-
8/10/2019 Nyska Et Al. (1996) - Posterior Talocalcaneal
Coalition
1/3
The Foot (1996) 6, 178-180
9 1996 Pearson Professmnal Lrd
CASE REPORT
Posterior talocalcaneal coalition
M. Nyska*, C. B. Howard*, Y. Kollander+,A. Payser, S. Porat*
*Department of Orthopaedic Surgery, Hudassah Medical Centre,
Hebrew University, Jerusalem and Department
of Orthopaedic Surgery, Soroka Medical Centre, Faculty of Health
Sciences, Ben-Gurion University of the Negev,
Beer-Sheva, Israel
SUMMARY
Tarsal coalition is a rare congenital deformity. The most common
coalitions involve the
calcaneonavicular joint and the medial facet of the
talocalcaneal joint. The posterior facet is rarely involved. We
report a case of a patient with a posterior talocalcaneal bar
who presented with painful limitation of subtalar
motion without the classical appearance of spastic flat foot.
Resection of the bar with interposition of fat graft
resulted in an almost full range of pain-free subtalar
motion.
INTRODUCTION
Tarsal coalition was described f irst by Buffon in 1750.
One of the earliest examples (c. 1769) is an original
specimen of John Hunters and resides in the
Hunterian Museum of the Royal College of Surgeons
in London. Talocalcaneal coalition was first reported
by Zuckerkandel in 1877 and Curvi lhier described the
calcaneonavicular bar in 1829.1 2.3 arris4 suggested
the linkage between spastic flat foot and tarsal coali-
tion. Moisher and Asherj revised the vast number of
reports on the clin ical appearance and incidence of
tarsal coalition. The most common coalitions involve
the calcaneonavicular joint and the medial facet of
the talocalcaneal joint. Salomao6 in a series of 32 feet
with medial facet talocalcaneal bar had satisfactory
results from surgical resection and free fat graft inter-
position. The posterior facet is rarely involved.
Harris7 in 1955 presented two such patients. In 1965
he reported a retrospective study of 102 cases of
tarsal coalition, of which only four had a posterior
talocalcaneal coalition.5 We have been able to find
only a further four cases in the literature that also
formed a part of a larger series.3A case with posterior
talocalcaneal coalition is reported.
CASE REPORT
A 16-year-old woman presented with a 2-year history
of effort-induced pain in her right foot. She was a
medium-distance runner. The pain was around the
sinus tarsi and gradually became severe enough to
Correspondence to M. Nyska, MD, Department of Orthopaedic
Surgery, Hadassah University Hospital, POB 12000. Ein-Kerem,
Jerusalem 9 1120, Israel.
prevent her from running. On examination the
appearance of the foot was normal and the ankle had
a full pain-free range of motion. There was severe
painful limitation in subtalar motion. No pain was
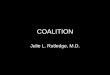
elicited in the toes during walking. Plain lateral radi-
ography demonstrated a bony mass protruding from
the posterior tuberosity of the calcaneum towards the
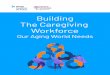
talus (Fig. 1). Coronal computerized tomography
(CT) demonstrated the area of fibrotic fusion to lie
on the posteromedial aspect of the talus (Fig. 2).
A gap between the bony mass and the talus was pre-
sent laterally. The bony mass was better visualized on
plain lateral radiographs than in the CT images.
There was increased uptake of Technetium 99m on
the posterior side of the ankle joint (Fig. 3).
The patient was treated conservatively with a
below-knee walking cast for two periods of 3 weeks
with only temporary relief of the pain and it was
therefore decided to resect the bony bridge. Through
Fig. 1-Plam lateral radiograph demonstrating the posterior
bar.
178
-
8/10/2019 Nyska Et Al. (1996) - Posterior Talocalcaneal
Coalition
2/3
Posterior talocalcaneal coalition 179
Fig. Increased uptake of the posterior side of the ankle m
Technetium 99m bone scan.
Fig. 2-A coronal CT of the talus and calcaneum showing the
posterior bar and fibrotic union to the talus.
a lateral curved incision the upper surface of the cal-
caneum was exposed and the base of the bony bridge
was resected flush with the upper border of the calca-
neum. The dissection was continued anteriorly
towards the posteromedial side of the talus and com-
plete resection of the medial tubercle of the talus was
performed. Good subtalar motion was obtained only
after resection of the tubercle and exposure of the
subtalar joint posteriorly. A free fat graft was inserted
into the defect and the wound closed. The postopera-
tive treatment consisted of posterior slab for a week,
followed by physiotherapy and non-weight-bearing
for 6 weeks. At 3 months follow-up there was sti ll
limitation of subtalar motion with mild pain on walk-
ing. After one year there was no pain on running, but
she had not returned to competitive sport. On exami-
nation there was almost full range of motion of the
subtalar joint. Radiographs taken postoperatively
showed complete resection of the bar (Fig. 4).
DISCUSSION
The clin ical appearance of this case shares some
of the typical features of other tarsal coalitions.8
Fig. LPostoperatlve lateral radiograph demonstrating
complete
resection of the posterior bar.
Children usually begin to complain from 12 to 15
years of age and pain i s exercise-related, vague and
diffuse. Our patient began to complain of pain after
long-distance running when she was 14 years old.
The exact cause of pain in tarsal coalition is
unknown but has been attributed to secondary strain
of the ankle ligaments, peroneal muscle spasm, sinus
tarsi irritation, subtalar joint irritation or degenera-
tive changes.5 Although our patient did not have the
-
8/10/2019 Nyska Et Al. (1996) - Posterior Talocalcaneal
Coalition
3/3
180 The Foot
typical peroneal spastic flat foot she did have pain in the
sinus tarsi and marked limitation in subtalar motion.
Plain lateral radiography clear ly demonstrated the
posterior bar. However, the standard images of CT
demonstrated the bar to lie more on the medial side of
the calcaneum. On the medial side the bony calcaneal
mass was intimately fused with the talus, making it
difficult to decide the exact plane of vertical resection
between these two bones. The CT showed that there
was a recess between the bony mass and the talus on
the lateral side. This was the deciding factor in choos-
ing the lateral approach. In the medial facet bar or the
calcaneonavicular bar there is a need for special radi-
ographic views - the Harris view and the lateral
oblique in 45 respectively. CT demonstrates these
bars better.4,9 However, in the present case a plain lat-
eral radiograph was sufficient to reveal the pathology.
The CT provided useful anatomical information that
aided the surgical approach.
In talocalcaneal bars the increased uptake in bone
scan is usually located in the talonavicular joint or the
posterior facet. This may be due to local inflamma-
tory reaction eventually leading to arthritic changes.
In our patient there were no arthrit ic changes (she
was only 16 years old at operation) and the increased
uptake may indicate a stress concentration area or
local synovitis.
Immobilization in a plaster cast gave only tempo-
rary relief and therefore an operative approach was
indicated. The operative alternatives for treatment are
either triple arthrodesis or resection of the bar. In cases
where there are no arthritic changes the preferred
method is resection of the bar. The space may be filled
with silicon, fascia, tendons from the area or fat graft.
Resection of the bar with a placement of fat graft
was performed, eventually leading to good results.
REFERENCES
1 .
2 .
3 .
4 .
5 .
6 .
I.
8 .
9.
ORahil ly R. A survey of carpal and tarsal anomalies. J Bone
Joint Surg 1953; 35A: 626-642.
ORahil ly R. Developmental deviat ions in the carpus and the
tarsus. Clin Orthon Rel Res 1957: 10: 9-18.
Scranton P E. Treatment of symptom atic talocalcaneal
coalit ion. J Bone Joint Surg 1987; 69A: 533-539.
Harris R I . Rigid valgus foot due to talocalcaneal bridge.
J Bone Joint Surer 1955: 37A: 169-183.
Moisher K M, her M. Tarsal coali tion and peroneal spast ic
f lat foot. A review . J Bone Joint Surg 1 984; 66A: 976984.
Salomao 0, Napoli M M M , De Ca alho A E Fernandes T D,
Maraues J . Hernandez A J. Talocalcaneal coal on: diagnosis
and surgical managem ent. Fo ot and Ankle 1992; 5: 251:256.
Harris R I . Follow-up notes on art ic les previously
published
in the journal. J Bone Joint S urg 1965; 47A: 1657-1667.
Nysk a M, Deke l S. Tarsal coalit ion: a review. Hareffuah
1989;
117: 454457.
Deutch A L, Resnick D, Campbell G. Compu ted tomography
and bone scintigraphy in the evaluation of tarsal coalition.
Radio1 1982; 144: 137.