profile and take a more GP-oriented approach to
marketing.
If we make a parallel with other technical therapeutic areas, such as AIDS and
Immunology, we can attest the adaptation of sales forces to GP practitioners: AIDS tri-
therapy is now prescribed in most countries by GPs even if hospital KOLs continue to
play a major role. To a lesser extent, the arrival of sub-cutaneous formulations of
biologic DMARDs in rheumatoid arthritis, e.g. Abbotts Humira, Schering Ploughs
Enbrel or BMSs Abatacept, has opened the door for ambulatory care. Even if GPs are
still not involved in prescribing these drugs, the hospital-to-ambulatory shift contributes
to the modification of the marketing approach in much the same way.
8/3/2019 Oncology Pipelines
32/92
32 Pharmaceuticals
No place for slow players
While we observed in the previous chapter that the current trends in the cancer market
imply a higher level of complexity for existing players and newcomers, we highlight inthis chapter the strong acceleration in cancer drugs lifecycle management.
First, there is clearly a strong first-mover advantage, which means that products must
be well differentiated within the scope of approved indications, in terms of organs and
therapeutic lines, and that these indications must be obtained before competitors.
Drugs that have been able to do so have maintained 50-70% market shares years after
competitors entry.
Second, given the increasing competition in cancer research, being first to market
requires very fast development. As a result, companies have adapted their approach
with what we call the blitz strategy, which consists of testing new drugs in parallel in a
large number of indications and sometimes in several settings. The emergence of this
strategy, as opposed to the more traditional step-by-step Domino strategy, stems from
the recent increase in the number of targeted therapies, mainly for two reasons:
targeted therapies often apply to biological mechanisms that are common to different
cancers, offering the possibility of addressing several of them.
targeted therapies often present lower levels of toxicity compared to traditional
chemotherapy allowing testing in numerous diseases.
Third, in the future, cancer drugs are expected to be under stronger price pressure from
the regulatory authorities and insurance companies as well as directly from
competition. The increasing use of generics in all therapeutic areas is already having
an effect and could influence the development of new guidelines. It is worth noting that
generic entries also free up money that can be used to fund new therapies. EGF-R and
anti-VEGF drugs are the two therapeutic classes that are the best positioned to benefit
from this situation.
In conclusion, as product differentiation is critical for cancer drugs, the main criteria are
the breadth of the indications and how fast they can be obtained. We believe that the
blitz strategy with a centralized organization is more suitable than a domino strategy
with a decentralized organization. In addition, the increasing number of trials in nearly
all therapeutic indications demonstrates that even a niche positioning is not a safe
harbour in the face of greater competitive intensity.
A strong first-mover advantage
There is clearly a strong first-mover advantage, which means that products must be
well differentiated within the scope of approved indications, in terms of organs and
therapeutic lines, and that these indications must be obtained before competitors.
Drugs that have been able to do so have maintained 50-70% market shares years after
competitors entry.
We present three case studies to illustrate the first-mover effects, in different
therapeutic classes with two, three or more competitors:
the taxanes market, with the Taxol vs Taxotere duopoly;
the aromatase inhibitors market, with Arimidex, Femara and Aromasin;
the poorly differentiated and crowded LHRH agonists market.
8/3/2019 Oncology Pipelines
33/92
33 Pharmaceuticals
First-mover case study number 1: Taxol vs Taxotere
This case study illustrates the first-mover advantage in a poorly differentiated duopoly.
BMSs paclitaxel Taxol was approv