Embed Size (px)
DESCRIPTION
OBVIOUS DIFFERENCES. Other medical conditions in adults - effects of [subclinical] organ dysfunction on drug disposition Better tolerance in children with ability to deliver repetitive courses more easily (eg. l-aspariginase) Need for more of a focus on long term toxicities in children. - PowerPoint PPT Presentation
Citation preview
OBVIOUS DIFFERENCES
• Other medical conditions in adults
- effects of [subclinical] organ dysfunction on drug disposition
• Better tolerance in children with ability to deliver repetitive courses more easily (eg. l-aspariginase)
• Need for more of a focus on long term toxicities in children
“BIOLOGIC” ISSUES• Cytogenetics
- differing incidence of tel/AML, hyperdiploidy, t(9;22)
- similar impact of t(4;11), t(8;14) and variants
- unknown effect of hypodiploidy, t(1;19) in adults but probably similar
(favorable - rare in adults)
(unfavorable - much more common in adults)
“Nobody does it better” (attributed to James Bond)
How about pediatric vs adult oncologists??
Outcome of adolescents and young adults with ALL: A comparison of Children’s Cancer Group (CCG) and Cancer and Leukemia Group B regimens [2009].
Stock, Sather, Dodge, Bloomfield, Larson, Nachman for CALGB and CCG.
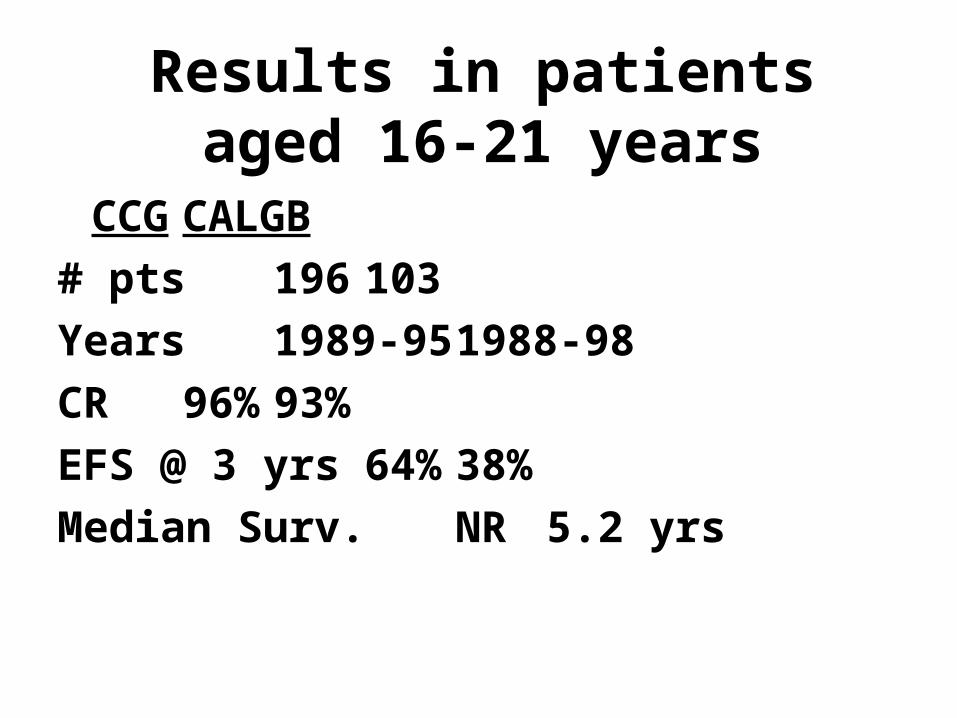
Results in patients aged 16-21 years
CCGCALGB
# pts 196 103
Years 1989-95 1988-98
CR 96% 93%
EFS @ 3 yrs 64% 38%
Median Surv. NR 5.2 yrs
POSSIBLE EXPLANATIONS
• Risk factors - groups were very similar except for slightly more pts (10 vs 5%) with t(9;22) or t(4;11) in the CALGB group
• Regimens
• Doses delivered
• Physicians and sites of treatment
Differences in:
Highly Specific Agents• Targeted inhibitors - STI571, antisense• Antibodies - anti CD33
Cytotoxics• Maybe a bit specific - 506U• Plain old new drugs
Supportive Care• Cytokines• Cardioprotectants
“Broad” Biologic Activity• Antiangiogenesis
In some ways this is also a discussion about how to develop therapeutic agents for uncommon (ie economically uninteresting for pharmaceutical companies) disorders.
Currently, this is a major issue re the discovery and development of molecularly targeted therapies for hematologic manignancies.
PROGNOSTIC FACTORS
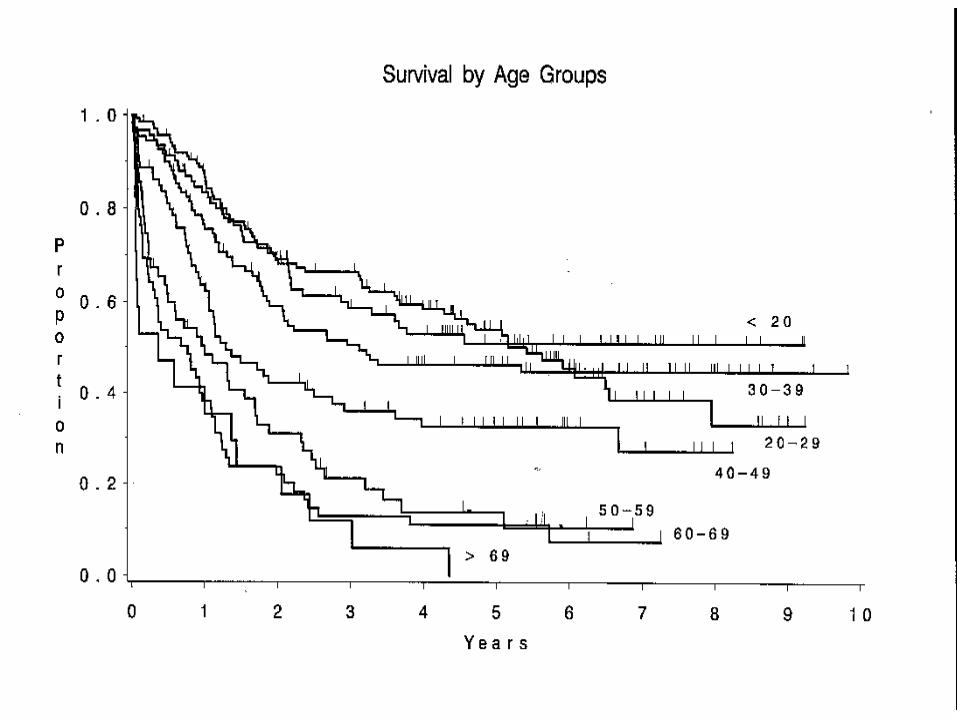
• Age (or stage??) • “Leukemia” vs “lymphoma”• LDH (or stage??)• CNS involvement at diagnosis• BUT…… many older patients with
ALL and CNS disease are cured
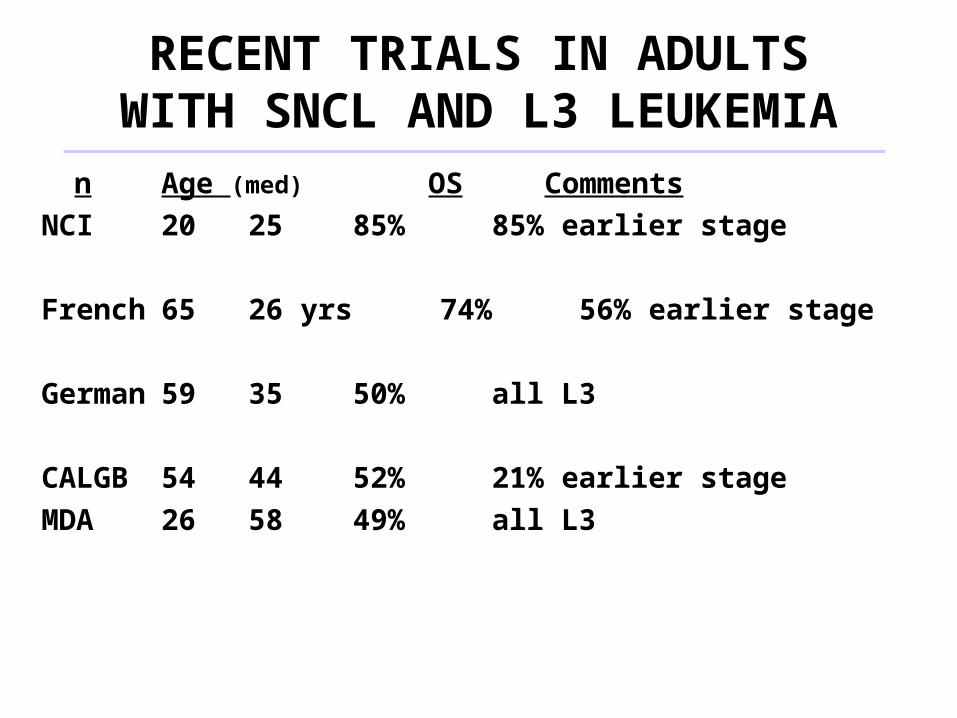
RECENT TRIALS IN ADULTS WITH SNCL AND L3 LEUKEMIA
n Age (med) OS Comments
NCI 20 25 85% 85% earlier stage
French 65 26 yrs 74% 56% earlier stage
German 59 35 50% all L3
CALGB 54 44 52% 21% earlier stage
MDA 26 58 49% all L3
STI 571 DOSING
Should Shaquille O’Neal and Mugsy Bogues receive the same dose simply because they are both old enough to vote?
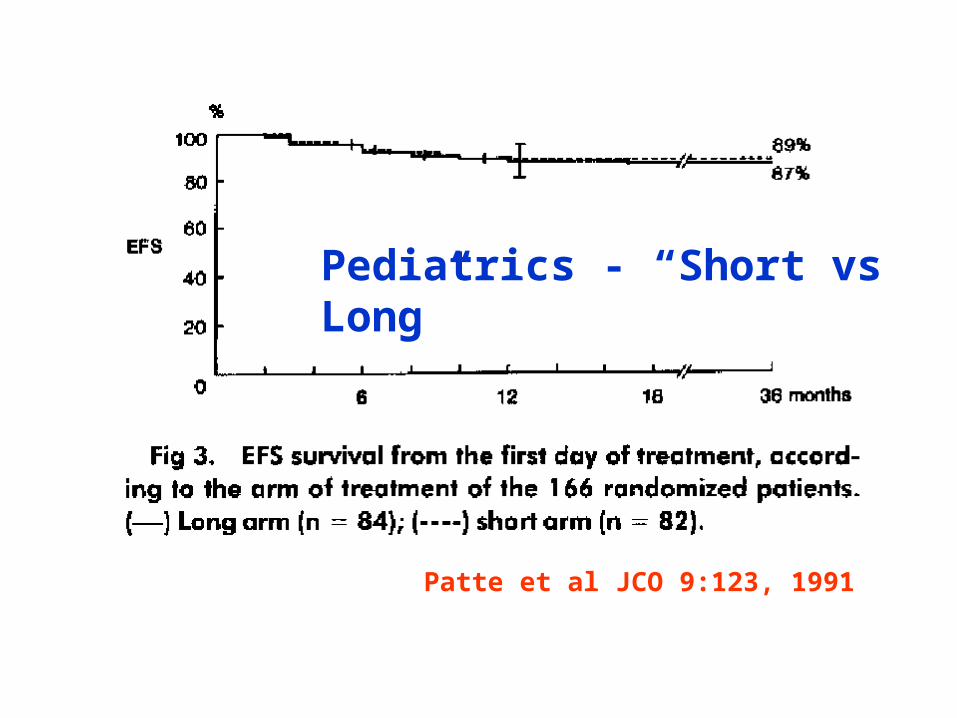
Pediatrics - “Short vs Long”
Patte et al JCO 9:123, 1991
Years from Study Entry
Pro
po
rtio
n
0 2 4 6
0.0
0.2
0.4
0.6
0.8
1.0
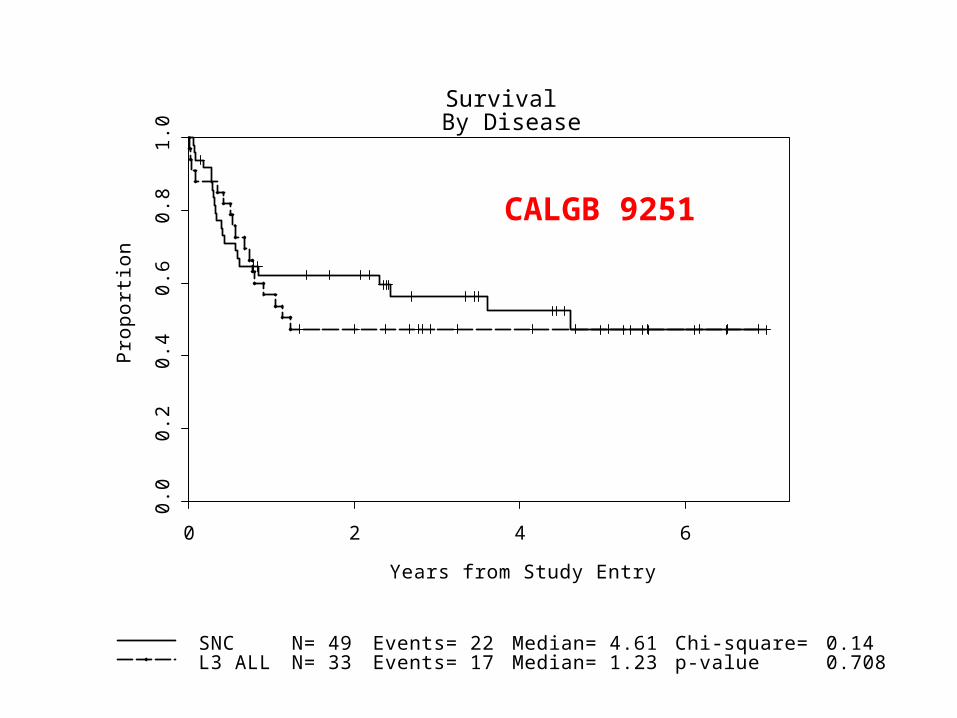
Survival By Disease
SNCL3 ALL
N= 49N= 33
Events= 22Events= 17
Median= 4.61Median= 1.23
Chi-square=p-value
0.140.708
CALGB 9251





























