Embed Size (px)
Citation preview
1
Normal and Abnormal Skeletal Metabolism;
Pathophysiology of Osteoporosis
Mishaela R. Rubin, MD
The Three Ages of Women
Gustav Klimt 1905
2
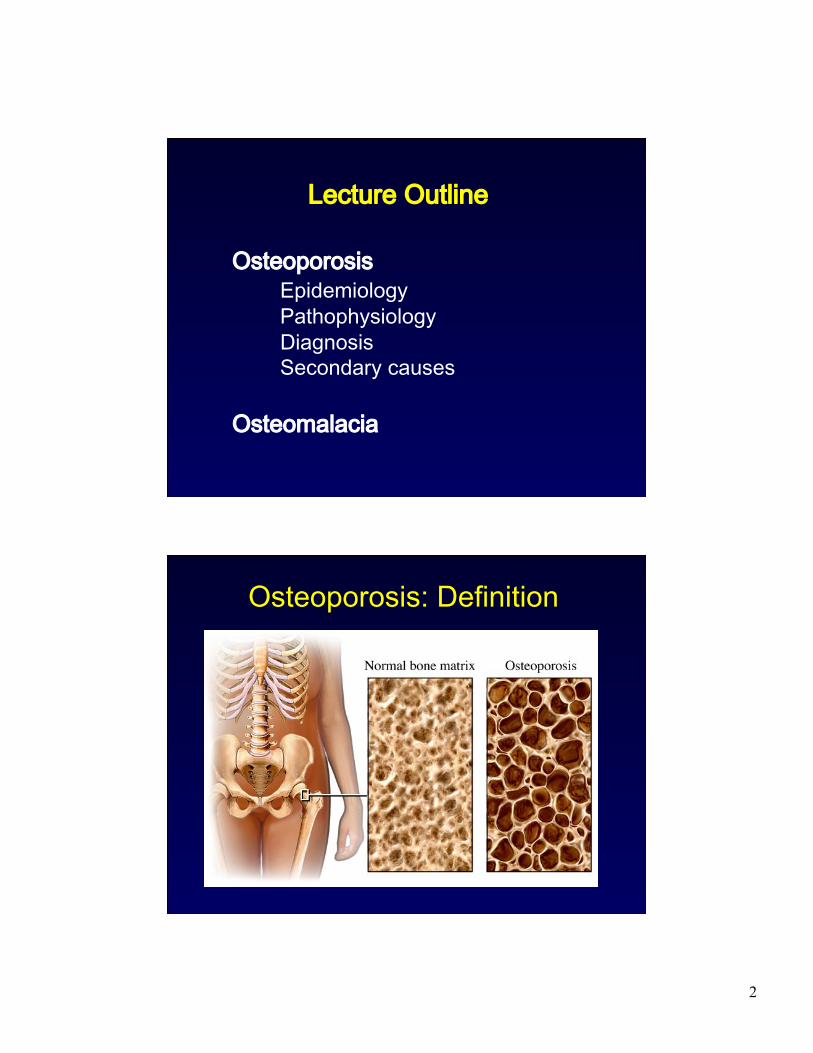
Osteoporosis Epidemiology Pathophysiology Diagnosis Secondary causes
Osteomalacia
Lecture Outline
Osteoporosis: Definition
3
Osteoporosis Epidemiology Pathophysiology Diagnosis Secondary causes
Osteomalacia
Lecture Outline
Osteoporosis: Prevalence and Epidemiology
• Osteoporosis • 8 million women and 2 million men
• Low bone mass • Additional 34 million
• Fractures • Approximately ½ of women and ¼ of men > 50 yrs will suffer an osteoporosis-related fracture in their lifetime
4
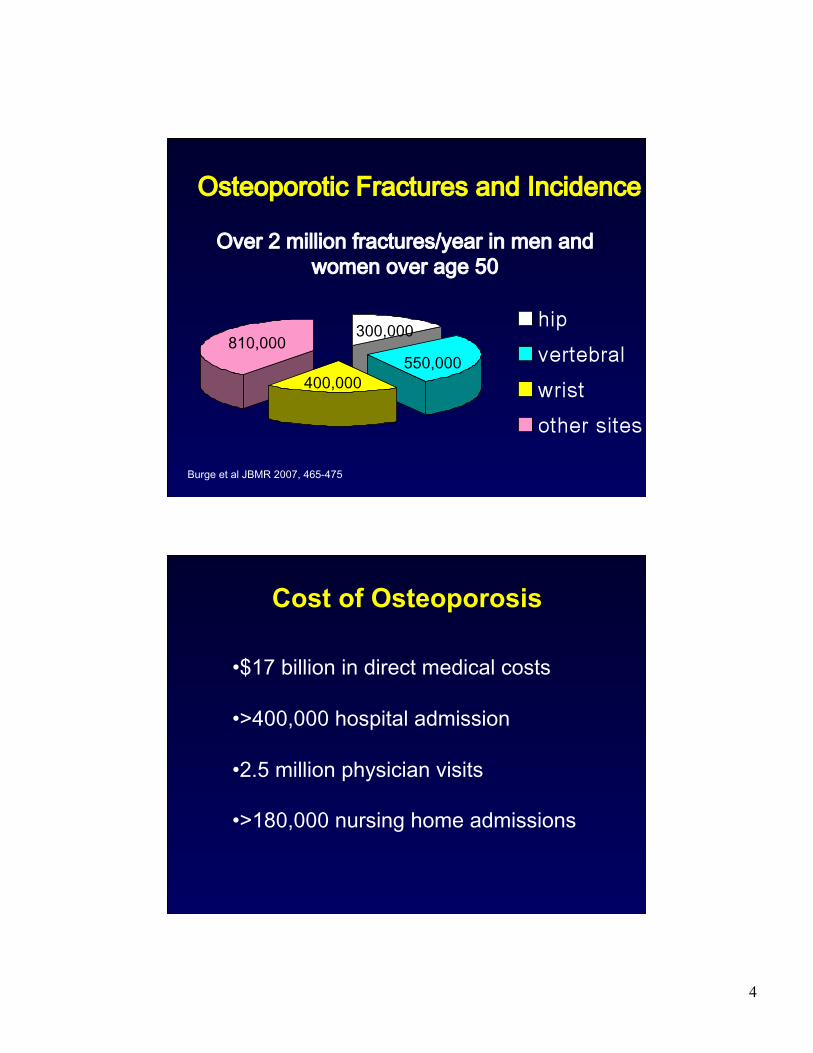
300,000
550,000 400,000
810,000
Burge et al JBMR 2007, 465-475
Osteoporotic Fractures and Incidence
Over 2 million fractures/year in men and women over age 50
Cost of Osteoporosis
• $17 billion in direct medical costs
• >400,000 hospital admission
• 2.5 million physician visits
• >180,000 nursing home admissions
5
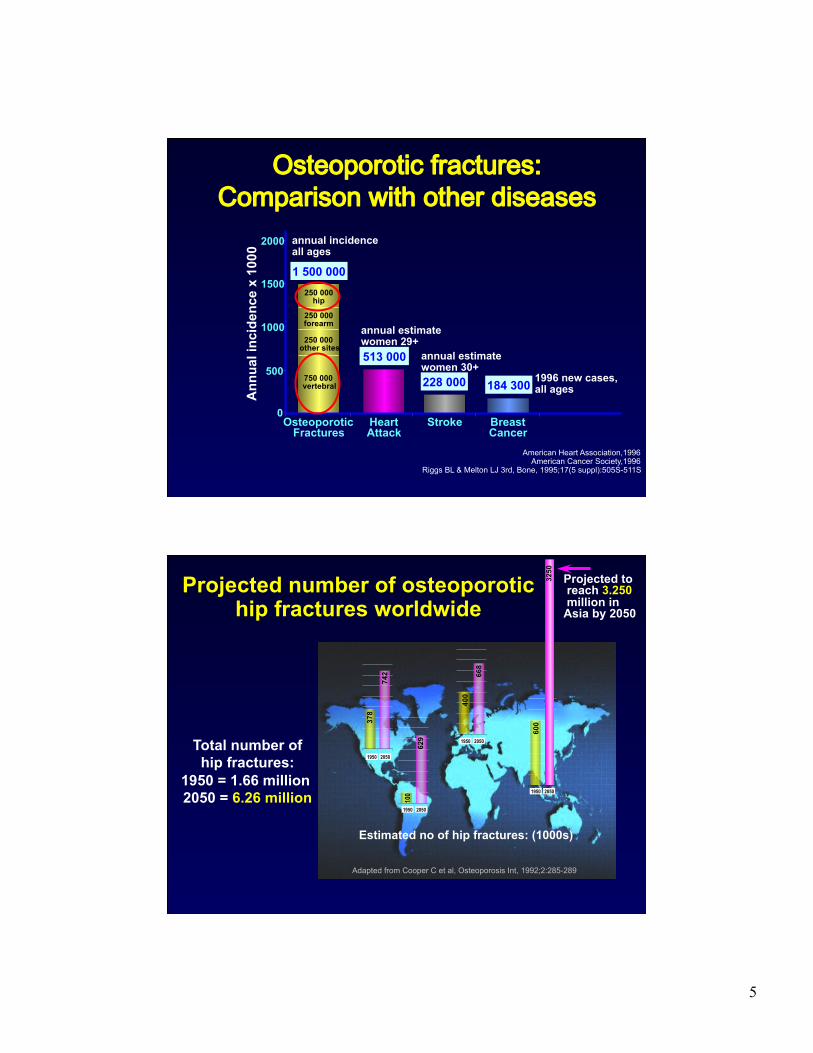
Osteoporotic fractures:Comparison with other diseases
1996 new cases, all ages 184 300 750 000
vertebral
250 000 other sites
250 000 forearm
500
1000
1500
2000
Osteoporotic Fractures
Heart Attack
Stroke Breast Cancer
Ann
ual i
ncid
ence
x 1
000
1 500 000
annual incidence all ages
513 000
annual estimate women 29+
228 000
annual estimate women 30+
American Heart Association,1996 American Cancer Society,1996
Riggs BL & Melton LJ 3rd, Bone, 1995;17(5 suppl):505S-511S
Projected number of osteoporotic hip fractures worldwide
Projected to reach 3.250 million in Asia by 2050
Adapted from Cooper C et al, Osteoporosis Int, 1992;2:285-289
Estimated no of hip fractures: (1000s)
1950 2050
600
3250
1950 2050
668
400
1950 2050
742
378
1950 2050
100
629 Total number of
hip fractures: 1950 = 1.66 million 2050 = 6.26 million
6
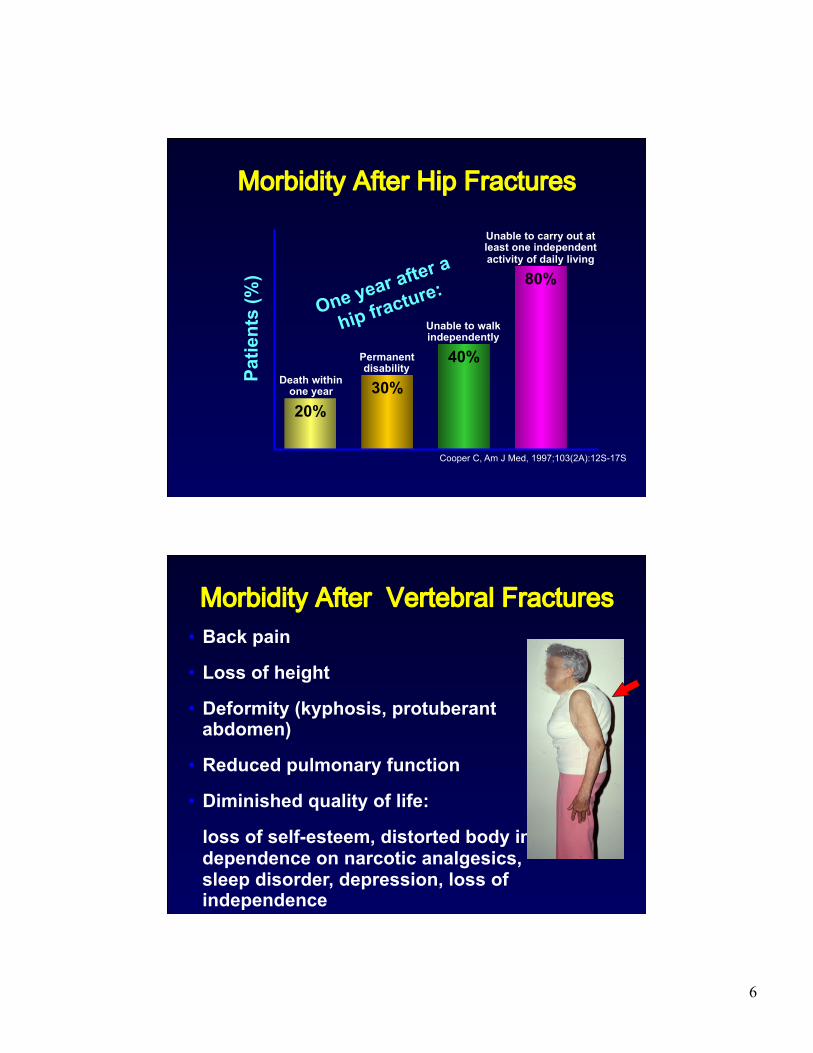
Morbidity After Hip Fractures
Cooper C, Am J Med, 1997;103(2A):12S-17S
40%
Unable to walk independently
30%
Permanent disability
20%
Death within one year
80%
One year after a
hip fracture:
Patie
nts
(%)
Unable to carry out at least one independent activity of daily living
Morbidity After Vertebral Fractures • Back pain
• Loss of height
• Deformity (kyphosis, protuberant abdomen)
• Reduced pulmonary function
• Diminished quality of life:
loss of self-esteem, distorted body image, dependence on narcotic analgesics, sleep disorder, depression, loss of independence
7
Osteoporosis Affects Men Also
women
men 10-12,000,000
23-32,000,000
National Osteoporosis Foundation, 2002
Osteoporosis Epidemiology Pathophysiology Diagnosis Secondary causes
Osteomalacia
Lecture Outline
8
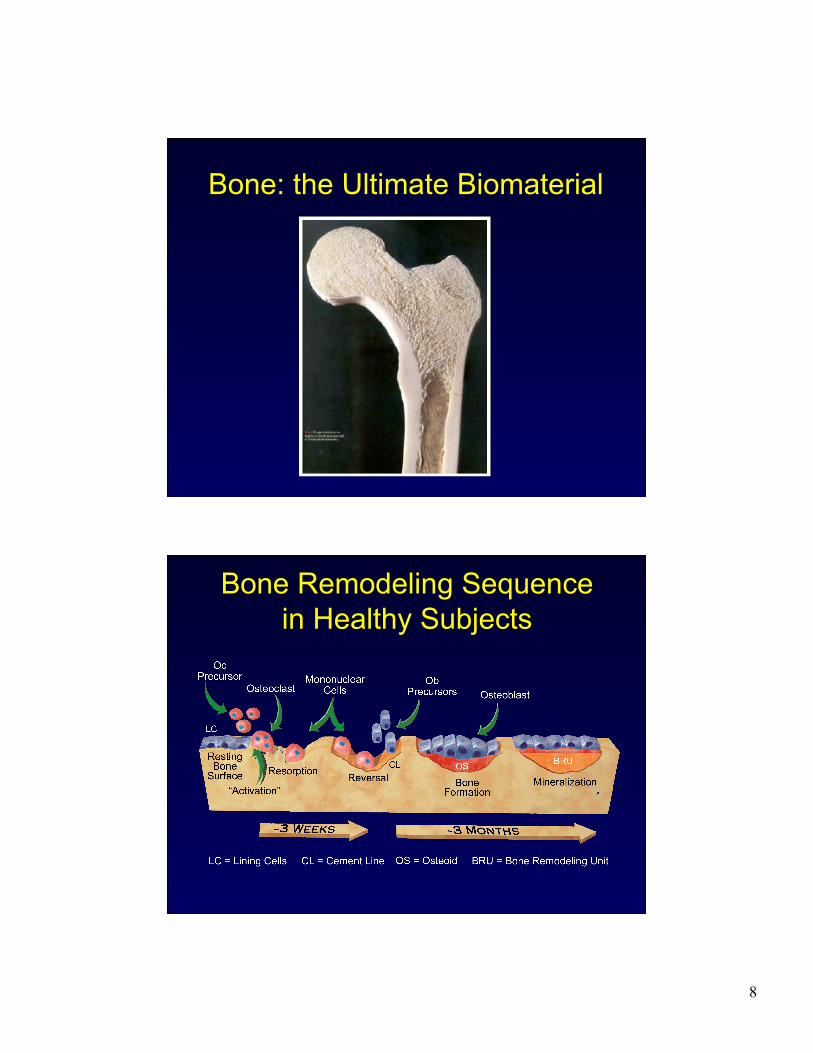
Bone: the Ultimate Biomaterial
9
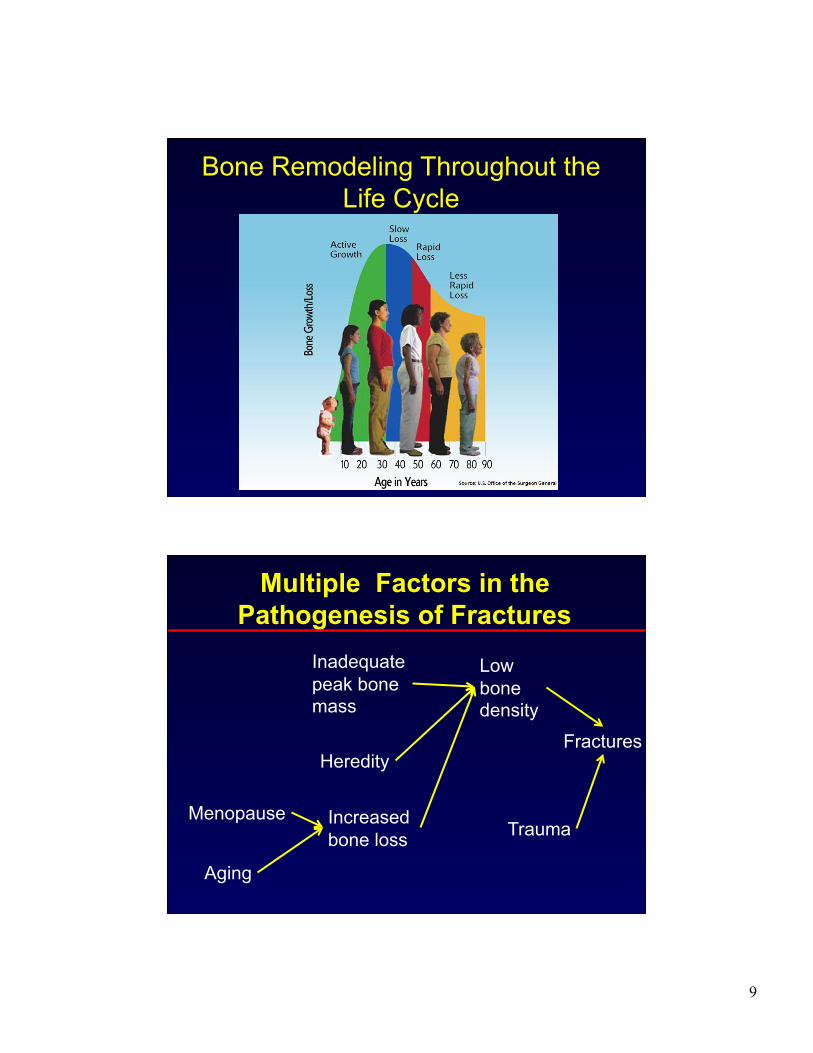
Bone Remodeling Throughout the Life Cycle
Multiple Factors in the Pathogenesis of Fractures
Menopause
Aging
Inadequate peak bone mass
Heredity
Increased bone loss
Low bone density
Trauma
Fractures
10
Osteoporosis Epidemiology Pathophysiology Diagnosis Secondary causes
Osteomalacia
Lecture Outline
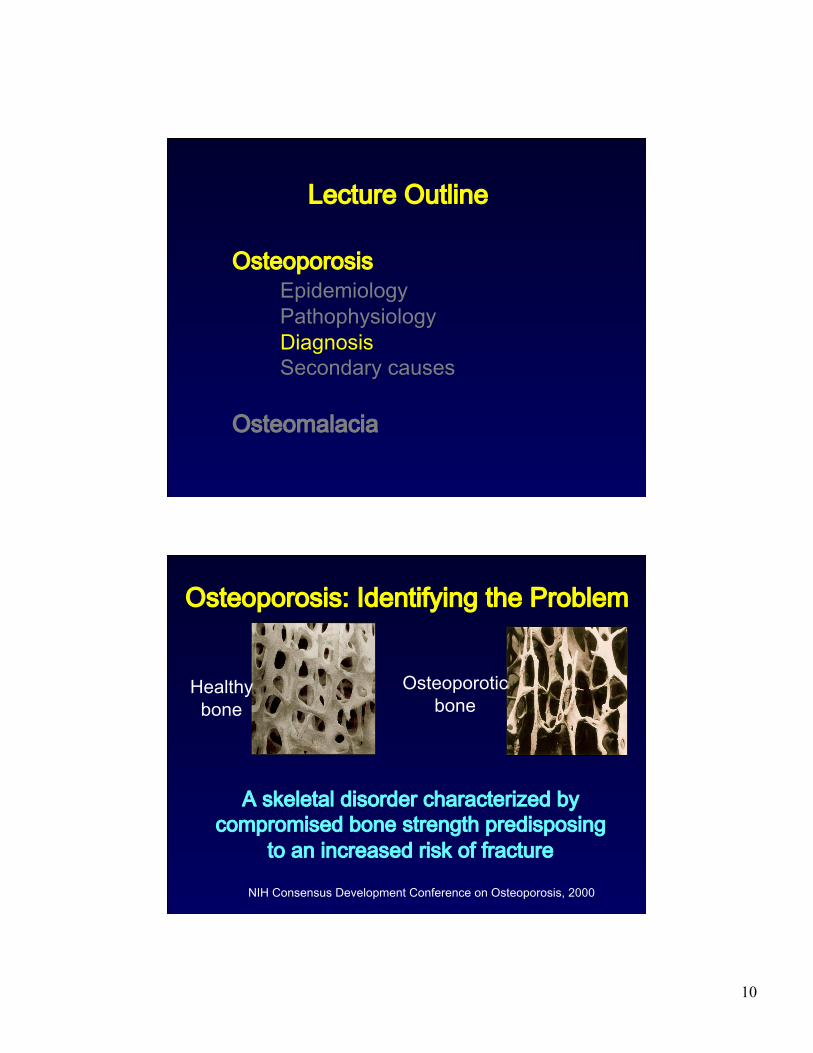
Osteoporosis: Identifying the Problem
Healthy bone
Osteoporotic bone
A skeletal disorder characterized by compromised bone strength predisposing
to an increased risk of fracture
NIH Consensus Development Conference on Osteoporosis, 2000
11
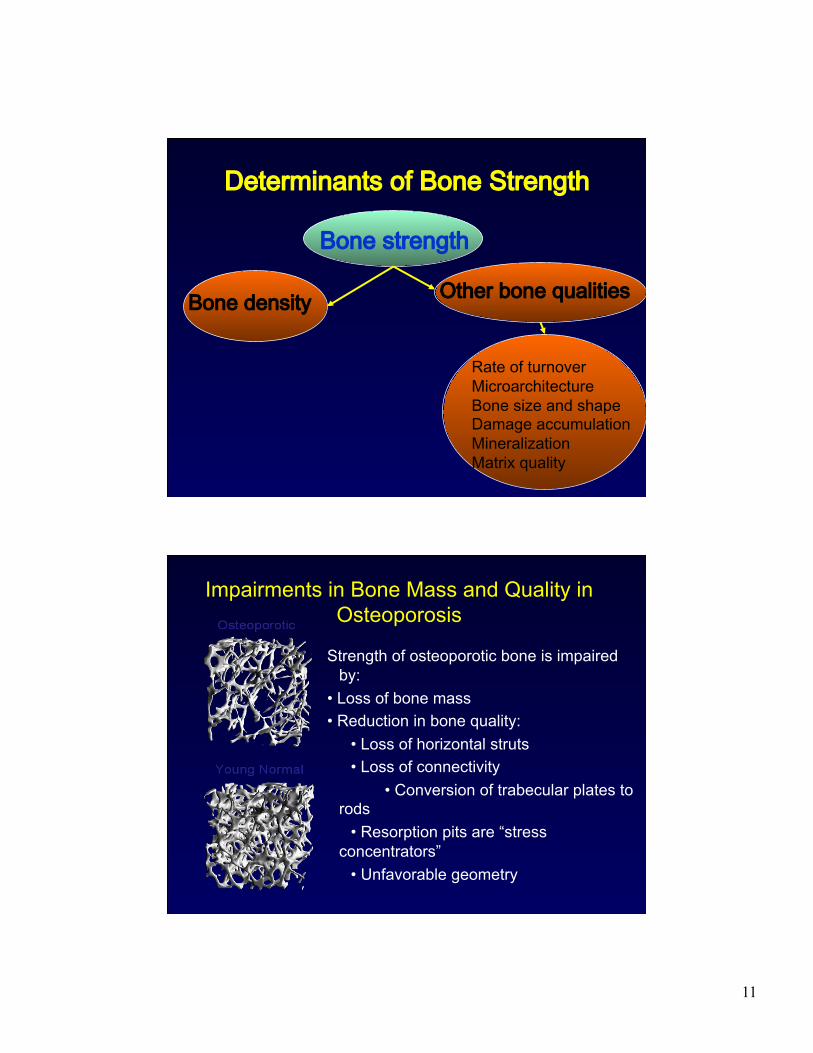
Determinants of Bone Strength
Bone strength
Bone density Other bone qualities
Rate of turnover Microarchitecture Bone size and shape Damage accumulation Mineralization Matrix quality
Strength of osteoporotic bone is impaired by:
• Loss of bone mass • Reduction in bone quality: • Loss of horizontal struts • Loss of connectivity • Conversion of trabecular plates to rods
• Resorption pits are “stress concentrators”
• Unfavorable geometry
Impairments in Bone Mass and Quality in Osteoporosis
12
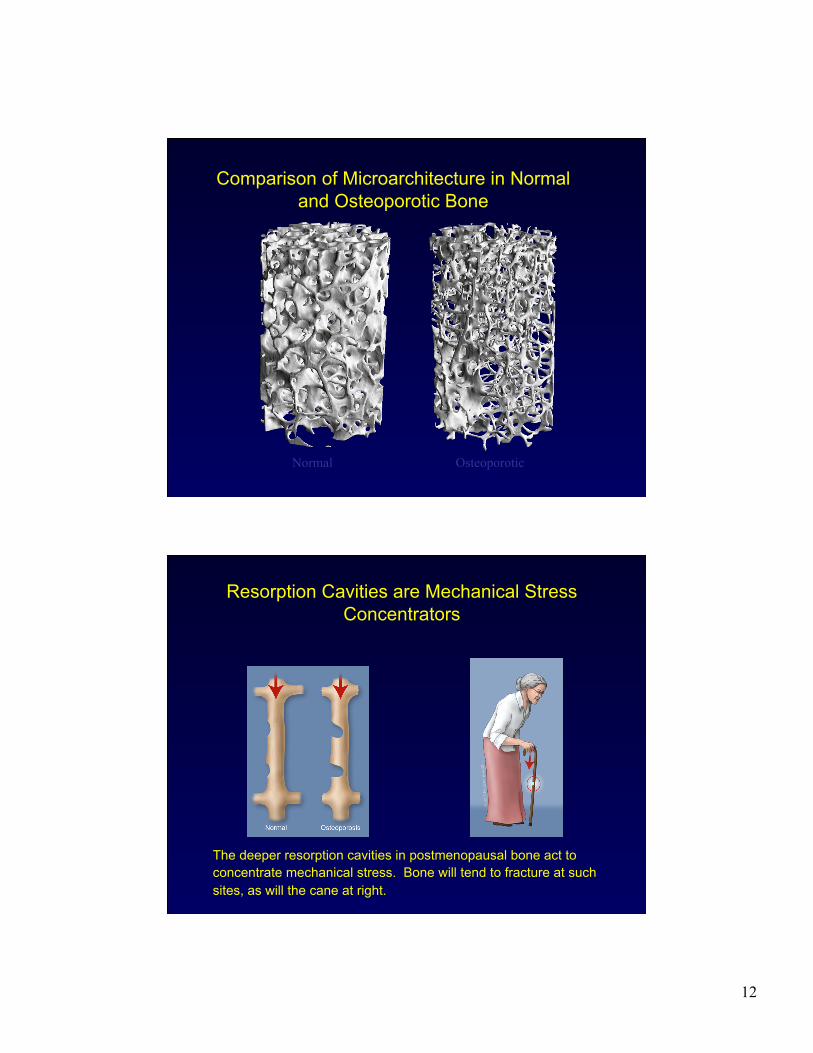
Normal Osteoporotic
Comparison of Microarchitecture in Normal and Osteoporotic Bone
Resorption Cavities are Mechanical Stress Concentrators
The deeper resorption cavities in postmenopausal bone act to concentrate mechanical stress. Bone will tend to fracture at such sites, as will the cane at right.
13
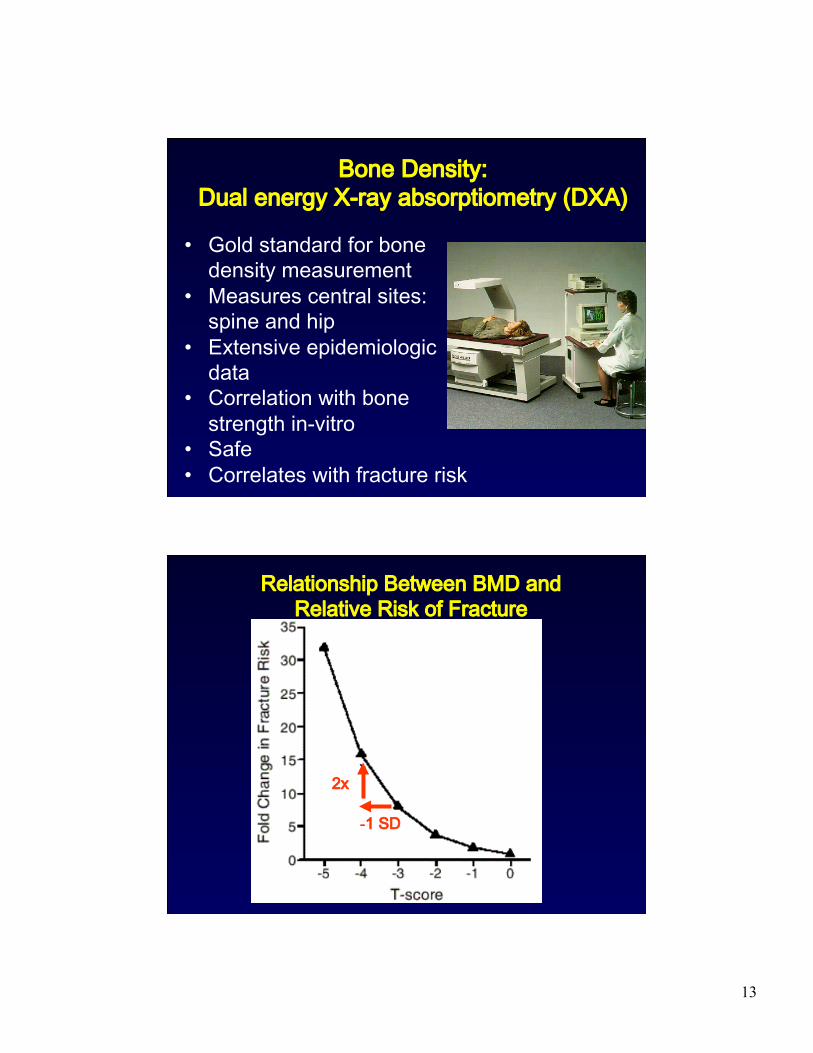
Bone Density: Dual energy X-ray absorptiometry (DXA)
• Gold standard for bone density measurement
• Measures central sites: spine and hip
• Extensive epidemiologic data
• Correlation with bone strength in-vitro
• Safe • Correlates with fracture risk
Relationship Between BMD and Relative Risk of Fracture
-1 SD
2x
14
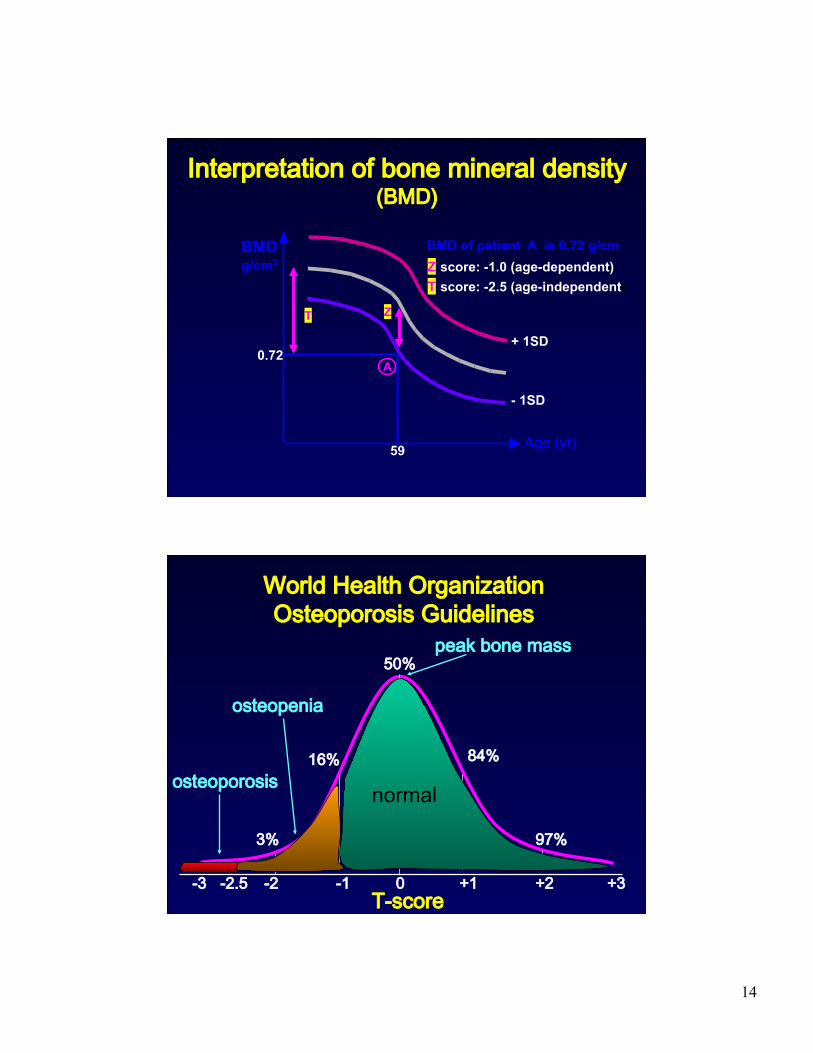
Interpretation of bone mineral density (BMD)
Z score: -1.0 (age-dependent) T score: -2.5 (age-independent)
BMD of patient A is 0.72 g/cm
0.72
T Z
+ 1SD
- 1SD
Age (yr)
A
BMD g/cm2
59
0 -3 +3 -2 -1 +1 +2
50%
3%
16% 84%
97%
peak bone mass
osteopenia
osteoporosis
-2.5
World Health Organization Osteoporosis Guidelines
T-score
normal

15
WHO Criteria for Osteoporosis in Women
Kanis JA et al, J Bone Miner Res, 1994;9:1137-1141
T-Score Normal -1 and above Low bone mass -1 to -2.5
Osteoporosis < -2.5 Established osteoporosis
< -2.5 and one or more fractures
Who Should Have a Bone Density Test: Screening Guidelines
• Women > 65 • Postmenopausal women with fragility fracture • Women and men on or starting steroids • Postmenopausal women <65 with risk factors:
weight <127 lbs early menopause smoking family history of fracture medical causes
16
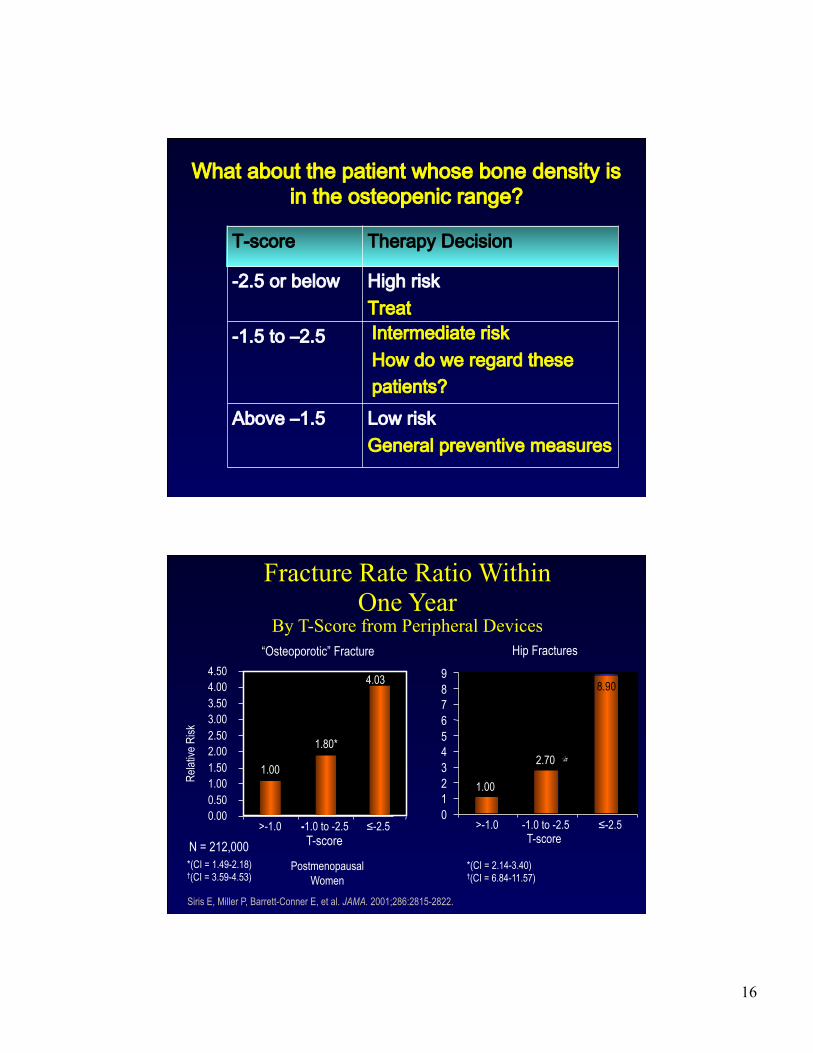
What about the patient whose bone density is in the osteopenic range?
T-score Therapy Decision
-2.5 or below High risk Treat
-1.5 to ‒2.5
Above ‒1.5 Low risk General preventive measures
Intermediate risk How do we regard these patients?
Hip Fractures
1.00
2.70
0 1 2 3 4 5 6 7 8 9
>-1.0 -1.0 to -2.5 ≤-2.5 T-score
“Osteoporotic” Fracture
0.00 0.50 1.00 1.50 2.00 2.50 3.00 3.50 4.00 4.50
>-1.0 -1.0 to -2.5 ≤-2.5 T-score
Relat
ive R
isk
Fracture Rate Ratio Within One Year
By T-Score from Peripheral Devices
Siris E, Miller P, Barrett-Conner E, et al. JAMA. 2001;286:2815-2822.
*(CI = 1.49-2.18) †(CI = 3.59-4.53)
*(CI = 2.14-3.40) †(CI = 6.84-11.57)
†
Postmenopausal Women
N = 212,000
1.80*
4.03 †
1.00
8.90
17
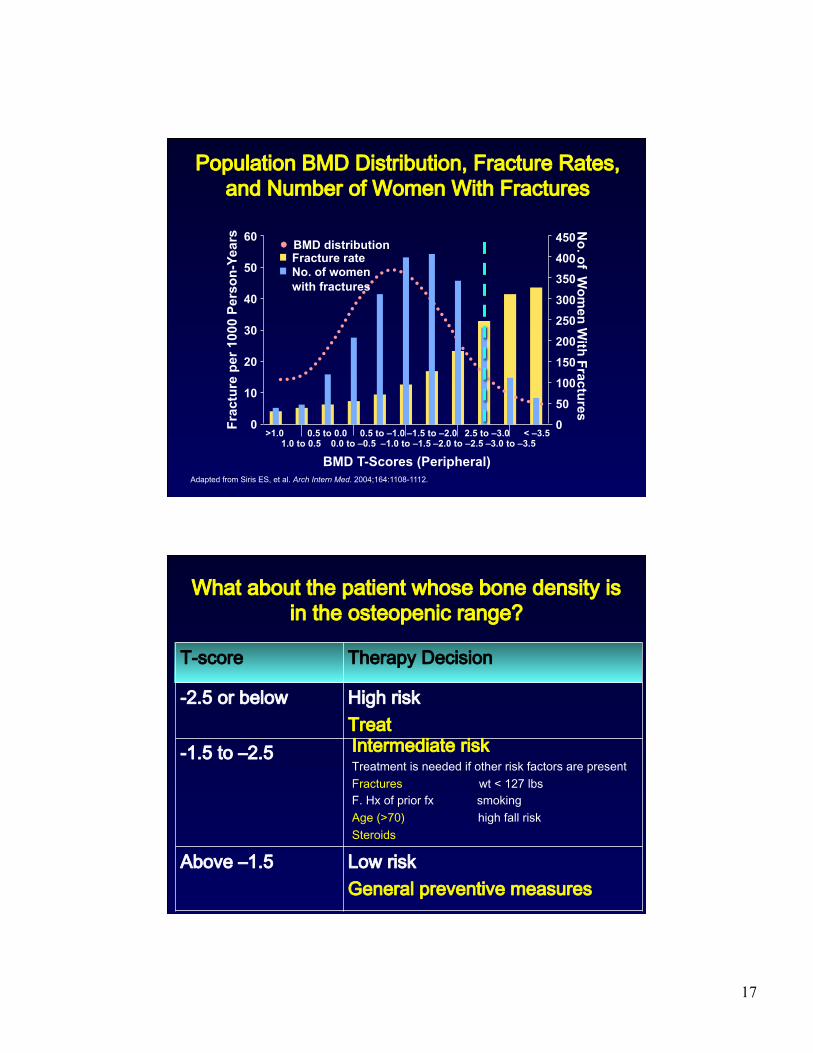
Adapted from Siris ES, et al. Arch Intern Med. 2004;164:1108-1112.
Population BMD Distribution, Fracture Rates, and Number of Women With Fractures
Fracture rate
60
50
40
30
20
10
0 Frac
ture
per
100
0 Pe
rson
-Yea
rs
BMD distribution
BMD T-Scores (Peripheral)
>1.0 1.0 to 0.5
0.5 to 0.0 0.0 to –0.5
–0.5 to –1.0 –1.0 to –1.5
–1.5 to –2.0 –2.0 to –2.5
–2.5 to –3.0 –3.0 to –3.5
< –3.5
No. of women with fractures
450
350
300 250
200
100
0
150
50
400
No. of W
omen W
ith Fractures
What about the patient whose bone density is in the osteopenic range?
T-score Therapy Decision
-2.5 or below High risk Treat
-1.5 to ‒2.5
Above ‒1.5 Low risk General preventive measures
Intermediate risk Treatment is needed if other risk factors are present Fractures wt < 127 lbs F. Hx of prior fx smoking Age (>70) high fall risk Steroids
18
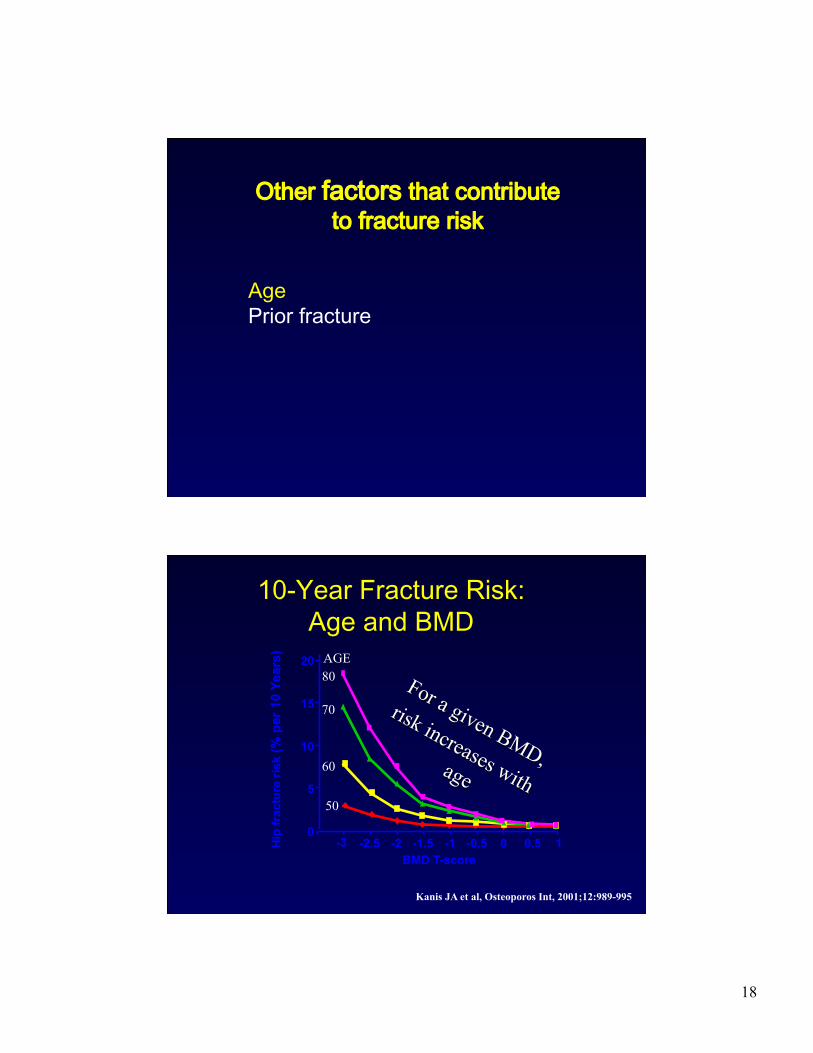
Other factors that contribute to fracture risk
Age Prior fracture
Hip
frac
ture
risk
(% p
er 1
0 Ye
ars)
-3
60
70
80 AGE
0
5
10
15
20
50
BMD T-score -2.5 -2 -1.5 -1 -0.5 0 0.5 1
10-Year Fracture Risk: Age and BMD
Kanis JA et al, Osteoporos Int, 2001;12:989-995
19
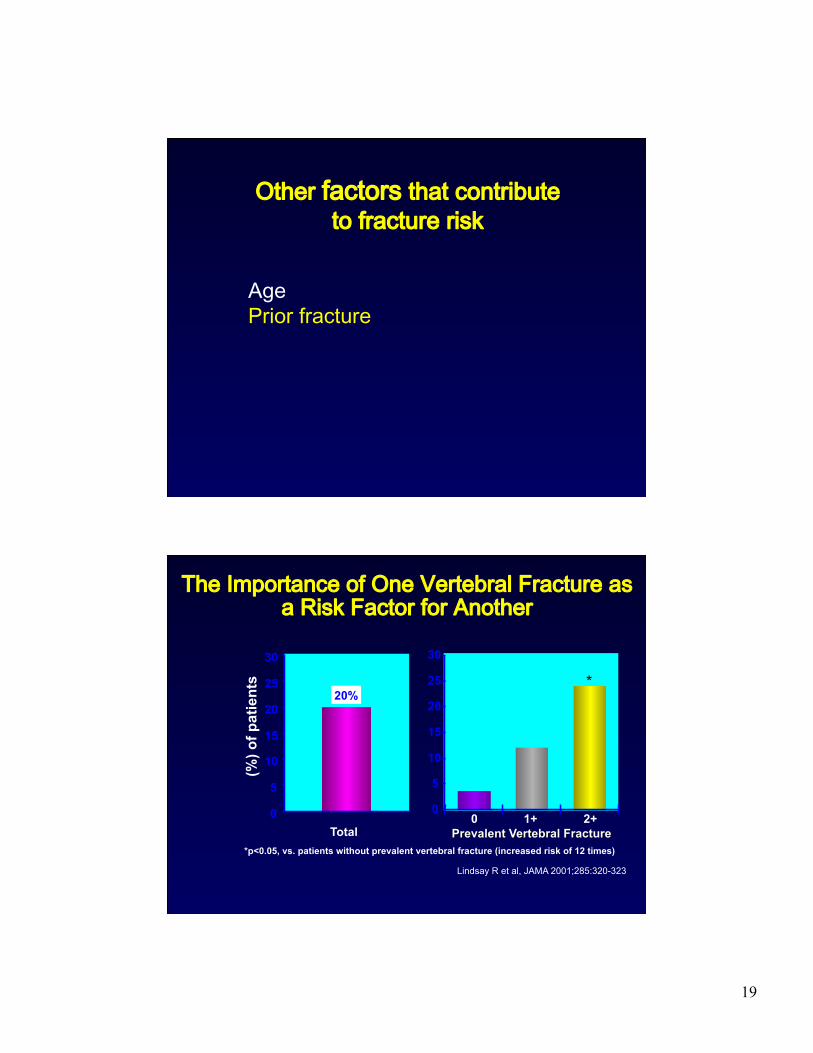
Other factors that contribute to fracture risk
Age Prior fracture
The Importance of One Vertebral Fracture as a Risk Factor for Another
*p<0.05, vs. patients without prevalent vertebral fracture (increased risk of 12 times)
*
Total
20%
(%) o
f pat
ient
s
Lindsay R et al, JAMA 2001;285:320-323
20
The osteoporotic fracture does not often lead to diagnosis or therapy
Postmenopausal Women with Distal Radial Fracture
Siris et al. J Clin Endocrinol Metab 88: 2003
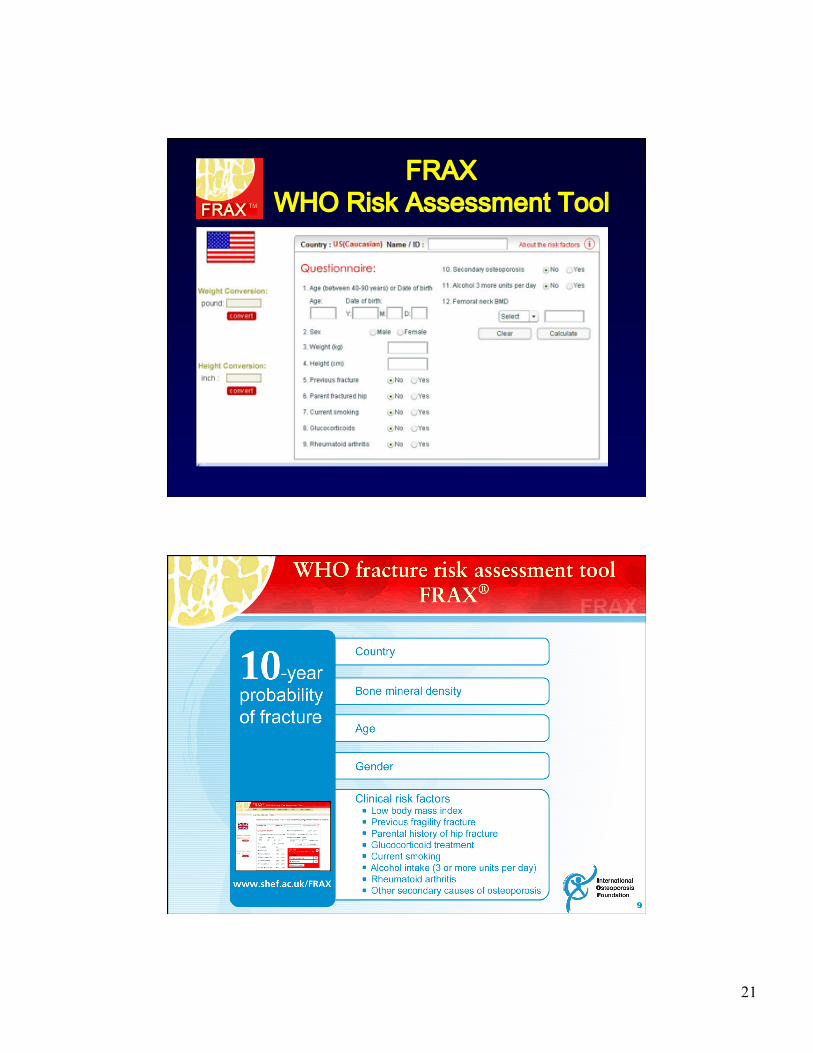
FRAX WHO Risk Assessment Tool • Developed by WHO to evaluate fracture risk
• Based on models that integrate the risks associated with clinical risk factors and BMD at the femoral neck
• Computer-driven: http://www.shef.ac.uk/FRAX/index.htm
• FRAX algorithms give the 10-yr probability of fracture 10-yr probability of hip fracture 10-yr probability of a major osteoporotic fracture (clinical spine, forearm, hip or shoulder fracture)
21
FRAX WHO Risk Assessment Tool
22
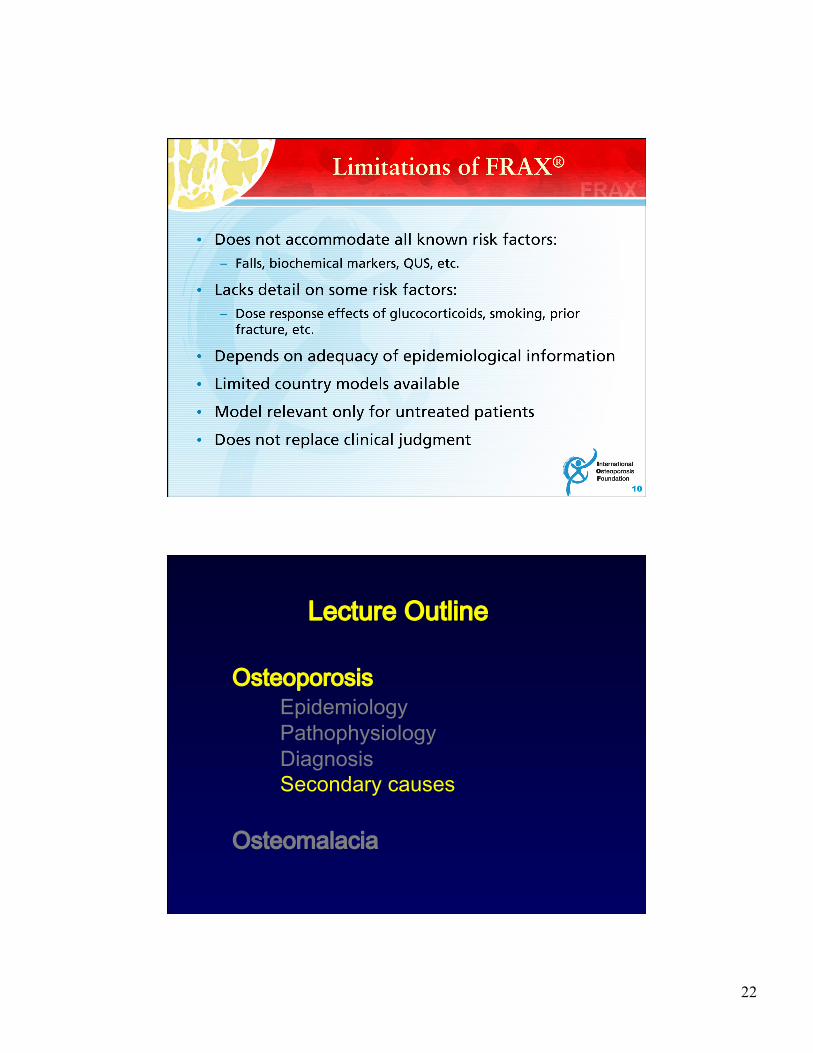
Osteoporosis Epidemiology Pathophysiology Diagnosis Secondary causes
Osteomalacia
Lecture Outline
23
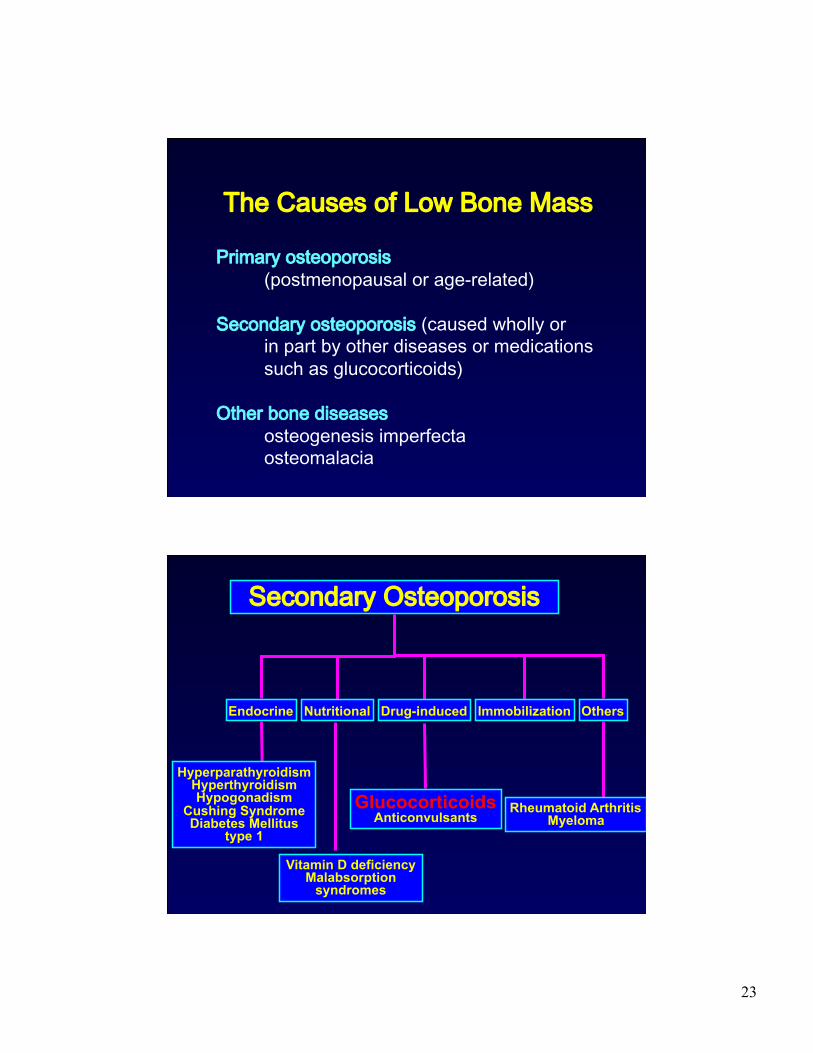
The Causes of Low Bone Mass
Primary osteoporosis (postmenopausal or age-related)
Secondary osteoporosis (caused wholly or in part by other diseases or medications such as glucocorticoids)
Other bone diseases osteogenesis imperfecta osteomalacia
Secondary Osteoporosis
Endocrine Nutritional Drug-induced Immobilization Others
Hyperparathyroidism Hyperthyroidism Hypogonadism
Cushing Syndrome Diabetes Mellitus
type 1
Glucocorticoids Anticonvulsants
Rheumatoid Arthritis Myeloma
Vitamin D deficiency Malabsorption
syndromes
24
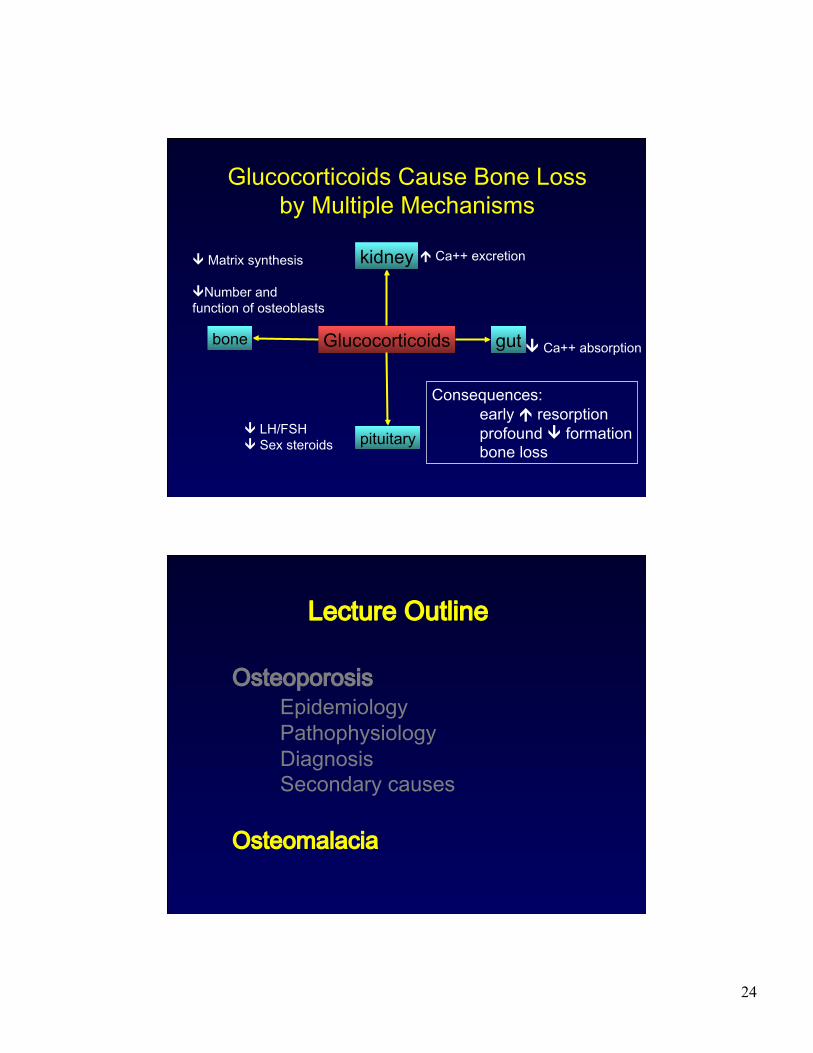
Glucocorticoids Cause Bone Loss by Multiple Mechanisms
Glucocorticoids
kidney
gut bone
pituitary
Ca++ excretion
Ca++ absorption
LH/FSH Sex steroids
Matrix synthesis
Number and function of osteoblasts
Consequences: early resorption profound formation bone loss
Osteoporosis Epidemiology Pathophysiology Diagnosis Secondary causes
Osteomalacia
Lecture Outline
25
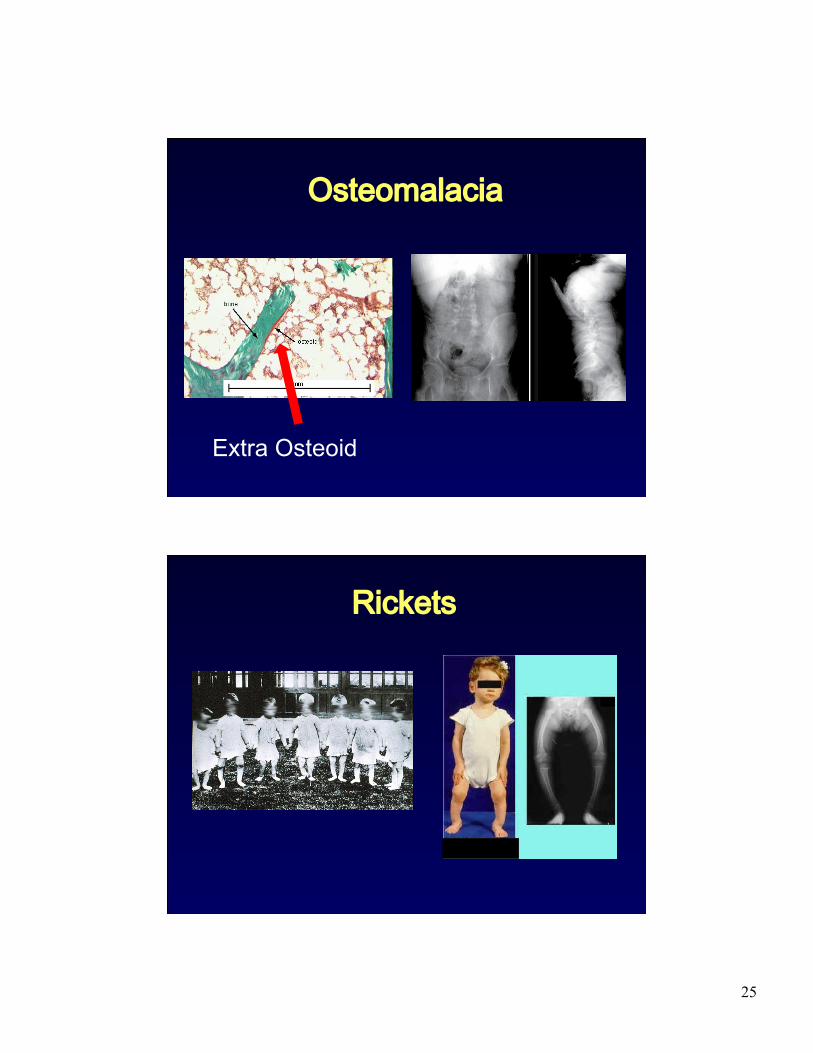
Osteomalacia
Extra Osteoid
Rickets
26
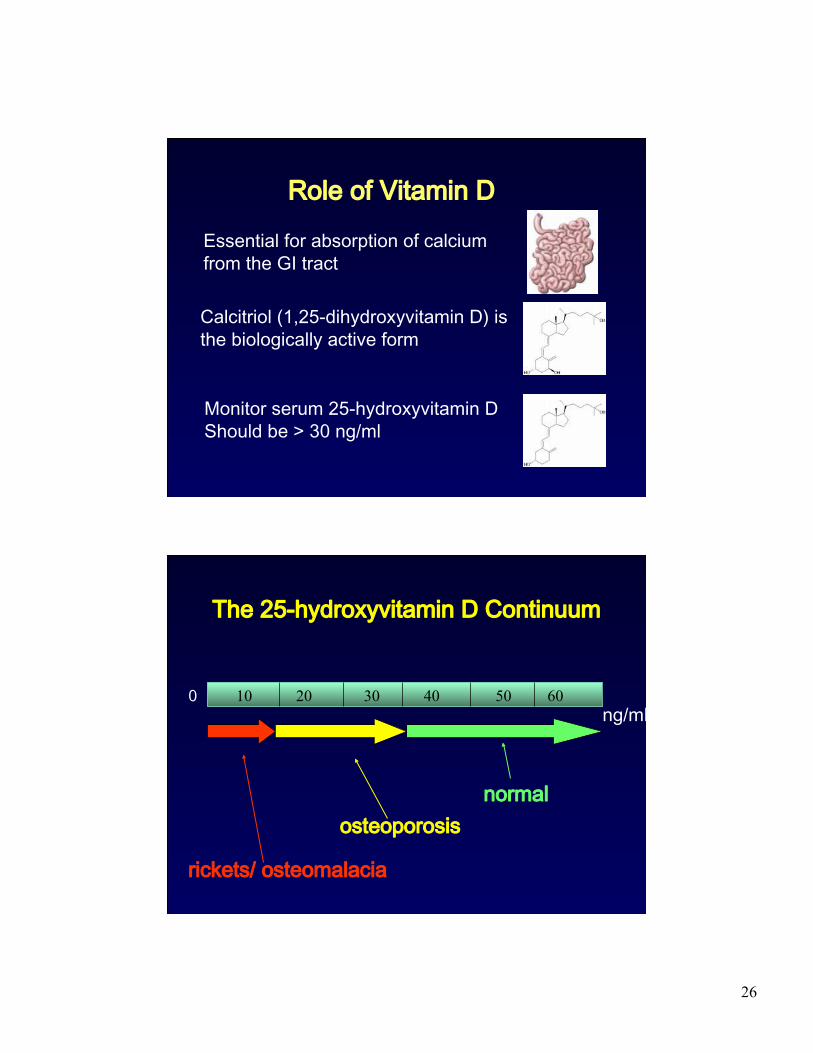
Role of Vitamin D
Essential for absorption of calcium from the GI tract
Calcitriol (1,25-dihydroxyvitamin D) is the biologically active form
Monitor serum 25-hydroxyvitamin D Should be > 30 ng/ml
ng/ml 0 10 20 40 30 60 50
osteoporosis
rickets/ osteomalacia
normal
The 25-hydroxyvitamin D Continuum
27
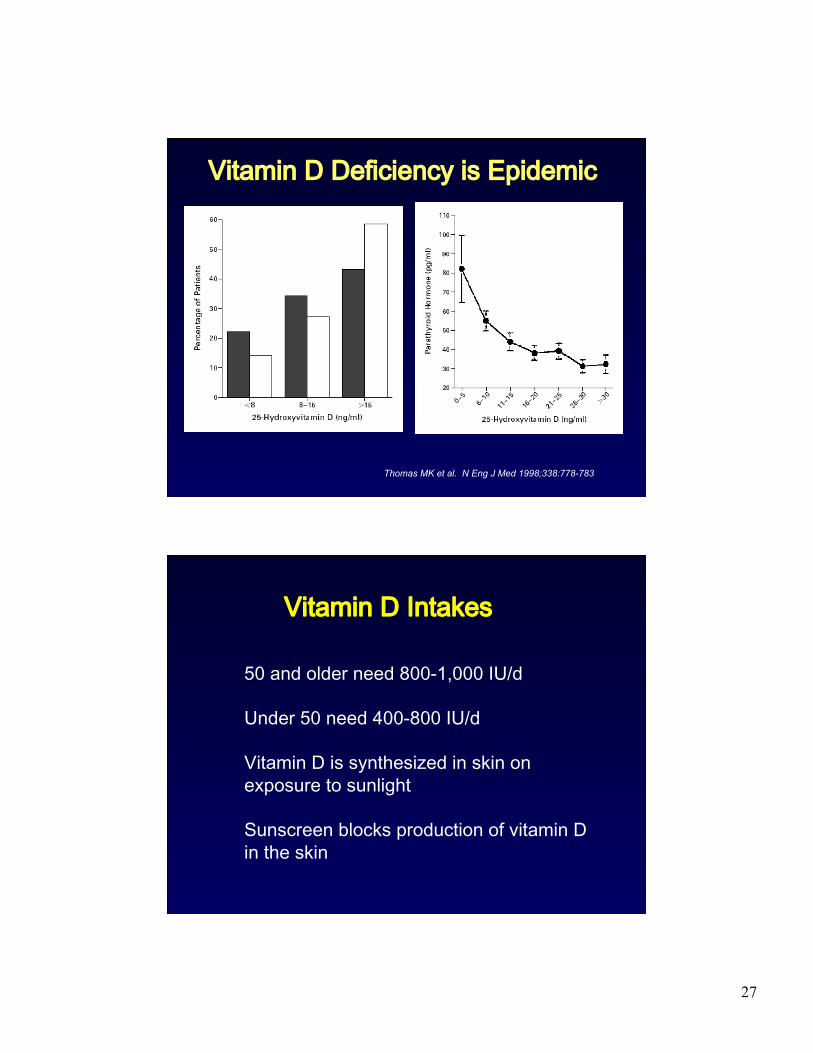
Thomas MK et al. N Eng J Med 1998;338:778-783
Vitamin D Deficiency is Epidemic
Vitamin D Intakes
50 and older need 800-1,000 IU/d
Under 50 need 400-800 IU/d
Vitamin D is synthesized in skin on exposure to sunlight
Sunscreen blocks production of vitamin D in the skin
28
Osteoporosis in 2010 Advances in Awareness, Diagnosis and Therapy