Embed Size (px)
Citation preview

NL Examination Part I
General Surgery

1.AAA
• ชาย 66 ป 1 วนหลงจาก emergency repair of rupture of aortic aneurysm ม urine output 35/4hr จาก Foley catheter ระหวางผาตดผ ปวยไดเลอดไป 4 U
• BT 37.3C , BP 104/68mmHg , PR 126/min
diffuse peripheral edema
CVS, RS, Abdomen : normal
• Lab : Hct 27%, Na 143, K 5
• อะไรนาจะเปนสาเหตของ Oliguria มากทสด
A:Heart failureB.HypovolemiaC.Occluded foley cathD.Renal a. thrombosisE.Tranfusion reaction

AAA Sx complication
1. MI or arrhythmia most common morbidity
2. Acute renal failure ruptured > elective
3. Ischemic colitis
4. Prosthetic graft infection

Renal failure s/p AAA Sx
1. Perioperative hypotension
2. Atheromatous embolization
3. Injury to the ureter
4. Preoperative contrast-induced nephropathy
5. Suprarenal aortic clamping

2.Urinary retention
A 70 year old man comes to the physician because of
urinary frequency , hesitancy and slow stream for 18 mo.
Rectal examination shows a firm slightly enlarged
prostate. After he voids, A Foley catheter is inserted and
Yields 500 ml of urine. Urinalysis is within normal limits. Which of the following is the most likely diagnosis?
A.Acute prostatitisB.BPHC.Neurogenic bladderD.Prostate cancerE.Urethral stricture

Lower urinary tract symptoms (LUTS)

Bladder Outlet Obstruction (BOO)
Complication of BOO1.Acute retention2.Chronic retention3.Impaired bladder emptying4.Hematuria5.Pain

3.Breast mass
A previously healthy 22 year old woman come to the
physician 3 months after discovering a mass in the lower
outer quadrant of her right breast. Examination shows a 2 cm
oval firm, smooth, mobile mass. No axillary masses are present.
Excision biopsy is most likely to show which of the following?
A. Fat necrosisB. FibroadenomaC. Fibrocystic chage of the breastD. Intraductal carcinomaE. Intraductal papillma

Approach Breast mass

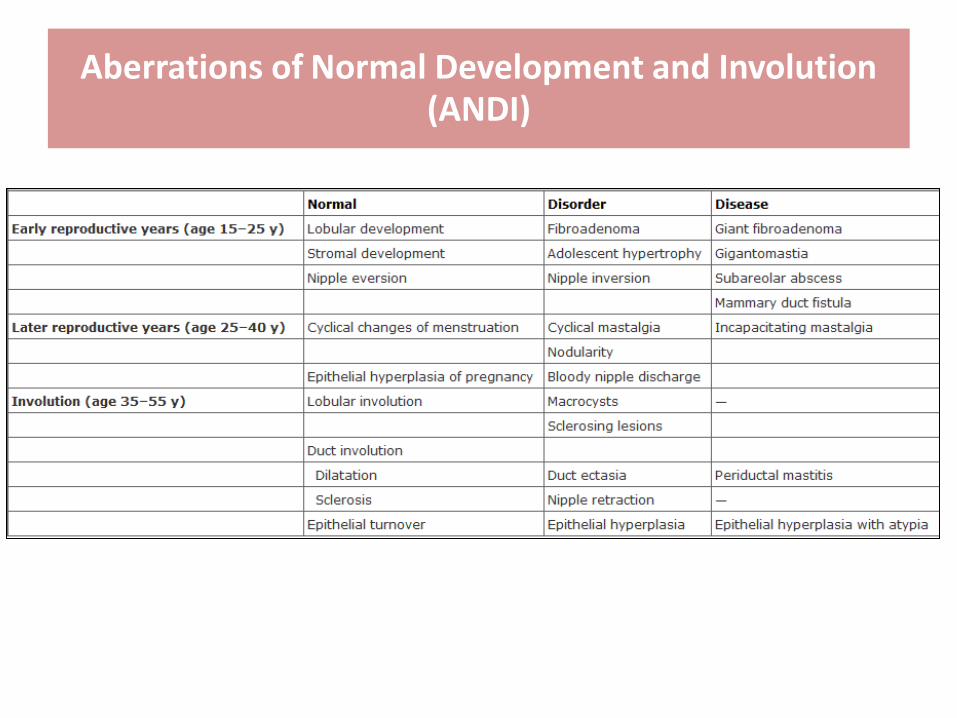
Aberrations of Normal Development and Involution (ANDI)

4.Benign breast mass
หญงโสดอาย 17 ป มกอนทเตานมซาย ไมเจบ
Left breast mass 3 cm. well circumscribe,
rubbery, movable, axillary LN-negative
?Management ทเหมาะสมA. Subcutaneous mastectomyB. Estrogen antagonizeC. Core needle biopsyD. Incisional biopsyE. Excision

5.Dysphagia 1
ผ ปวยชายอาย 50 ป มอาการกลนล าบากทงอาหารแขงและอาหาร
เหลวและมอาการไหลยอน ในชวง 4 เดอนทผานมา การตรวจรางกายอย
ในเกณฑปกต
Barium swallowing พบวาม dilatation of distal
esophagus and loss of peristalsis at distal
two-thirds. จงใหการวนจฉย

6.Dysphagia 2
ผ ปวยชายอาย 62 ป มอาการกลนเจบและน าหนกลดลง 4.5 กก.
ในชวง 1 เดอน ผ ปวยมประวตสบบหร ทกวน วนละ 2 ซอง เปนเวลา 40
ป ตรวจรางกายอยในเกณฑปกต
Barium swallowing พบ distal esophageal lumen
ตบแคบ และม partial obstruction จงใหการวนจฉย

7.Dysphagia 3
ผ ปวยหญงอาย 68 ป มอาการกลนล าบากทงอาหารแขงและอาหา
เหลวมานาน 7 เดอน รวมกบมผวหนงทมอเปลยนสเมอไดรบความเยน
และรสกแขงตรงทมอ
Barium swallowing พบวาม generally dilated
esophageal with loss of peristalsis. จงใหการวนจฉย


Barium swallowing

Barium swallowing

Barium swallowing

Achalasia

8.Trauma
A 21 yr old man is brought to the emergency department45 min after a head on motor vehicle collision in which he was the unrestrained driver. On arrival he is alert and coherent, he is breathing 100% O2.
Examination shows bruising over the central portion of the chest extending to both sides. Neck vein are not distended. His trachea is deviate to the right. Breath sounds are present on the right and absent on the left.
Following administration of 2 L of lactated Ringer’s solution, his systolic blood pressure is 80 mmHg.
Which of the following is the most appropriate next step in Tx?
A. IntubationB. Peritoneal lavageC. Blood transfusionD. ICD InsertionE. Pericardiocentesis

Primary survey

Secondary survey

Trauma Management


9.Inguinal Hernia
ผ ปวยชายไทยอาย 47 ป มกอนยบๆ บวมๆ ทขาหนบ เปนๆ หายๆ มา
3 ป มาดวย กอนบวม กดเจบ ดนกลบไมได 5 ชวโมง
ควรท าอะไรเปนอยางแรก
A) AnalgesicB) Try reducingC) ObserveD) SurgeryE) Analgesic + Try reducing

Approach

Type of Hernia

Strangulated Hernia
Golden period = 6 hours

Urgent Treatment

10.Colorectal polyp
• ชาย 56 ป พชายเปน ca colon แลวเสยชวต จงมาตรวจรางกาย ท า colonoscopy พบ polyps at descending colon แพทยท า polypectomy
• ถามวาขอใดมโอกาสพฒนาเปนมะเรงมากสด
A) Villous adenomaB) Tubulovillous adenomaC) Tubulous adenoma

Colorectal polyp
• Neoplastic polyp (Adenomatous polyps)• Harmatomatous polyp• Inflammatory polyp• Hyperplastic polyp
Risk of ca- Type of polyp- Size of polyp
Villous adenoma - 40%Tubulovillous - 20% Tubular adenoma - 5% Serrated polyp-ca 10%

Colorectal polyp

Colorectal polyp

11.Gross hematuria
ชาย 60 ป มาดวยปสสาวะเปนเลอด เปน ๆ หายๆ มา 1 เดอน ไมมไข
ไมมปสสาวะแสบขด ไมไดกนยาอะไร ตรวจรางกาย
PR = prostate gland grade II, smooth surface
ตรวจรางกายอนๆ ปกต ทานคดถงการวนจฉยใดมากทสด
A. Vesicle stoneB. CA prostateC. CA bladderD. Chronic pyelonephritisE. Chronic glomerulonephritis

Approach

Hematuria at beginning“lower tract”
Hematuria ตลอดสาย“upper tract ”
Terminal haematuria“severe bladder irritation”
(stone or infection)
Painless “? Malignancy”

12.BPH
ผชายปสสาวะไมพง ปสสาวะบอย ตรวจ prostate gland gr. IV,
smooth, ruberry, PSA ปกต จะ investigation อะไรตอ?
A. Tranabdominal U/SB. Urine C/SC. CrD. CystoscopeE. Prostate Bx

Investigation of men with LUTS

Investigation of men with LUTS

13.Gut obstruction
ชาย 40 ป ปวดทองมา 4 ชวโมง ปวดแบบบดๆ ทวทอง มคลนไสแตไมอาเจยน
ผายลมไดบาง เคยผาไสตงเมอ 10 ปกอน BT 37.5 PR 96 RR 20 BP 130/70
Mild abdominal distension, inc bowel sound with high pitch
no tender, PR ปกต ไมมเลอด plain abdomen ล าไสเลกโปงพองทวไป เรยง
ตว เปนระเบยบ ม air ใน rectum และ colon เลกนอย การรกษาทเหมาะสม
A. ยาแกปวดทองB. ยาปฏชวนะC. NG tube และ IV fluid
D. Rectal tubeE. Emergency laparotomy





14.Head injury
ชาย 20 ป ประสบอบตเหต 2 ชวโมงกอนมาโรงพยาบาล
GCS 8, pupil ขวา 3 mm RTL ซาย 5 mm SRTL
Rt. Hemiparesis จะจดการอยางไรตอไป
A. Observe neuro signB. ET tube + hyperventilationC. FurosemideD. Mannitol IVE. Craniotomy

GCS
Mild HI : 14-15/15 +LOC Mod HI : 9-13Severe HI : 3-8

15.CA breast
หญงอาย 50 ป มกอนทเตานมขวา กอนคอย ๆ โตขน ไมเจบ ตรวจ
รางกายมกอน 5 cm ท upper outer quadrant
Axillary node=fix ท า FNA ได malignant ท าอะไรดทสด
A. RadiationB. Simple mastectomyC. Radical mastectomyD. Hormanal therapyE. Neoadjuvant therapy

CA breast staging
T1=2cmT2=2-5cmT3=>5cmT4=local invade
N1=1-3 N2=4-9N3=>=10
N1=moveable ipsilat axillary LNN2N2a=fix/matted axillary LNN2b=ipsilat IM LN
N3N3a=ipsilat infraclavicular LNN3b=ipsilat IM LN and axillary LNN3c=ipsilat supraclavicular LN
Locally advanced CA = T3 or N2

CA breast Treatment
• Locally advanced Breast cancer
– Work up distant metastasis
– Neoadjuvant CMT reassess
• Response = Surgery
• No response = step up CMT / XRT
– Surgery
• MRM vs BCT
• ALND vs SLNBx

16.Peptic ulcer
ผ ปวยชาย 35 ป สบบหรวนละซองมา 10 ป มประวตปวดทองบรเวณลน
ปเปนๆหายๆมา 3 ป รบประทานยาน าโรคกระเพาะอาการดขน ไมเคยม
อาการถายเปนสด า หรออาเจยนเปนเลอด แพทยตรวจ upper GI
studies พบแผลขนาด 0.5 ซม. ท duodenal bulb
การรกษาทเหมาะสมทสดA. H.pylori eradicationB. Antisecretory agentC. High selective vagotomyD. Mucosal protective agentE. Antisecretory agent+giving up smoking

Peptic ulcer
? Cancer? H.pylori

H.pylori work up
• Histology (biopsy) = Gold std
• Rapid urease test (CLO test) = Simplest method
• Urea breath test = Confirm eradication
• Serologic test = Not confirm eradication
• Culture = Failure of ATB

17.Ischiorectal abscess
ผชาย 45 ป ปวดทวารหนก มไขมา 3 วน
ตรวจรางกาย tender over Rt.Ischiorectal space
PR: warm and tender along Rt. Side
รกษาอยางไรเหมาะสมทสด
A. Lateral sphincterectomyB. I&DC. DebridementD. Excision

Ischiorectal abscess


18.UGIB
ผชายอาย 60 ป อาเจยนเปนเลอดสด 2แกว 1 ชม.กอนมารพ.รสกตวด
V/S BP 90/60 mmHg PR 140/min RR 25/min
จงใหการดแลเบองตน
A. omeprazole IVB. Fluid resuscitationC. Retain NG TubeD. EsophagogastroscopyE. ซกประวตตรววจรางกายอยางละเอยด

Melena & Hematemesis
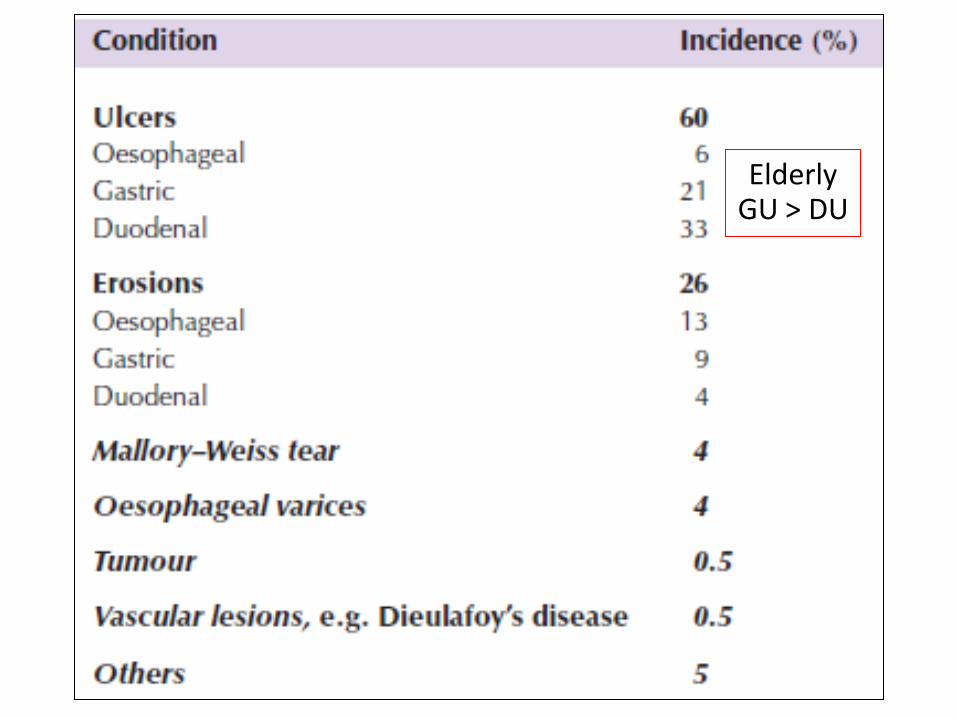
Elderly GU > DU

Varice vs Non varice

GIB treatment
1st = resuscitation

19.Pancreas
ชาย 60 ป ประวตดมสราเรอรงมาหลายป 1 เดอน มคลนไส อาเจยน
anorexia และมปวดทองทลนป 1 wk PTA ปวดทองท
epigastrium มากขน ม N/V คล าไดกอนแขงๆตงททอง
A. pancreatic pseudocystB. retroperitoneal lymphomaC. pancreatic cystadenomaD. pancreatic adenocarcinomaE. pancreatic cystadenocarcinoma

Chronic pancreatitis

Chronic pancreatitis
S&S1. Pain2. Malabsorption + wt loss3. Apancreatic DM (type 3 DM)
Complication1. Pseudocyst most common complication2. Pancreatic ascitis3. Pancreatic enteric fistula4. Pancreatic head mass5. PV/SV thrombosis

Pseudocyst
50% can resolve spontaneously (<6 cm)
? Infected FNA +ve Sx
Asymptomatic Conservative Treatment
Symptomatic or failed conservative Sx(Internal drain > external drain)

Pseudocyst
1. Percutaneous drainage2. Endoscopic drainage3. Open drainage
CystogastrostomyCystoduodenostomyCystojejunostomy (Roux En Y)
4. Resection Distal pancreatectomy5. ERCP Communicating duct

20.Acute Epididymo-Orchitis
ชายอาย 55 ป มาดวยกอนทอณฑะซาย 5 cm มอาการ ปวดบวม แดง
รอน จะรกษาอยางไร
A. CT scanB. UltrasoundC. morphine and try reductionD. ATBE. Immediate surgery
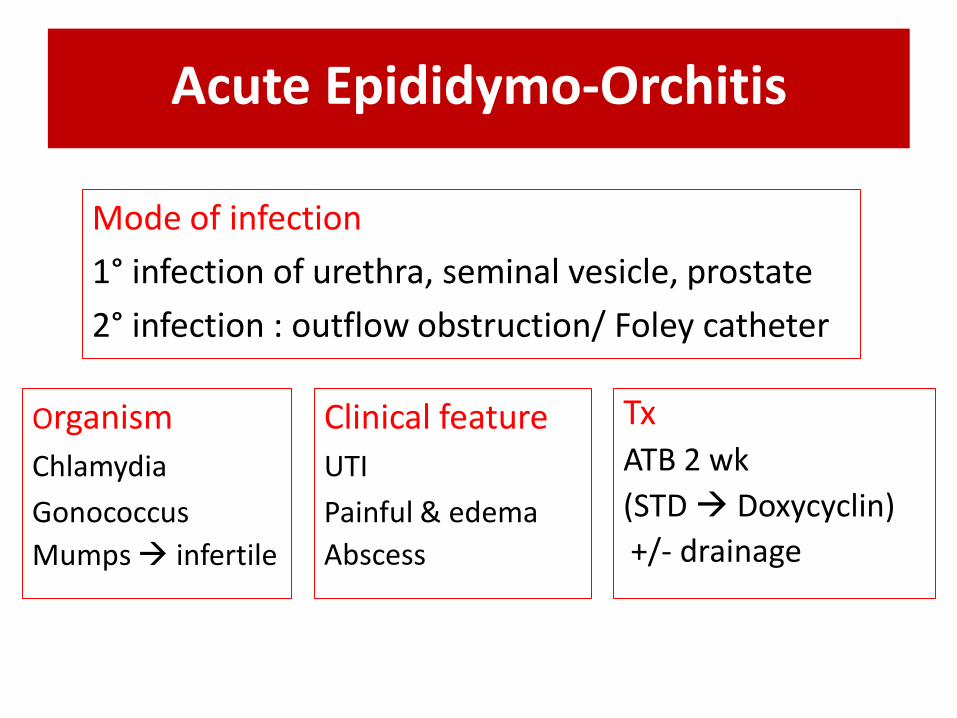
Acute Epididymo-Orchitis
Mode of infection
1° infection of urethra, seminal vesicle, prostate
2° infection : outflow obstruction/ Foley catheter
Organism
Chlamydia
Gonococcus
Mumps infertile
Clinical feature
UTI
Painful & edema
Abscess
TxATB 2 wk
(STD Doxycyclin)
+/- drainage

Chronic Epididymo-Orchitis
Organism
Tuberculous
Sarcoidosis LesionLower pole of the epididymis
2/3 =Renal Tuberculosis
InvestigationUrine/semen AFBIVPCXR
Tx
Tx primary lesion
Anti TB
Not resolved Sx

21.Acute cholecystits
หญง 40 ป ปวดทองใตชายโครงขวา 12 ชวโมง
PE BT 38.9 RUQ pain
U/S พบ gall stone, GB wall thickening, pericholecystic fluid
Management อะไรตอ
1. IV ATB2. IV ATB +ยาสลายนว3. IV ATB + percu.cholecystectomy4. IV ATB + LC ใน 48-72 hr
5. IV ATB+ ERCP


Acute cholecystits Tx

22.Liver Cyst
หญงอาย 50 ปมาตรวจสขภาพทโรงพยาบาลเอกชน ท า U/S เจอ
well-defined anechoic mass, strongly posterior
enhancement, 4 cm ท left lobe liver เปนอะไร
a. Hepatocellular carcinomab. Calcified granulomac. Liver abscessd. Hepatic cyst



23.Blunt abdominal injury
ชาย 35 ป ไดรบอบตเหตรถบรรทกชน คาดเขมขดนรภย มรอยช าทหนา
ทอง ขนาด 5 ซม จากดานขวาไปซายขนาด 5 ซม BP 110/70
PR 88 ตรวจทอง ม generalized mild tender
จะสงตรวจอะไร1. DPL2. FAST3. CT abdomen4. general abdominal exam5. Explore lap

DPL

Blunt abdominal injury

24.Head injury
ชายอาย 36 ป ขบรถชนตนไมรมทาง ท า CT brain ดงรป
(CT:cresent shape hemorrhage, midline shift)
a. Cerebral contusionb. EDHc. SDHd. SAH


25.Acute urinary retention
ชายอาย 72 ป ปสสาวะไมออกมา 1 วน ประวตเกาคอ 2 สปดาหกอน
admit ดวยเรองปสสาวะไมออกเฉยบพลน ไดใสสาวสวนปสสาวะคาไว
อยโรงพยาบาล 3 วน กลบมาบานมปสสาวะกลางคน 5-6 ครง ปสสาวะ
ไมพง กอนหนาจะมาโรงพยาบาลครงนเปนหวด และกนยาลดน ามก
1. retain foley catheter and off ยาลดน ามก2. intermittent catheter and refer for Sx3. retain foley cathteter and alpha blocker4. alpha blocker5. intermittent catheter , off ยาลดน ามก and alpha blocker


26.Acute pancreatitis
หญง 40 ป ปวดทองลนปมา 6เดอน ปวดเปนๆหายๆ นานครงละ1-2 hr
1 วนกอนมา รพ.ปวดทลนปอยางรนแรง
PE: moderate tenderness at epigastrium decrease BS
TB 0.5 AST/ALT 400/550 ALP 140 serum amylase 1500
investigation อะไรตอA. CT abdomenB. Serum lipaseC. Blood cultureD. Plain filmE. U/S abdomen


Severity assessment
• Early prognosis score
1. Ranson criteria (>=3 : severe pancreatitis)
2. APACHE II score (>=7 : severe pancreatitis)
• CT severity Index (CTSI) (>=4 : severe pancreatitis)
– Barthaza score + necrosis
(Gold std for severity assessment)


The End
part I





























