Embed Size (px)
Citation preview

CASE REPORT
Non-enhancing relapse of a primary CNS lymphoma with multiplediffusion-restricted lesions
Lars Fischer • Arend Koch • Uwe Schlegel •
Hans-Christian Koch • Rudiger Wenzel •
Nicolas Schroder • Eckhard Thiel • Agnieszka Korfel
Received: 29 January 2010 / Accepted: 21 June 2010 / Published online: 3 July 2010
� Springer Science+Business Media, LLC. 2010
Abstract Primary CNS lymphoma (PCNSL) and its vari-
ant primary intraocular lymphoma (PIOL) are rare forms of
extranodal non-Hodgkin’s lymphoma confined to the CNS
including the retina and the optical nerve; histologically,
most cases are diffuse large B cell lymphomas. PCNSL in
immunocompetent patients display typical radiological
features on MRI, i.e. intensely and homogeneously enhanc-
ing lesions with moderate edema. Here, we report a 52-year-
old male with a history of a PIOL and two consecutive
intracerebral relapses who presented with dysarthria, dys-
phagia, and gait ataxia. Gadolinium-enhanced T1 scans were
unremarkable but multiple lesions with restricted water
diffusivity were seen on diffusion-weighted imaging.
Relapse of his PCNSL was secured histologically only on
autopsy. The possible etiology of the diffusion-restricted
lesions is discussed.
Keywords Diffuse large B cell lymphoma �Primary CNS lymphoma � Diffusion weighed imaging �Non-enhancing
Case
A 52-year-old male with a history of primary intraocular
lymphoma (PIOL) and two consecutive intracerebral
relapses presented in November 2008 with rapidly pro-
gressive cerebellar dysarthria, dysphagia for solid food,
gait ataxia and a continuous rhythmic twitching of the soft
palate, suggestive of palatal myoclonus, not involving
other oromandibular or oculomotor muscles.
In October 2004, a PIOL of the right eye (high-grade B
cell non-Hodgkin’s lymphoma) was established by vitrec-
tomy. No further CNS or systemic lymphoma manifestations
were detected on cranial MRI (cMRI), in cerebrospinal fluid
(CSF), on chest and abdomen computed tomography (CT) or
in bone marrow. A complete remission (CR) was achieved in
February 2005 after six courses of intravenous ifosfamide. In
June 2006, the patient presented with dysarthria, right-sided
ataxia and facial nerve palsy due to an isolated cerebellar
relapse with a single right cerebellar lesion moderately
enhancing on T1-weighted MRI scans (Fig. 1a). Five cour-
ses of intravenous high-dose methotrexate (HD-MTX) (4 g/
m2/day 1) and ifosfamide (2.0 g/m2/day/days 3–5) were
given (with collection of peripheral blood stem cells after
course 3) resulting in a CR. In May 2008, ataxia, dysarthria
and paresis with hypesthesia of the left leg developed. Cra-
nial MRI showed a singular, intensely enhancing lesion in
the right semioval centre (Fig. 1b). No ocular or systemic
manifestations were detected. The patient was treated with
four cycles of HD-MTX (2 g/m2 due to renal insufficiency)
L. Fischer (&) � E. Thiel � A. Korfel
Department of Hematology and Oncology, Charite
Universitatsmedizin, Campus Benjamin Franklin,
Hindenburgdamm 30, 12200 Berlin, Germany
e-mail: [email protected]
A. Koch � N. Schroder
Department of Neuropathology, Charite Universitatsmedizin,
Campus Mitte, Berlin, Germany
U. Schlegel
Department of Neurology, Knappschaftskrankenhaus,
University of Bochum, Bochum, Germany
H.-C. Koch
Department of Neuroradiology, Charite Universitatsmedizin,
Campus Benjamin Franklin, Berlin, Germany
R. Wenzel
Department of Neurology, Charite Universitatsmedizin,
Campus Benjamin Franklin, Berlin, Germany
123
J Neurooncol (2011) 102:163–166
DOI 10.1007/s11060-010-0287-5
and myeloablative chemotherapy (carmustin 400 mg/m2
and thiotepa 4 9 5 mg/kg) followed by autologous stem cell
transplantation resulting in a CR.
In November 2008, the patient presented with the initially
described symptoms. On cMRI, multiple supratentorial white
matter lesions were visible on T2 and particularly on FLAIR
scans, but T1 scans were unremarkable and no gadolinium
enhancement was seen. Diffusion-weighted scans revealed
several small hyperintense lesions, some with corresponding
signal reduction on ADC mapping (Fig. 2). In the CSF, no
lymphoma cells were detected by cytomorphologic, im-
munocytologic or PCR evaluation, and PCR for HSV and JC
virus DNA was negative. A duodenal biopsy was negative
for Trophyrema whippeli. The patient declined another brain
biopsy and was temporarily treated with dexamethasone,
aciclovir, ceftriaxon and trimethoprim/sulfamethoxazole
with no clinical effect, but there was progression of the
multiple non-enhancing lesions on FLAIR and diffusion
weighed imaging (DWI) scans, both of periventricular and
peripheral location. His condition deteriorated and he died
shortly afterwards from central respiratory depression.
Post-mortem examination revealed an extensive infiltra-
tion of the brain with a diffuse large B cell lymphoma with a
typical perivascular accumulation (Fig. 3); an intravascular
lymphoma growth was not visible. In most brain specimens,
lymphoma cellular density was rather low or moderate.
Lymphoma diagnosis was further verified by PCR demon-
strating a clonal immunoglobulin rearrangement. The his-
tological examination of spleen, liver and bone marrow did
not yield any signs of lymphoma infiltration.
Discussion
The vast majority of immunocompetent primary CNS
lymphoma (PCNSL) patients exhibit characteristic MRI
features with intensely and homogeneously enhancing
lesions and moderate edema [1]. Very few PCNSL cases
lacking contrast enhancement have been reported, several
only at relapse despite characteristic MRI appearance at
first presentation [2–5]. In contrast to the rather dense focal
tumor cell infiltration in typical PCNSL, most of these
cases exhibited a diffuse brain infiltration with lymphoma
Fig. 1 MRI images of the two precedent intracerebral relapses with
a radiomorphologic appearance characteristic for PCNSL (T1,
gadolinium)
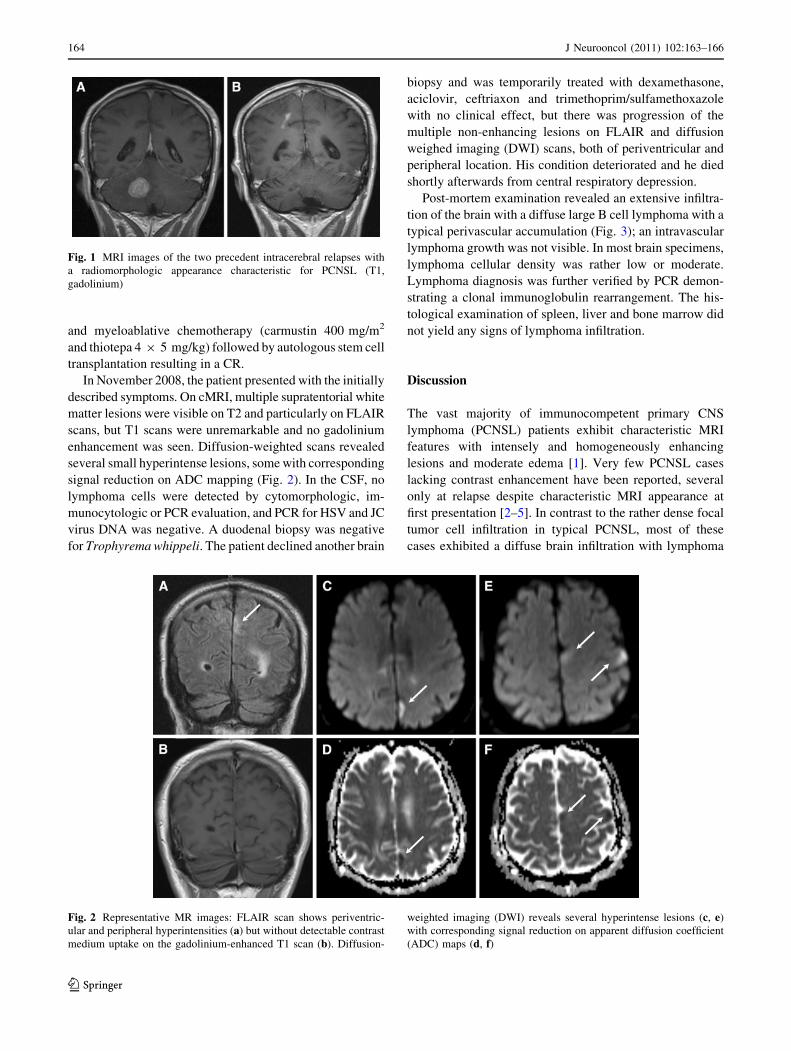
Fig. 2 Representative MR images: FLAIR scan shows periventric-
ular and peripheral hyperintensities (a) but without detectable contrast
medium uptake on the gadolinium-enhanced T1 scan (b). Diffusion-
weighted imaging (DWI) reveals several hyperintense lesions (c, e)
with corresponding signal reduction on apparent diffusion coefficient
(ADC) maps (d, f)
164 J Neurooncol (2011) 102:163–166
123

cells obviously not resulting in a significant disruption of
the blood–brain barrier. Thus, the term ‘‘lymphomatosis
cerebri’’ has been suggested to best describe this form of
PCNSL [6, 7].
Non-enhancing CNS lesions can frequently be found in
intravascular or angiotropic lymphoma (IVL), a rare variant
of aggressive (usually B cell) non-Hodgkin’s lymphoma
with selective growth of neoplastic cells within blood vessel
lumina [8]. It is a systemically disseminated lymphoma
with a high propensity for CNS and cutaneous lesions and
often infiltrating liver, spleen or bone marrow, but usually
sparing lymph nodes; patients often present with elevated
LDH, anemia and B symptoms [9]. CNS IVL may present
with infarct-like lesions and a rather ‘‘encephalopathic’’
syndrome due to intravascular lymphoma growth leading to
occlusion of many cerebral blood vessels [10–13].
PIOL is regarded a subtype of PCNSL which may occur
concomitantly with the cerebral manifestations or as an
ocular relapse of cerebral lymphoma. A small proportion of
patients (\20%) present initially with isolated intraocular
lymphoma; over 80% of these patients develop an intrace-
rebral relapse. Thus, the case presented here is typical for its
clinical course, also in terms of the subsequent remitting-
relapsing PCNSL [14]. However, our case is unique for its
combination of neuroradiologic features of lymphomatosis
cerebri (lack of gadolinium enhancement) and lesions
compatible with small infarctions (restricted water diffu-
sivity); moreover, those atypical features appeared only in
the third relapse. Due to the lack of enhancing lesions,
PCNSL relapse was not regarded as the preferred differen-
tial diagnosis. Although the progression of numerous
hyperintensities on T2 and FLAIR scans was suspicious,
they were not easily distinguishable from toxic leukoen-
cephalopathy [15].
The etiology of the various diffusion-restricted lesions
remains speculative. One explanation might be the pres-
ence of regional intravascular lymphoma growth causing
multiple small ischaemic lesions. However, no histologic
correlate for the infarct-like lesions could be found on the
brain autopsy specimens examined. On the other hand,
interspersed nodules with very dense lymphoma growth
may be responsible for the reduced water diffusion
observed, as markedly reduced ADC values have been
reported for PCNSL, especially in areas of dense cellularity
[16–18].
According to IPCG criteria lack of contrast-enhancing
lesions in the absence of other lymphoma manifestations is
regarded as CR in PCNSL [19]. However, as illustrated by
this case, the MRI appearance of a PCNSL relapse can
be atypical. In these patients, a brain biopsy should be
considered to secure the right diagnosis.
References
1. Kuker W, Nagele T, Korfel A, Heckl S, Thiel E, Bamberg M,
Weller M, Herrlinger U (2005) Primary central nervous system
lymphomas (PCNSL): MRI features at presentation in 100 patients.
J Neurooncol 72:169–177
2. Carlson BA (1996) Rapidly progressive dementia caused by
nonenhancing primary lymphoma of the central nervous system.
Am J Neuroradiol 17:1695–1697
3. DeAngelis LM (1993) Cerebral lymphoma presenting as a non-
enhancing lesion on computed tomographic/magnetic resonance
scan. Ann Neurol 33:308–311
4. Terae S, Ogata A (1996) Nonenhancing primary central nervous
system lymphoma. Neuroradiology 38:34–37
5. Ayuso-Peralta L, Orti-Pareja M, Zurdo-Hernandez M, Jimenez-
Jimenez FJ, Tejeiro-Martinez J, Ricoy JR, de la Lama A,
Bernardo AI (2001) Cerebral lymphoma presenting as a leuko-
encephalopathy. J Neurol Neurosurg Psychiatry 71:243–246
6. Bakshi R, Mazziotta JC, Mischel PS, Jahan R, Seligson DB,
Vinters HV (1999) Lymphomatosis cerebri presenting as a rap-
idly progressive dementia: clinical, neuroimaging and pathologic
findings. Dement Geriatr Cogn Disord 10:152–157
7. Rollins KE, Kleinschmidt-DeMasters BK, Corboy JR, Damek
DM, Filley CM (2005) Lymphomatosis cerebri as a cause of
white matter dementia. Hum Pathol 36:282–290
8. Swerdlow H, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H,
Thiele J, Vardiman JW (2008) WHO Classification of tumours of
haematopoietic and lymphoid tissues. IARC Press, Lyon
9. Ponzoni M, Ferreri AJ, Campo E, Facchetti F, Mazzucchelli L,
Yoshino T, Murase T, Pileri SA, Doglioni C, Zucca E, Cavalli F,
Nakamura S (2007) Definition, diagnosis, and management of
intravascular large B-cell lymphoma: proposals and perspectives
from an international consensus meeting. J Clin Oncol 25:
3168–3173
Fig. 3 Postmortem pathologic
specimen of the brain: CD79a
immunostaining (9100) for B
cells shows scattered infiltration
of the white matter with
lymphoma cells with some
perivascular cuffing
(a); hematoxylin and eosin (HE)
stain (9400) reveals blastic
morphology of lymphoma cells
typical for diffuse large cell
lymphoma (b)
J Neurooncol (2011) 102:163–166 165
123

10. Anghel G, Petrinato G, Severino A, Remotti D, Insabato L,
De Renzo A, Rotoli B, Majolino I (2003) Intravascular B-cell
lymphoma: report of two cases with different clinical presenta-
tion but rapid central nervous system involvement. Leuk Lym-
phoma 44:1353–1359
11. Holmoy T, Nakstad PH, Fredo HL, Kumar T (2007) Intravascular
large B-cell lymphoma presenting as cerebellar and cerebral
infarction. Arch Neurol 64:754–755
12. Iijima M, Fujita A, Uchigata M, Katoo H (2007) Change of brain
MRI findings in a patient with intravascular malignant lympho-
matosis. Eur J Neurol 14:e4–e5
13. Williams RL, Meltzer CC, Smirniotopoulos JG, Fukui MB,
Inman M (1998) Cerebral MR imaging in intravascular lym-
phomatosis. Am J Neuroradiol 19:427–431
14. Jahnke K, Thiel E, Abrey LE, Neuwelt EA, Korfel A (2007)
Diagnosis and management of primary intraocular lymphoma: an
update. Clin Ophthalmol 1:247–258
15. Lai R, Abrey LE, Rosenblum MK, DeAngelis LM (2004)
Treatment-induced leukoencephalopathy in primary CNS lym-
phoma: a clinical and autopsy study. Neurology 62:451–456
16. Zacharia TT, Law M, Naidich TP, Leeds NE (2008) Central
nervous system lymphoma characterization by diffusion-weigh-
ted imaging and MR spectroscopy. J Neuroimaging 18:411–417
17. Horger M, Fenchel M, Nagele T, Moehle R, Claussen CD,
Beschorner R, Ernemann U (2009) Water diffusivity: comparison
of primary CNS lymphoma and astrocytic tumor infiltrating the
corpus callosum. Am J Roentgenol 193:1384–1387
18. Barajas RF Jr, Rubenstein JL, Chang JS, Hwang J, Cha S (2010)
Diffusion-weighted MR imaging derived apparent diffusion
coefficient is predictive of clinical outcome in primary central
nervous system lymphoma. Am J Neuroradiol 31(1):60–66
19. Abrey LE, Batchelor TT, Ferreri AJ, Gospodarowicz M,
Pulczynski EJ, Zucca E, Smith JR, Korfel A, Soussain C,
DeAngelis LM, Neuwelt EA, O’Neill BP, Thiel E, Shenkier T,
Graus F, van den Bent M, Seymour JF, Poortmans P, Armitage
JO, Cavalli F (2005) Report of an international workshop to
standardize baseline evaluation and response criteria for primary
CNS lymphoma. J Clin Oncol 23:5034–5043
166 J Neurooncol (2011) 102:163–166
123





























