Embed Size (px)
Citation preview
Journal of Plastic, Reconstructive & Aesthetic Surgery (2010) 63, 410e415
Occipital artery Island VeY advancement flapfor reconstruction of posterior scalp defects
Ramesh Kumar Sharma*, Puneet Tuli
Department of Plastic Surgery, Postgraduate Institute of Medical Education and Research, Chandigarh 160012, India
Received 9 July 2008; accepted 13 December 2008
KEYWORDSScalp defects;Occipital region;Occipital island flap;VeY advancement;Primary closure;Direction of hair
* Corresponding author. Tel.: +91172fax: +911722756792.
E-mail address: drsharmark@yahoo
1748-6815/$-seefrontmatterª2009Bridoi:10.1016/j.bjps.2008.12.017
Summary Background: The management of the posterior scalp defects with ‘similar’ tissuecan be challenging. Currently available techniques of transposition/rotation result in creationof unwanted dog ears, change in direction of hairs and patches of skin-grafted areas withalopecia. We describe a new method of reconstruction of full-thickness scalp defects in theoccipital region by moving the locally available scalp tissue in a VeY advancement manner.The islanded flap is based upon the ipsilateral occipital artery in the substance of occipitalismuscle. The donor site/s can be closed primarily and the operation performed in a single stageMaterials and methods: A total of seven patients have undergone reconstruction in the last 2years with this technique. The defects in the posterior scalp region resulted either from theelectrical burns (two patients), tumour excision (two patients), encephalocoele excision(one patient) or post-traumatic loss of the scalp (two patients). In all the patients the under-lying bone was exposed. The remaining scalp tissue in the vicinity of the defect was moved asa VeY advancement flap either unilaterally or bilaterally depending upon the size of thedefect. The pedicle of the flaps contained ipsilateral occipital vessels at the base. The flapswere raised in the subgaleal plane and the pedicle included ipsilateral occipital artery inthe substance of the occipitalis muscle.Results: The donor area could be closed primarily in all cases. All the flaps survivedcompletely; one patient had postoperative superficial loss that eventually healed with dress-ings. All the wounds healed primarily with luxuriant hair growth, except one patient who hadpartial alopecia in the transferred flap although the flap survived completely.Conclusion: The islanded occipital artery VeY advancement flap provides a one-stage hair-bearing scalp tissue for closure of medium and moderately large defects (up to 7� 6.5 cm2)in the posterior region of the scalp with primary closure of the donor site.ª 2009 British Association of Plastic, Reconstructive and Aesthetic Surgeons. Published byElsevier Ltd. All rights reserved.
2756792;
.com (R.K. Sharma).
tishAssociationofPlastic,Reconstruc
The goals of reconstruction in full-thickness loss of scalpare protection of the underlying cranium/brain and theappearance of the scalp. These complex soft-tissue defects
tiveandAestheticSurgeons.PublishedbyElsevierLtd.All rightsreserved.
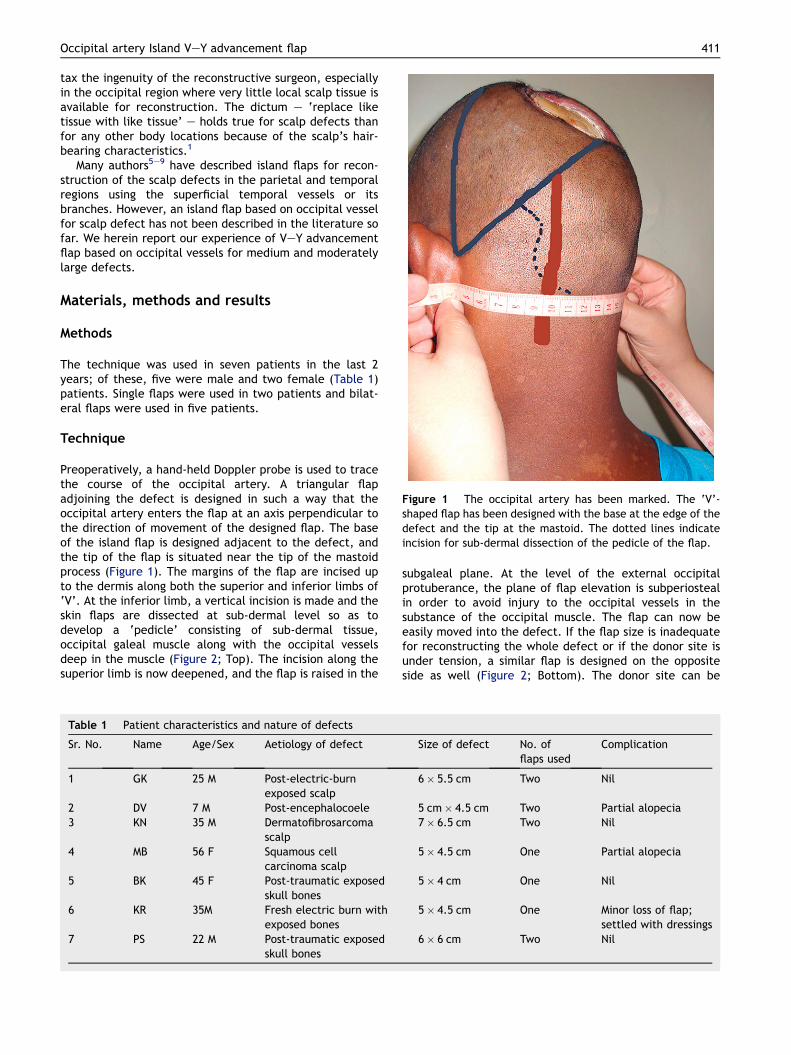
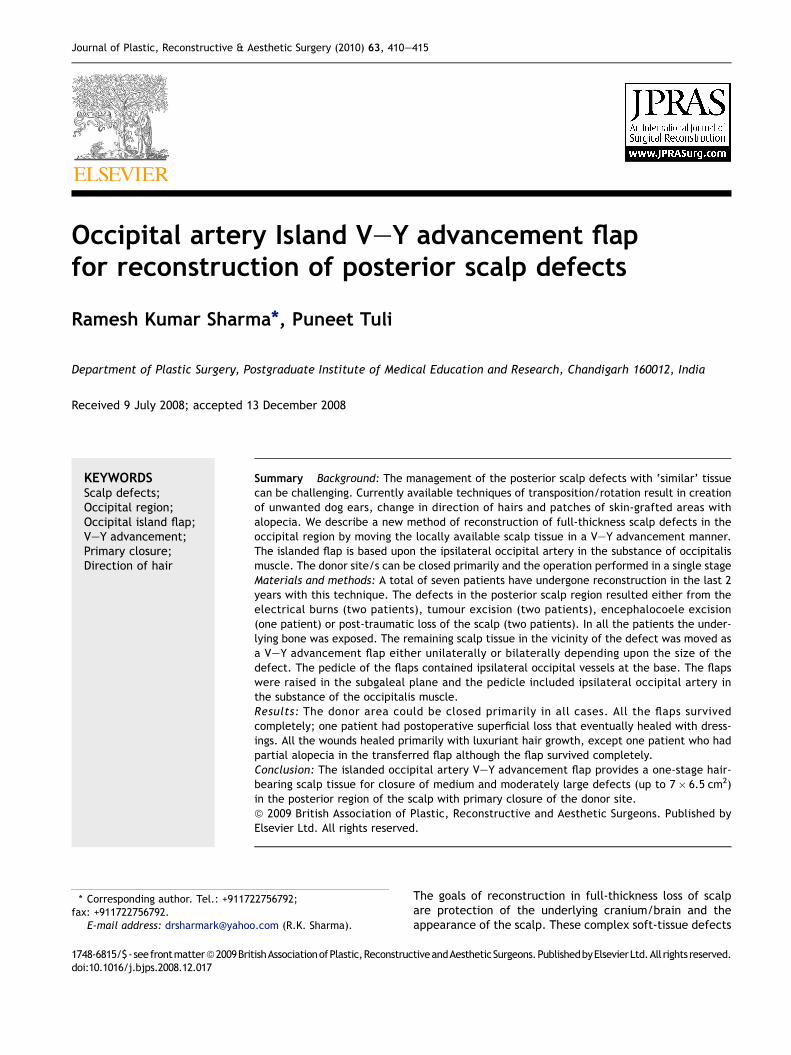
Figure 1 The occipital artery has been marked. The ‘V’-shaped flap has been designed with the base at the edge of thedefect and the tip at the mastoid. The dotted lines indicateincision for sub-dermal dissection of the pedicle of the flap.
Occipital artery Island VeY advancement flap 411
tax the ingenuity of the reconstructive surgeon, especiallyin the occipital region where very little local scalp tissue isavailable for reconstruction. The dictum e ‘replace liketissue with like tissue’ e holds true for scalp defects thanfor any other body locations because of the scalp’s hair-bearing characteristics.1
Many authors5e9 have described island flaps for recon-struction of the scalp defects in the parietal and temporalregions using the superficial temporal vessels or itsbranches. However, an island flap based on occipital vesselfor scalp defect has not been described in the literature sofar. We herein report our experience of VeY advancementflap based on occipital vessels for medium and moderatelylarge defects.
Materials, methods and results
Methods
The technique was used in seven patients in the last 2years; of these, five were male and two female (Table 1)patients. Single flaps were used in two patients and bilat-eral flaps were used in five patients.
Technique
Preoperatively, a hand-held Doppler probe is used to tracethe course of the occipital artery. A triangular flapadjoining the defect is designed in such a way that theoccipital artery enters the flap at an axis perpendicular tothe direction of movement of the designed flap. The baseof the island flap is designed adjacent to the defect, andthe tip of the flap is situated near the tip of the mastoidprocess (Figure 1). The margins of the flap are incised upto the dermis along both the superior and inferior limbs of‘V’. At the inferior limb, a vertical incision is made and theskin flaps are dissected at sub-dermal level so as todevelop a ‘pedicle’ consisting of sub-dermal tissue,occipital galeal muscle along with the occipital vesselsdeep in the muscle (Figure 2; Top). The incision along thesuperior limb is now deepened, and the flap is raised in the
Table 1 Patient characteristics and nature of defects
Sr. No. Name Age/Sex Aetiology of defect
1 GK 25 M Post-electric-burnexposed scalp
2 DV 7 M Post-encephalocoele3 KN 35 M Dermatofibrosarcoma
scalp4 MB 56 F Squamous cell
carcinoma scalp5 BK 45 F Post-traumatic exposed
skull bones6 KR 35M Fresh electric burn with
exposed bones7 PS 22 M Post-traumatic exposed
skull bones
subgaleal plane. At the level of the external occipitalprotuberance, the plane of flap elevation is subperiostealin order to avoid injury to the occipital vessels in thesubstance of the occipital muscle. The flap can now beeasily moved into the defect. If the flap size is inadequatefor reconstructing the whole defect or if the donor site isunder tension, a similar flap is designed on the oppositeside as well (Figure 2; Bottom). The donor site can be
Size of defect No. offlaps used
Complication
6� 5.5 cm Two Nil
5 cm� 4.5 cm Two Partial alopecia7� 6.5 cm Two Nil
5� 4.5 cm One Partial alopecia
5� 4 cm One Nil
5� 4.5 cm One Minor loss of flap;settled with dressings
6� 6 cm Two Nil
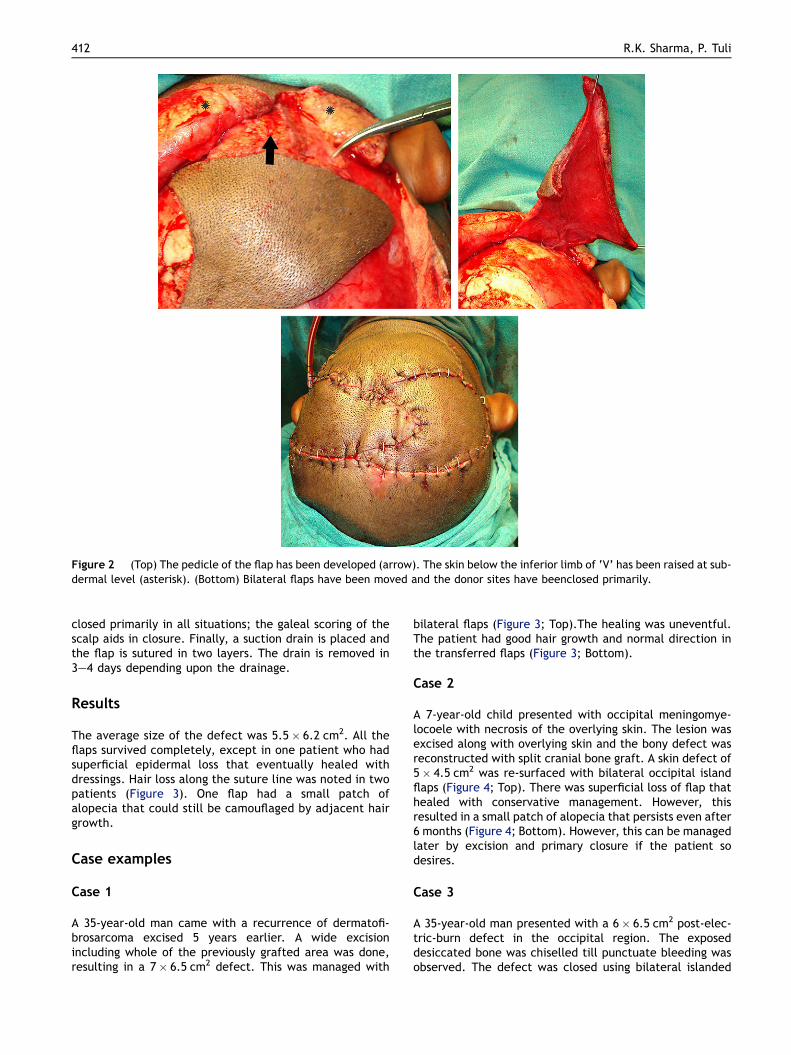
Figure 2 (Top) The pedicle of the flap has been developed (arrow). The skin below the inferior limb of ‘V’ has been raised at sub-dermal level (asterisk). (Bottom) Bilateral flaps have been moved and the donor sites have beenclosed primarily.
412 R.K. Sharma, P. Tuli
closed primarily in all situations; the galeal scoring of thescalp aids in closure. Finally, a suction drain is placed andthe flap is sutured in two layers. The drain is removed in3e4 days depending upon the drainage.
Results
The average size of the defect was 5.5� 6.2 cm2. All theflaps survived completely, except in one patient who hadsuperficial epidermal loss that eventually healed withdressings. Hair loss along the suture line was noted in twopatients (Figure 3). One flap had a small patch ofalopecia that could still be camouflaged by adjacent hairgrowth.
Case examples
Case 1
A 35-year-old man came with a recurrence of dermatofi-brosarcoma excised 5 years earlier. A wide excisionincluding whole of the previously grafted area was done,resulting in a 7� 6.5 cm2 defect. This was managed with
bilateral flaps (Figure 3; Top).The healing was uneventful.The patient had good hair growth and normal direction inthe transferred flaps (Figure 3; Bottom).
Case 2
A 7-year-old child presented with occipital meningomye-locoele with necrosis of the overlying skin. The lesion wasexcised along with overlying skin and the bony defect wasreconstructed with split cranial bone graft. A skin defect of5� 4.5 cm2 was re-surfaced with bilateral occipital islandflaps (Figure 4; Top). There was superficial loss of flap thathealed with conservative management. However, thisresulted in a small patch of alopecia that persists even after6 months (Figure 4; Bottom). However, this can be managedlater by excision and primary closure if the patient sodesires.
Case 3
A 35-year-old man presented with a 6� 6.5 cm2 post-elec-tric-burn defect in the occipital region. The exposeddesiccated bone was chiselled till punctuate bleeding wasobserved. The defect was closed using bilateral islanded
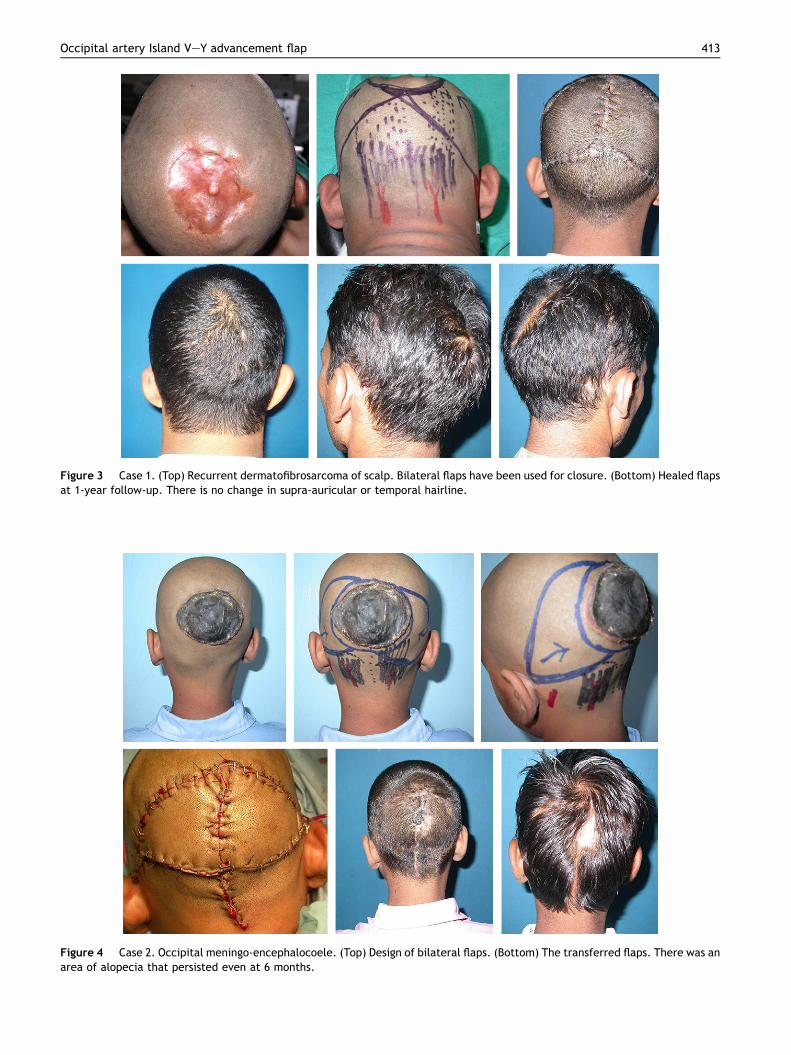
Figure 3 Case 1. (Top) Recurrent dermatofibrosarcoma of scalp. Bilateral flaps have been used for closure. (Bottom) Healed flapsat 1-year follow-up. There is no change in supra-auricular or temporal hairline.
Figure 4 Case 2. Occipital meningo-encephalocoele. (Top) Design of bilateral flaps. (Bottom) The transferred flaps. There was anarea of alopecia that persisted even at 6 months.
Occipital artery Island VeY advancement flap 413
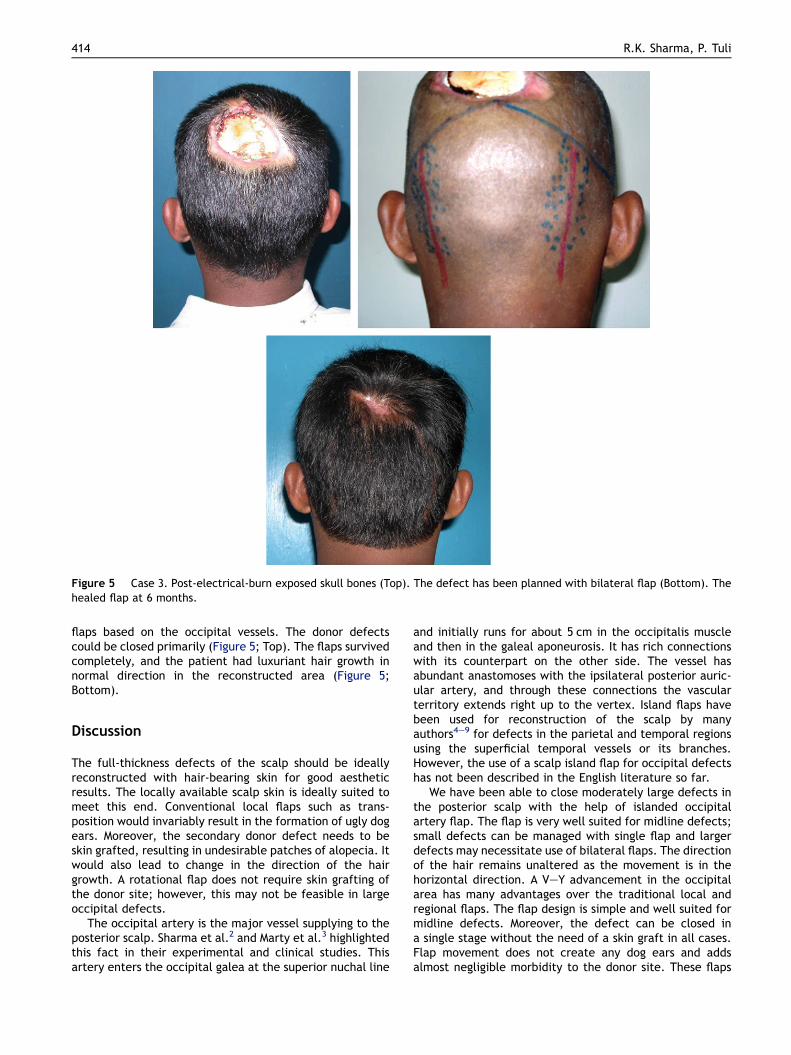
Figure 5 Case 3. Post-electrical-burn exposed skull bones (Top). The defect has been planned with bilateral flap (Bottom). Thehealed flap at 6 months.
414 R.K. Sharma, P. Tuli
flaps based on the occipital vessels. The donor defectscould be closed primarily (Figure 5; Top). The flaps survivedcompletely, and the patient had luxuriant hair growth innormal direction in the reconstructed area (Figure 5;Bottom).
Discussion
The full-thickness defects of the scalp should be ideallyreconstructed with hair-bearing skin for good aestheticresults. The locally available scalp skin is ideally suited tomeet this end. Conventional local flaps such as trans-position would invariably result in the formation of ugly dogears. Moreover, the secondary donor defect needs to beskin grafted, resulting in undesirable patches of alopecia. Itwould also lead to change in the direction of the hairgrowth. A rotational flap does not require skin grafting ofthe donor site; however, this may not be feasible in largeoccipital defects.
The occipital artery is the major vessel supplying to theposterior scalp. Sharma et al.2 and Marty et al.3 highlightedthis fact in their experimental and clinical studies. Thisartery enters the occipital galea at the superior nuchal line
and initially runs for about 5 cm in the occipitalis muscleand then in the galeal aponeurosis. It has rich connectionswith its counterpart on the other side. The vessel hasabundant anastomoses with the ipsilateral posterior auric-ular artery, and through these connections the vascularterritory extends right up to the vertex. Island flaps havebeen used for reconstruction of the scalp by manyauthors4e9 for defects in the parietal and temporal regionsusing the superficial temporal vessels or its branches.However, the use of a scalp island flap for occipital defectshas not been described in the English literature so far.
We have been able to close moderately large defects inthe posterior scalp with the help of islanded occipitalartery flap. The flap is very well suited for midline defects;small defects can be managed with single flap and largerdefects may necessitate use of bilateral flaps. The directionof the hair remains unaltered as the movement is in thehorizontal direction. A VeY advancement in the occipitalarea has many advantages over the traditional local andregional flaps. The flap design is simple and well suited formidline defects. Moreover, the defect can be closed ina single stage without the need of a skin graft in all cases.Flap movement does not create any dog ears and addsalmost negligible morbidity to the donor site. These flaps

Occipital artery Island VeY advancement flap 415
are sensate as the occipital nerves accompany the occipitalvessels and can be protected by careful sub-folliculardissection. The procedure can be safely used to closedefects up to 7.0� 6.5 cm2. We noted that small defects upto 4� 4.5 cm2 can be managed with single flap and largerdefects would necessitate bilateral flaps. Although hair lossalong the suture line was noted in few patients, we believethis complication can be decreased by carefully dissectingthe pedicle in the sub-dermal plane.
We find the islanded occipital artery flap to be veryadvantageous in management of defects in the posteriorscalp region. The flap provides a one-stage hair-bearing scalptissue for closure of medium and moderately large defects(up to 7� 6.5 cm2) with primary closure of the donor site.
All of the patients signed an informed consent form,including authorisation for the use of photographs inscientific publications and presentations.
Conflict of interest
None.
Funding
Nil.
References
1. Shestak KC, Ramasastry SS. Reconstruction of defects of thescalp and skull. In: Cohen M, editor. Mastery of Plastic andReconstructive Surgery, vol. 2. Boston: Little, Brown; 1994.
2. Sharma RK, Kobayashi K, Jackson IT, et al. Vascular anatomy ofgaleal occipitalis flap: a cadaver study. Plast Reconstr Surg1996;97:25e31.
3. Marty F, Montandon D, Gumener R, et al. Subcutaneous tissue inthe scalp: anatomical, physiological, and clinical study. AnnPlast Surg 1986;16:368e76.
4. Davis WH. Side burn reconstruction with an arterial VY hairbearing scalp after excision of Squamous cell carcinoma. PlastReconstr Surg 2000;106:94e7.
5. Tellioglu AT, Cimen K, Acar HI, et al. Scalp reconstructionwith island hair-bearing flaps. Plast Reconstr Surg 2005;115:1366e71.
6. Onishi K, Maruyama Y, Hayashi A, et al. Repair of scalp defectusing a superficial temporal fascia pedicle VY advancementscalp flap. Br J Plast Surg 2005;58:676e80.
7. Borah GL, Chick LR. Island scalp flap for superior foreheadreconstruction. Plast Reconstr Surg 1990;85:606e10.
8. De Haro F, Giraldo F. Bipedicled fronto-occipital flap forreconstruction of postoncologic defects of the lateral scalp.Plast Reconstr Surg 2001;107:506e10.
9. Mehrotra S, Nanda V, Sharma RK. The islanded scalp flap:a better regional alternative to traditional flaps. Plast ReconstrSurg 2005;116:2039e40.