Embed Size (px)
DESCRIPTION
Document
Citation preview
Obstetric Complications
Hypertensive Disorders of Pregnancy❏ Chronic HTN
❏ before 20 weeks❏ Gestational HTN (PRH)
❏ after 20 weeks❏ Preeclampsia
❏ more than or equal to 140/90 consistently❏ Preeclampsia superimposed on chronic HTN❏ Eclampsia
Risk Factors for Pregnancy Related HTN (PRH)❏ First pregnancy❏ Age > 35 (younger than 19 and over 40 in book)❏ Family history❏ Pre-existing HTN or pre-existing vascular disease❏ Renal disease❏ Obesity❏ DM❏ Multifetal pregnancy❏ Mother or sister with pre-eclampsia
Preclampsia
❏ What is it?❏ HTN, proteinuria, generalized edema❏ generalized edema: loss of protein causes fluid to shift to interstitial space❏ epigastric (non the main one though)
❏ When does it occur?❏ last half of pregnancy
❏ Beside HTN, what else would be present?❏ Effect of fetus
❏ decrease perfusion ❏ IUGR (IntraUterine Growth Restriction), baby can be term but small
❏ What is the cure?❏ delivery
Preventive Measures❏ Measures work best with high risk reoccurrences❏ Prenatal monitoring❏ meds: applicable on high risk women but does not seem to work on low risk women
❏ Low dose aspirin❏ Ca, Mg, Fish oil Supplements
Effects of Increased Vascular Resistance
❏ Renal perfusion❏ Proteins❏ Vascular volume: edema❏ Liver circulation: epigastric pain, liver not being perfused well❏ Cerebral vessels: headache and visual disturbances❏ Colloid oncotic pressure❏ Placental circulation❏ Vasospasm and vasoconstriction
❏ decreases blood flow to major organs → damages glomerulus and leaks protein → protein decreases osmotic pressure → results in edema → Na and H2O retention to increase HR to increase BP → increases edema even more → decrease perfusion to liver → results in epigastric pain → decrease perfusion causes headache and visual disturbances

ManifestationsClassic signs❏ BP increases❏ test for protein (24 hour urine test), then dipstick❏ Women with UTI watch for false positive❏ Deep tendon reflexes Additional signs❏ Liver enzymes may be up, creatinine and BUN may be up❏ Edema in the hands, face
CV system❏ Increased
❏ Response to angiotensin II❏ BP❏ SVR
❏ Decreased❏ CO❏ Plasma volume: protein loss due to the fluid shifting to the interstitial space
Hematologic❏ Increased
❏ Hemoconcentration❏ high H&H
❏ Viscosity❏ Platelet clumping
❏ Risk for strokes❏ Thrombocytopenia
❏ Risk for bleeding❏ Endothelium damage
Neurologic❏ Arterial vasospasm❏ Rupture of small capillaries❏ Small hemorrhages❏ Headache **❏ Hyperreflexia ** → Deep tendon Reflexes❏ Convulsions (eclampsia)
Renal❏ Decreased
❏ GFR❏ Colloid osmotic pressure
❏ Damage to glomeruli❏ Proteinuria❏ Fluid shift (edema)
❏ Hypovolemia❏ Increase
❏ HCT❏ Angiotensin II and aldosterone❏ BUN and Cr and uric acid

Hepatic
❏ Impaired
❏ Hepatic edema
❏ Epigastric pain
PlacentaDecreased❏ Perfusion❏ Fetal hypoxemia
❏ Acidosis: not enough O2❏ Perinatal death
❏ Nutrients❏ IUGR
Mild Preclampsia❏ Activity restrictions
❏ might be able to stay at home as long as patient adheres with plan❏ Rest few times a day to decrease pressure on v. cava❏ BP same position and same arm❏ kick counts
❏ UA❏ Fetal assessment❏ Diet:
❏ Lots of proteins and calories in diet❏ Na restriction
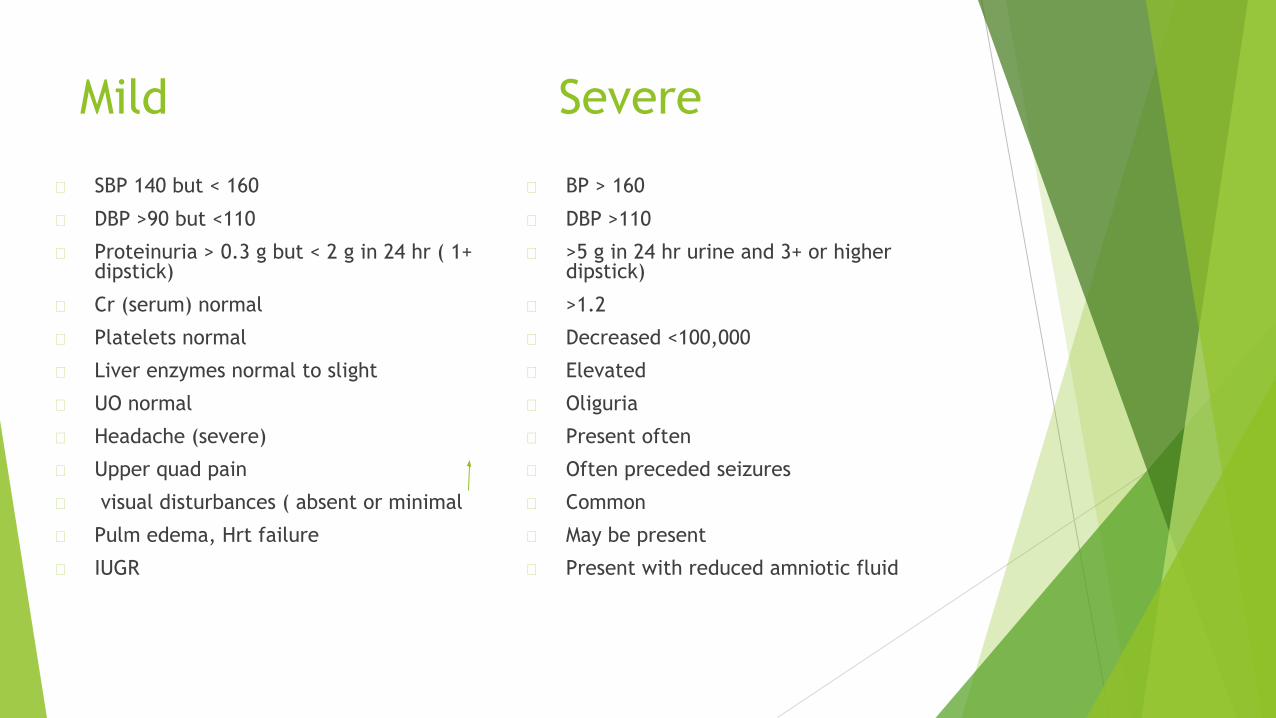
Mild Severe
� SBP 140 but < 160
� DBP >90 but <110
� Proteinuria > 0.3 g but < 2 g in 24 hr ( 1+ dipstick)
� Cr (serum) normal
� Platelets normal
� Liver enzymes normal to slight
� UO normal
� Headache (severe)
� Upper quad pain
� visual disturbances ( absent or minimal
� Pulm edema, Hrt failure
� IUGR
� BP > 160
� DBP >110
� >5 g in 24 hr urine and 3+ or higher dipstick)
� >1.2
� Decreased <100,000
� Elevated
� Oliguria
� Present often
� Often preceded seizures
� Common
� May be present
� Present with reduced amniotic fluid
Goals for treatmentMaternal goals
❏ Avoid Seizures❏ Increase CO❏ Prevent complications such as stroke
Fetal goals❏ Improve placental blood flow❏ Fetal Oxygenation
Inpatient Management Severe PreeclampsiaMost are hospitalized and put in private room
❏ Bedrest: cannot get up to use bathroom, bathe in bed❏ Antihypertensive❏ Anticonvulsants❏ Intrapartum management❏ Low stimulus environment: low lighting, no noise, soft relaxing music
Antihypertensives❏ Hydralazine: used often due to its history of safety, increases CO and improves
perfusion❏ Calcium channel❏ Beta blocker: decreases BP and HR
Anticonvulsants❏ Magnesium Sulfate (not really an anticonvulsants nor antihypertensive)
❏ Preeclampsia seizures❏ Prevents seizures❏ Given even after birth
❏ CNS depressant: Relaxes smooth muscles and uterus❏ Reduces vasoconstriction❏ Relaxes brain activity to prevent seizures
❏ seizures occurs 24 - 48 hrs after birth → watch mother carefully❏ may be on pitocin❏ Epidural is not given if pt has coagulation problems❏ IV❏ Safe❏ Therapeutic levels 4-8 mg/dl for MgSO4 for patients with preeclampsia
❏ IV, secondary infusion (for MgSO4 and Pitocin)❏ must have a primary bag of fluid hanging
❏ Recovery: UOP decrease, BP goes back to normal

Nursing ProcessAssessment❏ One-one nurse patient ratio: (like a little ICU: continuous monitoring when patient is
on MgSO4 and Pitocin)❏ Head to toe❏ Weight❏ Vitals every 4 unless on magnesium (According to the unit, ex. Q2H)❏ Breathe sounds for moistness❏ Check urine for protein❏ Fetal monitoring❏ Reflexes: Arm reflex(need baseline) Q2H, Absent , 1+, 2+, 3+, 4+ hyperreflexia❏ Question about symptoms
❏ headache, visual disturbances, edema (swelling around ring finger)

Interventions❏ Monitor constantly for??
❏ S&S seizures: hyperreflexia, twitching, epigastric pain - these s/s may happen right before seizure
❏ Lateral position (why??):❏ venous return, increase blood flow
❏ Control pain (why??)❏
❏ Pitocin and MgSO4 (how to infuse??)❏
❏ Epidural: only if there is no coagulation problem❏ EFM (Electronic Fetal Monitoring)❏ Prevent seizures
❏ reduce stimuli in the room❏ keep beeping in the room to a minimum, turn volume lower, not off
Magnesium Protocol❏ Need primary IV❏ MgSo4 is infused as a secondary infusion
❏ 4-6 gms loading dose in 100 ml over 15-20 min❏ 2 gm/hr continuous infusion
❏ Monitor for toxicity❏ BP every 2 hrs.❏ Reflexes every 2 hrs. → need at least 2+❏ UO every 2 hrs. → MgSO4 is excreted by kidneys❏ Serum levels every 4-6 hrs should be between 4-6❏ RR and O2 saturation every 2 hrs → CNS is depressed, turn MgSO4 or decrease
if RR is 12, if lower, turn it off❏ sensorium❏ Inform mother that she will feel a warm flush when medication is first
administered
Treatment for MgSo4 Toxicity
� Discontinue
� Notify Health Care Provider
� Have Calcium Gluconate available as antidote (1 gm) at 1 ml/min
Eclampsia❏ Generalized seizures❏ Breathing stops for a short time → results in fetal hypoxia❏ Temporarily in coma❏ Doesn’t remember seizure when conscious❏ May have nonreassuring fetal patterns❏ May occur during pregnancy, intrapartum or postpartum
Complications of Seizure❏ Blood volume severely reduced during seizure❏ Fluid shifts❏ Oliguria❏ Cerebral hemorrhage❏ Ruptured placenta❏ Early labor❏ HELLP Syndrome
Management of Eclampsia❏ Monitor for impending seizure: know S&S❏ Initiate preventive measures❏ Keep stimuli down❏ Padded side rails, bed low, wheels locked❏ O2 and suction❏ Intubation equipment❏ Meds
Actual Seizure❏ Remain in the room and activate emergency system❏ Attempt to place in lateral position❏ Note time and sequence of seizure❏ Insert airway after seizure and suction, Don’t open pts mouth if it’s closed you can
insert airways after seizure will end❏ Administer O2❏ Notify provider❏ Assess for complications❏ Admin MgSo4 - drug of choice
General Care for Preeclampsia and Eclampsia
� Weight
� Activity restrictions
� Reduce stimuli
� Vital signs
� Urinalysis for protein
� Fetal assessment
� Antihypertenives
� Give O2 and monitor O2 sat
� Monitor reflexes
� IV sites checked
� Monitor Pitocin and MgSo4

� Monitor for S/S of pulm edema and CHF after seizure� Lasix
� Digitalis
� Monitor for visual disturbances
� Monitor for headaches
� Monitor for gastric pain (N&V)
� Edema
� Breath sounds
� Prevent seizure related injury
� Prepare for delivery
� Emotional support
� Continue to monitor all of these postpartum period

HELLP
HELLP The pathogenesis of HELLP syndrome is not well understood. The findings of this multisystem disease are attributed to abnormal vascular tone, vasospasm and coagulation defects.To date, no common precipitating factor has been found. The syndrome seems to be the final manifestation of some insult that leads to microvascular endothelial damage and intravascular platelet activation. With platelet activation, thromboxane A and serotonin are released, causing vasospasm, platelet agglutination and aggregation, and further endothelial damage. Thus begins a cascade that is only terminated with delivery.
Incidence
❏ Very serious and life-threatening
❏ ½ of women with preeclampsia develop HELLP
❏ May occur post partum also

Manifestations� Hallmark symptom
� Pain in upper R quadrant
� Or lower R chest
� Or midepigastric
� Generalized malaise
� Abd. tenderness
� N/V
� Severe edema
� Headache
� Skin may look jaundice
Diagnostics� Liver enzymes
� Platelet count with CBC
� Decreased haptoglobin
� + D-Dimer in women with preeclampsia
Treatment� ICU
� MgSO4
� Hydralazine
� Fluid replacement
� Cervical ripening and induction if at least 34 weeks
� If stable may wait for induction if < 34 weeks

Complications� Bleeding
� include:
� Placental Abruption
� Pulmonary Edema ( fluid buildup in the lungs)
� Disseminated intravascular coagulation (DIC—blood clotting problems that result in hemorrhage)
� Adult Respiratory distress syndrome (lung failure)
� Ruptured liver hematoma
� Acute renal failure
� Intrauterine Growth restriction (IUGR)
� Infant respiratory Distress syndrome (lung failure)
� Blood transfusion
Chronic HTN� HTN preceded pregnancy or HTN before 20 weeks gestation
� Prescribe antihypertensive if diastolic consistently > 90 mmHg
� Tx
� Diet
� Prevent preeclampsia
� Meds
� Aldomet (Methydopa)
� Calcium channel
� Beta blockers
� ACE not receommendedpregnancy
� Diuretics are avoided





























