Embed Size (px)
Citation preview

e
pwcbaostcddCwoa
e
dM
BErpso
RA
The Journal of Emergency Medicine, Vol. 31, No. 3, pp. 259–262, 2006Copyright © 2006 Elsevier Inc.
Printed in the USA. All rights reserved0736-4679/06 $–see front matter
doi:10.1016/j.jemermed.2005.12.023
ClinicalCommunications
OCCIPITAL CONDYLE FRACTURE IN A VICTIM OF A MOTOR VEHICLECOLLISION
Hani O. Mowafi, MD and Kenneth S. Hickey, MD
Department of Emergency Medicine, Virginia Commonwealth University Medical Center, Richmond, VirginiaReprint Address: Kenneth S. Hickey, MD, Department of Emergency Medicine, Virginia Commonwealth University Medical Center, P.O.
Box 980401, Richmond, VA 23298
ca
AmacpdwiroT
iaPdappwmw
Abstract—Occipital condyle fractures are rarely re-orted in the Emergency Medicine literature. It is unclearhether these fractures are rare or under-diagnosed. Oc-
ipital condyle fractures are associated with high-energylunt trauma with significant cranial-cervical torque orxial loading. We report a case of a female patient with anccipital condyle fracture. The patient only complained ofhoulder pain, but was found to have high cervical spineenderness, after a moderate-speed front-end motor vehicleollision. Initial cervical spine radiographs were non-iagnostic. Computed tomography of the cervical spineemonstrated a non-displaced occipital condyle fracture.onservative management with a semi-rigid cervical collaras successful in treating this patient’s fracture. A reviewf the literature covers the diagnosis, radiographic findings,nd management of this fracture. © 2006 Elsevier Inc.
Keywords—Occipital condyle fracture; atlanto-axialislocation; cervical ligamentous instability; Anderson andontesano classification
INTRODUCTION
lunt head and neck trauma are common reasons formergency Department (ED) visits. Cervical spine inju-
ies occur frequently as a result of trauma, and theirresentation, diagnosis, and treatment have been exten-ively reported in the medical literature. We report a casef an occipital condyle fracture—an unusual head and
ECEIVED: 9 February 2005; FINAL SUBMISSION RECEIVED:
CCEPTED: 2 December 2005259
ervical spine injury. We include a discussion of thenatomy, diagnostics, and management of this injury.
CASE REPORT
19-year-old woman was transported by emergencyedical services (EMS) to our Level 1 trauma center
fter a motor vehicle collision. She was placed in aervical collar and on a backboard at the scene. Thearamedics reported that the patient was a restrainedriver struck at 40 miles-per-hour on the driver’s sideith air bag deployment and approximately 14 inches of
ntrusion into the passenger compartment. The patienteportedly lost consciousness, but was alert and orientedn EMS arrival and remained so throughout transport.he paramedics noted severe left shoulder pain.
In the trauma resuscitation bay, initial physical exam-nation revealed an obese female patient who was alertnd oriented. Vital signs were within normal limits.hysical examination revealed high cervical bony ten-erness, tenderness over the left shoulder musculature,nd an ecchymosis at the left anterior shoulder. Theatient was not found to have tenderness over the bonyrominences of the left shoulder or left clavicle. Thereas no crepitus and the patient had full passive range ofotion at the joint. The remainder of the examinationas without focal findings.
y 2005;
14 Jul
cb
sctwwpsci
awosrrN
BcScl
eovaactabmlv
dfdTatebmflms
lohgtdsa(shctggmf
cafsaca
Fc
260 H. O. Mowafi and K. S. Hickey
Laboratory studies included a basic metabolic panel,omplete blood count, and venous blood gas with wholelood lactate; all were within normal accepted ranges.
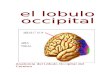
Plain radiographic studies included a lateral cervicalpine and anterior-posterior chest and pelvis. The cervi-al spine radiograph incompletely viewed all of the ver-ebral bodies. The chest and pelvis radiographs wereithout abnormality. The patient subsequently under-ent a head, cervical spine and abdominal-pelvic com-uted tomography (CT) scan. These studies demon-trated a non-displaced comminuted left occipitalondyle fracture (Figure 1). There was no evidence ofntracranial hemorrhage or intra-abdominal injury.
The patient’s cervical spine remained immobilized insemi-rigid cervical collar. Neurosurgical consultationas obtained. The patient was admitted for 23 h ofbservation. Re-examination before discharge demon-trated mild high cervical spine tenderness and no neu-ological deficits. The patient was discharged in a semi-igid cervical collar and scheduled for follow-up witheurosurgery in 4 weeks.
DISCUSSION
ritish surgeon Charles Bell first described an occipitalondyle fracture on postmortem examination in 1817 (1).ince this initial case report, fewer than 150 occipitalondyle fractures have been described in the medical
igure 1. Head CT scan demonstrates a left Type I occipitalondyle fracture (downward arrow).
iterature. t
Occipital condyle fractures are the result of high-nergy blunt trauma with axial loading, lateral bending,r rotational injury to the ligaments of the first cervicalertebrae and the occipital interface (2,3). The pairedlar ligaments, tectorial membrane, and the cruciate andpical dental ligaments maintain stability of the occipital-ervical interface (3). The paired alar ligaments attachhe dens with the occipital condyles. The cruciform lig-ments attach the body of C2 with the ring of C1 and thease of the occipital bone (clivus). Finally, the tectorialembrane is the superior-most portion of the posterior
ongitudinal ligament and provides stabilization of theertebral canal from the base of the skull to sacrum.
Anderson and Montesano have divided occipital con-yle fractures into three types (Figure 2) (4). Type Iractures are comminuted fractures of the occipital con-yle with no displacement into the foramen magnum.his fracture is stable because the tectorial membranend contralateral alar ligament are intact. Type II frac-ures are characterized by a basilar skull fracture thatxtends into the occipital condyle. This fracture is stableecause the alar ligaments and tectorial membrane re-ain intact. Type III fractures are defined as an avulsion
racture of the occipital condyle with stress of the ipsi-ateral and contralateral alar ligaments and tectorialembrane. Type III occipital condyle fractures are un-
table due to the ligamental stress and disruption (3,4).Blunt force trauma secondary to a motor vehicle col-
ision has been reported as the most common cause ofccipital condyle fractures (2,3,5–17). These fracturesave also been reported as the result of falls and stran-ulation (18,19). Patients with occipital condyle frac-ures resulting from motor vehicle collisions have beeniagnosed with other blunt trauma and torsion injuriesuch as atlanto-axial dislocation, duodenal hematoma,ortic disruption, lumbar vertebra fractures and others6–8,12,17,18). The entity of occipital condyle fractureshould be considered in patients who have experiencedigh velocity blunt force trauma with an altered level ofonsciousness, cranial nerve palsies, occipital pain orenderness, impaired cervical rotation, and retropharyn-eal swelling (10). Cranial nerves IX (glossopharyn-eal), X (vagus), and XII (hypoglossal) are most com-only injured in association with occipital condyle
ractures.There have been four major review articles specifi-
ally addressing occipital condyle fractures. Andersonnd Montesano described a model classification systemor these fractures in 1988 (4). Young et al. reported amall case series of occipital condyle fractures (3). Noblend Smoker reported a series of 15 patients with occipitalondyle fractures who presented over a 4-year period toLevel 1 trauma center (5). Finally, Hanso et al. reported
he largest series of patients to date with occipital con-

dcdcarrstcfsriwi
bsrrofaachu
fccTpsopr
ift(aa
Fw y. Nobm s. AJN
Occipital Condyle Fracture 261
yle fractures (13). They reviewed the radiographic andlinical presentation of 107 consecutive occipital con-yle fractures. The common theme shared by these arti-les is the observation that plain radiographs of the skullnd cervical spine were negative or non-diagnostic. Aecent prospective study of 1006 patients compared plainadiographs with CT scan for the evaluation of cervicalpine injury (20). The authors of this study concludedhat a complete cervical spine series missed 52.3% ofervical spine fractures and 93.3% of occipital condyleractures that were later found on CT scan. Cervicalpine CT scan missed only 1.7% of cervical spine inju-ies that were later found on magnetic resonance imag-ng. A CT scan of the cervical spine should be obtainedhen there is an appropriate mechanism of injury, clin-
cal and neurologic findings, such as cranial nerve palsy.Management of occipital condyle fractures is dictated
y their radiographic type. Type I and II fractures aretable and may be conservatively managed with a semi-igid cervical collar or halo-orthosis (3,5–15). Capuanoeported a series of 10 consecutive patients with Type Ir II occipital condyle fractures with complete fusion atollow-up 18 months to 2 years after conservative man-gement (14). Momjian reviewed the pediatric literaturend found that 8 weeks of immobilization in a semi-rigidervical collar or halo-vest was sufficient for fractureealing (15). Type III occipital condyle fractures are
igure 2. Line drawings illustrate Type I (A and B), Type II (Cith permission from the American Society of Neuroradiologorphology, and classification of occipital condyle fracture
nstable and require close clinical monitoring. These
ractures frequently require surgical fixation with occipital-ervical fusion; however, the majority have been suc-essfully managed with conservative treatment (3,13).ype III fractures may be more likely to result in com-ression of adjacent structures by a free-floating fractureegment. Tuli et al. reported that approximately one-thirdf occipital condyle fractures present with cranial nervealsies (9). The majority of these neuro-deficits are theesult of Type III occipital condyle fractures.
Occipital condyle fractures seem to be rare. Thesenjuries are typically indicative of high-velocity bluntorce trauma. Occipital condyle fractures occur in fewerhan 1% of patients complaining of neck injury or pain5). The physicians caring for these patients should belert to the mechanism, and look for clinical tendernessnd neurologic signs that indicate a search for this entity.
REFERENCES
1. Bell C. Surgical observations. Middx Hosp J 1817;4:469.2. Stroobants J, Fidlers L, Storms JL, et al. High cervical pain and
impairment of skull immobility as the only symptoms of occipitalcondyle fracture. Case report. J Neurosurg 1994;81:137–8.
3. Young WF, Rosenwasser RH, Getch C, et al. Diagnosis andmanagement of occipital condyle fractures. Neurosurgery 1994;34:257–61.
4. Anderson PA, Montesano PX. Morphology and treatment of oc-cipital condyle fractures. Spine 1988;13:731–6.
5. Noble ER, Smoker WRK. The forgotten condyle: the appearance,
), and Type III (E and F) occipital condyle fractures (5). Usedle ER, Smoker WRK. The forgotten condyle: the appearance,R Am J Neuroradiol 1996;17:507–13.
and D
morphology, and classification of occipital condyle fractures.AJNR Am J Neuroradiol 1996;17:507–13.

1
1
1
1
1
1
1
1
1
1
2
262 H. O. Mowafi and K. S. Hickey
6. Urcolo E, Arrazola M, Arrazola M Jr, et al. Delayed glossopha-ryngeal and vagus nerve paralysis following occipital condylefracture. Case report. J Neurosurg 1996;84:522–5.
7. Castling B, Hicks K. Traumatic isolated unilateral hypoglossalnerve palsy—case report and review of the literature. Br J OralMaxillofac Surg 1995;33:171–3.
8. Kaushik V, Kelly F, Richards SD, Saeed SR. Isolated unilateralhypoglossal nerve palsy after minor head trauma. Clin NeurolNeurosurg 2002;105:42–7.
9. Tuli S, Tator CH, Fehlings MG, et al. Occipital condyle fractures.Neurosurgery 1997;41:368–76.
0. Occipital condyle fractures. Neurosurgery 2002;50(3 Suppl):S114–9.
1. Wasserberg J, Bartlett RJ. Occipital condyle fractures diagnosedby high-definition CT and coronal reconstruction. Neuroradiology1995;37:370–3.
2. Clayman DA, Sykes CH, Vines FS. Occipital condyle fractures:clinical presentation and radiologic detection. AJNR Am J Neuro-radiol 1994;15:1309–15.
3. Hanson JA, Deliganis AV, Baxter AB, et al. Radiologic and
clinical spectrum of occipital condyle fractures: retrospective re-view of 107 consecutive fractures in 95 patients. AJR Am JRoentgenol 2002;178:1261–8.
4. Capuano C. Occipital condyle fractures: a hidden nosologic anentity. An experience with 10 cases. Acta Neurochir 2004;146:779–84.
5. Momjian S. Occipital condyle fractures in children. Case reportand review of the literature. Pediatr Neurosurg 2003;38:265–70.
6. Demisch S, Lindner A, Beck R, Zierz S. The forgotten condyle:delayed hypoglassal nerve palsy caused by fracture of the occipitalcondyle. Clin Neurol Neurosurg 1998;100:44–5.
7. Payer M, Delavelle J. Bilateral occipital condylar fracture. Casereport about successful treatment with SOMI brace. J Clin Neuro-sci 2004;11:211–4.
8. Devi BI, Dubey S, Shetty S, Jaiswal VK, Jayakumar PN. Fracturedoccipital condyle with isolated 12th nerve paresis. Neurol India2000;48:93–4.
9. Paul JS, Tracqui A, Ludes B. Homicide by manual occipitoatlantaldislocation. J. Forensic Sci 2004;49:601–3.
0. Diaz JJ, Gillman C, Morris JA, et al. Are five-view plain films ofthe cervical spine unreliable? A prospective evaluation in blunttrauma patients with altered mental status. J Trauma 2003;55:
658–64.