Embed Size (px)
Citation preview
Nutrition in the Patient with Anorexia and Cachexia
Jeanette N. Keith, M.D.
Associate Professor of Medicine
Departments of Nutrition Sciences and Medicine
University of Alabama at Birmingham
Protein-Energy Malnutrition
Two major types
• Marasmus• Kwashiorkor
(AKA: Protein Calorie Malnutrition)
Heimburger DC, Ard JD. Handbook of Clinical Nutrition 4/e, 2006

Marasmus
Clinical setting Decreased energy intake
Time course to develop Months or years
Clinical features Starved appearance
Weight < 80% standard for height
Triceps skinfold < 3 mm
Mid-arm muscle circumference < 15 cm
Laboratory findings Creatinine-height index <60% standard
Clinical course Reasonably preserved responsiveness to short term stress
Mortality Low, unless related to underlying disease
Heimburger DC, Ard JD. Handbook of Clinical Nutrition 4/e, 2006
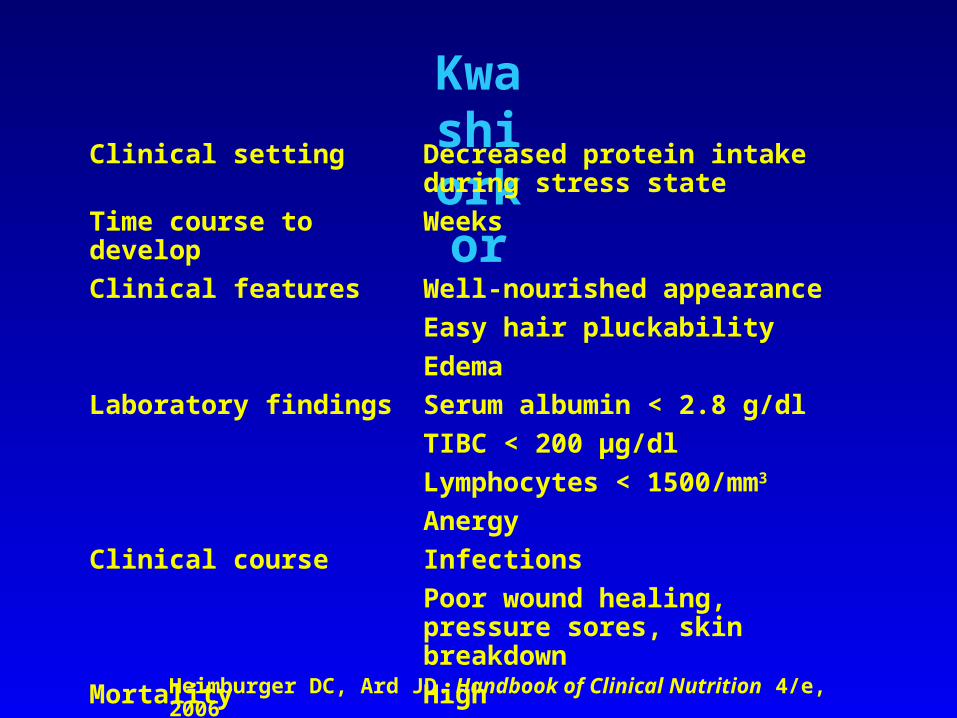
Kwashiorkor
Clinical setting Decreased protein intake during stress state
Time course to develop Weeks
Clinical features Well-nourished appearance
Easy hair pluckability
Edema
Laboratory findings Serum albumin < 2.8 g/dl
TIBC < 200 μg/dl
Lymphocytes < 1500/mm3
Anergy
Clinical course Infections
Poor wound healing, pressure sores, skin breakdown
Mortality High
Heimburger DC, Ard JD. Handbook of Clinical Nutrition 4/e, 2006
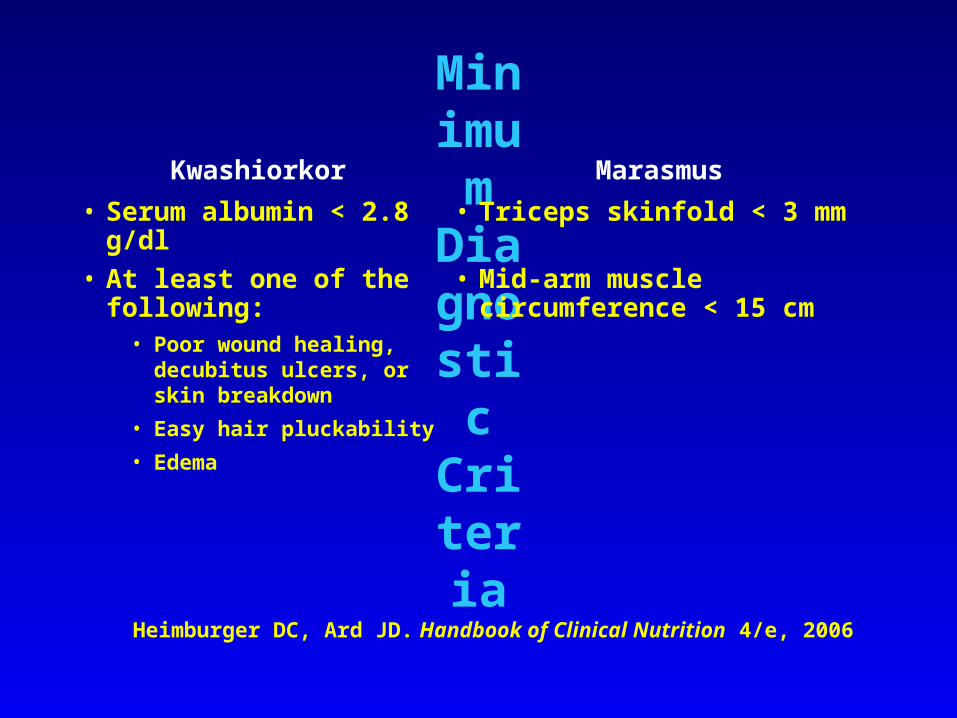
Minimum
Diagnostic Criteria
Kwashiorkor Marasmus
• Serum albumin < 2.8 g/dl • Triceps skinfold < 3 mm
• At least one of the following:
• Poor wound healing, decubitus ulcers, or skin breakdown
• Easy hair pluckability
• Edema
• Mid-arm muscle circumference < 15 cm
Heimburger DC, Ard JD. Handbook of Clinical Nutrition 4/e, 2006
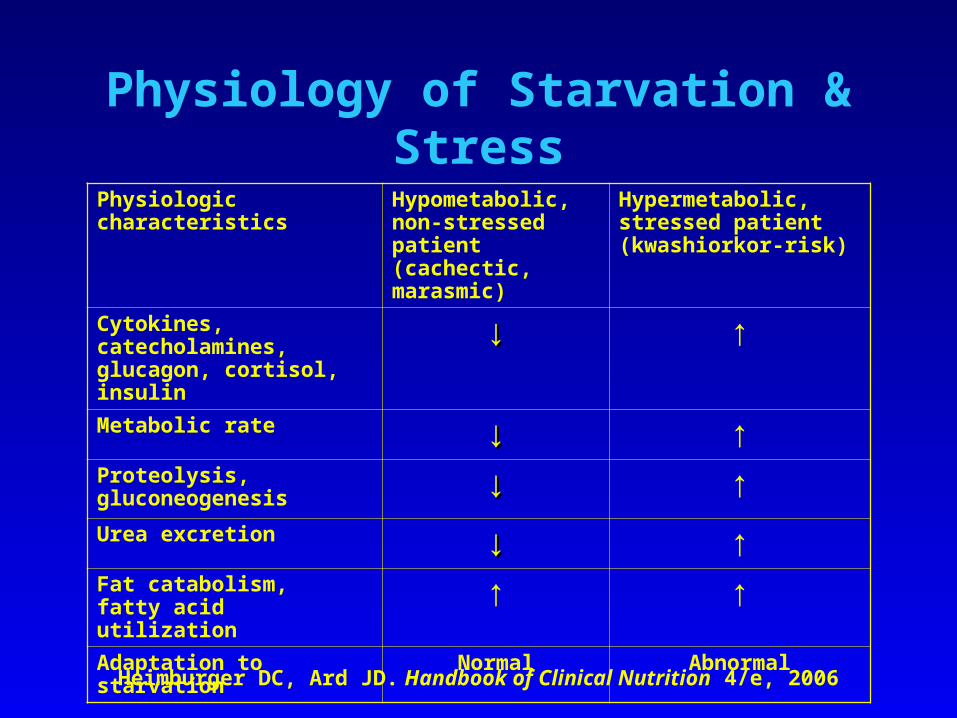
Physiology of Starvation & Stress
Physiologic characteristics Hypometabolic, non-stressed patient (cachectic, marasmic)
Hypermetabolic, stressed patient (kwashiorkor-risk)
Cytokines, catecholamines, glucagon, cortisol, insulin
↓↓ ↑
Metabolic rate ↓↓ ↑Proteolysis, gluconeogenesis ↓↓ ↑Urea excretion ↓↓ ↑Fat catabolism, fatty acid utilization ↑ ↑Adaptation to starvation Normal Abnormal
Heimburger DC, Ard JD. Handbook of Clinical Nutrition 4/e, 2006
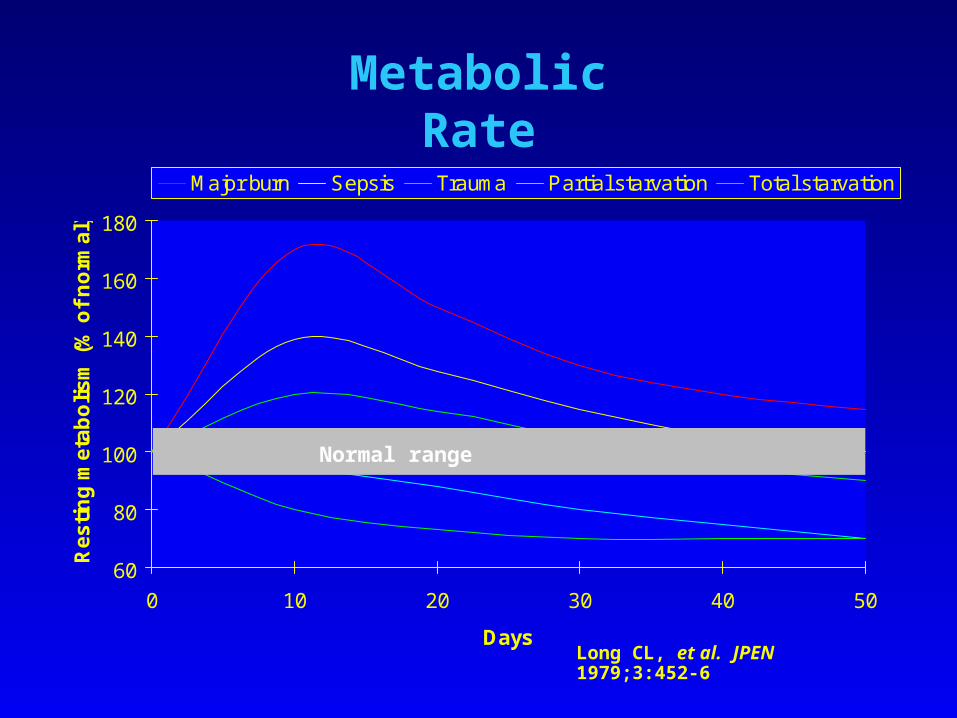
Metabolic Rate
60
80
100
120
140
160
180
0 10 20 30 40 50
Days
Re
sti
ng
me
tab
oli
sm
(%
of
no
rma
l)
Major burn Sepsis Trauma Partial starvation Total starvation
Long CL, et al. JPEN 1979;3:452-6
Normal range
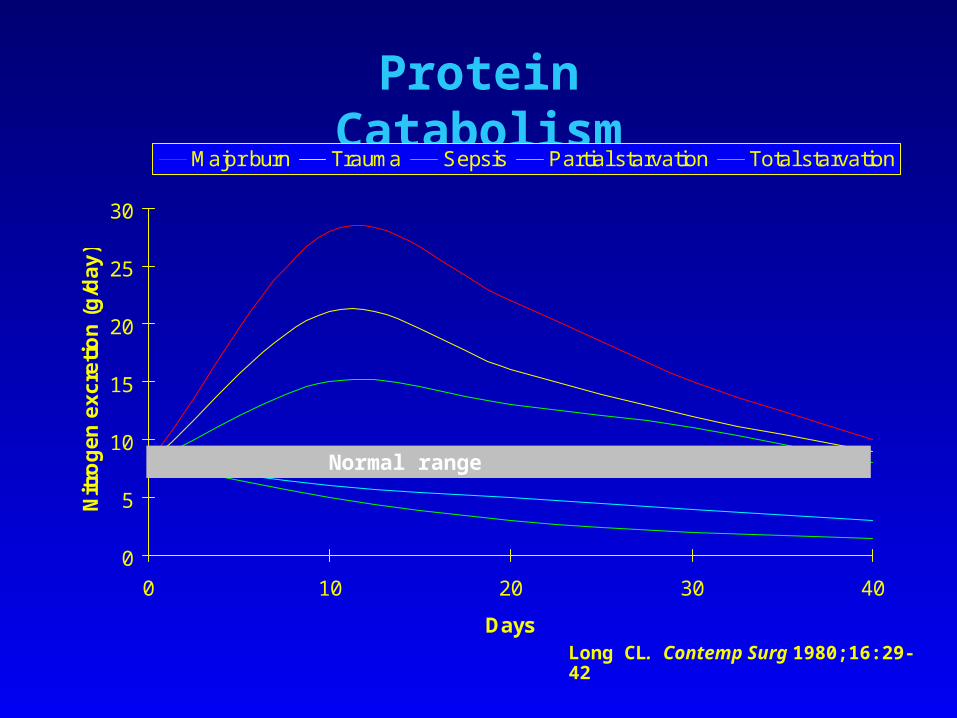
Protein Catabolism
0
5
10
15
20
25
30
0 10 20 30 40
Days
Nit
rog
en
ex
cre
tio
n (
g/d
ay
)
Major burn Trauma Sepsis Partial starvation Total starvation
Long CL. Contemp Surg 1980;16:29-42
Normal range
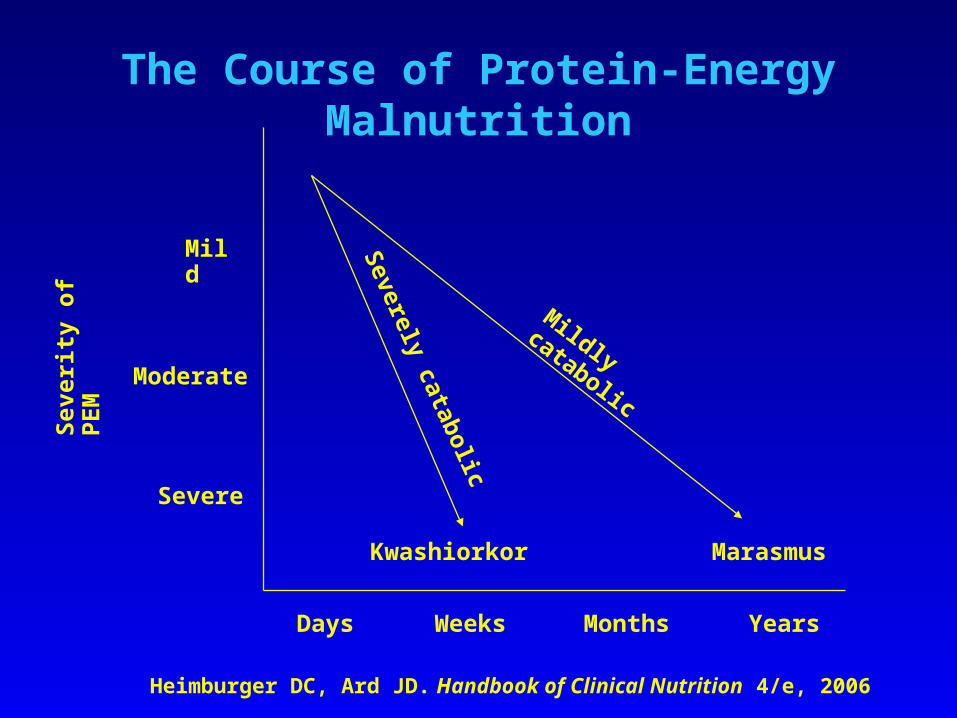
The Course of Protein-Energy Malnutrition
Mild
Moderate
Severe
Sev
erit
y o
f P
EM
Days Weeks Months Years
Kwashiorkor MarasmusS
everely catabolic
Mildly catabolic
Heimburger DC, Ard JD. Handbook of Clinical Nutrition 4/e, 2006
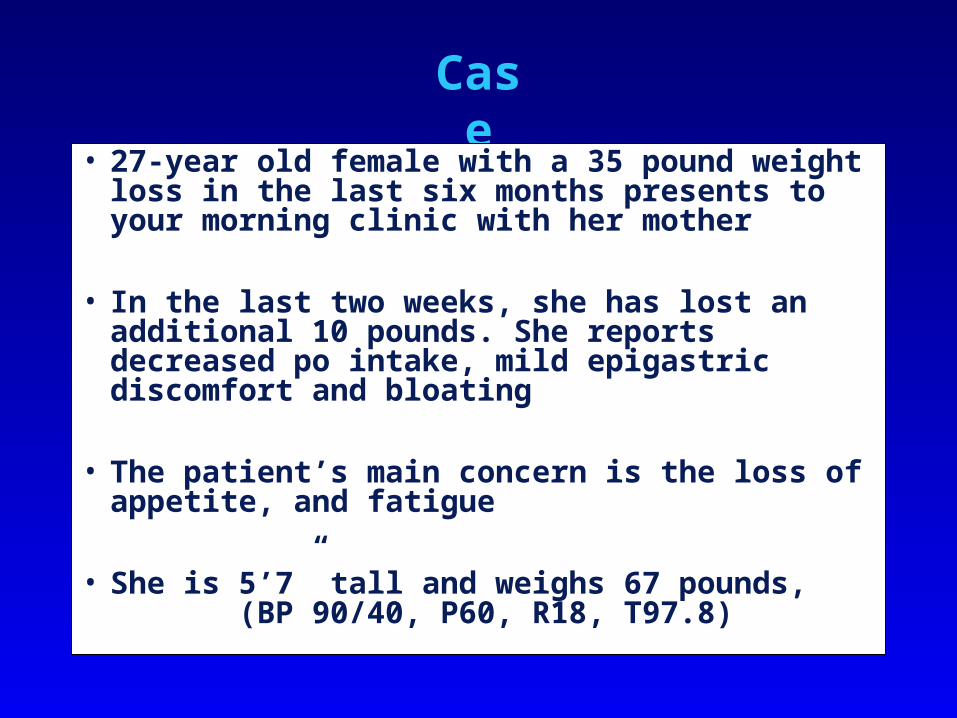
Case
Presentation
• 27-year old female with a 35 pound weight loss in the last six months presents to your morning clinic with her mother
• In the last two weeks, she has lost an additional 10 pounds. She reports decreased po intake, mild epigastric discomfort and bloating
• The patient’s main concern is the loss of appetite, and fatigue
• She is 5’7” tall and weighs 67 pounds, (BP 90/40, P60, R18, T97.8)
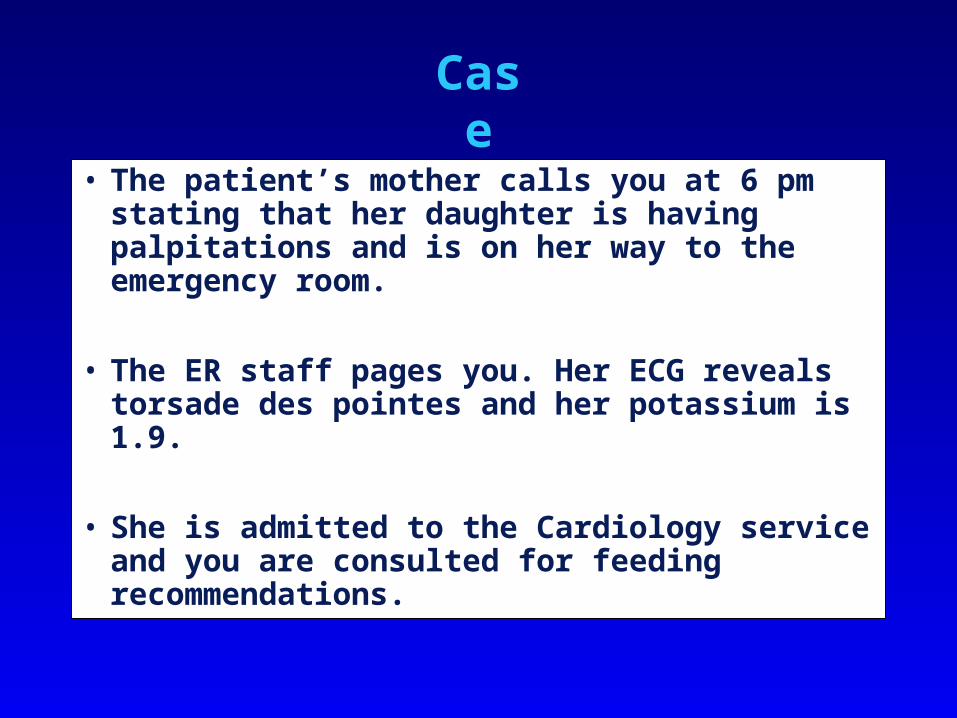
Case
Presentation
• The patient’s mother calls you at 6 pm stating that her daughter is having palpitations and is on her way to the emergency room.
• The ER staff pages you. Her ECG reveals torsade des pointes and her potassium is 1.9.
• She is admitted to the Cardiology service and you are consulted for feeding recommendations.
Case
Presentation
• What do you recommend now?– Immediate placement of a PICC catheter for TPN
initiation.
– Have the inpatient team place a dobhoff and begin tube feedings
– Call GI procedures to arrange for PEG placement and enteral feedings.
– Call Dietary for a 1600 kcal diet and begin a calorie count
– Intravenous fluids while correcting the potassium and awaiting other lab studies.
Case
Presentation
• The patient’s potassium is now normal but her course has been complicated by recurrent vomiting.
• EGD reveals a decreased gastric motility and a dilated duodenum bulb with normal motility in the second portion of the duodenum.
• What do you recommend next? – Advance her diet to clear liquids– Begin TPN– Place a post-pyloric feeding tube and begin enteral
nutrition
Case
Presentation
• You place a post pyloric feeding tube for enteral nutrition.
• What weight do you use for caloric provision?
– Ideal Body Weight– Actual Weight– Adjusted Body Weight
• How many calories per kilogram per day do you recommend?
– 35-40 kcal/kg/d– 25-30 kcal/kg/d– 15-20 kcal/kg/d– 20-30 kcal/kg/d
Case
Presentation
• On the morning after beginning her enteral feeding, the patient complains of palpitations and pain in her hands.
• On exam, her hands are swollen and she has pedal edema. Pulmonary exam reveals rales.
• Her potassium is now 2.9, phophorus is 1.8 and magnesium is 1.4.
• Diagnosis?
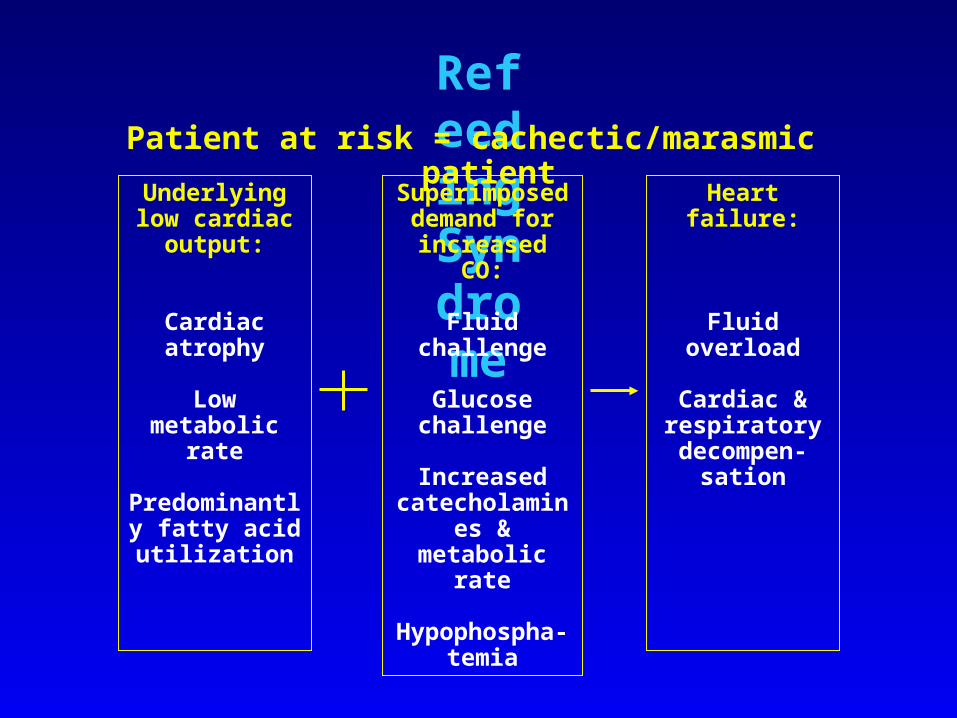
Refeeding
Syndrome
Underlying low cardiac output:
Cardiac atrophy
Low metabolic rate
Predominantly fatty acid utilization
Superimposed demand for
increased CO:
Fluid challenge
Glucose challenge
Increased catecholamines
& metabolic rate
Hypophospha-temia
Heart failure:
Fluid overload
Cardiac & respiratory decompen-
sation
Patient at risk = cachectic/marasmic patient
Case
Presentation
• The patient is admitted to inpatient psychiatry for the treatment of anorexia/bulimia nervosa.
• After 4 weeks on tube feedings, she was successfully transitioned to oral diet.
• At discharge, her weight was 99 pounds.
Selective Refeeding Approaches
• Hypometabolic, cachectic/marasmic patient– Aim = rebuild cautiously to avoid hypophosphatemia & repletion
heart failure
– Refeed gradually with
» a portion of fuel as fat
» ADEQUATE PHOSPHORUS
– Days 1-2 – BEE x 0.8
– Days 3-4 – BEE x 1.0
– Days 4-6 – BEE x 1.1-1.4
– Days 7+ – BEE x 2 if weight gain is desired
Selective Refeeding Approaches
• Hypermetabolic, stressed patient– Aim = Replace catabolic losses
– Refeed aggressively but not excessively
– Can often achieve calorie & protein goals within 48 hours
• Patient with mixed marasmic/kwashiorkor (starved but also stressed)– Metabolism is accelerated by stress
– Therefore, generally feed as you would a patient with kwashiorkor
– But watch carefully for refeeding syndrome
Key Points To Remember• The metabolic response to starvation for the
hypometabolic patient is to reduce their metabolic rate and use fat as the primary fuel source
• Visceral protein stores are preserved in early in the clinical course of the hypometabolic, starved state
• In underweight patients, use the actual body weight to avoid overfeeding.
• Monitor for re-feeding syndrome with oral, enteral or parenteral nutrition.
Take Home Points
• The stressed hypermetabolic patient is more likely to suffer the consequences of underfeeding.
• The starved, unstressed patient is at risk for the complications of overfeeding and rapid re-feeding.
• If protein calorie malnutrition (kwashiorkor-type) predominates, vigorous nutrition therapy is urgent.
• If marasmus predominates, feeding should be more cautious.