Embed Size (px)
Citation preview
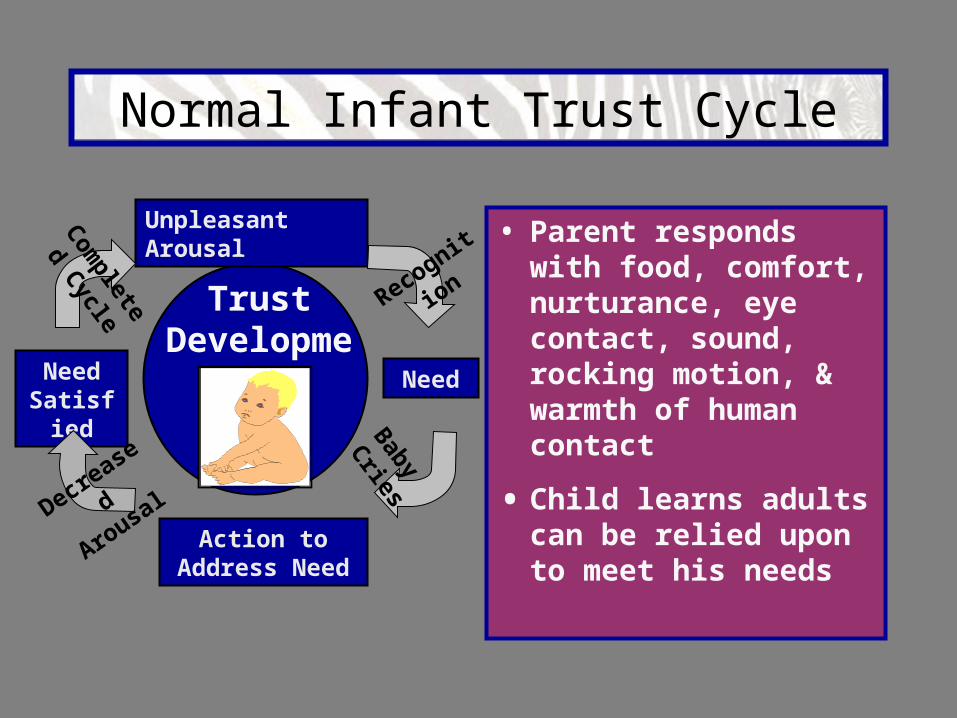
Normal Infant Trust Cycle
• Parent responds with food, comfort, nurturance, eye contact, sound, rocking motion, & warmth of human contact
• Child learns adults can be relied upon to meet his needs
Trust Development
Unpleasant Arousal
Need Satisfied
Need
Action to Address Need
Recognitio
n
Com
pleted
Cycle
Decreased
Arousal
Baby Cries
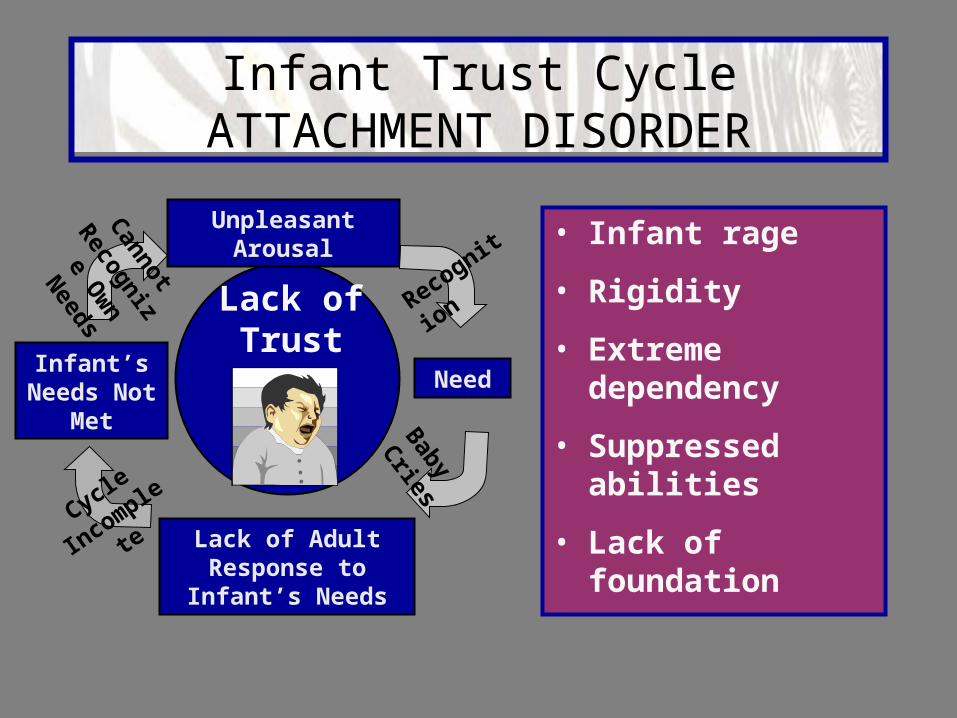
Infant Trust Cycle ATTACHMENT DISORDER
• Infant rage
• Rigidity
• Extreme dependency
• Suppressed abilities
• Lack of foundation
Lack of Trust
Unpleasant Arousal
Infant’s Needs Not
Met
Need
Lack of Adult Response to Infant’s
Needs
Recognitio
n
Cannot
Recognize
Ow
n Needs
Cycle
Incomplete
Baby Cries

Early Childhood Trust of Limits Cycle
• Unpleasant Arousal is Continuous
• Needs = Control
• Action— “I must take care of this myself”
• Limits = Obstacle
• Reinforced Arousal—“ I knew I had to do this myself”
No Trust of Limits-
Attachment Disorder
Unpleasant Arousal
Reinforced Arousal
Need
Placement of Limits
Action to Meet Need
Needs Never Totally Met

Dynamics of Attachment Disorder
Attachment Figure Unavailable
Negative Response Cycle
Self Protective Distancing
Loss of Caregivers
Unmet Needs
Lack of Pleasure in Relationships

Traumatic Stress Leading to Attachment Disorder
• Denial of pregnancy
• Dislike for father of child
• Substance abuse
• Prematurity risk factors
• Variable family support
• Inadequate diet; poor self-care
• Resentment
Pre-Natal
Factors

Traumatic Stress Leading to Attachment Disorder
• Lack of parenting skills
• Various caregivers
• Ongoing substance abuse
• “Mechanical parenting”
• Neglectful/Abusive parental reactions
• Prematurity factors
• Undetected/Unrelieved pain in the child
Post-Natal
Factors
Behavioral Checklist
• Indiscriminate affection towards strangers, willingness to go with them
• Face to face compliance with passive-aggressive resistance
• Absence of guilt; no remorse; lack of conscience development
• Provoking of anger in others almost continually
• Lack of ability to give and receive affection unless on their terms
Behavioral Checklist
• Chronic, non-sensical lying - “crazy lying”
• Theatrical displays of emotion
• Stealing or hoarding food; food refusal or gorging
• Cruelty to animals and/or children, especially younger children
• Firesetting - “controlled” fires
• Preoccupation with blood, fire, gore
Behavioral Checklist• Lack of cause & effect thinking - does not learn from consequences
• Poor eye contact
• Denial of accountability
• Self-injurious behavior
• Refusal to answer simple questions
• Unusual speech patterns or problems
• Poor peer relationships
• Learning disorders
• Theft, vandalism & destructiveness
• Seductive behavior or clothing
• Toileting issues
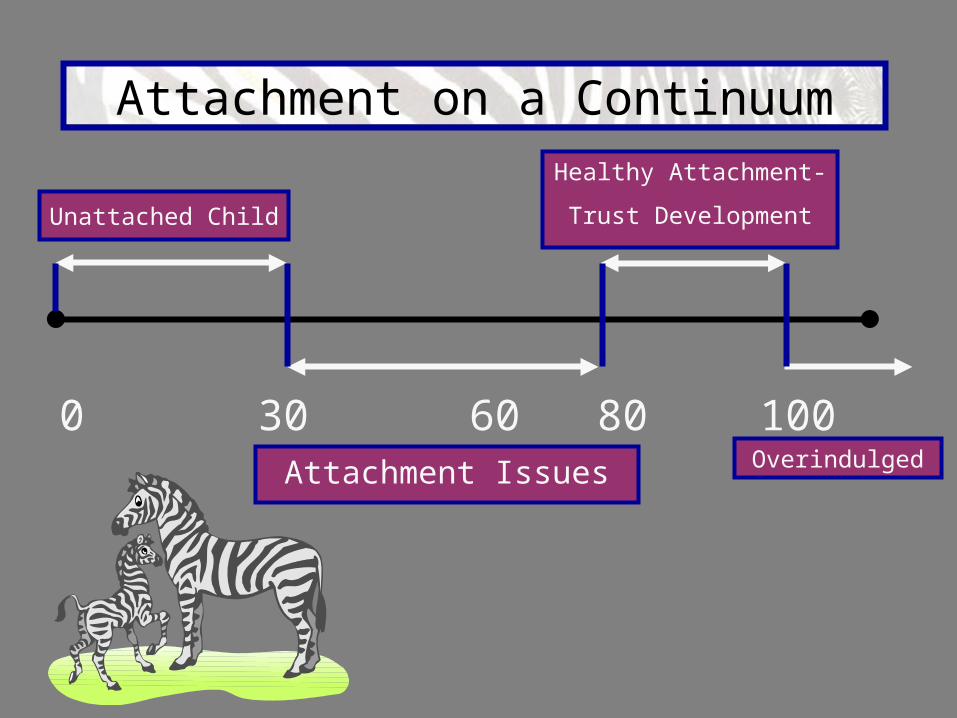
Attachment on a Continuum
0 60 10030 80Attachment Issues Overindulged
Unattached Child
Healthy Attachment-
Trust Development

Emotional Makeup of Attachment Disorder
Hopelessness Loss
Abandonment
Helplessness No Trust
Anger
PROFOUND SADNESS
FearRage

Parenting a Child With RAD

Post Traumatic Stress Disorder In Parents
Repeated rejection by child—no reciprocity
Personal and family changes out of
control
Avoidance of thoughts and feelings
Decreased affect—detachment from
others
Psychological and physical distress
Relentless control battles—constant
self-control
Primary Symptoms
Causes
Secondary Symptoms
Sleep problems; hypervigilant, irritable, angry
Victim identity; fatigue and
depression; loss of security
Feeling unlike others; emotions
out of control
Hopelessness
Helplessness
ANGER
RAGE

Adult Characteristics for Successful Parenting of Children With RAD
• Healthy sense of humor• Consistency with behavior management, yet flexible• Ability to handle interruptions to social schedules• Understanding that one parents a needy child, with parent’s personal needs met elsewhere• Ability to advocate for child in a
positive manner• Ability to promote positive growth• Sense of hope for the future, plus tolerance and perseverance

• Support in the marital relationship; communication and belief in what the other spouse says• Ability to react calmly; ability to display parental control of attitudes and abilities in the presence of the child• Ability to accept appropriate confrontation if it promotes positive changes• Ability to constantly redefine parental goals and expectations for the child; able to redefine “success”• Ability to withstand criticism & condemnation from family, friends and community
Adult Characteristics for Successful Parenting of Children With RAD

ATTACHMENT DISORDERParental Response Cycle
• The cycle is solely dependent on adult reactions
• Child’s response is directly relevant to degree of adult’s commitment & amount of consistency in terms of non-abusive or rejecting reactions
Building Trust
Capabilities
Unpleasant Arousal
CONFUSION Need
RAGE
Consisten
t
Inconsisten
cy
CO
MM
ITMEN
T
NON ABUSIV
E
Support
Response
Supportive
Control

Child’s View of Adult-Child Interactions
• Someone wins; Someone loses• Adult doesn’t take charge when child is out of control• Child senses this and becomes frightened• Child continues to set up opportunities for adult to take charge• When adult is unwilling or unable to take control, child’s out of control behavior escalates

Adult Attachment Disorder Progression
Unstable and
ImpulsiveSelf
Absorbed
Emotional and
Attention Seeking
Disregard for Others
BORDERLINE PERSONALITY
DISORDER
ANTISOCIAL PERSONALITY
DISORDER
HISTRIONIC PERSONALITY
DISORDER
NARCISSITIC PERSONALITY
DISORDER

The Child Welfare SYSTEM
State Child Welfare
Agencies
Local Child Welfare
Agencies
Private Service
Providers
Courts
Medicaid
Public Agencies
Welfare, Public
Assistance
Substance Abuse
Treatment
Mental Health
Counseling

Foster Care Statistics 2001
• 3 Million referrals made to CPS• 900,000 children found to be victims of maltreatment• 290,000 entered the foster care system• 800,000 children spent some time in the foster care system• 540,000 children in foster care at any given time*
*The Future of Children Winter 2004 www.futureofchildren.org
Foster Care Statistics 2001
*The Future of Children Winter 2004 www.futureofchildren.org
• Nearly one-third of maltreated children were under the age of 3• Forty percent of all child fatalities due to child abuse were infants under age 1• Over the past 10 years, the number of infants and toddlers coming into foster care has increased by 110%• Approximately 1 in 5 of the children entering foster care for the first time are infants under age 1*

Is Uncle Sam a Good Parent?
When the state assumes custody of a child, in
effect the government is stating that it can do a better job of protecting and providing for this child than his or her birth parents can.*
*The Future of Children Winter 2004 www.futureofchildren.org

Assessing the Degree of Attachment Damage
*The Future of Children Winter 2004 www.futureofchildren.org
To uphold the government’s responsibility to children in
foster care, addressing children’s needs must begin at
entry with initial health screening and continue with
regular assessments throughout a child’s time in
care.*

Pay Now or Pay Later
*Juvenile Offenders With Mental Health Disorders
Who Are They and What Do We Do With Them? By Lisa Melanie Boesky, Ph.D.
There is clear evidence that a significant
number of youth in the juvenile justice system
are suffering from serious emotional and behavioral disorders.*
Diathesis-Stress Model of Illness
*Hakim-Larson & Essau, 1999, Juvenile Offenders With Mental Health Disorders… Who Are They and What Do We Do With Them?
By Lisa Melanie Boesky, Ph.D.
“Diathesis” = Being vulnerable to, or having a predisposition to, develop a particular disorder. Psychopathology is thought to result when a diathesis interacts with stressful life events, unless there are ample protective factors or resources to offset it.*

Diathesis-Stress Model of Illness
Juvenile Offenders With Mental Health Disorders… Who Are They and What Do We Do With Them? By Lisa Melanie Boesky, Ph.D.
Mental health disorders are likely the result of a combination of juveniles’ :• Inherited biological or psychological vulnerabilities• Environmental stressors• Environmental supports• Particular abilities and coping skills
Post Traumatic Stress Disorder
Juvenile Offenders With Mental Health Disorders… Who Are They and What Do We Do With Them? By Lisa Melanie Boesky, Ph.D.
Biological influences = MR or ADHD
Environmental influences may be more
significant for youth suffering from Post-
traumatic Stress Disorder.