Embed Size (px)
Citation preview
Pediatric Pulmonology 36:369–375 (2003)
State of the Art
New Therapies for Asthma: Where Next?
Douglas S. Robinson, MA, MD, FRCP*
INTRODUCTION
The recent British Thoracic Society/Scottish Intercol-legiate Guideline Network guidelines on management ofasthma provide the first evidence-based framework fortherapy (BTS/SIGN), although it is of note that there islittle good evidence from specific pediatric studies toguide treatment of children with asthma.1 Although anti-inflammatory treatment with inhaled steroids (ICS) andlong-acting b2 agonists (LAB) is very effective, the guide-lines also document a lack of evidence for treatmentof more severe asthma at steps 4 and 5, and the continu-ed morbidity from asthma despite current medication.Asthma management plans and the appropriate use ofinhaler devices are important in improving delivery ofthese drugs, but there is a clear need for additionaltherapies for more severe asthma.
Over the last 20 years, there has been increased under-standing of the immunological basis of allergic asthma.There is now widespread acceptance of the Th2 hypoth-esis, whereby allergen activation of Th2T cells primes IgEsynthesis through interleukin (IL)-4 and IL-13, and eosi-nophilic airway inflammation through IL-5 (Fig. 1).2,3
Th2-type cytokines (as opposed to those from Th1 cells,such as interferon-g and lymphotoxin4) also have activityin promoting upregulation of adhesion molecules, che-mokine expression, and activation of structural cells, andthus may play a role in the further recruitment ofinflammatory cells and airway remodelling. Interestingly,similar immunopathology, with Th2 cell activation,eosinophilic inflammation, and even airwaymucosal localIgE synthesis, is seen in nonatopic or intrinsic and occu-pational asthma.5 Evidence from pediatric studies alsosupports a role for eosinophils and Th2 T-cell activation inchildhood asthma: eosinophilic inflammation wasdetected in bronchoalveolar lavage samples from infantswith asthma,6,7 and activated T cells and Th2 cytokineexpression were detected in blood T cells from childrenwith both atopic and nonatopic asthma.8,9 The delineationof the immunological pathways contributing to asthma
opened the possibility of novel therapy with specifictargeting of these processes. A number of such approacheswere recently tested in clinical trials and will be con-sidered below.
ANTI-IgE
The initiation of allergic reactions depends on the cross-linking of allergen-specific IgE bound to high-affinityreceptors (FceRI) on mast cells and basophils: blockingsuch immediate hypersensitivity reactions is thus clearlyan attractive target for allergic disease. A monoclonalantibodywas developed (termed E25) which could bind tofree IgE in the serum with very high affinity via the C3portion that interacts with FceRI. This antibody thereforeprevents binding of IgE to its receptor and does not cross-link any IgE already bound (an important feature, sincethis prevents any potential for triggering severe allergicreactions or anaphylaxis). This antibody has beenhumanized: the variable portions from the mouse mono-clonal antibodywere engineered onto a largely human IgGbackbone, to reduce immunogenicity so that repeatadminstration does not in itself cause an immune response.This preparation is termed omalizumab (XolairTM), and
Departments of Allergy and Clinical Immunology and Leukocyte Biology,
National Heart and Lung Institute and Basic Medical Sciences Division,
Faculty of Medicine, Imperial College London, and Royal Brompton and
St. Mary’s NHS Trusts, London, UK.
Grant sponsor: Wellcome Trust Research Leave Award for Clinicians.
*Correspondence to: Douglas S. Robinson, M.A., M.D., F.R.C.P., Basic
Medical Sciences Division, Faculty of Medicine, Imperial College London,
Dovehouse St., London SW3 6LY, UK.
E-mail: [email protected]
Received 3 July 2003; Accepted 17 July 2003.
DOI 10.1002/ppul.10375
Published online in Wiley InterScience (www.interscience.wiley.com).
� 2003 Wiley-Liss, Inc.
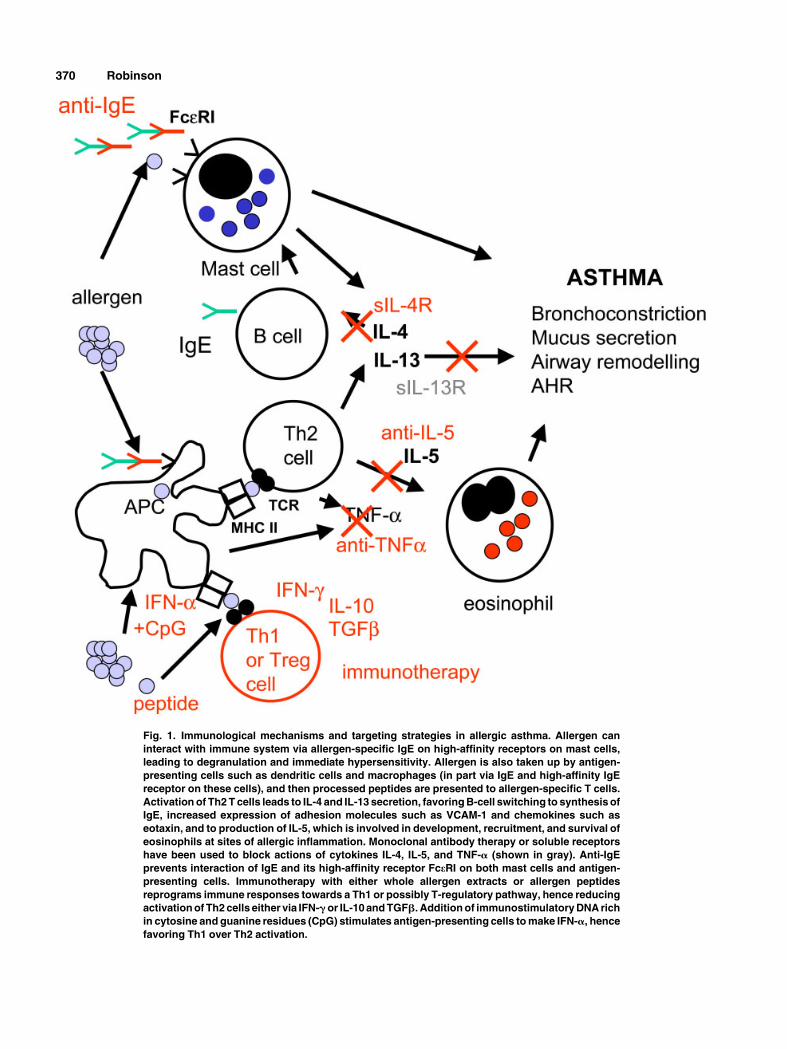
Fig. 1. Immunological mechanisms and targeting strategies in allergic asthma. Allergen can
interact with immune system via allergen-specific IgE on high-affinity receptors on mast cells,
leading to degranulation and immediate hypersensitivity. Allergen is also taken up by antigen-
presenting cells such as dendritic cells and macrophages (in part via IgE and high-affinity IgE
receptor on these cells), and then processed peptides are presented to allergen-specific T cells.
Activation of Th2 T cells leads to IL-4 and IL-13 secretion, favoring B-cell switching to synthesis of
IgE, increased expression of adhesion molecules such as VCAM-1 and chemokines such as
eotaxin, and to production of IL-5, which is involved in development, recruitment, and survival of
eosinophils at sites of allergic inflammation. Monoclonal antibody therapy or soluble receptors
have been used to block actions of cytokines IL-4, IL-5, and TNF-a (shown in gray). Anti-IgE
prevents interaction of IgE and its high-affinity receptor FceRI on both mast cells and antigen-
presenting cells. Immunotherapy with either whole allergen extracts or allergen peptides
reprograms immune responses towards a Th1 or possibly T-regulatory pathway, hence reducing
activation of Th2 cells either via IFN-gor IL-10 and TGFb. Addition of immunostimulatory DNA rich
in cytosine and guanine residues (CpG) stimulates antigen-presenting cells to make IFN-a, hence
favoring Th1 over Th2 activation.
370 Robinson

has been subject to a number of clinical studies in asthmaand other allergic diseases.10 Initial studies showed thatanti-IgE could reduce not only the mast cell-dependentimmediate response to inhaled allergen challenge (theearly asthmatic reaction), but also the delayed lateasthmatic reaction.11 While such activity could be due toreduced mast-cell activation, it is also of note that high-affinity IgE receptors are found on dendritic cells, i.e.,antigen-presenting cells that process allergen and activateTh2 cells: thus omalizumabmay target both the IgE and T-cell limbs of the allergic immune response.
To date there are three published studies of omaliuzu-mab in moderate/severe allergic asthma in adults, and onethat included children. All had a similar study design, andincluded patients with continuing symptoms and/or lungfunction impairment despite use of ICS and sometimesoral corticosteroids (though not LAB). The pediatric studyincluded 334 children with a mean age of 9.5 years. Aftera 4–6-week run-in phase, all children were switched tobeclomethasone dipropionate (BDP), and the dose wasadjusted to the minimum that controlled symptoms for afurther 4-week period. They were then randomized to twoweekly subcutaneous injections of Xolair or placebo for28 weeks. During the first 16 weeks of treatment the BDPdose was kept constant; thereafter it was systematicallyreduced. There was a significant reduction in steroidrequirement (median reduction in inhaled beclometasonewith Xolair was 100%, with complete withdrawal in 55%,whereas for placebo it was 66.7%, with complete with-drawal in 39%) and a reduced rate of asthma exacerbationsin the actively treated children (5 placebo-treated children,but none receivingXolair were admitted to hospital duringthe study with worsening asthma12). However, there wasno significant effect on lung function or symptom scores.There were also significant improvements in asthmaquality-of-life scores in the actively treated group,particularly in the activities and symptoms domains.These were most marked in the steroid reduction phase,where they reached the ‘‘clinically significant’’ cutoff innearly 50%of those treated.13 Two large adult studies usedsubcutaneous treatment and found that omalizumab treat-ment led to a reduced rate of exacerbations (0.28 perpatient for omalizumab vs. 0.54 per patient for placebo inthe steroid-stable phase of one study14), and a modestreduction in ICS dose,14,15 which was maintained in a24-week extension of the study.15,16 One study also show-ed a small but significant improvement in FEV1.
16Overall,a recent systematic review concluded that omalizumabhas activity in moderate/severe allergic asthma, but thatfurther comparative and pediatric data are required.17 Inparticular, studies in patients already taking LAB andother treatments in addition to ICS will be required, sincethis agent is likely to be expensive and perhapsmost usefulat step 4 of guidelines. Recent data from a study using thesame compound from another company showed that anti-
IgE may reduce symptoms from peanut allergy:18 thisagent acts systemically, and so should have the effect oftreating concomitant food allergy or rhinitis with asthma.
ANTICYTOKINE AGENTS
Studies from animal models of airway allergenchallenges allowed specific targeting of cytokines bygene disruption (knockouts), antibody treatment to blockcytokine activity, or the use of soluble receptors asblockers of cytokine activity. Such approaches suggestedthat IL-4, IL-5, and IL-13 would be valid targets fortherapy, though it is of note that different models can givedifferent results.19
ANTI-IL-4
An inhaled soluble IL-4 receptor was tested in twopublished studies of adult asthma.20,21 In both, the ap-proach was to study asthmatics with stable lung functionand symptomswhile taking ICS during a run-in phase, andthen to suddenly withdraw ICS treatment, substitutingeither sIL-4R or placebo. To optimize the chances ofdetecting a treatment effect, these volunteers had a trialwithdrawal of ICS before the sIL-4R was given, to ensurethat an exacerbation occurred on withdrawal, and werethen restabilized prior to the drug trial. In two studies ofover 100 asthmatics, the high-dose sIL-4R prevented theincrease in symptoms and fall in FEV1 seen in theasthmatics who had placebo substituted for ICS.20,21 Thiswork suggested that inhaled sIL-4R had promise as ananti-inflammatory agent in asthma. Although follow-upstudies on asthma were performed, and were thought tohave not confirmed this early promise, these have not yetbeen reported. The obvious reluctance of pharmaceuticalcompanies to publish adverse data from trials has impact-ed publication of studies of both anti-IL-4 and anti-IL-5,which is regrettable for asthmatics eagerly awaiting effec-tive new therapies. A monoclonal antibody has also beendescribed and is currently in human trials.22
IL-13 has activities similar to IL-4, which is not sur-prising since it shares receptor components, and thusblocking IL-13, like IL-4,might be expected to impact IgEswitching, and adhesion molecule and chemokine expres-sion. However, murine experiments suggest that IL-13,which also has its own unique receptor complex, may bean exciting target for asthma, since sIL-13R was able toblock airway hyperresponsiveness in a model withoutaffecting eosinophils or IgE.23,24 This approach has not yetbeen tested in humans.
ANTI-IL-5
Interleukin-5 emerged from the Th2/eosinophil hypoth-esis as perhaps that most attractive specific anti-asthmacytokine target: this cytokine is pivotal in eosinophil
New Therapies for Asthma 371

development, recruitment, and survival, yet seems to haveno other important function, and gene-deleted animals arehealthy. Animal studies suggested that one dose of anti-IL-5 antibody could reduce airway hyperresponsiveness toallergen challenge for up to 3 months. However, an initialhuman trial in 24 mild asthmatics showed that althoughanti-IL-5 could effectively reduce blood and sputumeosinophils, it had no effect on airway hyperresponsive-ness or the late asthmatic reaction to inhaled allergenchallenge.25 A study with another anti-IL-5 monoclonalantibody in more severe asthma similarly showed noclinical benefit.26 We recently reported on a study of theeffect of anti-IL-5 treatment on bronchial mucosal andbone marrow eosinophils in asthmatics. Despite dramaticreductions in blood eosinophils (over 90%) after threeinfusions of 750 mg of antibody, in this 12-week studythere was only about a 50% reduction in numbers ofairway and bonemarroweosinophils.27,28 This incompletedepletion of airway eosinophils27 may be because tissueeosinophils downregulated their IL-5 receptors,29,30 sothat they are no longer dependent on IL-5.Again, results oflarger trials, apparently negative (from presentations inabstract form), have not yet been published. It is of notethat IL-5 mRNA could be detected in peripheral bloodT cells from children,9 and it is possible that eosinophilsmay play a more important role in childhood asthmathan in adults, where airway remodeling may be morepronounced. There are no reported studies of anti-IL-5treatment of childhood asthma. As in adult severe asthma,it was suggested that there may be different subgroupsof children with severe asthma.7,31–33 In particular, it maybe of interest to study anti-IL-5 therapy in those childrenwith severe asthma and evidence of persistent airwayeosinophil infiltration despite compliance with steroidtreatment.
ANTI-TNF
Tumor necrosis factor-a is a proinflammatory cytokine,which activates macrophages and increases adhesionmolecule and chemokine expression in many inflamma-tory settings. Soluble receptor therapy has shown dramaticbenefit in rheumatoid arthritis and inflammatory boweldisease, and TNFa expression is increased in the airway inasthma,33 although it is of note that other anti-inflamma-tory agents effective in arthritis have not always shownefficacy in asthma. Nonetheless, a recent open-label study(reported in abstract form only) suggested an ability toimprove lung function and reduce asthma symptoms insevere asthmatics dependent on oral steroids,34 and furthertrials in severe asthma are awaited.
OTHER CYTOKINES
Although anti-TNF therapy may be promising, resultsfrom interventions based on IL-4 and IL-5 have been
disappointing. This has led some to conclude that singlecytokine targets are unrealistic. However, such pessimismwould seem premature, and results from targeting IL-13are eagerly awaited. Another approach was to usecytokines that might turn off the Th2-driven immuneprocess in asthma, such as IL-12 which favors Th1responses, or IL-10 which inhibits activation of both Th1and Th2 cells. However, initial studies of IL-12 showed noclinical effect despite reduction in sputum eosinophilia,35
and studies of IL-10 have not been published: a moreuseful and viable approach might be to redirect theimmune response away from the Th2 pathway, as dis-cussed below.
Chemokines are small chemotractant cytokines, initi-ally described as acting to recruit specific cell types to sitesof inflammation. These have cell specificity, and also act inotherways such as cell activation and degranulation. Sincethey use 7-trans-membrane spanning receptors, similarto b adenoceptors, small molecule antagonists are beingdeveloped in work largely driven by the identificationof chemokine receptors as coreceptors for HIV infection.In particular, chemokine receptor 3 (CCR3) is expressedby eosinophils, Th2 cells, mast cells, and basophils, and isanother future target for asthma therapy.36
IMMUNOTHERAPY FOR ASTHMA
Allergen immunotherapy was first described in 1911and consists of injecting increasing doses of allergen ex-tract subcutaneously into sensitized allergic patients.Frankland and Augustin confirmed the efficacy of grasspollen immunotherapy for severe summer hayfever in aplacebo-controlled study in 1954,37 and this was subse-quently confirmed in more recent trials, including thedemonstration that a 3-year course of such treatment gaveeffective symptom control for at least 3 years after dis-continuing treatment.38 Allergen immunotherapy is effec-tive for allergic asthma,39–41 although current evidence isonly for those with seasonal asthma to one pollen allergenor predominant house dust-related symptoms, and therehas been no comparative study with inhaled corticoster-oids. The treatment is used widely in the USA, but iscurrently contraindicated for asthma in the UK becausesurveys suggested that asthmatics were most at risk fordeaths associated with this therapy.42,43 Such risks resultfrom the ability of the allergen extract given to sensitizedpatients to cross-link IgE, leading to anaphylaxis or severeasthma attacks: such risk is rare and controllable in aspecialist hospital setting, but greatly restricts the use ofthis treatment (it is currently licensed in the UK only forbee and wasp venom anaphylaxis, and not for hayfever orother allergic disease). Nonetheless, allergen immu-notherapy offers the prospect of disease-modifyingtreatment for allergic disease in contrast to current drugs,which suppress inflammation. A number of strategies are
372 Robinson

being explored to modify the regimen and thus reduce theanaphylactic potential. In addition, some of the agentsused to modify allergen immunotherapy may have thepotential to reset allergic asthmatic Th2 immune re-sponses by themselves, in concordance with natural aller-gen exposure. Although some of these approaches havebeen used in initial trials, results are preliminary, and itwill be some years before any such approach findsapplication in the clinic.
MODIFICATION OF ALLERGEN
Since the benefit of AII is thought to result fromresetting of the immune response away from a Th2 profiletowards either Th1 or a suppressive regulatory T-cell re-sponse (in which IL-10 and/or TGFb may be importantsuppressive effector cytokines), whereas side effects resultfrom cross-linking IgE, a number of approaches seek toreduce the potential for interaction with IgE whilepreserving T-cell reactivity. Most well-established ischemical modification to produce allergoids:44 such ex-tracts have been used but tend to have reduced potency, yetretain some IgE reactivity. Another approach is togenetically modify allergen molecules to reduce IgEbinding potential: such recombinant allergens have to datebeen tested in model systems only.45 A third idea is touse peptides from allergen molecules, thus disrupting thethree-dimensional structure important for most IgEbinding, yet preserving T-cell reactivity.46 Initial studieswith Allervax catTM (two peptides derived from the majorcat allergen, Fel d1) showed some clinical efficacy in catallergic asthmatics, but these peptides were relativelylong, and some immediate hypersensitivity side effectsremained.47 Subsequent studies used smaller peptidesfrom the cat allergenmolecule Fel d1 that do not cross-linkIgE, and showed the ability of such immunotherapy toreduce the skin early and late response to cat allergen, andmodification of the in vitro T-cell response away fromTh2 (and Th1) cytokines towards IL-10 production.48 Asimilar approach was reported for bee venom. Onepotential problem is that T cell-dependent late-asthmaticreactions were described following peptide injection:whether such potential side effects can be avoided remainsto be seen.49
If switching to a Th1 or Treg response is the key effectof allergen immunotherapy, another approach to improv-ing therapy is to couple allergen to, or coadminister withallergen, agents that favor Th1 or Treg responses.Immunostimulatory DNA sequences (ISS) are nonmethy-lated DNA sequences derived from bacterial DNAsequences which interact with a specific pattern recogni-tion receptor of innate immune cells such as dendritic cellsand macrophages called Toll-like receptor 9 (TLR9).TLR9 activation leads to production of either IL-12 orIFN-a, both of which favor Th1 responses and can reduce
Th2 responses.50 Initial results of a vaccine using ISSconjugated to the ragweed allergen, Amb a1, for ragweedhayfever were reported in abstract form to show areduction in symptom scores after six injections givenbefore ragweed season.51 Such conjugation of ISS to theallergen has the additional benefit of reducing theinteraction of the allergen with IgE by simply blockingthe IgE-binding epitopes. However, such engineeredallergen vaccines will be expensive and highly specificfor a single allergen molecule. There is therefore interestin using ISS, or other immune modulating agents such asheat-killed Mycobacterium vaccae, alone and relyingon natural allergen exposure in the lung to switch offairway allergen-specific Th2 responses. Certainly datafrom animal experiments are encouraging.52 One study ofM. vaccae in 24 mild asthmatics showed a nonsignificantreduction in the late asthmatic response, serum IgE, andIL-5 to allergen challenge.53 Clearlymuchmoreworkwillbe required before it is known whether immunomodula-tion of asthma has any potential for asthma therapy, and ifso, who might benefit, but this concept holds the potentialfor a novel disease-modifying treatment.
PREVENTION
There is increasing interest in the causes of the increasein asthma prevalence across Western societies, and inparticular how this might be prevented. If genetic andepidemiological studies allow the firm identification ofchildren at risk, preventive strategies may becomeattractive. A number of studies suggested that allergenimmunotherapy can reduce the development of newallergen sensitivities in children with existing pollen orhouse dust mite allergy,54 and the recent PAT studysuggested that allergen immunotherapy for grass or treepollen in children with rhinitis could reduce the incidenceof asthma over the 3 years of treatment.55 If allergenimmunotherapy can be simplified and shown to be safe inboth the short and long term, such a preventive approachmay become feasible.
REFERENCES
1. British guideline on the management of asthma. Thorax [Suppl]
2003;58:1–83.
2. Kay AB. Allergy and allergic diseases. N Engl J Med 2001;344:
30–37, 109–113.
3. BusseWW, Lemanske RF. Asthma. N Engl J Med 2001;344:350–
362.
4. Mosmann TR, Cherwinski H, Bond MW, Giedlin MA, Coffman
RL. Two types of murine helper T cell clone. I. Definition
according to profiles of lymphokine activities and secreted
proteins. J Immunol 1986;136:2348–2357.
5. Humbert M, Menz G, Ying S, Corrigan CJ, Robinson DS, Durham
SR, Kay AB. The immunopathology of extrinsic (atopic) and
intrinsic (non-atopic) asthma: more similarities than differences.
Immunol Today 1999;20:528–533.
New Therapies for Asthma 373
6. Krawiec ME, Westcott JY, Chu HW, Balzar S, Trudeau JB,
Schwartz LB, Wenzel SE. Persistent wheezing in very young
infants is associated with lower respiratory inflammation. Am.J
Respir Crit Care Med 2001;163:1338–1343.
7. Stevenson EC, Turner G, Heaney LG, Schock BD, Taylor R,
Gallagher T, Ennis M, Shields MD. Bronchoalveolar lavage
findings suggest two different forms of childhood asthma. Clin
Exp Allergy 1997;27:1027–1035.
8. Gemou-Engesaeth V, Kay AB, Bush A, Corrigan CJ. Activated
peripheral blood CD4 and CD8 T-lymphocytes in child asthma:
correlation with eosinophilia and disease severity. Pediatr Allergy
Immunol 1994;5:170–177.
9. Gemou-Engesaeth V, Bush A, Kay AB, Hamid Q, Corrigan CJ.
Inhaled glucocorticoid therapy of childhood asthma is associated
with peripheral blood T cell activation and Th2-type cytokine
mRNA expression. Pediatrics 1997;99:695–703.
10. Busse WW. Anti-immunoglobulin E (omalizumab) therapy
in allergic asthma. Am J Respir Crit Care Med 2001;164:
12–17.
11. Fahy JV, Fleming HE, Wong HH, Liu JT, Su JQ, Reimann J, Fick
RB Jr, Boushey HA. The effect of an anti-IgE monoclonal
antibody on the early- and late-phase responses to allergen
inhalation in asthmatic subjects. Am J Respir Crit Care Med 1997;
155:1828–1834.
12. Milgrom H, Berger W, Nayak A, Gupta N, Pollard S, McAlary M,
Fowler-Taylor A, Rohane P. Treatment of childhood asthma
with anti-immunogolbulin E antibody (omalizumab). Pediatrics
2001;108:E36.
13. Lemanske RF, Nayak A, McAlary M, Everhard F, Fowler-Taylor
A, Gupta N. Omalizumab improves asthma-related quality of life
in children with allergic asthma. Pediatrics 2002;110:E55.
14. Busse WW, Corren J, Lanier Q, McAlary M, Fowler-Taylor A,
Della Chioppa G, van As A, Gupta N. Omalizumab, anti-IgE
recombinant humanised monoclonal antibody, for the treatment
of severe allergic asthma. J Allergy Clin Immunol 2001;108:184–
190.
15. Soler M, Matz J, Townley R, Buhl R, O’Brien J, Fox H, Thirwell
J, Gupta N, Della Chioppa G. The anti-IgE antibody omalizumab
reduces exacerbations and steroid requirements in allergic
asthmatics. Eur Respir J 2001;18:254–261.
16. Buhl R, Soler M, Matz J, Townley R, O’Brien J, Noga O,
Champain K, Fox H, Thirwell J, Della Chioppa G. Omalizumab
provides long-term control in patients with moderate to severe
allergic asthma. Eur Respir J 2002;20:73–78.
17. Walker S, Monteil M, Lasserson T, Phelan K, Walters H. Anti-IgE
for chronic asthma. The Cochrane Library; Issue 3, 2003. Oxford:
Update Software.
18. Leung DYM, Sampson HA, Yuninger JW, Burks AW, Schneider
LC, Wortel CH, Davis FM, Hyun JD, Shanahan WR. Effect of
anti-IgE therapy in patients with peanut allergy. N Engl J Med
2003;348:986–993.
19. Lloyd CM, Gonzalo JA, Coyle AJ, Gutierrez-Ramos JC. Mouse
models of allergic airway disease. Adv Immunol 2001;77:263–
295.
20. Borish LC, Nelson HS, Lanz MJ, Claussen L, Whitmore JB,
Agosti JM, Garrison L. Interleukin-4 receptor in moderate atopic
asthma. A phase I/II randomized, placebo-controlled trial. Am J
Respir Crit Care Med 1999;160:1816–1823.
21. Borish LC, Nelson HS, Corren J, Bensch G, Busse WW,
Whitmore JB, Agosti JM, IL-4R Asthma Study Group. Efficacy
of soluble IL-4 receptor for the treatment of adults with asthma. J
Allergy Clin Immunol 2001;107:963–970.
22. Hart TK, Blackburn MN, Brigham-Burke M, Dede K, Al-Mahdi
N, Zia-Amirhosseini P, Cook RM. Preclinical efficacy and safety
of paascolizumab (SB 240683): a humanised anti-interleukin 4
antibody with therapeutic potential in asthma. Clin Exp Immunol
2002;130:93–100.
23. Wills-Karp M, Luyimbazi J, Xu X, Schofield B, Neben TY, Karp
CL, Donaldson DD. Interleukin-13: central mediator of allergic
asthma. Science 1998;282:2258–2261.
24. Grunig G, Warnock M, Wakil AE, Venkayya R, Brombacher F,
Rennick DM, Sheppard D, Mohrs M, Donaldson DD, Locksley
RM, Corry DB. Requirement for IL-13 independently of IL-4 in
experimental asthma. Science 1998;282:2261–2263.
25. Leckie MJ, ten Brinke A, Khan J, Diamant Z, O’Connor BJ,
Walls CM, Mathur AK, Cowley HC, Chung KF, Djukanovic R,
Hansel TT, Holgate ST, Sterk PJ, Barnes PJ. Effects of an
interleukin-5 blocking monoclonal antibody on eosinophils,
airway hyper-responsiveness, and the late asthmatic response.
Lancet 2000;356:2144–2148.
26. Kips JC, Brian OJ, Langley SJ, Woodcock A, Kerstjens HA,
Postma DS, Danzig M, Cuss F, Pauwels RA. The effect of
SCH55700, a humanized anti-hIL-5 antibody in severe persis-
tent asthma: a pilot study. Am J Respir Crit Care Med 2003;
e-publication ahead of print.
27. Flood-Page PT, Menzies-Gow AN, Kay AB, Robinson DS.
Eosinophil’s role remains uncertain as anti-interleukin-5 only
partially depletes numbers in asthmatic airway. Am J Respir Crit
Care Med 2003;167:199–204.
28. Menzies-Gow A, Flood-Page P, Sehmi R, Burman J, Hamid Q,
Robinson DS, Kay AB, Denburg J. Anti-IL-5 (mepolizumab)
therapy induces bone marrow eosinophil maturational arrest and
decreases eosinophil progenitors in the bronchial mucosa of
atopic asthmatics. J Allergy Clin Immunol 2003;111:714–719.
29. Gregory B, Kirchem A, Phipps S, Gevaert P, Pridgeon C,
Rankin SM, Robinson DS. Differential regulation of human
eosinophil IL-3, IL-5 and GM-CSF receptor alpha chain expres-
sion by cytokines: IL-3, IL-5 or GM-CSF down regulate IL-5Raexpression with loss of IL-5 responsiveness, but up-regulate IL-
3Ra expression. J Immunol 2003;170:5359–5366.
30. Liu LY, Sedgwick JB, Bates ME, Vrtis RF, Gern JE, Kita H,
Jarjour NN, Busse WW, Kelly EA. Decreased expression of
membrane IL-5 receptor alpha on human eosinophils: I. Loss of
membrane IL-5 receptor alpha on airway eosinophils and
increased soluble IL-5 receptor alpha in the airway after allergen
challenge. J Immunol 2002;169:6452–6458.
31. Wenzel SE, Schwartz LB, Langmack EL, Halliday JL, Trudeau
JB, Gibbs RL, Chu HW. Evidence that severe asthma can be
divided pathologically into two inflammatory subtypes with
distinct physiologic and clinical characteristics. Am J Respir Crit
Care Med 1999;160:1001–1008.
32. Payne DNR, Adcock IM, Wilson NM, Oates T, Scallan M,
Bush A. Relationship between exhaled nitric oxide and mucosal
eosinophilic inflammation in children with difficult to treat
asthma, after treatment with oral prednisolone. Am J Respir Crit
Care Med 2001;164:1376–1381.
33. Ying S, Robinson DS, Varney V, Meng Q, Tsicopoulos A,
Moqbel R, Durham SR, Kay AB, Hamid Q. TNF alpha mRNA
expression in allergic inflammation. Clin Exp Allergy 1991;21:
745–750.
34. Babu K, Arshad SH, Howarth PH, Chauhan AJ, Bell EJ,
Puddicombe S, Davies DE, Holgate ST. Soluble tumor necrosis
factor alpha (TNF-alpha) receptor (Enbrel) as effective therapeu-
tic strategy in chronic severe asthma. J Allergy Clin Immunol
2003;111:838.
35. Bryan SA, O’Connor BJ, Matti S, Leckie MJ, Kanabar V, Khan J,
Warrington SJ, Renzetti L, Rames A, Bock JA, Boyce MJ, Hansel
TT, Holgate ST, Barnes PJ. Effects of recombinant human
interleukin-12 on eosinophils, airway hyper-responsiveness, and
the late asthmatic response. Lancet 2000;356:2149–2153.
374 Robinson

36. Menzies-Gow A, Robinson DS. Eosinophil chemokines and their
receptors: an attractive target in asthma? Lancet 2000;355:1741–
1743.
37. Frankland AW, Augustin R. Prophylaxis of summer hayfever and
asthma. A controlled trial comparing crude grass pollen extracts
with the isolated main protein component. Lancet 1954;i:1055–
1057.
38. Durham SR, Walker SM, Varga EM, Jacobson MR, O’Brien F,
Noble W, Till SJ, Hamid QA, Nouri-Aria KT. Long-term efficacy
of grass pollen immunotherapy. N Engl J Med 1999;341:468–
475.
39. Walker SM, Pajno GB, Torres Lima M, Wilson DR, Durham SR.
Grass pollen immunotherapy for seasonal rhinitis and asthma: a
randomised, controlled trial. J Allergy Clin Immunol 2001;107:
87–93.
40. Creticos PS, Reed CE. Ragweed immunotherapy in adult asthma.
N Engl J Med 1996;334:501–506.
41. Abramson M, Puy R, Weiner J. Immunotherapy in asthma: an
updated systematic review. Allergy 1999;54:1022–1041.
42. Committee on Safety of Medicines/Medicines Control Agency.
Desensitising vaccines. Br Med J [Clin Res] 1986;293:948.
43. Reid MJ, et al. Survey of fatalities from skin testing and
immunotherapy 1985–1989. J Allergy Clin Immunol 1993;92:6–
15.
44. Tari MG, Mancino M, Ghezzi E, Frank E, Cromwell O.
Immunotherapy with an alum-adsorbed Parietaria-pollen aller-
goid: a 2-year, double-blind, placebo-controlled study. Allergy
1997;52:65–74.
45. Valenta R. The future of antigen-specific immunotherapy of
allergy. Nat Rev Immunol 2002;2:446–453.
46. Larche M. Inhibition of human T-cell responses by allergen
peptides. Immunology 2001;104:377–382.
47. Norman PS, Ohman JL Jr, Long AA, Creticos PS, Gefter MA,
Shaked Z, Wood RA, Eggleston PA, Hafner KB, Rao P,
Lichtenstein LM, Jones NH, Nicodemus CF. Treatment of cat
allergy with T-cell reactive peptides. Am J Respir Crit Care Med
1996;154:1623–1628.
48. Oldfield WLG, Larche M, Kay AB. Effect of T cell peptides
derived from Fel d1 on allergic reactions and cytokine production
in patients sensitive to cats: a randomised controlled trial. Lancet
2002;360:47–53.
49. Haselden BM, Kay AB, Larche M. Immunoglobulin E-indepen-
dent major histocompatibility complex-restricted T cell peptide
epitope-induced late asthmatic reactions. J Exp Med 1999;189:
1885–1894.
50. Horner AA, Raz E. Immunostimulatory sequence oligonucleo-
tide-based vaccination and immunomodulation: two unique but
complimentary strategies for the treatment of allergic diseases.
J Allergy Clin Immunol 2002;110:706–712.
51. Creticos PS, Lighvani SS, Bieneman AP, Balcer-Whaley SL,
Norman PS, Lichtenstein LM, Schroeder JT. Enhanced IL-10
secretion by PBMC during the ragweed season: effect of AIC
immunotherapy vs placebo. J Allergy Clin Immunol 2003;
111:530.
52. Zuany-Amorim C, Sawicka E, Manlius C, Le Moine A,
Brunet LR, Kemeny DM, Bowen G, Rook G, Walker C.
Suppression of airway eosinophilia by killed Mycobacterium
vaccae-induced allergen-specific regulatory T-cells. Nat Med
2002;8:625–629.
53. Camporota L, Corkhill A, Long H, Lordan J, Stanciu L, Tuckwell
N, Cross A, Stanford JL, Rook GAW, Holgate ST, Djukanovic R.
The effects ofMycobacterium vaccae on allergen-induced airway
responses in atopic asthma. Eur Respir J 2003;21:287–293.
54. Des Roches A, Paradis L, Menardo JL, Bouges S, Daures JP,
Bousquet J. Immunotherapy with a staandradised Dematopha-
goides pteronyssinus extract. VI. Specific immunotherapy pre-
vents the onset of new sensitisations in children. J Allergy Clin
Immunol 1997;99:450–453.
55. Moller C, Dreborg S, Ferdousi HA, Halken S, Host A, Jaconsen L,
Koivikko A, Koller DY, Niggeman B, Norberg LA, Urbanek R,
Valovirta E, Wahn U. Pollen immunotherapy reduces the develop-
ment of asthma in children with seasonal rhinoconjunctivitis (the
PAT study). J Allergy Clin Immunol 2002;109:251–256.
New Therapies for Asthma 375





























