Embed Size (px)
DESCRIPTION
New-generation drug-eluting stents and dual antiplatelet therapy : overview. Giuseppe Biondi Zoccai, MD Department of Medico-Surgical Sciences and Biotechnologies Sapienza University of Rome , Rome , Italy [email protected]. Our original sin…. - PowerPoint PPT Presentation
Citation preview

New-generation drug-eluting stents and dual antiplatelet
therapy: overview
Giuseppe Biondi Zoccai, MDDepartment of Medico-Surgical Sciences and Biotechnologies
Sapienza University of Rome, Rome, [email protected]
Our original sin…

An ongoing challenge after stenting: preventing both…
THROMBOSIS
BLEEDING

Choice of aspirin was empirical from the beginning…
In the first reported case of PTCA by Andreas Gruentzig, 3 days of aspirin was empirically added to heparin therapy
Gruentzig et al. NEJM 1979

Addition of ticlopidine after stentingwas empiric at first and then
confirmed by more sound data
Serruys Roubin Schatz Fishman Colombo Leon0
5
10
15
20
25
30
24
7.66
3.51.4 0.5
30-d
ay s
tent
th
rom
bosi
s ra
te (%
)
ASA
ASA plus OAC
DAPT

The CREDO RCT of 1- vs 12-month* DAPT:1-year death, MI and stroke
Steinhubl et al. JAMA 2002*1-month regimen did not include clopidogrel front-loading

The PCI-CURE RCT of 0- vs 12-month DAPT:1-year CV death or MI
Mehta et al. Lancet 2001
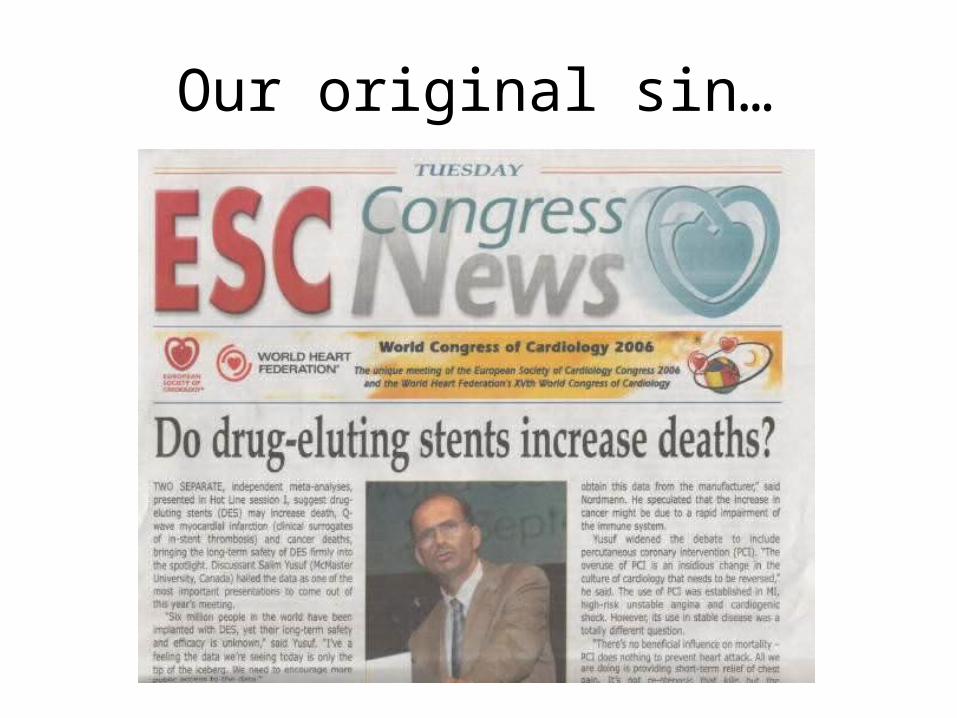
The TRITON RCT of 6- to 15-month* DAPT with clopidogrel vs prasugrel: stent thrombosis†
Wiviott et al. Lancet 2008*median 14.5 months; †definite or probable

The PLATO RCT of 6- to 12-month* DAPT with clopidogrel vs ticagrelor: stent thrombosis†
Cannon et al. Lancet 2010*median 9.3 months; †definite, probable or possible

Cannon et al. Lancet 2010*median 14.5 months
The PLATO RCT of 6- to 12-month* DAPT with clopidogrel vs ticagrelor: all cause death

The Duke observational study with CYPHER and TAXUS: 2-year events
Eisenstein et al. JAMA 2005

The VA observational study with CYPHER and TAXUS: events after discontinuing DAPT
Ho et al. JAMA 2008

The J-CYPHER observational study: 2-year stent thrombosis
Kimura et al. Circulation 2009
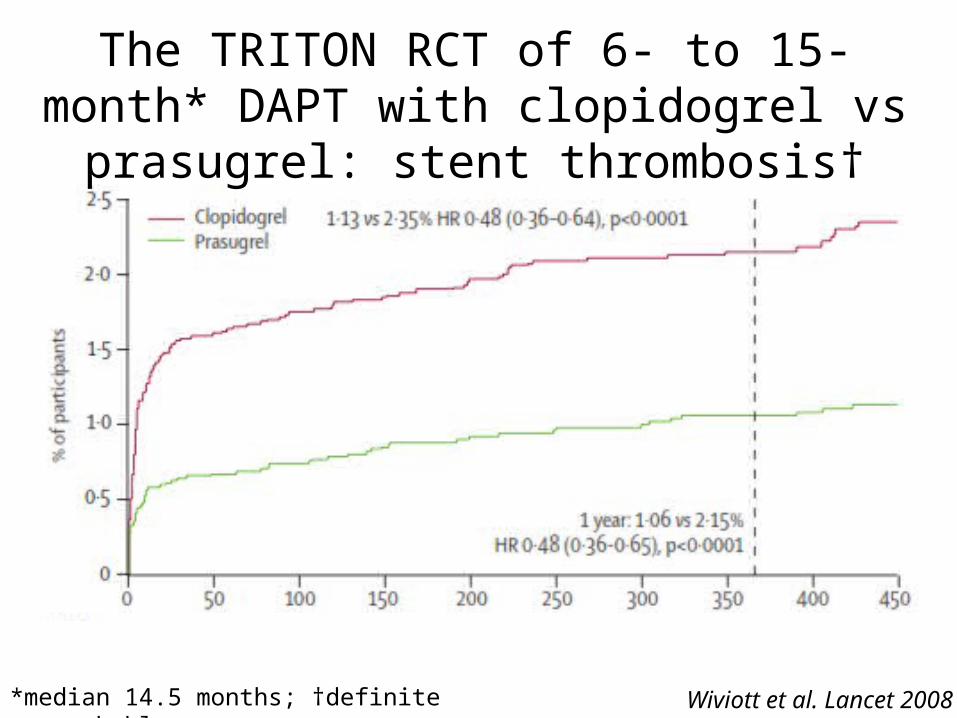
The Milan-Naples-Siegburg observational study with TAXUS and CYPHER
Airoldi et al. Circulation 2007

The LATE RCTs of 12- vs 24-month DAPT:2-year death, MI and stroke
Park et al. NEJM 2010

The PRODIGY RCT of 6- vs 24-month DAPT:2-year death, MI and stroke
Valgimigli et al. Circulation 2012

The PRODIGY RCT of 6- vs 24-month DAPT:2-year type II, III, or V BARC bleeding
Valgimigli et al. Circulation 2012
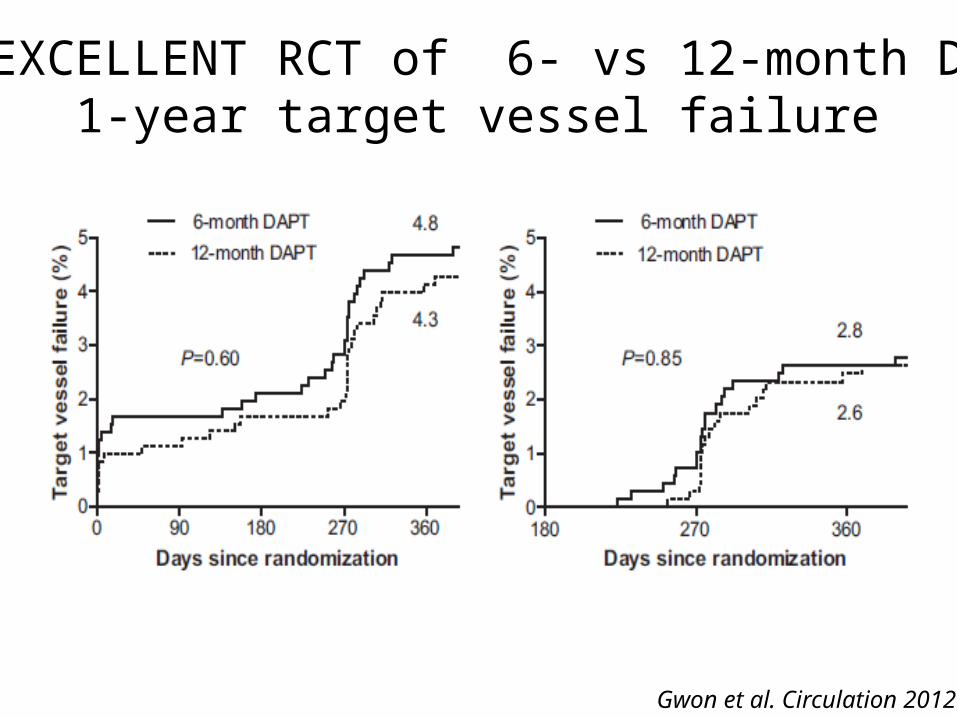
The EXCELLENT RCT of 6- vs 12-month DAPT:1-year target vessel failure
Gwon et al. Circulation 2012

The EXCELLENT RCT of 6- vs 12-month DAPT:other 1-year events
Gwon et al. Circulation 2012

Study Sample Size
DAPT (months)
Stent type
ITALIC 3,750 0 (ASA only) vs 6
EES
OPTIMIZE 3,120 3 vs 12 ZESISAR-SAFE 6,000 6 vs 12 DESDAPT 20,645 12 vs 30 DES (n=15,245) /
BMS (n=5,400)DES Late 5,000 12 vs >12 DESSCORE 280 12 vs 24 DESOPTIDUAL 1,966 12 vs 36 DES
Uncertainty will persist for some time: ongoing studies on DAPT

2010: ESC Guidelines on PCI/CABG

2011: ESC Guidelines on NSTEACS

The XIENCE V USA study including 5,054 unselected real-world patients
Hermiller, PCR 2010
AMI 18.1%
ACS 37.5%
Renal Insufficiency 11.1%
Multivessel Disease 40.8%
EF < 30% 3.4%
Multivessel Treated 13.8%
Left Main 1.6%
Graft Lesion 4.8%
CTO Lesion 2.5%
Direct Stenting 38.7%
Restenosis Lesion 9.5%
Ostial 11.9%
Bifurcation 9.0%
Diabetes 35.6%
A Real-World Population

The XIENCE USA study: DAPT details
Hermiller, PCR 2010
Temporary Interruption % (N) 5.6% (N = 243)
Number of Interruptions 1.1 ± 0.5 (N = 243)
Days to First Interruption (days) 134.3 ± 121.4 (N = 243)
Duration of Interruption (days) 20.3 ± 46.9 (N = 243)
Top 3 Reasons for Interruption Surgical Procedure = 35.4%Adverse Event** = 30.5%Patient Non-compliance = 9.5%
Permanent Discontinuation % (N) 8.5% (N = 366)
Days to Discontinuation (days) 239.2 ± 140.4 (N = 366)
Top 3 Reasons for Discontinuation Adverse Event** = 21.9%Surgical Procedure = 10.7%Increased Bleeding Risk = 9.6%

The XIENCE USA study: stent thrombosis according to DAPT interruption
Hermiller, PCR 2010

Study Patients Design SettingSPIRIT II 223 RCT On-labelSPIRIT III 669 RCT On-labelSPIRIT IV 2458 RCT On-labelSPIRIT V 1662 Non-RCT Real-world settingSPIRIT Women 1506 Non-RCT Real-world settingXIENCE V USA 3770 Non-RCT Real-world settingXIENCE V India 931 Non-RCT Real-world setting
Stone, TCT 2011
The SPIRIT/XIENCE pooled analysis on 11,219 patients: included studies

Stone, TCT 2011
The SPIRIT/XIENCE pooled analysis on 11,219 patients: 2-year stent thrombosis

Stone, TCT 2011
The SPIRIT/XIENCE pooled analysis on 11,219 patients: compliance to DAPT

The SPIRIT/XIENCE pooled analysis on 11,219 patients: stent thrombosis according to DAPT
Stone, TCT 2011
0.0
1.0
2.0
3.0
4.0
5.0ST
thro
ugh
2 ye
ars
(%)
No DAPT Interruption
DAPT Interruption within 90 Days
DAPT Interruption after 90 Days
0.66% 0.69%
2.61%
44/6648 16/613 23/3314
Timing of First DAPT Interruption and ALL Stent Thrombosis (ARC Definite/Probable)
Through 2 Years
No DAPT interruption
DAPT interruption
within 90 days
DAPT interruption after 90 days

The SPIRIT/XIENCE pooled analysis on 11,219 patients: days of DAPT discontinuation
Stone, TCT 2011

The SPIRIT/XIENCE pooled analysis on 11,219 patients: stent thrombosis according to DAPT
Stone, TCT 2011
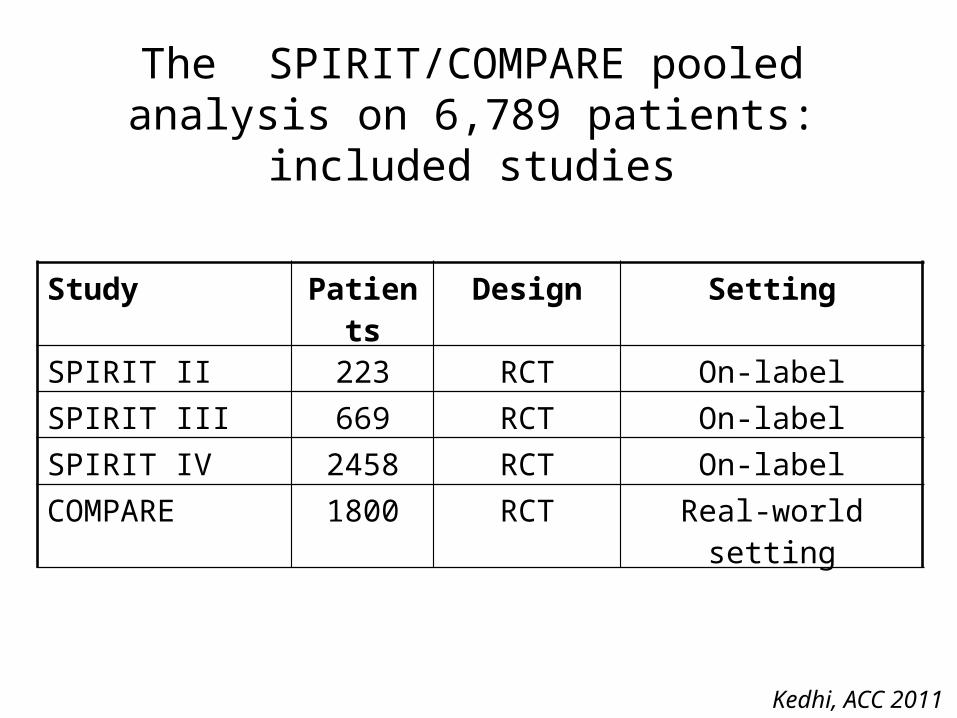
The SPIRIT/COMPARE pooled analysis on 6,789 patients: included studies
Kedhi, ACC 2011
Study Patients Design SettingSPIRIT II 223 RCT On-labelSPIRIT III 669 RCT On-labelSPIRIT IV 2458 RCT On-labelCOMPARE 1800 RCT Real-world setting

Kedhi, ACC 2011
1-6 mo DAPT
>24 moDAPT
6-12 moDAPT
12-24 moDAPT
The SPIRIT/COMPARE pooled analysis on 6,789 patients: stent thrombosis according to DAPT

The SPIRIT/XIENCE meta-analysis on 10,615 patients: included studies
Palmerini, PCR 2012
Study Patients Design SettingSPIRIT V 1662 Non-RCT Real-world settingSPIRIT Women 1506 Non-RCT Real-world settingXIENCE V USA 3770 Non-RCT Real-world settingXIENCE V India 931 Non-RCT Real-world setting
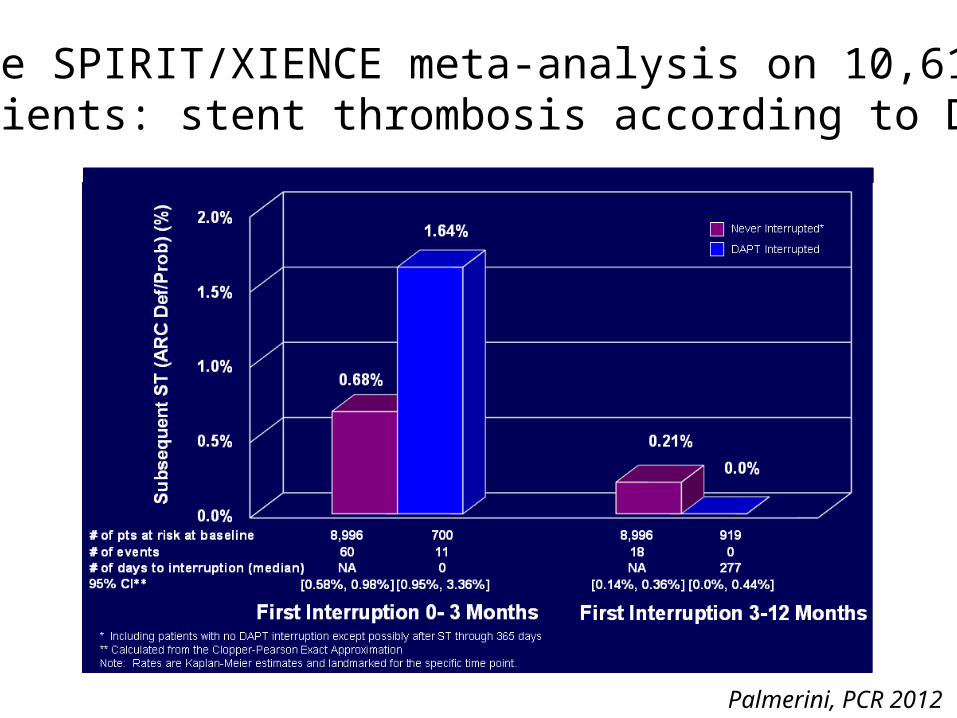
The SPIRIT/XIENCE meta-analysis on 10,615 patients: stent thrombosis according to DAPT
Palmerini, PCR 2012

CE mark indication for XIENCE 3-month DAPT
Language from CE IFU Section 8.1 for XIENCE:XIENCE demonstrated low stent thrombosis rates in patients who either discontinued or interrupted Dual Antiplatelet Therapy (DAPT) after 3 months post stent implantation. It is therefore recommended that patients treated with XIENCE stents remain on DAPT for at least 3 months after stent implantation.
New indication underlines the XIENCE safety outcomes even when patients interrupt DAPT
after 3 months

Mega-Meta AnalysisST & DAPT Interruption
at 3 Months2
7 XIENCE Trials (n=13,259)
ST rate after DAPT interruption beyond 3 months was low and numerically similar to no DAPT interruption
through 2 years
Real World Pooled Analysis:
3 Months DAPT Analysis3
All Comer Population 4 XIENCE Trials
(n=10,615)
XIENCE shows 0% ST after DAPT interruption
from 3 to 12 months
3 Months DAPT CE Submission Data
Source: 1. Based on data from the XIENCE V USA trial (Hermiller PCR 2012). 2. Based on data from the Mega-Meta Analysis of 7 XIENCE trials (Stone, TCT 2011). 3. Based on data from SPIRIT/XIENCE analysis (Palmerini PCR 2012).
XIENCE V USAST and DAPT Interruption at 3 Months1
All Comer Population (n=5,054)
ST rate after DAPT interruption beyond 3 months was low and
numerically similar to no DAPT
interruption through 1 year
PCR 2012
CE mark indication for XIENCE 3-month DAPT

Additional insights from a comprehensive network meta-analysis
Palmerini, Biondi-Zoccai et al, Lancet 2012

Evidence network9 studies PESBMS
SESEnd-ZES
Res-ZES PtCr-EES
CoCr-EES1 study
8 studies1 stu
dy4 stu
dies 9 studies
6 studies
6 studies
2 studies
2 studies 5 st
udie
s
Palmerini, Biondi-Zoccai et al, Lancet 2012
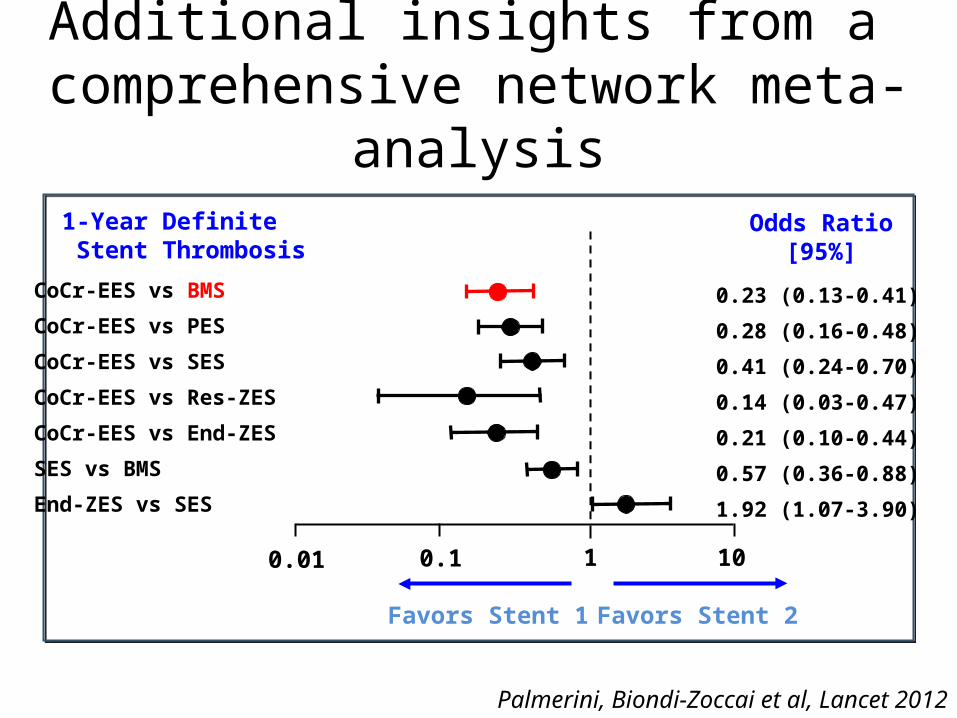
Additional insights from a comprehensive network meta-analysis
Odds Ratio[95%]
CoCr-EES vs BMS
CoCr-EES vs PES
CoCr-EES vs SES
CoCr-EES vs Res-ZES
CoCr-EES vs End-ZES
SES vs BMS
End-ZES vs SES
0.23 (0.13-0.41)
0.28 (0.16-0.48)
0.41 (0.24-0.70)
0.14 (0.03-0.47)
0.21 (0.10-0.44)
0.57 (0.36-0.88)
1.92 (1.07-3.90)
Favors Stent 1 Favors Stent 2
1010.10.01
Palmerini, Biondi-Zoccai et al, Lancet 2012
1-Year Definite Stent Thrombosis

Statistical consistency
IV = inverse varianceSE = standard error
Odds Ratio IVRandom, 95% CI
1010.10.001
Favors CoCr-EES Favors BMS
WeightSELog (odds ratio)
Definite stent thrombosisDirect estimateIndirect estimateTotal (95% CI)Test for overall effect Z=4.82 (p<0.00001)
Definite or probable thrombosisDirect estimateIndirect estimateTotal (95% CI)Test for overall effect Z=4.48 (p<0.00001)
-1.427-1.421
-0.968-1.122
0.5190.359
0.3770.304
32.4%67.6%
100.00%
39.4%60.6%
100.00%
0.24 (0.09-0.66)0.24 (0.12-0.49)0.24 (0.14-0.43)
0.38 (0.18-0.80)0.33 (0.18-0.53)0.35 (0.22-0.55)
Statistical inconsistency (I2): 0% for both comparisons
Palmerini, Biondi-Zoccai et al, Lancet 2012
• Statistical consistency or homogeneity is a measure of how similar are the estimates stemming from head-to-head RCTs and the indirect comparison

Other new-degeneration DES
Raber et al, JAMA 2012

Other new-degeneration DES
Raber et al, JAMA 2012

Prototypical clinical cases

The Good: ↓ risk of TLRand↓ risk of bleeding with long-term DAPT
46-year-old with effort angina: RCA as culprit♂

The Bad: ↑risk of TLR but↓ risk of bleeding with long-term DAPT
61-year-old ♀ with STEMI: LAD as culprit

The Ugly: ↑risk of TLR and ↑ risk of bleeding with long-term DAPT
74-year-old with NSTEMI & AF requiring oral ♂anticoagulants: LM-LAD as culprit

Take home messages• DAPT aims to prevent two different events: stent
thrombosis and non-target lesion thrombosis.• Long-term DAPT reduces the risk of non-target
lesion events.• However, there is mounting uncertainty on the
impact of long-term DAPT on stent thrombosis.• EES have a unique safety profile among coronary
stents:– After 3 months, patients with EES discontinuing DAPT
have a risk of stent thrombosis similar to those not discontinuing;
Take home messages– Accordingly, 3-month DAPT appears adequate to reduce the
risk of stent thrombosis in patients receiving EES;– Favorable yet much less thorough results have also been
reported for BES.• I personally do not recommend 3-month DAPT in all
patients, but surely do in carefully selected ones.• Moreover, I can be truly confident that any of my
patients who has received a EES and discontinue DAPT ≥3 months is not put at a higher risk of stent thrombosis.
• This property cannot so far be inferred for any other DES, and thus makes EES a unique treatment opportunity to maximize efficacy and safety.

Thank you for your attention
For any correspondence: [email protected]
For these and further slides on these topics feel free to visit the metcardio.org website: http://www.metcardio.org/slides.html
Meta-analysis and Evidence-based medicine Training in Cardiology














![Journal Papers [1-44] - biosensors.com · Polymer-Based Biolimus-Eluting Stents Versus Durable Polymer-Based Sirolimus-Eluting Stents in Patients With Coronary Artery Disease: Final](https://img.dokumen.tips/doc/110x75/5fae34968d5e227c587bb762/journal-papers-1-44-polymer-based-biolimus-eluting-stents-versus-durable-polymer-based.jpg)