Embed Size (px)
Citation preview
Nurse Education in Practice (2007) 7, 381–391
Nurse
www.elsevierhealth.com/journals/nepr
Educationin Practice
Nursing students in clinical practice – Developinga model for clinical supervision
Arja Haggman-Laitila a,*, Eriksson Elina b, Meretoja Riitta c,Sillanpaa Kirsi d, Rekola Leena e
a University of Kuopio, Helsinki Polytechnic, HealthCare and Social Services, P.O. Box 4030,FIN-00099 City of Helsinki, Finlandb University of Turku, Helsinki Polytechnic, HealthCare and Social Services, P.O. Box 4030,FIN-00099 City of Helsinki, Finlandc Corporate Headquarters, Hospital District of Helsinki and Uusimaa, P.O. Box 100,FIN-00029 City of Helsinki, Finlandd Hospital District of Helsinki and Uusimaa, P.O. Box 100, FIN-00029 City of Helsinki, Finlande Helsinki Polytechnic, HealthCare and Social Services, P.O. Box 4030, FIN-00099 City of Helsinki,Finland
Accepted 27 November 2006
Summary The aim of this study was to develop a model for clinical supervision topromote the clinical practice of nursing students. The study was implemented inFinland and it was carried out in three phases. Firstly, data were collected by meansof a literature review and focus group interviews. Secondly, the data were analysedand described in expert groups, and finally the model itself was evaluated by 23nursing experts. The data of literature review and focus group interviews consistedof 27 studies and four groups from three organisations: nurses (n = 7), managers(n = 6), teachers (n = 8) and students (n = 6). The data were analysed by qualitativecontent analysis. The model devolved from the study includes the concepts describ-ing prerequisites, content and influence of clinical supervision. The prerequisitesare nursing skills, a holistic view of the nursing curriculum, pedagogical, organisa-tional, development, cooperation and interaction competence and decision-makingskills. The content of clinical supervision includes support of professional develop-ment, pedagogical competence, research and development activities and collabora-tive working. Clinical supervision has influence on students’ professional andpersonal development and conception of the future of nursing profession, students’
KEYWORDSClinical supervision;Nursing students;Nursing teachers;Nursing preceptors
1d
h
471-5953/$ - see front matter �c 2006 Elsevier Ltd. All rights reserved.oi:10.1016/j.nepr.2006.11.011
* Corresponding author. Tel.: +358 44 5290065.E-mail addresses: [email protected], [email protected], [email protected], kirsi.sillanpaa@
us.fi, [email protected].

382 A. Haggman-Laitila et al.
preparedness for career planning and the teacher’s and preceptor’s professionaldevelopment. The model could unify the notions of all parties concerned of the pre-requisites, content and influence of clinical supervision. Furthermore, the entiresupervision process and its control could be clarified. The model may be utilisedin selecting and educating preceptors and evaluating the quality of clinical supervi-sion.
�c 2006 Elsevier Ltd. All rights reserved.
Introduction
Supervised clinical practice plays a significant rolein professional nursing studies. It guarantees thehigh quality of nursing education, reinforces theprofessionalism of graduating students and pro-motes the appeal of the nursing professions (Grayand Smith, 2000; Sue and Chow, 2001; Ohrling andHallberg, 2001; Aston and Molassiotis, 2003; Clearyet al., 2006). The provision of appropriate clinicalsupervision of nursing students is acknowledged tobe problematic for example in Finland, Great Brit-ain, Canada and Australia (Andrews and Wallis,1999; Koh, 2002; Aston and Molassiotis, 2003; Vuori-nen et al., 2005; Cleary et al., 2006; O’Donovan,2006). Government and professional recommenda-tions emphasise the need to develop learning inpractice settings in pre-registration programmes.The development of clinical supervision of nursingstudents is a mutual challenge to the health careorganisations and the nursing education.
Earlier studies show that the implementation ofsupervision in clinical practice varies in type,quality and quantity. Supervision occurs in con-junction with working with patients and variesaccording to the supervisor, the workload of theunit and the atmosphere of the setting. The defi-nition and purpose of clinical supervision lacksclarity. The content of supervision is defined pri-marily from the core curriculum and the input ofteachers. The views of students and employeesin clinical settings are not reflected adequately,although their role in student supervision is cen-tral. The effectiveness and cost-effectiveness ofclinical supervision has not been examined (An-drews and Wallis, 1999; Koh, 2002; Aston andMolassiotis, 2003; Vuorinen et al., 2005; Clearyet al., 2006).
The purpose of this article is to describe a mod-el for clinical supervision, which has been devel-oped in Finland to promote the clinical practiceof nursing students. This study is part of a cooper-ation project between health care organisationsand a polytechnic, which aims at developing apreceptor’s tasks and supervision environment.In Finland nursing education is provided at poly-
technics and universities. The extent of clinicalpractice at polytechnics is 75 credit units(2000 h), and it is set and qualified by EuropeanUnion directives. The clinical practice consists ofbasic and professional studies. It is implementedin a variety of clinical settings during differentstages of care provision both in primary and spec-ialised health care dissemination. The purpose ofthe clinical practice is to provide students withsupervised orientation to focal practical profes-sional tasks, which are central to their studies,as well as to qualify them for applying theirknowledge and competence in their professionallives. In Finland nursing managers are in chargeof the clinical supervision of students and the en-tire personnel partake in it. A preceptor, who hasbeen assigned for the task, is responsible for thesupervision of a single student. Preceptors workas subject matter experts and they supervise stu-dents while performing their duties as nurses.Moreover, they are responsible for the implemen-tation and evaluation of the student’s clinicalpractice with the teacher. Preceptors inform thepersonnel of the objectives and individual imple-mentation plan of the student. To meet therequirements, the preceptor must be willing toundertake the task and represent the same pro-fession as the student. The competence level ofpreceptors is varying because only few of themhave accomplished a preceptorship training pro-gramme. Furthermore, no general recommenda-tions exist concerning their work experience andits length. Close cooperation and mutual agree-ment on the division of labour is expected ofteachers, nursing managers and preceptors.
Development needs for clinicalsupervision
Research projects in the past have indicated indis-putable development needs regarding the content,preceptor’s role and supervision, and cooperationbetween teachers, students and preceptors in thesupervision of clinical practice. The content ofsupervision and the role of the preceptor involve

Nursing students in clinical practice – Developing a model for clinical supervision 383
ambiguity, which impedes the visualisation ofsupervision (Neary, 1997; Andrews and Wallis,1999; Vuorinen et al., 2005). The selection processfor the nurses working as preceptors is not system-atic, and the needs of their supplementary educa-tion are not recognised. According to students andpreceptors, preceptors lack resources for clinicalsupervision and this disrupts especially the stu-dents’ concretisation of nursing reality and envi-ronment. All these aspects have resulted inincreased workload, increased stress and feelingsof inadequacy experienced by many preceptorswith regard to the expectations placed on them(Yonge et al., 2002). Similarly, education is notfully utilised in the teaching process of supervision,although earlier studies show that it is possible todevelop the preceptors’ pedagogical and evalua-tion competence by means of supplementary edu-cation (Watson, 1999; Usher et al., 1999; Duffyet al., 2000; Pulsford and Owen, 2002; Clearyet al., 2006).
Cooperation and agreement on the division of la-bour between teachers, nursing management andpreceptors should be based on the defining of tasksin clinical supervision and the collaborative methodof working (Neary, 1997; Ohrling and Hallberg,2001). However, defining a preceptor’s tasks isinadequate on numerous occasions. Task define-ment can advance students’ learning in connectionwith simultaneous preceptors’ educational andorganisational support (Ohrling and Hallberg,2001). It has been established that close coopera-tion and distinct division of labour increase thequality of clinical supervision (for example Pulsfordand Owen, 2002; Yonge et al., 2002). Students andpreceptors need to be adequately prepared fortheir roles as supervisors and supervisees (Astonand Molassiotis, 2003).
The special characteristics and phases of thesupervision process between the preceptor andstudent have not been sufficiently identified,although single studies have paid attention tothe phenomenon nearly 10 years ago. For exam-ple, Neary (1997) reported on the partnershipmodel based on the experiences of nursing stu-dents and nursing staff. According this model, astaff member is responsible for students’ clinicalsupervision, with the support of other staff mem-bers in accordance with agreed guidelines. Stu-dents’ assessment is summative in nature. Thepartnership model takes into consideration thatpreceptors’ expertise is connected to theoreticalknowledge, which is central to students’ learning.This enables the gradual analysis of the connec-tion between theory and practice by utilising sin-gle patient situations in supervision. Moreover,
the student is instructed to evaluate the nursingsituations as unique experiences in which studentability to detect, recognise and understand theconnection between theory and practice will grad-ually develop into professional competence. Stu-dents regard the development of reflection skillsessential in their professional growth (Koh, 2002;O’Donovan, 2006). According to them, reflectionencourages the integration of theory and practice,increases self-awareness and leads to a morequestioning approach in the delivery of care. Cre-ative teaching methods based on reflection areneeded to facilitate student learning (Clearyet al., 2006; O’Donovan, 2006).
Student support is facilitated by the accepting,individual attitude of preceptors and by the posi-tive attitude of the health care personnel towardsthe students. The preceptors integrate the stu-dents into the community of clinical settings andshare their experiences of the teaching situations(Neary, 1997; Cleary et al., 2006). Learning worksbest when preceptors develop a caring and trustingrelationship with students (O’Donovan, 2006).Stress and anxiety commonly reported among stu-dents may be alleviated by appropriate supervi-sion. Students themselves also emphasise theneed for peer support and shared learning. Thesharing of experiences reveals to students thatthey are not alone with problems in practice andtheir self-confidence enhances (Koh, 2002; Astonand Molassiotis, 2003). There are only few pub-lished studies on the students’ peer systems (Astonand Molassiotis, 2003).
Aim of the study
The aim of this study was to develop a model forpromoting the clinical supervision of nursing stu-dents during their clinical practice. The modelcombines the perspectives of students, their teach-ers, the nurses working as preceptors and theirdirectors. The research question was: What arethe concepts describing prerequisites, contentand influence of clinical supervision?
Study design
The development of the model was implemented inthree phases. Firstly, data were collected by meansof a literature review and focus group interviews.Secondly, the data were analysed in expert groups,and finally the model itself was evaluated by 23nursing experts. The collected data and their anal-yses are central to the credibility of the model. In

384 A. Haggman-Laitila et al.
this study, the credibility of the research was rein-forced by methodological triangulation.
Literature review
The purpose of the literature review was to producereliable and extensive data of the phenomenon bycombining several study findings irrespective ofeach other (Evans and Pearson, 2001; Evans, 2002;Burns and Grove, 2005). The data for the literaturereview were collected from the CINAHL Database,Medline, British Nursing Index and the Finnish Medicdatabase. Search terms produced altogether 785references. The English terms ‘‘education’’, ‘‘nurs-ing’’, ‘‘students’’, ‘‘clinical & mentorship’’ pro-duced 237 references, whereas ‘‘learningenvironment’’ provided 220, ‘‘preceptorship’’ 198and ‘‘clinical supervision & education’’ providedfour references. The Finnish search terms produced126 references from the Medic database: ‘‘oppimi-nen’’ produced 65 references, ‘‘kaytanto’’ 40,‘‘harjoittelu’’ 17, ‘‘ohjaus & kaytannon ohjaaja’’one and ‘‘ohjaus’’ three. In addition, manualsearch was carried out with Finnish researches. Ofthe references obtained, those researches whosetopics or abstracts did not deal with the prerequi-sites, content or influence of the nursing students’clinical supervision were eliminated. The studiesthat were included described experiences of nurs-ing students and preceptors, the content of theconcept of supervision, the preceptors’ supportand the influence of education on their perfor-mance, and the influence of clinical supervisionon students’ learning. The final data consisted of27 researches between 1990 and 2003, and covered19 researches from the CINAHL Database, Medlineand British Nursing Index, seven from the Medicdatabase and one research as a result of the manualsearch.
Of the chosen studies, nine were carried out inGreat Britain, nine in Finland and six in Canada.Thirteen were qualitative and 11 were quantita-tive, whereas one of the studies was an action re-search. Methodological triangulation was used inthree of the studies. The sample size in the quanti-tative studies varied from 37 to 558 informants.The methods of analysis ranged from descriptivestatistical methods to statistical tests. At the sametime, the number of informants varied from 9 to105 in the qualitative studies. Their data were col-lected mainly by individual interviews.
Over 80% of the publications of the chosen re-search theme were identified through the Medlinedatabase (Brazier and Begley, 1996). The searchprocess was complicated because of the diversity
of the concepts concerning the research theme(cf. Andrews and Wallis, 1999; Saarikoski, 2002).This may have left some relevant research out ofthe review, but the data may be largely consideredrepresentative because the international re-searches have been reported in scientific journals.However, the Finnish nursing science researcheswere mainly master theses, which restricts thecredibility of the study for their part. Since onlyfew national scientific articles exist on the re-search topic and since applying international stud-ies to Finnish circumstances is not without itsproblems due to different nursing and educationalbackgrounds, the master theses were included inthe study.
Focus group interviews
The focus group interviews consisted of fourgroups (Webb and Kevern, 2001; McLafferty,2004). The participants for these groups wereselected from six specialist fields of a universityhospital as well as nursing teachers and studentsfrom two polytechnics. The organisations gavetheir written consent, which constituted ethicalapproval, to carry out the interviews. All partici-pants were chosen by convenience sample andtheir participation was on voluntary basis. Nursingteachers and students selected their representa-tives to take part in the interviews whereas nurs-ing directors decided on the representatives ofnursing managers. The first group was formed ofnurses (n = 7), the second of nursing managers(four ward managers and two directors of nurs-ing), and the third of nursing teachers (n = 8).The nursing students who were in the final stagesof their studies formed the fourth group (n = 6).All the interviewees were informed of the pur-pose of the study, method of data analysis,reporting and the ethical questions related tothe study in writing in advance. Likewise, the par-ticipants were informed of the tape-recording,interview themes and the estimated duration ofthe interview.
The interviews were carried out in October andNovember 2003. The average age of the nurses was45 years and their work experience ranged from 15to 34 years, of which they had worked from 7 to23 years in their current specialisation field. Theywere registered nurses and nurse specialists bytheir basic education. Four of the nurses hadaccomplished university studies in the field of nurs-ing science and education. The average age for thenursing managers was 49 years and their workexperience varied from 19 to 40 years, of which

Nursing students in clinical practice – Developing a model for clinical supervision 385
they had worked in their present position from 2months up to 22 years. In addition to their nursingeducation, they had a master degree or were in theprocess of completing it. The number of nursingstudents in the work units of the nurses and nursingmanagers’ varied from 2 to 10 per term, and thestudents’ phase of studies extended from initialto final stages. The nursing teachers’ average agewas 51 and their health care work experience var-ied from 20 to 34 years, of which they had heldtheir current position between 10 and 28 years.Apart from having a nursing education, the teach-ers all had a master degree. During each term,they counselled 10–40 students within variousmedical specialisation fields. The average age forthe nursing students was 28. Two students had aprevious health care degree and work experiencebetween 3 and 16 years.
The focus group interviews were carried out inthe premises of a polytechnic, and the durationof each interview was 1.5 h. The focus groups wereasked to describe their notions concerning the pre-requisites of clinical supervision, its content andinfluence on learning. The lead interviewer intro-duced the interview themes, focused the discus-sion when necessary and ensured the progressionof the discussion from one theme to another. Theassisting interviewer’s task was to guide the leadinterviewer in the allocation of time and recordthe contributions of each participant.
The members of each focus group gave their oralconsent to the tape-recording of the interviews andto the use of the collected information. Moreover,they were informed of the purpose for the inter-viewers’ presence. The background information ofthe interviewees was collected on a separate datacollection sheet after the interview. The interviewenvironment was quiet and no external distur-bances occurred.
From the perspective of the validity of the focusgroup results, it is essential that the informantshave personal experience of the topic under study.The participants in the study had different experi-ences of supervision in various contexts. Thisincreased the variability of the information col-lected through the focus group interviews (McLaff-erty, 2004). The participants proved to bemotivated to partake in the focus group interviews,and they were verbose in relating to their experi-ences. They had received information concerningthe interview themes in advance, and they wereprepared for the focus group interviews (Wilhelms-son and Foldevi, 2003; McLafferty, 2004).
The focus group interviews were presentedwith added depth because two researchers con-ducted them (Wilhelmsson and Foldevi, 2003).
They succeeded in creating the conditions for hav-ing an interview ambience in which openness andconfidentiality prevailed. The openness of theatmosphere was depicted by the fact that theinterviewees posed questions and comments toeach other (Webb and Kevern, 2001; McLafferty,2004). The interviewed focus groups had a homog-enous background, which added to the cohesion ofthem. It has been established that the cohesion ofthe focus group influences the intensity of theconversation, the extent to which topics underdiscussion are dealt with as well as the degreeto which the interview situations are experiencedconfidential in nature. It also increases the depthand genuineness of the extracted research data(McLafferty, 2004).
On the other hand, the presence of two inter-viewers can increase the control exercised duringthe focus group interview and create pressure toplease the interviewers. In focus group interviews,the interviewees also exercise control over eachother, which increases their attempts towardsproviding truthful information. All the participantsin the interviews had personal experience of thesame theme, which strengthened the share ofcontrol in the interview situation (McLafferty,2004).
Data analyses
The data were analysed by qualitative contentanalysis (Woods et al., 2002; Graneheim and Lund-man, 2004). The entire article or report served as aunit of analysis for the data collected through theliterature review. The focus group interviews weretranscribed in detail and the data were analysedseparately by the informant groups. The searchwas carried out deductively to find expressionsdescribing prerequisites, content and influence ofclinical supervision. The expressions were thenanalysed inductively. The expressions denotingsimilar meanings were entered in groups, and thesegroups were then named according to their con-tent. The categories containing similar contextswere combined, and main categories were formed.Lastly, the categorising process resulted in mainand subcategories describing prerequisites, con-tent and influence of clinical supervision (Figs. 1and 2, Table 1).
One researcher analysed the data of literaturereview, but in all ambiguous situations two otherresearchers participated in the analysis process.The data from focus group interviews were ana-lysed by the researchers who had acted as inter-viewers. However, the classification of that datawas verified with the research team formed by
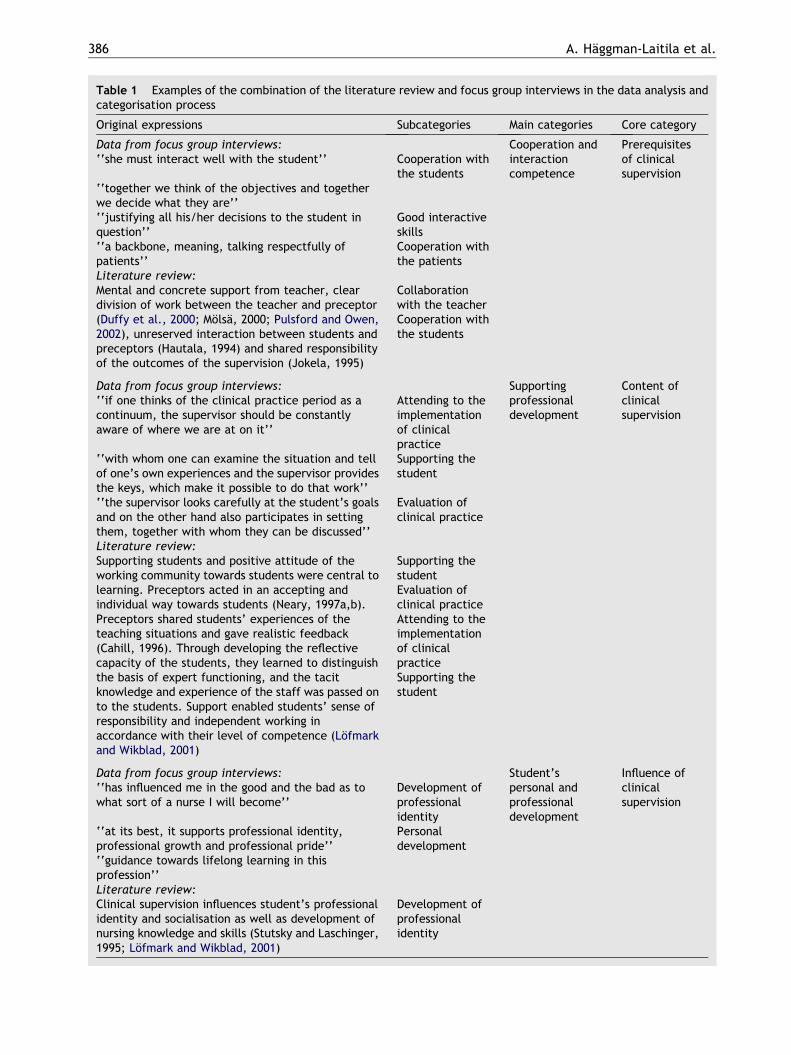
Table 1 Examples of the combination of the literature review and focus group interviews in the data analysis andcategorisation process
Original expressions Subcategories Main categories Core category
Data from focus group interviews: Cooperation andinteractioncompetence
Prerequisitesof clinicalsupervision
‘‘she must interact well with the student’’ Cooperation withthe students
‘‘together we think of the objectives and togetherwe decide what they are’’‘‘justifying all his/her decisions to the student inquestion’’
Good interactiveskills
‘‘a backbone, meaning, talking respectfully ofpatients’’
Cooperation withthe patients
Literature review:Mental and concrete support from teacher, cleardivision of work between the teacher and preceptor(Duffy et al., 2000; Molsa, 2000; Pulsford and Owen,2002), unreserved interaction between students andpreceptors (Hautala, 1994) and shared responsibilityof the outcomes of the supervision (Jokela, 1995)
Collaborationwith the teacherCooperation withthe students
Data from focus group interviews: Supportingprofessionaldevelopment
Content ofclinicalsupervision
‘‘if one thinks of the clinical practice period as acontinuum, the supervisor should be constantlyaware of where we are at on it’’
Attending to theimplementationof clinicalpractice
‘‘with whom one can examine the situation and tellof one’s own experiences and the supervisor providesthe keys, which make it possible to do that work’’
Supporting thestudent
‘‘the supervisor looks carefully at the student’s goalsand on the other hand also participates in settingthem, together with whom they can be discussed’’
Evaluation ofclinical practice
Literature review:Supporting students and positive attitude of theworking community towards students were central tolearning. Preceptors acted in an accepting andindividual way towards students (Neary, 1997a,b).Preceptors shared students’ experiences of theteaching situations and gave realistic feedback(Cahill, 1996). Through developing the reflectivecapacity of the students, they learned to distinguishthe basis of expert functioning, and the tacitknowledge and experience of the staff was passed onto the students. Support enabled students’ sense ofresponsibility and independent working inaccordance with their level of competence (Lofmarkand Wikblad, 2001)
Supporting thestudentEvaluation ofclinical practiceAttending to theimplementationof clinicalpracticeSupporting thestudent
Data from focus group interviews: Student’spersonal andprofessionaldevelopment
Influence ofclinicalsupervision
‘‘has influenced me in the good and the bad as towhat sort of a nurse I will become’’
Development ofprofessionalidentity
‘‘at its best, it supports professional identity,professional growth and professional pride’’
Personaldevelopment
‘‘guidance towards lifelong learning in thisprofession’’Literature review:Clinical supervision influences student’s professionalidentity and socialisation as well as development ofnursing knowledge and skills (Stutsky and Laschinger,1995; Lofmark and Wikblad, 2001)
Development ofprofessionalidentity
386 A. Haggman-Laitila et al.
* Support of professionaldevelopment
* Pedagogical competence* Research and development
activities* Collaborative
working
PREREQUISITES
INFLUENCES
Nursing skills
Holistic view of nursingcurriculum
Pedagogical and organisationalcompetence
Familiarisation with organisationand preceptors’ prerequisites of competence
Development competence
Cooperation and interactioncompetence
Decision-making skills
Content of clinical supervision:
Conception of nursing
Students’ professionaland personaldevelopment
Students’preparedness for career planning
Development of nursing profession
Teacher’s and preceptor’s professionaldevelopment
Figure 1 Model for clinical supervision.
Networks and their creationDevelopment of multi-professional cooperationDuties involving public relations and reporting
Establishing goalsPlanning implementation of clinical practiceAttending to implementationEvaluation of clinical practiceSupporting student
Education of staff and preceptorsDevelopment of learning methods and environmentVerifying and developing quality of clinical practice and environmentDevelopment of content of curriculum
Supervision and coordination of final thesisIntegration of final thesis and development projects into clinical practice processesPublication activitiesApplication of latest research knowledge
Support of professionaldevelopment
Pedagogicalcompetence
Research and developmentactivities
Collaborativeworking
Figure 2 The content of clinical supervision.
Nursing students in clinical practice – Developing a model for clinical supervision 387
the authors of this article, and the categoriesdescribing the data were reached on the principleof consensus. The research categories were re-
ported by describing their relation to the originalexpressions (Webb and Kevern, 2001; Woodset al., 2002; Wilhelmsson and Foldevi, 2003).

388 A. Haggman-Laitila et al.
Development of the model by expertanalysis
The authors of this article composed the modelpromoting clinical supervision based on the litera-ture review and the focus group interviews. Themodel was formulated according to research ques-tion on three core concepts, prerequisites, contentand influence of clinical supervision. The researchteam clarified the concepts produced by the dataand incorporated two main concepts to the coreconcept of ‘‘content’’, that is research and devel-opment activities as well as pedagogical compe-tence, which did not emerge clearly from thedata, but which were unanimously consideredimportant and significant to the model. After thedevelopment of the model, it was introduced tonursing experts in surgical and gynaecological set-tings. The groups consisted of 23 nurses, directorsand teachers of nursing, in total. They reportedtheir evaluation as a memorandum and verbally ina research team’s meeting. The groups approvedthe development model, and the improvementssuggested were mainly stylistic in nature.
Each core concept has been defined by usingmain concepts. The content of supervision hasbeen defined in more detail than the other con-cepts to maximise the development of the modelin the future. The definitions of the model arebased on the findings throughout the research pro-cess. The concepts of the model may be consideredexplicit and credible if the reader is able to followthe process, which resulted in the selection (cf.Woods et al., 2002; Graneheim and Lundman,2004). This was due to a careful and detaileddescription of the development process of themodel and the relationship of the results with theoriginal data (cf. Table 1). In the formulation ofthe concepts, the views of health care organisa-tions were taken into consideration. By this, thecomparability of the model to health care organisa-tions was increased.
Results
The model describing clinical supervision
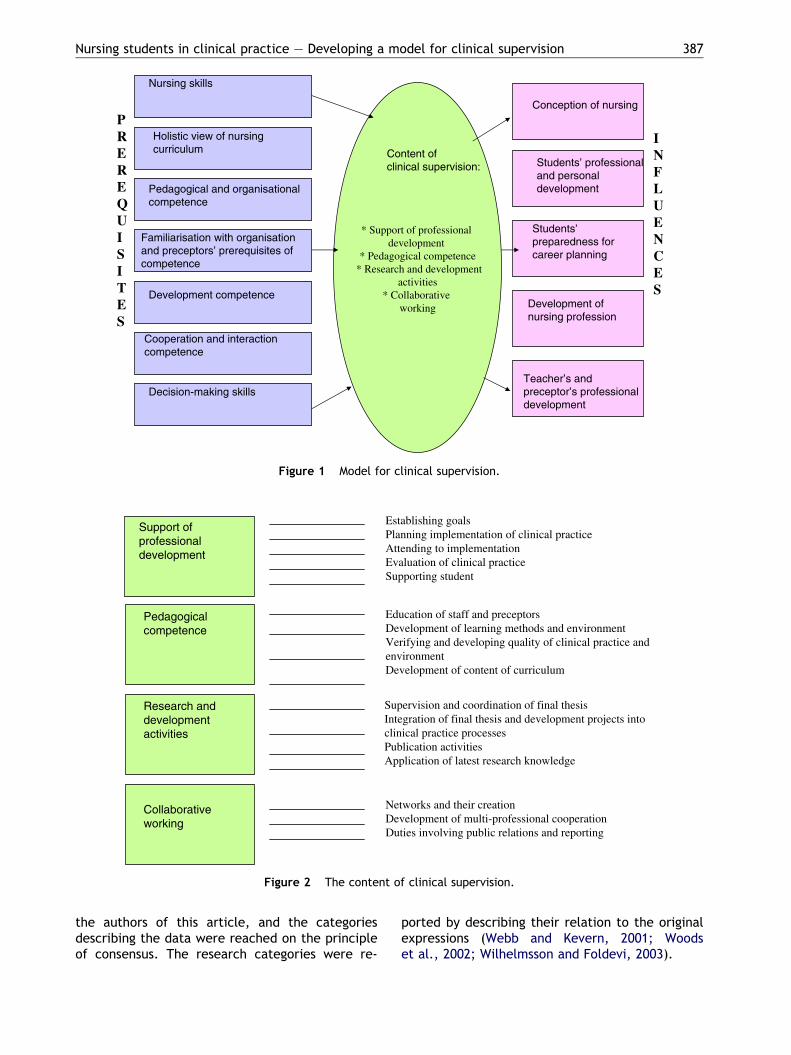
Fig. 1 illustrates the model for clinical supervisionbased on the literature review, focus group inter-views and expert analysis (cf. Table 1). The coreconcepts of the model are prerequisites, contentand influence of clinical supervision. The divisionof the core concepts into main categories is illus-trated in Fig. 1.
The prerequisites for clinical supervision
The prerequisites for clinical supervision were con-cretised in the competence of an individual pre-ceptor. The implementation of the model forsupervision requires nursing skills; a holistic viewof the nursing curriculum; pedagogical and organi-sational competence in supervision; developmentcompetence; cooperation and interaction compe-tence; decision-making skills; and familiarisationwith the organisation and preceptors’ prerequisitesof competence (Fig. 1).
Theoretical, clinical and ethical skills areemphasised as prerequisites for clinical supervisionin connection with nursing skills. The preceptorworks as an expert of nursing in a ward. Preceptorsshould possess comprehensive knowledge of nurs-ing; have solid practical skills; and high qualitystandards for ethics and their work. Motivation,understanding the significance of supervision andorganising the supervision are highlighted with re-gard to competence in supervision. If the precep-tors do not possess these skills or are notfamiliar with the curriculum, they cannot assumethe duties of a preceptor. Acquisition and accep-tance of current knowledge, and the recognitionof own development needs are included in thedevelopment competence. The preceptor shouldbe knowledgeable about the development innursing.
Organisational competence covers a preceptor’sbasic work duties and the familiarity with the pa-tient’s overall care and nursing path. In additionto these, the reflection of own activities in refer-ence to the care system, familiarity with the entireorganisation and the recognition of the basic dutiesof other health care professionals, such as doctorsand physiotherapists, are all included.
Preceptors cooperate with students, teachersand other preceptors. Therefore, it is assumedthat they are able to create and maintain positiveand goal-oriented relationships with students andteachers. Interaction and mutual responsibilityfor the results of the supervision are expectedof both students and preceptors. The teachershould provide both emotional and direct supportto the preceptor, and they should have clear divi-sion of labour concerning clinical supervision. Oneof the prerequisites of preceptors is also the abil-ity to justify and explain the decisions theymake.
Education deepens the pedagogical competenceof preceptors and clarifies their role. Various formsof support, such as recognition of the title, ap-proval of leadership and colleagues, possibility to
Nursing students in clinical practice – Developing a model for clinical supervision 389
teach and learn, and concrete measures of reward-ing promote the commitment of the preceptors inclinical supervision. Supervision is committed andenthusiastic in those wards in which good coopera-tion, high work morale and development activitiesthrive.
The content of clinical supervision
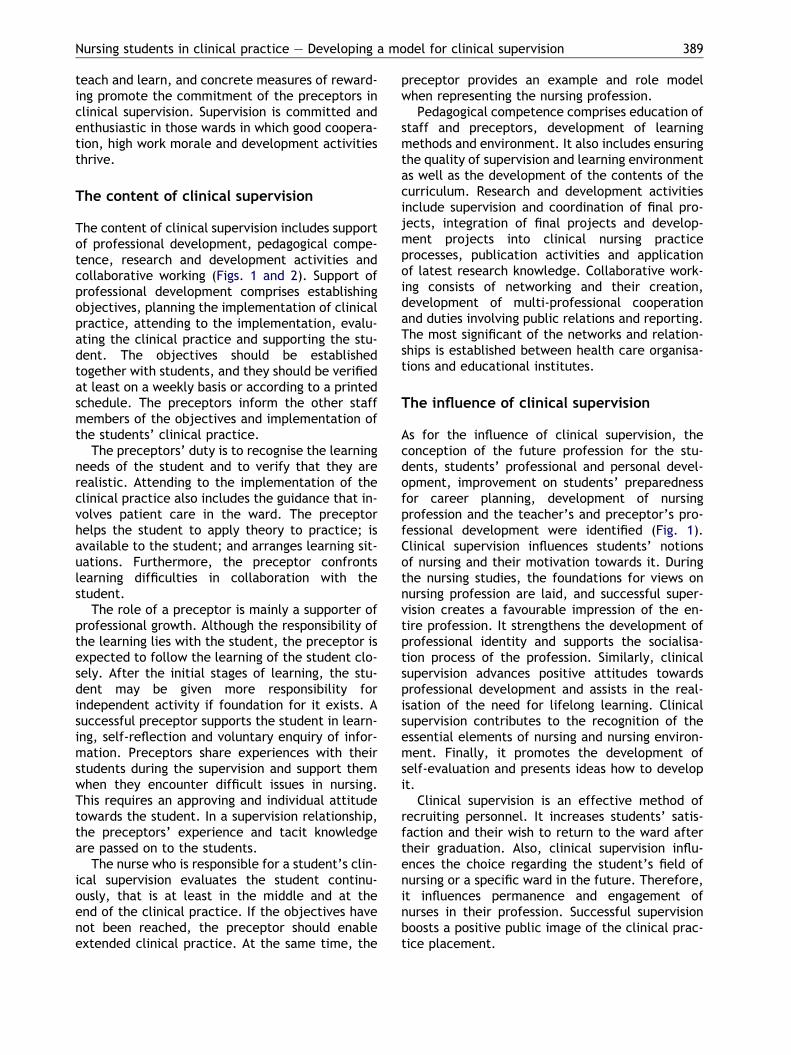
The content of clinical supervision includes supportof professional development, pedagogical compe-tence, research and development activities andcollaborative working (Figs. 1 and 2). Support ofprofessional development comprises establishingobjectives, planning the implementation of clinicalpractice, attending to the implementation, evalu-ating the clinical practice and supporting the stu-dent. The objectives should be establishedtogether with students, and they should be verifiedat least on a weekly basis or according to a printedschedule. The preceptors inform the other staffmembers of the objectives and implementation ofthe students’ clinical practice.
The preceptors’ duty is to recognise the learningneeds of the student and to verify that they arerealistic. Attending to the implementation of theclinical practice also includes the guidance that in-volves patient care in the ward. The preceptorhelps the student to apply theory to practice; isavailable to the student; and arranges learning sit-uations. Furthermore, the preceptor confrontslearning difficulties in collaboration with thestudent.
The role of a preceptor is mainly a supporter ofprofessional growth. Although the responsibility ofthe learning lies with the student, the preceptor isexpected to follow the learning of the student clo-sely. After the initial stages of learning, the stu-dent may be given more responsibility forindependent activity if foundation for it exists. Asuccessful preceptor supports the student in learn-ing, self-reflection and voluntary enquiry of infor-mation. Preceptors share experiences with theirstudents during the supervision and support themwhen they encounter difficult issues in nursing.This requires an approving and individual attitudetowards the student. In a supervision relationship,the preceptors’ experience and tacit knowledgeare passed on to the students.
The nurse who is responsible for a student’s clin-ical supervision evaluates the student continu-ously, that is at least in the middle and at theend of the clinical practice. If the objectives havenot been reached, the preceptor should enableextended clinical practice. At the same time, the
preceptor provides an example and role modelwhen representing the nursing profession.
Pedagogical competence comprises education ofstaff and preceptors, development of learningmethods and environment. It also includes ensuringthe quality of supervision and learning environmentas well as the development of the contents of thecurriculum. Research and development activitiesinclude supervision and coordination of final pro-jects, integration of final projects and develop-ment projects into clinical nursing practiceprocesses, publication activities and applicationof latest research knowledge. Collaborative work-ing consists of networking and their creation,development of multi-professional cooperationand duties involving public relations and reporting.The most significant of the networks and relation-ships is established between health care organisa-tions and educational institutes.
The influence of clinical supervision
As for the influence of clinical supervision, theconception of the future profession for the stu-dents, students’ professional and personal devel-opment, improvement on students’ preparednessfor career planning, development of nursingprofession and the teacher’s and preceptor’s pro-fessional development were identified (Fig. 1).Clinical supervision influences students’ notionsof nursing and their motivation towards it. Duringthe nursing studies, the foundations for views onnursing profession are laid, and successful super-vision creates a favourable impression of the en-tire profession. It strengthens the development ofprofessional identity and supports the socialisa-tion process of the profession. Similarly, clinicalsupervision advances positive attitudes towardsprofessional development and assists in the real-isation of the need for lifelong learning. Clinicalsupervision contributes to the recognition of theessential elements of nursing and nursing environ-ment. Finally, it promotes the development ofself-evaluation and presents ideas how to developit.
Clinical supervision is an effective method ofrecruiting personnel. It increases students’ satis-faction and their wish to return to the ward aftertheir graduation. Also, clinical supervision influ-ences the choice regarding the student’s field ofnursing or a specific ward in the future. Therefore,it influences permanence and engagement ofnurses in their profession. Successful supervisionboosts a positive public image of the clinical prac-tice placement.
390 A. Haggman-Laitila et al.
Discussion
Examining the model and its significance tohealth care settings and nursing education
Clinical supervision can be examined as an entitywith the developed model. The model enhancesthe understanding of health care organisationsand nursing education of clinical supervision andclarifies the supervision process and its control.The model may be utilised in selecting and educat-ing preceptors, evaluating the quality of clinicalsupervision and its implementation as well as indevelopment areas of various health care settings.Similarly, it may be employed in self and peer eval-uation and personal development plans. With theaid of the model, the roles of teachers, studentsand preceptors may be explored in the supervisionprocess. The successful implementation of themodel requires full commitment of the managersand employees in both health care organisationsand polytechnics.
Whilst the study was limited only to three largeorganisations in Finland and the number of studysubjects was low, the international utility of thisresearch lies on the concepts produced. It concep-tualises a subject area that has been scarcelyexamined (Aston and Molassiotis, 2003; Vuorinenet al., 2005; Cleary et al., 2006). Therefore, theconstructed concepts may be utilised in the identi-fication of the development needs of students’clinical supervision and its systematic develop-ment. Moreover, they may be utilised in furtherstudies of the subject area.
According to the model for clinical supervisionin this study, clinical practice requires multi-fac-eted skills of the preceptors. Although clinicalsupervision requires widespread skills, many ofthe skills stated in the prerequisites are part of apreceptor’s basic work and their good commandcreates the prerequisites of successful clinicalsupervision. The actual pedagogical skills are morerelated to teaching skills, and these may be rein-forced by education and cooperation with teach-ers. Earlier studies have shown that educationdeepens the preceptors’ pedagogical competenceand clarifies their role (Watson, 1999; Duffyet al., 2000; Yonge et al., 2002; Koh, 2002). Forthis reason, health organisations should in factplan a systematic clinical supervision educationto all preceptors jointly with polytechnics. Fur-thermore, launching development projects be-tween organisations would also increase thedevelopment skills of preceptors. As for prerequi-sites of clinical supervision, Usher et al. (1999)
have introduced novel and transformed coopera-tion that enables receiving support, creation ofgood supervision practices and handling of prob-lematic situations.
The content of clinical supervision described inthe model is wider than in average clinical prac-tice supervision (cf. Gray and Smith, 2000; Sueand Chow, 2001; Ohrling and Hallberg, 2001),and they indicate the demanding requirementsof the task. At its best, extensive clinical supervi-sion enables the improvement of quality, effec-tiveness and results both in nursing and nursingeducation. Research and development activitiesrequiring novel competence in clinical supervisionpose considerable challenges on both nursing andnursing education and demand full cooperationand right attitude. For their part, systematic edu-cation and clinical supervision guarantee the suc-cess of novel modes of operation. The contentof clinical supervision presented in the modelmay form the content of pedagogical educationas such.
As for the third core concept of the model, theinfluence of clinical supervision is of vital impor-tance when developing the content of clinicalpractice to match the required learning outcomes.The findings of this study support earlier studiesregarding the influence of clinical supervision.Clinical supervision influences the student’s learn-ing and career planning. In particular, it seems toaffect professional development, concretisation ofnursing environment and learning of nursingknowledge and skills. Moreover, it promotes thewell-being of students and enables peer support(Aston and Molassiotis, 2003; Koh, 2002; Vuorinenet al., 2005). The influence of clinical practiceand its supervision on the student have beenrecognised more clearly than the preceptor’slearning (Vuorinen et al., 2005). By identifyingthe multi-faceted influence of clinical supervision,it is possible to try to influence the content ofclinical supervision and the optimum selection cri-teria for the preceptors on a more focused mannerthan previously. In addition to nursing skills, thiswould include a positive attitude towards clinicalsupervision.
Conclusions and suggestions for furtherstudy
1. The model developed in this study may be usedto unify the notions of the parties concernedof the prerequisites, content and influence ofclinical supervision and to clarify the supervisionprocess and its control.

Nursing students in clinical practice – Developing a model for clinical supervision 391
2. The introduction of the model and its furtherdevelopment require preceptors’ systematiceducation and strong commitment of healthcare organisations and nursing education.
3. This study was a small-scale pilot study to definethe concepts of supervision. It produced descrip-tive information of the existing reality and couldnot show new correlations between the con-cepts. A general and well-constructed theory isbased on hypotheses, and therefore the modelrequires further development and testing withlarge data in various settings for these parts.
4. The findings of this research may be used forexamining the interrelation and structure ofthe concepts of the model with more demandingapproaches, such as correlative or experimentalstudy design.
5. The quality of clinical supervision should beexamined and followed systematically as part ofthe quality of learning in nurses’ basic education.
6. In the future, research should be directed morevigorously on the influence of clinical supervi-sion and to developing proficient supervisionand learning practices by means of action orintervention research, to mention a few.
References
Andrews, M., Wallis, M., 1999. Mentorship in nursing: a litera-ture review. Journal of Advanced Nursing 29, 201–207.
Aston, L., Molassiotis, A., 2003. Supervising and supportingstudent nurses in clinical placements: the peer supportinitiative. Nurse Education Today 23 (3), 202–210.
Brazier, H., Begley, C.M., 1996. Selecting database for literaturesearches in nursing: MEDLINE or CHINAL? Journal of AdvancedNursing 24 868–875.
Burns, N., Grove, S., 2005. The Practice of Nursing Research.Conduct, Critique, and Utilization, fifth ed. Elsevier Saun-ders, USA.
Cleary, M., Horsfall, J., De Carlo, P., 2006. Improving studentlearning in mental health settings: the views of clinicalstakeholders. Nurse Education in Practice 6, 141–148.
Duffy, K., Docherty, C., Cardnuff, L., White, M., Winters, G.,Greig, J., 2000. The nurse lecturer’s role in mentoring thementors. Nursing Standard 15, 25–31.
Evans, D., 2002. Database searches for qualitative research.Journal of the Medical Library Association 90, 290–293.
Evans, D., Pearson, A., 2001. Systematic reviews: gatekeepers ofnursing knowledge. Journal of Clinical Nursing 10, 593–599.
Graneheim, F., Lundman, B., 2004. Qualitative content analysisin nursing research: concepts, procedures and measures to
achieve trustworthiness. Nurse Education Today 24 (2), 105–112.
Gray, M., Smith, L., 2000. The qualities of an effective mentorfrom the student nurse’s perspective: findings from alongitudinal qualitative study. Journal of Advanced Nursing32, 1542–1549.
Koh, L.C., 2002. The perceptions of nursing students of practice-based teaching. Nurse Education in Practice 2 (1), 35–43.
Lofmark, A., Wikblad, K., 2001. Facilitating and obstructingfactors for development of learning in clinical practice: astudent perspective. Journal of Advanced Nursing 34, 43–50.
McLafferty, I., 2004. Focus group interviews as data collectingstrategy. Journal of Advanced Nursing 48 (2), 187–194.
Neary, M., 1997. Defining the role of assessors, mentors andsupervisors: part 2. Nursing Standard 11, 34–38.
O’Donovan, M., 2006. Reflecting during clinical placement –discovering factors that influence pre-registration psychiat-ric nursing students. Nurse Education in Practice 6, 134–140.
Ohrling, K., Hallberg, I., 2001. The meaning of preceptorship:nurses’ lived experience of being a preceptor. Journal ofAdvanced Nursing 33, 530–540.
Pulsford, D., Owen, S., 2002. Are mentors ready to make adifference? A survey of mentors’ attitudes toward nurseeducation. Nurse Education Today 22, 439–446.
Saarikoski, M., 2002. Clinical leaning environment and supervi-sion. Development and validation of the CLES evaluationscale, Turun yliopiston julkaisuja Sarja C osa 178, Depart-ment of Nursing Science, Turku.
Sue, L., Chow, F., 2001. Students’ perceptions of the effective-ness of mentors in an undergraduate nursing programme inHong Kong. Journal of Advanced Nursing 36, 505–511.
Usher, K., Nolan, C., Reser, P., Owens, J., Toffelson, J.,1999. An exploration of the preceptor role: preceptors’perceptions of benefits, rewards, supports and commitmentto the preceptors role. Journal of Advanced Nursing 29,506–514.
Vuorinen, R., Meretoja, R., Eriksson, E., 2005. Hoitotyonohjatun harjoittelun sisalto, edellytykset ja vaikutukset –systemoitu kirjallisuuskatsaus. Hoitotiede 17 (5), 270–281.
Watson, N., 1999. Mentoring today – the students’ views. AnInvestigative case study of pre-registration nursing students’experiences and perceptions of mentoring in one theory/practice module of the Common Foundation Programme on aProject 2000 course. Journal of Advanced Nursing 29, 254–262.
Webb, C., Kevern, J., 2001. Focus groups as a research method:a critique of some aspect of their use in nursing research.Journal of Advanced Nursing 33 (6), 798–805.
Wilhelmsson, S., Foldevi, M., 2003. Exploring views on Swedishdistrict nurses’ prescribing – a focus group study in primaryhealth care. Journal of Clinical Nursing 12, 643–650.
Woods, L., Priest, H., Roberts, P., 2002. An overview of threedifferent approaches to the interpretation of qualitative data.Part 2: practical illustrations. Nurse Researcher 10, 43–51.
Yonge, O., Krahn, H., Trojan, L., Reid, D., Haase, M., 2002.Supporting preceptors. Journal for Nurses in Staff Develop-ment 18, 73–77.





























