Embed Size (px)
Citation preview

NWP 4-02
1 JAN 2008
NAVY WARFARE PUBLICATION
NAVAL EXPEDITIONARY HEALTH SERVICE SUPPORT
AFLOAT AND ASHORE NWP 4-02
EDITION JANUARY 2008
DEPARTMENT OF THE NAVY OFFICE OF THE CHIEF OF NAVAL OPERATIONS
DISTRIBUTION RESTRICTION: APPROVED FOR PUBLIC RELEASE; DISTRIBUTION IS UNLIMITED. PRIMARY REVIEW AUTHORITY: CHIEF, BUREAU OF MEDICINE AND SURGERY
URGENT CHANGE/ERRATUM RECORD
NUMBER DATE ENTERED BY
0411LP1062147

NWP 4-02
JAN 2008 2
INTENTIONALLY BLANK


NWP 4-02
JAN 2008 4
INTENTIONALLY BLANK

NWP 4-02
DEPARTMENT OF THE NAVY BUREAU OF MEDICINE AND SURGERY
2300 E STREET NW WASHINGTON, DC 20372-5300
April 2008
LETTER OF APPROVAL
1. NWP 4-02 (2008), NAVAL EXPEDITIONARY HEALTH SERVICE SUPPORT AFLOAT AND ASHORE, is UNCLASSIFIED. Handle in accordance with the administrative procedures contained in NTTP 1-01.
2. NWP 4-02 (2008) is effective upon receipt and supersedes NWP 4-02, NAVAL EXPEDITIONARY HEALTH SERVICE SUPPORT AFLOAT AND ASHORE, dated April 2005 and NWP 4-02.3 (PART B), PLANNING, OPERATIONS, AND MEDICAL INTELLIGENCE, dated August 1995. Destroy superseded material without report.
3. NWP 4-02 (2008) addresses naval expeditionary health service support (HSS) capabilities available to the operational commander, the organization of Navy Medicine to support expeditionary HSS for forces afloat and ashore, the roles and responsibilities of supporting and supported commanders, and the capabilities and limitations of naval expeditionary HSS in an operational environment.
4. NWP 4-02 (2008) is approved for public release; distribution is unlimited.
Approved A.M. ROBINSON, JR.
5 JAN 2008

NWP 4-02
JAN 2008 6
INTENTIONALLY BLANK

NWP 4-02
7 JAN 2008
January 2008
PUBLICATION NOTICE ROUTING
1. NWP 4-02 (JAN 2008), NAVAL EXPEDITIONARY HEALTH SERVICE SUPPORT AFLOAT AND ASHORE, is available in the Navy Warfare Library. It is effective upon receipt.
2. Summary.
a. NWP 4-02 provides operational-level doctrine that covers mission areas, enabling functions, and the organization and support of naval expeditionary health service support.
b. This publication has been updated with current information throughout.
c. The intended audience includes operational commanders, supporting commanders, planners, logisticians, and health service support personnel. It incorporates lessons learned and includes guidance from current doctrine, tactics, techniques, and procedures.
Note to Navy Warfare Library Custodian
This notice should be duplicated for routing to cognizant personnel to keep them informed of changes to this publication.
Navy Warfare Library publications must be made readily available to all users and other interested personnel within the U.S. Navy.
Navy Warfare Library Custodian

NWP 4-02
JAN 2008 8
INTENTIONALLY BLANK

NWP 4-02
9 JAN 2008
CONTENTS
Page No.
CHAPTER 1 — NAVAL EXPEDITIONARY HEALTH SERVICE SUPPORT
1.1 HEALTH SERVICE SUPPORT MISSION................................................................................. 1-1
1.2 DOCTRINE DEVELOPMENT PROCESS ................................................................................. 1-1
1.3 NAVY MEDICINE EXPEDITIONARY HEALTH SERVICE SUPPORT CAPABILITIES ........................................................................................................................... 1-2
1.3.1 Taxonomy of Care ........................................................................................................................ 1-2 1.3.2 Navy Health Service Support Capabilities ................................................................................... 1-3
1.4 RANGE OF MILITARY OPERATIONS .................................................................................... 1-4 1.4.1 Military Engagement, Security Cooperation, and Deterrence ...................................................... 1-5 1.4.2 Crisis Response and Limited Contingency Operations ................................................................ 1-5 1.4.3 Major Operations and Campaigns ................................................................................................ 1-5
1.5 CAPABILITY DEVELOPMENT SYSTEM ............................................................................... 1-5 1.5.1 Capability Analysis Process ......................................................................................................... 1-6 1.5.2 Health Service Support Requirements Determination.................................................................. 1-7
1.6 RESOURCES ............................................................................................................................. 1-10 1.6.1 Planning, Programming, and Budgeting System........................................................................ 1-10 1.6.2 Transition Health Service Support Resourcing .......................................................................... 1-10
1.7 HEALTH SERVICES IN AN OPERATIONAL ENVIRONMENT ......................................... 1-11 1.7.1 Concepts of Care......................................................................................................................... 1-11 1.7.2 Quality of Care ........................................................................................................................... 1-11
1.8 DEPLOYABLE HEALTH SERVICE SUPPORT ..................................................................... 1-13 1.8.1 Hospital Ships............................................................................................................................. 1-13 1.8.2 Expeditionary Health Service Support Medical Facilities.......................................................... 1-13 1.8.3 Casualty Receiving and Treatment Ships ................................................................................... 1-14 1.8.4 Aircraft Carriers.......................................................................................................................... 1-14 1.8.5 Forward Deployable Preventive Medicine Unit ......................................................................... 1-14 1.8.6 Fleet Surgical Teams .................................................................................................................. 1-15 1.8.7 Special Psychiatric Rapid Intervention Team............................................................................. 1-15 1.8.8 Humanitarian Support Team....................................................................................................... 1-15 1.8.9 Seabased Medical Capabilities ................................................................................................... 1-15 1.8.10 Marine Corps Deployable Medical Systems .............................................................................. 1-15
1.9 LESSONS LEARNED ............................................................................................................... 1-18

NWP 4-02
JAN 2008 10
Page No.
CHAPTER 2 — NAVAL EXPEDITIONARY HEALTH SERVICE SUPPORT ORGANIZATION, COMMAND AND CONTROL, ROLES, AND RESPONSIBILITIES
2.1 INTRODUCTION ........................................................................................................................ 2-1
2.2 STRATEGIC ORGANIZATIONAL RELATIONSHIPS............................................................ 2-1 2.2.1 Health Service Support Planner Requirements............................................................................. 2-1 2.2.2 The National Command Authority ............................................................................................... 2-1 2.2.3 Establishment and Assignment of the Combatant Command....................................................... 2-1 2.2.4 Geographic and Nongeographic Areas of Responsibility............................................................. 2-3 2.2.5 The Services — Military Departments ......................................................................................... 2-3 2.2.6 Combatant Command Authority................................................................................................... 2-4 2.2.7 Subunified Commands.................................................................................................................. 2-4 2.2.8 Service Component Command ..................................................................................................... 2-4 2.2.9 Functional Component Command ................................................................................................ 2-4 2.2.10 Joint Task Force............................................................................................................................ 2-4
2.3 COMMAND AUTHORITY......................................................................................................... 2-5 2.3.1 Combatant Command ................................................................................................................... 2-5 2.3.2 Operational Control ...................................................................................................................... 2-5 2.3.3 Tactical Control ............................................................................................................................ 2-5 2.3.4 Support Authority ......................................................................................................................... 2-5 2.3.5 Administrative Control ................................................................................................................. 2-5 2.3.6 Coordinating Authority................................................................................................................. 2-6 2.3.7 Direct Liaison Authorized ............................................................................................................ 2-6
2.4 COMMAND AND CONTROL OF DEPLOYABLE MEDICAL SYSTEMS ............................ 2-6
2.5 HEALTH SERVICE SUPPORT CONSIDERATIONS AT THE STRATEGIC, OPERATIONAL, AND TACTICAL LEVELS ........................................................................... 2-6
2.5.1 Health Service Support Unit Relationship with Host Command.................................................. 2-7 2.5.2 Deployment Order Chain of Command........................................................................................ 2-7 2.5.3 Operational and Administrative Control....................................................................................... 2-8
2.6 COMMAND RELATIONSHIPS AND RESPONSIBILITIES.................................................. 2-10 2.6.1 Joint, Coalition, and Allied Operations ...................................................................................... 2-10 2.6.2 Unified Command Surgeon ........................................................................................................ 2-12 2.6.3 Joint Task Force Surgeon ........................................................................................................... 2-12 2.6.4 Component Elements.................................................................................................................. 2-14 2.6.5 Health Service Support Staff Officers ........................................................................................ 2-14 2.6.6 Task Force Surgeon .................................................................................................................... 2-14 2.6.7 Expeditionary Strike Group Surgeon.......................................................................................... 2-14 2.6.8 Landing Force Surgeon............................................................................................................... 2-14 2.6.9 Expeditionary Health Service Support Unit Commanders ......................................................... 2-15
2.7 NAVAL MEDICAL ORGANIZATIONAL RELATIONSHIPS AND RESPONSIBILITIES ................................................................................................................. 2-15
2.7.1 Office of the Chief of Naval Operations..................................................................................... 2-15 2.7.2 Bureau of Medicine and Surgery ................................................................................................ 2-20 2.7.3 Navy Medicine Regions ............................................................................................................ 2-20 2.7.4 Navy Medicine Support Command ............................................................................................ 2-21 2.7.5 Navy Medicine East/Navy Medicine West................................................................................. 2-23

NWP 4-02
11 JAN 2008
Page No.
2.8 MILITARY SEALIFT COMMAND.......................................................................................... 2-23
CHAPTER 3 — NAVAL EXPEDITIONARY HEALTH SERVICE SUPPORT PLANNING ACTIONS AND RESPONSIBILITIES
3.1 INTRODUCTION ........................................................................................................................ 3-1
3.2 PREDEPLOYMENT TOOLS AND CONSIDERATIONS......................................................... 3-1 3.2.1 Joint Operation Planning and Execution System.......................................................................... 3-1 3.2.2 Time-Phased Force and Deployment Data ................................................................................... 3-1 3.2.3 Annex Q, Planning Guidance, and Health Service Support Considerations ................................ 3-2
3.3 DEPLOYMENT CYCLE ............................................................................................................. 3-3 3.3.1 Predeployment/Deployment Planning .......................................................................................... 3-3 3.3.2 Activation ..................................................................................................................................... 3-7 3.3.3 Deployment/Operations................................................................................................................ 3-9 3.3.4 Redeployment ............................................................................................................................. 3-13
3.4 MEDICAL INTELLIGENCE..................................................................................................... 3-14 3.4.1 Medical Intelligence Defined ..................................................................................................... 3-14 3.4.2 Significance of Medical Intelligence .......................................................................................... 3-14 3.4.3 Intelligence Cycle ....................................................................................................................... 3-14 3.4.4 Intelligence Sources.................................................................................................................... 3-15 3.4.5 Other Sources of Medical Intelligence ....................................................................................... 3-16 3.4.6 Medical Threat............................................................................................................................ 3-17
3.5 THE COMMANDER’S ESTIMATE......................................................................................... 3-19 3.5.1 Development of the Commander’s Estimate .............................................................................. 3-19 3.5.2 Staff Estimates in the Estimate Development Process ............................................................... 3-19 3.5.3 Health Service Support Estimate ................................................................................................ 3-20
CHAPTER 4 — NAVAL EXPEDITIONARY HEALTH SERVICE SUPPORT CONSIDERATIONS
4.1 INTRODUCTION ........................................................................................................................ 4-1
4.2 HEALTH CARE IN AN AUSTERE WARTIME ENVIRONMENT.......................................... 4-1 4.2.1 Clinical Services ........................................................................................................................... 4-1 4.2.2 Nursing Services........................................................................................................................... 4-5 4.2.3 Combat Stress ............................................................................................................................... 4-5 4.2.4 Trauma Care ................................................................................................................................. 4-5 4.2.5 Naval Specialty Medicine............................................................................................................. 4-6 4.2.6 Other Requirements for Operational Medical Support................................................................. 4-8 4.2.7 Decedent Affairs........................................................................................................................... 4-8
4.3 COMMUNICATIONS ................................................................................................................. 4-9 4.3.1 Planning Considerations ............................................................................................................... 4-9 4.3.2 Medical Regulating Network...................................................................................................... 4-10 4.3.3 Other Wartime or Contingency Communications Capabilities .................................................. 4-10 4.3.4 Patient Evacuation ...................................................................................................................... 4-11 4.3.5 Communications Issues .............................................................................................................. 4-11
4.4 HOMELAND SECURITY......................................................................................................... 4-12

NWP 4-02
JAN 2008 12
Page No.
4.4.1 Humanitarian and Civic Assistance............................................................................................ 4-12 4.4.2 Health Service Support ............................................................................................................... 4-12
4.5 PATIENT MOVEMENT............................................................................................................ 4-13 4.5.1 Patient Regulating....................................................................................................................... 4-13 4.5.2 Patient Evacuation ...................................................................................................................... 4-13 4.5.3 Patient Movement Considerations for Special Operations Forces ............................................. 4-16 4.5.4 Patient Movement Items ............................................................................................................. 4-16 4.5.5 Health Care in Remote Locations............................................................................................... 4-16
4.6 CHEMICAL, BIOLOGICAL, RADIOLOGICAL, AND NUCLEAR DEFENSE OPERATIONS ........................................................................................................................... 4-16
4.6.1 Chemical, Biological, Radiological, and Nuclear Defense......................................................... 4-17 4.6.2 Chemical, Biological, Radiological, and Nuclear Defense Training.......................................... 4-19 4.6.3 Patient Decontamination............................................................................................................. 4-19
4.7 SECURITY/FORCE PROTECTION ......................................................................................... 4-20 4.7.1 External Security ........................................................................................................................ 4-20 4.7.2 Internal Security.......................................................................................................................... 4-20 4.7.3 Security Training ........................................................................................................................ 4-21 4.7.4 Visitor and Patient Security ........................................................................................................ 4-21
4.8 DETAINEES .............................................................................................................................. 4-21 4.8.1 Detainee Considerations ............................................................................................................. 4-21 4.8.2 Refugee Considerations .............................................................................................................. 4-22 4.8.3 Captured Enemy Materiel Considerations.................................................................................. 4-22
4.9 GENEVA CONVENTIONS ...................................................................................................... 4-22 4.9.1 Identification............................................................................................................................... 4-23 4.9.2 Hospital Ships............................................................................................................................. 4-23 4.9.3 Enemy Prisoners of War............................................................................................................. 4-23
APPENDIX A — NAVY HEALTH SERVICE SUPPORT ORGANIZATION
A.1 MISSION AND FUNCTIONS.................................................................................................... A-1 A.1.1 Activities Following OPNAVINST 5430.48 (series), OPNAV Organization Manual................ A-1 A.1.2 Activities Following BUMEDINST 5430.8, Bureau of Medicine and Surgery Organization
Manual......................................................................................................................................... A-1
APPENDIX B — MULTINATIONAL AGREEMENTS
B.1 NATO DIRECTIVES.................................................................................................................. B-1
B.2 NATO STANDARDIZATION AGREEMENTS ....................................................................... B-1
APPENDIX C — REPORTS
C.1 STATUS OF RESOURCES AND TRAINING SYSTEM ......................................................... C-1
C.2 REQUIRED MEDICAL REPORTS ........................................................................................... C-1 C.2.1 Unit Situation Report ................................................................................................................... C-2 C.2.2 Disease Surveillance Report ........................................................................................................ C-3

NWP 4-02
13 JAN 2008
Page No.
APPENDIX D — MEDICAL PLATFORM CHARACTERISTICS
APPENDIX E — BLOOD SUPPLY CAPABILITIES/PLANNING FACTORS
E.1 UNITS OF MEASURE ................................................................................................................E-1
E.2 CURRENT PLANNING FACTORS ...........................................................................................E-1 E.2.1 Pallet with Blood Products Shipping Data ...................................................................................E-2 E.2.2 Miscellaneous Blood Planning Factors.........................................................................................E-2
E.3 SHIPBOARD BLOOD PRODUCTS CAPABILITIES — OPNAVINST 6530.4 (SERIES)...................................................................................................E-3
E.4 BLOOD PRODUCTS (CLASS VIIIB) AVAILABLE TO THE THEATER ..............................E-3
E.5 BLOOD BANK PRODUCTS AND PROCEDURES BY CAPABILITY OF CARE.................E-4
APPENDIX F — RESPONSIBILITIES OF THE JOINT TASK FORCE SURGEON
F.1 JOINT TASK FORCE SURGEON ..............................................................................................F-1
F.2 EXPEDITIONARY STRIKE GROUP SURGEON.....................................................................F-1
F.3 LANDING FORCE SURGEON ..................................................................................................F-2
APPENDIX G — USEFUL WEBSITES
APPENDIX H — LESSONS LEARNED
H.1 GENERAL................................................................................................................................... H-1
H.2 AFTER ACTION REPORT ........................................................................................................ H-1
H.3 LESSONS LEARNED ................................................................................................................ H-1
REFERENCES
GLOSSARY
LIST OF ACRONYMS AND ABBREVIATIONS

NWP 4-02
JAN 2008 14
LIST OF ILLUSTRATIONS
Page No.
CHAPTER 1 — NAVAL EXPEDITIONARY HEALTH SERVICE SUPPORT
Figure 1-1. Taxonomy of Care Capabilities ............................................................................................... 1-2 Figure 1-2. Range of Military Operations .................................................................................................. 1-4 Figure 1-3. Resource Allocation Responsibilities for Programming and Budgeting ............................... 1-11 Figure 1-4. Shipboard Health Service Support Capabilities by Ship Class.............................................. 1-16
CHAPTER 2 — NAVAL EXPEDITIONARY HEALTH SERVICE SUPPORT ORGANIZATION, COMMAND AND CONTROL, ROLES, AND RESPONSIBILITIES
Figure 2-1. National Command Authority Chain of Command and Control ............................................. 2-2 Figure 2-2. Predeployment and Deployment of Health Service Support Units.......................................... 2-9 Figure 2-3. Health Service Support Command Relationships.................................................................. 2-10 Figure 2-4. Notional Joint Task Force Surgeon’s Office Organization.................................................... 2-13
CHAPTER 4 — NAVAL EXPEDITIONARY HEALTH SERVICE SUPPORT CONSIDERATIONS
Figure 4-1. Joint CBRN Defense Functional Concept — Operational Attributes.................................... 4-17
APPENDIX A — NAVY HEALTH SERVICE SUPPORT ORGANIZATION
Figure A-1. Chief, Bureau of Medicine and Surgery Organization and Shore Activities.......................... A-2
APPENDIX B — MULTINATIONAL AGREEMENTS
Figure B-1. NATO Standardization Agreement Publication List .............................................................. B-1
APPENDIX C — REPORTS
Figure C-1. Medical Reports, Reporting, and Periodicity Requirements .................................................. C-2 Figure C-2. Weekly DNBI Report ............................................................................................................. C-5
APPENDIX D — MEDICAL PLATFORM CHARACTERISTICS
Figure D-1. Medical Platform Characteristics............................................................................................ D-1 Figure D-2. Notional Shipboard Health Service Support Department Manning........................................ D-7
APPENDIX E — BLOOD SUPPLY CAPABILITIES/PLANNING FACTORS
Figure E-1. Units of Measure......................................................................................................................E-1 Figure E-2. Units per Hospital Casualty .....................................................................................................E-1 Figure E-3. Units per Hospital Casualty by Category ................................................................................E-1 Figure E-4. Pallet with Blood Products ......................................................................................................E-2 Figure E-5. Miscellaneous Blood Planning Factors....................................................................................E-2 Figure E-6. Shipboard Blood Products Capabilities ...................................................................................E-3

NWP 4-02
15 JAN 2008
Page No.
Figure E-7. Blood Products (Class VIIIB) Available to the Theater ..........................................................E-3 Figure E-8. Blood Bank Products and Procedures by Capability of Care ..................................................E-4
APPENDIX G — USEFUL WEBSITES
Figure G-1. Useful Websites ...................................................................................................................... G-1

NWP 4-02
JAN 2008 16
INTENTIONALLY BLANK

NWP 4-02
17 JAN 2008
PREFACE
NWP 4-02 (JAN 2008) is a reference for operational commanders, planners, and health service support (HSS) personnel. It incorporates lessons learned from recent operations and relevant existing doctrine from a broad range of related documents.
Report administrative discrepancies by letter, message, or e-mail to:
COMMANDER NAVY WARFARE DEVELOPMENT COMMAND ATTN: N5 686 CUSHING ROAD NEWPORT RI 02841-1207 [email protected]
ORDERING DATA
Order printed copies of a publication using the Print on Demand (POD) system. A command may requisition a publication using standard military standard requisitioning and issue procedure (MILSTRIP) procedures or the Naval Supply Systems Command website called the Naval Logistics Library (https://nll1.ahf.nmci.navy.mil). An approved requisition is forwarded to the specific DAPS site at which the publication’s electronic file is officially stored. Currently, two copies are printed at no cost to the requester.
CHANGE RECOMMENDATIONS
Procedures for recommending changes are provided below.
WEB-BASED CHANGE RECOMMENDATIONS
Recommended changes to this publication may be submitted to the Navy Warfare Development Doctrine Discussion Group, accessible through the Navy Warfare Development Command website at: http://www.nwdc.navy.smil.mil/.
URGENT CHANGE RECOMMENDATIONS
When items for changes are considered urgent send this information by message to the Primary Review Authority, info NWDC. Clearly identify and justify both the proposed change and its urgency. Information addressees should comment as appropriate. See accompanying sample for urgent change recommendation format on page 19.
ROUTINE CHANGE RECOMMENDATIONS
Submit routine recommended changes to this publication at any time by using the accompanying routine change recommendation letter format on page 20 and mailing it to the address below, or posting the recommendation on the NWDC Doctrine Discussion Group site.

NWP 4-02
JAN 2008 18
COMMANDER NAVY WARFARE DEVELOPMENT COMMAND DOCTRINE DIRECTOR (N5) 686 CUSHING ROAD NEWPORT RI 02841-1207
CHANGE BARS
Revised text is indicated by a black vertical line in the outside margin of the page, like the one printed next to this paragraph. The change bar indicates added or restated information. A change bar in the margin adjacent to the chapter number and title indicates a new or completely revised chapter.
WARNINGS, CAUTIONS, AND NOTES
The following definitions apply to warnings, cautions, and notes used in this manual:
An operating procedure, practice, or condition that may result in injury or death if not carefully observed or followed.
An operating procedure, practice, or condition that may result in damage to equipment if not carefully observed or followed.
Note
An operating procedure, practice, or condition that requires emphasis.
WORDING
Word usage and intended meaning throughout this publication is as follows:
“Shall” indicates the application of a procedure is mandatory.
“Should” indicates the application of a procedure is recommended.
“May” and “need not” indicate the application of a procedure is optional.
“Will” indicates future time. It never indicates any degree of requirement for application of a procedure.

NWP 4-02
19 JAN 2008
Urgent Change Recommendation Message Format
FM ORIGINATOR TO (Primary Review Authority)//JJJ// INFO COMNAVWARDEVCOM NEWPORT RI//N5// COMUSFLTFORCOM NORFOLK VA//JJJ// COMUSPACFLT PEARL HARBOR HI//JJJ// (Additional Commands as Appropriate)//JJJ// BT CLASSIFICATION//N03510// MSGID/GENADMIN/(Organization ID)// SUBJ/URGENT CHANGE RECOMMENDATION FOR (Publication Short Title)// REF/A/DOC/NTTP 1-01// POC/(Command Representative)// RMKS/ 1. IAW REF A URGENT CHANGE IS RECOMMENDED FOR (Publication Short Title) 2. PAGE ______ ART/PARA NO ______ LINE NO ______ FIG NO ______ 3. PROPOSED NEW TEXT (Include classification) 4. JUSTIFICATION. BT
Message provided for subject matter; ensure that actual message conforms to MTF requirements.

NWP 4-02
JAN 2008 20
Routine Change Recommendation Letter Format

NWP 4-02
1-1 JAN 2008
CHAPTER 1
Naval Expeditionary Health Service Support
1.1 HEALTH SERVICE SUPPORT MISSION
The Secretary of Defense (SecDef) defines the mission of military health services as providing and maintaining readiness and medical services and support to members of the armed forces during military operations, to their dependents, and to others entitled to Department of Defense (DOD) medical care. Naval expeditionary health service support (NEHSS) is capable of deploying naval personnel to promote physical and mental health readiness and to care for the sick and injured in military operations. According to Joint Publication (JP) 1-02, Department of Defense Dictionary of Military and Associated Terms, health service support (HSS) includes:
1. The management of health services resources such as manpower, monies, and facilities
2. Preventive and curative health measures
3. Evacuation of the wounded, injured, and sick
4. Selection of the medically fit and disposition of the medically unfit
5. Blood management
6. HSS supply, equipment, and maintenance
7. Combat and operational stress control
8. Medical, dental, veterinary, laboratory, optometric, medical food, and medical intelligence services. (Note: Veterinary services are provided by the United States Army (USA).)
This publication describes NEHSS and its capabilities, organizational relationships, deployed naval HSS unit command and control (C2), and planning, and considerations for their employment. It reinforces the concepts outlined in Joint Vision 2020, Sea Power 21, Marine Corps Strategy 21, and Naval Force Health Protection for the 21st Century (NFHP-21) and provides doctrinal support to the fleet operational health (FOH) concept of operations (CONOPS).
1.2 DOCTRINE DEVELOPMENT PROCESS
Navy Tactics, Techniques, and Procedures (NTTP) 1-01, The Navy Warfare Library, provides guidance on doctrine development and revision processes. The Navy Warfare Development Command (NWDC) Health Service Support Division (HSSD), Code N-55, manages the Navy HSS doctrinal review process, serves as the point of contact (POC) for doctrine management, and ensures that doctrine related to Navy Medicine, such as the medical sections of joint, allied, Navy, and North Atlantic Treaty Organization (NATO) standard agreement (STANAG) publications, is staffed within Navy Medicine. Specifically, the HSSD is the technical coordinating office (TCO) within doctrine development.
The technical reviewing office and overall HSS doctrine manager is the Bureau of Medicine and Surgery (BUMED), which solicits input regarding doctrinal revisions and new medical proposals from the United States Fleet Forces Command (USFLTFORCOM or USFFC) Budget Submitting Office (BSO)-60/70, Navy Medicine

NWP 4-02
JAN 2008 1-2
BSO-18, and Marine Corps BSO-27. The Office of the Chief of Naval Operations (OPNAV) N931 and USFFC act as the primary reviewing authority of doctrine at the tactical and operational levels. Upon receipt of doctrine development tasking, the HSSD coordinates doctrine development and review with BUMED and provides informational awareness to OPNAV N931 and USFFC. The HSSD formats and forwards doctrine to BUMED working groups, which review changes and adjudicate comments, deconflict issues, and provide visibility and feedback to the Navy Surgeon General (SG). BUMED provides proposed changes to the Navy SG before the signature and promulgation of doctrine take place.
1.3 NAVY MEDICINE EXPEDITIONARY HEALTH SERVICE SUPPORT CAPABILITIES
1.3.1 Taxonomy of Care
As discussed in JP 4-0, Doctrine for Logistics Support of Joint Operations, DOD developed the taxonomy of health care capabilities for HSS expeditionary forces through a continuum of care that supports patient movement in combat. The continuum extends from the point of injury, wounding, or onset of illness and progresses to more sophisticated and capable elements in the sustainment area. A facility in the continuum of care is defined in terms of care capabilities and by categories of patients it can receive. Lower capabilities of care are more mobile, with a limited capability for extensive medical care. Higher capabilities of care have a greater capability to provide medical care but are less mobile. Patients may access HSS at any point along the continuum of care. The five capabilities in the taxonomy of care are first responder, forward resuscitative care (FRC), theater hospitalization, definitive care, and en route care. (See Figure 1-1 for a taxonomy of care capabilities.)
Note: The Navy tactical task list (NTTL) does not reflect the recent change from levels of care to taxonomy of care.
CAPABILITY HEALTH CARE EXAMPLE* First Responder Medical care rendered at the point of
initial injury or illness Self Aid/Buddy Aid Hospital Corpsman Marine Corps Lifesavers
Forward Resuscitative Care
Forward advanced emergency medical treatment performed close to the point of injury/illness
Ship’s Medical Department Battalion/Wing Aid Station Shock Trauma Platoon Forward Resuscitative Surgery System Expeditionary Medical Facility Surgical Company Casualty Receiving and Treatment Ship Aircraft Carrier
Theater Hospitalization
Modular theater hospitals with medical and surgical capabilities required to support the theater
Hospital Ships Expeditionary Medical Facility
Definitive Care Full range of acute, convalescent, restorative, and rehabilitative care
OCONUS Medical Treatment Facility CONUS Medical Treatment Facility Veterans Administration National Disaster Medical System Hospital
En Route Care Medical treatment during movement between capabilities
Tactical En Route Care Teams**
* This is not an all-inclusive list of medical resources. ** En route care is used throughout all capabilities of care.
Figure 1-1. Taxonomy of Care Capabilities

NWP 4-02
1-3 JAN 2008
1.3.1.1 First Responder Capability
First responder capability is the initial stabilizing medical care rendered to ill or injured casualties at the point of initial injury or illness. First responder care can be provided throughout the continuum, to include FRC capability and theater hospitalization capability.
1.3.1.2 Forward Resuscitative Care Capability
FRC capability is forward advanced emergency medical treatment performed at the closest possible point of injury, based on current operational requirements. The goal of FRC is to achieve the most efficient use of life-and-limb-saving advanced emergency medical treatment that can attain stabilization.
1.3.1.3 Theater Hospitalization Capability
Theater hospitalization capability, which includes theater hospitals with modular configurations, is used to provide theater support. All care and HSS capabilities are required to provide support in theater, which includes emergency medical services, surgical services, primary care, veterinary services, dental services, preventive medicine, combat and operational stress control, blood bank services, hospitalization, laboratory and pharmacy services, radiology, and medical logistics. The theater hospitalization capability offers essential care to either return the patient to duty (within the theater evacuation policy) and/or stabilize to ensure the patient can tolerate evacuation to a definitive care facility outside the theater.
1.3.1.4 Definitive Care Capability
Definitive care capability includes care rendered to conclusively manage a patient’s condition, which leads to rehabilitation, return to duty, or discharge from the service. Definitive care capability includes the full range of acute, convalescent, restorative, and rehabilitative care sites outside the theater of operations.
1.3.1.5 En Route Care Capability
En route care capability is available for the medical treatment of injured and ill Service members during movement between one capability of care to another in the continuum of care capabilities.
Note
NATO retains levels of care, as its schema of the provision of health services, which correspond to the US taxonomy of care through levels 1 to 4, according to Allied Joint Publication (AJP) 4-10, Allied Joint Medical Support Doctrine. In coalition and multinational operations, personnel from non-NATO countries may have different interpretations of levels of care. In such circumstances, evacuation of casualties through progressive levels of care may not occur and patients may arrive at an expeditionary medical facility (EMF) without receiving first responder or FRC capability.
1.3.2 Navy Health Service Support Capabilities
NEHSS capabilities provide options across the range of military operations (ROMO). At the front line are corpsmen providing first responder capability to combat casualties. FRC capability is provided by general medical officers at battalion aid stations (BASs), by emergency medicine physicians at shock trauma platoons (STPs), or by nurses and physician assistants at far-forward HSS facilities. FRC capability is also provided by medical battalions and casualty receiving and treatment ships (CRTSs), where medical and surgical resuscitation and stabilization are focused. Casualties requiring hospitalization are evacuated to the theater hospitalization capability of care, which is provided by a hospital ship or an EMF. Definitive care capability is provided at a continental United States (CONUS) medical treatment facility (MTF), or, when an outside the continental United States (OCONUS) MTF is required, equipped with acute, convalescent, restorative, and rehabilitative care.

NWP 4-02
JAN 2008 1-4
Definitive care is the highest capability of care provided at facilities outside DOD, such as a Department of Veterans Affairs (DVA) hospital or a National Disaster Medical System (NDMS) hospital. Stabilized patients are evacuated from one capability of care to another, which includes available en route care capability to prevent the degradation of the patient’s clinical condition.
1.4 RANGE OF MILITARY OPERATIONS
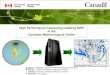
The United States employs its military capabilities at home and abroad in support of its national security goals in operations that vary in size, purpose, and combat intensity. The ROMO extends from military engagements, security cooperation, and deterrence, to crisis response, limited contingency operations, major operations, and major campaigns. In today’s security environment, the US military is often engaged in operations below the threshold of armed conflict in order to maintain US global influence and to achieve strategic goals.
Adapting to space, time, and force is critical to addressing ROMO. Unique Navy capabilities within the sea base, such as C2, heavy lift, reconnaissance, and access to sea lines of communication, provide a bridge in the operational environment. Naval forces cover the gap by establishing a sea base close to most areas of operations (AOs). They are able to arrive with critical mass quickly, commence and sustain operations, and do not rely on shore infrastructure. Naval forces reduce force protection concerns by minimizing their presence ashore. (See Figure 1-2 for the range and types of military operations that may require HSS capability.)
For further information on the range of military operations, refer to JP 3-0, Joint Operations.
Figure 1-2. Range of Military Operations
RANGE OF MILITARY OPERATIONS
TYPES OF MILITARY OPERATIONS
Military Engagement, SecurityCooperation, and Deterrence
Crisis Response andLimited Contingency Operations
Major OperationsHomeland DefenseCivil SupportStrikesRaidsShow of ForceEnforcement of SanctionsProtection of ShippingFreedom of NavigationPeace Operations
Support to InsurgencyCounterinsurgency OperationsCombating TerrorismNoncombatant Evacuation OperationsRecovery OperationsConsequence ManagementForeign Humanitarian AssistanceNation AssistanceArms Control and DisarmamentRoutine, Recurring Military Activities
Major Operations andCampaigns

NWP 4-02
1-5 JAN 2008
1.4.1 Military Engagement, Security Cooperation, and Deterrence
Military engagement, security cooperation, and deterrence are ongoing and specialized activities that shape, maintain, and refine relations with other nations. The general strategic and operational objective is to protect US interests at home and abroad. The United States Naval Ship (USNS) MERCY and USNS COMFORT humanitarian missions are examples of Navy Medicine participating in activities that build positive relations with other nations. OCONUS MTFs also work with each host nation (HN) to establish mutual aid agreements that provide common ground for HSS interaction and collaboration. In addition, forward operating HSS departments and units act in concert with their unit or supported command to provide cooperative security and deterrence.
1.4.2 Crisis Response and Limited Contingency Operations
A crisis response and limited contingency operation can be a single small-scale, limited-duration operation or a significant part of an extended major operation involving combat. The strategic and operational objectives of crisis response and limited contingency operations involve conventional and unconventional military forces used in cooperation with other government agencies, international government agencies, and nongovernmental organizations. The objectives protect US interests and prevent surprise attack and further conflict.
A crisis or emergency may prompt the conduct of humanitarian and civic assistance (HCA), civil support (CS), noncombatant evacuation operations (NEOs), peace operations, strikes, raids, and recovery operations. For domestic responses, Navy Medicine participates through the NDMS Federal Coordinating Centers (FCCs), several of which are Navy MTFs. Smaller facilities have mutual aid agreements with local and state health systems routinely training for catastrophic events. Recently, emphasis on planning has shifted to preparedness in the war on terror, tsunami and hurricane relief, and support operations, which highlight the taxonomy of care capabilities, with combat service support (CSS) functions playing a more prominent role in reaching the transitional phase of an operation.
1.4.3 Major Operations and Campaigns
The goals of major operations and campaigns are to achieve national strategic objectives and to protect national interests. The US national leadership may decide to conduct a major operation or campaign involving large-scale combat, which would place the United States in a wartime state. In such cases, the goals are to prevail against the enemy quickly and with as few casualties as possible, to conclude hostilities, and to establish conditions favorable to the HN and to the United States and its multinational partners. Stability operations are often established to restore security, provide services and humanitarian relief, and conduct emergency reconstruction. Major operations and campaigns comprise multiple phases that include mobilization, deployment, and shaping decisive operations and transitions. The length of a phase varies with different required medical capability.
1.5 CAPABILITY DEVELOPMENT SYSTEM
Navy Medicine fields its capabilities in response to its core mission as a component of joint forces. The capability development system is driven by top-down capability analysis, such as a needs identification process, and is supported by a bottom-up requirements determination process. The two processes meet to support ROMO and to field the right capability to accomplish assigned missions under varying conditions. The capability development system uses a common set of definitions, such as:
1. Capability. The ability to achieve a desired effect under specified standards and conditions through a combination of means and ways to perform a set of tasks. Capabilities contain key attributes with appropriate parameters, metrics, obstacles, and supportability.
2. Military requirement. An established need justifying the timely allocation of resources to achieve a capability to accomplish approved military objectives, missions, or tasks.

NWP 4-02
JAN 2008 1-6
3. Tasks. Actions or processes performed as part of an operation and derived from an analysis of the mission and CONOPS. The Universal Joint Task List (UJTL) describes in broad terms the requirements of the Armed Forces of the United States and can be applied to all levels of operations.
1.5.1 Capability Analysis Process
Navy Medicine defines required capabilities through direction found in Navy strategic guidance and a methodical analysis of current CONOPS and is aligned with the Joint Capabilities Integration and Development System (JCIDS). The capability analysis process is conducted through a methodical approach that assesses current NEHSS capabilities, gaps in capability and associated risks as they relate to future operations. Capabilities are expanded or developed, tested, and procured to leverage the Service’s unique capabilities and to integrate with the joint forces HSS capabilities. The process to identify both gaps and potential materiel and nonmateriel solutions must be supported by a robust analytical process. The capability analysis process consists of four steps: area analysis (AA), needs analysis (NA), solution analysis (SA), and post independent analysis (PIA).
1.5.1.1 Area Analysis
The AA can be initiated in several ways, through the FOH Board of Directors, a combatant commander (CCDR), or the SG. The AA is based upon approved CONOPS and examines in broad terms the ability to carry out the concept (e.g., en route care; evacuation to, around and from seabased assets; and the movement of patients up to 2,000 nautical miles (nm)). The concept should be a result of a joint integrated capability requirement. The analysis should identify operational general tasks, conditions, and standards needed to achieve the desired military objectives.
1.5.1.2 Needs Analysis
The NA is the second step in the capability analysis process. This step assesses the ability of the current and programmed capabilities to accomplish the tasks under the full range of operating conditions and to the designated standards identified in the AA. Using the tasks identified in the AA as primary input, the NA describes the gap or problem. It lists the key attributes of a capability that would resolve the issue in terms of purpose and identifies area metrics that can be used as measures of effectiveness. The result is a list of capability gaps, overlaps, and risks that require solutions and indicate the time frame in which those solutions can be accomplished. This step must be collaborative for Navy Medicine’s afloat and ashore forces. The NA could be used to identify the modularization, mobility, and sustainment of EMFs as identified in a notional AA of theater hospitalization.
1.5.1.3 Solution Analysis
The SA is the third step in the capability analysis process. In this step, the gaps identified in the NA are used as inputs. It is an assessment of potential doctrine, organization, training, materiel, leadership and education, personnel and facilities (DOTMLPF) and policy approaches to solving or mitigating one or more identified capability gaps. The order of priority for solution approaches includes changes to the existing DOTMLPF and/or policy; product improvements to existing materiel or facilities; adoption of interagency approaches that have limited nonmateriel DOTMLPF and/or policy consequences; and new materiel starts. One use of SA is to analyze Army medical evacuation (MEDEVAC) squadrons to shuttle patients to and from hospital ships to fill a need for dedicated MEDEVAC assets with some en route care capability during major combat operations.
1.5.1.4 Post Independent Analysis
The PIA is the final step in the capability analysis process. In this step, the compiled information and analysis resulting from the SA is independently analyzed to ensure that the list of approaches is complete and has the potential to deliver the capability identified in the AA and NA.

NWP 4-02
1-7 JAN 2008
Note
Developing Navy medical capabilities must closely correlate with the processes found in the JCIDS.
For further information on JCIDS, refer to Chairman of the Joint Chiefs of Staff Instruction (CJCSI) 3170.01 (series), Joint Capabilities Integration and Development System.
1.5.2 Health Service Support Requirements Determination
Navy Medicine provides HSS capability by assigning tasks to its organizations. These tasks are defined in the universal language of the joint tasking system and, in broad terms, are requirements for the medical departments. The Universal Naval Task List (UNTL) is a single-source document that includes the NTTL and the Marine Corps Task List (MCTL). As applied to joint training and readiness reporting, this task list provides a common language that commanders can use to document their command warfighting requirements as mission-essential tasks (METs). The UNTL’s tactical level of war tasks are a compilation of Navy, Marine Corps, and Coast Guard tasks that are written utilizing the common language and task hierarchy of the UJTL.
The UJTL identifies tasks at varying levels of operations by analyzing the Joint Strategic Capabilities Plan (JSCP), current operation plans (OPLANs), and the individual mission. The UJTL provides a detailed discussion of task conditions and standards. Conditions are variables of the environment that affect the performance of tasks in the context of the assigned mission. They are categorized as physical environment, military environment, or civil environment, with a minimum of acceptable proficiency required in the performance of a particular task under a specified set of conditions. Standards are established by the commander.
The tasks identified in the UJTL are architecturally linked to the tasks identified in the UNTL. They include strategic-national (SN), strategic-theater (ST), and operational (OP) levels of war tasks. Paragraphs 1.5.2.1 and 1.5.2.2 provide task lists at the joint and naval levels to include the HSS missions at the different levels of warfighting.
1.5.2.1 Universal Joint Task List
1. Strategic-National
a. SN 1.1.5, Determine Impact of Environmental Conditions on Strategic Mobility
b. SN 1.2.6, Conduct Redeployment or Retrograde of Personnel and Equipment from Theater
c. SN 1.2.8, Provide Global Patient Movement and Evacuation
d. SN 3.3.6, Determine National Residual Capabilities
e. SN 4.3.3, Coordinate Defensewide Health Services
f. SN 4.3.4, Develop and Maintain a Medical Surveillance Program
g. SN 6.6.4, Expand Health Service Support
h. SN 8.1, Support Other Nations or Groups
i. SN 8.1.5, Conduct Foreign Humanitarian Assistance and Humanitarian and Civic Assistance
j. SN 8.2.3, Support Evacuation of Noncombatants from Theaters

NWP 4-02
JAN 2008 1-8
k. SN 9.1.3, Coordinate Battle Management, Command, Control, Communications, Computers, Intelligence, Surveillance, and Reconnaissance
l. SN 9.2.2, Coordinate Consequence Management.
2. Strategic-Theater
a. ST 4.2.2, Coordinate Health Service Support
b. ST 4.2.2.1, Manage Theater Joint Blood Program
c. ST 4.2.2.2, Coordinate Patient Evacuation from Theater
d. ST 4.2.2.3, Manage Medical, Dental, and Veterinary Services and Laboratories and Supply
e. ST 4.2.2.4, Coordinate Joint Comprehensive Medical Surveillance
f. ST 4.3.1, Establish and Coordinate Movement Services within Theater
g. ST 8.2.4, Coordinate Humanitarian and Civic Assistance Programs
h. ST 9.5, Coordinate Consequence Management (CM) in Theater.
3. Operational
a. OP 1.6, Conduct Patient Evacuation
b. OP 4.4.3, Provide for Health Services in the Joint Operations Area (JOA)
c. OP 4.4.3.1, Manage Joint Blood Program in the Joint Operations Area (JOA)
d. OP 4.4.3.2, Manage Flow of Casualties in the Joint Operations Area (JOA)
e. OP 4.4.3.3, Manage Health Services Resources in the Joint Operations Area (JOA)
f. OP 4.4.5, Train Joint Forces and Personnel
g. OP 4.5.2, Supply Operational Forces
h. OP 4.5.3, Recommend Evacuation Policy and Procedures for the Joint Operations Area (JOA)
i. OP 6.2.6, Conduct Evacuation of Noncombatants from the Joint Operations Area (JOA).
1.5.2.2 Universal Naval Task List
1. Navy Tactical Task List
a. NTA 1.2.8, Conduct Tactical Reconnaissance and Surveillance
b. NTA 4.7.8, Provide Humanitarian Support
c. NTA 4.8.1, Support Peace Operations
d. NTA 4.12, Provide Health Services

NWP 4-02
1-9 JAN 2008
e. NTA 4.12.1, Perform Triage
f. NTA 4.12.2, Provide Ambulatory Health Care
g. NTA 4.12.3, Provide Surgical and Inpatient Care
h. NTA 4.12.4, Provide Dental Care
i. NTA 4.12.5, Coordinate Patient Movement
j. NTA 4.12.6, Provide Industrial and Environmental Health Services
k. NTA 4.12.7, Maintain Records
l. NTA 4.12.8, Obtain and Analyze Medical Information
m. NTA 4.12.9, Train Medical and Nonmedical Personnel
n. NTA 4.12.10, Provide Health Services in Support of Humanitarian and Civic Assistance
o. NTA 4.12.11, Provide Medical Staff Support
p. NTA 4.12.12, Perform Levels II/III Medical Support
q. NTA 6.5.1, Provide Disaster Relief (DR).
2. Marine Corps Task List
a. MCT 1.6.6.7, Conduct Humanitarian Assistance (HA) Operations
b. MCT 4.5, Provide Health Services
c. MCT 4.5.1, Conduct Health Maintenance
d. MCT 4.5.2, Perform Casualty Collection
e. MCT 4.5.3, Conduct Casualty Treatment
f. MCT 4.5.4, Conduct Temporary Casualty Holding
g. MCT 4.5.5, Conduct Casualty Evacuation
h. MCT 4.5.6, Conduct Mass Casualty Operations
i. MCT 4.6.1.7, Provide Civil Affairs Support
j. MCT 6.3, Perform Consequence Management.
Additional information on the development of Service component mission-essential tasks can be found in the Chairman of the Joint Chiefs of Staff Manual (CJCSM) 3500.03 (series), Joint Training Manual for the Armed Forces of the United States. Office of the Chief of Naval Operations Instruction (OPNAVINST) 3500.38 (series)/Marine Corps Order (MCO) 3500.26/United States Coast Guard Commandant Instruction (USCG COMDTINST) 3500.1B, Universal Naval Task List (UNTL), provides a breakdown of Navy tactical task (NTA) metrics.

NWP 4-02
JAN 2008 1-10
1.6 RESOURCES
1.6.1 Planning, Programming, and Budgeting System
The Planning, Programming, and Budgeting System (PPBS) is part of the strategic planning process. Once the National Military Strategy (NMS) has been set during the Quadrennial Defense Review (QDR), the Contingency Planning Guidance (CPG) outlines the areas that the United States will engage. The JSCP is then developed to provide guidance and tasking for war planning.
1.6.1.1 Planning
CJCSI 3110.3 (series), Logistics Supplement to the Joint Strategic Capabilities Plan (JSCP), provides CCDRs, Service chiefs, and defense agencies with overall planning guidance in support of HSS assigned tasks. Combatant command surgeon’s staff determine medical requirements to support JSCPs and match them against available resources. If there are not enough resources to meet the requirements, integrated priority lists establish precedence based on need.
1.6.1.2 Programming
Determining HSS requirements are part of the program objective memorandum (POM) process. In this instance, each Service provides its inputs for the POM to DOD, which submits to Congress requirements to be funded by the federal budget. The submission of the POM is a statement of need and funding for future resources and is built from illustrative theater operational scenarios instead of the OPLANs of current combatant commands.
1.6.1.3 Budgeting
Programming and budgeting for NEHSS is the responsibility of the resource sponsor, OPNAV N41, which includes providing funding to the BSO. The BSO in turn provides funding to BUMED BSO-18, USFFC BSO-60, and Commander, US Pacific Fleet (COMUSPACFLT) BSO-70. Program managers, EMFs, and hospital ships are responsible for planning and documenting justifications for program funding and for providing inputs in accordance with the PPBS timeline. These budget-planning inputs by the program managers are for reequipping and normal life-cycle maintenance.
1.6.2 Transition Health Service Support Resourcing
After activating the expeditionary HSS unit, personnel, equipment, and supplies must be transported to the operational site. Transportation from the point of origin to the port of embarkation (POE) is a service responsibility. Transportation from the POE to the unit’s final destination (deployment) is the responsibility of the theater commander/Navy component commander. Initial supply, including resupply, is a service responsibility until the joint theater single integrated logistics management system is established. The component commander possessing operational control (OPCON) is responsible for funding the expeditionary HSS units’ operating and sustainment costs once deployed. Operating target (OPTAR) funds provided by the supporting component commander are controlled in accordance with relevant publications and directives. The costs of intratheater patient movement and administration are a theater commander’s responsibility. Costs for strategic patient movement are charged to the Services. (See Figure 1-3 for a depiction of resource allocation responsibilities for programming and budgeting of expeditionary HSS capabilities.)

NWP 4-02
1-11 JAN 2008
FUNDING T-AH EMF
(Includes FDPMU)
FLEET SURGICAL
TEAM
Resource Sponsor OPNAV N4 (hull) OPNAV N1 (MTF personnel)
OPNAV N41 USFFC
Program Manager Military Sealift Command (MSC)
BUMED M5 Class Squadron
Type Commander MSC (hull) BUMED (MTF)
BUMED USFFC
Figure 1-3. Resource Allocation Responsibilities for Programming and Budgeting
1.7 HEALTH SERVICES IN AN OPERATIONAL ENVIRONMENT
The HSS capabilities offered by deployable medical systems (DEPMEDS) are dependent on the capability of care they are intended to provide. These capabilities in theater range from first responder to theater hospitalization. The practice of medicine on any operational platform or DEPMEDS is based on two concepts of care.
1.7.1 Concepts of Care
1. The first concept of care identified in the Navy Medical (NAVMED) P-117, The Manual of the Medical Department (MANMED), states that medical care delivered in an operational environment is different from the well-controlled environment of a fixed MTF. The mission of a combat environment MTF is to save lives, render emergency medical care, stabilize the patient’s condition, and transfer the patient to definitive care. As a result, the standards of the Joint Commission on Accreditation of Health Care Organizations (JCAHO) are not applicable to operational medicine.
2. The second concept of care is the return of patients to duty as soon as possible in order to preserve force-fighting strength. This is particularly true for the dental casualty and is one cornerstone for dental capabilities being in theater. If a patient cannot be returned to duty, treatment shall be based on performing procedures appropriate to stabilizing for the next capability of care.
1.7.2 Quality of Care
In an operational status, deployable HSS units experience varied patient workload levels. Levels may escalate to patient overload and exceed the unit’s capacity for concurrent patient care. Triage then becomes necessary. Triage is a sorting process that assesses the severity of each casualty based not only on the type of injury but also on the available capabilities and the overall casualty rate. Using this process permits the salvage of the greatest number of casualties given the limited capabilities available. The extent of care depends upon the casualty workload and the ability to administer care to the greatest number of casualties.
During mass casualty situations, medical care administered will be as thorough as possible given operational conditions. Quality assurance in the expeditionary HSS unit includes monitoring infection control and adhering to the patient movement policy, casualty reception, and triage plans. Unless a mass casualty situation exists, the HSS staff should not perform any procedure for which they are not privileged. The credentials review and privileging processes are performed prior to deployment.

NWP 4-02
JAN 2008 1-12
Quality of care services include:
1. Clinical Services. To the extent the operational environment permits, the HSS unit may be modified at the request of the unit’s senior medical department representative (SMDR)/senior medical representative (SMR) to provide additional care to operating forces. The operational commander and surgeon must consider mission requirements when adjudicating requests for HSS unit modification.
a. Clinical practice in an operational environment is based on applying practiced skills within facility limitations related to structure, equipment, supplies, or manpower. The requests are sent by the operational commander’s chain of command to BUMED through OPNAV N931 for further action. BUMED then tasks supporting commands to provide the capabilities that are required.
b. Because expeditionary HSS units may sometimes be employed in situations other than intensive combat, the type of practice can change. HSS units, in particular theater hospitalization capability facilities, may be used increasingly in protracted operations that require extensive hospital functions. The unit senior medical representative (SMR) should determine the extent of practice modification, basing the decision on the facility’s equipment, supplies, and personnel, and on the population at risk.
c. Multinational operations may present challenges where the SMR may rely on physicians, whose broad medical background includes general medicine, pediatrics, obstetrics, gynecology, and office practice of surgical procedures. During refugee operations, family practice providers can be ideal health care providers for onsite refugee care. With increased US involvement in peacetime operations, operational commanders should consider this capability. The employment of family practice physicians should augment, not replace, internal or emergency medicine specialists.
2. Dental Services. During a period of intense combat operations, with combat casualties, Marine logistics group (MLG) dental battalion personnel augment the medical battalion mission in various roles as well as provide treatment for acute dental needs. If the tempo of operations permits, definitive restorations are performed. As the length of deployment increases and combat operations subside, other procedures would include dental maintenance and require periodic examinations and the inclusion of other elective procedures. Oral surgeons and comprehensive trained dentists are augmented to CRTS units, EMFs, and hospital ships.
3. Optometry Services. Optometry services are typically limited to theater hospitalization capability and higher capability. While such facilities may have optical fabrication laboratories stocked to manufacture standard spectacles in a limited range, they are generally not equipped to produce spectacles requiring extreme single-vision prescriptions or multi-focal lenses. Spectacle fabrication becomes a critical requirement when glasses are lost or damaged and troops arrive without spare eyeglasses or inserts for their gas masks or combat eye protection. Personnel who use corrective lenses for seeing a distance may consider corrective surgery to obviate the need for eyeglasses or corrective lenses. Optometry and optical fabrication may be a significant source of care in humanitarian scenarios.
4. Credentials and Privileging. Per Bureau of Medicine and Surgery Instruction (BUMEDINST) 6320.66 (series), Credentials Review and Privileging Program, medical regional commanders (RCs), Navy Medicine East (NME), Navy Medicine West (NMW), and Navy Medicine National Capital Area (NCA), are designated privileging authorities for fixed medical and dental treatment facilities (MTFs/DTFs) within their area of responsibility (AOR). The RC may further delegate privileging authority for practitioners assigned to an MTF/DTF to the facility commanding officer (CO) or medical center deputy commander, as appropriate.
For the Fleet, privileging authority will be delegated from the USFFC Surgeon to the TYCOMs — air forces (AIRFOR), submarine forces (SUBFOR), surface forces (SURFOR), the Navy Expeditionary Combat Command (NECC), and special warfare (SPECWAR). The USFFC Surgeon will retain for selected groups like MSC, Safety Center, and numbered fleet surgeons. TYCOM surgeons will be privileged by USFFC.

NWP 4-02
1-13 JAN 2008
For the Marine Corps, the Medical Officer of the Marine Corps (TMO), as designated by the Surgeon General, is the privileging authority for medical personnel assigned to the Marines. The TMO may secondarily delegate that authority down to the level of the MEF surgeon, but not any further.
1.8 DEPLOYABLE HEALTH SERVICE SUPPORT
Navy Medicine’s deployable HSS is provided from a wide range of platforms and force structures. HSS is standardized among the Services to the maximum extent possible with their distinct missions and use of common components. These components are established by the Defense Medical Standardization Board and include only medical and dental items.
1.8.1 Hospital Ships
The hospital ship has a maximum capability of 12 operating rooms (ORs) and up to 1,000 beds within the MTF that can be tailored to meet expected patient throughput and variable lengths of stay based on the intensity of required care. Hospital ships represent a unique national asset: the ability to provide medical services worldwide in the largest afloat medical facility. They offer flexibility in responding to different mission scenarios, domestic and international, with extensive and diverse clinical facilities that can be tailored to meet different requirements. Each ship is staffed and equipped to provide care equal to that provided by any tertiary-care medical facility in the United States. Depending on the tactical situation, the mobility and flexibility of the hospital ships offer a continuum of care from initial resuscitative care to definitive long-term care.
A civilian mariner (CIVMAR) crew supplied by the Commander, Military Sealift Command (MSC) and an MTF crew provided by the Chief, Bureau of Medicine and Surgery (CHBUMED) jointly man the ships. The CIVMAR and MTF crews are separate but have interdependent command elements: the MSC civilian crew for ship operations and the embarked components for HSS requirements. The CIVMAR crew is responsible for the hull, propulsion, and auxiliary machinery systems, navigation, commercial communications, and overall ship’s safety. The MTF staff is responsible for the operation, maintenance, logistics, and administrative support of the MTF complex as well as critical MTF support functions such as naval communication, oxygen/nitrogen generation, aviation, galley, laundry, and vertical replenishment operations. The MTF staff also augments the CIVMAR crew for critical functions such as damage control, firefighting, and underway replenishment.
Both ships are maintained in a reduced operating status (ROS), which permits activation to full operating status (FOS) and deployment within 5 days (ROS-5). While in ROS, the CIVMAR crewmembers are responsible for ship’s security and the upkeep of the ship’s systems, and the Navy personnel are responsible for the readiness and maintenance of MTF spaces, supplies, and equipment.
For further information on hospital ships, refer to NTTP 4-02.6, Hospital Ships.
1.8.2 Expeditionary Health Service Support Medical Facilities
While initially conceived and developed as war reserve facilities to provide HSS during intense combat operations, EMFs can also be used in protracted low-intensity conflict scenarios and humanitarian operations, with design changes. EMFs are transportable, modular, medically and surgically intensive, and employable in a variety of operational environments. They are prepositioned in various CONUS and OCONUS locations, or deployed on maritime prepositioning force enhanced (MPF(E)) ships. Once transported to the desired location, they can be assembled and operational in a minimum of 10 days provided all components have been delivered to the site and the operational commander has completed site preparation by the EMF’s assigned staff. Time frame for assemblage varies with the size and/or capability of the EMF. EMFs, depending on the size, can provide theater hospitalization capability and capabilities similar to those on a hospital ship; however, they are not light and have a large footprint. Due to the size associated with some EMF platforms, significant logistical support is required to relocate these assets once assembly and activation have occurred. Smaller, task-organized DEPMEDS are easier to relocate, post-activation, with much less logistical support.

NWP 4-02
JAN 2008 1-14
EMFs are advanced base functional components (ABFCs). HSS expeditionary ABFCs are designated HSS facilities that are planned as a grouping of personnel, facilities, equipment, and materiel designed to perform a specific function or accomplish a particular mission. They incorporate almost all capabilities necessary to be self-sufficient. Smaller task-organized EMFs can be established to provide greater mobility required to support expeditionary forces. The scalable EMF configuration provides the medical core elements of the assembly required to meet mission requirements; it can be assembled and operational in three to five days. The EMF can be used with onsite infrastructure support and augmented with a base operating support (BOS) package, which increases personnel, facilities size, and area requirements substantially.
For further information on infrastructure and logistics requirements for expeditionary medical facilities, refer to NTTP 4-02.4, Expeditionary Medical Facilities.
1.8.3 Casualty Receiving and Treatment Ships
The commander, expeditionary strike group (CESG) designates specific ships as primary CRTSs to provide FRC capability to the landing force (LF) during expeditionary operations. Primary CRTSs have laboratory (including blood) and radiology capability to support surgical suites. During expeditionary operations, primary CRTSs are staffed with surgical and nonsurgical personnel who are required to provide extensive trauma support. Ships designated as primary CRTSs include the large-deck amphibious ships (LHAs, LHDs).
The expeditionary strike group (ESG) commander may designate other amphibious ships as secondary CRTSs. At a minimum, the ship should have the capability to receive and treat casualties, given that appropriate HSS materiel and personnel are available to provide resuscitative care. Ships designated as secondary CRTSs include LPD and LSD Class ships. (See Appendix D for the identification of CRTS capabilities.)
1.8.4 Aircraft Carriers
Aircraft carriers are equipped with a 51-bed FRC capability (with the exception of blood bank capabilities). The department has three dedicated intensive care unit (ICU) beds with coinciding equipment; one OR; basic x-ray and ultrasound capability; pharmaceutical services; physical exam services, including refractions, audio tests, and spectacle fabrication capability; clinical psychology services; physical therapy services; preventive medicine services; and dental services, including oral surgery and prosthetics.
Manning the aircraft carrier resuscitative care capability includes a senior medical officer (SMO) (flight surgeon); a general surgeon; a nurse anesthetist/anesthesiologist; a general medical officer; two flight surgeons attached to the air wing; a physician assistant; a clinical psychologist; a physical therapist; a health care administrator; a nurse corps officer; a radiation health officer; a senior dental officer; an oral surgeon; a prosthodontist; three general dentists; and fifty hospital corpsmen (including embarked units). The carrier HSS department also serves as a consultative and primary MEDEVAC facility for the other ships that make up the carrier strike group.
1.8.5 Forward Deployable Preventive Medicine Unit
Task-organized forward deployable preventive medicine units (FDPMUs) are joint force health protection (FHP) capabilities that are capable of providing specialized preventive medicine support to the operational commander within 96 hours of notification. Assigned to a joint task force (JTF) or other deployed HSS units to augment the theater commander or surgeon and other field personnel, FDPMUs are rapid-response, specialized preventive medicine platforms that focus on identifying, evaluating, and assessing the risk of environmental health hazards. They are deployed to assess, prevent, or reduce health threats in support of deployed operating forces, and to provide HCA and consequence management. Their capabilities include assessment of nuclear, biological, chemical health threats as well as toxic industrial chemicals/material detection and identification, disease vector surveillance, and control and assessment of endemic disease.

NWP 4-02
1-15 JAN 2008
1.8.6 Fleet Surgical Teams
Fleet surgical teams (FSTs) are operationally assigned to large-deck amphibious assault ships (LHAs/LHDs) to provide FRC capability in support of an ESG with an embarked Marine air-ground task force (MAGTF). FSTs are attached to operating forces of the Atlantic and Pacific Fleets. There are nine FSTs in service, each with 16 permanently assigned members, including a permanent officer in charge (OIC)/ESG surgeon, general surgeon, family practice/internal medicine/emergency room/pediatric physician, anesthetist/certified registered nurse anesthetist, perioperative nurse, ICU/critical care nurse, medical regulator, leading petty officer, four general duty corpsmen, two OR technicians, advanced laboratory technician, and respiratory therapy technician. Each FST has its own unit identification code (UIC) and a type commander (TYCOM)–managed budget. Ashore, the FST reports administratively to the respective amphibious squadron commander.
1.8.7 Special Psychiatric Rapid Intervention Team
The special psychiatric rapid intervention team (SPRINT) provides short-term (less than 180 days) HSS augmentation for the ROMO. The SPRINT provides mental health and emotional support immediately after a disaster with the goal of preventing long-term medical psychiatric dysfunction or disability. It may also be used in combat and operational stress scenarios.
1.8.8 Humanitarian Support Team
Humanitarian support teams (HSTs) care for noncombatant casualties or patients in response to migrant/refugee processing and support, natural HCA, NEO, and exposure to chemical or biological hazards. HSTs are also available for enhancement of MTF capabilities. HSTs are not standing medical capabilities, but rather ad hoc teams that are formed to address specific HA/DR requirements, functions, and capabilities.
1.8.9 Seabased Medical Capabilities
In addition to the DEPMEDS capabilities described above, individual Navy ships are equipped with organic health care capabilities primarily for support of in port and embedded personnel while at sea. The exception is the hospital ships that have HSS as their primary mission. The expanded spaces of the LHA- and LHD-class ships are designed to serve as CRTSs. These ships require an FST detachment when forward deployed and may require Health Services Augmentation Program (HSAP) personnel to meet increased operational requirements.
The number and type of health care personnel and the extent of medical facilities, equipment, and supplies on any ship are based generally on the ship’s type, mission, complement, and embarked personnel. The minimum shipboard HSS staffing is one independent duty corpsman (IDC) who provides routine health care, first aid, and emergency treatment consistent with capabilities.
Most afloat HSS facilities cannot be increased significantly by personnel augmentation alone because of space constraints. Carriers, ESG ships, some auxiliary ships, and transports are fitted with facilities to accommodate one or more assigned medical, dental, medical service, or nurse corps officers, as well as hospital corpsmen. The capability also exists, in varying degrees, to receive and employ HSAP personnel, equipment, and supply blocks, and to function as CRTSs.
The heads of ships’ HSS departments/divisions are the senior medical and dental corps officers assigned to the ship’s company. On ships without an assigned HSS officer, an IDC will normally be designated the SMDR. (See Figure 1-4 for the medical capabilities of various classes of Navy ships.)
1.8.10 Marine Corps Deployable Medical Systems
In garrison and during routine deployments, Marine Corps units are not staffed with the full wartime complement of HSS personnel. When increased HSS manning levels are required, units can be brought to wartime-level manning through HSAP. HSS units that are organic to the MAGTF are primarily staffed and equipped to provide first responder and FRC capability in support of MAGTF operations. Because of the necessity for MAGTF

NWP 4-02
JAN 2008 1-16
UNIT LPD
LPD 17
LSD
MCM/MHC
FFG/DDG/CG/DD/
HSV/PC
LCC AOE AS LHD LHA CVN T-AH
BED CAPACITY
Intensive Care Unit 0 6 0 0 0 0 0 0 15 15 2 80 Ward 6–8 18 6–8 0 0 20 6 20 45 45 52 920
OPERATING ROOMS
Medical Major ORs 0 1 0 0 0 0 0 0 4 2 1 12 Medical Minor ORs 1 1 1 0 0 1 0 1 2 2 1 0 Dental Operatories 1 2 2 0 0 2 2 4 4 3 7 2
X-RAY UNITS
CAT Scan 0 0 0 0 0 0 0 0 0 0 0 1 Fixed X-Ray Units 0 1 0 0 0 0 0 1 1 1 1 4 Portable X-Ray Units 1 0 1 0 0 1 1 0 1 1 1 5
LABORATORY 1 1 1 0 0 1 1 1 1 1 1 1 PHARMACY 0 1 1 0 0 1 1 1 1 1 1 1 BLOOD
Total Frozen Units 0 0 0 0 0 0 0 0 400 400 0 1,400
Total Liquid Units 0 0 0 0 0 0 0 0 0 0 10–15 2,000
MORGUE CAPACITY 0 0 0 0 0 0 0 0 12 12 0 22
Legend: AOE fast combat support ship DDG guided missile destroyer LPD landing platform, dock AS submarine tender FFG guided missile frigate LSD landing ship, dock CG guided missile cruiser HSV high-speed vessel MCM mine countermeasures ship CVN aircraft carrier, nuclear LCC amphibious command ship MHC coastal minehunter DD destroyer LHA landing helicopter, assault PC patrol craft LHD landing helicopter, dock T-AH hospital ship
Figure 1-4. Shipboard Health Service Support Capabilities by Ship Class
organic HSS units to conform to the mobility requirements of their supported units, they are not tasked to provide definitive, restorative, rehabilitative, or convalescent care. During expeditionary operations, the combined HSS capabilities of the ESG and LF provide the entire continuum of care in support of a MAGTF. MAGTF organic units facilitate the task organization of MEF HSS as required by the specific mission.
Embarked HSS personnel shall report to the ship’s SMO. While embarked aboard ship, corpsmen assigned to Marine units have their own responsibilities associated with the embarked Marines and may help the ship’s organic HSS personnel. However, embarked HSS personnel will assist ship’s company HSS personnel in caring for embarked personnel and casualties.
The core elements of the MEF are the Marine division (MARDIV) ground combat element (GCE), Marine aircraft wing (MAW) aviation combat element (ACE), and MLG. Task-organized elements of the MLG’s medical and dental battalions with additional support provided by the Navy or other Service-deployed HSS systems usually provide HSS beyond the organic capabilities of the GCE and ACE.

NWP 4-02
1-17 JAN 2008
1.8.10.1 Marine Division
Each MARDIV consists of infantry regiments and infantry battalions, as well as other combat elements. At the infantry battalion level, a medical platoon provides corpsmen to each rifle and weapons company and staffs the BAS. The normal complement is two medical officers, a battalion surgeon, an assistant battalion surgeon, and 65 corpsmen. Eleven corpsmen are assigned to the weapons company, 11 to each of three rifle companies, and 21 corpsmen to the BAS.
The division surgeon, HSS administrative officer, environmental health officer, division psychiatrist, and enlisted HSS assistants are within the headquarters (HQ) battalion at the division level. Their functions are to plan and establish HSS requirements for the GCE. When a unit smaller than a division deploys as the GCE, the regiment or battalion surgeon assumes much of the planning responsibility in addition to assigned clinical responsibilities.
1.8.10.2 Marine Aircraft Wing
The MAW has a Marine wing support group (MWSG) that includes a Marine wing support squadron (MWSS) aid station (one for each Marine aircraft group). The MWSS aid station medical staff, consisting of a flight surgeon and hospital corpsman, provides routine sick call, aviation medicine, preventive medicine, and laboratory, x-ray, and pharmacy services. At the wing level is a Marine wing HQ squadron with a wing medical officer, medical administrative officer, environmental health officer, industrial hygiene officer, and corpsmen. Their staff functions are similar to those for the MARDIV HQ HSS staff.
1.8.10.3 Marine Logistics Group
Most MEF medical/dental capabilities reside within the MLG. The preventive medicine personnel within the ACE, GCE, and MLG provide preventive medical services at the direction of the MEF preventive medicine officer. The group surgeon, group aid station, and health service support element (HSSE) are in the MLG’s HQ and Service battalion. The group surgeon advises the MLG commander and oversees the group aid station. The dental battalion commander has additional special staff officer duties as the MEF and MLG dental officer, and is the principal adviser to the MEF commander on dental issues. The mission of the HSSE is to coordinate requirements for HSS with the MAGTF and units external to the MLG. The MLG has a medical battalion that is organized to execute HSS functions in support of the MAGTF mission. The medical battalion provides initial resuscitative HSS to the MEF and is the only source of organic Marine Corps support above the aid station level. A medical battalion is composed of three surgical companies and a HQ and Service company.1 A medical battalion may be task-organized to provide STPs, forward resuscitative surgery systems (FRSSs), and en route care. The STPs report to the medical battalion’s HQ and Service company. Each STP has 10 patient holding cots, a stabilization area, and a collection/evacuation unit. Each surgical company has 60 cots and 3 ORs and consists of a HQ platoon, triage/evacuation platoon, surgical platoon, holding platoon, combat stress platoon, and ancillary services (laboratory, x ray, pharmacy) platoon. A dental detachment provides dental support.
Additionally, a preventive medicine unit is part of each medical battalion and is staffed and equipped to provide support beyond the organic capability of the MAGTF GCE and ACE. This unit comprises the bulk of preventive medicine capabilities in an MEF. When preventive medicine requirements exceed organic capabilities of a supported unit, the unit commander should submit a request for additional support to the MEF preventive medicine officer. The dental battalion provides field dentistry and augments the medical battalion capabilities, providing additional manpower support for combat casualty treatment.
1.8.10.4 Forward Resuscitative Surgery System
The FRSS consists of eight personnel: two general surgeons, an anesthesiologist, a critical care nurse, an IDC, two OR technicians, and a Navy enlisted classification (NEC) 8404 (field medical service technician) corpsman. It is capable of caring for five casualties at any one time (two preoperative, one intraoperative, and two postoperative), and can care for up to 18 casualties requiring surgery over a 48-hour period before requiring __________
1 Medical battalions are sized in accordance with the forces they support. First and second medical battalions have three surgical companies and eight STPs. Third and fourth medical battalions are smaller, with two surgical companies and six STPs.

NWP 4-02
JAN 2008 1-18
resupply and relief of personnel. It also requires an en route care system (ERCS) to move patients postoperatively, as holding capability is limited. The FRSS may augment a STP or a BAS. When augmenting a BAS, the FRSS can require personnel augmentation to accomplish triage and preoperative holding tasks more effectively. The augmented STP/BAS provides initial triage and assists in preoperative and postoperative patient holding, communications, security, and patient movement.
The doctrinal concept of employment utilizes the FRSS when the tactical situation precludes use of a surgical company or when rapid transport of casualties needing surgery to a higher capability of care is not available. During Operation IRAQI FREEDOM (OIF), the FRSS was utilized in an additional capacity, that of an initial surgical capability for a surgical company. The FRSS, along with an STP and a holding platoon, would jump to a forward support area and provide almost-immediate casualty care until the remainder of the surgical company was established and functional. The FRSS can be utilized in support of HCA operations when rapid response is required for a mission of short duration. It can also support a combat logistics regiment (CLR) during low-intensity conflicts. Other possible employments include use of the FRSS to provide surgical capability for split ESG operations, afloat and ashore. Future capabilities include surge augmentation of existing facilities. Because of its small size, the FRSS can be employed in a variety of tactical situations where surgical care is needed.
1.9 LESSONS LEARNED
Commanders of operational units are required to develop and forward lessons learned and after action reports through combatant commands and Service channels. Lessons learned systems provide information on system improvements developed and on areas in need of correction. The deployed unit prepares lessons learned in accordance with BUMEDINST 3500.3 (series), Naval Operational Medical Lessons Learned System (NOMLLS), for incorporation into NOMLLS. The Naval Operational Medical Lessons Learned Center (NOMLLC) collects, analyzes, and validates Naval Operational Medical Lessons Learned (NOMLL). All vetted and validated NOMLLs are stored in NOMLLS and when appropriate are exported to the Navy Lessons Learned System (NLLS) and/or the Marine Corps Lessons Learned Management System (MCLMS). Further Services’ lessons learned guidance is provided in OPNAVINST 3500.37 (series), Navy Lessons Learned System (NLLS) and Marine Corps Order (MCO) 3504.1, Marine Corps Lessons Learned Program (MCLLP) and the Marine Corps Center for Lessons Learned (MCCLL). Additional details on lessons learned are provided in Appendix H.

NWP 4-02
2-1 JAN 2008
CHAPTER 2
Naval Expeditionary Health Service Support Organization, Command and Control,
Roles, and Responsibilities
2.1 INTRODUCTION
NEHSS must be considered in the context of strategic organization, chain of command, command authority, C2, and strategic, operational, and tactical levels. Knowledge of strategic organization and command relationships enables HSS planners to understand the mechanism by which HSS capabilities are employed and how HSS is planned, requested, and utilized in various contingencies. HSS planners must take into account the responsibilities of participating activities, both supporting and supported, and the Navy medical organization to provide expeditionary HSS.
2.2 STRATEGIC ORGANIZATIONAL RELATIONSHIPS
2.2.1 Health Service Support Planner Requirements
Clear and effective command relationships must be understood to ensure the effective use of all resources. To apply military HSS principles to a US military organization effectively, the HSS planner should possess an awareness of command and support and a working knowledge of command terminology essential to understanding the relationships, responsibilities, and chains of command inherent in US military organizations.
2.2.2 The National Command Authority
According to the Goldwater-Nichols DOD Reorganization Act of 1986, the chain of command of the US military is made up of the President and the SecDef, or their deputized alternates or successors, who have constitutional authority to direct the Armed Forces of the United States in the execution of military action. Together they make up the National Command Authority with authority extending to the CCDRs for their assigned missions and forces. The National Command Authority extends to the Secretaries of the Military Departments, who are responsible for organizing, training, equipping, and providing forces, and the Chiefs of the Services, who are responsible for the execution of CRTS’s Service functions. (See Figure 2-1 for the National Command Authority chain of command and control.)
2.2.3 Establishment and Assignment of the Combatant Command
A combatant command is a unified or specified command that ensures US military unity of effort. It is a command that has a broad, continuing mission under a single commander and is composed of forces from two or more Services. The President, with the advice of the SecDef and the Chairman of the Joint Chiefs of Staff (CJCS), establishes and appoints CCDRs under the authority of the National Security Act of 1947 and Title 10, United States Code (USC), Armed Forces. The CCDR is responsible to the National Command Authority for command preparedness and the execution and accomplishment of the assigned mission. The CCDR leads a unified or specified functional command and is the only military leader with statutory authority to organize and task all Services under COCOM control. Paragraph 2.3 describes CCDR COCOM, OPCON, tactical control (TACON), and administrative control (ADCON).

NWP 4-02
JAN 2008 2-2
Figure 2-1. National Command Authority Chain of Command and Control

NWP 4-02
2-3 JAN 2008
2.2.4 Geographic and Nongeographic Areas of Responsibility
The Unified Command Plan (UCP) establishes the CCDRs, identifies the geographic AOR and theaters of operation, assigns primary tasks, defines authority of the commanders, establishes command relationships, and gives guidance on the exercise of COCOM.
2.2.4.1 Geographic Area of Responsibility
The AORs of the geographic CCDRs are:
1. United States Northern Command (USNORTHCOM)
2. United States Central Command (USCENTCOM)
3. United States European Command (USEUCOM)
4. United States Pacific Command (USPACOM)
5. United States Southern Command (USSOUTHCOM)
6. United States Africa Command (USAFRICOM).
2.2.4.2 Functional Area of Responsibility
CCDRs can be assigned a worldwide AOR in commands not bounded by geography:
1. United States Joint Forces Command (USJFCOM)
2. United States Special Operations Command (USSOCOM)
3. United States Strategic Command (USSTRATCOM)
4. United States Transportation Command (USTRANSCOM).
Note
Unified combatant commands can be either geographic combatant commands (GCCs) or functional combatant commands (FCCs). The chain of command runs from the President to the Secretary of Defense to the CCDRs of the unified combatant commands.
2.2.5 The Services — Military Departments
The chain of command for the Military Departments — the Headquarters, Department of the Army (HQDA), the Department of the Navy (DON), and the Department of the Air Force (DAF) — extends from the National Command Authority to the Secretaries of the Military Departments, who exercise authority, direction, and control through Service Chiefs not assigned to CCDRs, including all military service forces. The Military Departments and CCDRs have separate and distinct military branches in the chain of command. The Secretaries of the Military Departments are responsible for the administration and support of their forces, including those attached to CCDRs. They exercise ADCON through the Service component commanders assigned to the CCDRs. The Services’ administrative and support channels provide administrative, training, and logistic support to ensure that the CCDRs receive organized, equipped, and trained military forces.

NWP 4-02
JAN 2008 2-4
2.2.6 Combatant Command Authority
A CCDR may exercise COCOM through a subordinate activity such as a subordinate unified command, Service component commander, functional CCDR, and JTF.
For further information on COCOM, refer to JP 0-2, Unified Action Armed Forces (UNAAF).
CCDRs exercise COCOM by:
1. Establishing command relationships with subordinates
2. Delegating appropriate authorities
3. Assigning responsibilities to their subordinates to centralize direction and decentralize planning and execution.
2.2.7 Subunified Commands
Unified commanders, with approval from the National Command Authority, may establish subordinate unified commands, also called subunified commands, to conduct operations on a continuing basis according to established unified command criteria. The subunified commander exercises functions, authority, and responsibilities similar to those of a unified CCDR, except for COCOM. The subunified commander is authorized to exercise assigned command and force OPCON authority within the AOR or functional area. The Commander, United States Pacific Command (COMUSPACOM) established the subordinate unified commands, United States Forces, Japan (USFJ) and United States Forces, Korea (USFK).
2.2.8 Service Component Command
A Service component command consists of units, detachments, and installations of a single military service assigned to the unified command. The senior officer of the Service assigned to a unified command and who is qualified for command by the regulations of that Service is designated the Service component commander. The assignment of the Service component commander is subject to the concurrence of the CCDR. The Service component commander is responsible to the CCDR for all aspects of the force, including logistics, within the unified command.
2.2.9 Functional Component Command
A CCDR may establish a functional component command composed of like functional forces from more than one Service for major combat or stability operations to perform particular operational missions of short or extended duration. Functional component commands are organized according to joint coalition force land, air, maritime, and special operations component command missions, each focusing on operational responsibilities. A functional component command’s Service component command is responsible for logistical support.
2.2.10 Joint Task Force
A JTF is established in a geographical area or on a functional basis to execute missions with limited objectives that do not require centralized control of logistics. Although the JTF’s establishing authority is usually a CCDR, it can also be authorized by the SecDef, a subunified commander, a functional component commander, or an existing commander, joint task force (CJTF). A JTF is composed of two or more Services’ elements through mission completion. Some JTFs may expand to semipermanent JTFs that stay behind to maintain end-state conditions or accomplish a follow-on mission for an undetermined period. JTFs may take many forms and sizes as they are employed across ROMO in air, land, and maritime environments. JTF organization and staffing vary depending on the mission, the environment of operations, the composition of adversaries, and time. The JTF can be staffed in any manner that supports accomplishing the mission. Its HQ is traditionally staffed and sized according to mission requirements.

NWP 4-02
2-5 JAN 2008
For further information on the joint task force, refer to CJCSM 3500.05 (series), Joint Task Force Headquarters Master Training Guide; JP 4-0 series publications; and JP 3-33, Joint Task Force Headquarters.
2.3 COMMAND AUTHORITY
Command authority is central to military actions. The authority vested in a commander must be commensurate with the responsibility assigned. Levels of authority include the four types of command relationships: COCOM, OPCON, TACON, and support authority. The other authorities are ADCON, coordinating authority, and direct liaison authorized (DIRLAUTH).
2.3.1 Combatant Command
COCOM is the command authority authorized by Title 10, USC, Section 164, or as directed by the President in the UCP to unified or specified CCDRs. Through their Service component commanders, COCOMs provide to CCDRs full authority to organize and employ commands and forces; assign tasks; designate objectives; give authoritative direction over all aspects of military operations, joint training, and logistics; and exercise and delegate OPCON of assigned or attached forces. COCOM authority is neither delegated nor transferable.
2.3.2 Operational Control
OPCON is the command authority exercised by commanders at any echelon at or below the level of COCOM. OPCON is the authority to perform functions of command over subordinate forces involving organizing and employing commands and forces, assigning tasks, designating objectives, and giving authoritative direction necessary to accomplish the mission. The CCDR can delegate OPCON to subordinates. OPCON is the highest authority in which subordinates can direct military operations and joint training except for logistics, administration, discipline, internal organization, and unit training. An OPCON commander can control forces from one or more Services. OPCON authority also conveys the ability to exercise and delegate OPCON and TACON and to establish support relationships among subordinates. The Service component commander retains Service responsibility and authority for forces under OPCON of another command.
2.3.3 Tactical Control
The CCDR uses TACON to limit the authority to direct the tactical use of commands, military capabilities, or forces assigned, attached, or made available for tasking. TACON is inherent in OPCON and may be delegated or exercised by commanders below the level of COCOM. TACON is limited to local directions of the tactical force movement and maneuver to accomplish an assigned task. Service components continue to exercise organizational authority and administrative and support responsibilities.
2.3.4 Support Authority
Command authority established by a superior commander between subordinate commanders when one organization should aid, protect, complement, or sustain another force. Support may be exercised by commanders at any echelon at or below the combatant command level.
2.3.5 Administrative Control
ADCON is the direction or exercise of authority necessary to fulfill the statutory responsibilities of the Military Departments for administration and support. ADCON can be delegated to and exercised by Service commanders at any echelon at or below the Service component command. The Secretaries of the Military Departments are responsible for the administration and support of their forces assigned or attached to unified commands by exercising ADCON through the Service component commander of the unified command.

NWP 4-02
JAN 2008 2-6
2.3.6 Coordinating Authority
Coordinating authority is a consultation relationship between commanders, not an authority to exercise control. CCDRs and other subordinate commanders designate coordinating authority. COCOM specifies coordinating authority to foster effective coordination; however, coordinating authority does not compel any agreements.
2.3.7 Direct Liaison Authorized
DIRLAUTH, a coordination relationship and not a command relationship, is the authority granted by a commander at any level to a subordinate commander to coordinate an action directly with a command or agency within or outside the command.
For more information on command relationships and levels of authority, refer to JP 1, Doctrine for the Armed Forces of the United States.
2.4 COMMAND AND CONTROL OF DEPLOYABLE MEDICAL SYSTEMS
Unified commanders exercise COCOM over DEPMEDS capabilities that are assigned to their theater or AOR. CCDRs are responsible for establishing the appropriate levels of authority and command relationships of DEPMEDS within their respective theaters to accomplish the expeditionary HSS mission.
A CCDR may employ a number of options to exercise COCOM authority of DEPMEDS capabilities, including maintaining direct command and exercising COCOM authority through a subordinate activity, such as a subordinate unified command, Service component command, functional component command, or JTF. During OIF, USCENTCOM exercised the COCOM of two Navy EMFs and two FDPMUs through its Service component command subordinate activities, Commander, United States Navy, Central Command (COMUSNAVCENT); and Commander, United States Marine Forces, Central Command (COMUSMARCENT). COMUSNAVCENT assumed OPCON, and MEF, a subordinate activity of COMUSMARCENT, maintained TACON.
The CCDR can also elect to exercise COCOM of DEPMEDS through a joint, combined, or multinational task force (TF). During Operation Secure Tomorrow, USSOUTHCOM directed the Commander of the Multinational Interim Force in Haiti to accept OPCON of the supporting FDPMU. Although the CCDR has the option of maintaining direct control of DEPMEDS, COCOM is usually exercised through OPCON with a functional component command subordinate activity.
2.5 HEALTH SERVICE SUPPORT CONSIDERATIONS AT THE STRATEGIC, OPERATIONAL, AND TACTICAL LEVELS
At the top of the HSS hierarchy is the Assistant Secretary of Defense (Health Affairs), or ASD(HA), who sets policy for the MHS and establishes FHP strategic guidance for the Services. DOD’s strategic mission is to enhance the nation’s security by providing HSS for full ROMO and to sustain the health of those forces entrusted to their care. The ASD(HA) establishes objectives for the MHS. From the expeditionary HSS perspective, those objectives call for a medically ready total force, as measured by individual medical readiness (IMR); operational dental readiness (ODR); and a ready HSS capability, as measured by the resource status of deployable HSS units. The ASD(HA) establishes targets for each of the objectives. The IMR rate should be 75 percent medically ready to deploy, and 75 percent of deployable HSS units should be staffed, equipped, and trained. ODR should be 100 percent for deploying units and 95 percent for nondeploying units. These strategic readiness objectives are intended to meet the expectation of the operating forces for a healthy, fit, and medically protected force.
At the operational level, DOD’s strategic objectives for HSS are reflected in OPLANs, operation orders (OPORDs), and/or HSS planning guidance (Annex Q of OPORD/OPLAN) and translated into the following operational principles of conformity, proximity, flexibility, mobility, continuity, and coordination:
1. Conformity. Involve HSS planners in the development of the OPLAN/OPORD to ensure integration and compliance with the commander’s plan.

NWP 4-02
2-7 JAN 2008
2. Proximity. Provide HSS to injured or ill, as close to combat operations as the tactical situation permits, taking into account that time may be as important as distance in treating battlefield casualties.
3. Flexibility. Units must be prepared to shift HSS capabilities to meet changing requirements.
4. Mobility. Anticipate requirements for rapid movement of HSS units to support combat forces during operations.
5. Continuity. Provide optimum, uninterrupted initial and en route care to the injured or ill while moving them rearward through a progressive, phased HSS system, as dictated by the patient’s condition and tactical situation.
6. Coordination. Efficiently employ HSS resources to support the planned operation effectively.
As stated in JP 4-02, Health Service Support, geographic CCDRs are responsible for coordinating and integrating HSS within their theaters. A joint force surgeon (JFS) should be appointed for each combatant command, subordinate/unified command, and JTF. As a specialty adviser, the JFS reports directly to the joint force commander (JFC) and will coordinate HSS matters for the JFC. JFSs need to assess component command HSS requirements and capabilities and provide guidance to enhance the effectiveness of HSS through the shared use of capabilities. Liaison must be established between the JFS and each component surgeon.
Once the CCDR identifies HSS capabilities required to support the operation, a request is made for HSS unit support to the appropriate unified command, such as USJFCOM, USCENTCOM, and USPACOM. The unified command submits the request to the Service via the Joint Staff (JS). In the case of the Navy, the component commander (e.g., USFFC) will contact OPNAV N931 to forward the validated request to BUMED. BUMED will then task the MTF in support of the HSS unit. (See Paragraph 2.5.2 for the deployment order chain of command.)
At the tactical level, organic HSS capabilities and deployable HSS units support activated forces, such as the MEF and the surface action group. Depending on the size of the operation and the estimate of casualties, the size of HSS units can range from an EMF to a fully manned, 12-OR hospital ship.
2.5.1 Health Service Support Unit Relationship with Host Command
The relationship between the HSS unit and the host command is critical to the smooth functioning of the expeditionary HSS unit in an operational environment. To avoid misunderstandings between the supporting expeditionary unit and the supported or host activity, roles and responsibilities must be clearly understood. OPNAVINST 5440.75 (series), Administration, Operation, and Logistic Support of T-AH 19 MERCY Class Hospital Ships, identifies the responsibilities of the hospital ship Master or senior civilian OIC in comparison with the MTF CO/OIC.
Equally important to the smooth functioning of the expeditionary HSS units is their inclusion in the planning process and dissemination of important information to supporting HSS units. In addition to a predeployment briefing, the CO/OIC of the supporting HSS unit must be read in to mission planning by the CJTF, theater commander, or component commander surgeon. At that point, questions can be asked and answered about the locations of other supporting HSS units, communications and security capabilities and considerations, plans and resources for intratheater and intertheater patient movement, and the availability and location of logistics resources for resupply and sustainability.
2.5.2 Deployment Order Chain of Command
The process of filling the supported CCDR’s HSS requirements begins when the commander identifies a requirement that cannot be filled through organic or assigned HSS capability. The request is only for a capability, not for a specific type of unit, or even from a specific Service. The commander sends the request for a capability to the JS. After reviewing the requirement to ensure it is valid, the JS sends the request to the supporting

NWP 4-02
JAN 2008 2-8
CCDR/USJFCOM.2 In some cases, the request may go directly to a Service HQ. Upon receipt, USJFCOM reviews the request to determine which component is best suited to provide the capability. The action is then staffed to the Services for their inputs, which are considered before the final recommendation is made. The JS reviews the inputs and prepares a recommendation to the SecDef, who is the only individual authorized to sign a deployment order (DEPORD). Once the SecDef signs the order, DEPORDs are routed back through the JS to USJFCOM and the components for action.
The naval component commander directed to employ a deployable medical capability in support of military operations must advise and request activation. The USFFC or COMUSPACFLT, when directed, issues a formal activation order to OPNAV N931, and in the case of the hospital ships, to Commander, Military Sealift Command (COMSC) and respective area commander(s). The Chief of Naval Operations (CNO) directs the CHBUMED through OPNAV, Chief of Naval Personnel (CHNAVPERS); Commander, Naval Supply Systems Command (COMNAVSUPSYSCOM); Commander, Naval Reserve Force (COMNAVRESFOR); and other supporting commanders to execute activation plans for deployable HSS platforms, such as a hospital ship (a national asset), EMF, or FDPMU.
2.5.3 Operational and Administrative Control
As a general rule, for personnel and most administrative matters, ADCON over a deployable HSS capability prior to deployment belongs to the local or activity commander to which the unit’s personnel are assigned. The sourcing MTF exercises ADCON over active duty personnel assigned to deployable HSS unit mobilization billets, except for FDPMUs, whose personnel are sourced by the regional Navy Environmental and Preventive Medicine Unit (NEPMU). Commander, Naval Surface Reserve Force (COMNAVSURFRESFOR) has ADCON of Selected Reserve (SELRES) personnel assigned to naval HSS units.
Once the unit or personnel assigned to the unit is deployed, the theater’s Navy component commander is responsible for ADCON. An exception is the hospital ship, for which ADCON of the ROS MTF crew and CIVMARs remains with the MSC following activation, while ADCON for the FOS MTF crew remains with BUMED. If the operational commander is other than the CCDR to whom the unit was originally apportioned, unit C2 passes from the CCDR to the new operational commander when it enters the operational theater. COCOM transfers to the chain reporting to the respective unified commander and naval component commander.
OPCON and TACON are exercised at appropriate levels in the FLTCOM chain of command. In the case of a MAGTF, the operational commander would be the TF commander. The component commander exercising OPCON may be any Service component commander. Hospital ships are an exception. Since COMSC and subordinate area commanders have operational task designators, they may continue to be in the operational chain of command for the hospital ships, at the direction of the FLTCOM. (See Figure 2-2 for C2 of expeditionary HSS units, and Figure 2-3 for HSS command relationships.)
__________ 2 Per SecDef Memorandum dated 25 June 2004, Policy Implementation to Establish Commander, USJFCOM (CDRUSJFCOM) as the Primary Joint Force Provider (JFP). CDRUSJFCOM has been directed to assume duties as primary JFP to develop recommended global joint sourcing solutions for forces and capabilities worldwide, with fewer forces sourced by USSOCOM, USSTRATCOM, and USTRANSCOM. USJFCOM monitors commitment, availability, and readiness and supervises deployment and redeployment of such forces and capabilities.

ADMINISTRATIVE CONTROL OPERATIONAL CONTROL
COMBATANT COMMAND
TACTICAL CONTROL HSS
UNIT PRE-DEPLOYMENT
PRE-DEPLOYMENT
PRE-DEPLOYMENT
DEPLOYMENT
PRE-DEPLOYMENT
DEPLOYMENT
PRE-DEPLOYMENT
DEPLOYMENT
T-AH
COMSC – ROS Cadre and CIVMARs BUMED – FOS Crew
COMSC – ROS Cadre and CIVMARs BUMED – FOS Crew
COMSC – ROS Cadre and CIVMARs BUMED – FOS Crew
Unified Commander/ Naval Component Commander/ MSC Area Commander
N/A
Unified Commander/ Naval Component Commander
N/A
Unified Commander/ Naval Component Commander
EMF BUMED/ Sourcing MTF
Naval Component Commander
BUMED/ Sourcing MTF
Task Force Commander/ Component Commander
N/A Unified Commander N/A Unified
Commander
FDPMU NMCPHC/ NEPMU
Naval Component Commander
NMCPHC/ NEPMU
Component Commander N/A Unified
Commander N/A Unified Commander
FST CLASSRON ESG CLASSRON Task Force Commander N/A
Unified Commander/ Naval Component Commander
N/A Task Force Commander
Figure 2-2. Predeployment and Deployment of Health Service Support Units
2-9
JAN
2008
NW
P 4-02

NWP 4-02
JAN 2008 2-10
Figure 2-3. Health Service Support Command Relationships
2.6 COMMAND RELATIONSHIPS AND RESPONSIBILITIES
2.6.1 Joint, Coalition, and Allied Operations
Military medicine is experiencing significant transformation in the joint operations arena. As US joint military operations grow, NEHSS units become capable of deployment in support of another Service force, as in a large-scale Army operation. ADCON remains the responsibility of a Navy component commander, or the MSC in the case of hospital ships. OPCON can be the responsibility of an Army component commander, who may in turn report to an Air Force TF commander. The JTF can be in support of a coalition of forces, as it was in OIF, or a formalized United Nations (UN) operation, as it was in Operation Provide Promise in Sarajevo.
2.6.1.1 Joint Operations
1. Chain of Command. Joint operations are those in which forces of two or more Military Departments operate under a single commander authorized to exercise OPCON. The unified commander should define the mission for the expeditionary HSS unit in the OPLAN or OPORD in combat casualty care, community medicine, preventive medicine, and dentistry. The OPLAN/OPORD should delineate HSS unit supporting

NWP 4-02
2-11 JAN 2008
and supported commands, logistics availability, communications, and transportation capabilities. Joint operations HSS should be coordinated by a JFS who reports directly to the JFC.
2. Joint Operations Health Service Support. Increasing use of NEHSS units, to include hospital ships, in FHA and HCA operations.
3. Joint Operations Mission Planning. In joint operations mission planning, refugee care and HSS should focus on developing infrastructure, not on treating chronic illness in individuals who will not receive follow-on care. In support of health affairs operations, clinical care involves preventive medicine (e.g., in the form of a massive rubella immunization program for children to protect a population at risk). The beneficiary population should be defined in the OPLAN. As joint operations become a component of coalition and allied/UN operations, the unified commander should anticipate and identify the type of patient injuries and illnesses that the HSS mission will be able to treat.
4. Standing Joint Force Headquarters (SJFHQ). SJFHQ-Core Element (CE) provides each geographic CCDR with a trained and equipped, standing joint C2 element specifically organized to accelerate the transition of Service operational HQ to a JTF HQ. SJFHQ-CE personnel provide knowledge of the combatant command HQ as well as expertise in JTF HQ planning and execution processes. They are trained in a joint environment. When appropriately augmented, an SJFHQ-CE can form a small, short-duration JTF HQ.
5. Inplace Capability. The SJFHQ provides each geographic CCDR inplace C2 capability, allowing precrisis planning for focus areas designated by the CCDR based on improved situational awareness and the understanding of adversarial and friendly forces.
There are three primary employment options:
a. The SJFHQ-CE can form the core of a JTF HQ. In this case, the CCDR designates the SJFHQ-CE director or another flag officer as the CJTF and augments the SJFHQ-CE from the combatant command HQ and components as required.
b. The SJFHQ-CE can augment a designated JTF HQ. The SJFHQ-CE (in its entirety or selected portions) can provide additional expertise to an existing JTF HQ, JTF-designated Service component HQ, or other government agency (OGA).
c. The SJFHQ-CE can support the combatant command HQ. In this case, the CCDR is the JFC. The SJFHQ-CE can remain part of the combatant command staff or serve as the forward element of the joint force HQ.
2.6.1.2 Coalition and Allied Operations
1. NATO. In coalition operations, the United States functions in alliance with other nations and established groups of nations, such as NATO, which follows standardization agreements that specify HSS standards and procedures.
2. Non-NATO nations. In coalition operations that do not involve NATO, each national contingent is responsible for HSS except for small national force elements with limited or no organic HSS capability. They are provided HSS by the area coalition commander.
3. Mission guidelines. When other nations are involved in the military effort with the United States, a clear definition of the mission is crucial. Coalition operations affect the mission for which the expeditionary HSS unit is serving. Some operations place less emphasis on combat casualty care and more on community medicine and support of refugee populations. The beneficiary population also must be well-defined so that the HSS unit can anticipate the needs of patient diversity.

NWP 4-02
JAN 2008 2-12
4. Additional HSS. Multinational operations can require a higher capability of care than expected of the expeditionary HSS unit when nations lack the necessary capability of care for their forces in theater and at home. The level of practice establishes the requirements for additional personnel, equipment, and supplies that may not be part of the MTF’s activity manpower document (AMD) or authorized medical allowance list (AMAL) and authorized dental allowance list (ADAL). In dentistry, for instance, there are an increased number of emergencies secondary to prior inadequate dental care and poor dental hygiene.
5. HSS liaison planning. Component, joint, coalition, and individual national HQ should establish liaison early in mission planning to include a network for solving repatriation issues. US forces move patients from theater treatment facilities based on the health of the patient and theater evacuation policy. In coalition operations, other countries may not evacuate military personnel from treatment facilities as rapidly as the United States and may spend more time in continuing care and effecting repatriation.
6. Other planning issues. Treating, credentialing, and privileging of HSS personnel and medical support/trauma care for coalition forces should be addressed in coalition JTF planning documents. There are currently no coalition HSS units, although the US treats other countries’ personnel.
2.6.1.3 Language
Methods for overcoming language and communication barriers should be considered when deploying to non-English speaking countries. New language translation technology allows programmed YES/NO responses to questions asked when treating non-English-speaking patients. HSS planners, TF commander’s staff members, and a TF surgeon’s staff should anticipate these communication barriers and develop a pool of translators within the HSS unit such as other patients, area food service workers, JTF personnel, contract personnel, English speakers from the patient’s command, foreign language speakers from the HSS unit’s organic military personnel, and the theater component commander’s capabilities. In addition, HSS personnel can develop flash cards with standard questions and answers.
2.6.2 Unified Command Surgeon
The unified commander has directive authority for logistics and administrative support of component forces, including HSS of the unified command. To ensure joint coordination and review of HSS plans and operations, a unified command surgeon, such as the USCENTCOM surgeon or the JFC surgeon, is designated for each unified command. Additional personnel may be provided by components as tasked in OPLANs, OPORDs, standard operating procedures (SOPs), or as otherwise directed. Assigned personnel are responsible to the command surgeon, who reports to the unified commander. The unified command surgeon and dental officer coordinate planning for HSS through liaison with each component’s command surgeon and dental officer to ensure that the command’s requirements are met without duplication. The unified command surgeon also supervises the command’s Joint/Theater Patient Movement Requirements Center (J/TPMRC) and the Joint Blood Program Office (JBPO) activities.
Liaison is established among the unified command surgeon and each component, subordinate unified, and TF surgeon. The duties of the unified command surgeon are to advise the unified commander and to plan and coordinate the command’s overall HSS. The unified command surgeon’s responsibilities are delineated in JP 4-02, Health Service Support. In general, each Service component command is responsible for the HSS of its own personnel, the operation and support of joint HSS facilities, and the provision of specialized support, such as seaborne MEDEVAC by the Navy and strategic aeromedical evacuation (AE) by USTRANSCOM.
2.6.3 Joint Task Force Surgeon
A JTF is constituted and designated either by the SecDef, a theater CCDR, or an existing JTF commander. The SMDR of the JTF is the JTF surgeon who reports directly as personal staff and principal HSS adviser to the CJTF for HSS and the employment of HSS forces.

NWP 4-02
2-13 JAN 2008
2.6.3.1 Joint Task Force Surgeon Responsibilities
Appendix F contains a list of the JTF surgeon’s specific responsibilities. Responsibilities of the JTF surgeon’s office include the following HSS functional areas:
1. Force health protection
2. Medical plans, operations, and intelligence
3. HSS and veterinary services
4. HSS logistics, blood program, and J-4 medical coordination
5. Medical information management
6. Patient movement.
2.6.3.2 Joint Task Force Surgeon Office Organization
Even though a liaison officer is not required, one is customarily assigned to the JTF staff. The JTF surgeon’s office can be organized in different ways. (See Figure 2-4 for an illustration of a typical organization.)
Figure 2-4. Notional Joint Task Force Surgeon’s Office Organization

NWP 4-02
JAN 2008 2-14
2.6.4 Component Elements
The Navy component commander is responsible for identifying required Navy capabilities to support the unified command’s mission. Ships, personnel, and funding for Navy commands are furnished by the CNO from available resources. Once an initiating directive is issued, ships of the fleet are organized into a TF, sized, and composed to accomplish an assigned mission. A TF is composed of task groups oriented toward functional aspects of a particular mission and individual elements from a TYCOM. The operational chain of command in the joint operation is from the JTF commander to the combatant TF commander; to the task group commander; to the task unit commander; and to the task element commander. The provision of personnel, facilities, and supplies for administrative and logistic support, including HSS, is the responsibility of each service component, except for requirements specific to an assigned mission.
2.6.5 Health Service Support Staff Officers
HSS staff officers may be assigned to the operational commander to advise on the command’s HSS administration and operation. Most operational staffs have HSS officers assigned. In cases where no billet exists on an operational staff, a ship’s company SMO may be assigned the responsibility on an additional duty (ADDU) basis. The officers are responsible for advising the commander and other members of the staff on HSS matters. They monitor the health of the command, exercise technical supervision over its HSS care delivery and supply functions, integrate and coordinate the command’s health care efforts with higher and subordinate commands, and prepare the HSS portions of operation and logistic plans, orders, and instructions. The HSS staff officers’ duties and responsibilities are delineated in NAVMED P-117, Manual of the Medical Department (MANMED), in operational instructions, and in OPLANs. HSS officers must continuously participate in staff activities and opportunities to be effective, contributing members of the commander’s staff.
As one of their duties, HSS staff officers inspect health care facilities, supplies, and personnel. The dual purpose of inspections is to ascertain the readiness posture of subordinate elements for HSS and to assist in bringing them to an optimal condition. Inspections should be oriented to the command’s operational mission. Readiness assistance visits may be made at the request of a ship’s CO or by higher command to advise and assist the ship’s HSS personnel. Regular visits may also be arranged to provide in-service training for HSS personnel on ships without a medical officer assigned. Responsibilities for conducting such inspections and readiness assistance visits will vary in accordance with the organizational chain of command.
2.6.6 Task Force Surgeon
The organization and assignment of elements to a TF are predicated on the assigned operational mission. Once the TF mission and elements are known, the TF surgeon and dental officer will determine the availability and readiness state of HSS resources. Effective coordination through command channels will eliminate duplication, correct deficiencies, and provide HSS required by the TF mission. The commander coordinates effective use of HSS resources through the staff surgeon and dental officer.
2.6.7 Expeditionary Strike Group Surgeon
The ESG surgeon is the designated medical officer on the ESG staff and represents the commander in all matters pertaining to the HSS required for a projected amphibious operation. In consultation with the commander, landing force (CLF) surgeon, the ESG surgeon provides the OPLAN/OPORD medical section (Annex Q, Medical Services) to the ESG. The duties and responsibilities of the ESG surgeon are found in Appendix F.
2.6.8 Landing Force Surgeon
The LF includes aviation and ground elements assigned to an amphibious assault, including combat, combat service, and CSS forces. The LF HSS plans are based upon and support the plans and policies of the CLF and the Navy component command surgeon. They must also complement the HSS plans of the CESG. The LF surgeon is usually identified as the Marine expeditionary unit (MEU) or MEF surgeon, as appropriate for the MAGTF level. The specific duties and responsibilities of the LF surgeon are found in Appendix F.

NWP 4-02
2-15 JAN 2008
2.6.9 Expeditionary Health Service Support Unit Commanders
Expeditionary HSS unit commanders must be aware of their reporting chains of command as well as their responsibilities as unit COs/OICs. Expeditionary HSS units rely on the operational commander for support and security functions as discussed in Chapter 3.
When not assigned to the augmenting expeditionary unit, the HSS CO/OIC is assigned to the shore-based supporting HSS facility, such as the National Naval Medical Center (NNMC) or NEPMU, and reports to the commander or CO of the respective command/activity. COs and OICs of deploying HSS units are formally designated by CHNAVPERS ADDU or permanent change of station orders. Upon full or partial activation of the deploying unit, the CO/OIC reports to the unit and assumes command responsibility for its operation and maintenance. In the case of a hospital ship or EMF, this includes ensuring the granting of clinical privileges for all assigned health care providers based on the interfacility transfer form.
For further information on privileging, refer to BUMEDINST 6320.66 (series), Credentials Review and Privileging Program.
The HSS CO/OIC is responsible for the assignment of military personnel to watch stations, as required, and for the care and cleanliness of all spaces assigned to and occupied by unit personnel. Prior to departure for theater, the unit CO/OIC must be briefed on its environmental threats by medical intelligence and preventive medicine personnel, and must be thoroughly familiar with Annex Q of the OPLAN. Upon chopping (reporting) into theater, the HSS CO/OIC should report the unit under OPCON of the appropriate authority as designated in the DEPORD.
As a rule, the CO or OIC of the expeditionary HSS unit will report to an operational commander, such as the TF commander, in the case of an EMF in a combined Navy–Marine Corps operation or FST on a CRTS, to the regional FLTCOM in the FLTCOM chain (hospital ship), or to a component commander FDPMU. HSS units that are organic to MEFs report to company or battalion commanders in accordance with the chain of command. Deployed EMFs assigned to MEFs for additional support fall under MEF OPCON and TACON. In some instances, the HSS unit is a separate unit of the operating forces of the Navy with its own UIC and a permanently assigned OIC or, when activated, a CO of the hospital ships, EMFs, MTFs, and FSTs.
2.7 NAVAL MEDICAL ORGANIZATIONAL RELATIONSHIPS AND RESPONSIBILITIES
2.7.1 Office of the Chief of Naval Operations
2.7.1.1 Surgeon General of the Navy
The SG implements the CNO’s responsibilities for providing centralized, coordinated policy development, guidance, and professional advice on health care programs for the Navy; oversees the systems for providing health care services to all beneficiaries in wartime and peacetime; and acquires sufficient resources to provide these services. The Surgeon General of the Navy (N093) serves ADDU as CHBUMED. The following identifies specific expeditionary HSS–related functions:
1. Responsible for the health of Navy and Marine Corps active duty members, ensuring they are physically and mentally ready to carry out their worldwide mission
2. Maintains the capability to meet total force HSS requirements for the Navy and Marine Corps in support of their worldwide mission
3. Reviews and appraises naval HSS capabilities for health care delivery and ensures a timely response to operational contingencies
4. Assesses and promotes maximum readiness in support of established warfare plans and programs
5. Coordinates the Navy’s DEPMEDS (EMFs, FDPMUs, hospital ships).

NWP 4-02
JAN 2008 2-16
2.7.1.2 Dental Matters
The Deputy Chief for Health Care Operations Support serves as the adviser to the SG on all HSS operations support to the Navy. This function is provided to the Commandant of the Marine Corps (CMC) by the Dental Officer for the Marine Corps, who is resident within the offices of the TMO. The Chief, Navy Dental Corps, is the adviser to the SG on all dental officer career matters, to include accession, retention, promotion, and postgraduate education.
2.7.1.3 Assistant for Marine Corps Medical Matters/Medical Officer of the Marine Corps
OPNAV N093M advises and assists the SG in all aspects of Marine Corps medical support. This is an ADDU assignment for the TMO. In the latter capacity, the medical officer advises the CMC and HQ staff agencies on all HSS matters. In addition to serving as liaison between CMC and N093, the medical officer performs the following functions:
1. Serves as the functional expert in working with appropriate Marine Corps HQ staff agencies to determine requirements for, and make recommendations about, HSS to the Marine Corps
2. Initiates actions through HQ staff agencies to obtain HSS personnel and materiel to meet Marine Corps requirements
3. Assists staff agencies in formulating landing force and field HSS doctrine, procedures, and programs.
2.7.1.4 Supply, Ordnance and Logistics Operations Division
The Director, Supply, Ordnance and Logistics Operations Division (OPNAV N41) is the resource sponsor for medical readiness platforms, providing overall guidance and direction regarding the POM, and funding initial outfitting and maintenance costs of supplies and equipment for NEHSS units prior to activation/deployment.
The OPNAV N41 program performs the following functions:
1. Coordinates and implements N093 participation for resource requirements in the planning, programming, and budgeting system
2. Develops balanced HSS programs within available resources
3. Evaluates the impact of changing demands on the operating forces and recommends program changes for health care requirements
4. Conducts special projects, studies, and analyses regarding the operational aspects of health care policy issues and develops the recommended naval medical position
5. Develops and reviews the effectiveness of health care requirements and initiates development of operational alternatives
6. Integrates fleet health care support operations with appropriate warfare and platform sponsors
7. Monitors, appraises, and provides guidance for DEPMEDS, including EMFs and hospital ships, to ensure that all necessary requirements, including manpower, military construction, training, prepositioning, and other support, have been provided
8. Provides logistic support requirements for EMFs, hospital ships, war reserve HSS materiel requirements, and other mobilization materiel support requirements

NWP 4-02
2-17 JAN 2008
2.7.1.5 Director, Medical Resources, Plans and Policy Division
The Director, Medical Resources, Plans and Policy Division (OPNAV N931) performs the following functions:
1. Develops and evaluates plans and policy for HSS of general war and contingency operations
2. Develops and coordinates Navy and Marine Corps operational support requirements
3. Develops and evaluates policy in naval HSS research and development (R&D) initiatives consistent with operational support requirements
4. Develops and evaluates plans and policy in oversight and coordination of all aspects of DEPMEDS.
Expeditionary HSS performs the following related functions:
1. Develops, appraises, and reviews HSS doctrine, contingency HSS policy and requirements, HSS capabilities, adequacy of HSS, and guidance for HSAP
2. Directs and oversees NAVMED’s operational involvement in CBRN warfare defense matters
3. Directs and monitors medical and dental participation in readiness exercises
4. Monitors and reviews intelligence estimates for HSS implications
5. Develops, appraises, and reviews medical support of OPLANs and contingency response plans, to assess readiness and adequacy of supportability of HSS requirements to operational commanders
6. Reviews and evaluates requirements and directs concept development for theater HSS capabilities and patient evacuation
7. Establishes policy for time-phased total force health care manpower requirements
8. Conducts and reviews studies and analyses of Navy and Marine Corps casualty rates (battle injury (BI) and disease and nonbattle injury (DNBI))
9. Reviews and validates all HSS wartime mobilization requirements, including manning documents and Navy training plans (NTPs)/Navy training system plans (NTSPs).
2.7.1.6 United States Fleet Forces Command
The Commander, US Fleet Forces Command (COMUSFLTFORCOM) performs the following missions, functions, and tasks:
1. Authorities. CNO delegates to COMUSFLTFORCOM to:
a. Organize, man, train, maintain, and equip assigned Navy forces.
b. Provide BSO authority and responsibility for assigned forces, military and civilian personnel, infrastructure, and budget.
c. Generate and communicate Navy global force management solutions concerning general-purpose forces, ad hoc forces, and individual augments to Commander, USJFCOM.

NWP 4-02
JAN 2008 2-18
2. These authorities do not authorize the transfer of administrative control of forces under Commander, US Pacific Fleet (COMUSPACFLT), nor do they limit the execution of BSO authority for forces, military and civilian personnel, infrastructure, or budget of COMUSPACFLT.
3. Missions. COMUSFLTFORCOM has the following missions;
a. Navy Readiness: COMUSFLTFORCOM will generate ready Navy forces for assignment to CCDRs in response to force requirements and as such will:
(1) In collaboration with COMUSPACFLT, organize, man, train, maintain, and equip Navy forces, develop and submit budgets, and execute readiness and personnel accounts to develop required levels of Fleet readiness.
(2) In consultation with COMUSPACFLT, be the unified voice for Fleet training requirements and policies to generate combat-ready Navy forces per the fleet response plan (FRP) utilizing the fleet training continuum (FTC).
(3) As the Navy component commander to USJFCOM, perform duties as the Navy Global Force Manager and provide USJFCOM with collaboratively developed Navy global force solutions to CCDRs’ request for Navy general-purpose forces, ad hoc forces, and individual augments.
(4) Integrate and consolidate all matters concerning operations, readiness, and training in the development of current and future Navy shore requirements.
(5) Lead the Fleet Readiness Enterprise (FRE) to integrate planning, risk management, and readiness execution across the Warfare Enterprises and provide synchronization between Warfare Enterprises and Enabling Domains. The USFFC Surgeon has established the fleet health domain (FHD) within the FRE. The FHD is organized to drive additional improvements in HSS and maintain operational readiness by working collaboratively with senior operational medicine leaders assigned to CNO-931, BUMED, the Fleet Marine Force (FMF), MSC, USFLTFORCOM, and USPACOM, will ensure that individuals and units are medically ready for deployment according to the functional concepts in NFHP-21.
b. Navy warfighting capability requirements: COMUSFLTFORCOM articulate integrated authoritative Fleet warfighting, readiness, and personnel capability requirements, coordinated with other Navy component commanders, to the CNO and develop transformational concepts for maritime operations.
c. Joint operational and planning support: COMUSFLTFORCOM will provide planning and operational support to assigned and supported CCDRs and will exercise OPCON and/or TACON of forces when assigned in accordance with the orders and directions of the responsible CCDR.
d. Navy antiterrorism/force protection (AT/FP): COMUSFLTFORCOM is the CNO Executive Agent for AT/FP and will establish and implement AT/FP standards and policies for Navy units.
4. Command relationships. COMUSFLTFORCOM has the following command relationships:
a. Service assignments
(1) Echelon II commander under the CNO and reports to the CNO for administrative and service related matters.
(2) The immediate superior-in-command (ISIC) and has ADCON of the following Navy commands and their subordinates: Commander, Naval Air Forces, Atlantic; Commander, Naval Surface Forces, Atlantic; Commander, Submarine Force; Commander, Naval Network Warfare Command; Commander, Navy Expeditionary Combat Command; Commander, US Second Fleet; Commander,

NWP 4-02
2-19 JAN 2008
US Third Fleet (for Fleet training requirements and policies); Commander, Military Sealift Command (for mission areas funded by the Navy Working Capital Fund or uniquely Navy Service related mission areas); President, Board of Inspection and Survey; Commander, Navy Warfare Development Command; Commander, Naval Meteorology and Oceanography Command; Commander, Mid-Atlantic Regional Maintenance Center (RMC) , South Central RMC, and Southeast RMC; Commander, Navy Munitions Command; and Commanding General, Fleet Marine Forces Atlantic.
(3) The ISIC for operational employment of Navy regional commanders within CONUS, and Navy shore installations within CONUS.
b. Joint assignments
(1) Navy component commander to USJFCOM
(2) Supporting Navy commander to Commander, USNORTHCOM
(3) Joint Force Maritime Component Commander North in support of USNORTHCOM
(4) Supporting Navy commander to Commander, USSTRATCOM
5. As the Global Force Manager, the following request for forces (RFF) information provides the process for requesting forces.
a. Overview.
(1) RFF is a request from a CCDR or force provider for units or capabilities to address emergent (unforecasted) requirements within their area of responsibility that cannot be met by the requesting headquarters or its components, or the CCDR’s assigned or allocated forces. An RFF is not the proper vehicle to source exercises, individual requirements, or equipment-only requirements.
(2) HSS capabilities not identified in OPLANs are considered a BUMED capability. These HSS capabilities belong to the Secretary of the Navy (SECNAV). HSS capabilities that belong to the Service and are not allocated to a CCDR are categorized as “unassigned forces” per current DOD Global Force Management (GFM) policy guidance.
b. RFF process. An RFF is required when a CCDR service component requests a Navy HSS capability. The component commander will submit an RFF through his CCDR. The CCDR submits the RFF to the JS. The JS validates requirements and obtains approval from SECDEF/National Command Authority and then sends the RFF to USJFCOM. USJFCOM works with each of the Services to develop a recommended sourcing solution. COMUSFLTFORCOM is the Navy component commander to USJFCOM and the Navy’s GFM. During this RFF process, COMUSFLTFORCOM coordinates with the Chief of Naval Operations (OPNAV) to assess the feasibility of sourcing with unassigned forces. COMUSFLTFORCOM then provides the sourcing solution to USJFCOM. USJFCOM develops and submits a sourcing solution to the JS based on each component’s feasibility to source. The JS recommends the force allocation to SECDEF for approval. Upon approval, the JS issues a Global Force Management Allocation Plan (GFMAP) modification. Based on the GFMAP mod, USJFCOM adds new requirements to the conventional forces annex (Annex A). For unassigned HSS forces, OPNAV will review Annex A and coordinate preparations for deployment with BUMED. USFFC issues deployment orders for assigned forces, OPNAV for unassigned.
c. Request for support process. A Service-to-Service request for support (RFS) is the request from a Navy component for capabilities in support of Navy requirements. These are usually short-duration requests (under 30 days) in support of deployments, operations, or exercises. To request an HSS capability, a Navy component will submit the RFS to USFFC. USFFC will conduct an internal fleet review to

NWP 4-02
JAN 2008 2-20
validate the RFS and identify sourcing solutions. If Fleet support cannot be sourced, then USFFC and/or COMUSPACFLT will forward the request to OPNAV to request sourcing from unassigned (SECNAV) forces. OPNAV will coordinate with BUMED to source the RFS.
2.7.2 Bureau of Medicine and Surgery
2.7.2.1 BUMED Expeditionary HSS Functions
BUMED is an Echelon 2 command responsible for naval medical services and for providing primary and technical support for the BSO-18 treatment facilities. BUMED performs the following functions relating to expeditionary HSS:
1. Ensures the readiness of personnel and materiel under the command of BUMED
2. Provides primary and technical support for delivery of health care to all beneficiaries
3. Maintains cognizance and provides support to the health care and preventive medicine needs of the naval operating forces
4. Ensures implementation of policies and directives for the conduct of occupational health and preventive medicine programs
5. Implements assigned programs to meet Navy and Marine Corps mobilization and contingency plans
6. Ensures cooperation with civil authorities in matters of public health, disasters, and other emergencies
7. Formulates policy and provides oversight of NAVMED homeland security efforts and issues
8. Formulates policy and provides oversight of women’s health programs in support of health care and preventive medicine needs specific to women of the naval operating forces
9. Directs the planning and execution of biomedical research programs required to ensure delivery of state-of-the-art health care, operational medicine, and health support systems for the Navy and Marine Corps.
10. Oversees the Navy’s seven CONUS and OCONUS biomedical research facilities.
2.7.2.2 Navy Medicine Regions
There are four Echelon 3 NAVMED regional offices: NME, NMW, Navy Medicine NCA, and the Navy Medicine Support Command (NMSC). Flag-level officers, as RCs, serve as single points of reference for all NAVMED health care and support services. RCs exercise fiscal oversight of subordinate commands. NME, NMW, and Navy Medicine NCA provide HSS to their regional AOR. NMSC exercises command and fiscal oversight of subordinate commands and ensures effective execution of support services of subordinate commands. RCs report directly to the CHBUMED. Appendix A depicts the BUMED organization.
2.7.3 Navy Medicine Regions
The four NAVMED regional Echelon 3 activities report directly to BUMED. The regions provide support, monitoring, training, and consultation for Navy MTFs in their AOR as described in BUMEDINST 5450.156 (series), Mission, Functions, and Tasks of Naval HealthCare Support Offices. The regions perform the following operational and readiness support functions:
1. Coordinates with BUMED on HSAP and component unit identification codes (CUICs)
2. Coordinates with BUMED on operational training requirements

NWP 4-02
2-21 JAN 2008
3. Coordinates HSS for peacetime taskings, routine deployments, operational exercises, and wartime activation
4. Provides technical assistance, training, and support with readiness personnel initiatives to plans, operations, and medical intelligence (POMI) officers
5. Provides technical assistance and training to activity emergency preparedness officers.
2.7.4 Navy Medicine Support Command
NMSC provides a single point of accountability for all support services within NAVMED to exercise C2 and financial management oversight over subordinate commands assigned and to carry out the necessary course of action to ensure the economical and effective delivery of NAVMED enterprisewide support services. In addition to direct C2, NMSC exercises program executive office oversight of specified executive-level programs. NMSC, through the centralized credentialing and privileging department, provides management of the Naval Reserve component. Through a phased plan, NMSC implements an electronic document management program for credentialing and privileging Navy-wide. NMSC acts as the lead manpower analyst of BSO-18 personnel readiness status and manpower utilization. The Military Medical Support Offices are aligned under TRICARE management activity, with the remaining detachment for mortuary affairs services as a detachment linked to NMSC.
NMSC subordinate commands include:
1. Naval Medical Research Center (NMRC). The NMRC is responsible for R&D activities, including the overall planning, coordination, and oversight of biomedical R&D activities within the Navy. It focuses on the development of biomedical solutions to problems identified by Navy and Marine Corps operating forces. NMRC’s research concentrates on military operational medicine, combat casualty care, and infectious disease. Naval Health Research Center (NHRC) is a subordinate command under NMRC and oversees specialized laboratory facilities and researcher expertise focusing on such areas as undersea medicine, aerospace medicine, environmental and electromagnetic hazards, vaccine development, and dental treatment.
2. Naval Medical Logistics Command (NAVMEDLOGCOM). The NAVMEDLOGCOM or NMLC is an Echelon 4 command reporting to NMSC. NMLC provides and coordinates medical and dental materiel management and logistics to support the operating forces and shore activities. The Marine Corps support function is the responsibility of the Marine Corps Systems Command (MARCORSYSCOM). NMLC acts as the in-service engineering agent and technical support agent for medical equipment logistics support. NMLC is responsible for maintenance and accuracy of AMALs and ADALs. The expeditionary HSS performs the following related functions:
a. Coordinates with other BUMED principals, the BSO, and systems commands to ensure that timely HSS materiel and logistics planning are accomplished to fulfill new or changing requirements in support of projected peacetime and contingency missions, tasks, and functions.
b. Provides contract and equipment acquisition for naval MTFs, and mission-specific commands and detachments.
c. Provides logistics support management for the HSS equipment repair parts program for deployable units.
d. Develops and standardizes equipment maintenance procedures for naval MTFs, and mission-specific commands and detachments.
e. Provides HSS logistics consulting and data analysis support to the operating forces.

NWP 4-02
JAN 2008 2-22
f. Navy Expeditionary Medical Support Command (NEMSC). A subordinate command of NMLC, NEMSC provides logistics management support to the HSS prepositioned war reserve materiel and other war reserve materiel requirements programs.
g. Serves as the program manager for logistics.
h. Coordinates integrated logistics support planning for naval DEPMEDS.
i. Provides health care service acquisition for naval MTFs, and mission-specific commands and detachments.
j. Naval Ophthalmic Support ad Training Activity (NOSTRA). A subordinate command of NMLC, NOSTRA provides fabrication and worldwide delivery of prescription eyewear. NOSTRA is the executive agent (EA) for DOD’s Optical Fabrication Enterprise (automated ordering system). Located in Yorktown, Virgina, NOSTRA produces items such as standard and choice frame eyewear, protective mask inserts, operational frames, and ballistic eyewear inserts.
3. Navy and Marine Corps Public Health Center (NMCPHC). NMCPHC, an Echelon 4 command reporting to NMSC, provides worldwide FHP guidance for the protection of health and prevention of disease, ensuring Navy and Marine Corps readiness through their leadership. The NMCPHC CO is also the designated program manager for FDPMUs and serves as BUMED’s principal adviser for preventive medicine and environmental health. The NMCPHC coordinates and provides centralized support and services to medical activities afloat and ashore in the areas of occupational health; environmental health; preventive medicine; health promotion; population health; deployment health surveillance; chemical, biological, radiological, and environmental defense (CBRED) response; and drug screening. NMCPHC performs the following expeditionary HSS-related functions:
a. Develops, implements, monitors, and evaluates occupational safety and health, preventive medicine, health protection, population health, and deployment medical surveillance. The NMCPHC Epi Data Center provides valuable information regarding DNBI rates and manages the automated system that collects and analyzes the data from the deployment assessments.
b. Provides technical and professional consultation and assistance to activities responsible for identifying, evaluating, monitoring, and correcting health hazards.
c. Navy Entomology Center of Excellence (NECE), Jacksonville, FL, a subordinate command of NMCPHC, ensures US military operational and support forces readiness by providing expert, timely, and technical training and services in vector-borne disease prevention and pest management.
4. Navy Medicine, Manpower, Personnel, Training, and Education Command (NMMPT&E). NMMPT&E, an Echelon 4 command reporting to NMSC, supports NAVMED by preparing and delivering skilled personnel. MPT&E program managers are responsible for approximately 50 NEC code-granting programs, and ensure that curriculum and standards for those programs are current. NMMPT&E oversees the Naval Schools of Health Sciences and the Naval Hospital Corps School. Other expeditionary functions carried out at NMMPT&E subordinate commands include the following:
a. Naval Operational Medical Institute (NOMI). NOMI, an Echelon 5 command reporting to NMMPT&E, comprises components from all warfare areas throughout CONUS. Its goal is to ensure a tactically proficient, combat-credible medical force that provides optimal FHP to the full spectrum of operations. NOMI trains, supports, and sustains operational readiness for naval forces, other Service forces, allies, and selected civilians. The following activities serve as detachments under NOMI:
(1) Naval Expeditionary Medical Training Institute (NEMTI)
(2) Naval Aerospace Medical Institute (NAMI)

NWP 4-02
2-23 JAN 2008
(3) Naval Undersea Medical Institute (NUMI)
(4) Surface Warfare Medicine Institute (SWMI)
(5) Naval Survival Training Institute (NSTI)
(6) Naval Special Operations Medical Institute (NSOMI)
b. NOMI provides the following services:
(1) Provides specialized and operational HSS training to enlisted and officer medical forces in air, surface, ground, and subsurface warfare areas following the tenets of FHP. These medical forces are assigned to organic maneuver elements of the Navy and Marine Corps, or provide the basis of an augmentation surge force resident in our force projection platforms (MTFs).
(2) As a force enabler, provides specialized and operational HSS consultative services and fleet support to military forces worldwide, including key warfare expertise in HSS dispositions affecting the readiness and effectiveness of the joint warfighter. NOMI serves as a frontline facilitator, matching experiential-based HSS solutions with fleet-based problems.
(3) As a warfare center of excellence, supports fleet participation in the naval capabilities development process, and actively participates in concept and doctrine development and experimentation in support of Sea Trial and Joint Experimentation. A key enabler in this process is the NOMLLS.
(4) Manages the Naval Aviation Survival Training Program (NASTP) and enhances operational readiness by identifying issues relating to improving human performance and preventing human factor mishaps.
2.7.5 Navy Medicine East/Navy Medicine West
NEPMUs are organized under NME (NEPMU 2) and NMW (NEPMUs 5 and 6) and provide specialized consultation, advice, and recommendations in occupational health protection, preventive medicine, environmental health, deployment health surveillance, and CBRED response to CCDRs, Navy and Marine Corps component commanders, naval shore activities, and fleet units of the operational forces in the areas assigned. The NEPMUs are aligned under the respective medical centers. Personnel assigned to the NEPMUs are generally assigned to FDPMUs with augmentation from various other commands.
The NEPMUs have the following AORs:
1. NEPMU 2 — East Coast activites, USEUCOM, and USCENTCOM. A detachment will remain in the USEUCOM theater and will be ADDU to Commander, US Naval Forces Europe (COMUSNAVEUR).
2. NEPMU 5 — West Coast activities.
3. NEPMU 6 — USPACOM.
2.8 MILITARY SEALIFT COMMAND
Commander, Military Sealift Command Instruction (COMSCINST) 6000.1 (series), Military Sealift Command Medical Manual, documents the organization, functions, duties, responsibilities, and procedures of the MSC HSS department. BUMED guidance and directives that do not conflict with this guidance are applicable to the MSC.
The MSC HSS department ensures and preserves the operational readiness of MSC personnel afloat and ashore and advises MSC commanders and ships’ Masters how to accomplish the HSS mission in view of the command’s overall mission. The force medical officer advises COMSC on HSS, environmental protection, occupational

NWP 4-02
JAN 2008 2-24
safety, and health matters related to the mission and personnel of the organization; ensures access to and the quality of MSC HSS, environmental protection, and occupational and safety health programs; and provides medical, environmental protection, safety, and occupational health readiness to all MSC activities. The MSC Atlantic and MSC Pacific area commanders are advised by area command medical officers responsible for ensuring quality health care, which is provided to MSC personnel afloat and ashore and for implementing MSC HSS, and environmental and occupational health programs.
Medical services officers (MSOs), physician assistants, registered nurses, or current/former IDCs assigned to MSC ships share the same responsibilities as a Navy IDC. When afloat, they report directly to the ship’s Master. Hospital ships are MSC ships but have different procedures when deployed than other MSC ships. The primary purpose of the CIVMAR crew, when a hospital ship is activated, is to move the augmented MTF to the designated AOR. Although the CO of the MTF coordinates activities with the Master, the CO does not report to the Master.

NWP 4-02
3-1 JAN 2008
CHAPTER 3
Naval Expeditionary Health Service Support Planning Actions and Responsibilities
3.1 INTRODUCTION
Planning and logistics actions are necessary for the success of the expeditionary HSS mission. There are requirements for each phase of expeditionary HSS from predeployment through deactivation and reconstitution.
3.2 PREDEPLOYMENT TOOLS AND CONSIDERATIONS
3.2.1 Joint Operation Planning and Execution System
As defined in JP 4-02, Health Service Support, the Joint Operation Planning and Execution System (JOPES) is the policy, procedures, and automated data processing system used by the joint planning and execution community for developing, coordinating, reviewing, approving, and disseminating joint operation plans. The JOPES process is composed of two types of time-dependent planning, OPLANs and OPORDs.
3.2.1.1 Operation Plans
As the result of a deliberate planning process, OPLANs are developed for contingencies identified in strategic planning documents and are accomplished in prescribed cycles per the joint strategic planning system. They are prepared in response to threats of national interests involving large-scale operations requiring detailed planning. The process of developing, coordinating, reviewing, and approving an OPLAN may take up to a year and is described in CJCSM 3122.03 (series), Joint Operation Planning and Execution System (JOPES), Volume II (Planning Formats and Guidance). Variations of the OPLAN are the CONPLAN and functional plan (FUNCPLAN). The CONPLAN is an abbreviated OPLAN to address contingencies that are important to national security and directed against nonspecific threats. FUNCPLANs are prepared for secondary and tertiary missions, such as HCA operations and NEOs.
3.2.1.2 Operation Orders
OPORDs and campaign plans are developed in response to an imminent crisis. OPORDs follow crisis action planning procedures as delineated in CJCSM 3122.03 (series), Joint Operation Planning and Execution System (JOPES), Volume II (Planning Formats and Guidance).
3.2.2 Time-Phased Force and Deployment Data
Force flow uses time-phased force and deployment data (TPFDD) and is a product of the JOPES process and part of all OPLANs and, on occasion, CONPLANs. It identifies forces, incorporates accurate movement requirements for an OPLAN, and ensures that deployment transportation requirements are within the capabilities defined in Joint Chiefs of Staff guidance. USTRANSCOM administers the process in coordination with the supported commander, supporting commanders, and other Services and agencies.
Force flow is a timeline that identifies units, lift, and cargo flow by location and day into the AOR. The timeline is determined by the theater commander’s requirement for troops and supporting capabilities to arrive in theater. Force flow uses TPFDD to determine transportation feasibility within the commander’s CONOPS. It is not an employment document since TPFDD changes based on the commanders’ changing priorities during execution.

NWP 4-02
JAN 2008 3-2
From an HSS perspective, the theater commander may direct the unified commander to determine when HSS capabilities are required to meet anticipated patient streams and set the combatant commander’s required date (CRD), the date when the HSS asset must be in place and operationally ready to execute the mission.
Because OPLANs and force flows are classified, the strategic timelines are not always known at the tactical unit level unless staff has SIPR access. While the CRD may have a lead time of 30 days or longer (from the time the asset deploys until it is operationally ready in theater), the actual activation or DEPORD may give the HSS unit only a few days to deploy. Therefore, those units must be ready to deploy on short notice. For example, the hospital ships are maintained in a ROS-5 status, meaning that the FOS crew and all necessary supplies to sustain the crew for 30 days or longer have to be onboard and the ship has to be ready to sail within five days. Each expeditionary HSS unit must develop and maintain a timeline that allows it to meet the response time objectives.
The HSS planner and logistician must understand the deployment and employment of each asset required to support the mission and the intricacies involved in building a TPFDD. Each unit must be inserted with the timelines created from the origin of the unit to its POE and port of debarkation (POD) and, finally, to its final destination in synchronization with the commander’s scheme of maneuver. Additionally, based on the medical analysis tool, sustainment requirements must be determined and input into the TPFDD. For HSS, the required inputs include cargo increment numbers for patient movement items (PMIs), Class VIIIA and Class VIIIB supplies, and deratization supplements for DEPMEDS facilities, and include personnel increment numbers for evacuees and losses to ensure that lift is available to support these requirements.
3.2.3 Annex Q, Planning Guidance, and Health Service Support Considerations
The CJCS warning order to the CCDR that defines objectives, missions, constraints, and major forces available begins the HSS planning process. It continues with the commander’s planning guidance to the staff that includes the analysis of the mission, factors to consider, and the course-of-action analysis (COAA). Along with other members of the staff, medical and dental officers prepare systematic, comprehensive estimates of all HSS factors that affect accomplishment of the mission. The staff estimate provides the commander with information to decide the best course of action (COA) for the command and information for inclusion in the operation and logistic support plans. The HSS estimate will form the basis of Annex Q to the OPLAN. Annex Q identifies requirements and provides guidance to subordinate commanders and their HSS planners.
A sample format of medical Annex Q is illustrated in CJCSM 3122.03 (series), Joint Operation Planning and Execution System (JOPES), Volume II (Planning Formats and Guidance). Typical appendixes for Annex Q are as follows:
1. Patient movement
2. Blood and blood products (Class VIIIB)
3. Hospitalization
4. Return to duty
5. HSS logistics (Class VIIIA)
6. Force health protection
7. HSS command, control, and communications
8. Host-nation support
9. HSS sustainability
10. Medical intelligence

NWP 4-02
3-3 JAN 2008
11. HSS planning responsibilities
12. Theater evacuation policy.
HSS-related information is also contained in other OPLAN annexes. For example, telemedicine would be addressed in Annex K (C4 systems), mortuary affairs in Annex D (logistics), and chaplain activities/combat stress intervention in Annex R.
3.3 DEPLOYMENT CYCLE
3.3.1 Predeployment/Deployment Planning
3.3.1.1 HSS Requirements
HSS requirement factors need to be considered when planning any HSS mission. HSS planners need to understand the medical threat environment facing friendly forces as defined by medical intelligence and preventive medicine specialists, and devise measures for countering the threats and conducting effective deployment health surveillance. HSS planners must consider the sustainability requirements for the HSS units that will be deployed and develop a logistics strategy to ensure Class VIIIA and Class VIIIB supplies are provided to meet the needs of expected casualties.
HSS planners must also consider evacuation of forces, including movement from shore-to-ship, ship-to-ship, and ship-to-shore facilities. The responsibilities for patient movement must be included in the supported commander’s CONOPS with alternative arrangements to support the mission. Evacuation may require nonstandard capabilities to move patients. (See Paragraph 4.5 for additional information on patient movement.)
3.3.1.2 Manpower and Training
1. Manpower requirements. The process for determining Navy and Marine Corps expeditionary HSS manpower requirements varies with each wartime platform. Organic HSS requirements for day-to-day operational and wartime missions are based on a fixed population and a predictable workload. In general, Condition III readiness in the required operational capacity/projected operational environment determines these requirements. Conversely, other Navy platforms serve large populations with varying risk and uncertain casualty flows. Since circumstances do not lend themselves to workload models, these platforms rely on subject matter experts to determine manpower quality, such as NOBC, NEC, and quantity requirements. The Marine Corps derives its deployable HSS requirements from another set of processes determined by the task organization and mission-defined unit configurations.
a. Navy deployable military HSS and nonmedical billet requirements for hospital ships, EMFs, CRTSs, aircraft carriers, FDPMUs, and FSTs are identified in the respective activity manpower document. Augmenting personnel assigned to sourcing commands are ordered to a CUIC that identifies their platform assignment by billet sequence code (BSC).
b. The billet requirements may be tailored based on the assigned mission, particularly for humanitarian missions. Marine Corps deployable and nondeployable military billets are identified in tables of organization for the MARDIV, MAW, and MLG.
2. Training requirements.
a. Medical readiness training. The primary medical readiness and skill training requirements for deployable military HSS personnel are specified in Department of Defense Instruction (DODI) 1322.24, Medical Readiness Training. They consist of the following four categories.

NWP 4-02
JAN 2008 3-4
(1) Operational mission briefing. A briefing to HSS personnel during each training cycle on the member’s assigned billet for mobilization or deployment. It should be conducted in a like environment with the type of equipment the member will use.
(2) Initial medical readiness training. Training focused on individual development in weapons qualification or familiarization, CBRN warfare, site security, and firefighting. Initial medical readiness training must be completed within 12 months of arrival at the first permanent duty station.
(3) Sustainment medical readiness training. Training concentrated on continued individual development, maintaining Service-specific training, and emphasizing collective, unit, and platform training. It includes specific military specialty sustainment training and a list of minimum medical specialty sustainment requirements. Sustainment training must be completed during the Service-specific training cycle.
(4) Headquarters mission support training. The courses, training, and exercises that orient and develop HSS personnel assigned to deployable joint and Service component surgeon staffs, such as JTF/JFC, all Service forces, and special operations forces (SOF) component HQ. The training is intended for personnel assigned patient movement, command and control, blood program, HSS logistics, medical intelligence, and medical surveillance functions. It includes specific initial training requirements and sustainment training required to maintain certification to direct or work on a JTF or service component HQ staff.
In addition, HSS personnel with deployment assignments or identified as M+1 augmentees are required to perform a minimum of five days, preferably consecutive, of medical readiness training during each training cycle. The objective is to conduct training in the environment, with the type of equipment the member will use, and with a similar unit with which the member is to deploy or backfill.
The Service member’s commander is responsible for ensuring that all medical readiness training is documented in an individual’s medical readiness training record and in the Centralized Credential Quality Assurance System for health care providers with clinical privileges. This formal certification process is designed to verify that officers and enlisted health care personnel are prepared for operational requirements. The commander is required to ensure that validation of training status, capabilities, and readiness is reported in the Status of Resources and Training System (SORTS) report per NTTP 1-03.3 (series), Status of Resources and Training System Joint Report-Navy (SORTSREPNV).
b. Platform-related training. The various Navy and Marine Corps deployable platforms or systems must also comply with training requirements related to readiness. Commander, Naval Air Forces Instruction (COMNAVAIRFORINST) 3500.20 (series), Aircraft Carrier Training and Readiness Manual, and Commander, Naval Surface Forces Instruction (COMNAVSURFORINST) 3502.1 (series), Surface Force Training Manual, identify by ship, class, safety, and mission area, formal school training requirements that have to be completed to attain prescribed readiness. BUMEDINST 6440.5 (series), Health Services Augmentation Program, establishes specific formal training requirements by deployable platform, such as trauma, critical care, and medical regulating training. In addition, the SG has directed deployable units to obtain combat skills/force protection training in areas such as weapons and land navigation. Finally, personnel in certain billets require selected professional and skill enhancement courses, such as Plans, Operations, and Medical Intelligence, and Medical Department Management Development. These formal courses are necessary to ensure the platform can meet mission objectives.
c. Manpower and training requirements documentation.
(1) Deployable military HSS and nonmedical manpower and training requirements are documented in the DEPMEDS NTSP or, for the Marine Corps, a training system plan in accordance with Secretary

NWP 4-02
3-5 JAN 2008
of the Navy Instruction (SECNAVINST) 5000.2 (series), Implementation and Operation of the Defense Acquisition and the Joint Capabilities Integration and Development System. OPNAVINST 1500.75, Safety Policy and Procedures Conducting High-Risk Training, delineates the requirements, procedures, and format for developing an NTSP as a life-cycle document.
(2) The functions of each BSC are analyzed, and the training and/or formal courses required for officer and enlisted personnel to fulfill those functions are identified and recorded in a billet training profile (BTP). The BTP, an annex to the NTSP, provides the title, quality (rank/rate), designator/NEC, assigned department/division of the billet, and all training required to meet mission objectives. The BTP provides the commander of the sourcing MTF with a detailed approved list of the training that each augmentee must complete to be able to satisfy readiness requirements. Likewise, the BTP identifies and outlines the training that each augmenting member should have achieved to be fully ready.
(3) The NTSP also includes a master equipment list (MEL), which identifies all equipment and systems that deployable MTF HSS and nonmedical personnel operate, use, and maintain. The MEL ensures that training for all equipment/systems is documented by listing the source of training and the number of personnel requiring training on equipment/systems.
3.3.1.3 Readiness
Medical readiness is defined as encompassing the ability to mobilize, deploy, and sustain field medical services and support for any operation requiring the Military Services; maintain and project the continuum of health care resources required to provide for FHP; and operate in conjunction with the beneficiary health care mission. Readiness to provide combat health care is the essence of expeditionary HSS. The readiness mission requires that the following objectives be met:
1. While at home stations, active duty personnel must maintain optimal health for military effectiveness. Prior to deployment, MTFs oversee the health care of personnel under the TRICARE system.
2. Deployable HSS units must be manned by personnel trained in individual military skills and specific medical specialties required for wartime medicine.
3. Deployable HSS units must be continuously staffed at the level required in order to maintain equipment and perform military and medical-specific unit training.
Medical readiness is intended to support and meet the readiness objectives of the operational forces. The fleet readiness program creates an employment-capable and responsive force that is readily available to surge, more efficient to sustain, and able to reconstitute rapidly. Accordingly, the concept of progressive readiness was introduced to provide more ships in an employable status with a majority of forces deployed or surge-ready at any time.
1. Individual Medical Readiness.
a. DOD has instituted a deployment health surveillance program that documents individuals’ medical readiness to deploy. The program has improved occupational and environmental health surveillance for protecting Service members’ health during deployment.
b. Deploying personnel receive individual health assessments that are documented by DD Form 2795, Predeployment Health Assessment. Individual predeployment health assessments include eight questions and further include reviews of required immunizations and other protective medications/measures, personnel protective and medical equipment, deoxyribonucleic acid (DNA) and serum human immuno-deficiency virus (HIV) samples preserved in a DOD serum repository, dental classification, and briefings on deployment-specific health threats and countermeasures.

NWP 4-02
JAN 2008 3-6
c. Redeploying personnel receive individual health assessments that are documented on DD Form 2796, Postdeployment Health Assessment. These assessment forms include questions on health and exposure concerns. HSS personnel review the forms. Positive responses result in a review of deployment health records and appropriate referral for follow-up care.
d. In addition to deploying and redeploying personnel, all active duty members are required to receive individualized annual assessments of health status and current health care needs. Predeployment screening is essential to ensure that gynecological health care issues are addressed with servicewomen, to include the possibility of current pregnancy, and treatment and disposition of any other pertinent health care issues, as well as discussion of birth control options, to include emergency contraception. OPNAVINST 6000.1 (series), Guidelines Concerning Pregnant Servicewomen; and MCO 5000.12 (series), Marine Corps Policy Concerning Pregnancy and Parenthood, provide medical and administrative guidance for the management of pregnant servicewomen. OPNAVINST 6120.3, Preventive Health Assessment, consolidates medical, occupational health, and risk-screening services, medical record review, preventive counseling, and risk communication under the annual assessment. DD Form 2766, Adult Preventive and Chronic Care Flowsheet, is used to document provided services and results of the health assessment.
2. Health Services Augmentation Program.
a. Augmentation is the process by which wartime medical requirements of operating forces and HSS units are filled by active duty personnel to bring units to their full or partial wartime complement. Sourcing commands for augmentation include all MTFs. These activities are responsible for ensuring that apportioned forces are trained, and for providing a full complement of trained HSS personnel for operational assignments.
b. The CUIC process for major platforms is established to facilitate optimum platform manning and assignment of HSS and nonmedical personnel at sourcing commands. When fully implemented, personnel assigned to sourcing commands will be ordered to a CUIC that identifies their platform assignment by its BSC. HSAP units represent personnel augmentation packages providing trained HSS personnel to CRTSs, Marine Corps forces (MARFOR), hospital ships, FDPMUs, and active duty EMFs. CUICs have been assigned to hospital ship MTFs, FSTs, Marine Corps HSS units, and three of the six EMFs. This policy is designed to provide stability and consistency in platform staffing, thereby allowing the platform commander to rely upon it for contingency planning. Attention to the BSC training requirements and the experience of the personnel assigned are critical to ensuring the system works.
Policy and procedures for active duty naval HSS personnel assigned to augment operational platforms during contingency or wartime situations are provided in BUMEDINST 6440.5 (series), Health Services Augmentation Program.
3. Medical Fleet Response Plan (MFRP). The MFRP provides flexibility for Navy Medicine to surge HSAP and task-organize capabilities in timeframes consistent with Service and COCOM policies. Training will be the centerpiece for this effort and will mandate new opportunities to mazimize individual and collective platform readiness. Readiness categories include:
a. Routine deployable. Forward-deployed crisis response forces that are mission capable and ready to deploy within 5 days.
b. Surge ready. Forces designated for the force buildup stage that are ready and capable of mobilizing and deploying within 30 days.
c. Emergency surge. Additional forces designated for further follow-on stages that are ready and capable of deploying within 120 days.

NWP 4-02
3-7 JAN 2008
4. Readiness reporting. Navy HSAP units report their readiness to BUMED per the requirements in BUMEDINST 6440.5 (series), Health Services Augmentation Program. The current report is EMPARTS. All BSO-18 MTFs responsible for supporting operational platforms to manage the readiness status of HSAP will use EMPARTS. The readiness status of HSAP is updated monthly and is available online for authorized users at the EMPARTS website. Readiness is measured in terms of personnel status, training status, and HSAP readiness status.
Note
The only HSS units required to report their readiness via SORTS are the reserve EMFs and deployed active duty EMFs. Hospital ship MTFs provide inputs to the ship’s Master for incorporation into the ship’s SORTS report. (See Appendix C for additional information on SORTS.)
5. Medical Reserve Utilization Program (MEDRUP). Navy Medicine implemented the MEDRUP in November 2000 to ensure that HSS SELRES personnel can support operational requirements. Each SELRES continues training in a mobilization billet in a Naval Reserve HSS unit in order to be ready to support active HSS units when recalled. Under MEDRUP, the SG has OPCON of medical reserve units to be closely integrated into activities of the HSS active units. The CO of a reserve unit reports to the active HSS command that is held accountable for its support to naval HSS. Annual SELRES training is directed by the reserve unit CO to fulfill a requirement of the active HSS command.
The Medical Reserve Utilization Program Management Information System (MEDRUPMIS) tracks requirements for individual SELRES training requirements. Each gaining command or not mission capable command has a designated operational support officer who is responsible for establishing training and readiness metrics under MEDRUP. COMNAVSURFRESFOR oversees the mobilization of SELRES personnel and other administrative and training requirements during this phase. BUMED advises the sourcing MTF and OPNAV of administrative and training requirements and assists as requested by COMNAVSURFRESFOR.
3.3.2 Activation
3.3.2.1 Activation Process
Activation begins with an order to deploy, which can be released in several ways, such as a request for forces (RFF), DEPORD, execution order (EXORD), or the employment of an OPLAN. The release of an order to deploy stimulates the JOPES TPFDD process, which then initiates the activation of a unit, force, or capability. The activation requires units to mobilize and prepare to meet the schedule’s earliest or latest arrival date.
The CCDR to whom the expeditionary HSS is apportioned either releases an RFF through the appropriate chain of command or employs an OPLAN, which stimulates the TPFDD process. The TPFDD directs the supporting commands to issue warning/alert orders, DEPORDs, and/or EXORDs to deploy a unit or force into a theater of operations. These orders are released in message format and initiate the activation of a unit, force, or capability. Concurrently, several other messages are released to identify supporting and supported commanders, rules of engagement (ROE), FHP, unit CONOPS, and CCDR guidance.
MTFs, under the cognizance of BUMED BSO-18, use the activation process to ready affected units, mobilize clinical and nonclinical HSS personnel, and transition them to the operational platform they are intended to support. Upon receipt of the supported CCDR’s orders, OPNAV N931 tasks BUMED M3F with a message to activate and deploy the HSS capability to support the requirements of the CCDR. If the order involves a capability for the Marine Corps, the surgeon’s office Headquarters, Marine Corps (HQMC) or Marine Corps component commander will request HSS unit support from OPNAV N931, who then tasks BUMED M3F to activate HSS capabilities designated for Marine Corps units. The MTF sourcing command ensures that personnel are prepared to deploy to the theater of operations. This includes administrative tasks such as obtaining uniforms and dog tags, updating medical readiness status, placing legal and financial affairs in order, and receiving theater briefings.

NWP 4-02
JAN 2008 3-8
A mobilization/predeployment checklist and predeployment health assessment are completed for each individual. Personnel substitutions for HSS, humanitarian, or legal circumstances can be made during this phase. However, the operational forces expect the substituted person to have the requisite skill sets and expect training to be conducted for those personnel who may not possess the required operational platform skills or training. There is a potential for specialized clinical staff, who may require additional operational training prior to deployment.
The unit COs, executive officers, and/or OICs should be aware of administrative and training requirements. They should ensure that a plan is developed prior to activation and continued during the planning/predeployment phase. Once activated, the unit CO and executive staff should establish a clear understanding of the chain of command and command relationships/C2 as they relate to unit operations, the deployment process, and the theater of operations.
3.3.2.2 Activation Plans
Once the MTF receives the order to activate a capability or unit, HSS units will initiate and implement their mobilization and deployment plans. Each unit’s plan for activation or mobilization is unique, as there are different factors that are involved in moving the operational HSS unit or capability to the theater of operations. In the case of the hospital ship, a 5-day activation and mobilization plan delineates a specific timeline to get the ship underway within five days. For EMFs, a sequence of events must occur to move prepackaged materiel and personnel to the theater of operations.
Detailed procedures for activation of hospital ships are provided in COMSCINST 5400.8 (series), Consolidated Plan for the Activation and Deactivation of T-AH 19 Mercy Class Hospital Ships; and NTTP 4-02.6, Hospital Ships, and for EMFs in NTTP 4-02.4, Expeditionary Medical Facilities.
3.3.2.3 Activation Responsibilities
1. Principal activation-related responsibilities are summarized below:
a. USFFC. Release activation orders to activate the hospital ship. All other fleet capabilities receive alerts, warnings, or DEPORDS.
b. OPNAV N931. Initiate the activation order to BUMED to mobilize and deploy BSO-18 forces to support their assigned operational platforms.
c. BUMED. Activate requisite MTF clinical and nonclinical military personnel assigned to specific operational platforms to mobilize and prepare to deploy to the platform per the supporting or supported CCDR’s DEPORD. Monitor personnel shortfalls and initiate action to resolve them.
d. Sourcing MTFs. Activate a Health Services Augmentation Program Unit (HSAPU). Screen and indoctrinate personnel prior to movement to embarkation site. Provide activation and travel orders and privileging information on all health care providers. Inform BUMED and the cognizant health service support (HSO) of any personnel shortfalls.
e. CO/OIC. Direct unit activation. Monitor and report the status of activation. Ensure departmental activation checklists are completed. Identify requirements for mission-unique HSS equipment and personnel.
2. The activation of a unit, force, or capability alerts the following agencies:
a. NAVSUPSYSCOM. Provide teams when requested by the activated unit to assist supply department functions. In coordination with the Defense Logistics Agency (DLA), under the cognizance of Defense Supply Center Philadelphia (DSCP), monitor prime vendor (PV) contract support for activation and identify alternative sources in order to mitigate materiel shortfalls. Support load-out through the supporting fleet and industrial supply center (FISC) and small purchase activity.

NWP 4-02
3-9 JAN 2008
b. DSCP. Activate medical PV contracts, identify shortfalls, and expedite materiel procurement as necessary. Forward requisitions to sourcing activity within 24 hours and provide daily report to ship or unit on requisition status.
c. NMLC. As required or requested by the ship or DSCP, NMLC resolves HSS logistics issues; expedites procurement of medical equipment and supplies; and provides technical guidance, support services, and assistance with HSS equipment and materiel issues.
d. Navy Medical Region. Assists BUMED in resolving personnel shortfalls. Ensures the sourcing or supporting MTF establishes a HSAPU.
3.3.3 Deployment/Operations
The deployment/operations phase begins when personnel and materiel begin movement from the sourcing MTFs for active duty, predeployment mobilization site for reservists, or prepositioning site for materiel. The deployment phase begins after the activation phase and overlaps it. It ends when materiel and personnel arrive in the operational theater. The theater commander is responsible for several tasks during the deployment phase. In addition to sourcing transportation from the mobilization-staging site, responsibilities also include transporting personnel and materiel from the POD in theater to the assembly site, and coordinating ship offloading of materiel. The theater commander also must ensure the availability of petroleum, oil, and lubricants (POL), water, and waste disposal at the site prior to arrival of any shore-based HSS units. The HSS planner/logistician must ensure that the theater commander knows the daily requirements of each incoming capability in these areas so that the theater commander can adequately support them.
3.3.3.1 Time-Phased Force and Deployment List
The TF commander and the OPLANs, the time-phased force and deployment list (TPFDL), are the critical documents to use during this phase. The TPFDL details the movement of personnel and materiel from prepositioning sites to the theater, contains required and updated delivery dates for in-theater arrivals, and identifies POEs and PODs.
After the FLTCOM transmits the activation order, the Navy component commander will send a message to USTRANSCOM providing POCs for personnel and supplies being air-moved. The HQ Air Mobility Command (AMC) requirements cell contacts the POCs for final verification of the TPFDL’s unit type code with a 7-day window in which the aerial POE departure date falls. The commander exercising OPCON will establish theater aerial ports of debarkation (APODs) and seaports of debarkation (SPODs) with the Navy Material Transportation Office (NAVMTO), Norfolk, via message, for the deploying unit to ensure expeditious flow of resupply materiel and mail.
3.3.3.2 Operational Responsibilities
Once activated, the expeditionary HSS unit deploys to the AOR per the theater OPLAN. Movement of the MTF staff and associated logistic costs are the responsibility of the cognizant HSO and BUMED. The ongoing costs for sustainment are the responsibility of the Navy component commander. Operational commanders have the primary responsibility for exercising OPCON over a NEHSS unit through one of their component commanders. In addition, other responsibilities are imposed upon the operational command to which the unit is assigned. While some units such as hospital ships are self-sufficient, additional requirements are necessary. The operational commander’s responsibilities are listed below:
1. Selection of the operational site (stationing)
2. Coordination for any in-port support required, such as pierage and support for pilots
3. Transportation of materiel and personnel from the POD to the unit (not applicable to hospital ship or FST personnel if embarked on a CRTS prior to deployment)

NWP 4-02
JAN 2008 3-10
4. External security in the stationing area
5. Waste disposal, including hazardous materials and biomedical wastes
6. Surface and AE transportation services
7. Replacement of PMIs used in evacuation of patients
8. Provision of POL
9. Resupply
10. Contracting support
11. Security for all categories of detainees
12. Mortuary affairs, graves registration support, and decedent immigration status and customs clearance
13. Morale, welfare, and recreation services, normally provided by the Navy component commander’s organization
14. Personnel services detachment support, normally provided by the Navy personnel support activity
15. Disbursing services above that provided by the units’ disbursing office
16. Chemical, biological, and radiological (CBR) decontamination support
17. Establishment of an OPTAR during the unit’s activation/mobilization phase
18. Funding costs of transporting personnel and materiel from the sourcing MTF and prepositioned site to the operational site.
3.3.3.3 Operational Forces Medical Liaison Services
Fixed, shore-based MTFs are required per BUMEDINST 6440.8 (series), Operational Forces Medical Liaison Services, to establish and maintain an operational forces medical liaison service (OFMLS) to serve as a single POC and interface between the MTF and medical department representatives (MDRs) of the operational forces. The head of the OFMLS is a special assistant to the commander, CO, or OIC of the MTF. OFMLS functions that support operational forces include:
1. Providing a 24-hour POC between the MTF and operational MDRs
2. Providing follow-up information to operational MDRs on patients received from their unit for evaluation and/or treatment, such as referrals, consults, admissions, dispositions, and limited duty boards
3. Notifying operational units of any significant change in the status or movement of patients received
4. Maintaining liaison with medical holding companies and reporting the status of patients to operational units
5. Coordinating emergency medical logistic support
6. Coordinating emergency environmental health support.

NWP 4-02
3-11 JAN 2008
3.3.3.4 Phasing Support Ashore
During the movement phase of amphibious operations, the ESG has overall responsibility for HSS services to embarked personnel. The LF HSS personnel aboard ESG ships augment HSS departments by providing care to embarked personnel using the ship’s HSS facilities and supplies. Class VIIIA equipment will not be used aboard ship unless authorized by the MAGTF commander in response to an emergency.
During the assault phase, HSS ashore is limited to the capabilities organic to combat units. When the tactical situation permits, BASs are established and evacuation stations expanded and staffed by the supporting medical battalion. When established with the landing force support party (LFSP), the medical detachment of a combat logistics battalion (CLB) provides the HSS for the BESs with the primary role of evacuating assault force casualties to the CRTSs.
Following the landing of supporting BESs, the expansion of HSS facilities ashore begins, and BASs are relieved to conduct their missions in support of parent battalions. During follow-on assault, HSS shifts its posture to achieve shore-based health care consistent with expected combat intensity and duration, independent of seabased capabilities. If a sustained land campaign is envisioned, additional HSS is provided by EMFs and/or hospital ships.
3.3.3.5 Preventive Medicine
DODI 6490.3, Deployment Health, provides additional guidance for deployment preventive measures. Preventive medicine tasks during deployment include:
1. Disseminating militarily significant preventive medicine information to commanders and HSS units in theater
2. Initiating/completing ongoing environmental health site assessments at stationary base camps and other permanent or semipermanent basing locations
3. Conducting occupational and environmental health surveillance by sampling air, water, soil, and/or other environmental media necessary to assess the potential health significance of complete and/or potentially complete exposure pathways; monitoring disease surveillance data and field sanitation procedures; and providing disease vector surveillance and pest management services
4. Maintaining environmental health and pest control equipment
5. Conducting weekly disease and injury surveillance.
3.3.3.6 Health Service Logistic Support
1. Naval Supply System Overview. Naval supply operations are the functional area of naval logistics that equips and sustains operating forces from predeployment through combat operations and subsequent redeployment. Naval supply operations consist of functions necessary to receive, store, issue, and resupply materiel for naval operations. Supply functions include such varying actions as design, procurement, receipt, inventory control and issuance of end items, repairables, and consumable materiel, including eventual retrograde and disposal.
2. Health Service Logistic Support (HSLS), a naval supply management concept. Operating forces’ HSS facilities maintain selected stocks of HSS supplies, referred to as Class VIII, in accordance with AMALs and ADALs. These allowance lists are prepared by NMLC and are tailored to the HSS mission and capabilities of each unit. Replenishment materiel is requisitioned from the supply system via designated FISCs, overseas support bases, or CLF units. In urgent classes, afloat units may request Class VIII transfer from other ships.

NWP 4-02
JAN 2008 3-12
Class VIII medical supplies are described as:
a. Definition. Class VIII encompasses HSS supplies and equipment. This includes medicines, drugs, major and minor pieces of equipment, and human blood and blood products.
b. Subclasses. Class VIII subclasses are A–HSS materiel, and B–blood and blood products. Class VIIIB items are administered by the military blood program office and unified command joint blood program offices.
c. General Characteristics. HSS supplies and equipment are associated with the safety of life issues. Safety, reliability, and sterility standards are general considerations that affect Class VIII items. These strict standards and their associated mandatory quality assurance provisions often cause Class VIII items to cost much more than similar nonmedical items.
For additional information on medical logistics, refer to NTTP 4-02.1, Medical Logistics.
3. HSLS Business Practices. As a result of the change from warehouse stocked materiel to just-in-time delivery to the MTFs, means of providing materiel with insufficient commercial demand to support large-scale military operations required development of alternative solutions to meet these requirements.
a. Fleet Prime Vendor. The fleet PV is contracted to handle day-to-day operation of just-in-time procurement.
b. Prime Vendor War Readiness Materiel. The current generation contracts require the PV to be capable of meeting contingency support. The Services identify the coverage required by the PVs to meet deploying forces’ requirements.
c. Vendor Managed Inventory (VMI). These items are determined to have insufficient commercial requirement to support operational requirements and may have contracts negotiated with a contractor, either the manufacturer or a distributor. The government purchases an inventory, and the vendor holds and manages the inventory, rotating newly produced products into the inventory, and shipping to meet commercial requirements from the inventory, reducing the government’s cost due to shelf-life expiration.
d. Corporate Exigency Contracts (CEC). These contracts are an attempt to minimize the Services’ maintenance costs while providing rapid access to materiel. The government and corporations within a given manufacturing field enter into contracts where the contractors are required to deliver materiel based upon a time-phased requirement, at a negotiated price.
e. Shelf Life Extension Program. This program is an agreement between DOD and the Food and Drug Administration (FDA) where items for which the Services maintain large inventories of materiel can be tested to extend shelf life beyond the original manufacturer’s label.
3.3.3.7 Deployment Reports
Deployment report types are typically specified by the FLTCOM’s DEPORD, but additional reports may be required per the OPLAN or OPORD. Further information on deployment reports is provided in Appendix D. Deployment reports for expeditionary HSS units include, but are not limited to, the following:
1. Readiness reports (hospital ships and reserve EMFs only)
2. Operational reports
3. Joining

NWP 4-02
3-13 JAN 2008
4. Facility spot status
5. Disease surveillance
6. Situation report
7. Blood and blood request
8. Patient evacuation.
3.3.4 Redeployment
Redeployment, also referred to as deactivation, demobilization, or reconstitution, is usually initiated with a redeployment warning order from the FLTCOM who provides redeployment guidance. As described in JP 4-02, Health Service Support, redeployment must be planned and executed in a manner that facilitates the use of redeploying forces and sustainment equipment and supplies to meet a new crisis. Redeployment may involve a deployment back to a home station or, in some instances, to a new duty station to meet a new crisis. Redeployment is conducted in six phases:
1. Phase I: Reconstitution for Strategic Movement. Units move to tactical assembly areas. Major focus is on rebuilding unit integrity and accountability; turn-in of excess Class VIIIA supplies and unique HSS equipment; reconstitution and/or initial transfer of HSS supplies and equipment; and cleaning, repacking, and loading containers for shipment.
2. Phase II: Movement to the Redeployment Assembly Areas. Complete activities that could not be completed in Phase I.
3. Phase III: Movement to the POE.
4. Phase IV: Strategic Lift.
5. Phase V: Reception at a POD. Focus is on processing redeploying forces, supplies, and equipment, and on movement to follow-on destinations.
6. Phase VI: Onward Movement from a POD. Forces reorganized and moved to marshaling areas and then onward to destination.
Nonunit redeployed supplies and equipment are redistributed with priority given to Service forces committed to approved OPLANs. HSS logistics activities must coordinate with DLA for disposal and turn-in of excess equipment to DLA depots. Commanders must ensure postdeployment health briefings and completion of DD Form 2796 are accomplished for each redeploying individual within 30 days of return to home/processing station, per DODI 6490.3, Deployment Health.
3.3.4.1 Navy Expeditionary Health Service Support Redeployment
Upon receipt of deactivation orders, expeditionary HSS units will curtail admissions or discontinue accepting patients and begin to arrange for the evacuation of patients. After patients are evacuated, the hospital ship will detach from its component command and return to its layberth. All MTF departments will execute their deactivation plans. EMFs may undergo a phased reduction to a certain bed level and then be redeployed, or may be totally deactivated. In the latter case, patients are returned to duty or evacuated rearward, and the hospital is disassembled, repacked, and redeployed.
Once a deactivation date is known, a deactivation EMF assistance team will be sent to the operational site and remain onsite until the theater commander concurs with the completion of the deactivation. Other units, such as FDPMUs, may have a defined, short-term mission and will redeploy upon completion of the mission and release

NWP 4-02
JAN 2008 3-14
by the theater commander. FSTs remain with the CRTS for the duration of the deployment. MTF COs/OICs must be involved in deactivation planning with theater HSS planners in the chain of command.
3.3.4.2 Marine Corps Redeployment
Upon completion of operations, the medical logistics company CO will request cancellation of outstanding or open requisitions. Excess HSS materiel on hand or in transit will be evaluated for redistribution, and existing excesses reported to the theater Defense Reutilization Office. HSS materiel brought into theater as part of the MEF table of equipment and organic allowance will be retrograded using the same procedures. The capabilities of maritime prepositioning ships (MPS) that were offloaded and are reusable will be returned to the MPS program. All remaining expired and nonfunctional HSS materiel will be disposed of per local laws and Department of Defense directives (DODDs).
3.4 MEDICAL INTELLIGENCE
3.4.1 Medical Intelligence Defined
Medical intelligence results from the collection, evaluation, analysis, and interpretation of foreign medical, bio-scientific, epidemiological, and environmental information used for strategic planning, military operations, and military medical planning. Produced by a recognized member of the national intelligence community, medical intelligence helps to conserve the fighting strength of friendly forces and to form assessments of foreign medical capabilities in military and civilian sectors.
3.4.2 Significance of Medical Intelligence
Accurate and timely intelligence is a critical combat support tool for planning, executing, and sustaining military operations. It is equally important in achieving optimum planning, execution, and sustainment of HSS operations, the medical readiness of the command, and the overall combat readiness of the unit. Medical intelligence at the operational level focuses on Navy, Marine Corps, and joint operational planning. This is done through utilization of current operations and exercises, and deliberate planning as the backdrop for intelligence production. At the tactical level, medical intelligence is oriented toward the specific operational area and a given operation in greater detail. When properly used and applied, medical intelligence is a powerful force multiplier providing the critical essential elements of information required to assist HSS staff in developing plans and strategies that:
1. Identify the medical threat
2. Counter the medical threat
3. Are responsive to the unique aspects of the particular theater
4. Enable the commander to conduct operations
5. Conserve the fighting strength of friendly forces.
3.4.3 Intelligence Cycle
The intelligence cycle is the process by which information is levied into requirements, collected, converted into intelligence, and made available to users. There are six phases in the intelligence cycle:
1. Requirement. Determination of intelligence requirements, preparation of a collection plan, and issuance of orders and requests for information collection.
2. Collection. Acquisition and dissemination of information to processing and production elements.

NWP 4-02
3-15 JAN 2008
3. Processing/Exploiting. Conversion of collected information into a form suitable to the production of intelligence.
4. Analysis/Production. Conversion of information into intelligence through integration, analysis, evaluation, and interpretation of all-source data and the preparation of intelligence products in support of known or anticipated user requirements.
5. Dissemination/Integration. Conveyance of intelligence in a suitable form and the application of intelligence to appropriate missions, tasks, and functions.
6. Evaluation/Feedback. Continuous assessment of intelligence operations during each phase of the intelligence cycle to ensure that the commander’s intelligence requirements are being met.
3.4.4 Intelligence Sources
3.4.4.1 Operational Intelligence Sources
The first place to search for timely, applicable intelligence at the operational and tactical levels is the COCOM J-2 or joint intelligence support element (JISE) with geographic responsibility for the area where the JTF is being deployed. When properly facilitated by a POMI officer assigned to the CCDR, the CCDR surgeon should be intimately familiar with current intelligence for that region or health threats (epidemiological and environmental), HSS capabilities and infrastructure, industrial infrastructure posing health threats, tactical military threats such as CBRN, and regional capabilities for CBRN medical countermeasures.
3.4.4.2 Armed Forces Medical Intelligence Center
The Defense Intelligence Agency (DIA) has oversight authority on the collection, interpretation, and dissemination of intelligence, including medical intelligence, supporting DOD operations. Finished all-source medical intelligence is produced by the Armed Forces Medical Intelligence Center (AFMIC), Fort Detrick, Maryland. AFMIC is a field activity of DIA and is the focal point in DOD for the production of finished intelligence on foreign military and civilian HSS capabilities, including the health status of foreign military forces, and infectious disease and biomedical subjects of military importance. AFMIC produces and disseminates finished intelligence products via studies, message traffic, compact disk read-only memory (CD-ROM), and online electronic systems.
AFMIC products commonly used by HSS planners fall into the category of recurring-term finished intelligence. These products include (but are not limited to) the following:
1. Infectious Disease Risk Assessment (IDRA).
2. Environmental Health Risk Assessment (EHRA).
3. Industrial Facility Health Risk Assessment (IFHRA).
4. Toxic Industrial Chemical Health Risk Assessment (TICHRA).
5. Industrial Facility Dispersion Modeling and Risk Assessment (Tier III).
6. Health Service Assessment (HSA). Medical intelligence includes only finished intelligence products produced by an authorized intelligence agency such as AFMIC through the intelligence process. HSAs are designed to provide customers with the bottom-line assessment of the health service capabilities of a country that has limited descriptive data. Assessments relate to the critical elements of the civilian and military health systems that have an immediate or potential impact on policies, plans, and operations.

NWP 4-02
JAN 2008 3-16
7. Medical, Environmental, Disease, Intelligence, and Countermeasures (MEDIC). MEDIC CD-ROMs are updated regularly and provide worldwide infectious disease and environmental health risks that are hyperlinked to the joint Service-approved countermeasure recommendations, military and civilian health care delivery capabilities, operational information, disease vector ecology information, and reference data.
8. Medical Intelligence Note (MIN). MINs are current intelligence documents presenting analysis of newly reported information of potential interest to consumers. MINs are produced periodically, generally on topics of immediate interest to deployed or deploying forces.
9. Infectious Disease Alert (IDA). IDAs provide time-sensitive updates to IDRAs and are published daily or as required. Classification is subject to the content of the alert.
10. Request for Information (RFI). RFIs are requests for time-sensitive, quick-reaction intelligence reports and operational contingencies. RFIs are normally accepted by AFMIC, if the requirements of the task can be completed in a maximum of 40 personnel hours of analytical work. Requests are accepted by telephone (open and secure communications) and by direct correspondence or message format. Whenever possible, formal methods of communication are encouraged. Navy HSS personnel should request intelligence through the intelligence shop, when applicable. RFIs can be submitted to the following mailing and message traffic addresses:
Armed Forces Medical Intelligence Center Defense Intelligence Agency Bldg 6000 ATTN: AFMIC Operations Washington, DC 20340-5100
DIRAFMIC FT DETRICK MD//OPS// Watch desk: Comm: (301) 619-7574 (STE Capable) DSN: 343-7574
3.4.5 Other Sources of Medical Intelligence
3.4.5.1 Defense Pest Management Information Analysis Center
The Defense Pest Management Information Analysis Center (DPMIAC) publishes a series of disease vector ecology profiles (DVEPs) of many foreign countries and regions of the world that include disease risks, infectious agents, modes of transmission, geographic and seasonal incidence, and prevention and control recommendations. Some of its other publications are also available online. A CD-ROM of operational entomology references is also available.
3.4.5.2 Navy Preventive Medicine Information System
The Navy operates regional NEPMUs that periodically publish the bulletin Fleet Public Health and provide assistance throughout the world.
3.4.5.3 Walter Reed Army Institute of Research
Walter Reed Army Institute of Research (WRAIR) publishes a quarterly communicable disease report that identifies disease outbreaks worldwide. Additionally, WRAIR quickly responds to ad hoc queries and provides timely regional medical assessments.

NWP 4-02
3-17 JAN 2008
3.4.5.4 United States Army Research Institute of Environmental Medicine
The United States Army Research Institute of Environmental Medicine (USARIEM) publishes a series of deployment manuals that address soldier health and performance in a wide variety of environments.
3.4.5.5 State Department
The State Department publishes Background Notes, a series of publications on selected countries and regions.
3.4.5.6 Centers for Disease Control and Prevention
The Centers for Disease Control and Prevention (CDC) publishes Health Information for International Travel, a document often referred to as the Yellow Book, which identifies current vaccination requirements, immunization and prophylaxis recommendations, and regional health hazards. This information is also accessible online at http://www.cdc.gov/travel/.
3.4.5.7 World Health Organization
The World Health Organization (WHO) publishes Vaccination Certificate Requirements for International Travel and Health Advice to Travellers, a document that is similar to the Yellow Book and the Weekly Epidemiological Record (WER).
3.4.6 Medical Threat
3.4.6.1 General
The medical threat is the composite of all ongoing or potential enemy actions and environmental conditions that could reduce the effectiveness of friendly forces. These actions and conditions produce wounds, injuries, or disease. An example of significant medical threat is prolonged or intense periods of combat operations that may lead to high incidences and levels of combat stress. Throughout military history, disease has accounted for more force attrition during periods of conflict than battle or nonbattle injuries.
3.4.6.2 Threat Analysis
Intelligence and threat are not synonymous. Intelligence agencies and intelligence staffs produce finished and unfinished intelligence information on foreign areas and situations. Intelligence preparation of the operational environment (IPOE) aids in the accurate comparison of friendly and enemy capabilities, describes the medical situation in the AO, and enables the HSS staff to see areas of potential weakness in medical readiness.
3.4.6.3 Modern Warfare and Medical Threat
1. Characteristics. The characteristics of modern warfare that define the medical threat include the following:
a. The level of combat intensity, heavy use of supplies, and the ever-increasing range and lethality of indirect fire weapons.
b. The enhanced lethality, wounding capability, and destructive properties of munitions.
c. The collateral and residual effects of conventional or nuclear, biological, and chemical (NBC) weapons.
d. Infectious diseases that pose a major threat to combat forces; these diseases may be in the form of naturally occurring diseases or diseases introduced by a biological weapon.

NWP 4-02
JAN 2008 3-18
e. Environmental factors such as extremes in temperature and altitude and the presence of poisonous animals, plants, and insects; these factors are important considerations as causative agents of disease and injury casualties.
2. Risk to HSS organizations. Although premeditated attack upon HSS organizations, personnel, or Class VIII materiel may not be primary, it should not be ignored. A steady erosion of battlefield HSS resources will result from the following:
a. Significant increases in wounded casualties beyond the capability of the HSS system to provide timely care.
b. Enemy combat operations in friendly rear areas interdicting lines of communication, disrupting vital combat support, and CSS activities; this will seriously impact the ability of HSS personnel to retrieve, evacuate, and care for wounded, sick, and injured personnel.
c. Prolonged periods of intense, continuous operations under all types of conditions that tax sailors and Marines to the limits of their physiological and emotional endurance.
d. The actions of terrorists (individuals or groups) directed against HSS facilities.
3. Technological applications. Application of advanced technologies to enhance existing weapons and munitions and development of new weapon systems may provide the HSS system with new diagnostic and treatment challenges. Examples of technology-driven developments that may be confronted include:
a. Engineered biochemical compounds used as biological warfare agents
b. Genetically engineered microorganisms used as biological warfare agents
c. Directed energy (DE) weapons consisting of high- and low-energy lasers and high-energy microwave, radio frequency, and particle weapons
d. Enhanced blast effect weapons used against personnel
e. New flame and incendiary compounds and munitions
f. Enhanced nuclear weapons with increased lethality from radiation
g. Possible mind-altering agents.
3.4.6.4 Elements of the Medical Threat
1. Threat elements to HSS personnel. The threat elements with the greatest potential for HSS personnel degradation include:
a. Battle injuries caused by artillery, small arms, and fragmentation weapons
b. Casualties due to combat stress
c. CBRN and combined casualties
d. Premeditated attack upon HSS organizations, personnel, or Class VIII supplies
e. The continually increasing range of indirect weapons fire
f. The enhanced wounding capability and destructiveness of weapon systems

NWP 4-02
3-19 JAN 2008
g. The collective effects of conventional and CBRN weapons
h. Increases in casualty densities causing local or general overloads of the HSS system
i. Infectious diseases and environmental extremes.
2. Enemy operations. Enemy combat operations in friendly rear areas will interdict lines of communications and disrupt necessary logistics activity. This will produce a serious negative effect on the ability of personnel to conduct health care operations. Although enemy combat operations may threaten the survival of HSS, they are not considered to be medical threats for the purposes of this publication.
3. HSS personnel limitations. Prolonged periods of intense, continuous operations will tax HSS personnel to the limit of their physical, psychological, and emotional endurance. This will cause degradation in the ability of the HSS system to deliver health care at a sustained level.
4. HSS organizations as enemy targets. HSS organizations are not expected to be the primary target for biological and chemical attacks; however, logistic base complexes will be prime candidates for such enemy operations. As elements of logistic complexes, medical organizations must anticipate collateral contamination from attacks on adjacent facilities. Forward HSS assets have an even higher probability of being contaminated by biological and/or chemical weapons.
3.5 THE COMMANDER’S ESTIMATE
3.5.1 Development of the Commander’s Estimate
The development of the commander’s estimate is central to formulating and updating the military action to meet the requirements of any situation. The process of developing an estimate is used by commanders and staffs at all levels and should be considered a continuous process. Though the central framework for organizing inquiry and decision is essentially the same for any level of command, specific detailed questions within each part of this framework will vary depending on the level, type, and phase of operation. Both commander and staff estimates will become more detailed and refined as the planning process continues. This section briefly discusses the estimate and HSS role in the estimate process; however, a more detailed discussion of the estimate process is provided in JP 5-0, Joint Operation Planning, for medical planners and operational medical commanders.
The commander’s estimate provides a continuously updated source of information from the perspective of the JFC. Estimates are used by commanders at various levels to support all aspects of the determination of COAs and plan or order development. The commander’s estimate considers the operational environment, nature of anticipated operations, and national and multinational strategic direction. The commander submits an estimate that analyzes various COA that may be used to accomplish the assigned mission, and recommends the best COA. Supporting commanders provide estimates to the supported commander outlining the feasibility of support within each COA.
3.5.2 Staff Estimates in the Estimate Development Process
Staff estimates provide the foundation for COA selection. Each staff estimate takes on a different focus that identifies certain assumptions, detailed aspects of the tentative COA, and potential deficiencies and risks that are simply not known at any other level but nevertheless must be considered. Collaboration among relevant military, interagency, and multinational staff elements during the staff estimate process facilitates the iterative refinement of COA. Therefore, combined staff estimates help determine which COA best accomplishes the mission and which can best be supported. This, together with supporting discussion, gives the commander the best possible information to select a COA. In their staff estimates, each staff element:
1. Reviews the mission and situation from its own staff functional perspective.
2. Examines the factors and assumptions for which it is the responsible staff.

NWP 4-02
JAN 2008 3-20
3. Analyzes and refines each COA to determine its supportability from the perspective of the staff’s functional area.
4. Concludes whether the mission can be supported and which COA may best be supported.
Early staff estimates are frequently given as oral briefings to the rest of the staff. In the beginning, they tend to emphasize information collection more than analysis. Not every situation will require or permit a lengthy and formal staff estimate process. For a simple mission or during exercises, the commander may review the assigned mission, receive oral staff briefings, develop and select a COA informally, and direct the plan to commencement. It is only in the later stages of the process that the staff estimates are expected to indicate which COA are most likely to succeed and can best be supported.
3.5.3 Health Service Support Estimate
The HSS role in the estimate process is most apparent at the staff level. A medical staff estimate is an assessment of the HSS situation within the mission area. It is built through the use of medical intelligence discussed in the previous section. It identifies and addresses known or anticipated medical threat factors that may affect force health protection. These factors include theater patient movement policy; required medical treatment, evacuation, and hospitalization capabilities; preventive medicine, veterinary, and dental support required; health service logistics; and the medical aspects of chemical, biological, radiological, and nuclear defensive operations. As all staff functional areas, it includes an evaluation of how these health factors can influence each COA.
HSS planners use the medical estimate in completing the medical portion of the operation plan. Guidelines for developing a medical estimate are located in CJCSM 3122.01A, Joint Operations Planning and Execution System, Volume I; FMFM 3-1, Command and Staff Actions. Appendix K of FMFM 4-50, Health Service Support, provides an example of a medical estimate.

NWP 4-02
4-1 JAN 2008
CHAPTER 4
Naval Expeditionary Health Service Support Considerations
4.1 INTRODUCTION
Planners must consider a number of operational factors whenever NEHSS units are deployed. The unit’s mission affects these factors whether it is in support of combat operations or responding to a homeland security or disaster scenario. Planners must also consider lessons learned to ensure the best method of addressing HSS concerns from OPLAN and OPORD development to HSS unit redeployment.
4.2 HEALTH CARE IN AN AUSTERE WARTIME ENVIRONMENT
In wartime, the quality and scope of health care are often determined by factors that mitigate against the controlled environment of a fixed MTF. Saving lives, stabilizing and moving patients to the next capability of care, and returning patients to duty is often hindered by conditions beyond the control of the expeditionary HSS unit. Patient load may exceed the capacity of the unit, resulting in the need to triage patients. The wartime environment tests the skills of those assigned to the HSS units. Clinical staffs may lack the basic skills necessary to function in an operational environment. In some cases, physicians and other health care personnel may be required to perform tasks not usually delivered during peacetime in fixed MTFs.
4.2.1 Clinical Services
4.2.1.1 General Considerations
Clinical practice is based on applying practiced skills within facility limitations related to structure, equipment, supplies, and/or manpower. The expeditionary HSS MTF is designed for intensive combat casualty management providing theater hospitalization capability of care. The operational commander, the surgeon, and the MTF CO/OIC should consider mission requirements when determining requests for MTF modification. Requests are sent via the operational commander’s chain of command to the joint staff for further action. The supporting commands provide what is needed for the mission.
Other areas for consideration include the following.
1. To ensure proper utilization, the MTF CO/OIC should designate in writing a SMO to provide for:
a. Consultative services not provided in the HSS unit
b. Patient movement coordination
c. Medical intelligence support.
2. Psychiatric patients may require a separate secure area and frequent monitoring.
3. Despite surge protectors, electrical fluctuations can cause equipment problems, including loss of function.

NWP 4-02
JAN 2008 4-2
4. Medical regulating can be limited or challenging, resulting in patients arriving with little or no care, especially from non-US forces.
5. When utilizing foreign health care capabilities for support, the MTF staff should be aware of different capabilities, philosophies, and timeliness of the care provided.
6. The standard requirements for health care of servicewomen in military operations and isolated settings are similar to requirements in nonoperational settings. However, delivery of this care may be more problematic depending upon the capabilities and available resources within the particular operational setting. The principal factors that influence the capability and scope of care provided include the following:
a. Medical and surgical configuration/capability of the platform or contingency area under consideration
b. Level of HSS provider billets assigned, such as a general practice physician, an IDC, a physician assistant, and a nurse practitioner
c. Availability of obstetrics-gynecology (OB-GYN) consultation, including mode, such as in person, by radio, or telemedicine
d. Availability of current medical references, such as NAVMED P-6300-2 (series), Operational Obstetrics and Gynecology, The Health Care of Women in Military Settings
e. Inclusion of gender-specific medications and supplies in current AMALs
f. Current OB/GYN training requirements
7. Coalition operations may impose a requirement for a higher capability of care than is normally expected of an MTF. Other nations often lack the ability to provide more advanced capabilities of medical care for their forces in theater or at home. Health care providers may find it difficult to release patients for whom they were unable to provide the utmost in medical care. The level of practice required may exceed the availability of equipment and supplies that ordinarily equip the facility. In dentistry, there is an increased number of emergencies secondary to prior inadequate dental care and poor dental hygiene. The following are other cultural issues of concern to the MTF staff:
a. Language problems may occur when patients are foreign nationals.
b. Patient nutrition may be more difficult in certain cultures. Patients may be unable to eat foods such as pork, beef, or shellfish. Alternative foods are not easily obtained in the field environment.
c. Medical protocols for addressing military patients of other nations may need to be altered in an MTF. For example, in some cultures, addressing a patient by first name instead of by rank may be preferable to the patient and lead to greater patient compliance.
d. In assisting foreign nationals with establishing family contact, particular problems may be encountered due to language differences and/or lack of adequate communications equipment.
e. Liaison, especially in the emergency room, should be established immediately with all in theater police forces, such as the US military, foreign military, UN, and foreign civilian.

NWP 4-02
4-3 JAN 2008
4.2.1.2 Surgical Services
Surgical services, including subspecialties, should be limited to guidance provided in the HSS unit’s SOPs. Surgeons should also be cognizant of the theater evacuation policy and its implications. Because hospital ships may be employed in situations other than intensive combat, the type of practice within these specialties can change. Expeditionary HSS units, especially hospital ships and EMFs, may be increasingly employed in protracted operations that require extensive community hospital functions. The MTF CO/OIC should determine the extent of practice modification based on the facility’s equipment, supplies, and personnel and on the population receiving care.
4.2.1.3 Medical Services
Medical services are provided in the wards, ICUs, and casualty reception area by providers experienced in intensive care patient management. Specific considerations include:
1. Individuals trained in the operation and maintenance of ventilators and oxygen delivery systems are needed to support ventilated patients.
2. Nonsurgical support should be planned for patients expected during combat and low-intensity-conflict missions. The scope of knowledge, skills, and HSS capabilities supports patient populations being cared for during multinational and refugee operations.
3. Multinational operations may present challenges where the MTF CO/OIC may rely on providers whose broad medical background includes general medicine, pediatrics, obstetrics, gynecology, preventive medicine, and office practice of surgical procedures.
4. Respiratory isolation capabilities and special personal protective measures by all hospital staff are required to control the spread of infection, particularly when providing medical care for refugees or foreign nationals.
4.2.1.4 Emergency Medical Services — Casualty Reception
Many operations will require ambulatory, noncombatant patient care, pediatrics, and refugee care. Casualty reception, which is the entry point for all patients, is typically managed by nursing services. The MTF CO/OIC may decide that the best mix of MTF personnel should include emergency medicine specialists, who are not normally included but are the best trained and most qualified for staffing casualty reception. Other issues for consideration include:
1. Patients arriving by casualty evacuation (CASEVAC) or MEDEVAC unprepared for transport because they are medically unstable or armed
2. Casualty reception requiring continuous provision of the following:
a. Trauma resuscitation/stabilization
b. Triage
c. Efficient patient flow
d. MEDEVAC coordination.
3. Mission scenarios requiring the provision of emergency pediatrics or OB/GYN in the care of civilians
4. Toxicological problems in hazardous material accidents requiring management

NWP 4-02
JAN 2008 4-4
5. Mass casualty drills to be carried out realistically in preparation for emergency situations.
4.2.1.5 Anesthesia Services
The MTF is configured to provide anesthesia in support of combat casualty care, including casualty receiving, postanesthesia care, and ICUs. The anesthesia capability may also be provided for elective cases, with approval of the patient’s chain of command and when scheduled without requiring augmentation of equipment, supplies, or manpower. Elective procedures are not typically performed during combat operations.
4.2.1.6 Dental Services
During a period of intense combat operations with combat casualties, the practice of dentistry is limited to acute dental conditions. The progression of procedures, as the tempo permits, would then include dental maintenance and required periodic examinations. As the length of the deployment increases, inclusion of elective procedures, oral surgery, and limited prosthetics (if available) may become a necessity. Dentists also function as medical triage officers during mass casualty situations when physician manpower is exceeded.
4.2.1.7 Optometry Services
Hospital ships are equipped with optical fabrication laboratories that can be used to produce spectacles within a limited range of single-vision lenses. Spectacle fabrication becomes a critical requirement when glasses are lost or damaged and troops arrive without spare eyeglasses or inserts for their gas masks or combat eye protection. Optometry and optical fabrication may be a significant source of care in humanitarian scenarios.
4.2.1.8 Physical/Occupational Therapy
Physical/occupational therapy provides support in the treatment of burn patients and basic musculoskeletal injuries. Experience has shown that because some expeditionary HSS units, especially those that provide theater hospitalization capability, expend time treating patients other than combat casualties, the number of cases benefiting from physical therapy has increased. These cases include musculoskeletal injuries related to equipment handling and other industrial accidents, vehicular accidents, falls, minor burns, soft tissue trauma, sprains and strains, and surgical cases not requiring immediate evacuation from the theater.
Increased physical/occupational therapy services may be required during the employment of the expeditionary HSS unit in multinational or UN operations. The patients cared for may often require a level and sophistication of rehabilitative care not easily found in the individual’s home country. Lessons learned indicate that, by default, they may stay longer than expected and will require physical therapy for functional rehabilitation back into their own society.
4.2.1.9 Respiratory Therapy
The TF surgeon and the MTF CO/OIC should consider augmenting assigned respiratory technicians based on anticipated requirements. While other qualified personnel can manage individual cases, large-scale airway management will severely affect personnel and other services.
4.2.1.10 Clinical Nutrition
The Medical Service Corps dietitian oversees patient meal service at the theater hospitalization capability (hospital ships and EMFs), provides inpatient and outpatient care to both casualties and staff, coordinates nutrition-related classes with health promotion, and assists with general food service as required. When activated, the dietitian’s primary role is patient meal service and inpatient care. As the inpatient census increases, the dietitian’s primary role is to provide initial nutrition assessment, intervention, and follow-up as needed.

NWP 4-02
4-5 JAN 2008
4.2.2 Nursing Services
Nursing practice in expeditionary HSS should take into account the following general considerations:
1. Nursing subspecialties should match mission requirements to the maximum extent possible.
2. Quality patient care may require the use or combination of different systems or processes and skills in creativity, improvisation, and flexibility.
3. Environmental cleanliness may be more difficult to achieve. Increased efforts may be required to remove and protect against airborne particulates. All equipment and supplies require dust-cover protection.
4. Specialized equipment may not be available.
5. Wards are close quarters; staff must be aware of, and provide for, patient privacy in close-quarter wards.
6. Liaison should be established with nursing staffs at other military and civilian facilities, if available. This network can be crucial in achieving treatment goals.
4.2.3 Combat Stress
DODD 6490.5, Combat Stress Control (CSC) Programs, provides broad guidance on combat stress and combat stress control programs. Combat stress is defined as a change in mental functioning or behavior due to the challenges of combat and its aftermath. These changes can be positive and adaptive, or they can be indications of distress or loss of normal functioning that may be symptoms of a combat/operational stress injury. Operational stress is a change in mental functioning or behavior due to the challenges of military operations other than combat. Combat/operational stress is manifest on a continuum ranging from a brief stress reaction, to a more lingering or persistent stress injury, to the disabling impairment of a stress disorder. Stress response varies in quality and severity as a function of the intensity, duration, and frequency of exposure, as well as other factors affecting risk and resilience such as quality of training, rules of engagement, leadership, effectiveness of communication, unit morale, unit cohesion, and perceived importance of the mission. Stress reactions are usually transient and resolve within a few hours or days with unit-level intervention. However, when the reaction fails to resolve within a day or two, this may indicate a stress injury and should be monitored closely with a low threshold for referral for professional evaluation and treatment.
The Marine Corps Operational Stress Control and Readiness (OSCAR) program deploys embedded mental health assets with ground combat forces at the regimental level throughout the deployment cycle, and includes psychiatrists, psychologists, and chaplains. OSCAR teams provide continuous prevention services and command liaison, early identification of stress reactions and injuries, enhanced command confidence in psychological health services, and decreased barriers to mental health care for stress injuries.
4.2.4 Trauma Care
Successful management of major trauma requires a continuum of care, from point of wounding to return to duty or final disposition. In general, trauma care should be in accordance with accepted clinical practice, but with important consideration given to the operational mission, setting, location, resources of the expeditionary HSS, supporting echelons, and MEDEVAC capability. The goal of forward-based surgical units is to save life and limb of those who would be lost because of prolonged access times to surgery. In order to do so, the surgeon must utilize damage control surgical techniques. These are procedures to restore a more normal physiology, often at the expense of anatomic repair. It entails doing only what is required to keep a patient alive, not definitive treatment of the injuries. The objectives of this forward resuscitative surgery are to decrease mortality in this potentially salvageable group of casualties, and to decrease morbidity by rapid restoration of normal physiology and control of contamination. This concept of minimal acceptable care must be employed when weight, mobility, and footprint size are to be minimized.

NWP 4-02
JAN 2008 4-6
The deployment of highly mobile surgical units such as the FRSS has dramatically changed expeditionary HSS. These forward surgical units allow patients to be stabilized and life- and limb-saving surgery to be performed close to the point of injury, prior to transfer to rear echelon medical facilities. However, this capability must be provided with limited resources in order to maintain mobility. The FRSS occupies a fraction of the footprint of a surgical company or EMF but has the capability to provide resuscitative care up to and including blood transfusions.
The acute medical management of casualties includes triage, rapid identification, and management of injuries that will cause loss of life or limb. A primary survey is performed and airway and breathing issues are addressed first, followed by control of exsanguinating hemorrhage. Exsanguinating hemorrhage must then be managed either surgically or with local hemostatic agents. Open wounds should be assessed and fractures stabilized. This primary survey is rapidly followed by a comprehensive secondary survey to identify all remaining injuries. At that point, the decision to proceed to surgery or to MEDEVAC will depend on resources, patient’s hemodynamic stability, and MEDEVAC capability.
The aforementioned methods require postoperative care and evacuation. The FRSS has a limited ability to care for postoperative patients who require extensive resources for treatment. This limitation creates a need for rapid evacuation after stabilization. MEDEVAC with enhanced en route care capability is required to transport these casualties to the next capability of care. The Marine Corps ERCS addresses this issue.
4.2.5 Naval Specialty Medicine
Certain naval specialties have tailored medical programs to better fit the nature of the job and the physiology requirements. These specialties include aviation, undersea/diving, and special operations.
4.2.5.1 Aviation Medicine
The U.S. Naval Flight Surgeon’s Manual provides essential guidance for flight surgeons and supporting medical personnel. For those aboard aircraft carriers, the guidance derives from COMNAVAIRFORINST 6000.1 (series), Shipboard Medical Procedures Manual.
Aviation HSS personnel have the following responsibilities:
1. Conducting physical and psychological examinations of candidate and designated flight aircrew as appropriate
2. Conducting aeromedical safety inspections and providing preventive instruction and guidance as necessary
3. Conducting an appropriate aviation-specific environmental and industrial health monitoring program
4. Providing appropriate training in the physiological aspects of flight and survival to ensure aircrew proficiency in using personal life support and survival equipment
5. Providing aeromedical expertise in aircraft mishap investigations, aviation and specific administrative matters, and human factor issues
6. Providing input/serving on field naval aviator evaluation boards, field naval flight officer evaluation boards, human factor councils, and local boards of flight surgeons
7. Providing aeromedical expertise in the evacuation of patients
8. Providing aeromedical consultation to embarked commanders
9. Supporting hyperbaric and other environmental medicine needs.

NWP 4-02
4-7 JAN 2008
4.2.5.2 Undersea Medicine
Undersea medicine encompasses medical support to the submarine service and the diving community. Current policy assigns hospital corpsmen in pay grades E-5 through E-7 onboard submarines as MDRs. Undersea medical personnel are responsible for:
1. Conducting physical and psychological examinations of candidates and designated submarine and diving personnel as appropriate
2. Conducting submarine and diving medical safety inspections and providing accident prevention instruction and guidance
3. Conducting an appropriate submarine and diving-specific environmental and industrial health monitoring program
4. Ensuring appropriate training is provided for submarine and diving, including special operations, and HSS personnel
5. Providing medical expertise in diving mishap investigations, administrative matters, and human factor issues
6. Providing guidance and support for hyperbaric chamber use and all matters of hyperbaric medicine
7. Providing input/serving on boards and councils for issues of undersea and hyperbaric medicine
8. Providing medical expertise in the MEDEVAC of submarine and diving patients
9. Providing medical consultation to embarked commanders
10. Providing diving medical support and expertise to naval special warfare units (NSWUs) during all operations that involve diving
11. Providing liaison among submarine, diving operational units, and shore-based MTFs regarding HSS matters affecting operational readiness.
The U.S. Navy Diving Manual, Volume 5, addresses diving medicine and recompression chamber operations. For any diving operation, Navy policy calls for the dive team to have a MEDEVAC plan and to know the location of the nearest or most accessible diving medical officer and recompression chamber. Diving medical personnel should be involved in pre-dive planning and in training for diving-related medical emergencies.
For further information on undersea medicine, refer to COMSUBLANT/COMSUBPACINST 6000.2 (series), Standard Medical Department Organizational Manual for Submarines.
4.2.5.3 Naval Special Warfare Medicine
USSOCOM, a unified command, frequently relies on the Service component commands for much of the logistical support requirements. In special situations or selected operations, special medical augmentation packages can be attached to these units. The primary focus of SOF HSS is to provide essential care and sustain casualties until force extraction from the operational area. SOFs are characterized by an austere structure and a limited number of HSS personnel with enhanced medical skills.
The SOF HSS planner must coordinate closely with the TF surgeon and HSS staff during the preoperational planning phase for required HSS. Because of the operational security associated with special operations missions, the SOF HSS planner may only be able to provide a list of required HSS. Such requests must be accepted as presented, and the required support must be provided, if it is within the capabilities of the TF, the procedures

NWP 4-02
JAN 2008 4-8
provided in the NAVMED P-117, Manual of the Medical Department (MANMED), and other regulatory directives.
USSOCOM is responsible for first responder capability. For naval special warfare (NSW) forces, this care is provided by specially trained hospital corpsmen that are capable of providing first responder capability in the field for extended periods to injured or ill teammates. SOF technicians and an IDC are fully qualified as Navy sea-air-land team(s) (SEALs) and have advanced training in combat trauma management and field, environmental, and preventive medicine. In addition, diving medical technicians and independent duty diving medical technicians have expertise in diving medicine.
Health care for and evacuation of SEALs beyond first responder capability are provided by Navy and Marine Corps conventional units from which the teams stage, or by Service units providing HSS support on an area basis. Service units include Army SOF forward operating bases and Marine units with organic FRC capability. SOF units that utilize nonmedical assets and vehicles of opportunity without en route medical care often depend on CASEVAC. Supporting units, including SOF aviation elements, must provide AE. Navy SEAL teams have no preventive medicine, laboratory, or dental support and deploy with basic loads of HSS supplies.
4.2.6 Other Requirements for Operational Medical Support
Some naval operating forces may have special requirements for HSS. For example, naval construction battalion engineer reconnaissance teams and expeditionary logistics units conduct operations and are deployed in environments that can result in casualties. The Navy typically deploys an entire construction battalion, and smaller units break off to conduct operations. A smaller unit may take a corpsman from the battalion’s medical department for first responder capability, especially when deployed in remote areas where nonorganic HSS is unavailable. These units have to rely on nonorganic/Marine Corps HSS capabilities for FRC capability and, in many cases, for first responder support. With a requirement validated by OPNAV N931, personnel can be assigned to augment any unit.
4.2.7 Decedent Affairs
Decedent affairs are a line-unit responsibility. Specific guidance is provided in the OPLAN. The policy for the handling of deceased personnel must be addressed in the theater commander’s plan when a specific OPLAN in not in place. Expeditionary HSS units are neither equipped nor staffed to perform this function, and will require mortuary and graves registration support from the operational commander proportional to the casualties received, including augmentation following mass casualties. Until graves registration personnel arrive, the HSS unit will have to handle remains. EMFs and CRTSs have a limited capability to store remains. Hospital ships are equipped with a refrigerated morgue facility capable of holding up to 22 remains. Other concerns involve handling the remains of foreign nationals and relying on organizations without rapid response capability.
The HSS unit should develop plans based on the force composition supported by the MTF, and in coordination with component service logistic planners. When dealing with biologically or chemically contaminated remains, significant issues must be addressed. The CO/OIC of the HSS unit should refer to JP 4-06, Mortuary Affairs in Joint Operations, and the theater, component, or JTF commander’s mortuary affairs plan. Detailed guidance is provided in the Navy Medical Command Instruction (NAVMEDCOMINST) 5360.1, Decedent Affairs Manual; and DODD 1300.22, Mortuary Affairs Policy. The following is general guidance for the disposition of remains:
1. Provide postmortem care.
2. Place remains in body pouch.
3. Refrigerate remains at a temperature between 36 °F and 40 °F to slow decomposition.
4. Ensure space utilized contains no other items and is cleaned and disinfected prior to reuse.

NWP 4-02
4-9 JAN 2008
5. Identify remains with waterproof tags, mark with waterproof ink, and affix with wire ties to the right great toe and at each end of the body bag. At a minimum, identification should be full name, social security number, and rank/rate.
A ship or expeditionary HSS unit could have remains contaminated by CBRN agents. JP 4-06, Mortuary Affairs in Joint Operations, states that the remains of all members of the Armed Forces of the United States will be returned for permanent disposition according to the direction of the person authorized to direct disposition of remains. In war and operations other than war, geographic CCDR will determine whether and when operational constraints necessitate a transition to a program of temporary interment in the AOR. When military necessity or other factors prevent evacuation of the remains of US military and civilian personnel, or friendly, third country, or enemy dead, the remains will be interred temporarily according to established procedures. The geographic CCDR makes this decision. All interments performed within the scope of such a program are temporary, except for at sea disposition. Disinterment may commence when evacuation of the remains is operationally acceptable. Cremation is not considered an option. The recovery, evacuation, tentative identification, and final disposition of deceased military and civilian personnel under the jurisdiction of the Armed Forces of the United States are command responsibilities. For humanitarian, health, and morale reasons, this policy may be extended to the local populace fatalities.
For further information on mortuary affairs in an operation plan, refer to CJCS Memorandum of Policy #16, Joint Mortuary Affairs Policy.
DODD 1300.22, Mortuary Affairs Policy, states that temporary interment is a last resort to protect unit health safety and sanitation. The ship’s captain may authorize burial at sea only when preservation capability is unavailable aboard ship or when transfer to shore is not timely or is operationally inadvisable. The geographic commander of the combatant command should approve temporary interments when remains are contaminated from a chemical, biological, or nuclear event and decontamination is impossible without endangering other personnel. Remains will be disinterred when operational and safety requirements permit.
HSS units ashore will follow the policy discussed in JP 4-06, Mortuary Affairs in Joint Operations, and DODD 1300.22, Mortuary Affairs Policy. Since there is no proven method to decontaminate human remains resulting from a CBRN attack, a ship’s CO may elect to remove suspected contaminated remains immediately by burial at sea to ensure the safety of personnel. Prior to committal at sea, a tissue sample shall be harvested and forwarded to the Armed Forces DNA Identification Laboratory via the Dover Port Mortuary. All personnel aboard a contaminated ship must be treated as if contaminated until proven otherwise. Medical personnel will determine whether contamination has spread. Isolation may prove effective for live casualties; however, remains of deceased should be removed as soon as possible.
4.3 COMMUNICATIONS
4.3.1 Planning Considerations
As described in NTTP 4-02.2M/MCWP 4-11.1G, Patient Movement, the success of HSS depends on reliable communications over dedicated and parallel systems. A responsive communications system is critical to providing continuity of HSS support. Such a system allows the command surgeon to effectively and efficiently coordinate all the resources in a dynamic environment. For this reason, the HSS planner must identify communications requirements early in the planning process. At the very least, assignment of a radio network dedicated to patient movement is mandatory. The development of a communications requirements list for HSS must be thorough and must address initial and anticipated needs. The HSS planner will need to develop the conceptual structure for the treatment portion of the HSS system, including the numbers, types, and locations of HSS facilities. The HSS structure will form the basis of patient movement and the communications requirements.
Task force units must have communications that are compatible and will provide medical regulating. In operations where other services are responsible for air traffic control and/or medical regulating, communications incompatibilities should be resolved early in the planning phase of the operation. HSS units should establish early

NWP 4-02
JAN 2008 4-10
contact with fleet and MEF communications officers, who will assist with establishing the medical regulating network (MEDREGNET).
Expeditionary HSS units typically have a limited external communications capability. Medical communications equipment requirements should be documented in Annex K (C4 systems) of the OPLAN for the expeditionary HSS units. Exceptions are the hospital ships, which are equipped with a ship’s radio room, military communications suite, and organic/embarked HSS units that are able to utilize the communications capabilities of the parent or host command.
When deployed, expeditionary HSS units must be able to communicate with the following organizations:
1. Task force staff and other units in the task force
2. Surgeon’s office of the component command possessing OPCON
3. Medical regulating offices (MROs) such as the TF MRO, the Joint Medical Regulating Office (JMRO), and the J/TPMRC
4. Air traffic control agencies such as the helicopter direction center, helicopter control section, and tactical air control center (TACC)
5. Units providing supply support
6. Units providing blood bank support
7. Air and surface MEDEVAC control agencies and units
8. Units within the chain of command
9. Supporting and supported units within and outside theater.
4.3.2 Medical Regulating Network
The purpose of the MEDREGNET is to pass patient information and provide a rapid means of communication among the medical regulating control officer (MRCO) afloat, the patient evacuation officer (PEO) ashore, and the various medical regulating teams. The MEDREGNET ensures that the MRCO/PEO has current information on the requirements, capabilities, and status of all HSS facilities supporting the operation. It must be dedicated and used only for patient movement, HSS supplies, blood reporting, and blood and blood product requests within the AO. Units composing the MEDREGNET should be designated in the OPLAN.
4.3.3 Other Wartime or Contingency Communications Capabilities
The following are additional communications capabilities available to support expeditionary HSS units:
1. MAGTF Alert/Broadcast Network (HF)). Provide alert warnings or general traffic pertaining to all units assigned to the network. It is also used for passing CBRN warnings.
2. Color Beach Administrative Network (HF). Used to pass administrative information, request supplies and equipment, coordinate supply and equipment deliveries to specific beaches, and evacuate casualties from landing beaches. This network is monitored in the flagship’s landing force operations center (LFOC).
3. Tactical Air Request - Helicopter Request (TAR-HR) Network (HF, VHF). Used by forward ground combat units to request immediate air support from the TACC or the direct air support center (DASC). Intermediate ground combat echelons monitor this net and may modify, disapprove, or approve a specific request. The TACC/DASC uses this network to brief the requesting unit on the details of the mission and

NWP 4-02
4-11 JAN 2008
may pass along target damage assessments and emergency helicopter requests. In the initial stages of an amphibious operation or any MEU (special operations capable) (MEU(SOC)) operation, this may be the only network the unit can use. This network is monitored in the flagship’s LFOC.
4. Helicopter Direction Network (UHF, VHF, HF)). Used by the helicopter direction center (HDC) for positive control of inbound helicopters in the amphibious objective area (AOA). The radar controller in the HDC uses this network to direct the flight course and altitude of helicopters, holdings, let downs, and climb outs, when required. This is where inbound casualty details can be communicated; it is monitored in the flagship HDC.
5. Air Force AE Communications Capabilities. An Air Force aeromedical evacuation liaison team (AELT) provides support between the forward user and the AE system in the form of operational and clinical interface. AELTs may be assigned to locations that do not otherwise have Air Force personnel, such as a hospital ship and an EMF. The AELT includes communications personnel who will be integrated into the airlift operations element and may augment the HSS unit with robust communications capabilities. Other communications capabilities may be provided by mobile aeromedical staging facilities (MASFs).
6. Miscellaneous. Increasingly sophisticated computer networks that provide communications capabilities are medical department local area networks (LANs), ship’s LANs, wide-area networks (WANs), the World Wide Web (www), the Non-Secure Internet Protocol Router Network (NIPRNET), the SECRET Internet Protocol Router Network (SIPRNET), STU-III, and iridium/satellite phones.
4.3.4 Patient Evacuation
The DASC and patient evacuation team (PET) receive MEDEVAC requests via the NATO 9-line CASEVAC request over the TAR-HR network or alternate communication network. The PET then determines the appropriate means of patient movement and destination HSS facilities. If air is the appropriate evacuation means, the DASC coordinates air support. If ground evacuation is required or more appropriate, the PET informs the requesting unit to coordinate patient movement with G-4 and assists as necessary. The PET tracks all patient movement through completion of the mission. Depending on the size of the operation, the PET may assume responsibility only for patient movement to FRC capability. The medical support operations center or higher regulating authority will assume movement above FRC capability. Detailed information for patient movement is contained in Annex Q of an OPLAN or OPORD.
4.3.5 Communications Issues
The recurring communications findings/observations for expeditionary HSS units include limited availability of radio capabilities for a dedicated medical network, lack of bandwidth, limited access to SIPRNET, and difficulty in obtaining message release approval. During OIF, CASEVAC communications on the TAR-HR network were often crowded out by other traffic and/or provided insufficient information. Bandwidth is a recurring problem, necessitating coordination with communications personnel to ensure that sufficient time and space are available for transmission of medical data. Some medical communications, such as telemedicine and medical data transfer (x rays), may consume a significant amount of bandwidth.
Limited SIPRNET availability may hamper the necessary transfer of patient information or coordination among different HSS units in a TF, particularly if those units are part of a coalition. Operational commanders must ensure that provisions are made to grant expeditionary HSS units access to SIPRNET to the extent practicable in theater. In some cases, COs/OICs of HSS units are required to go through the Marine unit commander, ship’s CO, or ship’s Master to obtain message release approval. Consideration should be given to providing COs/OICs of deployed MTFs message release authority.
Emerging medical technologies will create even greater demands on the command, control, communications, computers, and intelligence (C4I) system. These technologies include computer-based patient records, telemedicine, personal information carrier, and the ability to link all health care and surveillance data in theater

NWP 4-02
JAN 2008 4-12
from first responder through forward resuscitative surgery, theater hospitalization, en route care, and definitive care. Planners must develop backup communications means for medical regulating communications.
4.4 HOMELAND SECURITY
USNORTHCOM was established in 2002 as a single unified command to consolidate existing missions that were previously executed by other military organizations. The command’s mission encompasses homeland defense and civil support to execute the following tasks:
1. Conduct operations to deter, prevent, and defeat threats and aggression aimed at the United States, its territories, and its interests within the assigned AOR.
2. Provide military assistance, including consequence management operations, to civil authorities as directed by the President or the SecDef.
3. Direct the homeland defense mission against military threats emanating from OCONUS.
4. Conduct military civil support missions to include domestic disaster relief operations subsequent to large-scale natural or technological disasters. Support also includes counterdrug operations and consequence management assistance, such as support after a terrorist event employing a weapon of mass destruction.
4.4.1 Humanitarian and Civic Assistance
For domestic emergencies and disasters, the lead federal agency (LFA) is either the Federal Emergency Management Agency (FEMA) or the Federal Bureau of Investigation (FBI). The State Department serves as the primary agency for foreign consequence management, including HCA operations. In some cases, DOD components or military commanders may provide immediate response to save lives, prevent human suffering, or mitigate property damage under imminently serious conditions, as described in DODD 3025.15, Military Assistance to Civil Authorities. Generally, an emergency must exceed the management capabilities of local, state, and other federal agencies before military forces are committed to these operations. JTFs are established to provide HCA and CS operations and are subordinate to the CCDR.
4.4.2 Health Service Support
The LFA, typically FEMA, initiates requests for HSS during disasters in CONUS and forwards them for execution to the director of military support in the Office of the Army Deputy Chief of Staff, Operations and Plans; to the SecDef; and to the CJCS. The CJCS validates the request prior to assignment to USNORTHCOM. USNORTHCOM in turn tasks USJFCOM, as a supporting command, to identify and procure military HSS capabilities from the Services. OPNAV N931 validates USJFCOM requests before specific tasking to BUMED for assignment of specific deployable capabilities. The process continues as described in Paragraph 2.5.2 for any unified commander requesting medical support for a contingency.
Conditions to consider for disaster relief include:
1. HSS assistance requires rapid assessment of the damage caused by the disaster and rapid tailoring of an HSS element to meet the needs of the affected populace.
2. The HSS element should have a wide range of specialties available.
3. The HSS response must be able to reach the disaster site rapidly, with the right mix of specialties, and be coordinated with concerned agencies.

NWP 4-02
4-13 JAN 2008
4.5 PATIENT MOVEMENT
The fundamental precept of patient movement is that only essential care is provided in theater in order to stabilize patients for evacuation to higher capabilities of care outside the theater. The SecDef, in coordination with the CCDR, sets the theater patient movement policy prior to execution of the OPLAN. CCDRs are responsible for patient movement within their theater. They execute the OPLAN and adjust the theater patient movement policy as required.
USTRANSCOM is the DOD single-point manager for intertheater and CONUS patient movement services, responsible for validating all patient movement requests and coordinating with appropriate lift agencies to meet requirements. USNORTHCOM is responsible under USTRANSCOM for patient movement within CONUS. Each Service is responsible for organizing, training, and equipping their forces to ensure the capability to meet patient movement requirements.
The SecDef and CJCS evacuation policy is 7 days for the combat zone (CBTZ), operation zone (OPZONE) I, and 15 days for the communications zone (COMMZ). The medical operations zone is the immediate COCOM AOR, and the medical communications zone is outside the immediate COCOM AOR or in a neighboring COCOM AOR. Patients not expected to return to duty within the number of days expressed in the theater patient movement policy will normally be evacuated:
1. As soon as their medical condition permits or when local stabilization capabilities have been reached
2. When medical authorities have determined that travel will not exacerbate their medical condition
3. When suitable receiving MTFs and transportation have been arranged.
Per NTTP 4-02.2M/MCWP 4-11.1G, Patient Movement, the patient movement system consists of three components: medical regulating, patient evacuation, and en route care. The goal of the patient movement system is to move patients from the point of injury or illness into and through the established HSS system as rapidly as possible. The guiding principle is that patients will be moved only as far rearward as the tactical situation or patient’s condition dictates. Prompt movement of patients to the required capability of clinical care is essential to avoid increased morbidity and mortality.
4.5.1 Patient Regulating
Patient regulating is defined as the actions and coordination to arrange for the movement of patients through the capabilities of care. This process matches patients with an MTF that has the necessary HSS capabilities and ensures that bed space is available. Medical regulating should occur at the headquarters that controls the means of evacuation. Operating forces’ HSS liaison services offices may assist with treatment and movement of patients. Afloat units should refer to the standing OPLANs, OPORDs, or SOPs for information regarding patient movement and medical regulating policies.
4.5.2 Patient Evacuation
Patient evacuation is the timely and efficient transportation of injured or ill personnel from the immediate AO to HSS facilities and between HSS facilities as required. In the lower levels of the continuum of care, patients are moved to the nearest HSS facility; in the higher levels, patients are regulated to a designated facility. CASEVAC refers to the movement of unregulated casualties aboard vehicles or aircraft. MEDEVAC refers to Service patient movement using predesignated tactical or logistic aircraft temporarily equipped and staffed with HSS attendants for en route care. USAF AE provides fixed-wing movement using organic airframes with AE aircrew specifically trained for this mission.

NWP 4-02
JAN 2008 4-14
Within each capability of care, patient movement is defined as follows:
1. Point of injury to FRC capability. In general, component commands are responsible for CASEVAC from point of injury to first responder capability and casualty movement to forward resuscitative care via dedicated, designated, or opportune ground or air transportation. The Marine Corps has some dedicated ground evacuation and relies on designated air and other lifts of opportunity.
2. FRC capability to theater hospitalization capability. Movement within and from forward resuscitative care is normally a Service component responsibility; however, some operations may require evacuation by the joint common user patient movement system. For example, the Marine Corps has no organic HSS capabilities beyond the FRC capability and relies on the Navy for care beyond this capability. The Navy does not have dedicated evacuation capabilities to retrieve patients from FRC capability and evacuate them to a higher capability. In this case, Army and Air Force evacuation capabilities may support the Navy and Marine Corps.
3. Theater hospitalization capability to definitive care capability. If a patient cannot be returned to duty within the limits of the theater patient movement policy, the casualty will require patient movement to another MTF for more definitive care and disposition. The originating MTF will submit a patient movement request to the appropriate Joint Patient Movement Requirements Center (JPMRC) to identify intratheater patient movement requirements.
Basic tenets of patient movement are as follows:
1. Patients generally are not evacuated farther rearward than their medical condition requires or the tactical situation dictates.
2. Supporting HSS units are responsible for evacuation of patients from HSS units forward of the supporting unit’s position.
3. The Service component commander is responsible for evacuation of patients to hospitals in their operational area.
4. The unified command is responsible for movement of patients among transportation facilities within their AOR.
5. The unified commander is responsible for issuing procedures for evacuation of formerly captured or detained US personnel.
6. The unified commander will issue procedures for the evacuation of detainees. The sick and injured detainees are treated and evacuated through normal medical channels but remain physically separated from allied patients and those of the United States.
Within the medical operations zone, patient evacuation is the responsibility of component commands from first responder through definitive care capability. The JPMRC is responsible for coordinating patient evacuation in the medical operations zone. Surface craft (land or water) or aircraft move patients. Within the AOR, medical regulating is accomplished at the theater level. Tactical AE from the medical operations zone (theater hospitalization capability) to definitive care capability is normally the responsibility of the supporting Air Force component.
4.5.2.1 Intratheater/Tactical Aeromedical Evacuation
Intratheater evacuation is the movement of patients between HSS facilities in the medical operations zone and the medical communications zone. Patients may be regulated as required from FRC capabilities to theater hospitalization capabilities by the medical regulating control center (MRCC), and among definitive care capabilities by the JPMRC.

NWP 4-02
4-15 JAN 2008
Note
Patients are not regulated from first responder to forward resuscitative care; they are evacuated. At this capability of care, only flowthrough beds exist. True hospital beds exist only at theater hospitalization capability and above. Forward resuscitative care holding beds are cots. Normally, these facilities may hold patients for up to 72 hours only.
During routine deployments, the TF surgeon will coordinate evacuation of patients between the requesting unit and appropriate shore-based MTFs. During combat operations, the TF MRCO will coordinate the evacuation and regulation of patients to MTFs. The AELT will coordinate the evacuation and regulation of patients among MTFs with the JPMRC.
1. Aeromedical evacuation transportation responsibilities. CRTS aviation capabilities are used to transport patients between the battlefield and supporting ships at sea during amphibious operations. The Marine Corps has no dedicated air ambulances but designates some rotary-wing or fixed-wing aircraft for that mission. The ERCS will provide the Marine Corps with an organic evacuation capability. The operational commander is responsible for providing air transportation for patient evacuation.
The Navy and Marine Corps have doctrinal responsibility for ship-to-shore and shore-to-ship movement of patients. However, the Army is responsible for providing dedicated medical rotary-wing support for all ship-to-shore and shore-to-ship patient transport to and from hospital ships. In joint operations, the Army is tasked with providing elements of an Army medical company (air ambulance) to theater hospitalization facilities (EMFs, hospital ships). In the event the Army cannot support this requirement, patients will be evacuated to hospital ships by lifts of opportunity or designated aircraft. AE to CRTSs is provided by Navy and Marine Corps lifts of opportunity or, in some cases, Army helicopters.
Primary CRTSs (LHAs and LHDs) have significant helicopter support facilities. The helicopter facility on hospital ships can accommodate certain types of helicopters as described in NTTP 4-02.6, Hospital Ships. Helicopter support on the hospital ships includes air traffic control in airspace adjacent to the ship, flight deck services for landing, casualty handling, helicopter handling, firefighting and crash rescue, and ondeck refueling.
During large-scale operations (joint and coalition), the unified commander is responsible for establishing a theater aeromedical evacuation system (TAES). The primary mission of the TAES is to transport patients by air from forward airfields in the medical operations zone to points of definitive medical care within the medical operations zone, and from the medical operations zone to HSS facilities in the medical communications zone. The Air Force is responsible for providing fixed-wing AE.
For strategic evacuation, the Air Force has AE teams that handle stabilized patients. The teams are typically stationed at forward-deployed expeditionary AE squadrons, staffed with three 3-person teams consisting of a doctor, nurse, and respiratory technician. The teams are responsible for patient collection, injury stabilization, airborne en route care, and transfer to the next capability of medical care.
2. Sea (waterborne) evacuation. During the initial phase of amphibious operations when aircraft are heavily involved in moving and supporting combat forces, patients may be evacuated from the beach on boats. Patients evacuated to a CRTS or hospital ship via boat will usually be staged at a beach evacuation station (BES) awaiting transportation. Waterborne transportation must be provided by the Navy component commander.
4.5.2.2 Intertheater/Strategic Evacuation
USTRANSCOM is responsible for intertheater/strategic evacuation. Strategic AE capabilities may consist of dedicated and/or opportune aircraft equipped and staffed for patient evacuation. The Air Force is the lead Service for strategic evacuation. Expeditionary HSS units must coordinate AE with an AELT and an air force aeromedical

NWP 4-02
JAN 2008 4-16
staging facility (ASF) or MASF. The Air Force in theater establishes these HSS facilities to coordinate the entry of patients into the TAES and temporarily hold patients prior to strategic AE. Patients will be transported to these facilities for strategic evacuation. If the HSS unit has insufficient transportation capabilities (e.g., when no Army medical company, air ambulance, or detachment is available to move patients from its facility to the ASF/MASF), it should request sufficient capabilities from the theater commander via the chain of command. Upon request, the Air Force will assign an AELT to a hospital ship. The AELT will provide strategic AE coordination services.
4.5.3 Patient Movement Considerations for Special Operations Forces
USSOCOM is responsible for patient evacuation, but not medical regulating. The OPLAN should contain specific information on SOF patient evacuation and medical regulating. Because of the nature of SOF operations, SOF aviation elements may be the primary means of tactical AE. The SOF command element will coordinate with appropriate HSS personnel to coordinate SOF evacuation. Whenever feasible, the established HSS system will provide evacuation support for SOF the same as for conventional forces.
4.5.4 Patient Movement Items
PMIs are HSS equipment and durable supplies. They include ventilators, litters, patient monitors, and pulse oximeters. The originating MTF will provide the PMIs that are required to support the patient during evacuation. PMIs will remain with the patient until arrival at the destination MTF. An exchange system should be established in the OPLAN to address the return of PMIs to the originating MTF. PMI centers and cells receive, refurbish, redistribute, and return equipment and supplies collected from MTFs.
4.5.5 Health Care in Remote Locations
In a country or territory served by a DOD MTF, the MTF is contacted first to determine its ability to care for the patient. At sea, when no US military health care MTF exists, it is customary to evacuate the ill and injured to non-US health care facilities in foreign countries. The TRICARE global remote overseas (TGRO) contract provides urgent and emergent health care through health care contracts. This service is available to active duty Service members, regardless of their parent command or TRICARE enrollment status, who are deployed, temporary additional duty (TAD) or temporary duty (TDY), or in an authorized leave status in remote overseas locations, such as in countries in which there are no DOD MTFs. The patient’s command refers the patient directly to TGRO contract providers in remote OCONUS locations for urgent or emergent health care.
4.6 CHEMICAL, BIOLOGICAL, RADIOLOGICAL, AND NUCLEAR DEFENSE OPERATIONS
The potential use of CBRN weapons or agents against US forces, the US homeland, or US interests overseas and the resulting severe consequences have become of increased concern. The presence of chemical or biological agents, radioactive fallout, or toxic industrial materials, or the possibility of exposure to these elements, forces afloat and ashore units into a protective posture that degrades mission capability. The wearing of mission-oriented protective posture (MOPP) gear, especially at higher protection levels, results in body heat buildup, reduced mobility, and increased wearer fatigue, thereby degrading an individual’s ability to care for patients and a unit’s medical effectiveness. Decontamination of patients and unique transportation requirements also cause treatment and evacuation delays. Clinical and logistical medical management of patients is extremely difficult to provide in a CBRN contaminated environment. The operational commander should make every effort to station expeditionary HSS units in low-threat areas to minimize the possibility of CBRN warfare and associated contamination impacts on medical capabilities. All units, however, must be equipped for minimal protection and decontamination capability.
For further information on chemical, biological, and nuclear defense operations, refer to FM 4-02.7/NTTP 4-02.7/AFMAN 44-149(I)/MCRP 4-11.1F, Multiservice Tactics, Techniques, and Procedures for Health Service Support in a Nuclear, Biological and Chemical (NBC) Environment (draft).

NWP 4-02
4-17 JAN 2008
4.6.1 Chemical, Biological, Radiological, and Nuclear Defense
Defense against attacks by these unconventional CBRN weapons requires active and passive defensive measures. Active defense includes offensive actions taken to prevent the conventional and unconventional delivery of CBRN weapons. Passive defense measures are required to reduce vulnerability and minimize the effects of CBRN weapons employed against host-nation installations, any US installation and facility, and POE/POD.
CCDRs are responsible for effectively employing appropriate CBRN defensive measures such as early and avoidance warning systems, unique operations security protocols, new individual and collective protection procedures, and improved HSS response capabilities in the areas of CBRN detection, reporting, and decontamination. Shipboard response to a radiological attack is similar to that of a chemical or biological attack. The primary difference is the need to set up and establish radiological monitoring stations. The tenets, or operational attributes, of joint CBRN defense are sense, shape, shield, and sustain. (See Figure 4-1 for a depiction of these attributes.)
Figure 4-1. Joint CBRN Defense Functional Concept — Operational Attributes

NWP 4-02
JAN 2008 4-18
For further information on chemical, biological, radiological, and nuclear defense, refer to JP 3-40, Joint Doctrine for Combating Weapons of Mass Destruction. Shipboard damage control manuals, such as NTTP 3-20.31.470/Naval Ships’ Technical Manual (NSTM) Chapter 470, Shipboard Biological Warfare/Chemical Warfare Defense and Countermeasures; NSTM 070, Nuclear Defense at Sea and Radiological Recovery of Ships After Nuclear Weapons Explosion, and NAVAIR 00-80T-121, Chemical and Biological Defense Naval Air Training and Operating Procedures Standardization (NATOPS) Manual, delineate CBRN defensive procedures.
Additional medical guidance is found in FM 4-02.7/NTTP 4-02.7/AFMAN 44-149(I)/MCRP 4-11.1F, Multiservice Tactics, Techniques, and Procedures for Health Service Support in a Nuclear, Biological and Chemical (NBC) Environment (draft). Additional biological warfare surveillance guidance is found in FM 3-11.86/NTTP 3-11.31/AFTTP(I) 3-2.52/MCRP 3-37.1C, Multiservice Tactics, Techniques, and Procedures for Biological Surveillance. Tactics, techniques, and procedures, and radiation health protection and radioactive contamination personnel management procedures are provided in NAVMED P-5055, Radiation Health Protection Manual, and BUMEDINST 6470.10 (series), Initial Management of Irradiated or Radioactivity Contaminated Personnel.
4.6.1.1 Preattack Defensive Measures
HSS personnel should train to operate in a CBRN environment, know how to survive an attack, and know how to care effectively for casualties. Pre-exposure prophylaxis against suspected biological agents through immunizations or administration of antibiotics, administration of antidote enhancers, or pretreatments against chemical agents are essential defensive measures. Contamination avoidance, such as storing Class VIIIA supplies and equipment in protected areas or in covered storage containers, is also important.
4.6.1.2 Postattack Measures
Following a CBRN weapon attack, patients, who could include HSS personnel, must be treated. All patients receiving treatment must be checked for CBRN contamination, and then decontaminated before entry into clean areas to reduce hazards to HSS personnel. Those who have injuries that are life-threatening and who require treatment before decontamination are treated in the HSS area of the decontamination station.
1. Nuclear warfare environment. Casualties of a nuclear attack will likely have incurred blast, thermal, and/or radiation injuries. These casualties will occur quickly, and locally available means for early resuscitative care may be inadequate. At the time of triage, it will be impossible to predict which patients with thermal or blast injuries will develop radiation sickness. Additionally, it will not always be possible to determine the dosage of radiation they have received. Radiation casualties include:
a. Irradiated. Exposed to ionizing radiation but not contaminated, such as exposure to initial nuclear radiation. These casualties are not radioactive and pose no danger to HSS personnel.
b. Externally contaminated. Radioactive dust and debris on clothing, skin, or hair, which may present a threat to HSS personnel. After lifesaving care is provided, the externally radiated casualty must be decontaminated as soon as possible. Simply removing clothing and footwear eliminates 90 percent of radiation contamination.
c. Internally contaminated. Ingestion or inhalation of radioactive materials, or entry through an open wound. This type of casualty presents a lower possibility of risk to HSS personnel due to the shielding effects of the patient’s body.
For further information on the treatment of nuclear and radiological casualties, refer to FM 4-02.283/NTRP 4-02.21/AFMAN 44-161(I)/MCRP 4-11.1B, Treatment of Nuclear and Radiological Casualties.
2. Biological warfare environment. Under biological warfare conditions, the control of epidemics will be of paramount importance. Initial diagnosis of disease due to a biological agent may be difficult if the attack was covert. Initial signs and symptoms may mimic more common, benign diseases. Passive defensive

NWP 4-02
4-19 JAN 2008
measures, including immunizations, good personal hygiene and sanitation, and the use of repellants and protective masks all lessen the incidence of biological agents. Incoming patients and equipment must be checked for contamination, and ventilation systems must be secured as necessary. To prevent contamination of HSS personnel, soap and water usually suffice to decontaminate patients and equipment exposed to biological agents. Keeping units on location will prevent the spread of contamination to unaffected areas.
For further information on the treatment of biological warfare agent casualties, refer to FM 8-284/NTRP 4-02.23/AFMAN 44-156(I)/MCRP 4-11.1C, Treatment of Biological Warfare Agent Casualties.
3. Chemical warfare environment. The handling of patients contaminated with chemical agents presents the greatest threat to HSS personnel and may require wearing MOPP gear for long periods. Decontamination will be time consuming and will create heavy demands on manpower for which medically trained personnel cannot be spared. Disposal of contaminated clothing and supply of clean clothing and decontaminants will pose logistical issues. The movement of the MTF to a clean environment is essential for HSS to be effectively provided.
For further information on the treatment of chemical casualties, refer to FM 4-02.285/NTRP 4-02.22/AFMAN 44-149(I)/MCRP 4-02.1E, Treatment of Chemical Agent Casualties and Conventional Military Chemical Injuries (draft).
4.6.2 Chemical, Biological, Radiological, and Nuclear Defense Training
Augmenting HSS personnel receive CBRN defense and orientation training in consequence management per OPNAV direction. This CBRN-related training is also offered by activities such as the NEPMU’s and MSC’s afloat training teams. Additionally, policy directs that all primary care clinicians receive at least 12 hours of training in the identification and management of chemical and biological casualties (see BUMED MSG 171921Z DEC 01). All privileged providers, including dental officers, are required to receive at least two hours of training in the identification and initial management of chemical and biological casualties.
Navy CBRN educational opportunities include but are not limited to: Navy Chemical, Biological, and Radiological Defense (CBR-D) Afloat Operations Specialist and Disaster Preparedness Ashore Operations Specialist. Also available are CBR-D training online and links to training on the NAVSEA webpage at: https://www.cbrd.navy.mil.
In addition, the Navy Medicine Office of Homeland Security provides training and exercises through its Disaster Preparedness, Vulnerability Analysis, Training and Exercise (DVATEX) Program. HSS personnel assigned to MARFOR units receive CBRN defense and consequence management training at Field Medical Service School. Navy HSS department officer personnel normally receive limited CBRN-related training during the Combat Casualty Care Course or while assigned to MARFOR units.
4.6.3 Patient Decontamination
In a CBRN environment, physical decontamination of casualties prior to transport to HSS units is the responsibility of line units. HSS units may receive patients who have residual contamination. These units must have personnel trained and equipped to handle contaminated patients. The objectives of patient decontamination are to:
1. Manage casualties to minimize the effects of chemical agent exposure without exacerbating injuries or illnesses
2. Protect persons handling contaminated casualties or working in contaminated areas
3. Control the spread of contamination
4. Continue the HSS mission.

NWP 4-02
JAN 2008 4-20
4.6.3.1 Decontamination Planning
HSS units should have a mass casualty plan that can be modified to meet varying situations. Decontamination should be decentralized to avoid a backup of casualties awaiting decontamination at a central location. Each medical facility should be able to establish its own decontamination area. Approximately 90 percent of all decontamination can be performed without interfering with medical treatment, simply by removing a casualty’s outer clothing and footwear. Expeditionary HSS personnel should be prepared to support patient decontamination efforts through participation in determining personnel and materiel requirements, augmenting decontamination stations with trained medical personnel, and conducting frequent decontamination procedure exercises. HSS personnel should be trained to manage and treat casualties in a contaminated environment, and to prevent the spread of contamination to clean areas. Nonmedical personnel require training in patient transport, handling, and decontamination procedures.
4.6.3.2 Decontamination Procedures
All casualties received from areas where chemical or biological agents have been employed shall, in the absence of compelling evidence to the contrary, be viewed as contaminated. Contaminated patients should not enter the MTF or transfer to another facility prior to thorough decontamination. Ambulatory casualties may be processed through personnel decontamination stations. Litter patients require a greater degree of medical supervision. Emergency treatment prior to decontamination is extremely challenging and difficult due to the interference of individual protection equipment and contamination issues.
Procedures for the assessment, management, and treatment of individuals who are irradiated or internally radioactively contaminated are described in BUMEDINST 6470.10 (series), Initial Management of Irradiated or Radioactively Contaminated Personnel. FM 3-11.5/NTTP 3-11.26/AFTTP(I) 3-2.60/MCWP 3.37.3, Multiservice Tactics, Techniques, and Procedures for Chemical, Biological, Radiological, and Nuclear Decontamination, provides general guidance on CBRN decontamination procedures. FM 4-02.7/NTTP 4-02.7/AFMAN 44-149(I)/ MCRP 4-11.1F, Multiservice Tactics, Techniques, and Procedures for Health Service Support in a Nuclear, Biological and Chemical (NBC) Environment (draft), provides detailed guidance on patient decontamination. (See Paragraph 4.2.7 for information on handling contaminated remains.)
4.7 SECURITY/FORCE PROTECTION
4.7.1 External Security
Expeditionary HSS units generally have little organic security capability; therefore, the operational commander is responsible for providing external security. Forward deployed units, such as FRSSs, STPs, EMFs, and FDPMUs, will typically accompany Marine combat elements and should be protected by those elements. However, the forward deployed units may be more exposed to enemy fire by virtue of their forward positions. These forward HSS units must plan for the possibility of self-protection. As demonstrated in OIF, HSS personnel assigned to forward units must have the training, equipment, and will to defend themselves and their patients. The SG has mandated combat skills/force protection training for deployable units.
Conversely, EMFs and hospital ships may be located in the company of rear combat support elements or in an isolated area without significant security support nearby. Choosing the operating area for the EMF and hospital ship is a critical consideration for force protection. The hospital ship may embark a military security detachment for additional force protection, particularly during transit of areas where the risk of attack from small boats or other threats may exist. COMSC Washington DC 272119Z May 03 provides guidance on the areas of authority of the ship’s Master, who is responsible for ship’s security and the military security detachment. Seabees provide additional security for EMFs.
4.7.2 Internal Security
EMFs and hospital ships have a master-at-arms (MAA) force for internal security duties. The table of equipment provides weapons sufficient to meet the MTF’s own security needs, including M-16 rifles and 9 mm pistols. Only

NWP 4-02
4-21 JAN 2008
weapons-qualified personnel are issued or allowed to use these weapons. All members of the MAA force will be weapons-qualified prior to assignment to the MTF.
4.7.3 Security Training
All expeditionary HSS units should have security plans that address security precautions, threat response, and disaster recovery. In addition, each unit should have a force protection officer (FPO) and antiterrorism training officer (ATTO). The FPO/ATTO is responsible for conducting Level I antiterrorism/force protection awareness training for the unit per the guidelines of DODI 2000.16, DOD Antiterrorism (AT) Standards. This training consists of training videos, handouts, and a threat brief applicable to the AOR and is annotated in the service records of MTF personnel. HSS units deployed to forward areas should ensure that all personnel receive small arms indoctrination.
4.7.4 Visitor and Patient Security
All visitors are subject to a security check upon entry to an EMF or hospital ship and are escorted during their visit. All patients, even the critically ill, are subject to a security check upon arrival. Security checks involve an identification check, determination as to the purpose of the visit, and visual inspection for concealed weapons. Patients and visitors often arrive with weapons. Those weapons are turned over to security personnel for temporary storage in the armory, if one is available. In the case of expeditionary HSS units serving with line units, weapons should be turned over to the line unit for custody and storage.
Since the EMF and hospital ship armories are designed to accommodate only weapons organic to the hospital, the MTF CO should be prepared to make other arrangements for patient and visitor weapons storage if volume exceeds existing capacity. Given that patients may be admitted and weapons storage required for an extended period, the patient’s weapon should be turned over to individuals accompanying the patient. If the MTF ever accepts custody of a weapon, custody transfer should be documented before the weapon is turned over to another organization. For those weapons accumulated by the MTF, a mechanism must be established with line combat support units to coordinate weapons transfer back to the line.
4.8 DETAINEES
DODD 2310.01E, The Department of Defense Detainee Program, defines detainee as any person captured, detained, or otherwise under the control of DOD personnel (military, civilian, or contract employee). The definition does not include persons being held primarily for law enforcement purposes. As a matter of policy, all detainees will be treated IAW the principles applicable to enemy prisoners of war (EPWs) unless or until a more precise legal status and accordant treatment are determined by competent authority. Priority of care will not be given to US and allied military force patients over detainee patients unless dictated by medical reasons. Triage by competent medical personnel is the only method to determine the priority of treatment.
For detailed guidance on the handling of enemy prisoners of war, retained personnel, civilian internees, and other detainees, all of whom will be referred to as detainees, refer to AR 190–8/OPNAVINST 3461.6/AFJI 31–304/MCO 3461.1, Enemy Prisoners of War, Retained Personnel, Civilian Internees, and Other Detainees.
4.8.1 Detainee Considerations
Providing HSS care to detainees can present a security challenge for expeditionary HSS units. The Army acts as the EA for the theater commander in most theaters of operation for civil affairs, including the handling of detainees. Therefore, the Army is the Service resourced and primarily charged with responsibility for the detainees in theater. Marine Corps doctrine stresses that detainees are turned over to the Army as soon as possible after capture. For this reason, the Marine Corps has limited facilities, staff, and other resources for long-term holding of detainees. Existing resources are only for temporary holding until detainees can be turned over to the Army.

NWP 4-02
JAN 2008 4-22
The doctrinal goal is to move detainees through the system, especially the medical care system, to the HN so that the impact on the HSS system is minimal. With rapidly shifting battle lines resulting from maneuver warfare, future conflicts are expected to produce significant numbers of detainees whom HSS units must consider treating. These categories of personnel are a line responsibility and primarily assigned to the Army, which is staffed and resourced to handle this issue. HSS personnel will not be used as guards. When possible, medical care of detainees will be provided by qualified retained or detained medical personnel from the same nation. Issues for expeditionary HSS units concerning detainees should be addressed to the theater commander’s staff.
4.8.2 Refugee Considerations
Doctrine regarding care for civilian refugees is essentially the same as that for detainees. The Army is the EA for the theater commander for civilian refugees, is resourced through its civil affairs units to handle civilian refugee problems, and is responsible for determining the ultimate disposition of refugees. Because civilian refugee care is funded separately from care of friendly forces and detainees, medical activities in theater cannot provide medical care to civilian refugees without prior theater commander direction and approval. As a rule, only urgent medical treatment within the capability of the deployed multinational medical force and medical treatment not otherwise available will be offered to civilian refugees. In the event that medical infrastructure is lost in the HN, it may be necessary to seek coordination from the Department of State in order to establish the required diplomatic channels to access care and transfer of displaced persons in an alternate country for required care.
Civilian refugees also present a significant potential security issue. As with detainees, expeditionary HSS units are not staffed to provide security for civilian refugees. Any security requirement that the expeditionary HSS unit is unable to meet should be addressed to the theater commander, who will arrange for assistance. Detainees may possibly present medical problems not normally seen by MTF staff, particularly infectious disease problems endemic to less-developed countries. There may also be special religious, messing, berthing, and sanitary requirements.
4.8.3 Captured Enemy Materiel Considerations
Captured enemy materiel (weapons and other war trophies) will normally be handled per Service regulations, including any disposal and reporting procedures. The Army civil affairs staff will be cognizant of these issues and can offer expert advice. For Navy–Marine Corps operations where no Army units are involved, HSS personnel may consult a Marine Corps civil affairs group. This group performs a more limited civil affairs role than an Army civil affairs unit but offers a possible source of assistance.
HSS capabilities and requirements for dealing with captured enemy materiel should be addressed in theater OPLANs. During UN and some coalition operations, the JTF, or the JTF-forward, may not be prepared to handle these issues, particularly if there are no Army civil affairs units or Marine Corps civil affairs group. In anticipation of this problem, the HSS unit should coordinate detailed resolution with the JTF commander, J-2, J-3, JTF surgeon, and allied or coalition staff.
4.9 GENEVA CONVENTIONS
Generally, the four Geneva Conventions of 1949 establish the protections afforded civilians, noncombatants, and the victims of war during international armed conflict. The Geneva Conventions prescribe the manner in which victims of war will be treated, and the conduct for HSS and religious personnel assigned to aid victims. Military and civilian personnel who are in HSS units share in this special protection and have responsibilities under the Geneva Conventions during times of war or conflict.
Expeditionary HSS units should address Geneva Conventions concerns in their SOPs, including procedures covering potential overrun by an enemy attack. The following points are relevant to expeditionary HSS units.
1. HSS units, facilities, and vehicles are marked with a distinctive Red Cross emblem and are afforded special protection. It is important to note that it is not the recognized emblem that conveys the protection,

NWP 4-02
4-23 JAN 2008
but rather the recognition that an item or person is entitled to protected status regardless of the presence of the emblem.
2. HSS personnel are noncombatants under the law of armed conflict (LOAC) and receive special protection.
Note
The Geneva Conventions should not be construed as prohibiting the right to self-defense. HSS personnel are allowed to use lethal self-defense to protect themselves and their patients from attackers using lethal force.
3. Sick or injured detainees must be treated humanely. Under the Geneva Conventions and the LOAC, the detaining power must provide detainees with HSS care.
4. Facilities, materiel, and stores of fixed MTFs, vehicles, and aircraft displaying the Red Cross emblem may not be used for nonmedical purposes. However, vehicles may have dual-purpose use if the protective emblem is removed and there is no attempt to mislead the enemy.
4.9.1 Identification
Expeditionary HSS facilities and vehicles will be marked with the distinctive Red Cross emblem. The direction not to mark should come through the chain of command.
4.9.2 Hospital Ships
Hospital ships enjoy special protection under the Geneva Conventions. The provisions specifically relating to the unique status of hospital ships are contained in the Second Geneva Convention for the Amelioration of the Condition of Wounded, Sick, and Shipwrecked Members of Armed Forces at Sea (GWS-Sea). Article 22 of GWS-Sea provides that military hospital ships may not be attacked or captured under any circumstances, but shall at all times be respected and protected, provided their names and descriptions have been provided to the adversary at least 10 days before they are deployed. This provision extends to hospital ships the immunity conferred on the injured, sick, and shipwrecked. Article 34 of GWS-Sea provides that the protection to which hospital ships are entitled shall not cease unless they are used to commit, outside their humanitarian duties, acts harmful to the enemy. Possession of secret codes for radios or other means of communication by a hospital ship is considered an act harmful to the enemy as noted in the Geneva Convention. The use of encrypted communication is currently in review by JS Legal. In short, hospital ships must refrain from all interference and communication, direct or indirect, during military tactical operations.
For detailed guidance on the applicability of the Geneva Conventions to hospital ships, refer to NTTP 4-02.6, Hospital Ships.
4.9.3 Enemy Prisoners of War
Priority of care will not be given to US and allied military force patients over detainee patients, unless dictated by medical reasons. Triage by competent HSS personnel is the only method to determine the priority of treatment.

NWP 4-02
JAN 2008 4-24
INTENTIONALLY BLANK

NWP 4-02
A-1 JAN 2008
APPENDIX A
Navy Health Service Support Organization
A.1 MISSION AND FUNCTIONS
The activities listed below have responsibility for expeditionary HSS. The OPNAV instructions can be accessed on the Navy directives website, http://doni.daps.dla.mil/. The BUMED instructions are found on the Navy Medicine website, http://navymedicine.med.navy.mil/. (See Figure A-1 for the CHBUMED organization and shore activities responsible for HSS.)
A.1.1 Activities Following OPNAVINST 5430.48 (series), OPNAV Organization Manual
1. Surgeon General of the Navy (N093)
2. Assistant for Dental Matters (N093D)
3. Assistant for Marine Corps Medical Matters (N093M)
4. Medical Resources, Plans, and Policy Division (N931).
A.1.2 Activities Following BUMEDINST 5430.8, Bureau of Medicine and Surgery Organization Manual
1. BUMED
2. Navy Medicine East
3. Navy Medicine West
4. National Capital Area
5. Navy Medicine Support Command.

NWP 4-02
JAN 2008 A-2
Figure A-1. Chief, Bureau of Medicine and Surgery Organization and Shore Activities (Sheet 1 of 2)
Figure A-1. Chief, Bureau of Medicine and Surgery Organization and Shore Activities (Sheet 2 of 2)

NWP 4-02
B-1 JAN 2008
APPENDIX B
Multinational Agreements
B.1 NATO DIRECTIVES
Allied Directive (AD) 85-8, Allied Command Europe (ACE) Medical Support Principles, Policies, and Planning Parameters, provides policy and guidance for planning HSS to multinational, highly mobile, and versatile forces operating in a multidirectional and unpredictable environment. It addresses the operational aspects of HSS and excludes the clinical aspects of care. Its annex provides terms and definitions applicable to NATO HSS.
Military Committee (MC) 326/1, Medical Support, Precepts, and Guidance for NATO, sets forth principles and policies for HSS to allied military forces in operations, and provides guidance on medical support concepts to NATO and national authorities for developing compatible HSS concepts, plans, structures, and procedures. It addresses the operational aspects of HSS and excludes the clinical aspects of HSS care.
B.2 NATO STANDARDIZATION AGREEMENTS
NATO STANAGs address the various aspects of HSS. (See Figure B-1 for a list of NATO STANAGs.) They can be found at the protected website of the NATO Standardization Agency (NSA) at http://nsa.nato.int.
STANAG ALLIED PUBLICATIONS LONG TITLE
1185 Minimum Essential Medical and Survival Equipment for Ship Life Rafts Including Guidelines for Survival at Sea
1208 Minimum Requirements of Emergency Medical Supplies Onboard Ships 1269 AMedP-11 NATO Handbook on Maritime Medicine
1412 Minimum Requirements for a Litter to Transfer Patients Ship-to-Ship to Air
2037 Vaccination of NATO Forces 2040 Stretchers, Bearing Brackets, and Attachment Supports 2048 AMedP-3 Chemical Methods of Insect and Rodent Control 2050 Statistical Classification of Diseases, Injuries, and Causes of Death 2060 Identification of Medical Materiel for Field Medical Installations 2061 Procedures for Disposition of Allied Patients by Medical Installations 2068 Emergency War Surgery 2087 Medical Employment of Air Transport in the Forward Area 2105 AMedP-1(E) NATO Table of Medical Equipment 2121 Cross-Servicing of Medical Gas Cylinders 2122 Medical Training in First-Aid, Basic Hygiene, and Emergency Care 2126 First-Aid Kits and Emergency Medical Care Kits
Figure B-1. NATO Standardization Agreement Publication List (Sheet 1 of 3)

NWP 4-02
JAN 2008 B-2
STANAG ALLIED PUBLICATIONS LONG TITLE
2127 Medical, Surgical, and Dental Instruments, Equipment, and Supplies 2128 Medical and Dental Supply Procedures 2131 AMedP-5(A) Multilingual Phrase Book for Use by the NATO Medical Services
2132 Documentation Relative to Medical Evacuation, Treatment, and Cause of Death of Patients
2136 Minimum Standards of Water Potability in Emergency Situations 2178 Medical Tubing and Connectors in the Field 2179 Minimum Requirements for Medical Care of Women on Ships
2219 Medical Preventive and Protective Measures Associated with Missile Operations
2342 Minimum Essential Medical Equipment and Supplies for Motor Ambulances at All Levels
2345 Evaluation and Control of Personnel Exposure to Radio-Frequency Fields — 3 kHz to 300 GHz
2346 Standard Method of Writing Prescriptions for Spectacles 2347 Medical Warning Tag 2348 Basic Military Hospital (Clinical) Records 2350 Morphia Dosage and Casualty Marking 2357 X Ray, Film Formats, Cassettes, and Screens 2358 First Aid and Hygiene Training in NBC Operations 2361 Minimum Essential Medical Supply Items in Theaters of Operations 2408 AMedP-12 NATO Blood Brochure 2409 AMedP-13 NATO Glossary of Medical Terms and Definitions
2453 The Extent of Dental and Maxillofacial Treatment and Minimum-Essential Dental Field Equipment at the First through Third Echelon
2457 Examination and Treatment of Special Groups of Personnel in Peace 2458 AMedP-14 Handling of Casualties in Extreme Climatic Environments
2461 AMedP-6(C) VOL I NATO Handbook on the Medical Aspects of NBC Defensive Operations (Nuclear)
2462 AMedP-6(C) VOL II NATO Handbook on the Medical Aspects of NBC Defensive Operations (Biological)
2463 AMedP-6(C) VOL III NATO Handbook on the Medical Aspects of NBC Defensive Operations (Chemical)
2464 Military Dental Field Identification
2465 Tasks for the Appropriate Staffing and Training of Dental Officers and Dental Ancillary Personnel for Wartime Operations and Operational Deployments
2466 Dental Fitness Standards and Classification System for Military Personnel
2469 External Fixation Devices for Bone Injuries 2474 Recording of Low-Level Radiation for Medical Staff 2475 AMedP-8(A) VOL I Planning Guide for the Estimation of NBC Battle Casualties (Nuclear) 2476 AMedP-8(A) VOL II Planning Guide for the Estimation of NBC Battle Casualties (Biological)
Figure B-1. NATO Standardization Agreement Publication List (Sheet 2 of 3)

NWP 4-02
B-3 JAN 2008
STANAG ALLIED PUBLICATIONS LONG TITLE
2477 AMedP-8(A) VOL III Planning Guide for the Estimation of NBC Battle Casualties (Chemical) 2478 Medical Support in a Nuclear Environment 2479 Medical Support in a Biological Environment 2480 Medical Support in a Chemical Environment 2481 Medical Information Collection and Reporting 2491 Biological Warfare Immunization Program 2500 AMedP-6(B) NATO Handbook on the Medical Aspects of NBC Defensive Operations 2871 First Aid Materiel for Chemical Injuries 2872 Medical Design Requirements for Military Motor Ambulances
2873 AMedP-7(A) Concept of Operations of Medical Support in Nuclear, Biological, and Chemical Environments
2879 Principles of Medical Policy in the Management of Mass Casualty Situations
2899 Protection of Hearing
2900 Laser Radiation — Medical Surveillance and Evaluation of Over-Exposure
2905 Basic Voltage and Current Characteristics of Electro-Medical Equipment
2906 Essential Physical Requirements and Performance Characteristics of Field Type High Pressure Steam Sterilizers
2908 Preventive Measures for an Occupational Health Program
2937 Survival, Emergency, and Individual Combat Rations — Nutritional Values and Packaging
2939 Medical Requirements for Blood, Blood Donors, and Associated Equipment
2954 Training of Medical Personnel for NBC Operations 2977 Medical Situation Reporting 2979 Essential Characteristics of Electro-Surgical Apparatus 2981 Prevention of Cold Injury 2982 Essential Field Sanitary Requirements
Figure B-1. NATO Standardization Agreement Publication List (Sheet 3 of 3)

NWP 4-02
JAN 2008 B-4
INTENTIONALLY BLANK

NWP 4-02
C-1 JAN 2008
APPENDIX C
Reports
C.1 STATUS OF RESOURCES AND TRAINING SYSTEM
The SORTS reports are required from deployable units with a UIC. Expeditionary HSS unit SORTS reports are required from hospital ships, reserve EMFs, and deployed EMFs. Hospital ship SORTS reports are sent to the MSC TYCOM, and EMF SORTS reports are sent to the fleet force commander/COMUSPACFLT. FSTs are assigned UICs but are not required to submit SORTS reports.
For further information on SORTS reporting requirements, refer to NTTP 1-03.3, Status of Resources and Training System Joint Report — Navy (SORTSREPNV), for EMF SORTS report requirements; and COMSCINST 3501.2 (series), Status of Resources and Training System (SORTS) Reporting for MSC Units, for hospital ship SORTS report requirements.
Effective October 2002 all Navy reporting shifted to the joint SORTS reporting format that uses the TYCOM-managed Training Readiness Management System Afloat software. The SORTS message feeds the Global Command and Control System–Maritime (GCCS-M), which in turn feeds the joint staff database called the Global Status of Resources and Training System (GSORTS).
C.2 REQUIRED MEDICAL REPORTS
HSS units may be required to submit operational reports. The FLTCOM, CJTF, or component commander for the AO should provide reporting guidance through an Annex Q, HSS Annex, or a medical supplement for the operation or exercise. The following reports are the minimum required reports:
1. A joining report provides HSS manning and capability and is classified confidential when completed.
2. A facility spot status report is used to report the status, such as for admissions and manning and supplies for a specified period.
3. Blood and blood request reports are from forward resuscitative care and theater hospitalization facilities that have fresh or frozen blood capability.
4. An actual casualty report is for personnel casualties.
5. An admission to MTF and HN medical facility report documents the movement of personnel to inpatient status.
6. A hospitalization report is followed up on a 24-hour basis until the patient is discharged.
7. A weekly disease surveillance report allows the surgeon to review the disease and injury rate for units during a specified period.
For additional information and examples of HSS reports, refer to NTTP 4-02.2M/MCWP 4-11.1G, Patient Movement. The FHP readiness reports are illustrated in DODI 6490.3, Deployment Health.

NWP 4-02
JAN 2008 C-2
Reports First
Responder Capability
Forward Resuscitative
Care Capability
Theater Hospitalization
Capability
Definitive Care Capability
Joining X Initial X Initial X Initial Facility spot status X x 12 hours X x 12 hours X x 12 hours Blood X Daily X Daily X Daily Blood request X As required X As required X As required Actual casualty X As required X As required X As required X As required Admission to medical treatment facility X As required X As required X As required X As required
Admission to host nation hospital X As required X As required X As required X As required
Disease surveillance X Weekly X Weekly X Weekly
Figure C-1. Medical Reports, Reporting, and Periodicity Requirements
C.2.1 Unit Situation Report
REQUIRED BY COMMANDER, US PACIFIC FLEET (COMUSPACFLT) FOR EXERCISE
1. THE ADMINISTRATIVE REPORTS ARE REQUIRED FROM ALL THEATER HOSPITALIZATION AND DEFINITIVE CARE MTF(S).
A. MEDICAL SITUATION REPORT (SITREP). MEDICAL SITREPs WILL BE SUBMITTED TO COMUSPACFLT FOR COMMUNICATIONS ZONE (COMMZ) UNITS AND BE INCLUSIVE INFORMATION FOR THAT DAY FOR THE PERIOD ENDING 2359Z AND REPORTED BY 0600.
FROM:
TO:
UNCLASS N06300
MESSAGE IDENTIFICATION (MSGID) MEDICAL SITUATION REPORT (MEDSITREP)
ASOFDTG//
1. OPERATING BEDS
2. BEDS AVAILABLE
3. ADMISSIONS
4. OUTPATIENT VISITS
5. SUPPLY SHORTFALL CLASS VIII(A)
6. BLOOD AVAILABILITY AND OR REQUIREMENTS

NWP 4-02
C-3 JAN 2008
7. STAFFING SHORTFALLS
8. DISCHARGES, US MILITARY, US CIVILIANS, OTHERS
A. TO DUTY
B. MEDEVAC
9. MEDICAL INTELLIGENCE ISSUES
10. COMMENTS
C.2.2 Disease Surveillance Report
The purpose of weekly DNBI reporting/tracking is for HSS personnel to review on a routine basis the categories of illness/injury that a unit is experiencing. Most of these categories have proven public health intervention strategies that can help to decrease DNBI in a unit.
Note
The disease surveillance report is designed for DNBIs. Combat-associated injuries should not be included.
1. Weekly tabulations of disease surveillance should be submitted to the Navy forces (NAVFOR) surgeon no later than 1800 each Sunday and 24 hours following the end of the exercise. The reporting period is from 0001 Sunday to 2359 Saturday.
2. The attack rate should be calculated by dividing total weekly cases in each category by average troop strength for the reporting period.
3. Disease, Category, Definition. Diagnoses should be noted and numbered in the comments block.
4. Count each diagnosis, not each visit.
5. Categorize each initial visit, even if not certain of diagnosis.
6. If the diagnosis changes during follow-up visits in the same week, report only the latest diagnosis.
7. If more than one category is determined, such as sexually transmitted disease and gynecologic, report both.
8. Record and note with an asterisk sequential diagnoses or complications, whether in the same category as the initial or not. Record multiple simultaneous diagnoses in one category as a single event, using the most serious or underlying condition. Conditions include:
a. Combat and Operational Stress Reactions (COSR). New (incident) acute reaction to stress and transient disorders that occur without any apparent mental disorder in response to exceptional physical and mental stress. Also includes post-traumatic stress disorder, which arises as a delayed or protracted response to a stressful event or situation of an exceptionally threatening or catastrophic nature.
b. Dermatologic (All). New (incident) diseases of the skin and subcutaneous tissue, including heat rash, fungal infection, cellulitis, impetigo, contact dermatitis, blisters, ingrown toenails, unspecified dermatitis, etc. Includes sunburn. Neoplasms do not constitute an epidemic threat but may be included.
c. Gastrointestinal (Infectious). All new (incident) diagnoses consistent with infection of the intestinal tract. Includes any type of diarrhea, gastroenteritis, stomach flu, nausea/vomiting, hepatitis, etc. Does

NWP 4-02
JAN 2008 C-4
NOT include noninfectious intestinal diagnoses such as hemorrhoids, ulcers, etc. Diarrhea is identified as three or more loose stools in a 24-hour period or one unformed stool associated with fever, bloody stools, abdominal pain, and/or tenesmus.
d. Gynecologic. New (incident) menstrual abnormalities, vaginitis, pelvic inflammatory disease, or other conditions related to the female reproductive system.
e. Heat/Cold Injuries. New (incident) climatic injuries, including heat stroke, heat exhaustion, heat cramps, dehydration, hypothermia, frostbite, trenchfoot, immersion foot, and chilblain.
f. Injury, Recreational/Sports. Any new (incident) injury occurring as a direct consequence of the pursuit of personal and/or group fitness, excluding formal training.
g. Injury, Motor Vehicle Accidents. Any new (incident) injury occurring as a direct consequence of a motor vehicle accident.
h. Injury, Work/Training. Any new (incident) injury occurring as a direct consequence of military operations/duties or of an activity carried out as part of formal military training, to include organized runs and physical fitness programs.
i. Injury, Other. Any new (incident) injury not included in the previously defined injury categories.
j. Ophthalmologic. Any new (incident) acute diagnosis involving the eye, including pink-eye, conjunctivitis, sty, corneal abrasion, foreign body, vision problems, etc. Does NOT include routine referral for glasses (non-acute).
k. Psychiatric, Mental Disorders. Any new (incident) conventionally defined psychiatric disorder as well as behavioral changes and disturbance of normal conduct that is either out of normal character or is coupled with unusual physical symptoms such as paralysis.
l. Respiratory (All). Any new (incident) diagnosis of the lower respiratory tract, such as bronchitis, pneumonia, emphysema, reactive airway disease, and pleurisy; or the upper respiratory tract, such as the common cold, laryngitis, tonsillitis, tracheitis, otitis, and sinusitis.
m. Sexually Transmitted Diseases. All new (incident) sexually transmitted infections, including such diseases as chlamydia, HIV, gonorrhea, syphilis, herpes, chancroid, and venereal warts.
Note
Follow-up and monitoring for HIV and other STDs must be instituted, whether classified as GI or as STD.
n. Fever, Unexplained. New temperature of 100.5 °F or greater for 24 hours, or history of chills and fever without a clear diagnosis. (This is a screening category for many tropical diseases, such as malaria, dengue fever, and typhoid fever.) Such fever cannot be explained by other inflammatory/infectious processes such as respiratory infections, heat, and overexertion.
o. All Other, Medical/Surgical. Any new (incident) medical or surgical condition not fitting into any other defined category.

C
-5 JA
N 2008
NW
P 4-02 Unit Name UIC 2185300.0%
Predominant Location this Week or LAT/Long:
Onboard Total Strength this Week:
Onboard Female Strength this Week: (Need for Gyn calculation.)
Period Covered by this Report (Sun-Sat):
Preparer's Name
Email address
CATEGORY Sunday New Visits
Monday New Visits
Tuesday New Visits
Wednesday New Visits
Thursday New Visits
Friday New Visits
Saturday New Visits
Total for week
Original JCS Ref Rate
NEHC Ground Forces
Reference Rate/1000/Wk
Days of Light Duty
Lost Work Days Admits
Combat/Operational Stress Reactions 0 0 0 0 0 0 0 0 0.1% 1.0Dermatologic--All 0 0 0 0 0 0 0 0 0.5% 9.1 Dermatologic-Unclear 0 0 0 0 0 0 0 0 0.5% 1.0GI - Infectious 0 0 0 0 0 0 0 0 0.5% 3.0Gynecologic 0 0 0 0 0 0 0 0 0.5% 7.4Heat/Cold Injuries 0 0 0 0 0 0 0 0 0.5% 1.0Injury, Rec./Sports 0 0 0 0 0 0 0 0 1.0% 3.0Injury, MVA 0 0 0 0 0 0 0 0 1.0% 1.0Injury, Work/Training 0 0 0 0 0 0 0 0 1.0% 9.1Injury, Other 0 0 0 0 0 0 0 0 1.0% 7.0Ophthalmologic 0 0 0 0 0 0 0 0 0.1% 1.0Psychiatric, Mental Disorders 0 0 0 0 0 0 0 0 0.1% 1.0Respiratory-All 0 0 0 0 0 0 0 0 0.4% 8.3 Respiratory-Lower 0 0 0 0 0 0 0 0 0.4% 1.0Sexually Transmitted 0 0 0 0 0 0 0 0 0.5% 1.0Fever, Unexplained 0 0 0 0 0 0 0 0 0.0% 1.0Neurological 0 0 0 0 0 0 0 0 0.1% 1.0All Other Medical-Surgica 0 0 0 0 0 0 0 0 NA NA
Total DNBI 0 0 0 0 0 0 0 0 4.0% 43.8 Dental 0 NA 6.1Admin, Misc., Follow-up 0 NADefinable 0 NA
Notes: 1. HIGHLIGHTED CELLS REPRESENT THE 5 LINE DAILY CATEGORIES 2. Report initial sick-call visits only. Do not report routine or screening exams. 3. Call Division Preventive Medicine if you have questions.
JCS Category Current Week Ref RateJCS 1 #REF! 0.1%JCS 2 #REF! 0.5%Derm Unclear #REF! 0.5%JCS 3 #REF! 0.5%JCS 4 #REF! 0.5%JCS 5 #REF! 0.5%JCS 6 #REF! 1.0%JCS 7 #REF! 1.0%JCS 8 #REF! 1.0%JCS 9 #REF! 1.0%JCS 10 #REF! 0.1%JCS 11 #REF! 0.1%JCS 12 #REF! 0.4%LRI #REF! 0.4%JCS 13 #REF! 0.5%JCS 14 #REF! 0.0%Neuro #REF! 0.1%JCS 15 #REF! NATotal DNBI #REF! 4.0%
Problems Identified:Corrective Actions:Comments:
Preparer's phone #
WeeklyDNBI
Report
Fleet Weekly DNBI
0.0%0.5%1.0%1.5%2.0%2.5%3.0%3.5%4.0%4.5%
JCS 1
JCS 2
Derm U
nclea
rJC
S 3JC
S 4JC
S 5JC
S 6JC
S 7JC
S 8JC
S 9JC
S 10JC
S 11JC
S 12 LRI
JCS 13
JCS 14Neu
roJC
S 15Tota
l DNBI
JCS Category
Figure C-2. Weekly DNBI Report

NWP 4-02
JAN 2008 C-6
INTENTIONALLY BLANK

NWP 4-02
D-1 JAN 2008
APPENDIX D
Medical Platform Characteristics
WASP (LHD 1) CLASS AMPHIBIOUS ASSAULT SHIP (MULTIPURPOSE)
MEDICAL DEPARTMENT/DIVISION: 4 OFFICERS/19 ENLISTED*
LHD 1 WASP LHD 2 ESSEX LHD 3 KEARSARGE LHD 4 BOXER LHD 5 BATAAN LHD 6 BON HOMME RICHARD LHD 7 IWO JIMA LHD 8 MAKIN ISLAND
LENGTH: 849′ DRAFT: 28′ 8″ DISPLACEMENT: 47,500 tons
ROUTINE STEAMING BEDS ICU: 3/WARD: 10 MOBILIZATION BEDS ICU: 15/WARD: 45 ORS: 6 M+1 MEDICAL AUGMENT: 84
TARAWA (LHA 1) CLASS AMPHIBIOUS ASSAULT SHIP (GENERAL PURPOSE)
MEDICAL DEPARTMENT/DIVISION: 4 OFFICERS/19 ENLISTED*
LHA 1 TARAWA LHA 2 SAIPAN LHA 4 NASSAU LHA 5 PELELIU
LENGTH: 778′ DRAFT: 28′ DISPLACEMENT: 39,300 tons
ROUTINE STEAMING BEDS ICU: 3/WARD: 10 MOBILIZATION BEDS ICU: 15/WARD: 45 ORS: 4 M+1 MEDICAL AUGMENT: 84
Routine Steaming (FST embarked): Medical Department/Division is staffed to man 1 OR and receive 13 patients per day, sustained, based on patient evacuation policy of 24 hours (1 day). Mobilization: Medical Department/Division is staffed to man 4 ORs and receive 60 patients per day for 1 day, 40 patients for 3 days, and 30 patients, sustained, based on patient evacuation policy of 24 hours (1 day).
* Not including FST augmentation: 7 Officers/9 Enlisted
Figure D-1. Medical Platform Characteristics (Sheet 1 of 6)

NWP 4-02
JAN 2008 D-2
HARPERS FERRY (LSD 49) CLASS DOCK LANDING SHIP (CARGO VARIANT)
MEDICAL DEPARTMENT/DIVISION: 2 OFFICER/8 ENLISTED
LSD 49 HARPERS FERRY LSD 50 CARTER HALL LSD 51 OAK HILL LSD 52 PEARL HARBOR
LENGTH: 609′ DRAFT: 19′ 6″ DISPLACEMENT: 16,740 tons
BEDS ISOLATION: 2 INTERMEDIATE CARE (WARD): 8
WHIDBEY ISLAND (LSD 41) CLASS DOCK LANDING SHIP
MEDICAL DEPARTMENT/DIVISION: 2 OFFICER/8 ENLISTED
LSD 41 WHIDBEY ISLAND LSD 42 GERMANTOWN LSD 43 FORT MCHENRY LSD 44 GUNSTON HALL LSD 45 COMSTOCK LSD 46 TORTUGA LSD 47 RUSHMORE LSD 48 ASHLAND
LENGTH: 609′ DRAFT: 19′ 6″ DISPLACEMENT: 15,726 tons
BEDS ISOLATION: 2 INTERMEDIATE CARE (WARD): 8
SAN ANTONIO (LPD 17) CLASS AMPHIBIOUS TRANSPORT DOCK
MEDICAL DEPARTMENT/DIVISION: 2 OFFICER/15 ENLISTED
LPD 17 SAN ANTONIO LPD 18 NEW ORLEANS (Precomm) LPD 19 MESA VERDE (Precomm)
LENGTH: 684′ DRAFT: 23′ DISPLACEMENT: 18,517 tons
OPERATING ROOMS: 2 INTERMEDIATE CARE (WARD): 24
Figure D-1. Medical Platform Characteristics (Sheet 2 of 6)

NWP 4-02
D-3 JAN 2008
AUSTIN (LPD 4) CLASS AMPHIBIOUS TRANSPORT DOCK
MEDICAL DEPARTMENT/DIVISION: 2 OFFICER/9 ENLISTED
LPD 5 OGDEN LPD 7 CLEVELAND LPD 8 DUBUQUE LPD 9 DENVER LPD 10 JUNEAU LPD 12 SHREVEPORT LPD 13 NASHVILLE LPD 14 TRENTON LPD 15 PONCE
LENGTH: 570′ DRAFT: 23′ DISPLACEMENT: 17,000 tons
BEDS ISOLATION: 4 INTERMEDIATE CARE (WARD): 13
BLUE RIDGE (LCC 19) CLASS AMPHIBIOUS COMMUNICATIONS SHIP
MEDICAL DEPARTMENT/DIVISION: 2 OFFICER/15 ENLISTED
LCC 19 BLUE RIDGE LCC 20 MOUNT WHITNEY
LENGTH: 636′ 6″ DRAFT: 30′ DISPLACEMENT: 18,372 tons
BEDS ISOLATION: 4 INTERMEDIATE CARE (WARD): 20
Figure D-1. Medical Platform Characteristics (Sheet 3 of 6)

NWP 4-02
JAN 2008 D-4
MERCY (T-AH 19) CLASS HOSPITAL SHIP
T-AH 19 MERCY T-AH 20 COMFORT
LENGTH: 894′ DRAFT: 32′ 9″ DISPLACEMENT: 69,360 tons
STAFFING BEDS READINESS STATE OFFICER ENLISTED ICU INT MIN TOTAL ORS
PATIENT LOAD PER DAY
I 272 943 100 400 500 1,000 12
300/1 DAY; 200/3 DAYS;
100/DAY SUSTAINED
II 225 711 75 320 105 500 6
150/1 DAY; 100/3 DAYS;
50/DAY SUSTAINED
III 163 550 50 200 – 250 4
75/1 DAY; 50/3 DAYS;
25/DAY SUSTAINED
Patient Onload/Offload Data: lifting patients 1-2 1/2 minutes per lift; 24 flight deck/20 small boat and hoist per hour.
Figure D-1. Medical Platform Characteristics (Sheet 4 of 6)

NWP 4-02
D-5 JAN 2008
LANDING CRAFT AIR CUSHION (LCAC)
AMBULATORY PATIENTS: 12 LITTER PATIENTS: 3 PERSONNEL TRANSPORT MODULE (PTM) CAPABLE
Litters are stacked three high in helos and LCAC (PTM); ensure craft has stanchions to support multiple litters.
GENERAL MEDICAL CHARACTERISTICS
TYPE RANGE SPEED LITTER* AMBULATORY* Amphibious Assault Vehicle (AAV) 300 20 12 25 Engineer Support Vehicle (ESV) 300 40 0 18 LCAC (with patient module) 200 45 55 110 Landing Craft, Mechanized (LCM) 6 130 10 24 48 LCM 8 190 10 24 48 Landing Craft, Utility (LCU) 1,110 12 24 48 * Capacity is the maximum for each type of patient.
PTM CHARACTERISTICS
NOMINAL DIMENSIONS IN FEET
FOOTPRINT PTM TYPE
MAXIMUM SEATING/
LITTER CAPACITY* LENGTH WIDTH HEIGHT SQ
FT CU FT
WEIGHT LBS — EMPTY
MODULES PER SET REMARKS
6X3 180/54 42.6 18.8 6.8 868 5,906 11,215 1
5X3 150/45 38.6 18.8 6.8 725 4,934 9,685 1 Plus 1 3X1
4X3 120/36 31.0 18.8 6.8 582 3,963 8,155 1 Plus 1 3X1 or
3X2 3X3 90/27 23.4 18.8 6.8 439 2,991 6,625 2 2X3 60/18 15.8 18.8 6.8 297 2,091 5,095 2 1X3 30/9 8.2 18.8 6.8 154 1,048 3,780 2
Figure D-1. Medical Platform Characteristics (Sheet 5 of 6)

NWP 4-02
JAN 2008 D-6
MEDICAL EVACUATION ASSETS AND CAPABILITIES
CLASS: Fixed-Wing Air Assets
SERVICE: Various
MISSION: Provide air evacuation of casualties
UNITS IN SERVICE: Various
GENERAL MEDICAL CHARACTERISTICS
TYPE RANGE SPEED LITTER* AMBULATORY* C-5 Galaxy 5,940 541 0 70 C-12 Huron 1,824 300 0 8 C-17A Globemaster 5,200 518 48 44 U-21 Ute 2,306 426 3 10 C-27A Spartan 1,727 288 27 34 C-130 Hercules 2,350 374 70 85 C-141B Starlifter 6,390 495 103 147 CRAF Boeing 767 3,745 535 111 111 * Capacity is the maximum for each type of patient.
MEDICAL EVACUATION ASSETS AND CAPABILITIES
CLASS: Rotary and Tilt-Wing Air Assets
SERVICE: Various
MISSION: Air capable of transporting patients
UNITS IN SERVICE: Various
GENERAL MEDICAL CHARACTERISTICS
TYPE RANGE SPEED LITTER* AMBULATORY* CH-47D Chinook 490 163 24 33 UH-60A/Q Blackhawk 373 184 6 7 CH-46 Sea Knight 132 167 15 25 CH-53D/E Sea Stallion 1,120 150 24 55 V-22 Osprey (Notional) 500 327 12 24 * Capacity is the maximum for each type of patient.
Figure D-1. Medical Platform Characteristics (Sheet 6 of 6)

NWP 4-02
D-7 JAN 2008
PLATFORM MEDICAL CORPS
NURSE CORPS
DENTAL CORPS
MEDICAL SERVICE CORPS
HOSPITAL CORPSMAN
Carrier 5 2 5 5 45
Cruiser 0 0 0 0 3
Destroyer 0 0 0 0 3
Fast Frigate 0 0 0 0 2
LHA 2 0 1 1 19
LHD 2 0 1 1 23
LHA/D (contingency augment) 11 22 1 1 48
Fleet Surgical Team 3 3 0 1 (2 in 2008) 9 (10 in 2008)
LPD 4 1 0 1 0 9
LPD 17 1 0 1 0 15
LSD 1 0 1 0 9
LCC 1 0 1 0 15
MCM/MHC 0 0 0 0 1
SSN/SSBN/SSGN 0 0 0 0 1
AS (submarine tenders) 2 0 3 1 17
PC (coastal patrol craft) 0 0 0 0 1
LCS 0 0 0 0 1
Source: 2006 BUMED Contingency Fact Book.
Figure D-2. Notional Shipboard Health Service Support Department Manning

NWP 4-02
JAN 2008 D-8
INTENTIONALLY BLANK

NWP 4-02
E-1 JAN 2008
APPENDIX E
Blood Supply Capabilities/ Planning Factors
E.1 UNITS OF MEASURE
BLOOD PRODUCT UNITS OF MEASURE RED BLOOD CELLS (FOR OXYGEN TRANSPORT)
Red Blood Cells 250 mL Red Blood Cells, Deglycerolized 200 mL
FLUIDS Crystalloids
Saline 1,000 mL Ringer’s Lactate Solution 1,000 mL
Colloids Fresh Frozen Plasma (FFP) 200 mL
Figure E-1. Units of Measure
E.2 CURRENT PLANNING FACTORS3
BLOOD PRODUCT UNITS PER HOSPITAL CASUALTY Red Blood Cells 4.0 units per wounded in action (WIA)/DNBI (across all echelons)
Fluid Approximately 3 percent of total fluid units can be a colloid. The remainder of total fluid units is crystalloid.
Fresh Frozen Plasma 0.08 units per WIA/DNBI Platelets 0.04 units per WIA/DNBI
Figure E-2. Units per Hospital Casualty
BLOOD PRODUCT
TOTAL UNITS
FORWARD RESUSCITATIVE CARE
CAPABILITY
THEATER HOSPITALIZATION
DEFINITIVE CARE
CAPABILITY Red Blood Cells 4 1 2 1 Fresh Frozen Plasma 0.08 None 0.06 0.02
Figure E-3. Units per Hospital Casualty by Category
__________ 3 Guidance only; may be adjusted to meet mission requirements.

NWP 4-02
JAN 2008 E-2
E.2.1 Pallet with Blood Products Shipping Data
TRANSPORTATION DATA RED BLOOD CELLS FFP RCF
Units/box 30 18/13 Boxes/pallet 120 120 Units/pallets 3,600 2,160/1,560 Weight/box 45 lb 39 lb Weight of shipment 5,280 lb 4,680 lb Volume of shipment 360 cu ft 360 cu ft
Figure E-4. Pallet with Blood Products
E.2.2 Miscellaneous Blood Planning Factors
PLANNING FACTORS
18 frozen blood units Frozen blood shipping container 20 to 30 pounds dry ice Per standard shipping container 30 units packed red blood cells (PRBC) Per standard shipping container 14 pounds cubed ice Per standard shipping container 120 boxes Per 463L pallet, weight 5,394 lb 3,600 units PRBC Per 463L pallet, size 442 cu ft 7,200 units PRBC Per blood transshipment center/day
250 units PRBC Contingency blood at Armed Services Whole Blood Processing Laboratories (ASWBPL)
480 units PRBC Per DEPMEDS D303 ISO 500 units PRBC Per DEPMEDS D404 ISO 1 unit thawed/washed Per hour, per wash, per technician 2 to 3 washers 1 technician can operate at a time 1.550 L wash solution Per unit washed 48 boxes or 1,440 units Containerized delivery system (CDS) 50 boxes or 1,500 units UH-60 (inside) 48 boxes or 1,440 units UH-60 (sling load) 30 boxes or 900 units UH-1 (inside) 40 boxes or 1,200 units UH-1 (sling load) 1 to 6 ºC Blood storage temperature 1 to 10 ºC Blood shipment temperature -80 ºC or below Frozen blood storage temperature -40 ºC or below Frozen blood shipment temperature -18 ºC or below Fresh frozen plasma storage/shipment temperature 20 to 24 ºC Platelet storage/shipment temperature Deglycerolized frozen blood Shelf life 1 day (extend to 3 days if emergent) Frozen blood Shelf life 10 years (FDA)/21 years (DOD) Fresh blood Shelf life 35 days (CPDA-1) and 42 days (w/additives) Fresh Frozen Plasma (once thawed) Shelf life 24 hours
Figure E-5. Miscellaneous Blood Planning Factors

NWP 4-02
E-3 JAN 2008
E.3 SHIPBOARD BLOOD PRODUCTS CAPABILITIES — OPNAVINST 6530.4 (SERIES)
SHIP TYPE OF DEPLOYMENTS
FROZEN RED BLOOD CELLS
FFP FROZEN PLATELETS
NO. FREEZERS CAPACITY
NO. REEFERS CAPACITY
Contingency 400 25 — 2 2 LHA/ LHD Mobilization 950 50 — 1,000 600
Contingency 2,375 100 25 6 4 T-AH
Mobilization 2,850 120 30 1,400 2,000 Note: Forward resuscitative care capabilities only maintain/hold blood Group O.
Figure E-6. Shipboard Blood Products Capabilities
E.4 BLOOD PRODUCTS (CLASS VIIIB) AVAILABLE TO THE THEATER
DISTRIBUTION PRODUCT
UNIT OF
ISSUE
SHELF LIFE FOR STORAGE
TREATMENT LEVEL AVAILABILITY O A B AB
RBCs Approx. 250 mL
35 days (42 days additive solution)
Forward resuscitative care capability, theater hospitalization, and definitive care capability
100% 50%
— 40%
— 10%
— —
Frozen Deglycerolized RBCs
Approx. 250 mL
10 years Theater hospitalization and definitive care capability
100% — — —
Fresh Frozen Plasma
Approx. 200 mL
1 year Theater hospitalization and definitive care capability
— 50% 25% 25%
*Platelets Varies 5 days Theater hospitalization and definitive care capability
50% 50% — —
* Shipping platelets into theater is a major challenge due to limited shelf life, temperature storage requirements, and the requirement for continuous agitation. The JBPO evaluates HN sources if determined to be a requirement for that operation. Frozen platelets are currently in R&D pending FDA approval.
Figure E-7. Blood Products (Class VIIIB) Available to the Theater

NWP 4-02
JAN 2008 E-4
E.5 BLOOD BANK PRODUCTS AND PROCEDURES BY CAPABILITY OF CARE
Figure E-8. Blood Bank Products and Procedures by Capability of Care
TREATMENTLEVEL
FIRSTRESPONDER
FORWARDRESUSCITATIVECARE CAPABILITIES
THEATERHOSPITALIZATIONCARE CAPABILITY- CSH- EMF- T-AH- EMEDS+25
* AVAILABILITY PENDING FDA LICENSURE ** RED BLOOD CELLS CAN BE SUPPLIED FROM HIGHER LEVELS VIA SPECIAL CONTAINERS*** NOT NECESSARY IF ASWBPL HAS VERIFIED THE ABO GROUP
DEFINITIVE CARE IN CONUS MTF AND OTHER MEDICAL CENTERS WITH BROAD TRANSFUSION MEDICINE CAPABILITIES.
ACRONYMS: CSHEMEDSHBOC
COMBAT SUPPORT HOSPITAL (ARMY UNIT)EXPEDITIONARY MEDICAL SUPPORT SYSTEM (AF UNIT)HEMOGLOBIN-BASED OXYGEN CARRIER
RED BLOOD CELLS
RED BLOOD CELLS
FROZEN/DEGLYCEROLIZEDRBC
FRESH FROZENPLASMA (FFP)
FROZENPLATELETS*
ORh + -
O, A, BRh + -
ORh + -
A, B, ABRh + -
O, ARh +
HBOC* NONE NONE
NONE
ABO/Rh GROUPPATIENT ANDDONOR RBCs***IMMEDIATE SPINCROSSMATCH
N/A
N/A
N/A
480 UNITSLIQUID RBCsCSH/EMF90/EMEDS+25840/LHD/LHA2000/T-AH
400 UNITSFROZENLHA or T-AH
20 UNITS
20 UNITS
BSU/BTC
BSU OR BPD
BSU/BTC
BSU/BTC
50 UNITS RBCPER MEDICAL FIELDREFRIGERATOR
BSU/BTC ORTHEATER HOSP
NONE NONE**
BLOOD PRODUCTS ABO & RhGROUP
TRANSFUSIONSERVICEPROCEDURES
STORAGECAPACITY
BLOODSUPPLY

NWP 4-02
F-1 JAN 2008
APPENDIX F
Responsibilities of the Joint Task Force Surgeon
F.1 JOINT TASK FORCE SURGEON
The responsibilities of the JTF surgeon are as follows:
1. Advise the CJTF and staff on the health of JTF forces and the conservation of fighting strength.
2. Determine requirements, establish, and organize the JTF surgeon’s office, and prepare to deploy the unit to conduct continuous 24-hour operations.
3. Determine requirements to establish, at a minimum, an Area Joint Blood Program Office (AJBPO) and a JPMRC. If a JPMRC is not established to provide management for regulating and patient evacuation, the JTF surgeon must establish direct liaison between the Theater Patient Movement Requirements Center (TPMRC) and Global Patient Movement Requirements Center (GPMRC) and the Service’s patient movement components.
4. Establish the JTF operational area HSS and patient evacuation plan and ensure efficient and effective interface of the theater and strategic AE systems through the JPMRC.
5. Monitor medical regulating and patient movement activities of the JPMRC and ensure that procedures are established to provide patient in-transit visibility (ITV) information to the J-1.
6. Advise the CJTF of comparison results between the medical proposed COA and available HSS capabilities.
7. Establish and maintain liaison with component surgeons.
8. Set priorities for actions within the surgeon’s staff and assign responsibilities to specific units and individuals.
9. Provide limited patient status and clinical information on selected patients to commanders and authorized representatives, as requested, based on the level of capability for patient ITV.
10. Establish HSS procedures for operations in a CBRN contaminated environment.
11. Provide preventive medicine support and participate in selection of bed-down locations.
F.2 EXPEDITIONARY STRIKE GROUP SURGEON
The duties and responsibilities of the ESG surgeon are as follows:
1. Advise the CESG and staff, ESG units, and the numbered fleet surgeon on HSS matters.
2. Optimize HSS readiness of all ESG units.

NWP 4-02
JAN 2008 F-2
3. Coordinate OPLANs and OPORDs with the CLF surgeon in preparing HSS units.
4. Ensure that LF HSS personnel augment the ESG HSS departments.
5. Ensure appropriate HSS to all embarked personnel using the ESG HSS department and medical supplies, reserving the LF HSS supplies for ultimate use ashore.
6. Monitor and coordinate quality assurance, risk management, credentials, and privileging issues for the amphibious task force (ATF).
7. Ensure optimal use of all embarked HSS personnel and materiel throughout the ESG.
8. Implement and manage ESG medical regulating.
9. Implement preventive medicine measures throughout the ESG.
10. Submit postdeployment lessons learned reports through the appropriate chain of command.
11. Coordinate with the State Department Office of Military Cooperation to establish and maintain medical liaison with US and foreign medical facilities ashore.
12. Advise the CESG in designating CRTSs, and request required HSS augmentation.
13. Implement, coordinate, and oversee HSS exercises, training, and education throughout the ESG, to include afloat continuing HSS education and continuing education unit documentation and PQS training.
14. In coordination with the CLF surgeon and other staff officers, plan for transporting casualties, including mass casualties, to the CRTS.
15. Request and disseminate medical intelligence.
16. Maintain liaison with other CESG staff officers on issues and actions related to the health care of the ESG.
17. Plan and provide for HSS support of NEO.
18. Coordinate communications support to complete the HSS mission.
19. Manage the whole blood program.
20. Provide projected HSS supply and resupply needs to cognizant supply system planners.
21. Represent the ATF in all matters pertaining to HSS for an operational mission.
22. Advise as to the status and capabilities of HSS elements supporting the mission.
F.3 LANDING FORCE SURGEON
The duties and responsibilities of the LF surgeon are as follows:
1. Ensure HSS provision for the LF before embarkation.
2. Assist the ships’ HSS department in providing HSS for embarked LF personnel.
3. Support the evacuation of casualties from the LF area to BESs during and after the assault phase.

NWP 4-02
F-3 JAN 2008
4. Provide HSS for personnel ashore in the objective area.
5. Make evacuation policy recommendations to the CESG and CLF for the operation.
6. Identify and request external HSS to fulfill requirements beyond the capability of LF HSS elements.
7. Determine requirements for HSS supply and sustainment for LF HSS units.
8. Establish emergency surgical treatment capabilities ashore.
9. Ensure continuity and interoperability of the MEDREGNET to coordinate the movement of casualties to appropriate treatment facilities ashore or afloat after control passes to the CLF.

NWP 4-02
JAN 2008 F-4
INTENTIONALLY BLANK

NWP 4-02
G-1 JAN 2008
APPENDIX G
Useful Websites
ORGANIZATION WEBSITE
Assistant Secretary of Defense (Health Affairs) http://www.ha.osd.mil/
Federal Emergency Management Agency http://www.fema.gov/ Naval Expeditionary Medical Training Institute (NEMTI) http://www.nomi.med.navy.mil/NEMTI/index.htm
International SOS, Inc. http://www.internationalsos.com/
Joint Center for Lessons Learned http://www.jfcom.mil/about/fact_jcoa.htm
Medical Deployers under Navy Knowledge Online Library https://www.nko.navy.mil/
Medical Officer of the Marine Corps http://hqinet001.hqmc.usmc.mil/hs/staffhtm.htm
Military Sealift Command http://www.msc.navy.mil/
Naval Electronic Directives System (On-line Database of SECNAV and OPNAV issuances) http://doni.daps.dla.mil/
Naval Health Research Center http://www.nhrc.navy.mil/
Naval Medical Education and Training Command http://nshs.med.navy.mil
Naval Medical Information Management Center http://navymedicine.med.navy.mil/nmimc/
Naval Medical Logistics Command http://www.nmlc.med.navy.mil
Naval Medical Research Center http://www.nmrc.navy.mil Naval Operational Medical Lessons Learned Center (NOMLLC) https://mll.nomi.med.navy.mil
Naval Operational Medicine Institute http://www.nomi.med.navy.mil/
Navy and Marine Corps Public Health Center http://www-nehc.med.navy.mil/
Navy Lessons Learned System http://www.nwdc.navy.mil/
Navy Medicine Online (Digital Health Services Library) http://navymedicine.med.navy.mil/
Navy Warfare Development Command http://www.nwdc.navy.mil/
North Atlantic Treaty Organization http://www.nato.int/
United States Northern Command http://www.northcom.mil/
United States Special Operations Command http://www.socom.mil/
United States Transportation Command http://www.transcom.mil/
Figure G-1. Useful Websites

NWP 4-02
JAN 2008 G-2
INTENTIONALLY BLANK

NWP 4-02
H-1 JAN 2008
APPENDIX H
Lessons Learned
H.1 GENERAL
The NOMLLC collects, analyzes, manages, and disseminates relevant medical observations, insights, and lessons learned in support of HSS operations.
New information is gathered from deployments, operations, and exercises. It is used to confirm existing tactics, techniques, and procedures and to identify areas needing improvement. Lessons learned are submitted by personnel throughout the course of deployment; an AAR is conducted following each major portion of the evolution.
H.2 AFTER ACTION REPORT
An after action review (AAR) is an assessment conducted during various phases of deployments, operations, and exercises that provides operational commanders and Navy Medicine a mechanism for identifying and evaluating an event and learning from the experience.
The AAR is planned at different intervals of deployment, operation, and exercise from which feedback is provided, lessons are learned, and ideas and suggestions are generated for the improvement of the next evolution based on the outcome of the review. Additionally, capturing observations and lessons into the NOMLLC LMS early on in order to impact predeployment training is crucial to increasing the effectiveness of the follow-on units.
H.3 LESSONS LEARNED
Collecting and analyzing lessons and observations is a means of improving the decisionmaking process and effecting needed changes to the HSS process using the DOTMLPF format.
Personnel prepare lessons learned in accordance with BUMEDINST 3500.3 (series), Naval Operational Medical Lessons Learned System (NOMLLS). All vetted and validated NOMLL are stored in the NOMLLS and when appropriate are exported to the Navy Lessons Learned System (NLLS) and/or the Marine Corps Lessons Learned Management System (MCLMS). Further Services’ lessons learned guidance is provided in OPNAVINST 3500.37 (series), Navy Lessons Learned System (NLLS) and MCO 3504.1, Marine Corps Lessons Learned Program (MCLLP) and the Marine Corps Center for Lessons Learned (MCCLL).
The NOMLLC website can be accessed at: https://mll.nomi.med.navy.mil and https://www.mccll.usmc.mil/nomi/index.cfm.

NWP 4-02
JAN 2008 H-2
INTENTIONALLY BLANK

NWP 4-02
Reference-1 JAN 2008
REFERENCES
The following publications and documents are for use in the planning and delivery of NEHSS. Many are referenced in this publication. NATO directives and STANAGS are identified in Appendix B.
ALLIED PUBLICATIONS
AD 85-8, Allied Command Europe (ACE) Medical Support Principles, Policies, and Planning Parameters.
AJP 4-10, Allied Joint Medical Support Doctrine.
MC 326/1, Medical Support, Precepts, and Guidance for NATO.
Second Geneva Convention for the Amelioration of the Condition of Wounded, Sick, and Shipwrecked Members of Armed Forces at Sea.
DOD PUBLICATIONS
DODD 1300.22, Mortuary Affairs Policy.
DODD 2310.01E, The Department of Defense Detainee Program.
DODD 3025.15, Military Assistance to Civil Authorities.
DODD 6490.5, Combat Stress Control (CSC) Programs.
DODI 1322.24, Medical Readiness Training.
DODI 2000.16, DOD Antiterrorism (AT) Standards.
DODI 6490.3, Deployment Health.
JOINT PUBLICATIONS
CJCS Memorandum of Policy #16, Joint Mortuary Affairs Policy.
CJCSI 3110.3 (series), Logistics Supplement to the Joint Strategic Capabilities Plan (JSCP).
CJCSI 3170.01 (series), Joint Capabilities Integration and Development System.
CJCSM 3122.01 (series), Joint Operation Planning and Execution System (JOPES), Volume I (Planning Policies and Procedures).
CJCSM 3122.03 (series), Joint Operation Planning and Execution System (JOPES), Volume II (Planning Formats and Guidance).
CJCSM 3500.03 (series), Joint Training Manual for the Armed Forces of the United States.
CJCSM 3500.05 (series), Joint Task Force Headquarters Master Training Guide.

NWP 4-02
JAN 2008 Reference-2
Joint Vision 2020.
JP 1, Doctrine for the Armed Forces of the United States.
JP 0-2, Unified Action Armed Forces (UNAAF).
JP 1-02, Department of Defense Dictionary of Military and Associated Terms.
JP 3-0, Joint Operations.
JP 3-33, Joint Task Force Headquarters.
JP 3-40, Joint Doctrine for Combating Weapons of Mass Destruction.
JP 3-63, Detainee Operations (Final Coordination Draft).
JP 4-0, Doctrine for Logistics Support of Joint Operations.
JP 4-02, Health Service Support.
JP 4-06, Mortuary Affairs in Joint Operations.
JP 5-0, Joint Operation Planning.
MARINE CORPS PUBLICATIONS
FMFM 3-1, Command and Staff Actions.
FMFM 4-50, Health Service Support.
Marine Corps Strategy 21.
MCO 3504.1, Marine Corps Lessons Learned Program (MCLLP) and the Marine Corps Center for Lessons Learned (MCCLL).
MCO 5000.12 (series), Marine Corps Policy Concerning Pregnancy and Parenthood.
MULTISERVICE PUBLICATIONS
AR 190–8/OPNAVINST 3461.6/AFJI 31–304/MCO 3461.1, Enemy Prisoners of War, Retained Personnel, Civilian Internees, and Other Detainees.
FM 3-11.5/NTTP 3-11.26/AFTTP(I) 3-2.60/MCWP 3.37.3, Multiservice Tactics, Techniques, and Procedures for Chemical, Biological, Radiological, and Nuclear Decontamination.
FM 3-11.86/NTTP 3-11.31/AFTTP(I) 3-2.52/MCRP 3-37.1C, Multiservice Tactics, Techniques, and Procedures for Biological Surveillance.
FM 4-02.283/NTRP 4-02.21/AFMAN 44-161(I)/MCRP 4-11.1B, Treatment of Nuclear and Radiological Casualties.
FM 4-02.285/NTRP 4-02.22/AFMAN 44-149(I)/MCRP 4-02.1E, Treatment of Chemical Agent Casualties and Conventional Military Chemical Injuries (draft).

NWP 4-02
Reference-3 JAN 2008
FM 4-02.7/NTTP 4-02.7/AFMAN 44-149(I)/MCRP 4-11.1F, Multiservice Tactics, Techniques, and Procedures for Health Service Support in a Nuclear, Biological and Chemical (NBC) Environment (draft).
FM 8-284/NTRP 4-02.23/AFMAN 44-156(I)/MCRP 4-11.1C, Treatment of Biological Warfare Agent Casualties.
NTTP 4-02.2M/MCWP 4-11.1G, Patient Movement.
NAVY PUBLICATIONS
2006 BUMED Contingency Fact Book.
BUMEDINST 3500.3 (series), Naval Operational Medical Lessons Learned System (NOMLLS).
BUMEDINST 5430.8, Bureau of Medicine and Surgery Organization Manual.
BUMEDINST 5450.156 (series), Mission, Functions, and Tasks of Naval Healthcare Support Offices.
BUMEDINST 6320.66 (series), Credentials Review and Privileging Program.
BUMEDINST 6440.5 (series), Health Services Augmentation Program.
BUMEDINST 6440.8 (series), Operational Forces Medical Liaison Services.
BUMEDINST 6470.10 (series), Initial Management of Irradiated or Radioactively Contaminated Personnel.
BUMED MSG 171921Z DEC 01.
COMNAVAIRFORINST 3500.20 (series), Aircraft Carrier Training and Readiness Manual.
COMNAVAIRFORINST 6000.1 (series), Shipboard Medical Procedures Manual.
COMNAVSURFORINST 3502.1, Surface Force Training Manual.
COMNAVSURFORINST 6000.1, Shipboard Medical Procedures Manual.
COMSC Washington DC 272119Z May 03.
COMSCINST 3501.2 (series), Status of Resources and Training System (SORTS) Reporting for MSC Units.
COMSCINST 5400.8 (series), Consolidated Plan for the Activation and Deactivation of T-AH 19 Mercy Class Hospital Ships.
COMSCINST 6000.1 (series), Military Sealift Command Medical Manual.
COMSUBLANT/COMSUBPACINST 6000.2 (series), Standard Medical Department Organizational Manual for Submarines.
Fleet Medicine Pocket Reference 2007.
Naval Force Health Protection for the 21st Century (NFHP-21).
NAVAIR 00-80T-121, Chemical and Biological Defense Naval Air Training and Operating Procedures Standardization (NATOPS) Manual.
NAVMED P-117, Manual of the Medical Department (MANMED).

NWP 4-02
JAN 2008 Reference-4
NAVMED P-5055, Radiation Health Protection Manual.
NAVMED P-6300-2 (series), Operational Obstetrics and Gynecology, the Health Care of Women in Military Settings.
NAVMEDCOMINST 5360.1, Decedent Affairs Manual.
Navy Environmental and Preventive Medicine, Fleet Public Health.
NSTM 070, Nuclear Defense at Sea and Radiological Recovery of Ships after Nuclear Weapons Explosion.
NTRP 1-02, Navy Supplement to the DOD Dictionary of Military and Associated Terms.
NTTP 1-01, The Navy Warfare Library.
NTTP 1-03.3 (series), Status of Resources and Training System Joint Report — Navy (SORTSREPNV).
NTTP 3-20.31.470 (NSTM Chapter 470), Shipboard Biological Warfare/Chemical Warfare Defense and Countermeasures.
NTTP 4-02.1, Medical Logistics.
NTTP 4-02.4, Expeditionary Medical Facilities.
NTTP 4-02.6, Hospital Ships.
OPNAVINST 1500.75 (series), Safety Policy and Procedures Conducting High-Risk Training.
OPNAVINST 3500.37 (series), Navy Lessons Learned System (NLLS).
OPNAVINST 3500.38B/MCO 3500.26/USCG COMDTINST 3500.1B, Universal Naval Task List (UNTL).
OPNAVINST 5430.48 (series), Office of the Chief of Naval Operations (OPNAV), Organization Manual.
OPNAVINST 5440.75 (series), Administration, Operation, and Logistic Support of T-AH 19 MERCY Class Hospital Ships.
OPNAVINST 6000.1 (series), Guidelines Concerning Pregnant Servicewomen.
OPNAVINST 6120.3, Preventive Health Assessment.
OPNAVINST 6530.4 (series), Department of the Navy Blood Program.
Sea Power 21.
SecDef Memorandum, Forces for Unified Commands.
SecDef Memorandum, Policy Implementation to Establish Commander, USJFCOM (CDRUSJFCOM), as the Primary Joint Force Provider.
SECNAVINST 5000.2 (series), Implementation and Operation of the Defense Acquisition and the Joint Capabilities Integration and Development System.
U.S. Navy Diving Manual, Volume 5, Diving Medicine and Recompression Chamber Operations.

NWP 4-02
Reference-5 JAN 2008
U.S. Naval Flight Surgeon’s Manual.
OTHER PUBLICATIONS
Centers for Disease Control and Prevention (CDC), Health Information for International Travel (the Yellow Book).
Department of State, Background Notes.
Goldwater-Nichols DOD Reorganization Act of 1986.
National Security Act of 1947.
Title 10, United States Code, Armed Forces.
World Health Organization (WHO), Vaccination Certificate Requirements for International Travel and Health Advice to Travellers.
World Health Organization (WHO), Weekly Epidemiological Record (WER).

NWP 4-02
JAN 2008 Reference-6
INTENTIONALLY BLANK

NWP 4-02
Glossary-1 JAN 2008
GLOSSARY
aeromedical evacuation (AE). The movement of patients under medical supervision to and between medical treatment facilities by air transportation. (JP 1-02)
aeromedical evacuation system. A system that provides: a. control of patient movement by air transport; b. specialized medical aircrew, medical crew augmentees, and specialty medical attendants and equipment for inflight medical care; c. facilities on or in the vicinity of air strips and air bases for the limited medical care of in-transit patients entering, en route via, or leaving the system; and d. communication with originating, destination, and en route medical facilities concerning patient transportation. See also aeromedical evacuation. (JP 1-02)
amphibious objective area (AOA). A geographical area (delineated for command and control purposes in the order initiating the amphibious operation) within which is located the objective(s) to be secured by the amphibious force. This area must be of sufficient size to ensure accomplishment of the amphibious force’s mission and must provide sufficient area for conducting necessary sea, air, and land operations. (JP 1-02)
amphibious task force (ATF). A Navy task organization formed to conduct amphibious operations. The amphibious task force, together with the landing force and other forces, constitutes the amphibious force. (JP 1-02)
battle injury (BI). Damage or harm sustained by personnel during or as a result of battle conditions. (JP 1-02)
battlespace. The environment, factors, and conditions that must be understood to successfully apply combat power, protect the force, or complete the mission. This includes the air, land, sea, space, and the included enemy and friendly forces; facilities; weather; terrain; the electromagnetic spectrum; and the information environment within the operational areas and areas of interest. (JP 1-02)
buddy-aid. Acute medical care (first aid) provided by a nonmedical Service member to another person. (JP 1-02)
casualty. Any person who is lost to the organization by having been declared dead, duty status — whereabouts unknown, missing, ill, or injured. See also hostile casualty; wounded in action. (JP 1-02)
casualty evacuation (CASEVAC). The movement of casualties. It includes movement both to and between medical treatment facilities. Any vehicle may be used to evacuate casualties. See also casualty; evacuation; medical treatment facility. (JP 1-02)
casualty receiving and treatment ship (CRTS). In amphibious operations, a ship designated to receive, provide treatment for, and transfer casualties. (JP 1-02)
civil support (CS). Department of Defense support to US civil authorities for domestic emergencies, and for designated law enforcement and other activities. (JP 1-02)
combat and operational stress. The expected and predictable emotional, intellectual, physical, and/or behavioral reactions of Service members who have been exposed to stressful events in war or military operations other than war. Combat stress reactions vary in quality and severity as a function of operational conditions, such as intensity, duration, rules of engagement, leadership, effective communication, unit morale, unit cohesion, and perceived importance of the mission. (JP 1-02)
combat and operational stress control. Programs developed and actions taken by military leadership to prevent, identify, and manage adverse combat and operational stress reactions in units; optimize mission

NWP 4-02
JAN 2008 Glossary-2
performance; conserve fighting strength; prevent or minimize adverse effects of combat and operational stress on members’ physical, psychological, intellectual, and social health; and to return the unit or Service member to duty expeditiously. (JP 1-02)
combatant command. A unified or specified command with a broad continuing mission under a single commander established and so designated by the President, through the Secretary of Defense and with the advice and assistance of the Chairman of the Joint Chiefs of Staff. Combatant commands typically have geographic or functional responsibilities. (JP 1-02)
combat and operational stress injury (COSI). A combat and operational stress injury is a potentially irreversible change in the mind and brain due to combat or operational stress that exceeds in intensity or duration the ability of the Sailor or Marine to adapt. Combat and operational stress injury symptoms normally resolve over time as the injury heals but intervention may be required to promote healing. Combat and operational stress injuries include three types: traumatic stress injury, fatigue stress injury, and grief. Many combat and operational stress injuries include components of more than one type of stress injury because trauma, fatigue, and grief are not mutually exclusive.
combatant command (command authority) (COCOM). Nontransferable command authority established by Title 10 (“Armed Forces”), United States Code, section 164, exercised only by commanders of unified or specified combatant commands unless otherwise directed by the President or the Secretary of Defense. Combatant command (command authority) cannot be delegated and is the authority of a combatant commander to perform those functions of command over assigned forces involving organizing and employing commands and forces, assigning tasks, designating objectives, and giving authoritative direction over all aspects of military operations, joint training, and logistics necessary to accomplish the missions assigned to the command. Combatant command (command authority) should be exercised through the commanders of subordinate organizations. Normally this authority is exercised through subordinate joint force commanders and Service and/or functional component commanders. Combatant command (command authority) provides full authority to organize and employ commands and forces as the combatant commander considers necessary to accomplish assigned missions. Operational control is inherent in combatant command (command authority). See also combatant command; combatant commander. (JP 1-02)
combatant commander (CCDR). A commander of one of the unified or specified combatant commands established by the President. See also combatant command. (JP 1-02)
combat service support (CSS). The essential capabilities, functions, activities, and tasks necessary to sustain all elements of operating forces in theater at all levels of war. Within the national and theater logistic systems, it includes but is not limited to that support rendered by service forces in ensuring the aspects of supply, maintenance, transportation, health services, and other services required by aviation and ground combat troops to permit those units to accomplish their missions in combat. Combat service support encompasses those activities at all levels of war that produce sustainment to all operating forces on the battlefield. (JP 1-02)
combat zone (CBTZ). 1. That area required by combat forces for the conduct of operations. 2. The territory forward of the Army rear area boundary. See also communications zone. (JP 1-02)
command and control (C2). The exercise of authority and direction by a properly designated commander over assigned and attached forces in the accomplishment of the mission. Command and control functions are performed through an arrangement of personnel, equipment, communications, facilities, and procedures employed by a commander in planning, directing, coordinating, and controlling forces and operations in the accomplishment of the mission. (JP 1-02)
communications zone (COMMZ). Rear part of a theater of war or theater of operations (behind but contiguous to the combat zone) which contains the lines of communications, establishments for supply and evacuation, and other agencies required for the immediate support and maintenance of the field forces. See also combat zone. (JP 1-02)

NWP 4-02
Glossary-3 JAN 2008
definitive care. Care rendered to conclusively manage a patient’s condition. It includes the full range of preventive, curative acute, convalescent, restorative, and rehabilitative medical care. This normally leads to rehabilitation, return to duty, or discharge from the Service. (JP 1-02)
detainee. Any person captured, detained, held, or otherwise under the control of DOD personnel (military, civilian, or contract employee). It does not include persons being held primarily for law enforcement purposes, except where the United States is the occupying power. (DODD 2310.01E)
direct air support center (DASC). The principal air control agency of the US Marine air command and control system responsible for the direction and control of air operations directly supporting the ground combat element. It processes and coordinates requests for immediate air support and coordinates air missions requiring integration with ground forces and other supporting arms. It normally collocates with the senior fire support coordination center within the ground combat element and is subordinate to the tactical air command center. (JP 1-02)
directed energy (DE). An umbrella term covering technologies that relate to the production of a beam of concentrated electromagnetic energy or atomic or subatomic particles. (JP 1-02)
disease and nonbattle injury (DNBI). All illnesses and injuries not resulting from enemy or terrorist action or caused by conflict. Indigenous disease pathogens, biological warfare agents, heat and cold, hazardous noise, altitude, environmental, occupational, and industrial exposures, and other naturally occurring disease agents may cause disease and nonbattle injury. Disease and nonbattle injuries include injuries and illnesses resulting from training or from occupational, environmental, or recreational activities, and may result in short- or long-term, acute, or delayed illness, injury, disability, or death. (JP 1-02)
en route care. Continuation of the provision of care during movement (evacuation) between the health service support capabilities in the continuum of care, without clinically compromising the patient’s condition. See also evacuation; patient. (JP 1-02)
essential care. Medical treatment provided to manage the casualty throughout the range of care. This includes all care and treatment to either return the patient to duty (within the theater evacuation policy), or begin initial treatment required for optimization of outcome, and/or stabilization to ensure the patient can tolerate evacuation. See also en route care; first responders; forward resuscitative care; patient. (JP 1-02)
evacuation. 1. Removal of a patient by any of a variety of transport means (air, ground, rail, or sea) from a theater of military operation, or between health service support capabilities, for the purpose of preventing further illness or injury, providing additional care, or providing disposition of patients from the military health care system. 2. The clearance of personnel, animals, or materiel from a given locality. 3. The controlled process of collecting, classifying, and shipping unserviceable or abandoned materiel, US or foreign, to appropriate reclamation, maintenance, technical intelligence, or disposal facilities. 4. The ordered or authorized departure of noncombatants from a specific area by Department of State, Department of Defense, or appropriate military commander. This refers to the movement from one area to another in the same or different countries. The evacuation is caused by unusual or emergency circumstances and applies equally to command or non-command sponsored family members. (JP 1-02)
executive agent (EA). A term used to indicate a delegation of authority by the Secretary of Defense to a subordinate to act on the Secretary’s behalf. Designation as executive agent, in and of itself, confers no authority. The exact nature and scope of the authority delegated must be stated in the document designating the executive agent. An executive agent may be limited to providing only administration and support or coordinating common functions; or it may be delegated authority, direction, and control over specified resources for specified purposes. (JP 1-02)
first responders. The primary health care providers whose responsibility is the provision of immediate clinical care and stabilization in preparation for evacuation to the next health service support capability in the continuum

NWP 4-02
JAN 2008 Glossary-4
of care. In addition to treating injuries, they treat Service members for common acute minor illnesses. See also essential care; evacuation; patient. (JP 1-02)
force health protection (FHP). Measures to promote, improve, or conserve the mental and physical well-being of Service members. These measures enable a healthy and fit force, prevent injury and illness, and protect the force from health hazards. (JP 1-02)
foreign humanitarian assistance (FHA). Programs conducted to relieve or reduce the results of natural or man-made disasters or other endemic conditions, such as human pain, disease, hunger, or privation, that might present a serious threat to life or that can result in great damage to or loss of property. Foreign humanitarian assistance provided by US forces is limited in scope and duration. The foreign assistance provided is designed to supplement or complement the efforts of the host-nation civil authorities or agencies that may have the primary responsibility for providing foreign humanitarian assistance. Foreign humanitarian assistance operations are those conducted outside the United States, its territories, and its possessions. (JP 1-02)
forward resuscitative care (FRC). Care provided as close to the point of injury as possible based on current operational requirements to attain stabilization and achieve the most efficient use of life-and-limb saving medical treatment. Forward resuscitative care typically provides essential care for stabilization to ensure the patient can tolerate evacuation. See also essential care; evacuation; medical treatment facility; patient. (JP 1-02)
Global Patient Movement Requirements Center (GPMRC). A joint activity reporting directly to the Commander, US Transportation Command, the Department of Defense single manager for the strategic and continental United States regulation and movement of uniformed services and other authorized patients. The Global Patient Movement Requirements Center provides medical regulating and aeromedical evacuation scheduling for the continental United States and intertheater operations and provides support to the Theater Patient Movement Requirements Center. The Global Patient Movement Requirements Center coordinates with supporting resource providers to identify available assets and communicates transport to bed plans to the appropriate transportation agency for execution. See also medical treatment facility. (JP 1-02)
health care provider. Any member of the Armed Forces, civilian employee of the Department of Defense, or personal services contract employee under Title 10 United States Code Section 1091 authorized by the Department of Defense to perform health care functions. The term does not include any contract provider who is not a personal services contract employee. (JP 1-02)
health service logistic support (HSLS). A functional area of logistic support that supports the joint force surgeon’s health service support mission. It includes supplying Class VIII medical supplies (medical materiel to include medical peculiar repair parts used to sustain the health service support system), optical fabrication, medical equipment maintenance, blood storage and distribution, and medical gases. See also health service support. (JP 1-02)
health service support (HSS). All services performed, provided, or arranged to promote, improve, conserve, or restore the mental or physical well-being of personnel. These services include, but are not limited to, the management of health services resources, such as manpower, monies, and facilities; preventive and curative health measures; evacuation of the wounded, injured, or sick; selection of the medically fit and disposition of the medically unfit; blood management; medical supply, equipment, and maintenance thereof; combat stress control; and medical, dental, veterinary, laboratory, optometric, nutrition therapy, and medical intelligence services. See also health service logistic support. (JP 1-02)
health surveillance. The regular or repeated collection, analysis, and interpretation of health-related data and the dissemination of information to monitor the health of a population and to identify potential health risks, thereby enabling timely interventions to prevent, treat, reduce, or control disease and injury. It includes occupational and environmental health surveillance and medical surveillance subcomponents. (JP 1-02)

NWP 4-02
Glossary-5 JAN 2008
health threat. A composite of ongoing or potential enemy actions; adverse environmental, occupational, and geographic and meteorological conditions; endemic diseases; and employment of nuclear, biological, and chemical weapons (to include weapons of mass destruction) that have the potential to affect the short- or long-term health (including psychological impact) of personnel. (JP 1-02)
helicopter direction center (HDC). In amphibious operations, the primary direct control agency for the helicopter group/unit commander operating under the overall control of the tactical air control center. (JP 1-02)
hospital. A medical treatment facility capable of providing inpatient care. It is appropriately staffed and equipped to provide diagnostic and therapeutic services, as well as the necessary supporting services required to perform its assigned mission and functions. A hospital may, in addition, discharge the functions of a clinic. (JP 1-02)
hostile casualty. A person who is the victim of a terrorist activity or who becomes a casualty “in action.” “In action” characterizes the casualty as having been the direct result of hostile action, sustained in combat or relating thereto, or sustained going to or returning from a combat mission provided that the occurrence was directly related to hostile action. Included are persons killed or wounded mistakenly or accidentally by friendly fire directed at a hostile force or what is thought to be a hostile force. However, not to be considered as sustained in action and not to be interpreted as hostile casualties are injuries or death due to the elements, self-inflicted wounds, combat fatigue, and except in unusual cases, wounds or death inflicted by a friendly force while the individual is in an absent-without-leave, deserter, or dropped-from-rolls status or is voluntarily absent from a place of duty. See also casualty; wounded in action. (JP 1-02)
host nation (HN). A nation that receives the forces and/or supplies of allied nations, coalition partners, and/or NATO organizations to be located on, to operate in, or to transit through its territory. (JP 1-02)
humanitarian and civic assistance (HCA). Assistance to the local populace provided by predominantly US forces in conjunction with military operations and exercises. This assistance is specifically authorized by Title 10, United States Code, Section 401, and funded under separate authorities. Assistance provided under these provisions is limited to (1) medical, dental, veterinary, and preventive medicine care provided in rural areas of a country; (2) construction of rudimentary surface transportation systems; (3) well drilling and construction of basic sanitation facilities; and (4) rudimentary construction and repair of public facilities. Assistance must fulfill unit-training requirements that incidentally create humanitarian benefit to the local populace. See also foreign humanitarian assistance. (JP 1-02)
intertheater patient movement. Moving patients between, into, and out of the different theaters of the geographic combatant commands and into the continental United States or another supporting theater. See also en route care; evacuation; intratheater patient movement; patient. (JP 1-02)
in-transit visibility (ITV). The ability to track the identity, status, and location of Department of Defense units, and non-unit cargo (excluding bulk petroleum, oils, and lubricants) and passengers; patients; and personal property from origin to consignee or destination across the range of military operations. (JP 1-02)
intratheater patient movement. Moving patients within the theater of a combatant command or in the continental United States. See also en route care; evacuation; intertheater patient movement; patient. (JP 1-02)
Joint Patient Movement Requirements Center (JPMRC). A joint activity established to coordinate the joint patient movement requirements function for a joint task force operating within a unified command area of responsibility. It coordinates with the Theater Patient Movement Requirements Center for intratheater patient movement and the Global Patient Movement Requirements Center for intertheater patient movement. See also health service support; medical treatment facility; patient. (JP 1-02)

NWP 4-02
JAN 2008 Glossary-6
logistic support (medical). Medical care, treatment, hospitalization, and evacuation, as well as the furnishing of medical services, supplies, materiel, and adjuncts thereto. (JP 1-02)
mass casualty. Any large number of casualties produced in a relatively short period of time, usually as the result of a single incident such as a military aircraft accident, hurricane, flood, earthquake, or armed attack that exceeds local logistic support capabilities. See also casualty. (JP 1-02)
medical evacuation (MEDEVAC). Refers to Army, Navy, Marine Corps, and Coast Guard patient movement using designated tactical or logistic aircraft, boats, ships, and other watercraft temporarily equipped and staffed with medical attendants for en route care. (NTTP 4-02.2M/MCRP 4-11.1G)
medical intelligence. That category of intelligence resulting from collection, evaluation, and analysis, and interpretation of foreign medical, bio-scientific, and environmental information that is of interest to strategic planning and to military medical planning and operations for the conservation of the fighting strength of friendly forces and the formation of assessments of foreign medical capabilities in both military and civilian sectors. (JP 1-02)
medical protocols. Directives issued by competent military authority that delineate the circumstances and limitations under which US medical forces will initiate medical care and support to those individuals that are not Department of Defense health care beneficiaries or designated eligible for care in a military medical treatment facility by the Secretary of Defense. (JP 1-02)
medical regulating. The actions and coordination necessary to arrange for the movement of patients through the levels of care. This process matches patients with a medical treatment facility that has the necessary health service support capabilities and available bed space. See also health service support; medical treatment facility. (JP 1-02)
medical regulating control center (MRCC). The coordination center for movement of casualties within and out of a naval task force. Normally located with the flagship, the medical regulating control center is supervised by the medical regulating control officer. (NTRP 1-02)
medical regulating control officer (MRCO). A medical administrative officer or senior enlisted person from the health service support staff of the amphibious task force who directs and supervises the operation of the medical regulating team, is net control for the medical regulating network, and maintains liaison with the Joint/Theater Patient Movement Requirements Center. The medical regulating control officer also keeps the amphibious task force and landing force surgeons and the Joint/Theater Patient Movement Requirements Center informed on the current status and operations of patient movement within the task force. (COMNAVSURFORINST 6000.1)
medical regulating network (MEDREGNET). The formal radio communication network for the medical regulating system. The success of the medical regulating system depends upon reliable communications over dedicated and parallel systems. Both the commander, amphibious task force medical regulating control officer and the commander, landing force patient evacuation officer must have the same dedicated radio communications network. This is coordinated by the amphibious task force communications officer and the landing force communications–electronics officer ensuring that communication requirements for the medical regulating system are addressed in all operation orders/operation plans. The primary purpose of the medical regulating network is to provide a means of rapid communications between the medical regulating control officers, medical regulating teams, and the Joint/Theater Patient Movement Requirements Center. This ensures a constant flow of current capability information between medical treatment facilities and control agencies. (Fleet Medicine Pocket Reference 2007)
medical regulating team. A team of medical regulators and Navy or Marine Corps radio operators assigned to mobile or fixed medical treatment facilities, under the direct supervision of a medical regulating officer. The team receives and maintains information regarding the health service support capabilities of the medical treatment facilities within the amphibious area of operations and coordinates the regulation of casualties under

NWP 4-02
Glossary-7 JAN 2008
their cognizance. Within the landing force, this team is called the patient evacuation team. (COMNAVSURFORINST 6000.1)
medical surveillance. The ongoing, systematic collection, analysis, and interpretation of data derived from instances of medical care or medical evaluation, and the reporting of population-based information for characterizing and countering threats to a population’s health, well-being and performance. (JP 1-02)
medical treatment facility (MTF). A facility established for the purpose of furnishing medical and/or dental care to eligible individuals. (JP 1-02)
military health system. A health system that supports the military mission by fostering, protecting, sustaining, and restoring health. It also provides the direction, resources, health care providers, and other means necessary for promoting the health of the beneficiary population. These include developing and promoting health awareness issues to educate customers, discovering and resolving environmentally based health threats, providing health services, including preventive care and problem intervention, and improving the means and methods for maintaining the health of the beneficiary population, by constantly evaluating the performance of the health care services system. (JP 1-02)
occupational and environmental health surveillance. The regular or repeated collection, analysis, archiving, interpretation, and dissemination of occupational and environmental health-related data for monitoring the health of, or potential health hazard impact on, a population and individual personnel, and for intervening in a timely manner to prevent, treat, or control the occurrence of disease or injury when determined necessary. (JP 1-02)
operational environment. A composite of the conditions, circumstance, and influences that affect the employment of capabilities and bear on the decisions of the commander. (JP 1-02)
operation order (OPORD). A directive issued by a commander to subordinate commanders for the purpose of effecting the coordinated execution of an operation. (JP 1-02)
operation plan (OPLAN). 1. Any plan for the conduct of military operations prepared in response to actual and potential contingencies. 2. In the context of joint operation planning level 4 planning detail, a complete and detailed joint plan containing a full description of the concept of operations, all annexes applicable to the plan, and time-phased force and deployment data. It identifies the specific forces, functional support, and resources required to execute the plan and provide closure estimates for their flow into the theater. See also operation order. (JP 1-02)
originating medical facility. A medical facility (MTF) that initially transfers a patient to another medical facility. (JP 1-02)
patient. A sick, injured, wounded, or other person requiring medical and/or dental care or treatment. (JP 1-02)
patient evacuation. The removal of a patient by a variety of transport means (air, ground, rail, or sea) from a theater of military operation and between health service support capabilities to prevent further illness or injury and to provide additional care and disposition of patients from the military health care system. (NTTP 4-02.2M/MCRP 4-11.1G)
patient movement policy. Command decision establishing the maximum number of days that patients may be held within the command for treatment. Patients who, in the opinion of responsible medical officers, cannot be returned to a duty status within the period prescribed are evacuated by the first available means, provided the travel involved will not aggravate their disabilities. See also evacuation; patient. (JP 1-02)
population at risk. The strength in personnel of a given force structure in terms of which casualty rates are stated. (JP 1-02)

NWP 4-02
JAN 2008 Glossary-8
port of debarkation (POD). The geographic point at which cargo or personnel are discharged. This may be a seaport or aerial port of debarkation; for unit requirements, it may or may not coincide with the destination. See also port of embarkation. (JP 1-02)
port of embarkation (POE). The geographic point in a routing scheme from which cargo or personnel depart. This may be a seaport or aerial port from which personnel and equipment flow to a port of debarkation; for unit and non-unit requirements, it may or may not coincide with the origin. See also port of debarkation. (JP 1-02)
preventive medicine. The anticipation, communication, prediction, identification, prevention, education, risk assessment, and control of communicable diseases, illnesses and exposure to endemic, occupational, and environmental threats. These threats include nonbattle injuries, combat stress responses, weapons of mass destruction, and other threats to the health and readiness of military personnel. Communicable diseases include anthropod-, vector-, food-, waste-, and waterborne diseases. Preventative medicine measures include field sanitation, medical surveillance, pest and vector control, disease risk assessment, environmental and occupational health surveillance, waste (human, hazardous, and medical) disposal, food safety inspection, and potable water surveillance. (JP 1-02)
rehabilitative care (restorative care). Therapy that provides evaluations and treatment programs using exercises, massage, or electrical therapeutic treatment to restore, reinforce, or enhance motor performance and restores patients to functional health allowing for their return to duty or discharge from the Service. See also patient; patient movement policy. (JP 1-02)
resuscitative care. Advanced emergency medical treatment required to prevent immediate loss of life or limb and to attain stabilization to ensure the patient could tolerate evacuation. (JP 1-02)
seriously ill or injured. The casualty status of a person whose illness or injury is classified by medical authority to be of such severity that there is cause for immediate concern, but there is not imminent danger to life. (JP 1-02)
seriously wounded. A casualty whose injuries or illnesses are of such severity that the patient is rendered unable to walk or sit, thereby requiring a litter for movement and evacuation. See also evacuation; patient. (JP 1-02)
slightly wounded. A casualty whose injuries are relatively minor, permitting the patient to walk and/or sit. See also patient. (JP 1-02)
stabilized patient. A patient whose airway is secured, hemorrhage is controlled, shock treated, and fractures are immobilized. See also patient. (JP 1-02)
tactical aeromedical evacuation. That phase of evacuation which provides airlift for patients from the combat zone to points outside the combat zone, and between points within the communications zone. (JP 1-02)
tactical air control center (TACC). The principal air operations installation (ship-based) from which all aircraft and air warning functions of tactical air operations are controlled. (JP 1-02)
telemedicine. Rapid access to shared and remote medical expertise by means of telecommunications and information technologies to deliver health services and exchange health information for the purpose of improving patient care. (JP 1-02)
theater hospitalization capability. Essential care and health service support capabilities to either return the patient to duty and/or stabilization to ensure the patient can tolerate evacuation to a definitive care facility outside the theater. It includes modular hospital configurations required to support the theater (emergency medical services, surgical services, primary care, veterinary services, dental services, preventive medicine, and

NWP 4-02
Glossary-9 JAN 2008
combat and operational stress control, blood banking services, hospitalization, laboratory and pharmacy services, radiology, medical logistics, and other medical specialty capabilities as required). (JP 1-02)
Theater Patient Movement Requirements Center (TPMRC). The activity responsible for intratheater patient movement management (medical regulating and aeromedical evacuation scheduling), the development of theater-level patient movement plans and schedules, the monitoring and execution in concert with the Global Patient Movement Requirements Center. (JP 1-02)
unstable patient. A patient whose physiological status is in fluctuation. Emergent, treatment and/or surgical intervention are anticipated during the evacuation. An unstable patient’s rapidly changing status and requirements are beyond the standard en route care capability and requires medical/surgical augmentation. (JP 1-02)
very seriously ill or injured (VSII). The casualty status of a person whose illness or injury is classified by medical authority to be of such severity that life is imminently endangered. See wounded in action. (JP 1-02)
wounded. See seriously wounded; slightly wounded. (JP 1-02)
wounded in action (WIA). A casualty category applicable to a hostile casualty, other than the victim of a terrorist activity, who has incurred an injury due to an external agent or cause. The term encompasses all kinds of wounds and other injuries incurred in action, whether there is a piercing of the body, as in a penetration or perforated wound, or none, as in the contused wound. These include fractures, burns, blast concussions, all effects of biological and chemical warfare agents, and the effects of an exposure to ionizing radiation or any other destructive weapon or agent. The hostile casualty’s status may be categorized as “very seriously ill or injured,” “seriously ill or injured,” “incapacitating illness or injury,” or “not seriously injured.” See also casualty; hostile casualty; very seriously ill or injured; wounded. (JP 1-02)

NWP 4-02
JAN 2008 Glossary-10
INTENTIONALLY BLANK

NWP 4-02
LOAA-1 JAN 2008
LIST OF ACRONYMS AND ABBREVIATIONS
AA area analysis
AAR after action review
ABFC advanced base functional component
ACE aviation combat element (MAGTF); Allied Command Europe
AD Allied Directive
ADAL authorized dental allowance list
ADCON administrative control
ADDU additional duty
AE aeromedical evacuation
AELT aeromedical evacuation liaison team
AFMIC Armed Forces Medical Intelligence Center
AIRFOR air forces
AJBPO Area Joint Blood Program Office
AJP allied joint publication
AMAL authorized medical allowance list
AMC Air Mobility Command
AMD activity manpower document
AO area of operations
AOA amphibious objective area
AOR area of responsibility
APOD aerial port of debarkation
ASD(HA) Assistant Secretary of Defense (Health Affairs)
ASF aeromedical staging facility
AT/FP antiterrorism/force protection
ATF amphibious task force
ATTO antiterrorism training officer

NWP 4-02
JAN 2008 LOAA-2
BAS battalion aid station
BES beach evacuation station
BI battle injury
BOS base operating support
BSC billet sequence code
BSO Budget Submitting Office
BTP billet training profile
BUMED Bureau of Medicine and Surgery
BUMEDINST Bureau of Medicine and Surgery instruction (Navy)
C2 command and control
C4 command, control, communications, and computers
C4I command, control, communications, computers, and intelligence
CASEVAC casualty evacuation
CBR chemical, biological, and radiological
CBR-D chemical, biological, and radiological defense
CBRED chemical, biological, radiological, and environmental defense (USN)
CBRN chemical, biological, radiological, and nuclear
CBTZ combat zone
CCDR combatant commander
CDC Centers for Disease Control and Prevention
CDRUSJFCOM Commander, United States Joint Forces Command
CD-ROM compact disc read-only memory
CEC corporate exigency contracts
CESG commander, expeditionary strike group
CHBUMED Chief, Bureau of Medicine and Surgery
CHNAVPERS Chief of Naval Personnel
CIVMAR civilian mariner
CJCS Chairman of the Joint Chiefs of Staff

NWP 4-02
LOAA-3 JAN 2008
CJCSI Chairman of the Joint Chiefs of Staff instruction
CJCSM Chairman of the Joint Chiefs of Staff manual
CJTF commander, joint task force
CLB combat logistics battalion
CLF commander, landing force
CLR combat logistics regiment
CM consequence management
CMC Commandant of the Marine Corps
CNO Chief of Naval Operations
CO commanding officer
COA course of action
COAA course-of-action analysis
COCOM combatant command (command authority)
COMMZ communications zone
COMNAVAIRFORINST Commander, Naval Air Forces instruction
COMNAVRESFOR Commander, Naval Reserve Force
COMNAVSUPSYSCOM Commander, Naval Supply Systems Command
COMNAVSURFORINST Commander, Naval Surface Forces instruction
COMNAVSURFRESFOR Commander, Naval Surface Reserve Force
COMSC Commander, Military Sealift Command
COMSCINST Commander, Military Sealift Command instruction
COMUSFLTFORCOM Commander, US Fleet Forces Command
COMUSMARCENT Commander, United States Marine Forces, Central Command
COMUSNAVCENT Commander, United States Navy, Central Command
COMUSNAVEUR Commander, US Naval Forces Europe
COMUSPACFLT Commander, US Pacific Fleet
COMUSPACOM Commander, United States Pacific Command
CONOPS concept of operations

NWP 4-02
JAN 2008 LOAA-4
CONPLAN concept plan
CONUS continental United States
COSI combat and operational stress injury
COSR combat and operational stress reactions
CPG Contingency Planning Guidance
CRD combatant commander’s required date
CRTS casualty receiving and treatment ship
CS civil support
CSS combat service support
CUIC component unit identification code
CUSFFC Commander, United States Fleet Forces Command
DAF Department of the Air Force
DASC direct air support center
DE directed energy
DEPMEDS deployable medical systems
DEPORD deployment order
DIA Defense Intelligence Agency
DIRLAUTH direct liaison authorized
DLA Defense Logistics Agency
DNA deoxyribonucleic acid
DNBI disease and nonbattle injury
DOD Department of Defense
DODD Department of Defense directive
DODI Department of Defense instruction
DON Department of the Navy
DOTMLPF doctrine, organization, training, materiel, leadership and education, personnel and facilities
DPMIAC Defense Pest Management Information Analysis Center

NWP 4-02
LOAA-5 JAN 2008
DR disaster relief
DSCP Defense Supply Center Philadelphia
DTF dental treatment facility
DVA Department of Veterans Affairs
DVEP disease vector ecology profile
EA executive agent
EHRA environmental health risk assessment
EMF expeditionary medical facility
EPW enemy prisoner of war
ERCS en route care system
ESG expeditionary strike group
EXORD execution order
FCC Federal Coordinating Center (NDMS); functional combatant command
FDA Food and Drug Administration
FDPMU forward deployable preventive medicine unit
FEMA Federal Emergency Management Agency
FFP fresh frozen plasma
FHA foreign humanitarian assistance
FHD fleet health domain
FHP force health protection
FISC fleet and industrial supply center
FLTCOM fleet commander
FMF Fleet Marine Force
FMFM Fleet Marine Force Manual
FOH fleet operational health
FOS full operating status
FPO force protection officer
FRC forward resuscitative care

NWP 4-02
JAN 2008 LOAA-6
FRE fleet readiness enterprise
FRP fleet response plan
FRSS forward resuscitative surgery system
FST fleet surgical team
FTC fleet training continuum
FUNCPLAN functional plan
GCC geographic combatant command
GCE ground combat element (MAGTF)
GCCS-M Global Command and Control System–Maritime
GFM Global Force Management
GFMAP Global Force Management Allocation Plan
GI gastrointestinal
GPMRC Global Patient Movement Requirements Center
GSORTS Global Status of Resources and Training System
HA humanitarian assistance
HCA humanitarian and civic assistance
HDC helicopter direction center
HIV human immuno-deficiency virus
HN host nation
HQ headquarters
HQDA Headquarters, Department of the Army
HQMC Headquarters, Marine Corps
HSA health service assessment
HSAP Health Services Augmentation Program
HSAPU Health Services Augmentation Program Unit
HSLS health service logistic support
HSO healthcare support office
HSS health service support

NWP 4-02
LOAA-7 JAN 2008
HSSD Health Service Support Division
HSSE health service support element
HST humanitarian support team
ICU intensive care unit
IDA infectious disease alert
IDC independent duty corpsman
IDRA infectious disease risk assessment
IFHRA industrial facility health risk assessment
IMR individual medical readiness
IPOE intelligence preparation of the operational environment
ISIC immediate superior-in-command
ITV in-transit visibility
J/TPMRC Joint/Theater Patient Movement Requirements Center
JBPO Joint Blood Program Office
JCAHO Joint Commission on Accreditation of Health Care Organizations
JCIDS Joint Capabilities Integration and Development System
JFC joint force commander
JFP joint force provider
JFS joint force surgeon
JISE joint intelligence support element
JMRO Joint Medical Regulating Office
JOA joint operations area
JOPES Joint Operation Planning and Execution System
JP joint publication
JPMRC Joint Patient Movement Requirements Center
JS joint staff
JSCP Joint Strategic Capabilities Plan
JTF joint task force

NWP 4-02
JAN 2008 LOAA-8
JPMRC Joint Patient Movement Requirements Center
LAN local area network
LF landing force
LFA lead federal agency
LFOC landing force operations center
LFSP landing force support party
LMS lessons management system
LOAC low of armed conflict
MAGTF Marine air-ground task force
MANMED Manual of the Medical Department
MARCORSYSCOM Marine Corps Systems Command
MARDIV Marine division
MARFOR Marine Corps forces
MASF mobile aeromedical staging facility
MAW Marine aircraft wing
MC Military Committee (NATO)
MCCLL Marine Corps Center for Lessons Learned
MCLLP Marine Corps Lessons Learned Program
MCLMS Marine Corps Lessons Management System
MCO Marine Corps order
MCT Marine corps task
MCTL Marine Corps task list
MDR medical department representative
MEDEVAC medical evacuation
MEDIC medical, environmental, disease, intelligence, and countermeasures
MEDREGNET medical regulating network
MEDRUP Medical Reserve Utilization Program
MEDRUPMIS Medical Reserve Utilization Program Management Information System

NWP 4-02
LOAA-9 JAN 2008
MEF Marine expeditionary force
MEL master equipment list
MET mission-essential task
MEU Marine expeditionary unit
MEU(SOC) Marine expeditionary unit (special operations capable)
MFRP Medical Fleet Response Plan
MIN medical intelligence note
MLG Marine logistics group
MOPP mission-oriented protective posture
MPF(E) maritime prepositioning force (enhanced)
MPS maritime prepositioning ships
MPT&E manpower, personnel, training, and education
MRCC medical regulating control center
MRCO medical regulating control officer
MRO medical regulating office
MSC Military Sealift Command
MSO medical services officer
MTF medical treatment facility
MWSG Marine wing support group
MWSS Marine wing support squadron
NA needs analysis
NAMI Naval Aerospace Medical Institute
NASTP Naval Aviation Survival Training Program
NATO North Atlantic Treaty Organization
NAVFOR Navy forces
NAVMED Navy medical; Navy Medicine
NAVMEDCOMINST Navy Medical Command instruction
NAVMEDLOGCOM Naval Medical Logistics Command

NWP 4-02
JAN 2008 LOAA-10
NAVMTO Navy Material Transportation Office
NAVSUPSYSCOM Naval Suppy Systems Command
NBC nuclear, biological, and chemical
NCA national capital area
NCO noncommissioned officer
NDMS National Disaster Medical System
NEC Navy enlisted classification
NECC Navy Expeditionary Combat Command
NECE Navy Entomology Center of Excellence
NEHSS naval expeditionary health service support
NEMSC Navy expeditionary medical support command
NEMTI Naval Expeditionary Medical Institute
NEO noncombatant evacuation operation
NEPMU Navy Environmental and Preventive Medicine Unit
NHRC Naval Health Research Center
NIPRNET Non-Secure Internet Protocol Router Network
NLLS Navy Lessons Learned System
nm nautical mile
NMCPHC Navy and Marine Corps Public Health Center
NME Navy Medicine East
NMLC Naval Medical Logistics Command
NMMPT&E Navy Medicine, Manpower, Personnel, Training, and Education Command
NMRC Naval Medical Research Center
NMS national military strategy
NMSC Navy Medicine Support Command
NMW Navy Medicine West
NNMC National Naval Medical Center

NWP 4-02
LOAA-11 JAN 2008
NOBC naval officer billet classification
NOMI Naval Operational Medical Institute
NOMLL naval operational medical lessons learned
NOMLLC Naval Operational Medical Lessons Learned Center
NOMLLS Naval Operational Medical Lessons Learned System
NOSTRA Naval Ophthalmic Support and Training Activity
NSA NATO Standardization Agency
NSOMI Naval Special Operations Medical Institute
NSTI Naval Survival Training Institute
NSTM Naval Ships’ Techincal Manual
NSW naval special warfare
NSWU naval special warfare unit
NTA Navy tactical task
NTP Navy training plan
NTSP Navy training system plan
NTTL Navy tactical task list
NTTP Navy tactics, techniques, and procedures
NUMI Naval Undersea Medical Institute
NWDC Navy Warfare Development Command
OB-GYN obstetrics-gynecology
OCONUS outside the continental United States
ODR operational dental readiness
OFMLS operational forces medical liaison service
OGA other government agency
OIC officer in charge
OIF Operation IRAQI FREEDOM
OP operational
OPCON operational control

NWP 4-02
JAN 2008 LOAA-12
OPLAN operation plan
OPNAV Office of the Chief of Naval Operations
OPNAVINST Chief of Naval Operations instruction
OPORD operation order
OPTAR operating target
OPZONE operation zone
OR operating room
OSCAR operational stress control and readiness
PEO patient evacuation officer
PET patient evacuation team
PIA post independent analysis
PMI patient movement item
POC point of contact
POD port of debarkation
POE port of embarkation
POL petroleum, oil, and lubricants
POM program objective memorandum
POMI plans, operations, and medical intelligence
PPBS Planning, Programming, and Budgeting System
PRBC packed red blood cells
PV prime vendor
QDR Quadrennial Defense Review
R&D research and development
RC regional commander
RCC regional combatant commander
RFF request for forces
RFI request for information
RFS request for support

NWP 4-02
LOAA-13 JAN 2008
RMC regional maintenance center
ROE rules of engagement
ROMO range of military operations
ROS reduced operating status
SA solution analysis
SEAL sea-air-land team
SecDef Secretary of Defense
SECNAV Secretary of the Navy
SECNAVINST Secretary of the Navy instruction
SELRES Selected Reserve
SG Surgeon General
SIPRNET SECRET Internet Protocol Router Network
SJFHQ standing joint force headquarters
SJFHQ-CE standing joint force headquarters-core element
SMO senior medical officer
SMDR senior medical department representative
SMR senior medical representative
SN strategic-national
SOF special operations forces
SOP standard operating procedure
SORTS Status of Resources and Training System
SORTSREPNV Status of Resource and Training System Report — Navy
SPECWAR special warfare
SPOD seaport of debarkation
SPRINT special psychiatric rapid intervention team
ST strategic-theater
STANAG standard agreement
STD sexually transmitted disease

NWP 4-02
JAN 2008 LOAA-14
STP shock trauma platoon
SUBFOR submarine forces
SURFOR surface forces
SWMI Surface Warfare Medicine Institute
TACC tactical air control center (USN)
TACON tactical control
TAD temporary additional duty
TAES theater aeromedical evacuation system
TCO technical coordinating office
TDY temporary duty
TF task force
TGRO TRICARE global remote overseas
TICHRA toxic industrial chemical health risk assessment
TMO The Medical Officer of the Marine Corps
TPFDD time-phased force and deployment data
TPFDL time-phased force and deployment list
TPMRC Theater Patient Movement Requirements Center
TYCOM type commander
UCP Unified Command Plan
UIC unit identification code
UJTL Universal Joint Task List
UN United Nations
UNTL Universal Naval Task List
USA United States Army
USAFRICOM United States Africa Command
USARIEM United States Army Research Institute of Environmental Medicine
USC United States Code
USCENTCOM United States Central Command

NWP 4-02
LOAA-15 JAN 2008
USCG COMDTINST United States Coast Guard Commandant instruction
USEUCOM United States European Command
USFFC United States Fleet Forces Command
USFJ United States Forces, Japan
USFK United States Forces, Korea
USFLTFORCOM United States Fleet Forces Command
USJFCOM United States Joint Forces Command
USMC United States Marine Corps
USN United States Navy
USNORTHCOM United States Northern Command
USNS United States Naval Ship
USPACOM United States Pacific Command
USSOCOM United States Special Operations Command
USSOUTHCOM United States Southern Command
USSTRATCOM United States Strategic Command
USTRANSCOM United States Transportation Command
VMI vendor managed inventory
WAN wide-area network
WER Weekly Epidemiological Record
WHO World Health Organization
WIA wounded in action
WRAIR Walter Reed Army Institute of Research
WWW World Wide Web

NWP 4-02
JAN 2008 LOAA-16
INTENTIONALLY BLANK

NWP 4-02
LEP-1 JAN 2008
LIST OF EFFECTIVE PAGES
Effective Pages Page Numbers
JAN 2008 1 thru 20 JAN 2008 1-1 thru 1-18 JAN 2008 2-1 thru 2-24 JAN 2008 3-1 thru 3-20 JAN 2008 4-1 thru 4-24 JAN 2008 A-1, A-2 JAN 2008 B-1, B-4 JAN 2008 C-1 thru C-6 JAN 2008 D-1 thru D-8 JAN 2008 E-1 thru E-4 JAN 2008 F-1 thru F-4 JAN 2008 G-1, G-2 JAN 2008 H-1, H-2 JAN 2008 Reference-1 thru Reference-6 JAN 2008 Glossary-1 thru Glossary-10 JAN 2008 LOAA-1 thru LOAA-16 JAN 2008 LEP-1, LEP-2

NWP 4-02
JAN 2008 LEP-2
INTENTIONALLY BLANK


NWP 4-02 JAN 2008