Embed Size (px)
Citation preview

Non-invasive blood pressure measurements and aortic blood flow velocity in neonates
Eero Rahiala*, Tero Tikanoja
Department of Paediatrics, Kuopio University Hospital, FIN- 70211 Kuopio, Finland
Received 4 November 1996; revised 1 February 1997; accepted 18 February 1997
Abstract
We studied the systolic blood pressure difference between me upper and the lower extremities in healthy newborn infanta and the effect of the istbmic narrowing of the aorta on the possible difference. The blood pressure was measured with an oscillometric blood pressure device from every extremity of 36 healthy infants aged 2-5 days. A Doppkr echocardiogrqrhy was performed for each infant to measure the aortic blood flow velocity in the ascending aorta and in the aortic arch above and below the isthmic narrowing. The mean blood pressure readings (S.D.) were the following: the right arm 76.8 (7.3)/48.1 (6.9), the left arm 77.5 (7.4)/51.6 (7.0), the right thigh 77.7 (7.1)/40.7 (5.8), the left thigh 76.8 (6.4)/39.6 (5.Q the right calf 75.5 (7.1)/46.6 (5.7) and the left calf 77.1 (8.6)/48.7 (6.7). The aortic blood flow was faster below the istbmic narrowing of the aorta (1.1520.19 m/s) than in the ascending aorta (0.93kO.12 m/s) or in the aortic arch above the isthmus (0.99kO.15 m/s). The cakulated pressure gradient between the ascending aorta and aorta below the isthmus was 2.02 1.8 mmHg and between opposite sides of the isthmus 1.5? 1.2 mmHg. Unlike in childhood and adolescence, the systolic blood pressure in the lower extremities of healthy newborn infants is not higher than in the upper extremities. The physiological narrowing of the aortic arch does not explain this phenomenon. If blood pressure measurements are performed on a neonate to rule out aortic coarctation, the readings obtained must be interpreted in respect to normal values in newborns. 0 1997 Elsevier Science Ireland Ltd.
Keywords: Blood pressure; Oscillometric method; Newborn infant: Aortic coarctation: Doppler echocardiography
*Corresponding author. Tel.: + 358 17 173311; fax: + 358 17 172410.
037X-3782/97/$17.00 0 1997 Elsevier Science Ireland Ltd. All rights reserved PI1 SO378-3782(97)01883-5
108 E. Rahiala, T. Tikanoja / Early Human Development 49 (1997) 107-112
1. Introduction
An oscillometric non-invasive blood pressure device provides a reliable method to measure blood pressure in infants [ 1,2]. However, only a few studies have been published on the blood pressure differences between the arm and the calf in neonates [3,4]. The systolic blood pressure in the arm of a healthy newborn seems to equal the corresponding pressure in the calf. In childhood and adolescence, the systolic blood pressure has been reported to be 5-9 mmHg higher in the calf [5]. Aortic coarctation results in decreased pressures in the lower extremities.
The normal narrowing of the aortic arch called the isthmus causes a transitory elevation in the blood flow velocity. The role of the isthmus in healthy neonates in explaining the absence of the systolic blood pressure difference has been suggested but not previously studied [5]. The purpose of this study was to confirm further that there is no or only a small systolic blood pressure difference between the upper and the lower extremities of a healthy newborn infant, and to enlighten the effect of the isthmic narrowing as an explanation for this phenomenon.
2. Materials and methods
With the approval of the ethical council of Kuopio University Hospital healthy newborns were randomly chosen for the study. Informed consent was obtained from the parents. All infants were examined in the maternal care unit of Kuopio University Hospital, before they left the hospital.
We measured the systolic (SP) and the diastolic (DP) blood pressure from every extremity of 36 healthy neonates aged 2-5 days (mean 2.9 days). Nineteen babies (53%) were girls and 17 (47%) boys. The exclusion criteria were: (1) any perinatal problem, (2) heart or other anomalies (one boy with a small ventricular septal defect was found and excluded from the study), and (3) change in state of arousal (6 infants) during the measurements. Birth weight ranged from 2680-4140 g (mean 34202420 g) and height from 46-55 cm (mean 5022 cm). The mean gestational age at birth was 39 weeks and 5 days. The number of infants born by caesarean section (8/36, 22%) was slightly higher than the average section rate at Kuopio University Hospital (18%). Mothers anatomical reasons and/or breech position was the indication for operative delivery in 5 cases. Prolonged delivery led to caesarean section in 3 cases. None of the neonates suffered from intrapartal asphyxia.
In order to obtain the blood pressure non-invasively, we used a Dinamap 1846 SX (Criticon Inc., Tampa, FL) oscillometric blood pressure device. Blood pressure readings by Dinamap have been reported to be closely similar to invasive readings in newborns [ 1,6]. The blood pressure was measured from both arms, thighs and calves. The cuff sizes were chosen by the recommendations of the American Heart Association [7-91. For all arm and calf measurements the same cuff size was used with every infant. The thigh cuff was larger, but again the same in all infants. This was to mimic a clinical situation as much as possible. The environment was dim and quiet, the infant lying supine under a warming lamp. The babies were fed before the
E. Rahiala, T. Tikanoja I Early Human Development 49 (1997) 107-112 109
measurements and they were sleeping or sleepy. Thus the error caused by a possible arousal of the infant was minimized [lo]. The cuffs for the arm and calf measure- ments were placed first and the thigh cuffs after 5 measurements. This was to minimize the handling of the neonate, which could have resulted in an elevation of blood pressure. If the state of arousal of the infant changed during the measurements, he or she was excluded from the study.
We measured the blood pressure by the following program: right arm, right calf, left arm, left calf, right arm, right thigh, left thigh, right arm and right calf. It has been reported that the first blood pressure reading obtained with the Dinamap 1846 SX is a little higher than the following ones [ 111. Thus, the readings of the first measurements were analyzed separately. The first author performed all the measurements to avoid methodological errors.
After the blood pressure measurements a Doppler echocardiography was performed to ensure the normal structure of the heart and to measure the blood flow velocity in the aorta [12]. The same paediatric cardiologist (IT), who was at this stage unaware of the blood pressure readings of the infant, performed every examination using Vingmed CPM 750 and a 5 MHz probe.
Blood flow velocities in the ascending aorta immediately before arching, as well as above and below the isthmic narrowing of the aorta were measured from the suprasternal notch. Pulsed wave Doppler was used in all three measurements. The angle of insonnation was kept as small as possible and no angle correction was used. At each site, the means of three measurements with good envelopes were calculated. The respective pressure gradients were calculated according to the Bernoulli equation, Pl - P2 = 4 X (V2’ - Vl’). Ductus arteriosus had closed in all neonates.
The statistical calculations were performed using the SPSS/PC + program (SPSS Inc., IL, USA). Student’s t-test for paired samples, Pearson’s correlation analysis, and Kolmokorov-Smirnov test for normal deviation were performed.
3. Results
3. I. Blood pressure
The mean blood pressure values according to sex and site are shown in Table 1. The first right arm measurement (SP 77.4k8.6 mmHg, DP 48.428.1 mmHg} did not differ from the later two measurements (SP 76.827.3 mmHg, DP 48.126.9 nunFIg). The only statistically significant differences were the low DPs from both thighs compared with both arm or calf DP readings (P < 0.001).
When all arm and calf measurements were summarized, the mean SP difference between arm and calf pressure was l.Ok4.7 mmHg. The difference ranged from - 9.3 to + 13.3 mmHg. The mean SP difference was higher in boys than in girls (3.0 vs. 0.75 mmHg, P = 0.015).
Blood pressure values did not correlate with age or way of birth. A low positive linear correlation between the mean systolic blood pressure and weight (r = 0.39) and
110 E. Rahiala, T. Tikanoja I Early Human Development 49 (1997) 107-112
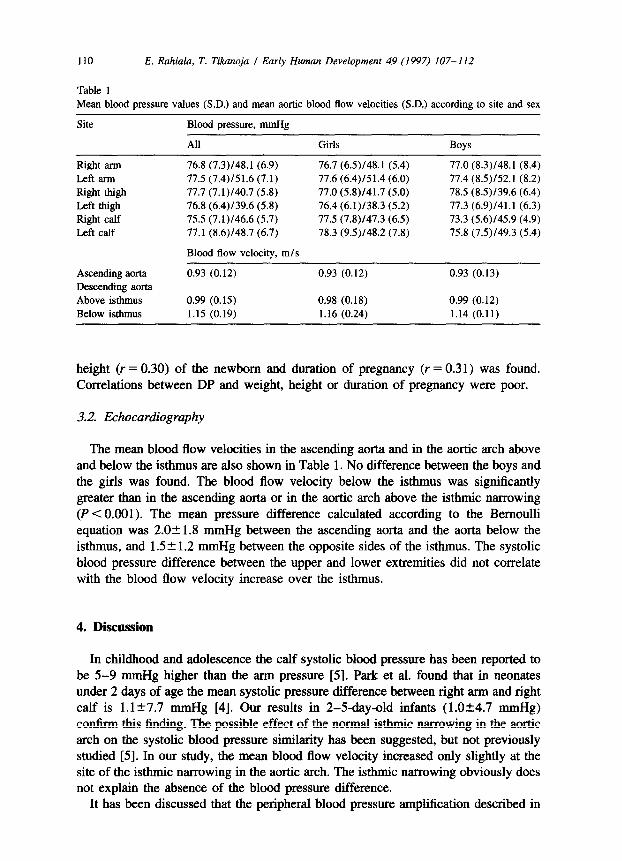
Table 1 Mean blood pressure values (SD.) and mean aortic blood flow velocities (S.D.) according to site and sex
Site Blood pressure, mmHg
All Girls Boys
Right arm 76.8 (7.3)/4&l (6.9) 76.7 (6.5)/48.1 (5.4) 77.0 (8.3)/48.1 (8.4) Leftaml 77.5 (7.4)/51.6(7.1) 77.6 (6.4)/51.4 (6.0) 77.4(8.5)/52.1 (8.2) Right thigh 77.7(7.1)/40.7(5.8) 77.0(5.8)/41.7(5.0) 78.5 (8.5)/39.6 (6.4) Leftthigh 76.8(6.4)/39.6(5.8) 76.4(6.1)/38.3 (5.2) 77.3 (6.9)/41.1(6.3) Right calf 75.5 (7.1)/46.6(5.7) 77.5 (7.8)/47.3 (6.5) 73.3 (5.6)/45.9(4.9) Left calf 77.1 (8.6)/48.7 (6.7) 78.3 (9.5)/48.2 (7.8) 75.8 (7.5)/49.3 (5.4)
Blood flow velocity, m/s
Ascending aorta Descending aorta Above isthmus Below isthmus
0.93 (0.12) 0.93 (0.12) 0.93 (0.13)
0.99 (0.15) 0.98 (0.18) 0.99 (0.12) 1.15 (0.19) 1.16 (0.24) 1.14 (0.11)
height (r = 0.30) of the newborn and duration of pregnancy (r = 0.31) was found. Correlations between DP and weight, height or duration of pregnancy were poor.
3.2. Echocardiography
The mean blood flow velocities in the ascending aorta and in the aortic arch above and below the isthmus are also shown in Table 1. No difference between the boys and the girls was found. The blood flow velocity below the isthmus was significantly greater than in the ascending aorta or in the aortic arch above the isthmic narrowing (P < 0.001). The mean pressure difference calculated according to the Bernoulli equation was 2.0+ 1.8 mmHg between the ascending aorta and the aorta below the isthmus, and 1.5+ 1.2 mmHg between the opposite sides of the isthmus. The systolic blood pressure difference between the upper and lower extremities did not correlate with the blood flow velocity increase over the isthmus.
4. Discussion
In childhood and adolescence the calf systolic blood pressure has been reported to be 5-9 mmHg higher than the arm pressure [5]. Park et al. found that in neonates under 2 days of age the mean systolic pressure difference between right arm and right calf is 1.157.7 mmHg [4]. Our results in 2-May-old infants (1.024.7 mmHg) confirm this finding. The possible effect of the normal isthmic narrowing in the aortic arch on the systolic blood pressure similarity has been suggested, but not previously studied [5]. In our study, the mean blood flow velocity increased only slightly at the site of the isthmic narrowing in the aortic arch. The isthmic narrowing obviously does not explain the absence of the blood pressure difference.
It has been discussed that the peripheral blood pressure amplification described in
E. Rahiala, T. Tkanoja I Early Human Development 49 (1997) 107- 112 III
children may not be operative in newborn infants [ 13,141. According to our results, it seems that the absence of peripheral amplification could have a stronger effect on the blood pressure similarity in arm and calf than the isthmic narrowing.
We tried to mimic the clinical measurements performed in the maternal care unit of Kuopio University Hospital as much as possible to give the results a greater clinical value. We found the blood pressure readings in the thigh to differ from the calf and arm readings. The systolic blood pressure was identical, but the diastolic considerably lower. The different cuff size, the variation in thigh circumference among neonates. the shape of the thigh and the more delicate way needed to place the cuff could be reasons for this. Since the same cuff is appropriate for the arm and calf measure- ments, we recommend the use of calf blood pressure rather than thigh blood pressure in neonates.
We found the SP difference between arm and calf to be higher in boys than in girls. Similar observations have not been reported previously. The sex difference observed awaits further confirmation.
In clinical practice, ruling out aortic coarctation in a neonate with a cardiac murmur or decreased femoral pulses is essential. We suggest that in these infams blood pressure measurements should be performed from both arms and both calves, at least twice from each extremity. Too rapid repetitive measurement from the same limb may cause erroneous readings. Therefore, following a predetermined protocol that includes a change in measurement location each time is advisable. Park et al. previously suggested that differential blood pressures (arm - calf) greater than 6-9 mmHg necessitate a thorough investigation for coarctation of the aorta [4]. In our study, the mean + 1 S.D. systolic blood pressure difference between the arm and the calf was 6 mmHg and the mean + 2 S.D. 11 mmHg. The individual range of arm vs. calf systolic blood pressure was from - 9 to + 13 mmHg in the 36 healthy neonates. Thus, recognizing the clear difference in normative values between neonates and older children is important. Slightly lower systolic blood pressure in the calf than in the arm is normal. However, duct-dependent aortic coarctation is a potentially life-threatening condition. Therefore we suggest Doppler echocardiography to be performed liberally, at least in every newborn infant with pressure difference greater than 10 mmHg.
References
[I] Park, M.K. and Menard, SM. (1987): Accuracy of blood pressure measurements by the Dinamap monitor in infants and children. Pediatrics, 79, 907-914.
[Z] Papadopoulos, G., Oldrop, B. and Mieke, S. (1994): Arterial blood pressure measurement with oscillometric instruments in newborns and infants. Anaesthetist, 43, 441-446.
[3] Cowan, F., Thoresen, M. and Walleoc, L. (1991): Arm and leg blood pressures - are they really so different in newborns? Early Hum. Dev., 26, 203-211.
[4] Park, M.K. and Lee, D. (1989): Normative arm and calf blood pressure values in the newborn. Pediatrics, 83, 240-243.
[5] Park, M.K., Lee, D. and Johnson, G.A. (1993): Oscillometric blood pressures in the arm, thigh, and calf in healthy children and those with aortic coarctation. Pediatrics, 91, 761-765.
112 E. Rahiakz, T. Tikanoja / Early Human Development 49 (1997) 107-112
[6] Borow, K.M. and Newburger, J.W. (1982): Noninvasive estimation of central aortic pressure using the oscillometric method for analyzing systemic artery pulsatile flow: comparative study of indirect systolic, diastolic, and mean brachial artery pressure with simultaneous direct ascending aortic pressure measurements. Am. Heart J., 103, 879-886.
[7] Perloff, D., Grim, C., Flack, J., Frohlich, E.D., Hill, M., McDonald, M. and Morgenstem, B.Z. (1993): Human blood pressure determination by sphygmomanometry. AHA Medical/Scientific Statement. Circulation, 88, 2460-2470.
[8] Whincup, PH., Cook, D.G. and Shaper, A.G. (1989): Blood pressure measurements in children: the importance of cuff bladder size. J. Hypertens., 7, 845-850.
[9] Lum, L.G. and Jones, M.D. (1977): The effect of cuff width on systolic blood pressure measurement in neonates. J. Pediatr., 91, 936-966.
[lo] Sitka, U., Weinert, D., Berle, K., Rtier, W. and Schuh, J. (1994): Investigations of the rhythmic function of heart rate, blood pressure and temperature in neonates. Eur. J. Pediatr., 153, 117-122.
[ll] Gillman, M.W. and Cook, N.R. (1995): Blood pressure measurement in childhood epidemiological studies. Circulation, 92, 1049-1057.
[12] Rao, P.S. and Carey, P. (1989): Doppler ultrasound in the prediction of pressure gradients across aortic coarctation. Am. Heart J., 118, 299-307.
[13] Park, M.K., Robotham, J.R. and German,VF. (1983): Systolic pressure amplification in pedal arteries in children. Crit. Care Med., 11, 286-289.
[14] Butt, W.W. and Whyte, H. (1984): Blood pressure monitoring in neonates: comparison of umbilical and peripheral artery catheter measurements. J. Pediatr., 105, 630-632.




![Impaired aortic distensibility and elevated central blood pressure … · dilatation [2], hypertension [7], bicuspid aortic valve (BAV) [8], 45,X karyotype, and coarctation of the](https://img.dokumen.tips/doc/110x75/604569b791851d060a0e93f7/impaired-aortic-distensibility-and-elevated-central-blood-pressure-dilatation-2.jpg)
























