Embed Size (px)
Citation preview

Journal of Neurology, Neurosurgery, and Psychiatry 1984;47:936-942
Occasional review
The differential diagnosis of congenital nystagmusMICHAEL GRESTY, NICHOLAS PAGE, HILARY BARRATT
From the MRC Neuro-Otology Unit, The National Hospital, Queen Square, London, UK
SUMMARY The decision whether a nystagmus is congenital or acquired may be difficult and is ofimportance in patients presenting with neurological complaints. In this article, established diag-nostic criteria are critically reviewed with particular emphasis on types of nystagmus waveformand their relationship to pursuit and optokinetic responses. Attention is drawn to certainacquired nystagmus which may have similar features which have hitherto been accepted aspathognomonic of congenital nystagmus. Symptoms due to congenital nystagmus are discussedand related to the oculomotor abnormalities. The importance of the characteristics of congenitalnystagmus are evaluated for use in differential diagnosis.
"Congenital nystagmus is observed at or shortly afterbirth and continues throughout life: it is sometimesassociated with movements of the head which tend todisappear." (Walshe and Hoyt 1969).
Congenital nystagmus may be horizontal but onrare occasions is vertical or torsional; it is usually,but not invariably, conjugate and consists of combi-nations of pendular and jerk nystagmus with linearand exponential waveforms there is frequently anull point or position of the eyes in which the nys-tagmus waveform affords best vision; if the nullpoint is eccentric this leads to a head turn in theopposite direction; there may be a family history ofnystagmus. Despite these variations a florid congeni-tal nystagmus has a distinctive appearance of hori-zontal oscillations in all positions of gaze, often ofhigh frequency, with irregular jerk and pendularmovements.Although congenital nystagmus is presumed to be
present from birth (or early infancy) it may not beobserved until later in life, when it may cause adiagnostic problem particularly if it resembles themore common forms of acquired nystagmus andneurological disease is suspected. Thus, Walshe andHoyt state that "It may be impossible to differenti-ate between congenital nystagmus and that associ-ated with disseminated sclerosis other than on thebasis of history and other evidences of disseminatedsclerosis" .' This article discusses the characteristics
Address for reprint requests: Dr M Gresty, MRC Neuro-OtologyUnit, The National Hospital for Nervous Diseases, Queen Sq,London WC1N 3BG, UK.
Received 21 February 1984Accepted 10 March 1984
of congenital nystagmus which can be helpful indiagnosis (table, compiled from recent texts'-') anddraws attention to the acquired forms of oculomotordisorders which have similar features.
PRESENCE OF NYSTAGMUS THROUGHOUT LIFEWe continue to encounter patients who undoubtedlyhave a marked congenital nystagmus which has pas-sed unnoticed until school age and, on occasions,adult life. There are several reasons why the nys-tagmus has not been detected. Firstly, the null pointof the nystagmus (at which the nystagmus is of min-imal amplitude) may subtend a wide angle of ocularmovement about the primary position of gaze inwhich case the nystagmus is only visible on eccentricgaze which the patient inherently avoids. Secondly,when the nystagmus waveform allows good fovea-tion, acuity is preserved and the person is asymp-tomatic. In these cases the nystagmus is detected atschool and armed service medicals, by opticians, andin medical examination for neurological symptoms.Some children are brought with compensatory headturn or head shaking without the nystagmus itselfhaving been noticed by the parents.
Alternatively, the nystagmus is observed but mis-taken for normal movements; it is thought to bea special feature of the child's eyes as opposed to anabnormality. For example, patients with congenitalnystagmus have told us that in their youth they weresaid to have eyes that were "twinkling", "dancing","roving" or "sexy"-adjectives which do not nec-cessarily imply abnormal movement. Some normalpeople have frequent square wave jerks of largeamplitude which are provoked by social eye contact.These "benign" square wave jerks have a superficial
936
Protected by copyright.
on 6 August 2019 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.47.9.936 on 1 Septem
ber 1984. Dow
nloaded from

The differential diagnosis of congenital nystagmus
Table Characteristics and diagnostic criteria ofcongenital nystagmus
May be dominant or sex linked recessive traitUsually noted during first few months of lifeThe pendular type is sometimes accompanied by head noddingPresence of a "null point" or position where nystagmus is least and vision bestSomtimes accompanied by turning of the headOften absent, asymmetrical and "defective" optokinetic responseAllways affects two eyes conjugately*Frequent other ocular anomalities: astigmatism, convergent strabismus,
hypoacitive vestibulo-ocular reflexesSuppressed by convergencePreservation of sufficient acuity for readingHead movements are (in some subjects) compensatoryAmplitude of eye and head movements diminish during maturationOccasionally multiplanar, monocular*Characterised by distinct waveforms (especially with exponentially increasing
slow phases)Binocular and uniplanar*Increased by fixation attemptNo oscillopsiaSometimes superimposed latent componentAbsent in sleepSimilar amplitude in both eyesOften an inversion of optokinetic responseHighly dependent on fixation with diminution abolition or reversal in darkness
or eye closureHigh frequency of nystagmus "beats" unusual in acquired nystagmusSome head movements are compensatory other are "involuntary" tremorsDeranged pursuit and vestible-ocular suppressionPursuit (includes fast onset OKN) can be inverted
937
Cogan (1956)2
Walshe and Hoyt (1969)'
Dell'Osso and Daroff (1975)3
Daroff et al (1978)4
Baloh and Honrubia (1979)5
Gresty and Halmagyi (1980)6Halmagyi and Gresty (1981)'Leigh and Zee (1982)'
*The authors would concur with Walshe and Hoyt that there are monocular and multiplanar forms of congenital nystagmus albeit these arerare and may have a different pathophysiology.
resemblance to nystagmus and may have anemotional significance (Dell'Osso and Gresty,personal observations), so it is not surprising thatsome nystagmus is misinterpreted as a normalphenomenon. In circumstances such as these, it maynot be possible to determine whether the nystagmushas been lifelong.
NYSTAGMUS WAVEFORMSTwelve waveforms of congenital nystagmus havebeen described consisting of combinations of jerkand pendular movements. These can be simplifiedfor the purposes of this discussion into pendular anduni-directional or bi-directional jerk waveforms (fig1). The cause of congenital nystagmus is a defect inthe slow eye movement system which is operatingunder unusual conditions of increased feedbackgain.9 The specific abnormality may be positivefeedback in eye position and velocity signals fromextra-ocular muscle proprioceptors.'° As a consequ-ence of this feedback instability, eye position isunstable and tends to "run away". This runawayconstitutes the slow phase of the nystagmus whichmay show linear or exponential increasing ordecreasing velocities. Saccades brake the slow phaseand return the eyes to the fixation point constitutingthe fast phases of the nystagmus. Objective record-ing of eye movements is necessary to distinguish the
waveforms; clinically it is only possible to differenti-ate pendular and jerk waveforms.When a unidirectional jerk nystagmus in the hori-
zontal plane has an exponentially increasing slowphase velocity then it is almost certainly congenital;there has only been one report of an acquired nys-tagmus having this waveform"I and in this case thenystagmus was in the vertical plane. The appearanceof an exponentially increasing slow phase mayappear artefactually on electro-oculographic record-ing of other nystagmus if there is a torsional compo-nent. This would be readily detected clinically by anexaminer alerted to the possibility of artefact. Asecond waveform which is undoubtedly congenital isthe bidirectional jerk nystagmus with exponentiallyincreasing slow phase velocities in both directions.When these waveforms are clearly identified thenthey are highly characteristic of congenital nystag-mus: however, many of the congenital waveformsshow linear or exponentially decreasing slow phasevelocities which may be mimicked by the waveformsof acquired nystagmus. Of particular note is that thependular forms of congenital nystagmus can closelyresemble the acquired variety.'2 Acquired pendularnystagmus can occur in conjunction with a jerk nys-tagmus, as in some cases of multiple sclerosis, result-ing in a complex waveform which resembles com-bined pendular and jerk forms of congenital nys-
Protected by copyright.
on 6 August 2019 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.47.9.936 on 1 Septem
ber 1984. Dow
nloaded from

RV20
Jt AJNC 20
Gaze evoked nystogmus
0
Gresty, Page, Barratt
Optokinetic responses
P"A-WADrum 600/s R
A/\J
NV
NB
0DW^N ll,NH
(M)XF
-A
RB
I-W" ls
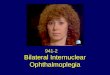
Fig 1 Waveforms: Examples ofnystagmus waveforms incentre, right and left gaze recorded from patients withcongenital and acquired nystagmus showing that they mayhave similar characteristics, A, congenital nystagmus withexponentially increasing slow phases ofunidirectional jerknystagmus, B, congenital nystagmus with bidirectional jerknystagmus in primary and right gaze and undirectional jerknystagmus in left gaze, C, congenital nystagmus withcombined pendular and jerk waveforms, D, combinedpendular and unidirectional jerk nystagmus in the pnrmaryposition ofgaze recorded from 24 year old male withproven multiple sclerosis, E, combined pendular and jerknystagmus, lutter and square wave jerks recorded from a34-year-old female with proven multiple sclerosis.
tagmus. Such acquired nystagmus waveforms arealso illustrated in figure 1.
OPTOKINETIC RESPONSESThe optokinetic response is the slow phase followingeye movement evoked by movement of large areasof the visual field. This is tested using a rotatingdrum which surrounds the patient and subtendsalmost the entire visual field. The patient isinstructed to stare straight ahead at the stripes sothat the response is not contaminated by gazeevoked (paretic) nystagmus or active followingmovements ("active optokinetic response"). Anormal optokinetic response will generate slowphase eye movements at velocities up to about 60°/second'3 with an upper frequency limit of 1-5 Hz.'4In congenital nystagmus optokinetic responses are
0D41Al~
Drum 600/s L KL
Drum 30°/s R
Drum 300/s LR30° ,IV\
(i) O \'N\V1NNNNN Drum UlOs R
L30°-is Drum I./s L
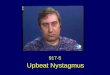
Fig 2 Reversed Optokinetic Responses: A and B,nystagmus in centre, right and left gaze and optokineticresponses recorded from patients with congenitalnystagmus. C, similar recordings taken from a 40 year oldfemale with acquired PAN, dysarthria and gait ataxia. Thenystagmus is illustrated in the right beating phase.
nearly always abnormal:5-'9 they may havederanged waveforms, abnormally high or low slowphase velocities, or be absent or reversed as illus-trated in fig 2.The reversal of the slow phase direction of the
optokinetic response may be uni or bi-directional. Itmay occur with all velocities of stimulus or be pro-voked at certain velocities. It has been consideredthat a reversed optokinetic response, that is wherethe slow phase of the nystagmus is in the oppositedirection from the direction of movement of the vis-ual field, is pathognomic of congenital nystag-mus.20 21 However this is not the case; an apparentlyreversed optokinetic response may occur in acquiredoculomotor disease when there is a second or thirddegree spontaneous nystagmus and no optokineticreflex. Under these conditions the optokineticresponses will apparently be present to stimuli in thedirection of the slow phase of the nystagmus andreversed in the opposing direction.
Periodic alternating nystagmus, which may be of a
congenital or acquired variety, is a specific case of athird degree nystagmus which changes directionover a time period of several tens of seconds(reviewed by Rudge, 198322). The nystagmus con-tinues through pursuit and optokinetic stimuli andtrue optokinetic responses are minimal or absent.The result is that during the right beating phase ofthe nystagmus optokinetic responses appear to be inthe normal direction for leftwards stimuli andreversed to rightwards stimuli. When the spontane-ous nystagmus reverses to beating leftwards, the
938
(D
Protected by copyright.
on 6 August 2019 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.47.9.936 on 1 Septem
ber 1984. Dow
nloaded from

The differential diagnosis of congenital nystagmus
inverse pattern of 'optokinetic" responses appears(fig 2).
In acquired oculomotor disorders reversal of theoptokinetic response only occurs in one direction atany one time which is determined by the direction ofthe spontaneous nystagmus. In congenital nystag-mus bidirectionally reversed optokinetic responsesmay sometimes occur although the reversal is moreoften unidirectional and occurs only at certainstimulus velocities. The presence of bidirectionallyreversed optokinetic responses, when an alternatingnystagmus has been excluded, is pathognomonic ofcongenital nystagmus.
PURSUIT RESPONSESThe pursuit response is a slow phase eye movementevoked by a small target moving across the visualfield. Pursuit is usually tested using sinusoidal andtriangular waveforms of target motion which arevaried in velocity and frequency. Normal pursuitmovements, within certain velocity and frequencylimits (<1 Hz, <3YS40o/s2-324) closely follow thetrajectory of the target with minimal saccadic inter-ruptions.The majority of patients with congenital nystag-
mus do not have an organised slow phase of smoothpursuit; the envelope of eye movement accuratelymatches the target trajectory but the congenital nys-tagmus waveform is superimposed which gives theappearance of a grossly impaired response.2' In sub-jects whose congenital nystagmus shows a clearlydefined null point, that is those with jerk waveformson lateral gaze, pursuit is impaired in the followingway, as illustrated in fig 3: attempts to pursueinfluence the position of the null point of the nys-tagmus so that the null point shifts to the left whenthe eyes are moving towards the right and vice versa.In consequence, when the eyes are moving towardscentre from lateral gaze the superimposed nystag-mus has a slow phase in the opposite direction to thetarget motion, which gives the appearance of"reversed pursuit". Although reversal of pursuit,specifically during target motion towards centre, isstrongly indicative of congenital nystagmus, a simi-lar reversal can occur when there is acquired thirddegree, centripetal or periodic alternating nystag-mus.Emphasis here is laid on the significance of rever-
sal of pursuit occurring when the eyes are trackingfrom an eccentric position towards centre gaze.Apparent reversal of pursuit for movements awayfrom centre is a common finding in acquiredoculomotor disorders which occurs when there is acombination of absent pursuit and gaze paretic nys-tagmus. In all forms of pendular nystagmus, congen-
0D
939
Gaze evoked nyVnagmus Pursuit responses
sTar;get MT
R30
L30 K Bls
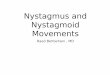
Fig 3 Pursuit Responses: Nystagmus in centre, right andleft gaze and pursuit responses to sinusoidal target motion ata frequency of 0-2 Hz, peak amplitude of20' (red lasertarget at 2 m distance). A and B, congenital nystagmus. C,Third degree spontaneous nystagmus in a 30-year-oldfemale with a 16 year history of idiopathic spino-cerebellardegeneration. D, acquired periodic alternating nystagmus(same patient as fig 2).
ital or acquired, the nystagmus waveform issuperimposed on the pursuit movement and can givethe appearance of reversal.Mechanism of reversed pursuit and optokinetic responses:Hood and Leech25 proposed that in congenital nystagmusthere is an algebraic addition of the nystagmus waveformand the optokinetic response which produces a compositewaveform giving the impression of a fast phase in the direc-tion of the stimulus and an inverted slow phase. The alter-native theory, which has had widespread acceptance,26springs from the observation by Halmagyi et a120 andDell'Osso2' that the waveforms of inverted optokineticresponses are similar to the spontaneous gaze evoked nys-tagmus. This suggests that the optokinetic stimulus shiftsthe null point of the congenital nystagmus in the oppositedirection to the stimulus motion. The nystagmus evoked bygaze in the direction of stimulus motion also shifts so that itextends across the range of movement. This nystagmuspersists during the eye movement and has a slow phase inthe opposite direction to the stimulus motion which givesthe appeararnce of an "inverted" response. The inversionof pursuit responses is explained similarly.Both of these theories are inadequate to explain the
wide variety of responses encountered when large numbersof subjects with congenital nystagmus are examined indetail.'9 It is quite clear that not all waveforms of invertedoptokinetic responses can be construed either as combina-tions of normal optokinetic and congenital nystagmus oras manifestations of gaze evoked nystagmus provoked byshifts of the null point. Trace A of fig 2 shows examples of
Protected by copyright.
on 6 August 2019 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.47.9.936 on 1 Septem
ber 1984. Dow
nloaded from

940
exceptions. The response to drum rotation to the rightclosely resembles the nystagmus seen in the region of thenull and not the nystagmus of rightwards gaze. In additionresponses to leftwards stimuli have an exponentially decay-ing waveform and not the exponentially increasingwaveform of the leftwards gaze evoked nystagmus. In con-
trast the optokinetic responses of fig 2 B resemble thegaze evoked nystagmus as if the null had shifted. Our ownexperience is that shifting of the null point during pursuitand optokinetic stimuli is a variable phenomena which can
fluctuate from moment to moment in response to stimulusdirection and velocity. At present there is no explanationof these phenomena.
ABNORMAL HEAD MOVEMENTS AND POSTURESASSOCIATED WITH NYSTAGMUSIt is currently accepted that two forms of head shak-ing may be associated with congenital nystagmus.fFirstly, there is involuntary head tremor which doesnot improve visual acuity and secondly, there are
compensatory movements of the head which areopposite in direction to the beating of the nystag-mus. Tremor and compensatory shaking can be dif-ferentiated by asking the patient to read a Snellenchart with head free and head held stationary-ifvision improves significantly when the head is free tomove then the shaking is compensatory.We have recently observed a third type of head
movement in a patient referred by Mr Peter Fells ofMoorfields Eye Hospital. The patient, with definitecongenital nystagmus, shook her head rhythmicallyto improve her vision. Eye and head movementrecordings revealed that during head shaking thenystagmus was suppressed and replaced by normalcompensatory "dolls head" eye movements. Headshaking which suppresses nystagmus is alsoobserved in the rare entity of spasmus nutans,6which is a high frequency nystagmus that developsduring infancy and is reported to remit during child-hood. We have also observed the suppression ofacquired pendular nystagmus by head shakingalthough the patients do not seem to adopt thismanoeuvre to improve visual acuity. The requiredcondition for the suppression of nystagmus appearsto be vestibular stimulation, for the suppression alsooccurred during passive movements.Abnormal head postures adopted to improve vis-
ual acuity occur frequently with congenital nystag-mus but may also result from acquired nystagmus. Ineach case there is a position or positions of the eyesin the orbit in which nystagmus has the least amp-litude or the lowest frequency, and in which vision isbest. Accordingly, the head is turned to an eccentricposition which allows the eyes to fixate from theorbital position which affords best acuity. Inperiodic alternating nystagmus the head posture var-
ies as the null point of the nystagmus shifts with the
Gresty, Page, Barratt
reversal of the nystagmus.Shaking and posturing of the head to improve vis-
ual acuity are extremely rare in acquired oculomotordisorders. Such manoeuvres, particularly if long-standing, are most likely to indicate congenital nys-tagmus. Involuntary movements and abnormalpostures of the head unrelated to visual acuity haveno differential diagnostic value and occur commonlyin neurological disorders.628
VESTIBULAR RESPONSES TO ROTATIONALTESTINGAbnormalities of responses to rotational testingoccur in about 50% of asymptomatic patients withcongenital nystagmus.2930 Short or apparentlyabsent responses to rotational steps may occur, withpersistence of the spontaneous nystagmus whichswamps or masks any induced nystagmus. Wander-ing eye movements and extreme gaze deviations inthe dark as a consequence of lack of position orvelocity sensitivity in these subjects may also maskany underlying vestibular response and do not per seindicate vestibular derangement. In contrast, testingwith sinusoidal stimuli shows appropriate phasemodulation of the spontaneous nystagmus suggest-ing that underlying vestibular function is essentiallynormal. In asymptomatic patients, highly abnormalresponses that defy conventional neuro-otologicalinterpretation strongly suggest the presence ofcongenital nystagmus.
FLUCTUATIONS IN AMPLITUDE OF NYSTAGMUSWITH FIXATION/DARKNESS/EYE CLOSURECongenital nystagmus changes its characteristics inthe presence or absence of vision. The nystagmushas the most consistent waveform and amplitudewith fixation. In darkness the amplitude mayincrease or the nystagmus may cease. The nystag-mus almost always disappears with eye closure. Incontrast most forms of acquired nystagmus persist indarkness and with eye closure and may increase inamplitude and slow phase velocity. In some forms ofacquired nystagmus the brainstem mechanismswhich generate the fast position corrective phase arealso defective. Accordingly, in darkness or with eyeclosure, fast phases may not be generated and theeyes drift with the slow phase.3' Thus, the rare com-bination of maintainance of a steady gaze position inthe dark together with the cessation of nystagmus isstrongly indicative of congenital nystagmus.
SYMPTOMATOLOGYThe commonest symptom of congenital nystagmus isreduced visual acuity which can range from mild tosevere. The patients describe their visual impair-
Protected by copyright.
on 6 August 2019 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.47.9.936 on 1 Septem
ber 1984. Dow
nloaded from

The differential diagnosis of congenital nystagmus
ment in terms of blurring and defocussing. Clearly,there is least impairment at the null point of thenystagmus which, if eccentric, leads to a markedhead turn which may itself be symptomatic. Whenthe patient looks with his eyes away from the nullpoint (nystagmus being faster and/or larger amp-litude) then blurring increases with a loss of acuitywhich can be detected on a Snellen chart. Nystag-mus of high frequency is particularly detrimental tovisual acuity and we have encountered one patientwith beats in excess of 7/second who was effectivelyblind.When viewing a stationary target under normal
illumination oscillopsia is generally not a symptomof congenital nystagmus regardless of eye position.We have, on rare occasions, encountered a patientwith congenital nystagmus who does experienceoscillopsia under these conditions. Their nystagmushas been intermittent or alternating with long quies-cent periods. Presumably these individuals have notbeen forced to adapt to their involuntary eye move-ments unlike those with continuous nystagmus.Oscillopsia may occur under the unusual conditionsof viewing solitary points of light in darkness andthere may be excessive awareness of the flicker offluorescent lights.More frequently, patients experience oscillopsia
when attempting to track moving targets such asreading the number of a moving omnibus. Underthese circumstances it would seem that the deficit inthe pursuit system becomes symptomatic. Allpatients with congenital nystagmus have greatdifficulty in reading within a moving vehicle whichrequires suppression of the vestibulo-ocular reflexby a mechanism closely related to pursuit.7 Theyexperience increased blurring of vision and havesymptoms of motion sickness. Some report blurringof a moving visual scene, for example when theylook out of a train window; this may result fromtheir abnormal optokinetic responses.
In general people with congenital nystagmus havefew complaints apart from reduced acuity. The prob-lems for the clinician lies in the interpretation oftheir symptoms which are not in commonplaceexperience.
Conclusions
The clinician should be aware of the possibility ofcongenital nystagmus when a patient presents with amarked nystagmus which seems inappropriate toother neurological symptoms and signs. Diagnosiscan be particularly difficult when there is a less floridcongenital nystagmus which is of low amplitude inlateral gaze and has a large null region which thusresembles the usual acquired gaze evoked nystag-
941
mus. In the absence of a definite lifelong history ofnystagmus a detailed oculomotor examinationshould be performed with special attention to theslow eye movement systems. In problem patientsobjective recordings of eye movements may beneeded which can elucidate characteristic nystagmuswaveforms, pursuit and optokinetic responses.
Nicholas Page was supported financially by theSmith Charity.
References
'Walshe FB, Hoyt WH. Clinical Neuro-ophthalmology.Vol 1. Baltimore, Williams and Wilkins. 1969.
2 Cogan DG. Neurology of the Ocular Muscles. Spr-ingfield, Ill. CC Thomas. 1956.
3Dell'Osso LF, Daroff RB. Congenital nystagmuswaveforms and foveation strategy. Documenta Oph-thalmologica 1975;39:155-82.
Daroff RB, Troost BT, Dell'Osso LF. Nystagmus andrelated ocular oscillations. In: Glaser JS ed. Neuro-Ophthalmalogy. Hagarstown, Maryland. Harper andRow, 1978:219-43.
Baloh RW, Honrubia V. Clinical Neurophysiology oftheVestibular System. Philadelphia, Davies FA. 1979.
6 Gresty MA, Halmagyi GM. Abnormal head movements.J Neurol Neurosurg Psychiatry 1979;42:705-14.
Halmagyi GM, Gresty MA. Clinical signs of visual ves-tibular interaction. J Neurol Neurosurg Psychiatry1979;42:934-9.
8 Leigh RJ, Zee DS. The Neurology of Eye Movements.Philadelphia. Davis FA. 1982.
Dell'Osso LF, Gauthier G, Liberman G, Stark L. Eyemovement recordings as a diagnostic tool in a case ofcongenital nystagmus. Am J Optom and Arch AmAcad Ophthmol 1972;49:3-13.
'0 Zee DS, Optican LM. J Bio Eng 1984 In press."Zee DS, Leigh J, Mathieu-Millaire F. Cerebellar control
of ocular gaze stability. Ann Neurol 1980;7:37-40.12 Gresty MA, Ell JJ, Findley LJ. Acquired pendular nys-
tagmus: its characteristics, localising value andpathophysiology. J Neurol Neurosurg Psychiatry1982;45:431-9.
3 Honrubia V, Downey WL, Mitchell DP, Ward PH.Experimental studies on optokinetic nystagmus. II.Normal Humans. Acta Oto-laryngol 1968;65:441-8.
4 Tinker D, Sieber J, Bartual J. Schuingungsanalyse dervestubulaer, optokinetisch und durch elektrischeReizungausgelosten Augenbewegungen beim Mens-chen. 1 Mittleilung: Steitge Augenbewegungen: Fre-quenzgange und Ootskurven. Kybernetik1961; 1:21-8.
Barany R, Zur Klinik und Theorie des Eisenbahn nys-tagmus. Acta Oto-laryngol 1921;3:260-5.
6 Brunner H. Zur Klinischen der Inversion desoptokinetischen Nystagmus. Albrecht v Graeves ArchOphthalmol 1922; 129:30-56.
Dichgans J, Jung R. Oculomotor anbnormalities due tocerebellar lesions. In: Lennerstrand G, Bach-Y-Rita P. Basic Mechanisms ofOcular Motility and Their
Protected by copyright.
on 6 August 2019 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.47.9.936 on 1 Septem
ber 1984. Dow
nloaded from

942
Clinical Implications. Pergamon, Oxford. 1975:281-98.
8 Abadi RV, Dickinson CM, Lomas MS. Inverted andasymmetrical optokinetic nystagmus. In: Lenners-trand G, Zee DS, Keller E, eds. Functional Basis ofOcular Motility Disorders. Ne'w York: Pergamon.1982:143-6.
9 Kommerell G, Mehdorn E. Is an optokinetic defect thecause of congenital nystagmus? In: Lennerstrand G,Zee DS, Keller E, eds. Functional Basis of OcularMotility Disorders. New York: Pergammon.1982:159-67.
20 Halmagyi GM, Gresty MA, Leech J. Reversed optokine-tic nystagmus (OKN): Mechanism and clinicalsignificance. Ann Neurol 1980;7:429-35.
21 Dell'Osso LF. Congenital nystagmus: basic aspects. In:Lennerstrand G, Zee DS, Keller, eds. FunctionalBasis of Ocular Motility Disorders. New York:Pergammon. 1982:129-38.
22 Rudge P. Clinical Neuro-Otology. Edinburgh, ChurchillLivingstone. 1983.
23 Stark LG, Vossius G, Young LR. Predictive control ofeye tracking movements. IRE Trans. Human Factorsin Electronics 1962:HLE3:52-7.
24 Young LR. Pursuit eye tracking movements. In:
Gresty, Page, Barratt
Bach-Y-Rita P, Collins CC, eds. The Control of EyeMovements. New York: Academic Press. 1971:429-44.
25 Hood JD, Leech J. The significance of peripheral visionin the perception of movement. Acta Otolaryngol1974;77:72-9.
26 Kommerell G. Congenital nystagmus: discussion. In:Lennerstrand G, Zee DS, Keller E, eds. FunctionalBasis of Ocular Motility Disorders. New York: Per-gammon. 1982:169-70.
27 Gresty MA, Ell JJ. Normal modes of head and eye coor-dination and the symptomatology of their disorder. In:Lennerstrand G, Zee DS, Keller E, eds. FunctionalBasis of Ocular Motility Disorders. New York: Per-gammon. 1982:391-405.
28 Brain WR. On the rotated or "Cerebellar" posture ofthe head. Brain 1926;49:61-76.
29 Forssman B. A study of congenital nystagmus. ActaOto-laryngol 1964;57:427-49.
Yee RD, Baloh RW, Honrubia V, Kim YS. A study ofcongenital nystagmus: vestibular nystagmus. J Oto-laryngol 1981;10:89-98.
3' Leech J, Gresty MA, Hess K, Rudge P. Gaze failure,drifting eye movements and centripetal nystagmus incerebellar disease. Br J Ophthalmol 1977;61:774-81.
Protected by copyright.
on 6 August 2019 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.47.9.936 on 1 Septem
ber 1984. Dow
nloaded from