Embed Size (px)
Citation preview

AesCbs(fiso
FM
Sp@
2
Fom
IMAGES IN CLINICAL UROLOGY
3
OCCULT RENAL SEGMENTAL ARTERIAL INJURYAFTER TRAUMA
NATHAN LAWRENTSCHUK AND DAMIEN M. BOLTON
sSdmdhwata
orvpebv
Fcoccnma
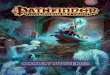
48-year-old man presented after a signifi-cant left-sided fall with no hematuria. How-
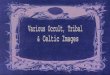
ver, abdominal computed tomography demon-trated poor perfusion in the right kidney.omputed tomography angiography delineatedranches of the right renal artery, with no perfu-ion posteriorly, due to traumatic thrombosisFig. 1). Coronal computed tomography con-rmed absent perfusion anteriorly in the apicalegment (Fig. 2), with absent perfusion posteri-rly in the apical and posterior segments and
rom the Department of Surgery and Urology, University ofelbourne, Austin Hospital, Heidelberg, Victoria, Australia.Reprint requests: Dr. Nathan Lawrentschuk, Department of
urgery and Urology, University of Melbourne, Austin Hos-ital, Heidelberg, Victoria, 3084, Australia. E-mail: nayjayozemail.com.auSubmitted: June 28, 2004, accepted (with revisions): September
IGURE 1. Computed tomography angiography dem-nstrating poor perfusion in right kidney posterior seg-ent and posterior branch of right renal artery (arrow).
j2, 2004
© 2005 ELSEVIER INC. U86 ALL RIGHTS RESERVED
ome perfusion of the lower segment (Fig. 2).egmental renal arterial supply (Fig. 2) wasemonstrated owing to selective injury.1 For-erly, patients with such injuries may have un-
ergone surgical exploration,2 but other series3
ave supported conservative management,hich we followed. At the 3-month review, im-
ging revealed renal atrophy, but perfusion ofhe posterior branch (Fig. 3). His blood pressurend renal function remained normal.Major renovascular injuries are rare (3% to 9%
f renal injuries are grade 4).2,4,5 Theoretically,evascularizing thrombosed segments may pre-ent infarction and hypertension, but such com-lex surgery risks nephrectomy.3 In a series ofxpectantly managed isolated traumatic throm-oses, no patient required delayed surgical inter-ention.3 Surgery of hemorrhaging segmental in-
IGURE 2. Computed tomography angiography withoronal reformatting demonstrating segmental naturef injury anteriorly (left) and posteriorly (right). This isompared with segmental arterial supply below eachoronal slice, viewed from posterior aspect, as per coro-al computed tomography reformatting. Affected seg-ents are shaded and levels of coronal sections forngiography and diagram indicated.
uries has demonstrated that de-arterialization is
ROLOGY 65: 386–387, 2005 • 0090-4295/05/$30.00doi:10.1016/j.urology.2004.09.054

ecto
a1
at
s1
h2
lr1
n
Firwhich has undergone atrophy.
UROLOGY 65 (2), 2005
ffective in controlling hemorrhage, with paren-hymal preservation and minimal risk of hyper-ension.6 This supports conservative treatmentf isolated arterial thrombosis, as in this case.
REFERENCES
1. Graves FT: The anatomy of the intrarenal arteries and itspplication to segmental resection of the kidney. Br J Surg 42:32–139, 1954.2. Knudson MM, Harrison PB, Hoyt DB, et al: Outcome
fter major renovascular injuries: a Western trauma associa-ion multicenter report. J Trauma 49: 1116–1122, 2000.
3. Cass AS, and Luxenberg M: Traumatic thrombosis of aegmental branch of the renal artery. J Urol 137: 1115–1116,987.4. Bertini JE Jr, Flechner SM, Miller P, et al: The natural
istory of traumatic branch renal artery injury. J Urol 135:28–230, 1986.5. Lang EK, Sullivan J, and Frentz G: Renal trauma: radio-
ogical studies—comparison of urography, computed tomog-aphy, angiography, and radionuclide studies. Radiology 154:–6, 1985.6. Angorn IB: Segmental dearterialization in penetrating re-
IGURE 3. Computed tomography scan 3 months afternjury with perfusion present in posterior branch of rightenal artery (arrow) and its segmental area of supply,
al trauma. Br J Surg 64: 59–65, 1977.
387